")
Back to Journals » Psychology Research and Behavior Management » Volume 13
Night-Eating Syndrome and Depressive Symptoms in College Freshmen: Fitness Improvement Tactics in Youths (FITYou) Project
Authors Guo F, Tian Y , Cui Y, Huang C
Received 9 October 2019
Accepted for publication 5 February 2020
Published 24 February 2020 Volume 2020:13 Pages 185—191
DOI https://doi.org/10.2147/PRBM.S234025
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Feng Guo,1 Ying Tian,2 Yufei Cui,1 Cong Huang3,4
1Institute of Exercise Epidemiology and Department of Physical Education, Huaiyin Institute of Technology, Huai’an, People’s Republic of China; 2College of Sports Science, Shenyang Normal University, Shenyang, People’s Republic of China; 3Department of Sports and Exercise Science, College of Education, Zhejiang University, Hangzhou, People’s Republic of China; 4Department of Medicine and Science in Sports and Exercise, Tohoku University Graduate School of Medicine, Sendai, Japan
Correspondence: Feng Guo
Institute of Exercise Epidemiology and Department of Physical Education, Huaiyin Institute of Technology, Huai’an 223003, People’s Republic of China
Email [email protected]
Cong Huang
Department of Sports and Exercise Science, College of Education, Zhejiang University, 148 Tianmushan Road, Hangzhou 310007, People’s Republic of China
Email [email protected]
Background: Emerging evidence has shown that night-eating syndrome is correlated to depressive symptoms. However, these studies were mainly small-scale investigations.
Purpose: This study aimed to examine the association of night-eating syndrome with depressive symptoms among college students using a large-scale sample.
Methods: A cross-sectional study, which was a part of the Fitness Improvement Tactics in Youth Project, was conducted in 2017. The current study included 3278 college freshmen from Shenyang, China. They completed self-administered questionnaires and provided their sociodemographic and lifestyle information. Night-eating syndrome was assessed using the night-eating questionnaire (NEQ). Depressive symptoms were measured using the Self-rating Depression Scale (SDS).
Results: Of participants, 5.4% had night-eating syndrome (NEQ score ≥ 30), and 21.3% had depressive symptoms (SDS score ≥ 53). Prevalence of night-eating syndrome was higher in male than female students (p = 0.006). Logistic regression analysis indicated that students with night-eating syndrome had a higher prevalence of depressive symptoms than those without the syndrome after adjusting covariates (odds ratios [95% CI]: 3.28 [2.40, 4.48], p < 0.001). Consistent results were found when night-eating syndrome was defined as NEQ score ≥ 25. In addition, analysis of covariance showed a significant association between NEQ quartiles and SDS score (mean [95% CI]: Q1, 44.4 [43.8, 45.0]; Q2, 43.4 [42.7, 44.0]; Q3, 44.4 [43.7, 45.1]; Q4, 47.5 [46.9, 48.2], p < 0.001 for linear and quadratic trend).
Conclusion: This study showed an association between night-eating syndrome and depressive symptoms among Chinese college freshmen.
Keywords: night eating, eating behaviors, depressive symptoms, college students, youth
Introduction
Depression is a common psychiatric disorder, characterized by persistent sadness and a loss of interest in activities. It can be long-lasting or recurrent, substantially impairing an individual’s ability to function at work or school or cope with daily life. When maximally severe, it can even lead to suicide.1 Moreover, depressive symptoms were critical risk factors for loss of life,2 even at low levels of symptom severity.3 Evidence has shown that the prevalence of depressive symptoms was higher in younger than middle-aged and older adults, which indicates the importance of preventing depressive symptoms in younger people.4 In China, the overall prevalence of depressive symptoms among college students was high. The reported prevalence of depression among the 39 individual study populations ranged from 3.0% to 80.6%, with a pooled prevalence of 23.8%.5 This previous study revealed that the prevalence of depressive symptoms in southern areas of China was higher than in northern areas of China. This variance could be explained by differences in education, family income, medical insurance, and other social-culture factors between southern and northern parts of China.5 This suggests that it is important to pay more attention to the development of appropriate mental health-care strategies for university students in China.
Emerging evidence has indicated that night-eating syndrome may be a potential contributor to depressive symptoms. The clinical phenomenon of night-eating syndrome was first described by Stunkard et al6 as a disordered eating style characterized by morning anorexia, evening hyperphagia, and insomnia. Geliebter et al reported that the subjects with night-eating syndrome, primarily an eating disorder, were more likely to have a depressed mood.7 Most recently, a study of 301 Italian non-clinical adolescents aged 15–19 years indicated a significant association between night-eating syndrome and depressive symptoms.8 We previously reported that habitual snacking after dinner was significantly associated with the incidence of depressive symptoms in Japanese middle-aged adults during a 2-year follow-up.9 Moreover, we found an interaction effect of snacking after dinner and dining shortly before bedtime on depressive symptoms.9 Although the association between night-eating disorders and depressive symptoms has been examined by several studies, such an association in young adults is still unclear. Furthermore, a large-scale epidemiological investigation is needed to confirm the association of night-eating syndrome with depressive symptoms.
Thus, this study aimed to investigate the association between night-eating syndrome and depressive symptoms among Chinese college students. Further, the second purpose of the current study was to determine whether night-eating syndrome was linearly (or nonlinearly) associated with depressive symptoms.
Methods
Study Participants
The data for this study were taken from the baseline survey of the project of Fitness Improvement Tactics in Youths (FITYou), which is a research project dedicated to promoting the physical and mental health of college students. The data were collected through health checkups, physical fitness tests, and self-reported questionnaires. The main indicators included blood parameters, body composition, physical fitness, mental health, and quality of life, etc. The FITYou Project seeks to find the risk factors affecting the health status of college students through socioeconomic status and lifestyles. Details of the FITYou Project are described elsewhere.10
In September 2017, 4717 freshmen from Shenyang Normal University in China were invited to participate in the study, of which 4323 agreed to participate and submitted written informed consent (response rate = 91.6%). In addition, 218 students had missing data on physical examination, 436 on depressive symptoms, and 259 on night-eating behaviors. Among the remaining 3410 students, data were missing on sex (n=9), age (n=31), body mass index (BMI) (n=8), smoking status (n=11), drinking status (n=36), and sleep duration (n=37) to different degrees. Finally, a total of 3278 freshmen were included in the study. The study was conducted in strict adherence to the Helsinki Declaration,11 protecting the rights of participants and ensuring their safety. The research plan was approved by the Ethics Committee of College of Education, Zhejiang University.
Assessment of Depressive Symptoms
The Self-rating Depression Scale (SDS) is a tool for measuring depressive symptoms. It was developed by Zung in 1965.12 SDS has a good internal consistency with a Cronbach alpha exceeding 0.8 among the general population.13,14 It consists of 20 items, including two on psycho-emotional symptoms, eight on physical disorders, two on psychomotor disorders, and eight on depressive psychological disorders. Each item was divided into four grades according to the frequency of symptoms, 10 of which were positive scores and 10 were reverse scores. If it is a positive score, it is rated as 1, 2, 3, and 4 points in turn; the reverse score is rated as 4, 3, 2, and 1. After the evaluation is completed, the scores of the 20 items are added together to obtain the total coarseness, and then the coarse fraction is multiplied by 1.25 to obtain the integer part, and the standard score is obtained. According to the Chinese version of the scale, the SDS standard score is 53 points.15 In this study, depressive symptoms were defined as having SDS scores ≥53.
Assessment of Night-Eating Syndrome
Night-eating syndrome was assessed using the night-eating questionnaire (NEQ), which is a validated 14-item instrument asking respondents to rate their night-eating behaviors.16 The Cronbach’s alpha for the total scale was 0.70.16 A 5-point Likert scale is used to measure the severity of symptoms associated with this syndrome. It measures four features of night-eating, including nocturnal ingestion, evening hyperphagia, morning anorexia, and mood/sleep. The total score of 13 items ranges from 0 to 52, and each item is scored from 0 to 4. Higher scores indicate more severe pathology. Two commonly used cutoff values of night-eating syndrome are ≥25 or ≥30 points,16 and both were used in this study. Also, NEQ scores were divided into 4 categories according to its distribution to examine the linear or quadratic trends of SDS scores in quartiles of NEQ scores.
Relevant Covariates
The potential covariates regarding sociodemographic (sex and age) and lifestyle-related factors (smoking status, alcohol use, and sleep duration) were assessed using a self-administered questionnaire. Age was calculated based on the birthdate and date of anthropometric examination. Lifestyle-related information containing questions about smoking status (current, former, or never), alcohol use (current drinker, non-drinker), and sleep duration (<6, 6–7, 7–8, >8 hrs) were obtained directly through multiple choices in the questionnaire. The anthropometric parameter of BMI was calculated using the height and weight [body weight (kg)/height (m2)], which were measured in health examinations by medical practitioners. BMI was used as a continuous variable for statistical analysis.
Statistical Analysis
For participants’ characteristics according to night-eating syndrome, t-test was used for continuous variables and chi-squared test for categorical variables. Dichotomous variables were described as percentages, and continuous variables were expressed as arithmetic means (standard deviations [SD]).
To examine the association between night-eating syndrome and depressive symptoms, logistic regression analyses were used to show the odds ratios (ORs) and 95% confidence interval (CI) of depressive symptoms in college freshmen with night-eating syndrome, and they were compared with those without the syndrome. In multivariable analyses, there were three statistical models adjusted for covariates. Model 1 included age and sex. Model 2 added lifestyle-related variables, such as smoking status, alcohol use, and sleep duration. Model 3 further added BMI as a covariate. Moreover, to determine the linear or quadratic association of night-eating syndrome and depressive symptoms, analysis of covariance was also conducted. A Bonferroni's test was then used to assess the difference among each category of NEQ scores. Data were shown as mean and 95% CI.
All tests were two-tailed, and p < 0.05 was considered statistically significant. All statistical analyses were executed using IBM SPSS Statistics 22.0 software (IBM Corp, Armonk, NY, USA).
Results
Participants’ Characteristics
According to the descriptive analysis, a proportion of female college freshmen accounted for 71.7% (n=2349) of 3278 study participants. Average age (± SD) of the total sample was 18.4 ± 1.3 years. Average NEQ scores were 28.2 ± 3.9 points, and the prevalence of night-eating syndrome was 9.2% (n=303) for NEQ ≥25 points and 5.4% (n=176) for NEQ ≥30 points. The prevalence of depressive symptoms was 21.3% (n=697) in this study.
Table 1 shows the characteristics of the study participants according to night-eating syndrome. When night-eating syndrome was defined as NEQ score ≥25 points, participants with night-eating syndrome tended to be male (p = 0.007), be older (p = 0.031) and have longer sleep duration (p = 0.051) than those without the syndrome. Associations of the syndrome with other variables including smoking status, alcohol use, and BMI were not observed. A significant association between sex (male) and night-eating syndrome was also found, but not other variables, when night-eating syndrome was defined as NEQ score ≥30 points.
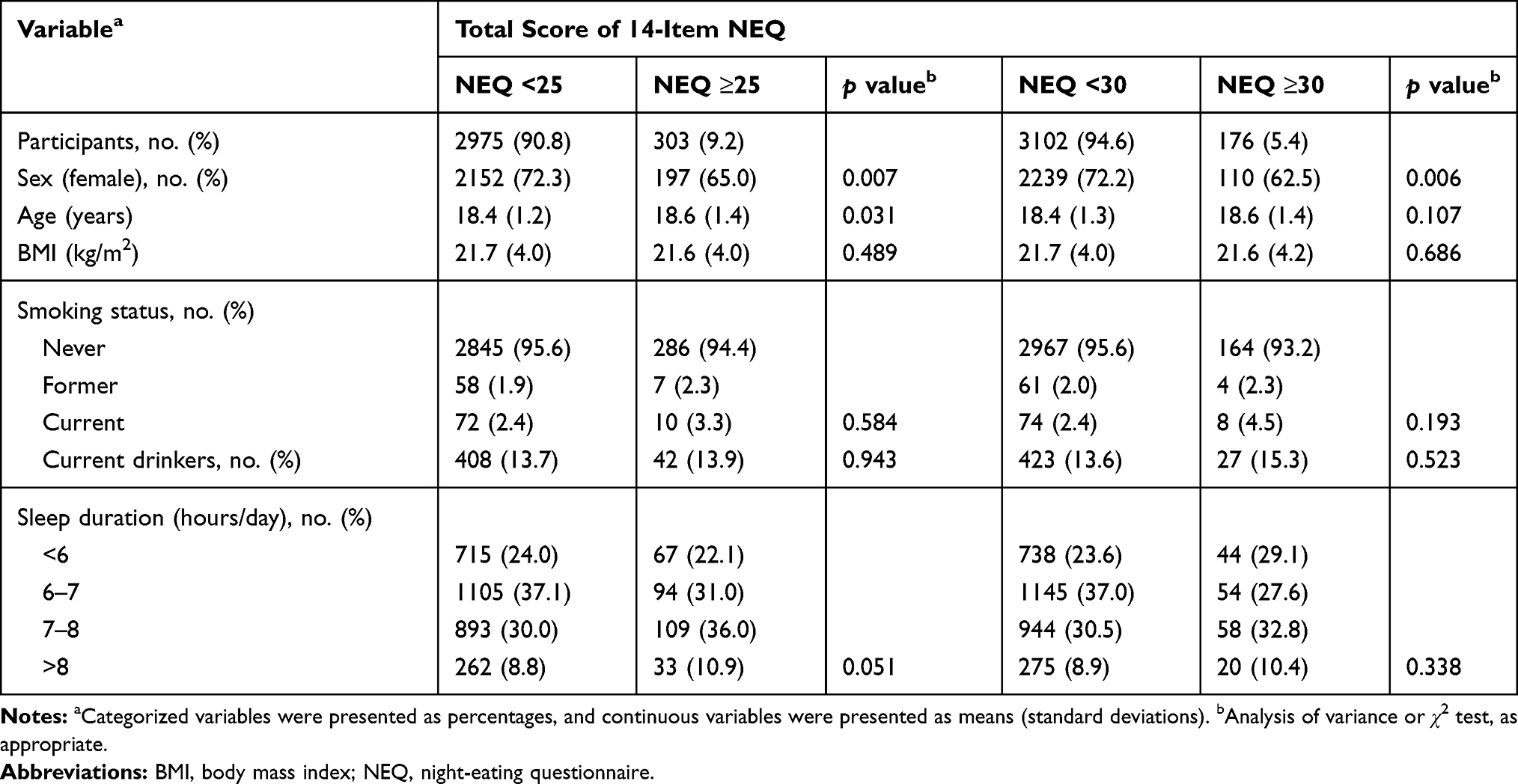 |
Table 1 Participants’ Characteristics According to Night-Eating Syndrome in College Freshmen (n=3278) |
Association Between Night-Eating Syndrome and Depressive Symptoms
Logistic regression analysis showed that the students with the syndrome had a higher prevalence of depressive symptoms (Figure 1), with ORs (95% CI) of 2.52 (1.96, 3.23) for NEQ ≥25 points (p < 0.001) and 3.19 (2.34, 4.35) for NEQ ≥30 points (p < 0.001). Table 2 shows the results of multivariate logistic regression analysis. The results of the three statistical models were consistent with the non-adjusted analysis, and night-eating syndrome (NEQ ≥30) was positively associated with depressive symptoms (p < 0.001 for all models). In the fully controlled model (Model 3), students with night-eating syndrome had a 3.28-fold higher probability of having depressive symptoms than those without the syndrome.
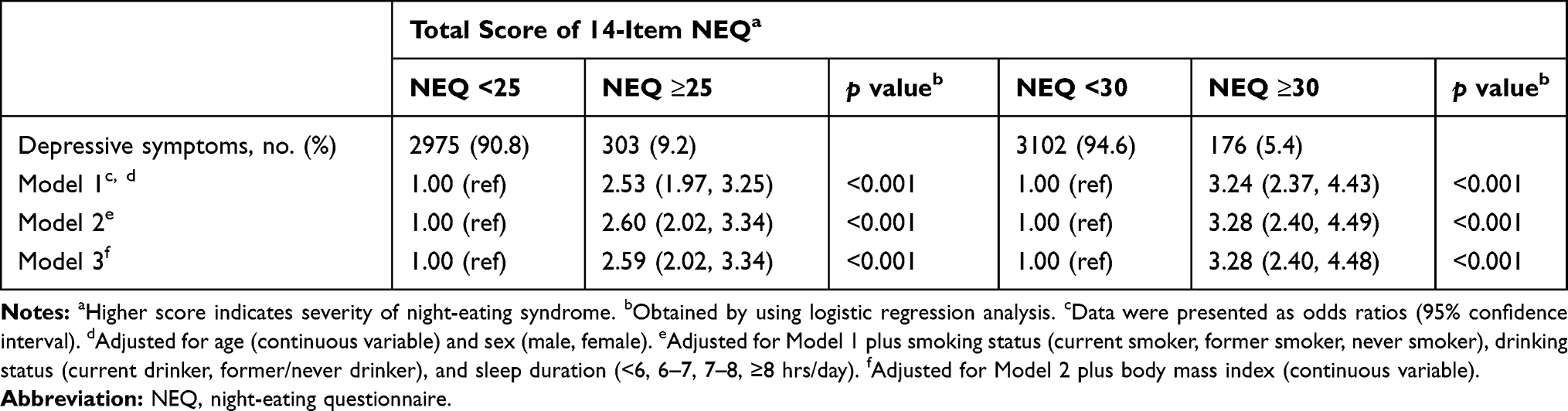 |
Table 2 Logistic Regression Analysis of Association Between Night-Eating Syndrome and Depressive Symptoms in College Freshmen (n=3278) |
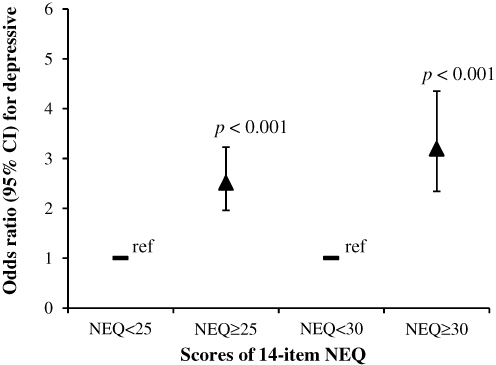 |
Figure 1 Association of night-eating syndrome with depressive symptoms using logistic regression analysis. Data are presented as odds ratios and 95% confidence intervals (CI). Definition of night-eating syndrome was considered as night-eating questionnaire (NEQ) scores ≥25 or ≥30 points. |
Analysis of covariance showed that quartiles of NEQ linearly or quadratically correlated with SDS scores in the non-adjusted model (mean [95% CI]: Q1, 44.4 [43.7, 45.0]; Q2, 43.2 [42.5, 43.9]; Q3, 44.4 [43.7, 45.1]; Q4, 47.6 [46.9, 48.3], p < 0.001) (Table 3). Bonferroni's test indicated that SDS score in the highest quartile of NEQ was significantly higher than in the other three groups. These associations were confirmed after adjusting for several potential confounding factors (p < 0.001 for all models).
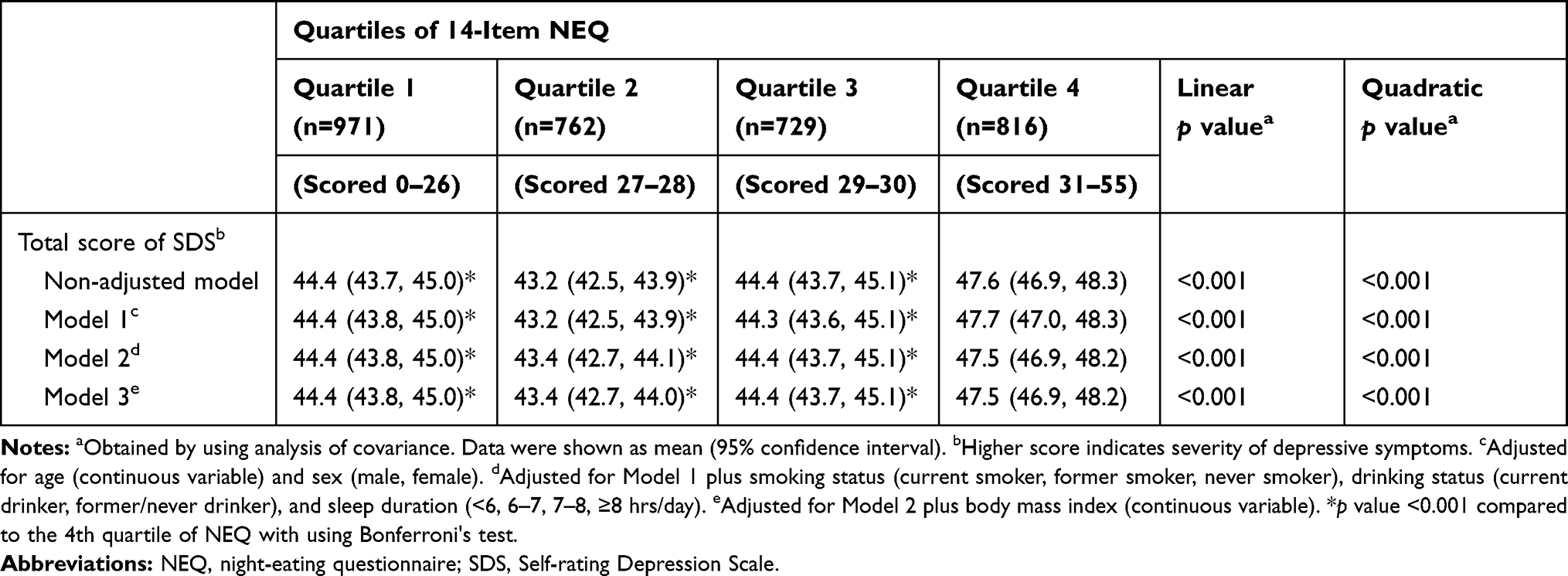 |
Table 3 Analysis of Covariance of Association Between Quartiles of Night-Eating Questionnaire and Depressive Symptoms Score in College Freshmen (n=3278) |
Discussion
In this large-scale cross-sectional study, we examined the association between night-eating syndrome and depressive symptoms among Chinese college freshmen. The results showed that the prevalence of night-eating syndrome and depressive symptoms were 5.4% and 21.3%, respectively. The students with night-eating syndrome tended to have higher depressive symptoms than those without the syndrome. Moreover, a linear and quadratic association between NEQ quartiles and SDS scores was also observed. As the night-eating behaviors could be modifiable, it is considered to be potentially valuable targets for the prevention of depressive disorders.
The present study found a positive association between night-eating syndrome and depressive symptoms, which is consistent with several previous studies. Geliebter et al reported that the people with night-eating syndrome were more likely to have a depressed mood than those without the syndrome, by using univariate analysis.7 A cross-sectional study including 404 Korean nurses indicated that those with night-eating syndrome were 1.65 times more likely to have a greater severity of depressive symptoms than those without the syndrome.17 Another observational study investigated the prevalence of night-eating syndrome among patients with major depression and clinical differences between patients with and without night-eating syndrome. Results showed that the syndrome was significantly associated with the severity of depression.18 In a sample of 1514 young adults aged 18–26 years in Switzerland, compared to healthy controls, individuals with night-eating syndrome reported more pronounced eating disorder pathology as well as depressive symptoms.19 Our previous prospective finding showed an interactive impact of snacking after dinner and dining shortly before bedtime on depressive symptoms among 376 Japanese middle-aged employees during a two-year follow-up period.9 A short-term behavioral intervention using education, relaxation strategies, and exercise is efficacious in relieving the symptoms of night-eating syndrome and depression. Reductions in night-eating syndrome scores were significantly associated with reductions in measures of depression in the interventional group.20 The present study confirmed the covariates-adjusted association of night-eating syndrome with depressive symptoms in a population of Chinese college students using a large-scale sample.
The prevalence of depressive symptoms in this study accounted for 21.3% of the total study sample, which is similar to that among other college students from China. The reported prevalence of depression among the 39 individual study populations ranged from 3.0% to 80.6%, with a pooled prevalence of 23.8%.5 On the other hand, the prevalence of night-eating syndrome (5.4%) was higher than other college students from China (0.4%)21 and USA (4.2%).22 The prevalence of night-eating syndrome was as high as 9.2% when NEQ ≥25 points was used to define the syndrome. This reflects the urgent need for improvement in the eating behaviors of college students in northeast China.
There are two possible mechanisms underlying the association between night-eating syndrome and depressive symptoms. First, decreases in serotonin in night-eaters may play a role in the progress of depressive symptoms. Night-eaters had significantly greater serotonin transporter uptake ratios in the midbrain than healthy controls did.23 These findings reflect a syndrome-specific increase in serotonin transporter that results in an overall decrease in serotonin within the synapse, which may be involved in the pathophysiology of night-eating syndrome. It is well-known that lower circulating serotonin levels were associated with a higher prevalence of depressive symptoms.24 Second, night-eating syndrome was accompanied by disordered biological rhythm. A previous study by Haraguchi et al suggested that the night-eating syndrome feeding pattern causes a shift of phases of peripheral clocks, which may result in the development of time-specific depression.25
Some study limitations were summarized as follows. First, causal inference from cross-sectional studies is limited. We cannot confirm the causal relationship between night-eating syndrome and depressive symptoms. Second, research data were collected from a single university, which may result in selection bias. The findings could not be generalized to other regions and age groups. Third, covariates included in the present study were limited. Food intakes, nutrition status, physical exercise, as well as genetic factors should be considered as potential confounding factors.
Conclusions
In conclusion, our study confirms that night-eating syndrome is significantly associated with depressive symptoms among Chinese college students. The findings of the present study suggest that healthy eating habits should be promoted to avoid psychiatric disorders among the population of college students. Future research should focus on the causal relationship between night-eating syndrome and depressive symptoms using interventional trials.
Abbreviations
BMI, body mass index; CI, confidence interval; NEQ, night-eating questionnaire; ORs, odds ratios; SD, standard deviations; SDS, Self-rating Depression Scale.
Ethics Approval and Consent to Participate
All procedures performed in this study were in accordance with the ethical standards of the institutional research committee and the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study protocol was approved by the Ethics Committee of the College of Education, Zhejiang University. Informed consent was obtained from individual participants included in the study.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
The authors are extremely grateful to all the participants of this study. The authors would also like to express their sincere gratitude to the staff of College of Sports Science, Shenyang Normal University.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
The present study was partially supported by the “Hundred Talents Program” funding from Zhejiang University (188020*194221802/004/001).
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. 2017. Depression and Other Common Mental Disorders: Global Health Estimates; World Health Organization. No. WHO/MSD/MER/2017.2.
2. White J, Zaninotto P, Walters K, et al. Duration of depressive symptoms and mortality risk: the English Longitudinal Study of Ageing (ELSA). Brit J Psychiat. 2016;208(4):337–342. doi:10.1192/bjp.bp.114.155333
3. White J, Zaninotto P, Walters K, et al. Severity of depressive symptoms as a predictor of mortality: the english longitudinal study of ageing. Psychol Med. 2015;45(13):2771–2779. doi:10.1017/S0033291715000732
4. Nolen-Hoeksema S, Aldao A. Gender and age differences in emotion regulation strategies and their relationship to depressive symptoms. Pers Indiv Differ. 2011;51(6):704–708. doi:10.1016/j.paid.2011.06.012
5. Lei XY, Xiao LM, Liu YN, Li YM. Prevalence of depression among chinese university students: a meta-analysis. PLoS One. 2016;11(4). doi:10.1371/journal.pone.0153454
6. Stunkard AJ, Grace WJ, Wolff HG. The night-eating syndrome - a pattern of food intake among certain obese patients. Am J Med. 1955;19(1):78–86. doi:10.1016/0002-9343(55)90276-X
7. Geliebter A, McOuatt H, Tetreault CB, et al. Is night eating syndrome associated with obstructive sleep apnea, BMI, and depressed mood in patients from a sleep laboratory study? Eat Behav. 2016;23:115–119. doi:10.1016/j.eatbeh.2016.08.008
8. Riccobono G, Pompili A, Iannitelli A, Pacitti F. The relationship between night eating syndrome, depression and chronotype in a non-clinical adolescent population. Riv Psichiatr. 2019;54(3):115–119. doi:10.1708/3181.31600
9. Huang C, Momma H, Cui YF, et al. Independent and combined relationship of habitual unhealthy eating behaviors with depressive symptoms: a prospective study. J Epidemiol. 2017;27(1):42–47. doi:10.1016/j.je.2016.08.005
10. Zhang Z, Tian Y, Zhong F, et al. Association between oral health-related quality of life and depressive symptoms in Chinese college students: Fitness Improvement Tactics in Youths (FITYou) project. Health Qual Life Out. 2019;17(1):96.
11. World Medical Association. Declaration of helsinki ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
12. Zung WW, Richards CB, Short MJ. Self-rating depression scale in an outpatient clinic. Further validation of the SDS. Arch Gen Psychiatry. 1965;13(6):508–515. doi:10.1001/archpsyc.1965.01730060026004
13. de Jonghe JF, Baneke JJ. The Zung self-rating depression scale: a replication study on reliability, validity and prediction. Psychol Rep. 1989;64(3):833–834. doi:10.2466/pr0.1989.64.3.833
14. Campo-Arias A, Diaz-Martinez LA, Rueda-Jaimes GE, Cadena LD, Hernandez NL. Validation of Zung’s self-rating depression scale among the Colombian general population. Soc Behav Personal. 2006;34(1):87–94. doi:10.2224/sbp.2006.34.1.87
15. Su L. Chinese version of the Zung self-rating depression scale (in Chinese). Chin J Ment Health Psychol. 1993;Suppl 160–161.
16. Allison KC, Lundgren JD, O’Reardon JP, et al. The Night Eating Questionnaire (NEQ): psychometric properties of a measure of severity of the night eating syndrome. Eat Behav. 2008;9(1):62–72. doi:10.1016/j.eatbeh.2007.03.007
17. Kim OS, Kim MS, Lee JE, Jung H. Night-eating syndrome and the severity of self-reported depressive symptoms from the Korea Nurses’ Health Study: analysis of propensity score matching and ordinal regression. Public Health. 2016;141:80–87. doi:10.1016/j.puhe.2016.08.018
18. Kucukgoncu S, Tek C, Bestepe E, Musket C, Guloksuz S. Clinical features of night eating syndrome among depressed patients. Eur Eat Disord Rev. 2014;22(2):102–108. doi:10.1002/erv.2280
19. Fischer S, Meyer AH, Hermann E, Tuch A, Munsch S. Night eating syndrome in young adults: delineation from other eating disorders and clinical significance. Psychiat Res. 2012;200(2–3):494–501. doi:10.1016/j.psychres.2012.07.028
20. Vander Wal JS, Maraldo TM, Vercellone AC, Gagne DA. Education, progressive muscle relaxation therapy, and exercise for the treatment of night eating syndrome. A pilot study. Appetite. 2015;89:136–144. doi:10.1016/j.appet.2015.01.024
21. He JB, Huang F, Yan JJ, Wu W, Cai ZH, Fan XT. Prevalence, demographic correlates, and association with psychological distress of night eating syndrome among Chinese college students. Psychol Health Med. 2018;23(5):578–584. doi:10.1080/13548506.2017.1400669
22. Runfola CD, Allison KC, Hardy KK, Lock J, Peebles R. Prevalence and clinical significance of night eating syndrome in University Students. J Adolesc Health. 2014;55(1):41–48. doi:10.1016/j.jadohealth.2013.11.012
23. Lundgren JD, Newberg AB, Allison KC, Wintering NA, Ploessl K, Stunkard AJ. I-121-ADAM SPECT imaging of serotonin transporter binding in patients with night eating syndrome: a preliminary report. Psychiatry Res. 2008;162(3):214–220. doi:10.1016/j.pscychresns.2007.07.006
24. Payne JK, Piper BF, Rabinowitz I, Zimmerman MB. Biomarkers, fatigue, sleep, and depressive symptoms in women with breast cancer: a pilot study. Oncol Nurs Forum. 2006;33(4):775–783. doi:10.1188/06.ONF.775-783
25. Haraguchi A, Fukuzawa M, Iwami S, et al. Night eating model shows time-specific depression-like behavior in the forced swimming test. Sci Rep. 2018;8(1):1–4.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.