Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 15
No Influence on Cardiac Arrhythmia or Heart Rate from Long-Term Treatment with Tiotropium/Olodaterol versus Monocomponents by Holter ECG Analysis in Patients with Moderate-to-Very-Severe COPD
Authors Andreas S ![]() , Bothner U, de la Hoz A, Kloer I, Trampisch M, Alter P
, Bothner U, de la Hoz A, Kloer I, Trampisch M, Alter P ![]()
Received 17 January 2020
Accepted for publication 20 April 2020
Published 10 August 2020 Volume 2020:15 Pages 1945—1953
DOI https://doi.org/10.2147/COPD.S246350
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Stefan Andreas,1,2 Ulrich Bothner,3 Alberto de la Hoz,3 Isabel Kloer,3 Matthias Trampisch,3 Peter Alter4
1Department of Cardiology and Pneumology, University Medical Centre Göttingen, Göttingen, Germany; 2LungClinic Immenhausen, Immenhausen, Germany, Member of the German Center for Lung Research (DZL); 3Boehringer Ingelheim International GmbH, Ingelheim am Rhein, Germany; 4Department of Medicine, Pulmonary and Critical Care Medicine, Philipps University of Marburg (UMR), Marburg, Germany, Member of the German Center for Lung Research (DZL)
Correspondence: Stefan Andreas
Department of Cardiology and Pneumology, Robert-Koch-Str. 40., Göttingen, Germany
Tel +49 05673 501 1112
Fax +49 05673 501 1101
Email [email protected]
Background: Patients with chronic obstructive pulmonary disease (COPD) and cardiovascular comorbidities may have an increased risk of medication-related cardiac arrhythmias. We therefore performed an analysis of Holter electrocardiogram (ECG) data from two large, long-term, controlled clinical COPD trials to investigate whether tiotropium/olodaterol increased the risk of cardiac arrhythmia and mean heart rate.
Methods: We analyzed Holter ECG data from a representative subset of patients (N=506) from the two pooled replicate studies (TONADO 1 and 2) assessing tiotropium/olodaterol 5/5 μg therapy versus tiotropium 5 μg or olodaterol 5 μg monotherapy, inhaled once daily (two single inhalations) using the Respimat® Soft Mist™ inhaler device. Additionally, major adverse cardiac events (MACE) with tiotropium/olodaterol were assessed versus the respective monotherapies.
Results: After 12 weeks of treatment, there was no difference in the number of patients who had an increase or decrease from baseline in 24-hour supraventricular premature beats or ventricular premature beats between tiotropium/olodaterol 5/5 μg combination therapy and its monocomponents. Compared with baseline, a small but statistically significant increase in adjusted mean heart rate was observed for tiotropium 5 μg (+1.6 beats per minute [bpm]; P=0.0010), but no difference was observed for olodaterol 5 μg (+0.3 bpm; P=0.2778) or tiotropium/olodaterol 5/5 μg (– 0.1 bpm; P=0.4607). MACE and fatal MACE were limited to 1 to 3 patients across treatment groups.
Conclusion: Compared with the compounds given as monotherapy, treatment with tiotropium/olodaterol fixed-dose combination therapy is not associated with medically relevant or statistically significant effects on arrhythmia as assessed by Holter ECG. Based on these findings, there is no evidence to assume a clinically relevant impact on cardiac function from dual tiotropium/olodaterol treatment.
Trial Registration: TONADO 1 (ClinicalTrials.gov: NCT01431274); TONADO 2 (ClinicalTrials.gov: NCT01431287).
Keywords: tiotropium, olodaterol, Holter ECG, heart rate, arrhythmia, safety
Plain Language Summary
Patients with COPD often have heart conditions and thus may have a greater risk of developing arrhythmias (ie, change in heart rhythm) compared with healthy individuals. Tiotropium/olodaterol is an inhaled combination drug used for the treatment of COPD. To provide doctors with appropriate safety advice, we wanted to test whether tiotropium/olodaterol had any adverse effects on the heart in patients with COPD.
We collected data from a large COPD clinical trial called TONADO®, which compared the combination drug tiotropium/olodaterol with tiotropium or olodaterol given alone in patients with COPD. Some patients in the TONADO trial had their heart rhythm recorded with a 24-hour monitoring device. We analyzed their data after the patients had received treatment for 12 weeks.
We found no difference in the number of patients with arrhythmia between the tiotropium/olodaterol combination group and the groups who received tiotropium or olodaterol alone. There was a small increase in heart rate for the tiotropium group but not for the olodaterol group or tiotropium/olodaterol combination group.
In summary, treatment with the combination drug tiotropium/olodaterol did not increase the risk of heart arrhythmias in patients with COPD compared with tiotropium or olodaterol given alone.
Introduction
Patients with chronic obstructive pulmonary disease (COPD) often have cardiovascular (CV) comorbidities and a substantially greater risk of developing cardiac arrhythmias, thromboembolic disorders, myocardial ischemia and stroke compared with healthy individuals.1–3 Although the precise impact on ischemic and arrhythmic events is unknown, COPD is an independent predictor of death and hospitalization in patients with heart failure,4 and arrhythmogenic events may contribute to this poor prognosis. In addition, cardiac arrhythmia is thought to be a potential pharmacologic class risk of both long-acting muscarinic antagonists (LAMAs) and long-acting β2-agonists (LABAs).5,6
Extensive clinical trial data have established the efficacy and long-term safety of the LAMA tiotropium (SPIRIVA®; Boehringer Ingelheim Pharma GmbH & Co K.G., Ingelheim, Germany)7–10 and the LABA olodaterol.11–15 Similarly, their use in combination has been widely studied, with results showing superior effects on lung function, breathlessness and health-related quality of life compared with the drugs given as monotherapy.16–19
Initial concerns were identified regarding the CV safety of LAMA/LABA combined therapy.20–22 However, there are a number of reassuring analyses of clinical trial data focusing on cardiac function parameters (rhythm, heart rate and blood pressure)15,23,24 in addition to the general and CV adverse events (AEs) suggesting that tiotropium and olodaterol have similar, or lower, AE rates than placebo;11,25 combined tiotropium/olodaterol data suggest they can be administered safely to patients with moderate-to-very-severe COPD, including patients with significant CV comorbidity.26 Similar findings have been reported for the tiotropium Respimat® Soft Mist™ inhaler (SMI),27,28 including real-world evidence that tiotropium plus a second bronchodilator, in the setting of COPD, does not increase the risk of most CV events.29 However, the authors of this study, which included new users of LABA or tiotropium between 2002 and 2012, suggest a modest increase for heart failure warrants further investigation.29
In the case of olodaterol and LABAs in general, concerns result from the possible off-target interaction with β2-adrenoceptors (ARs) located in the atria, ventricles and peripheral vasculature.30 The clinical data are contradictory, with some studies showing an increase in heart rate when treated with salmeterol30,31 and others showing no increase in salmeterol-related CV AEs versus placebo.32 Olodaterol, a once-daily LABA, was designed with the aim of improving AR selectivity and intrinsic activity.
Long-term Holter electrocardiograms (ECGs) are commonly used to detect and monitor cardiac arrhythmias.33 However, published Holter ECG data from large cohorts of patients with COPD and CV comorbidities remain rare, but do include two studies showing that both tiotropium and olodaterol monotherapy are not associated with increased risk of arrhythmia compared with placebo.23,24 Given continuous Holter ECG investigations were conducted in the TONADO 1 and 2 studies, we pooled these data and conducted an analysis to investigate whether tiotropium/olodaterol combination increased the risk of cardiac arrhythmia in patients with moderate-to-very-severe COPD.
Methods
Study Designs
Detailed study methods have been published previously.26,34 Briefly, TONADO 1 and 2 (studies 1237.5 and 1237.6) were 52-week, replicate, phase III, multicenter, randomized, double-blind, parallel-group studies. Overall, 5,162 patients with moderate-to-very-severe COPD based on the Global Initiative for Chronic Obstructive Lung Disease (GOLD) grading system (spirometric GOLD grade 2–4)35 were treated with tiotropium/olodaterol fixed-dose combination 5/5 μg or 2.5/5 μg, or the individual monocomponents, each delivered via the SMI device.26,34
Sub-Analyses on Holter ECGs
For each study, 24-hour Holter ECG monitoring was performed at selected sites among a subset of patients who were capable and trained to handle centralized Holter ECG monitoring. All patients at selected sites were invited to participate in this sub-study. Holter ECG monitoring was performed in patients giving informed consent to participate in the sub-study, and able to carry and return the equipment after 24 hours. Sites were provided with standard equipment by the sponsor (12-Lead Mortara H12+ Digital Holter Recorder, eResearchTechnology, Inc., Philadelphia, USA). Holter ECG recordings were transferred to the central vendor (eResearchTechnology, Inc.), evaluated, validated by a cardiologist, and data uploaded to the study database. Holter ECG monitoring was performed prior to randomization at Visit 2 (Day –1, baseline) and during randomized treatment at Visit 5 (Day 85, Week 12).
Safety
During these studies, participants were assessed for AEs and serious AEs, and reported events were coded using MedDRA version 16.6. Major adverse cardiac events (MACE) were assessed for the different treatment arms included in this study.
Statistical Analysis
The 24-hour Holter ECG records were evaluated for mean heart rate, as well as the number of supraventricular premature beats (SVPBs) and ventricular premature beats (VPBs). Increase or decrease in SVPBs and VPBs from baseline on treatment were established using two-way shift tables. Shifts were defined based on predefined cut-offs with the following categories: <10, ≥10 to <30, ≥30 to <50, ≥50 to <100, ≥100 to <500, ≥500 to <1000, ≥1000 to <2000, and ≥2000. Categories assigned at baseline and Week 12 were compared to give shifts in SVPBs and VPBs. Differences in the frequency of shifts (increase, decrease or unchanged from baseline) were evaluated between treatments using Chi-squared testing. The 24-hour Holter ECG mean heart rates were adjusted with a mixed-effect model repeat measurement (MMRM) and analyzed for the adjusted mean changes from baseline and treatment differences. Fixed effects for the MMRM model included treatment, visit, treatment-by-visit interaction and baseline. P<0.05 was considered a significant difference for all post hoc statistical analyses at an alpha level of 0.05.
Only the treatment groups in TONADO 1 and 2 with licensed doses of study medication are included in this analysis: tiotropium/olodaterol 5/5 µg, tiotropium 5 µg and olodaterol 5 µg.
Results
Baseline Demographics
In total, 506 patients from the Holter ECG monitoring subsets of TONADO 1 and 2 were included in this analysis. The overall patient characteristics of the studies have been described previously.34
In the subset of patients included in the Holter ECG examinations, patients had a mean age of 64 years, 64% were male and all patients were current smokers (47%) or ex-smokers (53%). When classified by GOLD, most patients were spirometric GOLD grade 2 (51.0%) or GOLD grade 3 (36.6%), with 12.3% in GOLD grade 4; 12.3% of patients had cardiac arrhythmia at baseline and 13.4% of patients had ischemic heart disease at baseline (Table 1). The Holter subset was representative of the full study population regarding their CV risk, indicated by their CV diseases and CV medication received at baseline.
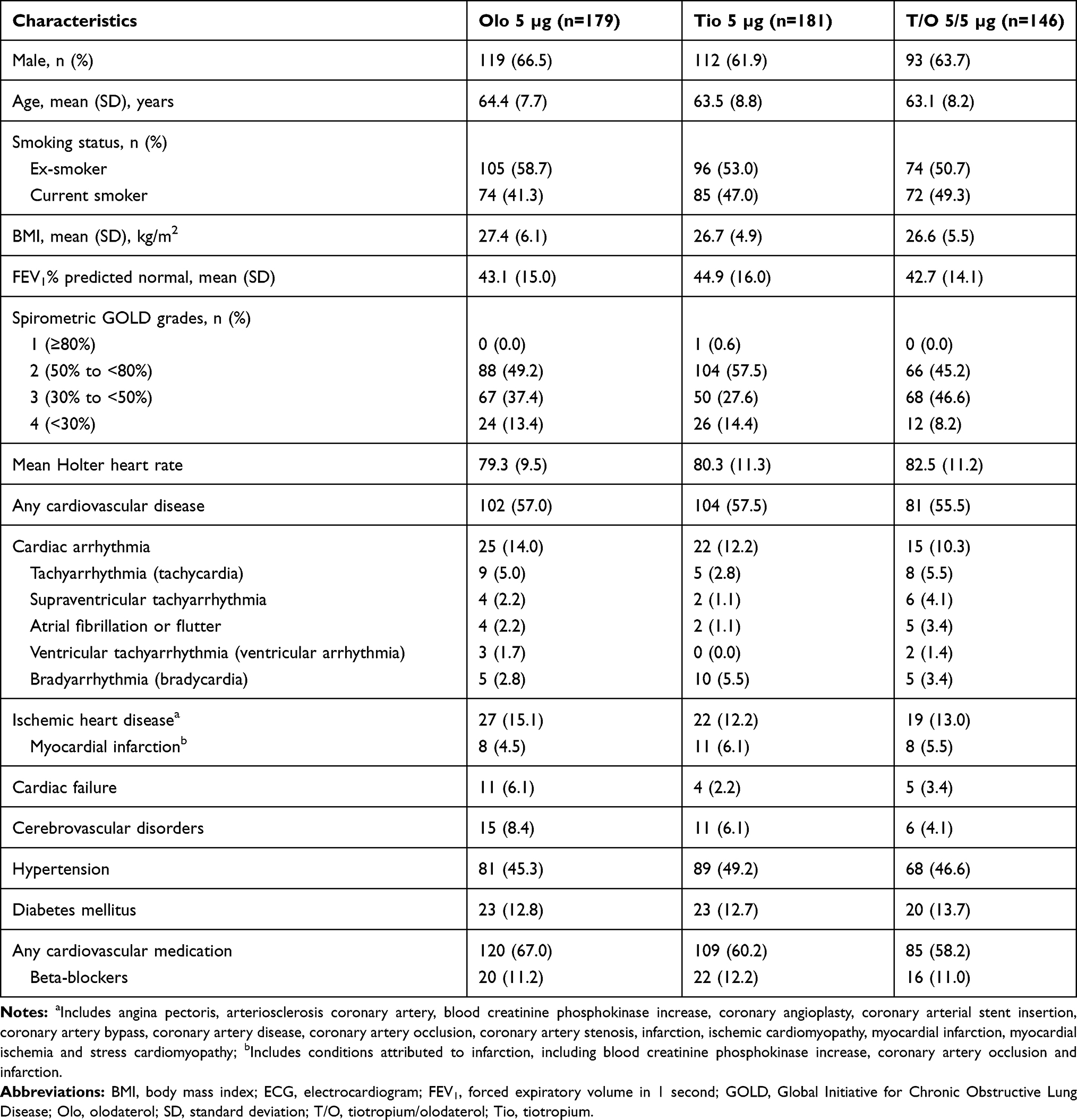 |
Table 1 Baseline Demographics of Holter ECG Subgroup (TONADO 1 and 2) |
Holter ECG Data
Shift in SVPB
No significant difference was observed in the shifts (ie, proportion of patients whose SVPB increased or decreased from baseline) of tiotropium/olodaterol combination therapy and its monocomponents (Chi-squared test P=0.6053; Figure 1A). At Week 12, 21.2%, 27.1% and 25.3% of patients had an increase in SVPBs from baseline with olodaterol 5 µg, tiotropium 5 µg and tiotropium/olodaterol 5/5 µg, respectively; 26.8%, 21.5% and 28.1% had a decrease from baseline with olodaterol 5 µg, tiotropium 5 µg and tiotropium/olodaterol 5/5 µg, respectively.
 |
Figure 1 (A) Shifts in SVPB: T/O vs monocomponents at Week 12 (TONADO 1 and 2), and (B) shifts in VPB: T/O vs monocomponents at Week 12 (TONADO 1 and 2). P-value based on Chi-squared test: no statistical difference in frequency of increase or decrease. Abbreviations: Olo, olodaterol; SVPB, supraventricular premature beat; T/O, tiotropium/olodaterol; Tio, tiotropium; VPB, ventricular premature beat. For definition of shifts in SVPB and VPB, see Methods section (Sub-analyses on Holter ECGs). |
Shift in VPB
No significant difference was observed in the shifts (ie, proportion of patients whose VPB increased or decreased from baseline) of tiotropium/olodaterol combination therapy and its monocomponents (Chi-squared test P=0.9790; Figure 1B). At Week 12, 21.2%, 22.7% and 22.6% of patients had an increase in VPBs from baseline with olodaterol 5 µg, tiotropium 5 µg and tiotropium/olodaterol 5/5 µg, respectively; 21.2%, 21.5% and 24.0% had a decrease from baseline with olodaterol 5 µg, tiotropium 5 µg and tiotropium/olodaterol 5/5 µg, respectively. In general, a similar proportion of patients had a decrease in VPBs as an increase in VPBs for all treatment groups.
Holter ECG Heart Rate Data
The adjusted mean heart rate at Week 12 was slightly higher for tiotropium 5 µg compared with the other treatment arms (olodaterol 5 µg: 80.6 beats per minute [bpm]; tiotropium 5 µg: 81.9 bpm; tiotropium/olodaterol 5/5 µg: 80.2 bpm; Figure 2). Compared with baseline, a significant increase in adjusted mean heart rate was observed for tiotropium 5 µg (+1.6 bpm; P=0.0010) but no difference was observed for olodaterol 5 µg (+0.3 bpm; P=0.2778) or tiotropium/olodaterol 5/5 µg (–0.1 bpm; P=0.4607). The between-treatment group comparisons of the adjusted mean changes from baseline were significant between tiotropium/olodaterol 5/5 µg and tiotropium 5 µg (–1.7 bpm; P=0.0149) but not significant between tiotropium/olodaterol 5/5 µg and olodaterol 5 µg (–0.4 bpm; P=0.3187). Overall, the changes in the adjusted mean heart rates from baseline to Week 12 were small.
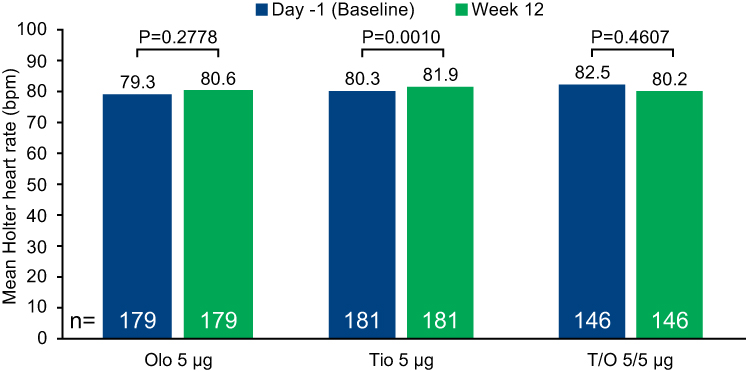 |
Figure 2 Adjusted mean Holter heart rate over 24 hours at Week 12: T/O vs monocomponents at baseline and Week 12 (TONADO 1 and 2). Treated set: adjusted data. Baseline data are unadjusted. P-values are for adjusted mean change from baseline data. Standard errors for baseline are 0.71, 0.84 and 0.93, respectively, and for week 12 were 0.53, 0.53 and 0.72, respectively. Abbreviations: bpm, beats per minute; Olo, olodaterol; T/O, tiotropium/olodaterol; Tio, tiotropium. |
Safety
There were very few patients with MACE (olodaterol 5 µg: 1 patient; tiotropium 5 µg: 2 patients; tiotropium/olodaterol 5/5 µg: 3 patients) or fatal MACE (olodaterol 5 µg: 1 patient; tiotropium 5 µg: 1 patient; tiotropium/olodaterol 5/5 µg: 2 patients). The overall number of patients with cardiac arrhythmia was not higher with tiotropium/olodaterol 5/5 µg (supraventricular tachyarrhythmia: 0.0%; atrial fibrillation or flutter: 0.0%; ventricular tachyarrhythmia: 0.7%; Table 2) compared with the monocomponents olodaterol 5 µg and tiotropium 5 µg (supraventricular tachyarrhythmia: 0.6% and 1.1%, respectively; atrial fibrillation or flutter: 0.6% and 0.6%, respectively; ventricular tachyarrhythmia: 1.1% and 0.0%, respectively; Table 2).
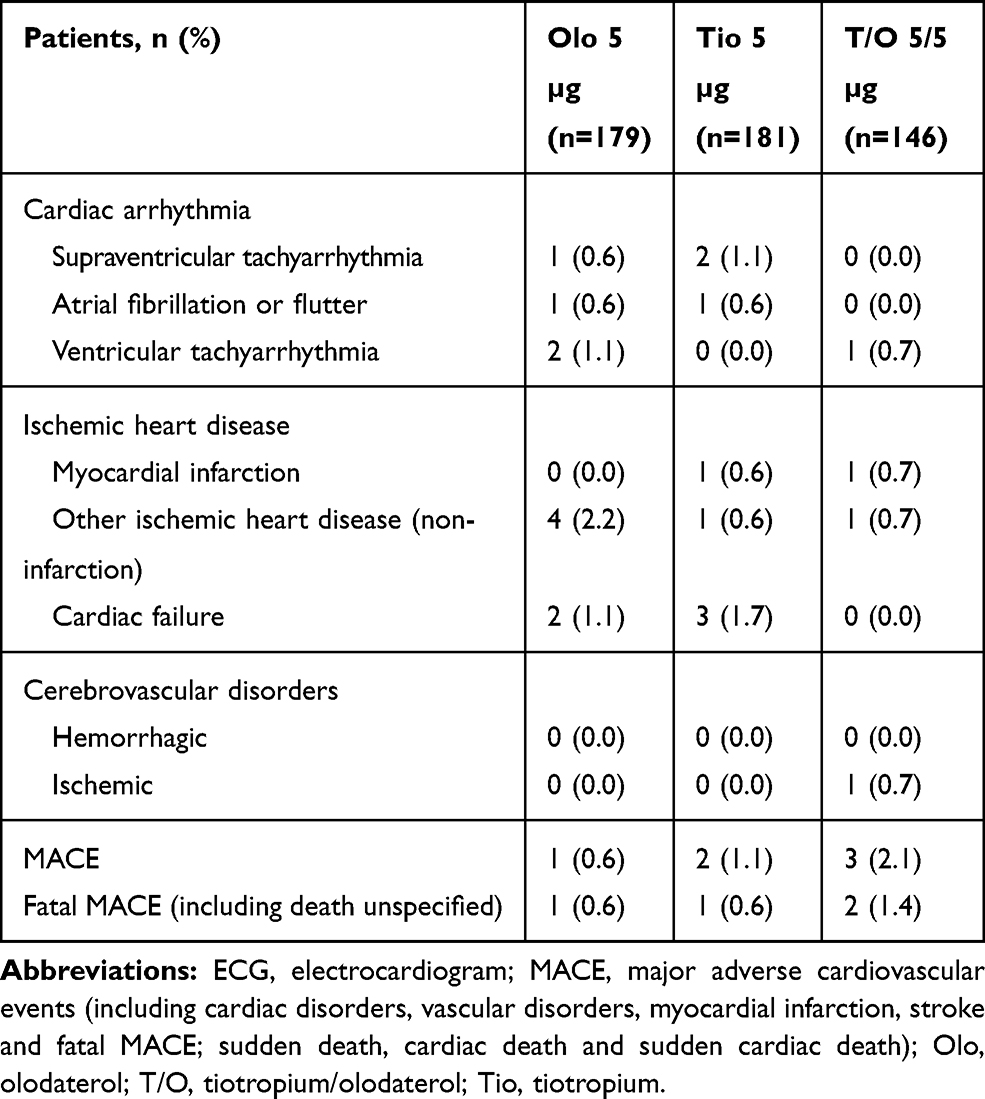 |
Table 2 Cardiovascular Adverse Events of Holter ECG Subgroup (TONADO 1 and 2) |
Discussion
The present study found no evidence of a pro-arrhythmic effect on SVPB and VPB for tiotropium/olodaterol combination therapy versus its monocomponents. We also report very few MACE or fatal MACE in this study population, indicating that the combination of tiotropium/olodaterol in patients does not increase the risk of CV AEs.
As LABAs are an established therapy for COPD, their safety, both alone and in combination with LAMAs, in COPD patients with CV comorbidities have previously been investigated26,35,36 Olodaterol, a once-daily LABA, was designed with the aim of improving AR selectivity and intrinsic activity. LABAs as a class are not all the same structurally; for instance, olodaterol is structurally distinct from formoterol and salmeterol. β-agonists are racemates37 – with the (R)-enantiomer being the active component and the (S)-enantiomer being inactive at therapeutic concentrations38 – though in vitro studies have shown the (S)-enantiomer may induce tachyphylaxis or receptor desensitisation39 Olodaterol, a pure (R,R)-β-agonist, provides bronchodilation at lower doses, potentially allowing for fewer β2-AR-mediated side effects39,40
To further evaluate the cardiac safety profile of olodaterol, both alone and in combination with LAMAs, in COPD patients with CV comorbidities, we report cardiac arrhythmia and heart rate data from a subset of patients with moderate-to-very-severe COPD subject to Holter ECG assessment during two large Phase III trials comparing tiotropium/olodaterol (5/5 μg and 2.5/5 μg) with the monocomponents tiotropium (5 μg and 2.5 μg) and olodaterol (5 μg).
This study is one of the largest and most detailed data sets of Holter ECG measurements in patients with COPD on bronchodilation therapy. Further strengths of this analysis include the large size of the TONADO trials and that they were active-comparator controlled.34 Also, the trials included patients with CV comorbidities and 58% of all patients were receiving CV medication, including 10% on β-blockers. We also used highly standardized methodologies for data collection across centers, and the trials were blinded, and active-comparator controlled. Previous data showed no pro-arrhythmic effect of tiotropium 1.25–10 µg delivered via SMI and 18 µg delivered via dry powder inhaler versus placebo.24 These results are in line with the pooled TONADO trial data, which reported MACE rate ratios of 1.07 (95% confidence interval [CI] 0.66–1.73) and 1.11 (95% CI 0.68–1.80) when comparing the combination with the monotherapies, respectively.34
Regarding Holter ECG heart rates, differences (small increases with monocomponents and a small decrease for dual bronchodilation) from baseline to Week 12 and between treatment groups were small and not clinically relevant. It is unknown whether the Holter ECG heart rate evaluated in this analysis is influenced more by any pharmacologic effects of treatment or is rather an indirect reflection of improved daily physical activity resulting from effective maintenance of bronchodilation. Dedicated analyses of long-term heart rate from TONADO 1 and 2 have shown no relevant increases in resting heart rate and blood pressure from baseline with tiotropium/olodaterol versus its monocomponents.15,41 The findings of this study are important given that elevated heart rate has been reported in patients who have had COPD for many years, and is a risk factor for adverse outcomes in this population.42,43 A post hoc analysis in the Study to Understand Mortality and Morbidity in COPD (SUMMIT) trial confirmed the association of elevated heart rate with increased mortality and CV events in patients with COPD.44 Patients with COPD often have comorbid CV diseases whereby elevated resting heart rate may contribute to CV morbidity and mortality via neurohumoral activation, and thus provide a potential mechanism that links heart rate to increases in mortality in COPD.1,42-48
The present study benefits from the availability of baseline and follow-up data for each defined time point, and analysis of the Holter ECG data was better refined versus previous studies.
There are limitations in this analysis. Treatment centers that were not able to perform Holter ECGs and patients who were not able to carry the equipment were not included in the analysis; this meant that the subset of patients included were not selected at random. Patients with more unstable CV diseases may have been excluded from the trials or may not have participated in the Holter ECG subset study for individual reasons, although this would have similarly influenced the primary randomized treatment groups. CV conditions in very high-risk patients warrant further investigation either in a larger clinical practice population or in individual case analyses.
Conclusion
In conclusion, compared with monocomponents, treatment with tiotropium/olodaterol combination therapy is neither associated with SVPB or VPB, nor with changes in heart rate as assessed by Holter ECG. Based on these findings, there is no evidence to assume a clinically relevant impact on cardiac function from dual tiotropium/olodaterol treatment.
Abbreviations
AE, adverse event; AR, β2-adrenoceptors; bpm, beats per minute; COPD, chronic obstructive pulmonary disease; CV, cardiovascular; ECG, electrocardiogram; GOLD, Global Initiative for Chronic Obstructive Lung Disease; LABA, long-acting β2-agonist; LAMA, long-acting muscarinic antagonist; MACE, major adverse cardiac event; MMRM, mixed-effect model repeat measurement; SMI, Soft Mist™ inhaler; SVPB, supraventricular premature beat; T/O, tiotropium/olodaterol combination therapy; VPB, ventricular premature beat.
Data Sharing Statement
Data are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
All studies included in this analysis were performed in accordance with the provisions of the Declaration of Helsinki (1996 version), the International Conference on Harmonization Tripartite Guideline for Good Clinical Practice, and applicable regulatory requirements and Boehringer Ingelheim Standard Operating Procedures. All patients provided written informed consent. This article does not report individual patient data; all data presented here are anonymized. The clinical trial protocols and the informed consent and patient information forms were reviewed and received approval/favorable opinion from a constituted local Institutional Review Board or an Independent Ethics Committee at each center prior to the start of the study. Approval was granted from institutional review boards (Coordinating Investigator’s [Prof. Roland Buhl] Independent Ethics Committee: Ethik-Kommission bei der Landesärztekammer Rheinland-Pfalz, Deutschhausplatz 3, 55116 Mainz, Germany) and patients provided written informed consent for these studies.
Acknowledgments
All authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation. Medical writing assistance, in the form of the preparation and revision of the manuscript, was supported financially by Boehringer Ingelheim and provided by Ishmam Nawar of MediTech Media (London, UK), based on a draft provided by the authors, their feedback and under their conceptual direction.
Author Contributions
The authors meet criteria for authorship as recommended by the International Committee of Medical Journal Editors (ICMJE). The authors received no direct compensation related to the development of this manuscript. Boehringer Ingelheim was given the opportunity to review the manuscript for medical and scientific accuracy, as well as intellectual property considerations. All authors contributed to data analysis, drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
SA reports personal fees from Boehringer Ingelheim and GlaxoSmithKline, and payments for presenting from Boehringer Ingelheim, AstraZeneca, Berlin Chemie, Chiesi and Novartis, outside the submitted work. UB, AdlH, IK and MT are employees of Boehringer Ingelheim. PA reports grants from the German Federal Ministry of Education and Research (BMBF) Competence Network Asthma and COPD (ASCONET), AstraZeneca, GlaxoSmithKline, Grifols Deutschland, MSD Sharp & Dohme, Pfizer, Takeda, Boehringer Ingelheim and Novartis Deutschland, grants and non-financial support from Bayer Schering Pharma AG and Chiesi, and grants, personal fees and non-financial support from Novartis Deutschland, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Feary JR, Rodrigues LC, Smith CJ, Hubbard RB, Gibson JE. Prevalence of major comorbidities in subjects with COPD and incidence of myocardial infarction and stroke: a comprehensive analysis using data from primary care. Thorax. 2010;65(11):956–962. doi:10.1136/thx.2009.128082
2. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report: GOLD executive summary. Am J Respir Crit Care Med. 2017;195(5):557–582. doi:10.1164/rccm.201701-0218PP
3. Cazzola M, Calzetta L, Bettoncelli G, et al. Cardiovascular disease in asthma and COPD: a population-based retrospective cross-sectional study. Respir Med. 2012;106(2):249–256. doi:10.1016/j.rmed.2011.07.021
4. Hawkins NM, Petrie MC, Macdonald MR, et al. Heart failure and chronic obstructive pulmonary disease the quandary of beta-blockers and beta-agonists. J Am Coll Cardiol. 2011;57(21):2127–2138. doi:10.1016/j.jacc.2011.02.020
5. Boehringer Ingelheim International GmbH. Striverdi Respimat 2.5 microgram, solution for inhalation – Summary of Product Characteristics, Europe; 2019. Available from: https://www.medicines.org.uk/emc/product/3255/smpc.
6. Boehringer Ingelheim International GmbH. Spiriva® Respimat® 2.5 microgram, solution for inhalation – Summary of Product Characteristics, Europe; 2016. Available from: https://www.spiriva.com/uk/sites/default/files/Spiriva%20Respimat%20SPC%20(1).pdf.
7. Tashkin DP, Celli B, Senn S, et al. A 4-year trial of tiotropium in chronic obstructive pulmonary disease. N Engl J Med. 2008;359(15):1543–1554. doi:10.1056/NEJMoa0805800
8. O’Donnell DE, Fluge T, Gerken F, et al. Effects of tiotropium on lung hyperinflation, dyspnoea and exercise tolerance in COPD. Eur Respir J. 2004;23(6):832–840. doi:10.1183/09031936.04.00116004
9. Wise RA, Anzueto A, Cotton D, et al. Tiotropium Respimat inhaler and the risk of death in COPD. N Engl J Med. 2013;369(16):1491–1501. doi:10.1056/NEJMoa1303342
10. Anzueto A, Wise R, Calverley P, et al. The tiotropium safety and performance in Respimat® (TIOSPIR®) trial: spirometry outcomes. Respir Res. 2015;16:107. doi:10.1186/s12931-015-0269-4
11. McGarvey L, Niewoehner D, Magder S, et al. One-year safety of olodaterol once daily via Respimat® in patients with GOLD 2-4 chronic obstructive pulmonary disease: results of a pre-specified pooled analysis. COPD. 2015;12(5):484–493. doi:10.3109/15412555.2014.991864
12. Ferguson GT, Feldman GJ, Hofbauer P, et al. Efficacy and safety of olodaterol once daily delivered via Respimat® in patients with GOLD 2-4 COPD: results from two replicate 48-week studies. Int J Chron Obstruct Pulmon Dis. 2014;9:629–645. doi:10.2147/COPD.S61717
13. Koch A, Pizzichini E, Hamilton A, et al. Lung function efficacy and symptomatic benefit of olodaterol once daily delivered via Respimat® versus placebo and formoterol twice daily in patients with GOLD 2–4 COPD: results from two replicate 48-week studies. Int J Chron Obstruct Pulmon Dis. 2014;9:697–714. doi:10.2147/COPD.S62502
14. Koch A, Watz H, Maleki-Yazdi MR, et al. Comprehensive assessment of the safety of olodaterol 5 µg in the Respimat® device for maintenance treatment of COPD: comparison with the long-acting β2-agonist formoterol. NPJ Prim Care Respir Med. 2017;27(1):60. doi:10.1038/s41533-017-0059-1
15. Andreas S, Bothner U, Trampisch M, Haensel M, Buhl R, Alter P. Effect of long-acting β2-agonists olodaterol and formoterol on heart rate and blood pressure in chronic obstructive pulmonary disease patients. Pulm Pharmacol Ther. 2018;52:1–6. doi:10.1016/j.pupt.2018.08.002
16. Singh D, Ferguson GT, Bolitschek J, et al. Tiotropium + olodaterol shows clinically meaningful improvements in quality of life. Respir Med. 2015;109(10):1312–1319. doi:10.1016/j.rmed.2015.08.002
17. Singh D, Gaga M, Schmidt O, et al. Effects of tiotropium + olodaterol versus tiotropium or placebo by COPD disease severity and previous treatment history in the OTEMTO® studies. Respir Res. 2016;17(1):73. doi:10.1186/s12931-016-0387-7
18. Beeh KM, Westerman J, Kirsten AM, et al. The 24-h lung-function profile of once-daily tiotropium and olodaterol fixed-dose combination in chronic obstructive pulmonary disease. Pulm Pharmacol Ther. 2015;32:53–59. doi:10.1016/j.pupt.2015.04.002
19. Maltais F, Hamilton A, Voss F, Maleki-Yazdi MR. Dose determination for a fixed-dose drug combination: a Phase II randomized controlled trial for tiotropium/olodaterol versus tiotropium in patients with COPD. Adv Ther. 2019;36(4):962–968. doi:10.1007/s12325-019-00911-y
20. Lahousse L, Verhamme KM, Stricker BH, Brusselle GG. Cardiac effects of current treatments of chronic obstructive pulmonary disease. Lancet Respir Med. 2016;4(2):149–164. doi:10.1016/S2213-2600(15)00518-4
21. Singh S, Loke YK, Enright PL, Furberg CD. Mortality associated with tiotropium mist inhaler in patients with chronic obstructive pulmonary disease: systematic review and meta-analysis of randomised controlled trials. BMJ. 2011;342:d3215. doi:10.1136/bmj.d3215
22. Singh S, Loke YK, Furberg CD. Inhaled anticholinergics and risk of major adverse cardiovascular events in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. JAMA. 2008;300(12):1439–1450. doi:10.1001/jama.300.12.1439
23. Andreas S, Bothner U, de la Hoz A, Kloer I, Trampisch M, Alter P. A post hoc Holter ECG analysis of olodaterol and formoterol in moderate-to-very-severe COPD. Int J Chron Obstruct Pulmon Dis. In press 2020.
24. Hohlfeld JM, Furtwaengler A, Konen-Bergmann M, Wallenstein G, Walter B, Bateman ED. Cardiac safety of tiotropium in patients with COPD: a combined analysis of Holter-ECG data from four randomised clinical trials. Int J Clin Pract. 2015;69(1):72–80.
25. Halpin DM, Dahl R, Hallmann C, Mueller A, Tashkin D. Tiotropium HandiHaler(®) and Respimat(®) in COPD: a pooled safety analysis. Int J Chron Obstruct Pulmon Dis. 2015;10:239–259. doi:10.2147/COPD.S75146
26. Buhl R, Magder S, Bothner U, et al. Long-term general and cardiovascular safety of tiotropium/olodaterol in patients with moderate to very severe chronic obstructive pulmonary disease. Respir Med. 2017;122:58–66. doi:10.1016/j.rmed.2016.11.011
27. Karner C, Chong J, Poole P. Tiotropium versus placebo for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2014;11(7):CD009285.
28. Dong YH, Lin HH, Shau WY, Wu YC, Chang CH, Lai MS. Comparative safety of inhaled medications in patients with chronic obstructive pulmonary disease: systematic review and mixed treatment comparison meta-analysis of randomised controlled trials. Thorax. 2013;68(1):48–56. doi:10.1136/thoraxjnl-2012-201926
29. Suissa S, Dell’Aniello S, Ernst P. Concurrent use of long-acting bronchodilators in COPD and the risk of adverse cardiovascular events. Eur Respir J. 2017;49(5):1602245. doi:10.1183/13993003.02245-2016
30. Cazzola M, Imperatore F, Salzillo A, et al. Cardiac effects of formoterol and salmeterol in patients suffering from COPD with preexisting cardiac arrhythmias and hypoxemia. Chest. 1998;114(2):411–415. doi:10.1378/chest.114.2.411
31. Haarmann H, Mohrlang C, Tschiesner U, et al. Inhaled β-agonist does not modify sympathetic activity in patients with COPD. BMC Pulm Med. 2015;15:46. doi:10.1186/s12890-015-0054-7
32. Ferguson GT, Funck-Brentano C, Fischer T, Darken P, Reisner C. Cardiovascular safety of salmeterol in COPD. Chest. 2003;123(6):1817–1824. doi:10.1378/chest.123.6.1817
33. Galli A, Ambrosini F, Lombardi F. Holter monitoring and loop recorders: from research to clinical practice. Arrhythm Electrophysiol Rev. 2016;5(2):136–143. doi:10.15420/AER.2016.17.2
34. Buhl R, Maltais F, Abrahams R, et al. Tiotropium and olodaterol fixed-dose combination versus mono-components in COPD (GOLD 2-4). Eur Respir J. 2015;45(4):969–979. doi:10.1183/09031936.00136014
35. Global Initiative for Chronic Obstructive Lung Disease. Pocket guide to COPD diagnosis, management and prevention – A guide for health care professionals (2019report); 2019. Available from: https://goldcopd.org/wp-content/uploads/2018/11/GOLD-2019-POCKET-GUIDE-FINAL_WMS.pdf.
36. Ferguson GT, Buhl R, Bothner U, et al. Safety of tiotropium/olodaterol in chronic obstructive pulmonary disease: pooled analysis of three large, 52-week, randomized clinical trials. Respir Med. 2018;143:67–73. doi:10.1016/j.rmed.2018.08.012
37. Handley DA, Morley J. The pursuit of precision pharmaceuticals: divergent effects of β2 agonist isomers. Expert Opin Investig Drugs. 1998;7(10):1601–1616. doi:10.1517/13543784.7.10.1601
38. Ramsay CM, Cowan J, Flannery E, McLachlan C, Taylor DR. Bronchoprotective and bronchodilator effects of single doses of (S)-salbutamol, (R)-salbutamol and racemic salbutamol in patients with bronchial asthma. Eur J Clin Pharmacol. 1999;55(5):353–359. doi:10.1007/s002280050640
39. Lötvall J, Palmqvist M, Ankerst J, et al. The effect of formoterol over 24h in patients with asthma: the role of enantiomers. Pulm Pharmacol Ther. 2005;18(2):109–113. doi:10.1016/j.pupt.2004.10.007
40. Terasaki J, Nishi S, Ameredes B, Sharma G. Arformoterol: rationale for use in chronic obstructive pulmonary disease. Clin Investig (Lond). 2014;4:429–439.
41. Andreas S, McGarvey L, Bothner U, et al. Absence of adverse effects of tiotropium/olodaterol compared with the monocomponents on long-term heart rate and blood pressure in patients with moderate-to-very-severe COPD. Int J Chron Obstruct Pulmon Dis. In press 2020.
42. Andreas S, Anker SD, Scanlon PD, Somers VK. Neurohumoral activation as a link to systemic manifestations of chronic lung disease. Chest. 2005;128(5):3618–3624. doi:10.1378/chest.128.5.3618
43. Andreas S, Haarmann H, Klarner S, Hasenfuss G, Raupach T. Increased sympathetic nerve activity in COPD is associated with morbidity and mortality. Lung. 2014;192(2):235–241. doi:10.1007/s00408-013-9544-7
44. Byrd JB, Newby DE, Anderson JA, et al. Blood pressure, heart rate, and mortality in chronic obstructive pulmonary disease: the SUMMIT trial. Eur Heart J. 2018;39(33):3128–3134. doi:10.1093/eurheartj/ehy451
45. Huiart L, Ernst P, Suissa S. Cardiovascular morbidity and mortality in COPD. Chest. 2005;128(4):2640–2646. doi:10.1378/chest.128.4.2640
46. Fuhrman C, Jougla E, Nicolau J, Eilstein D, Delmas MC. Deaths from chronic obstructive pulmonary disease in France, 1979–2002: a multiple cause analysis. Thorax. 2006;61(11):930–934. doi:10.1136/thx.2006.061267
47. Jensen MT, Suadicani P, Hein HO, Gyntelberg F. Elevated resting heart rate, physical fitness and all-cause mortality: a 16-year follow-up in the Copenhagen Male Study. Heart. 2013;99(12):882–887. doi:10.1136/heartjnl-2012-303375
48. Schrier RW, Abraham WT. Hormones and hemodynamics in heart failure. N Engl J Med. 1999;341(8):577–585. doi:10.1056/NEJM199908193410806
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.