Back to Journals » Infection and Drug Resistance » Volume 13
No Evidence for Ceftobiprole-Induced Immune Hemolytic Anemia in Three Phase 3 Clinical Trials
Authors Hamed K ![]() , Wiktorowicz T, Assadi Gehr M
, Wiktorowicz T, Assadi Gehr M
Received 18 June 2020
Accepted for publication 29 August 2020
Published 16 September 2020 Volume 2020:13 Pages 3209—3215
DOI https://doi.org/10.2147/IDR.S268269
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Kamal Hamed, Tatiana Wiktorowicz, Maziar Assadi Gehr
Basilea Pharmaceutica International Ltd., Basel, Switzerland
Correspondence: Kamal Hamed
Basilea Pharmaceutica International Ltd., Grenzacherstrasse 487, Basel 4005, Switzerland
Tel +41 61 567 1588
Fax +41 61 606 1216
Email [email protected]
Purpose: Drug-induced immune hemolytic anemia (DIIHA) is a rare but serious adverse event associated with a number of drugs, including second- and third-generation cephalosporins. A positive direct antiglobulin test (DAT) is a reliable finding in DIIHA, but positive results without evidence of hemolysis can occur, particularly in hospitalized patients. There have been no reports of hemolytic anemia in four previous Phase 3 trials or from post-marketing surveillance of the advanced-generation, broad-spectrum cephalosporin, ceftobiprole. The aim of this analysis was to review the incidence of positive DAT results and any evidence of hemolytic anemia from three recent Phase 3 trials of ceftobiprole.
Patients and Methods: Patients were enrolled in three Phase 3 randomized controlled trials: 94 pediatric patients with pneumonia received ceftobiprole in the BPR-PIP-002 trial; 335 adults with acute bacterial skin and skin structure infections received ceftobiprole in the TARGET trial; and 201 adults with Staphylococcus aureus bacteremia have been randomized 1:1 to ceftobiprole or daptomycin ± aztreonam in the ongoing ERADICATE trial. In all three trials, DAT results were obtained at baseline, and follow-up tests were performed either at the test of cure (TOC) visit (BPR-PIP-002), end-of-treatment (EOT) visit (TARGET), or both EOT and post-treatment Day 70 visits (ERADICATE).
Results: In the BPR-PIP-002 trial, five patients (all ceftobiprole treated) had a documented negative DAT result at baseline followed by a positive result at the TOC visit. One patient in the ongoing, blinded ERADICATE trial had a positive DAT result at both baseline and EOT. Results from other laboratory investigations showed no evidence of hemolytic anemia in these patients. No positive DAT results were reported in the TARGET trial.
Conclusion: No evidence of hemolytic anemia associated with ceftobiprole was observed in either adults or children across several indications in this analysis of three large Phase 3 trials.
Keywords: DIIHA, direct antiglobulin test, hemolysis, pneumonia, ABSSSIs, Staphylococcus aureus bacteremia
Erratum for this paper has been published
Plain Language Summary
Drug-induced immune hemolytic anemia is an extremely rare form of anemia. It occurs when red blood cells are destroyed by the immune system in response to treatment with certain pharmacological therapies. Evidence obtained over many decades has demonstrated that the second- and third-generation cephalosporin antibiotics are a leading cause of drug-induced hemolytic anemia. However, a similar association has not been reported for the advanced-generation cephalosporins. In cases of drug-induced immune hemolytic anemia, a laboratory investigation known as the direct antiglobulin test (DAT; colloquially known as the direct Coombs’ test) is usually positive. However, this test can be positive without evidence of hemolytic anemia, particularly in hospitalized patients, and results must be evaluated in the context of other laboratory or clinical findings.
The objective of this analysis was to evaluate the frequency of positive DAT results and hemolytic anemia in patients treated with the advanced-generation cephalosporin, ceftobiprole. In three large Phase 3 trials in both adults and children, we found no evidence of hemolytic anemia in any patient treated with ceftobiprole. A small number of positive DAT results were reported at baseline and/or after treatment with ceftobiprole. However, in the absence of other laboratory or clinical findings indicative of hemolytic anemia, these results may simply reflect the fact that these patients had infections severe enough to warrant hospitalization. These results are consistent with earlier Phase 3 trials of ceftobiprole and other advanced-generation cephalosporins. Our analysis provides further evidence that hemolytic anemia may not be associated with advanced-generation cephalosporin treatment.
Introduction
Drug-induced immune hemolytic anemia (DIIHA) is a rare but serious complication of drug treatment, with an estimated incidence of approximately 1 case per million individuals, per year.1 The mechanism of DIIHA is complex and poorly understood,2–4 and there is usually no relationship between drug dose and reaction.5 Most antibodies that cause DIIHA are categorized as drug-dependent, ie, they demonstrate reactivity only in the presence of drug.2 Less commonly, DIIHA is caused by drug-independent antibodies, ie, antibodies that are capable of in vitro reactivity in the absence of drug.2 Antibodies may be directed against the drug, a neoantigen formed by the drug and red blood cell (RBC) membrane components, or against membrane components (autoantibodies) (Figure 1).3,4,6 Additionally, some drugs can cause serum proteins, including immunoglobulins, to be adsorbed onto RBC membranes, potentially mediating their destruction.6 To date, the best-understood mechanisms of DIIHA involve penicillin and cefotetan, which covalently bind to RBC membranes and induce binding of IgG antibodies to drug epitopes. These coated RBCs then undergo extravascular destruction via Fc-receptor recognition by splenic macrophages.2
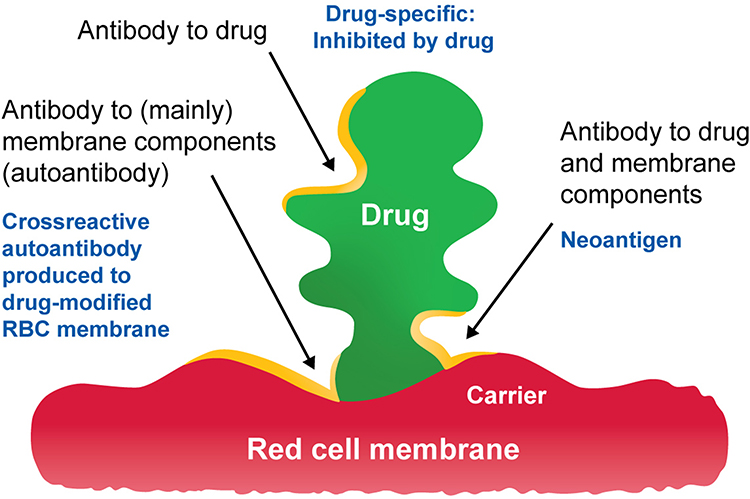 |
Figure 1 A proposed unifying model of drug-induced immune hemolytic anemias based on the hapten theory of antibody production. Reproduced with permission from Branch DR. Drug-induced immune haemolytic anaemias. ISBT Sci Ser. 2018;14(1):49-52.© 2018 International Society of Blood Transfusion.6 |
A reliable laboratory finding in DIIHA is a positive direct antiglobulin test (DAT; colloquially referred to as a positive direct Coombs’ test).2 This is a method of detecting the presence of antibodies or complement directly bound to RBC membranes.7 However, up to 0.1% of healthy individuals and up to 15% of hospitalized patient specimens can have a positive DAT result without evidence of hemolysis (reviewed by Zantek et al8). It is therefore important that the significance of a positive result is interpreted in the context of the clinical situation.8
As of 2014, 136 drugs had been reported to cause DIIHA.9 Historically, the most common drugs associated with this condition were methyldopa and high-dose intravenous penicillin.10 However, over the past 50 years, the spectrum of medications implicated in DIIHA has changed considerably and the focus has shifted to the cephalosporins and other β-lactam antibiotics, such as piperacillin.9,11 Evidence shows that first-generation cephalosporins (eg, cephalexin, cephalothin, and cefazolin) rarely caused immune hemolytic anemia, with only five well-documented cases since their first introduction in 1964.12 Second- and third-generation cephalosporins, especially cefotetan and ceftriaxone, have been associated with severe, sometimes fatal hemolytic anemia.12 In a reference laboratory in the USA, these agents accounted for over 80% of reported cases of DIIHA over the ten-year period to 2005, with cefotetan being the most frequently suspected cephalosporin.10 Similarly, in a case–control study in Germany, second- and third-generation cephalosporins were a frequent cause of DIIHA.1 However, in this study, the proportion of cases caused by cephalosporins was lower than that observed in the USA study. This may reflect the fact that cefotetan was no longer available in Germany during the study period.1 Of note, children may be more vulnerable to ceftriaxone-induced hemolytic anemia than adults, and reactions in children can be severe and often fatal.13 However, the condition is rare, and affected children commonly have underlying chronic hematologic or immunologic disorders or chronic/recurrent infections (reviewed by Northrop and Agarwal14). Since 2008, piperacillin has superseded cefotetan and ceftriaxone as the leading cause of DIIHA.9
Although hemolytic anemia has not been observed in clinical trials of the advanced-generation cephalosporin, ceftaroline, DAT seroconversion has been reported.15–18 In the Phase 3, multicenter, randomized, double-blind FOCUS trials in community-acquired bacterial pneumonia, there were more positive DAT results with ceftaroline versus ceftriaxone (9.8% versus 4.5%), but no difference in the rates of anemia (0.8% versus 0.4%), and no patients in either treatment arm were identified with a clinical presentation of hemolytic anemia.16,17 In the Phase 3, multicenter, randomized, double-blind CANVAS trials in acute bacterial skin and skin structure infections (ABSSSIs), 11.6% of ceftaroline-treated patients had positive DAT results, compared with 4.3% of patients treated with vancomycin plus aztreonam, with no reports of hemolytic anemia in either group.15
Ceftobiprole, the active moiety of the prodrug ceftobiprole medocaril, is an advanced-generation, broad-spectrum cephalosporin, which has a rapid bactericidal effect against both methicillin-sensitive and methicillin-resistant Staphylococcus aureus infections.19 It is currently approved in many European and non-European countries for the treatment of community- and hospital-acquired pneumonia (excluding ventilator-associated pneumonia).20 DATs were not performed in four previous Phase 3 trials of ceftobiprole; however, there were no adverse events of hemolytic anemia reported in these trials.21–24 Also, to date, no cases of hemolytic anemia have been reported in the post-marketing setting, where experience of >70,000 patient-days has been recorded (unpublished data).
Here, we review safety data from three recent Phase 3 trials of ceftobiprole (one in pediatric patients with pneumonia, one in adults with ABSSSIs, and one in adults with S. aureus bacteremia), with regard to the incidence of positive DAT results and hemolytic anemia.
Patients and Methods
Design and Participants
This analysis includes patients enrolled in three recent or ongoing clinical trials. BPR-PIP-002 (NCT03439124) was a Phase 3, randomized, investigator-blinded, active-controlled, multicenter trial of ceftobiprole (n=94) versus intravenous standard-of-care cephalosporin ± vancomycin (n=44) in patients aged 3 months to <18 years with hospital- or community-acquired pneumonia requiring hospitalization and administration of intravenous antibiotics.25 TARGET (NCT03137173) was a Phase 3, randomized, double-blind, active-controlled, parallel-group, multicenter, non-inferiority trial of ceftobiprole (n=335) compared with vancomycin plus aztreonam (n=344) in hospitalized patients aged ≥18 years with a diagnosis of ABSSSI, who required intravenous antibacterial treatment.26 ERADICATE (NCT03138733) is an ongoing Phase 3, randomized, double-blind, active-controlled, parallel-group, multicenter, trial of ceftobiprole compared with daptomycin ± aztreonam in hospitalized patients aged ≥18 years with complicated forms of S. aureus bacteremia, including infective endocarditis.27 As of August 2020, 201 patients have been randomized 1:1 to ceftobiprole or daptomycin ± aztreonam in this trial. Safety assessments, including adverse event monitoring, physical examination, vital signs, safety laboratory tests, and other assessments, were performed regularly throughout all three trials.
Laboratory Assessments and Methodology
DATs were performed according to the following schedules: in the BPR-PIP-002 trial, in all children aged ≥6 years and in younger patients not treated with vancomycin, a DAT was performed at screening and at the test of cure (TOC) visit (7–14 days after the end of treatment [EOT]); in TARGET, a DAT was performed at baseline and EOT; and in ERADICATE, a DAT was performed at baseline, EOT, and at a post-treatment Day 70 visit.
For the BPR-PIP-002 trial, DATs were performed at Gdańsk Laboratory, Gdańsk, Poland (for samples from patients in Bulgaria, Hungary, and Romania) or at IMD Laboratory, Tbilisi, Georgia (for samples from patients in Georgia). For the TARGET and ERADICATE trials, DATs were performed at PPD Laboratories USA (Kentucky, USA) or PPD Laboratories Europe (Zaventem, Belgium). For all three trials, the DAT performed was an agglutination tube assay using polyspecific antiglobulin sera (BioRad Laboratories, California, USA). For the BPR-PIP-002 trial, positive tests were further analyzed by a semi-quantitative DG Gel card test (Grifols Diagnostics, Barcelona, Spain).
Results
Direct Antiglobulin Tests
BPR-PIP-002
A total of 102 patients (ceftobiprole n=72, ceftriaxone n=28, and ceftazidime n=2) had a DAT at baseline and 113 patients had a test at the TOC visit (ceftobiprole n=74, ceftriaxone n=37, and ceftazidime n=2) (Table 1). One patient had a test at an unscheduled visit on treatment day 9 (ceftobiprole n=1).
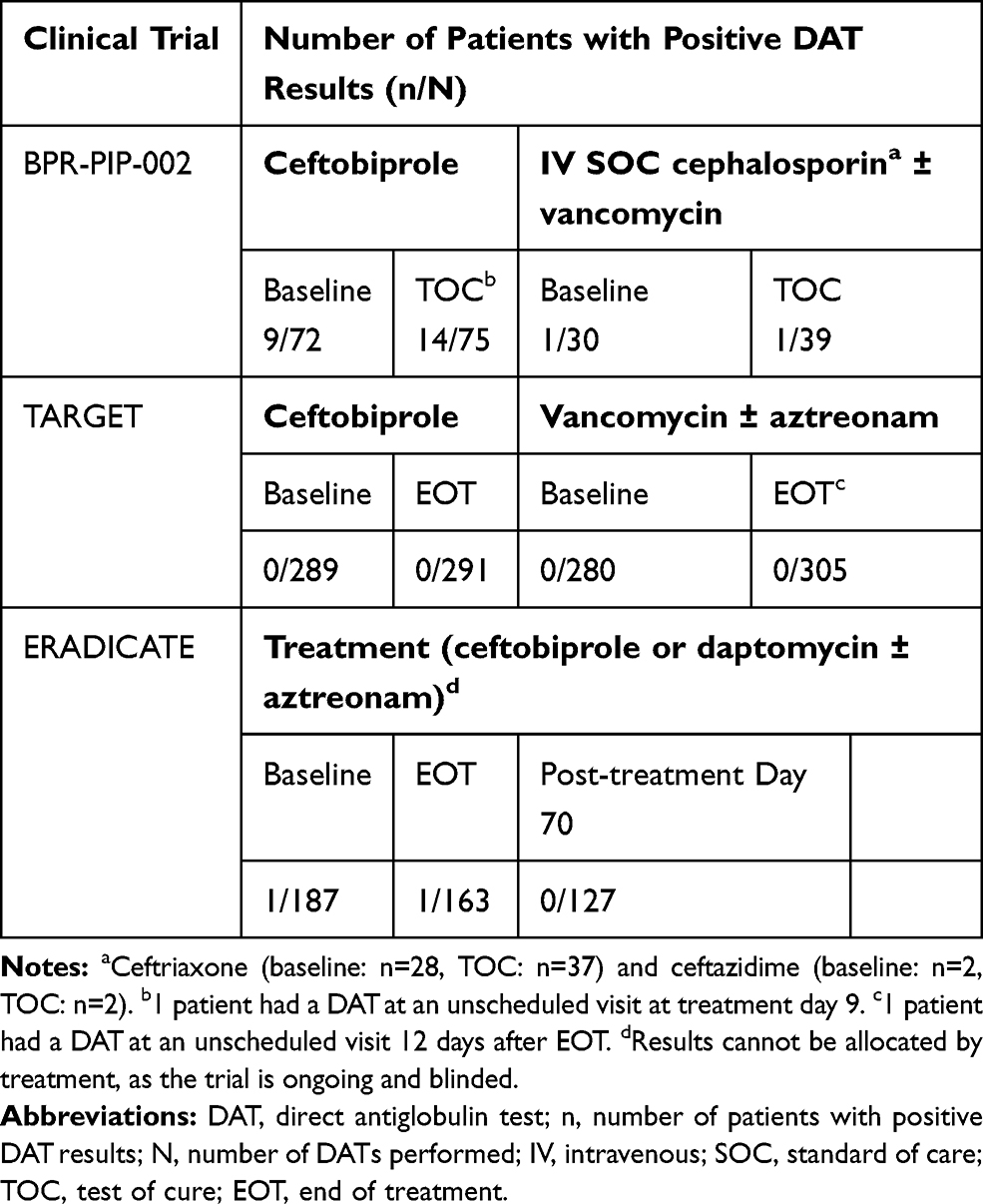 |
Table 1 Outcome of Direct Antiglobulin Testing in Phase 3 Clinical Trials of Ceftobiprole |
Of the ceftobiprole patients, a total of 18 recorded a positive DAT result. Nine had a positive result at baseline, five reported seroconversion (negative at baseline and positive at the TOC visit), and a further four had a positive result at the TOC visit but were not tested at baseline (Table 2). Only two patients had an increase in reaction strength from baseline to follow-up visit (the first patient had an increase from 1+ at baseline to 2+ at the TOC visit, and the second had an increase from 0.5+ at baseline to 1+ at treatment day 9). Of the ceftriaxone patients, a total of two patients recorded a positive DAT result. One had a positive result at baseline, but a subsequent negative result at the TOC visit. The other had a positive result at the TOC visit but was not tested at baseline (Table 2).
 |
Table 2 Breakdown of Positive Direct Antiglobulin Test Results in BPR-PIP-002 Trial by Visit |
TARGET
In the ceftobiprole group, 289 patients had a DAT at baseline and 291 patients at the EOT visit. In the vancomycin ± aztreonam group, 280 patients had a test at baseline and 304 patients at the EOT visit. One patient in the vancomycin ± aztreonam group had a DAT 12 days after EOT. All DATs were negative in both treatment groups (Table 1).
ERADICATE
As the trial is currently ongoing and blinded, the results cannot be reported by treatment group. One patient had a positive DAT result at baseline and at EOT. This patient did not have a test after EOT, including at the Day 70 visit. There was no evidence of hemolysis or hemolytic anemia in this patient at any time during the trial. All other DAT results were negative, including 186 patients at baseline, 162 patients at EOT visit, and 127 patients at the Day 70 visit. A total of 120 patients had negative DAT results both at the EOT and the Day 70 visits, and 114 patients had negative DAT results at all three visits. The results are summarized in Table 1.
Other Laboratory Tests
For all three trials, results of other blood tests, ie, hemoglobin, hematocrit, reticulocyte count and percent, haptoglobin, lactate dehydrogenase, bilirubin, and hepatic transaminases (alanine aminotransferase, aspartate aminotransferase) showed no evidence of hemolysis or hemolytic anemia in any patient.
Adverse Events
The adverse event profile for all three trials was consistent with that reported previously for ceftobiprole.21–24 No adverse events of hemolytic anemia were reported in any of the three trials included in this analysis.
Discussion
In this analysis of three large Phase 3 trials (n=1018), no evidence of hemolytic anemia associated with ceftobiprole was observed in either adults or children across several indications. Furthermore, no patients discontinued ceftobiprole treatment as a result of anemia. Evidence of DAT seroconversion was reported in five children treated with ceftobiprole in the BPR-PIP-002 trial. An additional four children had a positive result at the TOC visit, but a DAT was not conducted at baseline. For each of these cases, there were no other laboratory or clinical findings of hemolytic anemia. No evidence of DIIHA was reported in either the TARGET or ERADICATE trials, echoing results observed with another advanced-generation cephalosporin, ceftaroline, which reported no cases of DIIHA in several large Phase 3 trials.15–17
The differences in the frequency of positive DAT results between the BPR-PIP-002 trial and the TARGET/ERADICATE trials may reflect the use of different testing laboratories. Alternatively, as the patients were randomized 2:1 (ceftobiprole to standard-of-care cephalosporin) in the BPR-PIP-002 trial, these results may be due to the fact that a larger proportion of ceftobiprole-treated patients were included in this trial compared with TARGET and ERADICATE. It should also be noted that in the BPR-PIP-002 trial, after a minimum of 3 days’ treatment with intravenous antibiotics, patients who met standardized criteria for clinical improvement could be switched to an oral antibiotic (penicillins, cephalosporins, macrolides, clindamycin, or linezolid) at the discretion of the blinded investigator, to complete a minimum of 7 days’ antibiotic treatment. As such, there may be an influence of the oral antibiotics on the DAT result at the TOC visit. In the TARGET and ERADICATE trials, patients received intravenous antibiotics throughout the treatment course.
In a small number of hospitalized patients described in this analysis (10 in the BPR-PIP-002 trial and 1 in the ERADICATE trial), a positive DAT result was reported at baseline, ie, prior to initiation of treatment. This accounts for 1.3% of all baseline tests and is consistent with previous reports demonstrating that positive DAT results without evidence of hemolysis can occur in hospitalized patients.8 There are a number of potential causes of such results, of varying clinical significance.28 These can include older age, malignancy, and some infectious diseases including human immunodeficiency virus infection.7,28
There are a number of limitations associated with our analysis. Firstly, drug-dependent antibodies were not measured in patients with a positive DAT in the three trials described here. This may be relevant, as drug-dependent antibodies have previously been detected in patients without clinical evidence of significant hemolytic anemia, eg, in a single-center study, antibodies to piperacillin were detected in two out of 43 (4.7%) patients with cystic fibrosis; of these, one patient developed a mild immune hemolytic anemia.29 Secondly, in the BPR-PIP-002 trial, the DAT was performed 7–14 days after the end of treatment and therefore ceftobiprole would not be present in the sample. Of note, this should not impact the results from the TARGET and ERADICATE trials, where the DAT was performed at EOT.
Conclusions
Consistent with previous Phase 3 trials, the evidence presented here indicates that ceftobiprole administration may not be associated with DIIHA. A small number of positive DAT results were reported without evidence of hemolysis; this is consistent with previous reports from hospitalized patients.
Data Sharing Statement
All data relevant to the analysis are included in the article. The deidentified datasets used and analyzed during the current analysis are available from the corresponding author at any time upon reasonable request.
Ethics Approval and Informed Consent
All three trials described in this manuscript were conducted in compliance with applicable laws and regulations, ICH Good Clinical Practice guidelines and the Declaration of Helsinki, and the protocols were approved by the relevant Independent Ethics Committees/Institutional Review Boards (Supplementary Table 1). For adult patients, written informed consent was required prior to the conduct of any trial procedures. For pediatric patients, each child’s parent or legal guardian provided written informed consent. If appropriate, the child’s assent was also sought prior to participation in the trial.
Acknowledgments
The authors are grateful to the investigators, site personnel, patients, and parents who participated in these trials. Under the direction of the authors, medical writing support for the manuscript was provided by Stephanie Carter of Arc, a division of Spirit Medical Communications Group Limited, funded by Basilea Pharmaceutica International Ltd.
Author Contributions
KH contributed to analysis conceptions and designs, and acquisition of data. All authors made substantial contributions to analysis of data, took part in drafting the article or revising it critically for important intellectual content, agreed to submit to the current journal, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Disclosure
KH, TW, and MAG are employees of Basilea Pharmaceutica International Ltd. The authors report no other conflicts of interest in this work.
References
1. Garbe E, Andersohn F, Bronder E, et al. Drug induced immune haemolytic anaemia in the Berlin Case-Control Surveillance Study. Br J Haematol. 2011;154(5):644–653. doi:10.1111/j.1365-2141.2011.08784.x
2. Pierce A, Nester T. Pathology consultation on drug-induced hemolytic anemia. Am J Clin Pathol. 2011;136(1):7–12. doi:10.1309/AJCPBVLJZH6W6RQM
3. Habibi B. Drug induced red blood cell autoantibodies co-developed with drug specific antibodies causing haemolytic anaemias. Br J Haematol. 1985;61(1):139–143. doi:10.1111/j.1365-2141.1985.tb04069.x
4. Mueller-Eckhardt C, Salama A. Drug-induced immune cytopenias: a unifying pathogenetic concept with special emphasis on the role of drug metabolites. Transfus Med Rev. 1990;4(1):69–77. doi:10.1016/S0887-7963(90)70249-0
5. Salama A. Drug-induced immune hemolytic anemia. Expert Opin Drug Saf. 2009;8(1):73–79. doi:10.1517/14740330802577351
6. Branch DR. Drug-induced immune haemolytic anaemias. ISBT Sci Ser. 2019;14(1):49–52. doi:10.1111/voxs.12469
7. Parker V, Tormey CA. The direct antiglobulin test: indications, interpretation, and pitfalls. Arch Pathol Lab Med. 2017;141(2):305–310. doi:10.5858/arpa.2015-0444-RS
8. Zantek ND, Koepsell SA, Tharp DR
9. Garratty G, Arndt PA. Drugs that have been shown to cause drug-induced immune hemolytic anemia or positive direct antiglobulin tests: some interesting findings since 2007. Immunohematology. 2014;30(2):66–79.
10. Arndt PA, Garratty G. The changing spectrum of drug-induced immune hemolytic anemia. Semin Hematol. 2005;42(3):137–144. doi:10.1053/j.seminhematol.2005.04.004
11. Mayer B, Bartolmäs T, Yürek S, Salama A. Variability of findings in drug-induced immune haemolytic anaemia: experience over 20 years in a single centre. Transfus Med Hemother. 2015;42(5):333–339. doi:10.1159/000440673
12. Arndt PA, Leger RM, Garratty G. Serology of antibodies to second- and third-generation cephalosporins associated with immune hemolytic anemia and/or positive direct antiglobulin tests. Transfusion. 1999;39(11–12):1239–1246. doi:10.1046/j.1537-2995.1999.39111239.x
13. Arndt PA, Leger RM, Garratty G. Serologic characteristics of ceftriaxone antibodies in 25 patients with drug-induced immune hemolytic anemia. Transfusion. 2012;52(3):602–612. doi:10.1111/j.1537-2995.2011.03321.x
14. Northrop MS, Agarwal HS. Ceftriaxone-induced hemolytic anemia: case report and review of literature. J Pediatr Hematol Oncol. 2015;37(1):e63–66. doi:10.1097/MPH.0000000000000181
15. Corrado ML. Integrated safety summary of CANVAS 1 and 2 trials: phase III, randomized, double-blind studies evaluating ceftaroline fosamil for the treatment of patients with complicated skin and skin structure infections. J Antimicrob Chemother. 2010;65(Suppl 4):iv67–iv71. doi:10.1093/jac/dkq256
16. Goodman JJ, Martin SI. Critical appraisal of ceftaroline in the management of community-acquired bacterial pneumonia and skin infections. Ther Clin Risk Manag. 2012;8:149–156.
17. Rank DR, Friedland HD, Laudano JB. Integrated safety summary of FOCUS 1 and FOCUS 2 trials: phase III randomized, double-blind studies evaluating ceftaroline fosamil for the treatment of patients with community-acquired pneumonia. J Antimicrob Chemother. 2011;66(Suppl 3):iii53–iii59. doi:10.1093/jac/dkr099
18. Allergan. TEFLARO® (ceftaroline fosamil) prescribing information. 2019. Available from: https://media.allergan.com/actavis/actavis/media/allergan-pdf-documents/product-prescribing/Teflaro-USPI-09_2019-2.pdf.
19. Liapikou A, Cilloniz C, Torres A. Ceftobiprole for the treatment of pneumonia: a European perspective. Drug Des Devel Ther. 2015;9:4565–4572.
20. Electronic Medicines Compendium. Zevtera 500 mg powder for concentrate for solution for infusion. 2018. Available from: https://www.medicines.org.uk/emc/product/9164.
21. Noel GJ, Strauss RS, Amsler K, Heep M, Pypstra R, Solomkin JS. Results of a double-blind, randomized trial of ceftobiprole treatment of complicated skin and skin structure infections caused by gram-positive bacteria. Antimicrob Agents Chemother. 2008;52(1):37–44. doi:10.1128/AAC.00551-07
22. Noel GJ, Bush K, Bagchi P, Ianus J, Strauss RS. A randomized, double-blind trial comparing ceftobiprole medocaril with vancomycin plus ceftazidime for the treatment of patients with complicated skin and skin-structure infections. Clin Infect Dis. 2008;46(5):647–655. doi:10.1086/526527
23. Nicholson SC, Welte T, File TM
24. Awad SS, Rodriguez AH, Chuang YC, et al. A phase 3 randomized double-blind comparison of ceftobiprole medocaril versus ceftazidime plus linezolid for the treatment of hospital-acquired pneumonia. Clin Infect Dis. 2014;59(1):51–61. doi:10.1093/cid/ciu219
25. NCT03439124. Ceftobiprole in the treatment of pediatric patients with pneumonia. 2020. Available from: https://clinicaltrials.gov/ct2/show/NCT03439124.
26. Overcash J, Kim C, Keech R, et al. Ceftobiprole compared with vancomycin plus aztreonam in the treatment of acute bacterial skin and skin structure infections: results of a Phase 3, randomized, double-blind trial (TARGET). Clin Infect Dis. In press 2020. doi:10.1093/cid/ciaa974
27. Hamed K, Engelhardt M, Jones ME, et al. Ceftobiprole versus daptomycin in Staphylococcus aureus bacteremia: a novel protocol for a double-blind, phase III trial. Future Microbiol. 2020;15:35–48. doi:10.2217/fmb-2019-0332
28. Kim TO, Grimes AB, Kirk S, et al. Association of a positive direct antiglobulin test with chronic immune thrombocytopenia and use of second line therapies in children: a multi-institutional review. Am J Hematol. 2019;94(4):461–466. doi:10.1002/ajh.25409
29. Roehmel J, Specht P, Staab D, Schwarz C, Salama A, Mayer B. Risk of piperacillin-induced hemolytic anemia in patients with cystic fibrosis and antipseudomonal treatment: a prospective observational study. Transfusion. 2019;59(12):3746–3754. doi:10.1111/trf.15591
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.