Back to Journals » Journal of Pain Research » Volume 15
No Detectable Phenytoin Plasma Levels After Topical Phenytoin Cream Application in Chronic Pain: Inferences for Mechanisms of Action
Authors Kopsky DJ ![]() , Keppel Hesselink JM
, Keppel Hesselink JM ![]() , Russell AL, Vrancken AFJE
, Russell AL, Vrancken AFJE
Received 3 November 2021
Accepted for publication 27 January 2022
Published 9 February 2022 Volume 2022:15 Pages 377—383
DOI https://doi.org/10.2147/JPR.S345347
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Robert B. Raffa
David J Kopsky,1,2 Jan M Keppel Hesselink,1 Alan L Russell,3 Alexander FJE Vrancken2
1Institute for Neuropathic Pain, Amsterdam, the Netherlands; 2Department of Neurology, Brain Centre University Medical Center Utrecht, Utrecht University, Utrecht, the Netherlands; 3 Brampton, Ontario, Canada
Correspondence: David J Kopsky, Vespuccistraat 64-III, Amsterdam, 1056 SN, the Netherlands
, Tel +31-6-28671847
, Email [email protected]
Purpose: Topical phenytoin can act as an analgesic in chronic pain, but it is unclear if topical phenytoin gives rise to systemic side effects. Therefore, the aim of this study is: 1) to evaluate safety in chronic pain patients who used topical phenytoin up to 30% applied daily on intact skin and mucous membrane, through determining phenytoin plasma levels; and 2) to elaborate on the analgesic mechanism of action.
Patients and Methods: In this retrospective study, we collected demographic and clinical data from 33 chronic pain patients who used 10% to 30% phenytoin cream, and in whom blood samples were drawn for phenytoin concentration measurement between January 2017 until September 2020. The instruction was to withdraw blood 1 to 4 hours after the last topical phenytoin application. The primary outcome was the detectability of plasma phenytoin after daily use of topical phenytoin.
Results: Blood withdrawal was carried out after on average 14 treatment days with topical phenytoin and on average 2.5 hours after topical phenytoin application. The median daily applied amount of phenytoin cream was 1.2 grams, resulting in a median daily amount of 120 mg phenytoin on the skin. Phenytoin levels were below the limit of detection in all patients and no side effects were reported.
Conclusion: Plasma phenytoin levels were below the limit of detection after topical use of phenytoin cream formulations up to 30% on intact skin and mucous membrane for the treatment of chronic pain, without side effects emerging. This finding suggests that the mechanism of analgesic action resides in the skin.
Keywords: phenytoin cream, pain, plasma concentration, neuropathy, skin
Introduction
Phenytoin, a broad acting voltage-gated sodium channel (Nav) blocker, has been used for the treatment of epilepsy since 1938.1 The observation of gingival overgrowth in patients who used oral phenytoin initiated the idea to repurpose phenytoin for wound healing. In studies investigating topical phenytoin for the treatment of wounds, there was no evidence of systemic absorption or toxicity.2 One trial with a phenytoin-containing alginate-based hydrogel dressing (delivering 6 mg/cm2) for treatment of diabetic ulcers reported plasma levels between 0.6 and 2.2 mg/L, well below the therapeutic range of 10–20 mg/L as used for the treatment of epilepsy and neuropathic pain.3 In one case report, a phenytoin plasma level of 4.3 mg/L was reached after treatment of 2 pressure ulcers by applying topically a total of 12.5 grams daily 100% phenytoin powder during 4 months.2,4
To date, four published double-blind randomized placebo-controlled trials (RCTs) evaluated the effectiveness of oral phenytoin for the treatment of neuropathic pain and three of these evaluated how the pain reducing effect is related to plasma phenytoin concentrations (see Table 1 for details).5–8
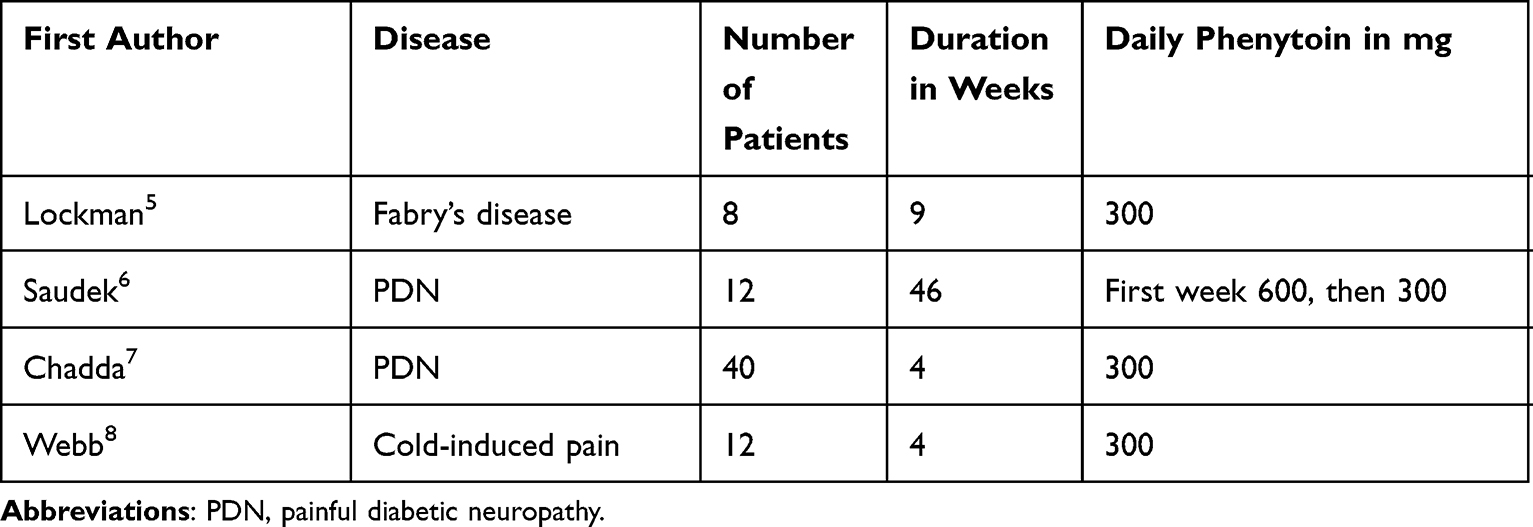 |
Table 1 Double-Blind Placebo-Controlled Cross-Over Trials Evaluating Pain Reduction After Oral Phenytoin |
Lockman et al revealed a correlation with pain relief and phenytoin plasma levels of more than 4 mg/L (range 1.6 to 33.3).5 In the trial by Saudek et al, oral phenytoin was adjusted if needed to achieve a therapeutic plasma level of 5 to 20 mg/L, reaching a mean plasma phenytoin concentration of 12.1 mg/L.6 No significant difference in analgesic effects was seen between oral phenytoin or placebo. In the trial by Chadda and Mathur, pain decreased in most patients after 4 days, which is about the time needed to reach a steady-state of phenytoin plasma levels, suggesting a central mechanism of action.7 Webb and Kamali revealed a significant association between analgesia and plasma phenytoin concentration.8 At 4¼ hour post-dose phenytoin maximum pain relief was achieved with a mean plasma concentration of about 4 mg/L. Interestingly, after 1¼ hours post-dose the mean maximum pain score was higher for phenytoin than for placebo, corresponding to a mean plasma phenytoin of around 2.5 mg/L, suggesting an analgesic effect above 2.5 mg/L.
While exploring several established oral drugs for their effectiveness in the form of topical application to treat neuropathic pain, we discovered that topical phenytoin had a pain relieving effect, and more surprisingly we found that the pain reducing effect had an onset of action of around 15 minutes.9 Also, there were no detectable phenytoin plasma levels after the application of phenytoin 10% and 20% formulations on intact skin, even not at high amounts up to 670 mg phenytoin per application.9,10 Based on these observations, we postulated an independent peripheral mechanism of action of topical phenytoin that is probably quite different from the central mode of action for oral phenytoin that requires therapeutic plasma concentrations.11
To monitor safety and to elaborate more on the mechanism of action, we determined phenytoin plasma levels after topical phenytoin application up to 30% for the treatment of chronic pain.
The collected data are part of daily clinical practice to ensure that the patient is being treated safely and was not carried out with the aim of systematic data collection and analysis. Therefore, according to Dutch law on the conduction of medical research, and in line with European guidelines, no approval from the ethics committee is needed.12,13 Also the Canadian authorities declared in article 2.4 of the Tri-Council Policy Statement that no research ethics approval is required, when human data, originally not gathered for research purposes, are used anonymously.14
Materials and Methods
Between January 2017 until September 2020, three pain physicians (DJK, ALR, JMKH) collected blood samples for the detection of phenytoin plasma levels from their patients using various concentrations of phenytoin cream. The samples were sent to independent laboratories in the Netherlands and Canada, the 2 countries in which the blood samples were taken. Inclusion criteria for phenytoin plasma level determination were: 1) age at least 18 years; 2) presence of chronic pain; and 3) use of topical phenytoin cream with a concentration of at least 10%. Because several different laboratories performed the plasma phenytoin measurement, the limit of detection varied between <0.2 and <1.8 mg/L, mostly between <0.5 and <0.8 mg/L. To ensure maximum concentration of phenytoin plasma round the time of blood withdrawal, patients were instructed to apply the phenytoin cream 1 to 4 hours before blood withdrawal. The following clinical and demographic data were collected retrospectively: gender, age, diagnosis, used phenytoin cream concentration, number of treatment days before blood withdrawal, hours between blood withdrawal and last application, number of daily applications, amount per application, onset of action, duration and degree of pain reduction. In follow-up visits patients were asked about the treatment effect and possible side effects while using topical phenytoin. Clinical details of 17 patients have been described previously.9,10
Descriptive statistics are summarized as mean (standard deviation) for normally distributed continuous data or median (interquartile range) in case of a non-normal distribution, and frequency (proportion) for categorical data. As described earlier, the standard phenytoin plasma determination was measured with high-performance liquid chromatography of the plasma protein bound phenytoin fraction, which is approximately 90% of the total amount of phenytoin in plasma.9,15 The statistical analysis was performed using SPSS 22 (SPSS Inc., Chicago, IL, USA).
Results
From January 2017 until September 2020 blood samples for phenytoin concentration measurement were taken from 33 patients, of which 14 were Canadian. Demographic data, diagnoses and phenytoin cream and usage characteristics are presented in Table 2. In all patients, phenytoin levels were below the limit of detection after topical phenytoin application up to 30%. Blood withdrawal was carried out after on average 16 treatment days and on average 2.5 hours after topical phenytoin application. The median daily amount of phenytoin cream was 1.2 grams, resulting in a median daily amount of 120 mg phenytoin on the skin. In Figure 1, the distribution of hours between last topical phenytoin application and blood withdrawal, the number of treatment days with topical phenytoin before blood withdrawal, the amount of daily phenytoin and the topical phenytoin concentration is presented. In 3 patients who used phenytoin 20%, 25% and 30% cream, phenytoin plasma levels were tested twice with at least 2 months between the laboratory tests. One 27-year-old patient applied phenytoin cream intravaginally, 0.6 grams per application twice daily. Her first application was phenytoin 10%, whereafter phenytoin 20%, with 46 and 13 treatment days before blood withdrawal, respectively and one month interval between blood withdrawals. Also, in this patient no phenytoin plasma levels were detected. No side effects were reported.
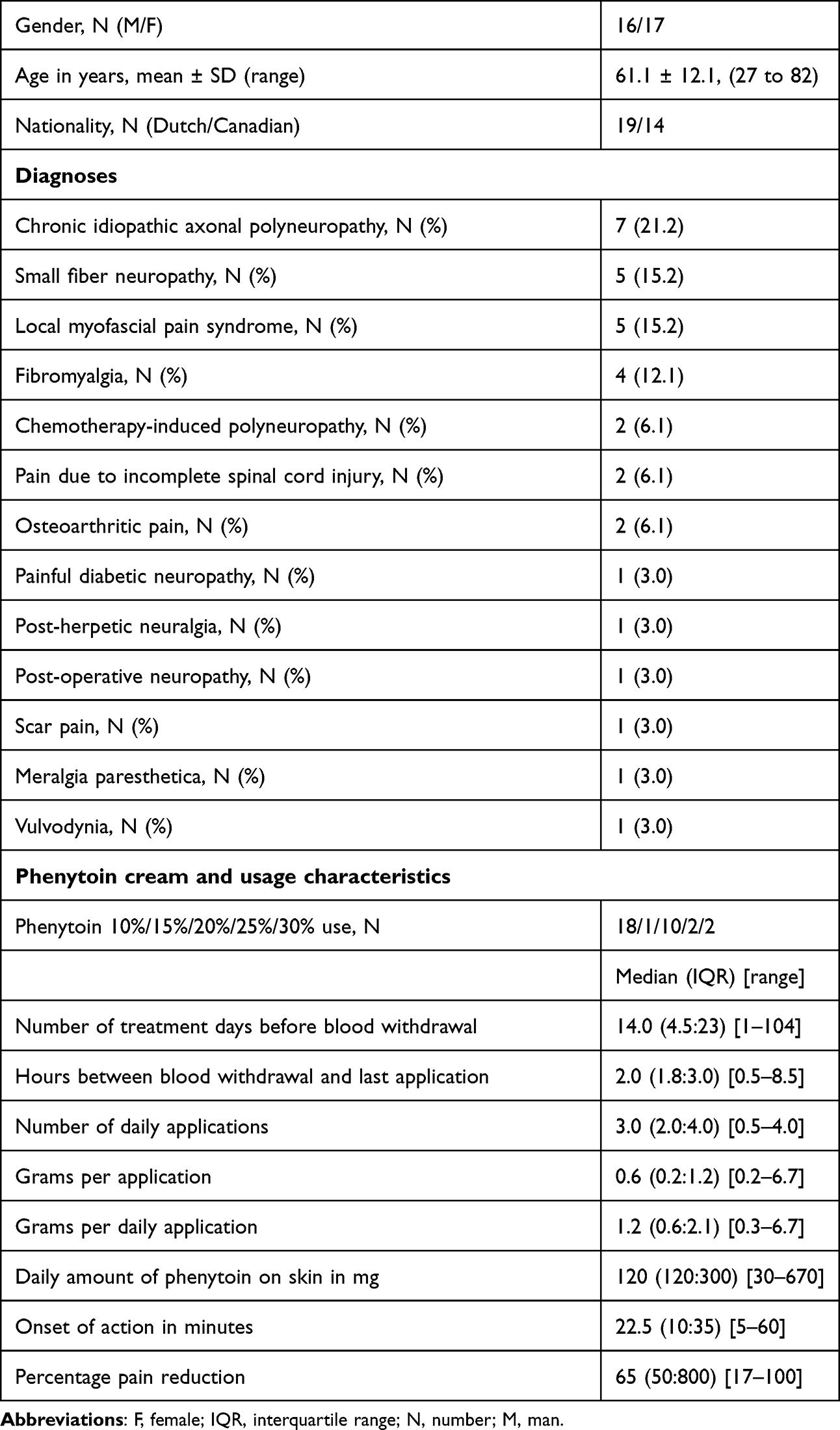 |
Table 2 Demographic Data, Diagnoses and Use Characteristics |
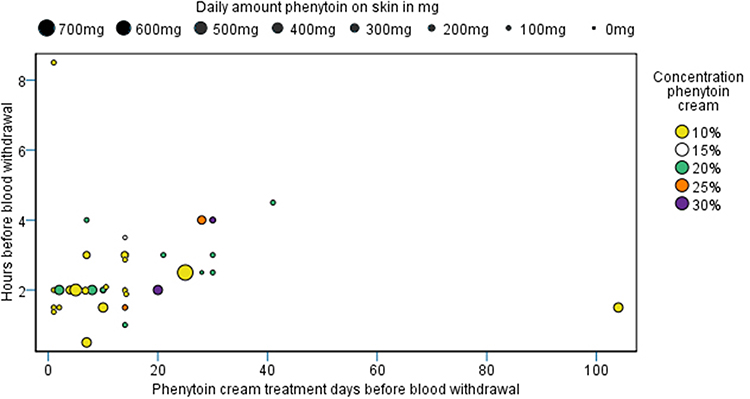 |
Figure 1 Topical phenytoin characteristics before blood withdrawal. Note: In 4 patients the second-time phenytoin plasma measurement is not shown in the figure. |
Discussion
No phenytoin plasma levels were detected and no side effects were reported after the topical use of phenytoin cream in a dose-range from 10% to 30%. These findings support earlier similar findings in 17 patients, included in this cohort.9,10 In 4 patients blood withdrawals were conducted twice with 1 to 2 months’ time interval (not presented in Figure 1) and no phenytoin plasma levels were detected. This indicates that phenytoin does not accumulate in the plasma. Even after vaginal application no plasma levels were detected. The vagina and vulva have a stratum corneum which is non-keratinized and do not have an impermeable intercellular lipid envelope as in the epidermis.16,17
The absence of plasma phenytoin might be related to some of its physicochemical properties of phenytoin such as its lipophilicity.18 Phenytoin can easily penetrate the lipophilic stratum corneum due to its high lipophilicity and low molecular weight of 252 Daltons; the penetration rate might slow down when phenytoin reaches the viable layers of the epidermis, especially since the epidermis is more aqueous and avascular.19 Possibly after the topical application of phenytoin a temporary reservoir of phenytoin might develop in the stratum corneum and in a lesser extent in the viable layers of the epidermis. Future studies would be necessary to elucidate the variable penetrance of phenytoin in the epidermis.
A noticeable pain reduction was reported after a median onset of action of 22.5 minutes. This fast onset of action and no systemic side effects also correspond with earlier reports,9,20,21 and supports a peripheral mechanism of action. In contrast, pain reduction after intake of oral phenytoin emerges approximately after 24 hours, supporting a central mechanism of action.22–25 Following oral phenytoin withdrawal, recurrence of pain did not appear for 48 to 72 hours, also suggestive for an effect related to phenytoin plasma levels and thus a central mechanism of action.23 Results from the RCTs examining oral and intravenous phenytoin furthermore indicate that relevant phenytoin plasma levels are needed for obtaining some pain relief in several neuropathic pain syndromes.26
Although onset of pain reduction was fast, there was a difference in onset of pain relief from 5 to 60 minutes. This could be explained by variable thickness of the stratum corneum and the main type of cells influenced. The very fast onset of action might mainly be due to the influence of phenytoin on keratinocytes; the slower onset of action might be mainly from an effect on the peripheral nerves after diffusion through upper epithelial layers.
The keratinocytes act as an umbrella of tissue covering the peripheral nerve endings in the epidermis, influencing each other. The expression of neuroactivators and voltage and ion-gated channels in the epidermis are suggestive for complex autocrine and paracrine signaling between keratinocytes and neural tissues, influencing sensory signaling.27 For example, activation with light of keratinocytes, through genetically engineered channel rhodopsin, resulted in a withdrawal reflex, similar to a painful stimulus.27 This behavior coincided with electrical signals in the nerves, even though the nerves themselves were not light sensitive. Another animal study showed that stimulation with capsaicin in mice with TRPV1 receptors expressed only on the keratinocytes but not on peripheral nerves evoked acute paw-licking nocifensive behavior and a conditioned place aversion reaction.28 Another animal model revealed that stimulation of CB2 cannabis receptors present on keratinocytes, but not on peripheral nerves, led to an indirect antinociceptive effect through release of β-endorphin from keratinocytes.29 These experiments clearly indicate that keratinocyte stimulation alone can result in the activation of peripheral sensory nerve endings embedded in the epidermis.
Nav receptors, the main targets of phenytoin, are not only widely distributed on the peripheral nerve endings in the epidermis but also on the keratinocytes.30,31 In chronic pain states, the expression on keratinocytes of the subtypes Nav1.5, 1.6 and 1.7 is increased, while Nav1.1, 1.2 and 1.8 also appear on keratinocytes.31 The fast onset of action and the absence of detection of phenytoin levels in the blood thus might be explained by the fact that phenytoin besides directly acting on Nav receptors of peripheral nerve endings, also acts on Nav receptors on keratinocytes.
Our observation that phenytoin cream also has an analgesic effect beyond placebo in patients with musculoskeletal pain can be explained, and can be observed in two further diagnoses: fibromyalgia and myofascial pain syndrome. Fibromyalgia is chronic widespread diffuse musculoskeletal pain and tenderness, with the presence of peripheral and central sensitization.32 About 50% of fibromyalgia patients have concomitantly a small fiber neuropathy, which has been confirmed with skin biopsy.33,34 The pain reducing effect of phenytoin cream in fibromyalgia patients could be explained due to dampening the coexistent small fiber neuropathic pain, and reduction of peripheral input, resulting in silencing central sensitization.
Myofascial pain syndrome consists of focal hyperalgesic myofascial contractures, termed myofascial trigger points, which results in hyperalgesia at the trigger points involving the muscle, subcutis and the skin.35,36 In this pain syndrome peripheral and central sensitization have been described.35 Hyperalgesia can be effectively reduced with a local topical Nav blocker, such as lidocaine,36 and possibly also with phenytoin.
Previously, we speculated that the mechanism of action of topical phenytoin would be linked to three tissue components of the skin: small nerve fibers, keratinocytes and immunocompetent cells.11 Our current findings further support this speculation, and encourage a rethinking about the therapeutic role of targeting the skin in chronic pain. The skin might very well function as a biofeedback system, sending inhibiting signals to the central nervous system.37
Conclusion
In patients with chronic pain, no phenytoin plasma levels were detected after around 2 weeks usage of topical phenytoin cream in a dose-range of 10% to 30%. Furthermore, no systemic side effects were reported. This is suggestive of a peripheral mechanism of action, in which the skin seems to act as a biofeedback system.
Acknowledgments
We would like to acknowledge Mrs Janice Thompson, who helped to collect phenytoin plasma data.
Disclosure
DJK and JMKH are holders of two patent applications: Topical phenytoin for use in the treatment of peripheral neuropathic pain (WO2018106107); and Topical pharmaceutical composition containing phenytoin and a (co-)analgesic for the treatment of chronic pain (WO2018106108). AFJEV reports grants from Prinses Beatrix Spierfonds and Dr C.J. Vaillantfonds for EPHENE-study (randomized trial on effectiveness of phenytoin cream vs placebo cream for neuropathic pain in idiopathic polyneuropathy). DJK and JMKH are involved in the EPHENE-study. The authors report no other conflicts of interest in this work.
References
1. Keppel Hesselink JM, Kopsky DJ. Phenytoin: 80 years young, from epilepsy to breast cancer, a remarkable molecule with multiple modes of action. J Neurol. 2017;264(8):1617–1621. doi:10.1007/s00415-017-8391-5
2. Bhatia A, Prakash S. Topical phenytoin for wound healing. Dermatol Online J. 2004;10(1):5. doi:10.5070/D30Z3612W1
3. Shaw J, Hughes CM, Lagan KM, Stevenson MR, Irwin CR, Bell PM. The effect of topical phenytoin on healing in diabetic foot ulcers: a randomized controlled trial. Diabet Med. 2011;28(10):1154–1157. doi:10.1111/j.1464-5491.2011.03309.x
4. Anstead GM, Hart LM, Sunahara JF, Liter ME. Phenytoin in wound healing. Ann Pharmacother. 1996;30(7–8):768–775. doi:10.1177/106002809603000712
5. Lockman LA, Hunninghake DB, Krivit W, Desnick RJ. Relief of pain of Fabry’s disease by diphenylhydantoin. Neurology. 1973;23(8):871–875. doi:10.1212/WNL.23.8.871
6. Saudek CD, Werns S, Reidenberg MM. Phenytoin in the treatment of diabetic symmetrical polyneuropathy. Clin Pharmacol Ther. 1977;22(2):196–199. doi:10.1002/cpt1977222196
7. Chadda VS, Mathur MS. Double blind study of the effects of diphenylhydantoin sodium on diabetic neuropathy. J Assoc Physicians India. 1978;26(5):403–406.
8. Webb J, Kamali F. Analgesic effects of lamotrigine and phenytoin on cold-induced pain: a crossover placebo-controlled study in healthy volunteers. Pain. 1998;76(3):357–363. doi:10.1016/S0304-3959(98)00068-2
9. Kopsky DJ, Keppel Hesselink JM. Phenytoin cream for the treatment of neuropathic pain: case series. Pharmaceuticals. 2018;11(2):53. doi:10.3390/ph11020053
10. Russell AL, Kopsky DJ, Hesselink JMK. Phenytoin cream for the treatment of sciatic pain: clinical effects and theoretical considerations: case report. J Pain Palliat Care Pharmacother. 2020;34(2):99–105. doi:10.1080/15360288.2020.1733169
11. Keppel Hesselink JM, Kopsky DJ, Bhaskar AK. Skin matters! The role of keratinocytes in nociception: a rational argument for the development of topical analgesics. J Pain Res. 2016;10:1–8. doi:10.2147/JPR.S122765
12. Your research: is it subject to the WMO or not? Central Committee on Research Involving Human Subjects. Available from: https://english.ccmo.nl/investigators/legal-framework-for-medical-scientific-research/your-research-is-it-subject-to-the-wmo-or-not.
13. Regulation (EU) No 536/2014 of the European Parliament and of the council of 16 April 2014 on clinical trials on medicinal products for human use, and repealing Directive 2001/20/EC. Available from: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=celex%3A32014R0536. Accessed November 2, 2021.
14. Canadian Institutes of Health Research, Natural Sciences and Engineering Research Council of Canada, and Social Sciences and Humanities Research Council. Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans; December, 2018.
15. Peterson GM, McLean S, Aldous S, Von Witt RJ, Millingen KS. Plasma protein binding of phenytoin in 100 epileptic patients. Br J Clin Pharmacol. 1982;14(2):298–300. doi:10.1111/j.1365-2125.1982.tb01981.x
16. Farage M, Maibach H. Lifetime changes in the vulva and vagina. Arch Gynecol Obstet. 2006;273(4):195–202. doi:10.1007/s00404-005-0079-x
17. Anderson DJ, Marathe J, Pudney J. The structure of the human vaginal stratum corneum and its role in immune defense. Am J Reprod Immunol. 2014;71(6):618–623. doi:10.1111/aji.12230
18. Widanapathirana L, Tale S, Reineke TM. Dissolution and solubility enhancement of the highly lipophilic drug phenytoin via interaction with Poly(N-isopropylacrylamide-co-vinylpyrrolidone) excipients. Mol Pharm. 2015;12(7):2537–2543. doi:10.1021/acs.molpharmaceut.5b00202
19. Nielsen JB, Benfeldt E, Holmgaard R. Penetration through the Skin Barrier. Curr Probl Dermatol. 2016;49:103–111.
20. Kopsky DJ, Keppel Hesselink JM. Single-Blind Placebo-Controlled Response test with phenytoin 10% cream in neuropathic pain patients. Pharmaceuticals. 2018;11(4):122. doi:10.3390/ph11040122
21. Kopsky DJ, Vrancken AFJE, van Eijk RPA, Notermans NC. Usefulness of a double-blind placebo-controlled response test to demonstrate rapid onset analgesia with phenytoin 10% cream in polyneuropathy. J Pain Res. 2020;13:877–882. doi:10.2147/JPR.S243434
22. Bergouignan M, d’Aulnay N. Effect of diphenyl-hydantoinate salt on essential trigeminal neuralgia. Rev Otoneuroopthal (Paris). 1951;23:427–431.
23. Iannone A, Baker AB, Morrell F. Dilantin in the treatment of trigeminal neuralgia. Neurology. 1958;8(2):126–128. doi:10.1212/WNL.8.2.126
24. Lamberts AE. Tic doulourex. J Mich State Med Soc. 1959;58(1Part 1):95–96.
25. Ellenberg M. Treatment of diabetic neuropathy with diphenylhydantoin. N Y State J Med. 1968;68(20):2653–2655.
26. Tremont-Lukats IW, Megeff C, Backonja MM. Anticonvulsants for neuropathic pain syndromes: mechanisms of action and place in therapy. Drugs. 2000;60(5):1029–1052. doi:10.2165/00003495-200060050-00005
27. Baumbauer KM, DeBerry JJ, Adelman PC, et al. Keratinocytes can modulate and directly initiate nociceptive responses. eLife. 2015;4:e09674. doi:10.7554/eLife.09674
28. Pang Z, Sakamoto T, Tiwari V, et al. Selective keratinocyte stimulation is sufficient to evoke nociception in mice. Pain. 2015;156(4):656–665. doi:10.1097/j.pain.0000000000000092
29. Ibrahim MM, Porreca F, Lai J, et al. CB2 cannabinoid receptor activation produces antinociception by stimulating peripheral release of endogenous opioids. Proc Natl Acad Sci U S A. 2005;102(8):3093–3098. doi:10.1073/pnas.0409888102
30. Bennett DL, Clark AJ, Huang J, Waxman SG, Dib-Hajj SD. The role of voltage-gated sodium channels in pain signaling. Physiol Rev. 2019;99(2):1079–1151. doi:10.1152/physrev.00052.2017
31. Zhao P, Barr TP, Hou Q, et al. Voltage-gated sodium channel expression in rat and human epidermal keratinocytes: evidence for a role in pain. Pain. 2008;139(1):90–105. doi:10.1016/j.pain.2008.03.016
32. Sluka KA, Clauw DJ. Neurobiology of fibromyalgia and chronic widespread pain. Neuroscience. 2016;338:114–129. doi:10.1016/j.neuroscience.2016.06.006
33. Grayston R, Czanner G, Elhadd K, et al. A systematic review and meta-analysis of the prevalence of small fiber pathology in fibromyalgia: implications for a new paradigm in fibromyalgia etiopathogenesis. Semin Arthritis Rheum. 2019;48(5):933–940.
34. Kelley MA, Hackshaw KV. Intraepidermal nerve fiber density as measured by skin punch biopsy as a marker for small fiber neuropathy: application in patients with fibromyalgia. Diagnostics (Basel, Switzerland). 2021;11(3):536.
35. Niddam DM, Chan RC, Lee SH, Yeh TC, Hsieh JC. Central representation of hyperalgesia from myofascial trigger point. NeuroImage. 2008;39(3):1299–1306. doi:10.1016/j.neuroimage.2007.09.051
36. Affaitati G, Fabrizio A, Savini A, et al. A randomized, controlled study comparing a lidocaine patch, a placebo patch, and anesthetic injection for treatment of trigger points in patients with myofascial pain syndrome: evaluation of pain and somatic pain thresholds. Clin Ther. 2009;31(4):705–720. doi:10.1016/j.clinthera.2009.04.006
37. Baron R, Hans G, Dickenson AH. Peripheral input and its importance for central sensitization. Ann Neurol. 2013;74(5):630–636. doi:10.1002/ana.24017
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.