Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
New Progress in Therapeutic Modalities of Striae Distensae
Authors Huang Q, Xu LL, Wu T, Mu YZ
Received 24 June 2022
Accepted for publication 22 September 2022
Published 30 September 2022 Volume 2022:15 Pages 2101—2115
DOI https://doi.org/10.2147/CCID.S379904
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Qing Huang, Liu-li Xu, Ting Wu, Yun-Zhu Mu
Department of Dermatology, Affiliated Hospital of North Sichuan Medical College, Nanchong, People’s Republic of China
Correspondence: Yun-Zhu Mu, Department of Dermatology, Affiliated Hospital of North Sichuan Medical College, No. 1 Maoyuan South Road, Shunqing District, Nanchong, Sichuan, 637000, People’s Republic of China, Tel +8615984833231, Email [email protected]
Abstract: Striae distensae (stretch marks/striae gravidarum) is one of the common cosmetic problems that can cause psychological distress and anxiety to patients due to its disfiguring damage, especially for women. The etiology of striae distensae is currently unknown, and risk factors include low maternal age, family history of stretch marks, excessive weight gain during pregnancy, and high neonatal weight. This article reviews the latest literature on the most commonly used, most popular, and novel treatment modalities and analyzes the hot spots and difficulties in striae distensae treatment in recent years. Topical treatment modalities are mainly used as an adjunctive treatment. Ablative lasers and non-ablative lasers are the most popular, among which picosecond has been tried in striae distensae treatment in the last two years. Combined treatment modalities are currently a hot spot for SD treatment, and microneedle radiofrequency and fractional CO2 laser combined with other treatments are the most common. Microneedle radiofrequency is the most commonly used and achieved therapeutic effect among the combined treatment modalities.
Keywords: striae distensae, stretch marks, striae gravidarum, treatment
Introduction
Striae distensae (SD) (stretch marks/striae gravidarum) is a typical dermal lesion that can occur during pregnancy, adolescence, and obesity as well as disease (eg Cushing’s syndrome/chronic steroid use). In the available literature, the prevalence of SD has been described as varying from 11% to 88%, with the vast majority of SD patients being pregnant women and adolescents and pregnancy-related SD, also known as SG (striae gravidarum). Research on the treatment of SD has been a hot topic due to its high prevalence and the psychosocial disorders it causes, which seriously affects patients’ quality of life. SD is divided into striae rubrae (SR) and striae albae (SA). SR appears as red/purple, flat, or sometimes slightly convex striae in the early stage and become white striae called SA in the late stage due to melanin reduction and atrophy. SD is often located in the abdomen, breasts, buttocks, and thighs.1–3 Studies have shown that maternal underage or weight gain during pregnancy is associated with SG formation. In contrast, fetal birth weight, gestational age at delivery, and family history of SG are associated with moderate and severe SG.4
The pathogenesis of SD is unclear, but the prevailing view is that it is related to changes in the extracellular matrix (ECM) components, including fibrillin, elastin, and collagens. These structures provide skin resistance to tension and elasticity. Compared to normal skin, patients with SD had increased glycosaminoglycan content and a significant decrease in vertical fibrillin fibres under the dermal-epidermal junction (DEJ) and elastic fiber dermis. The orientation of elastin and fibrillin fibres in the deep dermis was realigned.5 In the early stages of SD, the elastic fiber network is markedly disrupted, and the newly synthesized tropoelastin-rich fibrils are thin and disorganized and do not work like standard elastic fibers to produce the skin laxity of SD.6 Together with the significant separation of collagen bundles during this period, the newly disorganized collagen fibrils cannot repair the collagen bundles due to intense skin stretching, which together leads to atrophy of SD.7
There are various treatment modalities for SD, but there is still no “gold standard” for SD treatment. Single treatment modalities for SD include topical treatment, lasers, light devices, and others, with lasers and light devices being more effective and widely used than topical treatment. In recent years, more combination therapies have been proposed and tried. In general, they are more clinically effective than single therapies, but it depends on the type of therapies combined.2 Among the treatment modalities that have been explored so far, the therapeutic targets broadly include increasing collagen production, reducing vascularity, increasing pigmentation, and others.3
Topical Treatment
Tretinoin
Tretinoin is a recognized treatment for repairing skin damage associated with photoaged skin and histologic changes have been shown to be associated with reversal of photodamage, such as increased collagen production, fibroblast activity and angiogenesis. Therefore, some researchers tried to use tretinoin to treat skin damage caused by excessive stretching.8 A 0.1% retinoic acid has a good clinical outcome for pregnancy-related SD, and most of the current literature confirms its use in the treatment of SR.2,3 In a multicenter prospective study, 20 patients treated with 1% retinoic acid for 12 weeks showed a 20% reduction in SG length compared to the control group. Erythema, scarring, pruritus, and burning sensation were expected adverse effects, most of which appeared early in the treatment period and gradually resolved with emollients.9 Meanwhile, in the Hexsel et10 study, the clinical effectiveness of 0.05% retinoic acid compared to superficial dermabrasion for SR was evaluated. The width and length of the treated SD were measured, which were the main outcomes. A 5-point scale was used to evaluate the Global Aesthetic Improvement Scale (GAIS: worse, no change, improved, much improved, very much improved) and patient satisfaction (very unsatisfied, unsatisfied, neither satisfied nor unsatisfied, satisfied, very satisfied) in the treatment area. The width and length of SD were significantly decreased in both groups after treatment. All the patients were satisfied or indifferent and no one was dissatisfied. Both showed significant improvements in clinical performance, patient satisfaction, and aesthetic scores in SR. Other studies demonstrated no significant improvement in SD after seven months of 0.025% retinoic acid treatment.11 Low levels of tretinoin may be the primary cause.
Glycolic Acid (GA)
Glycolic acid is an effective peeling agent, and topical application of 25% AHAs (glycolic, lactic, and citric acid) can increase the thickness of the epidermis and papillary dermis, increase acid mucopolysaccharide, improve the quality of elastic fibers, and increase collagen density. The combination of GA and the tretinoin mentioned above is effective in reducing photodamaged skin, as is AHAs, and the combination is a safe and effective treatment for acne vulgaris. It is not hard to see GA being mainly used in combination with other treatments. For example, in a study by Ash et al8 10 SA samples of different Fitzpatrick skin types (I–IV) were selected. The objective blind method is done by visual grading method and histopathologic analysis was performed. Both treatments increased the epidermal thickness compared to untreated striae distensae. The application of 20% GA in combination with 0.05% retinoic acid or 10% L-ascorbic acid was safe and effective in improving the clinical performance of SA. The side effects were less than mild irritation. Glycolic acid can co-regulate collagen synthesis through cytokines released by fibroblasts and keratin-forming cells. In a double-blind controlled study, the treatment of 40 SD patients with 70% GA for six months was effective in reducing the striae width and hemoglobin content of SR and significantly reducing SA striae width and increasing melanin deposition, but not wholly repairing SD.12
Lasers and Light Devices
Ablative Lasers
Fractional CO2 Laser (FrCO2)
The Fractional Ablative CO2 laser is the most commonly used laser treatment for SD and has satisfactory efficacy in promoting the regeneration and remodeling of collagen and elastin fibers.2 In the study by Crocco et al,13 13 SG patients were treated with a 10,600-nm Fractional CO2 laser, and each patient experienced four sessions of increasing pulse energy levels (80, 90, 100 and 110 m J/MTZ), respectively. Maximum striae widths and skin tissue biopsies were measured before and after treatment. Biopsies of untreated normal skin were also obtained, and superficial and deep skin tissue samples for analysis of collagen fibers and recent, intermediate, and mature elastic fiber changes. The width of the largest striae was significantly reduced after treatment, with significant thickening of the epidermal cell layer and a significant increase in collagen fibers, which were not significantly different from normal untreated skin. However, no significant increase in the number of elastic fibers was seen in all periods, which the researchers speculate may be related to the additional thermal stability of elastic and collagen fibers. It was reported that clear boundary lines and parallel collagen fibers appeared in the distorted dermo-epidermal junction area as potential markers of SD improvement when the treated skin was observed by reflectance confocal microscopy. Of concern is that the higher the laser energy, the greater the risk of post-inflammatory hyperpigmentation, and in some patients, PIH can last up to a year.14 Studies have also shown comparable efficacy of FrCO2 laser and micro-needling for SR.15
Fractional Er:YAG Laser
Fractional Er:YAG laser has similar treatment effects to the Fractional Ablative CO2 laser described above, but the 2940 nm Er:YAG causes less thermal damage to the surrounding tissues and thus allows for faster wound healing causing milder side effects such as erythema, edema, and PIH. PIH is more difficult to accept for Fitzpatrick skin type IV–V people so it can be used as favorable alternative treatment for darker skin people.16 It was reported that the researchers applied short pulse (SP) mode plus smooth (SM) mode to treat one side of SD and the other side with two short pulses (SP) modes for two months. All SD volumes were significantly reduced, and all patients showed more than 25% improvement. There was no significant difference between the two modalities regarding treatment effect. However, at the 6-month follow-up, the incidence of PIH in the SM&SP model was only 12.5% compared with 23.5% in SP&SP. Researchers believe this is related to the SM mode slowly penetrating heat from the skin surface into the deeper tissues, resulting in minor thermal damage. Therefore, to prevent and reduce PIH in dark-skinned people, it is necessary to apply SM mode and topical preparations of the affected area pre- and post-treatment.17 Interestingly, two years later, Meningaud et al18 explored an alternative treatment modality to reduce PIH and shorten recovery time. Applying a 2940 nm Er:YAG laser with an SMA module to split the laser beam into several micro spots scanning patterns, which only penetrate the epidermis by 50 mm, while also inducing acoustic waves generation to promote tissue regeneration. A 85% of patients reported great improvement, with significant improvements in skin thickness, elasticity, and quality in the affected areas by instrumental analysis. Only 15% reported average or slight improvement. These patients had late-stage and mature SD, which the researchers believe could be improved by increasing the number of treatment sessions or decreasing the interval between each treatment, but this would also require a larger RCT trial to demonstrate. The study suggests that the 2940 nm Er:YAG laser requires at least six treatments to be effective and that no side effects occurred in the 20 patients with long-term follow-up while recovery time was only five days. In addition, another study evaluated the efficacy of laser treatment of SA with a 2940 nm Er:YAG laser for six sessions, supplemented with bovine basic fibroblast growth factor (rb-bFGF) for one week light-emitting diode-red light (LED-RL) every seven days between laser treatments. At 6-month follow-up, 27 of 30 patients reported more than 50% improvement. At the same time, biopsies suggested thickening of both epidermis and dermis and an increase in the density of both elastic and collagen fibers.16
Non-Ablative Lasers
Er:Glass Laser
Given that histologically SD and scar healing are very similar, the 1540-nm Er:glass laser can enable dermal remodeling to treat atrophic scarring, which has recently been attempted in studies to treat SD. The researchers applied treatment 2 to 4 times, and after a one-month follow-up biopsy comparison, the epidermis and dermis were thickened, and collagen fibers and elastic fibers were increased. After three months, image comparison revealed a 50–75% improvement in all SD. After six months and even longer follow-up, patients had more than 50% improvement by visual assessment, and none had a recurrence. In addition, the study suggests that the optimal treatment parameters for the laser are 30 to 50 m J/µb, and it is hypothesized that the stamping mode energy pattern is more suitable for SD treatment, ensuring the effectiveness and consistent distribution of microbeams into the skin. Also, this study selected 51 patients (II–IV), including SR and SA, in which 14% striae of more than 20 years and the farthest years were 40 years. Because of the experience with the treatment of the striae ranging in maturation age from 1 to 40 years, the researchers propose a different view from the previous treatment of SD. They concluded that the superiority of the treatment effect lies more in the length, width, and density of Striae compared to the maturity of SD.19 In a prospective study, the Fractional 1565-nm Er:glass with picosecond 1064 nm or 532nm Nd:YAG laser was evaluated to be equally effective in treating SA.20
Picosecond Lasers
In the study by Fusano et al21 after 27 Caucasian women with SA were treated with the 1064 nm picosecond laser over four months, clinicians observed clinical improvement in 81.4% of patients and 66.6% of patients perceived clinical improvement and satisfactory outcomes. Meanwhile, at the 6-month follow-up, the 3D analysis showed a significant improvement in the overall texture and depth of the striae. However, no significant reduction in width and collagen remodeling and dermal papillae were observed at Reflectance Confocal Microscopy (RCM), all of which indicate that 1064 nm picosecond laser treatment is an effective treatment option for SA but not a complete cure. After one year, the same conclusions were reached in another study evaluating the efficacy of 1064-nm picosecond laser treatment in 20 patients with dark-skinned (IV–V) SA. At 6-month follow-up, more than 90% of patients reported moderate to significant improvement, sustained improvement in skin texture, more evenness of striae color, and side effects of only mild erythema, edema, crusting, and PIH, with a 10% incidence of PIH.22
Pulsed Dye Laser (PDL)
PDL increases collagen fiber production and reduces the degree of erythema in SR, which significantly improves SR.23,24 Based on the high affinity of hemoglobin for 585 nm PDL during treatment, all can effectively reduce the degree of erythema of SR.23 Also, because melanin as a chromogenic group competes with hemoglobin for the light energy from the 585 nm PDL, dark-skinned people are highly susceptible to PIH, so even low-energy lasers are not recommended for use in dark-skinned (IV–V) people. The study by GLORIA et al24 demonstrated that 585 nm PDL was effective in improving SR but had no significant clinical efficacy in SA, even though an increase in collagen fibers was detected in SA after treatment. This conclusion was similarly supported in another study, confirming that IPL and PDL are equally effective for SR.
Nd:YAG Laser
In a study conducted by Elsaie et al25 comparing the efficacy of two energies (75 and 100 J/cm2) of long-pulsed Nd:YAG laser in the treatment of SD, it was confirmed that 100 J/cm2 improved the appearance of SA significantly, while 75 J/cm2 was more effective for SR, with a significant increase in collagen fibers and elastic fibers in post-treatment sample, and satisfactory changes were observed from both clinical and histological evaluation. The skin color of the 45 patients in this study sample included III–V, where the dark-skinned population did not show significant PIH.
Lights
Intense Pulsed Light (IPL)
In a prospective study evaluating the efficacy of IPL for SA at wavelengths between 515 nm and 1200 nm, all 15 patients reported satisfactory outcomes, with the average number of SD per patient decreasing from 7.8 to 6.26. The average length of SD decreased from 25 cm to 15.93 cm. There was an increase in both epidermal and dermal thickness under the microscope, confirming the effectiveness of IPL for the treatment of SA.26
Others
Radiofrequency (RF)
A prospective randomized controlled study conducted by Harmelin et al27 evaluated the effect of Fractionated Bipolar Radiofrequency versus Bipolar Radiofrequency Potentiated by Infrared Light for the treatment of SD. The abdomen was divided into four quadrants representing the four groups: the blank group, the two separate RF groups, and the combined treatment group. At the 6-month follow-up of the combined treatment group, 3D photography showed a 21.6% decrease in mean streak depth and a 1.73% increase in the control group. The distribution of collagen fibers was more uniform than in pre-treatment, and the distribution of elastic fibers was reduced. Both the physician and the patient reported significant improvement in SD but not in the width of the striae. The efficacy of combination therapy is superior to monotherapy in all aspects and is an effective treatment modality for SA and SR. Side effects were mainly associated with Fractionated Bipolar Radiofrequency, and the presence of PIH in two patients suggests caution in dark-skinned people. Interestingly, in a study by Manuskiatti et al28 it was noted that TriPollar RF is an excellent alternative treatment even for dark-skinned people. Improvement of more than 50% was perceived by 11.8% of patients after just one week of treatment, and persistent improvement was found at a follow-up kind of 6 weeks later. The clinical outcome of 1 patient with SR was better than all other SA patients, with 65% of patients reporting satisfactory treatment results. Even more satisfying for patients is that TriPollar RF side effects are only brief and mild erythema and edema while being essentially painless. From the results of the two research experiments mentioned above, the authors concluded that the treatment of SD requires developing an individualized treatment plan. Selecting treatment parameters and frequency and intervals needs to be considered thoroughly according to various aspects such as the patient’s skin color, striae depth, clinical response, and tolerance level.
Micro-Needling
Unlike laser treatments, micro-needling does not cause thermal injury to the skin, so it reduces the risk of post-inflammatory hyperpigmentation, especially for darker skin phototypes. The advantages of fewer side effects, shorter recovery time, and lower cost have made it a hot spot for SD treatment in the last two years. The principle of action is similar to that of laser in that it promotes new collagen synthesis and dermal remodeling through dermal damage. In a recent study of 25 SD patients (I–V) treated with 1–3 consecutive Micro-needling sessions, all striae improved by more than 50%, and 28% of SD patients demonstrated more than 75% improvement. There was no significant difference in efficacy between patients with different skin types and no difference between thicker and thinner skin areas.29 West et al30 applied micro-needling to treat SR. Biopsies showed many regular collagen fiber bundles and dermal fibroblast proliferation but an insignificant increase in elastic fibers. Except for one case of Fitzpatrick type VI skin with PIH that resolved with topical treatment such as retinoic acid, no distant PIH appeared. In another study, micro-needling was shown to be as effective as 1340 nm Nd: YAP non-ablative fractional laser in the treatment of SA, and it was also observed that pain was more pronounced in the micro-needling group, so it was suggested that when the penetration depth was greater than 3 mm, local anesthetics were needed to pre-treatment.31 Studies have also shown that a combination of micro-needling with PRP is more effective than micro-needling alone.32
Platelet-Rich Plasma (PRP)
PRP is a concentrated platelet centrifuged and sunk into a small amount of plasma. PRP induces extracellular matrix remodeling, collagen fiber, and elastic fiber formation.
Studies have shown that local PRP injections are more effective than 0.05% retinoic acid for SA, especially striae alba. Of the 30 SD patients, 86.6% of the PRP group reported improvement, and patient satisfaction was 89.9%, compared with 60% in the retinoic acid group in both areas. At the same time, PRP also had the advantages of easy access and no risk of hyperpigmentation or infection.33 It has also been shown that PRP and carboxytherapy are essentially equivalent in the treatment of SA.34 This year, Ebrahim et al35 researchers tried the superiority of PRP combined with subcision or peeling/medium-depth peeling (GA 70% + TCA 35%) compared to PRP alone. After clinical improvement, patients’ satisfaction and Dermatology Life Quality Index (DLQI), and skin biopsy assessments, it was confirmed that both combined treatments were superior to PRP alone. At the same time, subcutaneous separation was superior in the treatment of SA and safer in dark-skinned populations.
Microdermabrasion (MDA)
Microdermabrasion removes aged skin cells through mechanical damage and stimulates new cell production, collagen fiber, and elastic fiber synthesis. In an RCT involving 48 SA, it was demonstrated that both Galvano-puncture and MDA effectively reduced the length and width of SA, with thermography showing more significant improvement with Galvano-puncture and no statistically significant difference in pain.36 In another single-center clinical trial, Hexsel et al10 evaluated the efficacy of Superficial Dermabrasion versus 0.05% retinoic acid for the treatment of 32 SR. Confirmed by comparing the width and length of the striae, Global Aesthetic Improvement Scale scores, patient satisfaction, and histological analysis, both treatments were significantly effective and did not differ. In addition, histological analysis showed a reduction in elastolysis, collagen fragmentation, epidermal atrophy, and an improvement in dermis and epidermis, confirming the clinical presentation. Both exhibited pruritus, erythema, and scaling. However, the incidence was higher in the retinoic acid group, which led to better patient compliance and safety in superficial dermabrasion, which the researchers concluded could be used for early and localized SR.
Carboxytherapy
Carboxytherapy, meaning cutaneous and subcutaneous injection of carbon dioxide gas, has been popular in dermal rejuvenation treatments since 1995. Water molecules react with carbon dioxide to produce molecular carbonic acid, which reduce the pH of tissue. According to the Bohr effect, this causes hemoglobin to release oxygen and microcirculatory vasodilation, while increasing peripheral blood flow (Bohr effect: A decrease in pH can cause a decrease in the affinity of hemoglobin and oxygen). Tissue stretching during carbon dioxide injection induces subclinical inflammation that activates macrophages, fibroblasts and endothelial cells. This stimulates neovascularization and extracellular matrix remodeling for skin repair and tissue regeneration.37 Studies have shown carboxytherapy effectively improves the skin elasticity of SD, reducing the width and length of striae. At the same time, the color of SD becomes more like the natural skin, with hematoma being the most significant side effect.38 In recent years, Elmorsy et al37 demonstrated no significant difference in efficacy between carboxytherapy and FrCO2. Up to 80% of SD patients had significant clinical improvement with carboxytherapy. SR was more effective than SA. The mean striae length decreased from 13.1 cm to 9.3 cm after only one month of treatment, and no patient in the carboxytherapy group had more severe striae than FrCO2. The majority of the sample population in this study was Fitzpatrick skin type IV. No patients experienced PIH with carboxytherapy. Only temporary erythema and bruising at the injection site. Another study suggested that the clinical improvement of the carboxytherapy was comparable to the PRP. However, patients’ satisfaction was higher with carboxytherapy. Because PRP was more likely to have pain and ecchymosis, carboxytherapy was effective for any part of the body and both types of SD.39 Some of the clinical trials of single treatment modalities have been tabulated in Table 1.
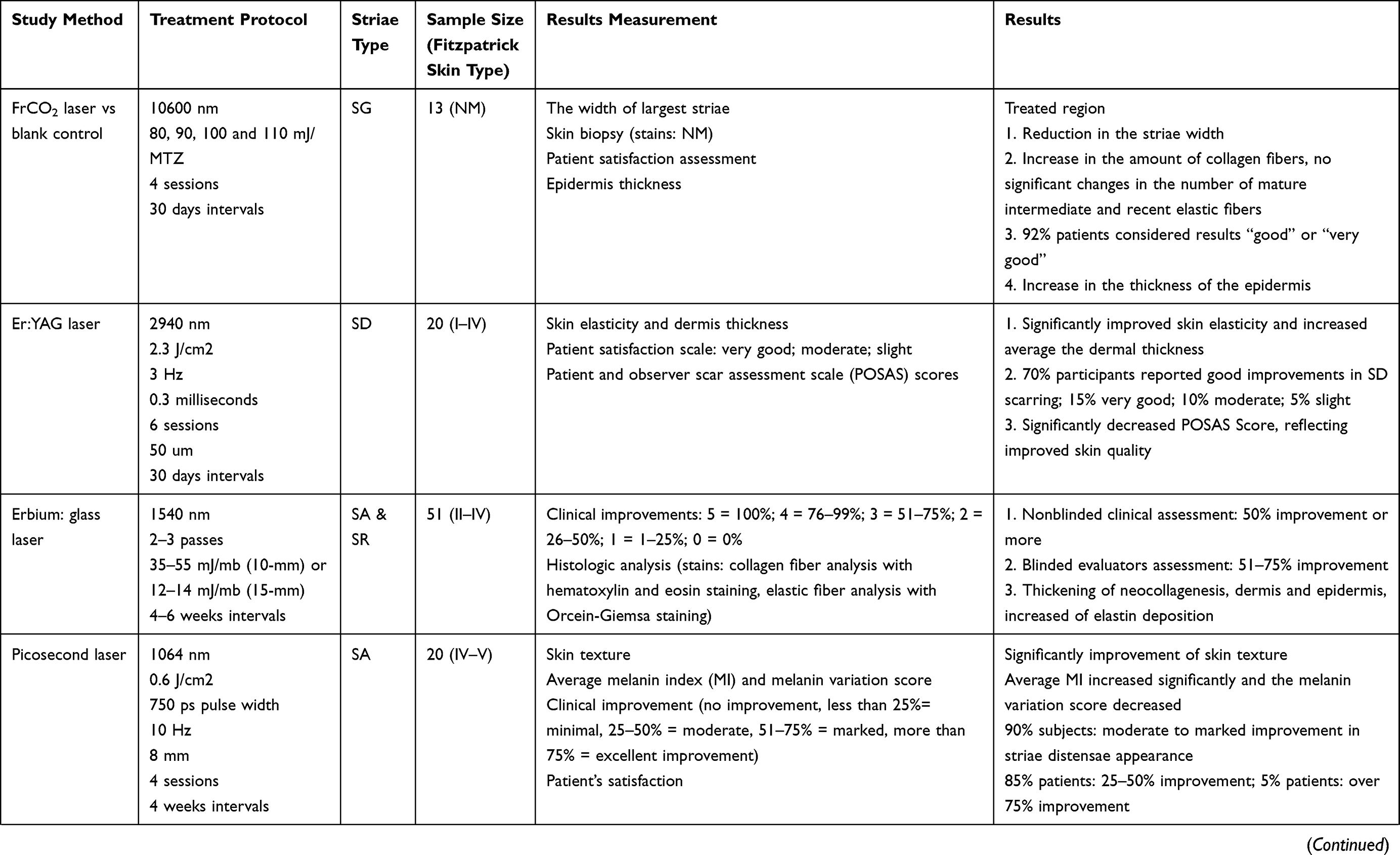 | 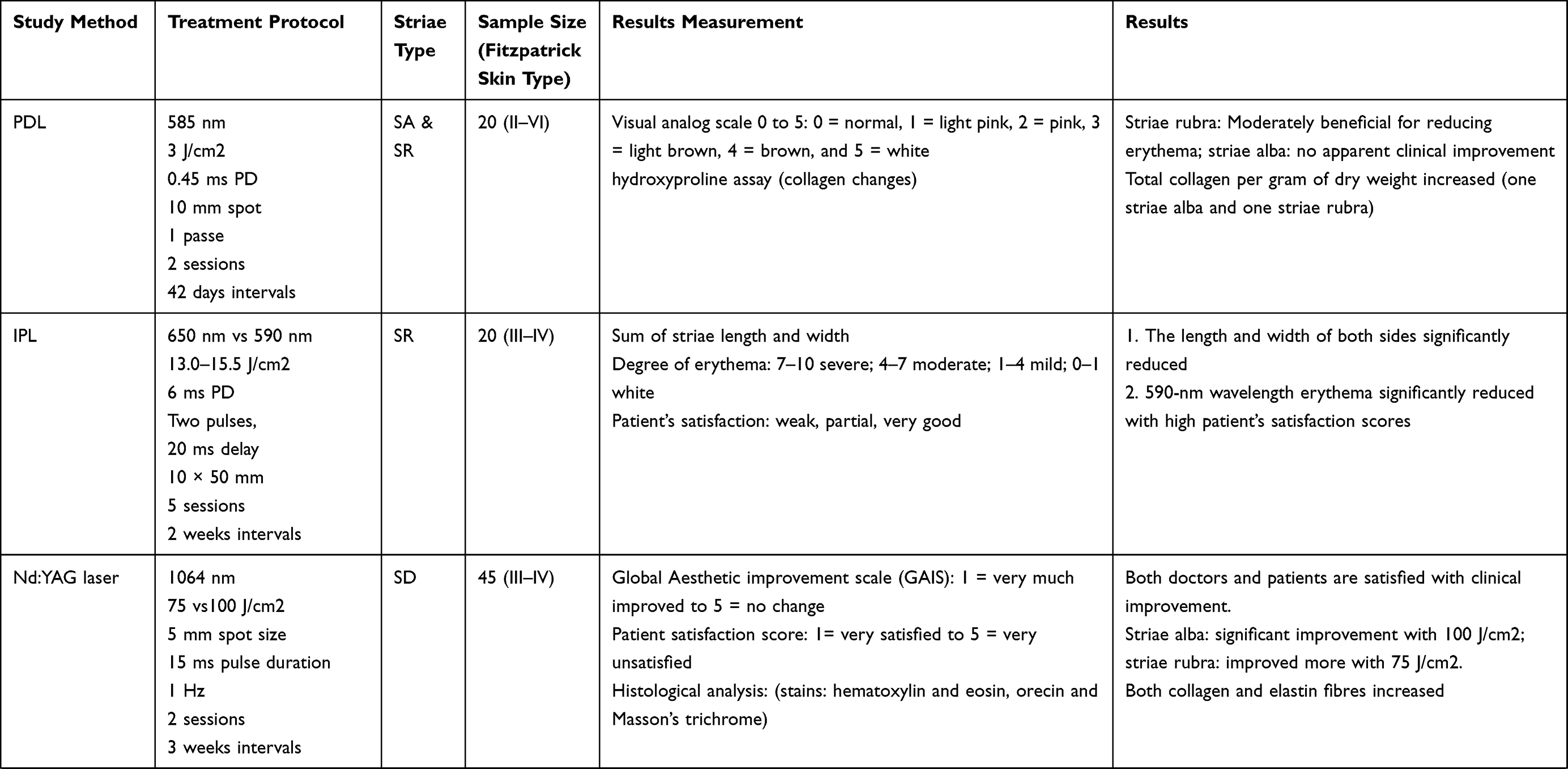 | 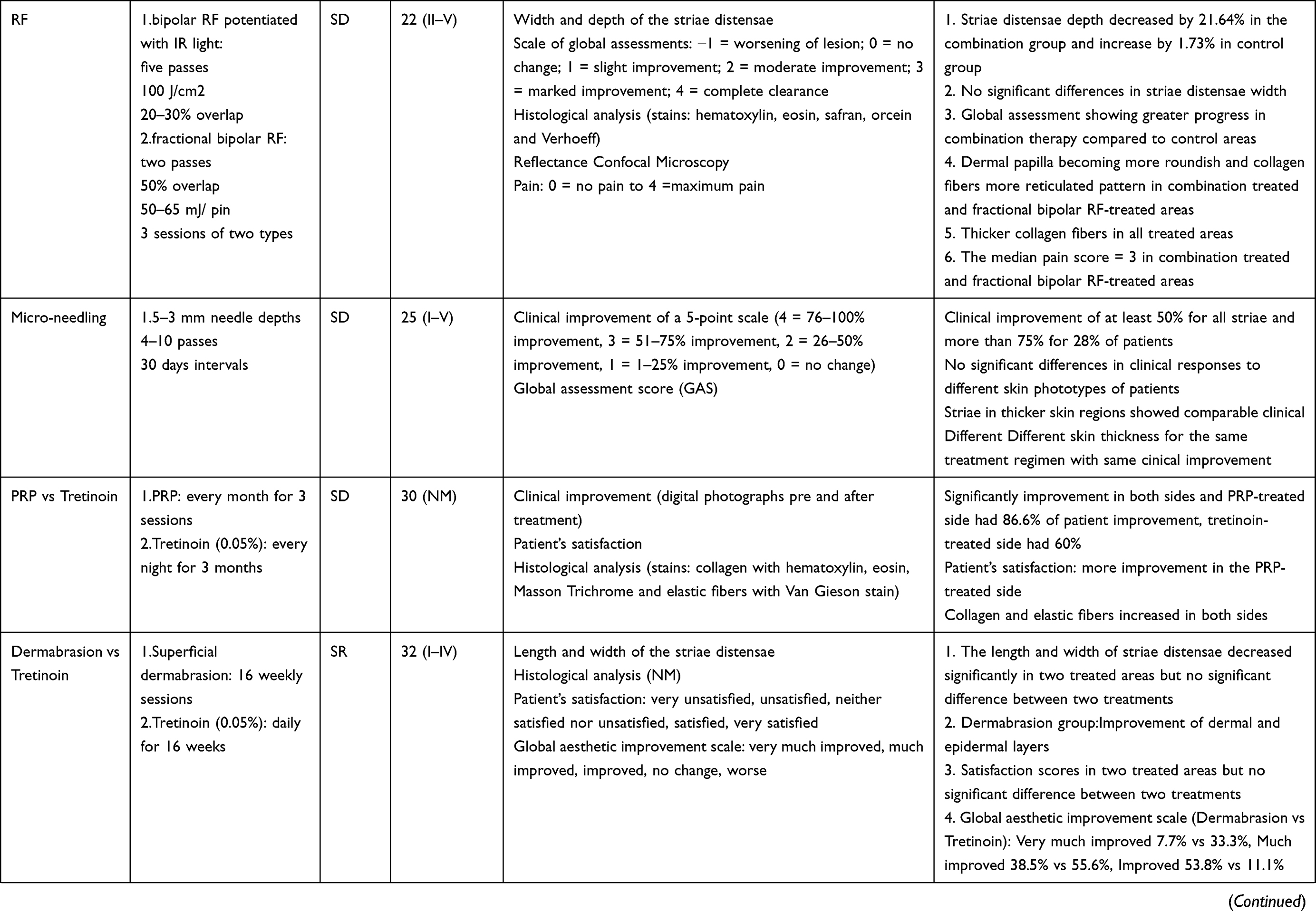 | 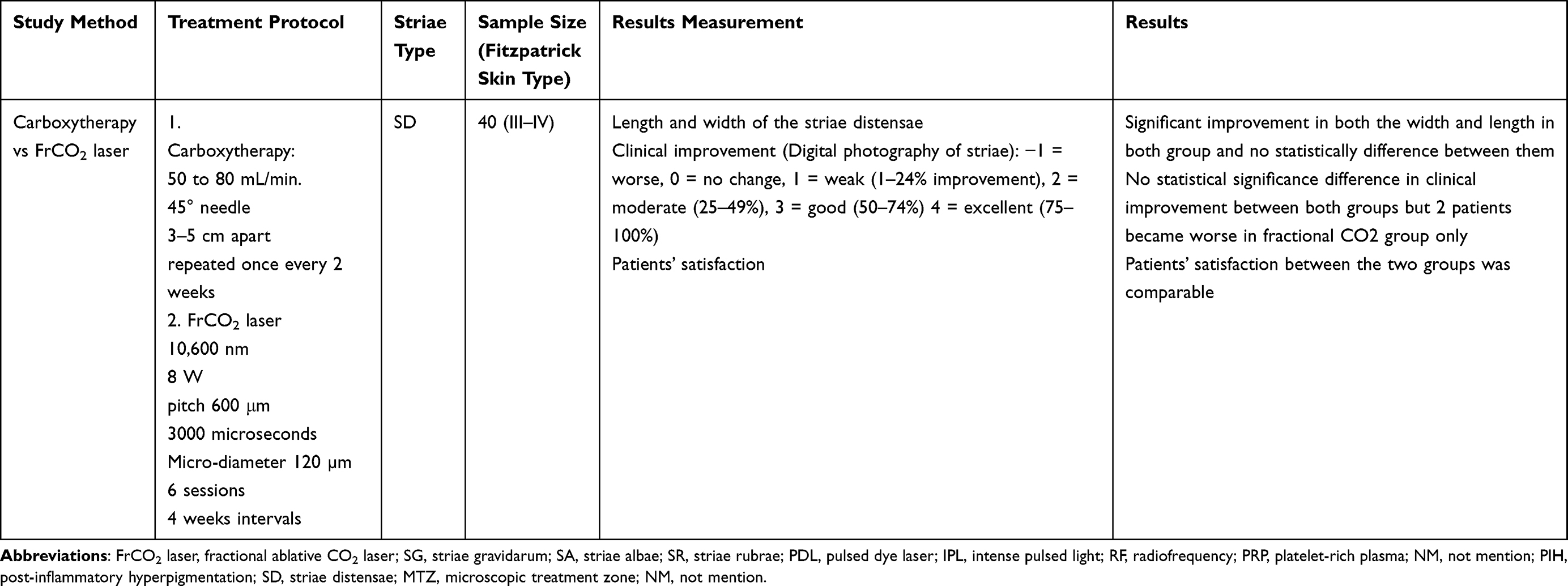 |
Table 1 Clinical Trials of Single Treatment Modalities |
Combination Therapies
RF Plus Others
Microneedling and radiofrequency (MRF) have been successfully applied to treat atrophic scarring and facial wrinkles in recent years. Many researchers have tried to use it to treat SD, given the similarity between them, the histological characteristics of SD, and atrophic scarring. In the study by Al-Muriesh et al40 non-insulated MRF with FrCO2 indicated an improvement and no statistical difference in the treatment of SD as assessed by the Global Aesthetic Improvement Scale, dermoscopy, and VISIA imager (3D images). The VISIA system uses virtual shadow overlaps to provide reproducible targeting to accurately observe changes before and after treatment at the same position, generate corresponding regular and rendered 3D images. Regular images include skin tone and grayscale photograph to measure the depth and range of skin color changes. Red and yellow color in rendered 3D images represent the elevation of the skin, in this case SD lesions. These 3D images can make up for the deficiencies visual contrast in 2-dimensional images. Both groups after treatment, rendered 3D images showed a decrease in red and yellow color, while grayscale and skin tone color showed flatten of SD. Dermoscopy revealed a 5–32% reduction in striae width in the MRF group and a 6–31% reduction in the FrCO2 group. The pain index was significantly higher in the MRF group but was tolerated by both patients, and although PIH occurred in both groups, it was more likely to occur in the FrCO2 group. The above findings are generally consistent with those of Sobhi et al.41 The only difference is the absence of PIH in the MRF group in the latter study, which the authors suggest is related to the choice of the treatment protocol and instrumentation as well as pre- and post-treatment management. In another study, they asked whether the combination of FrCO2 and MRF for SD could improve efficacy and reduce side effects, given the paradox that high-energy FrCO2 is more effective for SD and has a greater risk of causing PIH. The results showed a slightly more significant improvement with the combination treatment than the conventional FrCO2 treatment. The hyperpigmentation and erythema severity were more severe than in the MRF group. At the same time, the side effects are similar to the FrCO2 group. After a combined treatment, the skin ultrasound scanner showed an increase in average skin thickness of 204.9 μm and an increase in dermal density of 8.8%, indicating that the dermal improvement would last for a more extended time.42 In addition, it has been shown that the efficacy of MRF and Er:YAG treatment for SA is comparable. However, the dermal and epidermal thickening in the MRF group was more significant but not statistically different in the optical coherence tomography instrument.43 It is noteworthy that no PIH was reported in the MRF group in the latter two studies, in keeping with Sobhi above. MRF is more capable of stimulating SA collagen fiber regeneration than NAFL but is more painful.44
Ablative Fractional radiofrequency combined with Acoustic Pressure Ultrasound transdermal delivery of 0.05% retinoic acid cream is also an effective treatment modality for SA. Combining the two devices can increase the penetration of retinoic acid and improve the clinical efficacy with an improvement of up to 76–100% with fewer side effects and only one case of PIH.45 Sublative bipolar fractional radiofrequency combined with 0.1% retinoic acid is a promising treatment modality for SG.46
FrCO2 Plus Others
A randomized, double-blind study compared the efficacy of FrCO2 combined with recombinant human epidermal growth factor (AFXL-rhEGF) and FrCO2 combined with aloe vera gel (AFXL-Aloe) in the treatment of SA. Human epidermal growth factor and aloe vera gel are hydrophilic substances that can penetrate deeper into the skin through the MTZ produced by FrCO2 to achieve better efficacy. The results showed a significant improvement in both subjective and objective assessments, which lasted for up to 6 months. At 6-month follow-up, up to 50% of patients reported significant improvement in patient satisfaction with AFXL-rhEGF compared with only 25% with AFXL-Aloe. At the same time, both had better efficacy in the SD of the buttocks than the thighs and abdomen. With little difference in efficacy, AFXL-Aloe is significantly more economical. Notably, the 24 SA involved in this study were all dark-skinned (III–IV) and had a high incidence of PIH of 95.8%, but hyperpigmentation improved at the 6-month follow-up.47 In the last two years, it has been shown that FrCO2 combined with PRP is also an effective treatment for SD and is superior to FrCO2 alone or PDL combined with PRP.48,49 Some of the clinical trials of combined treatment modalities have been tabulated in Table 2.
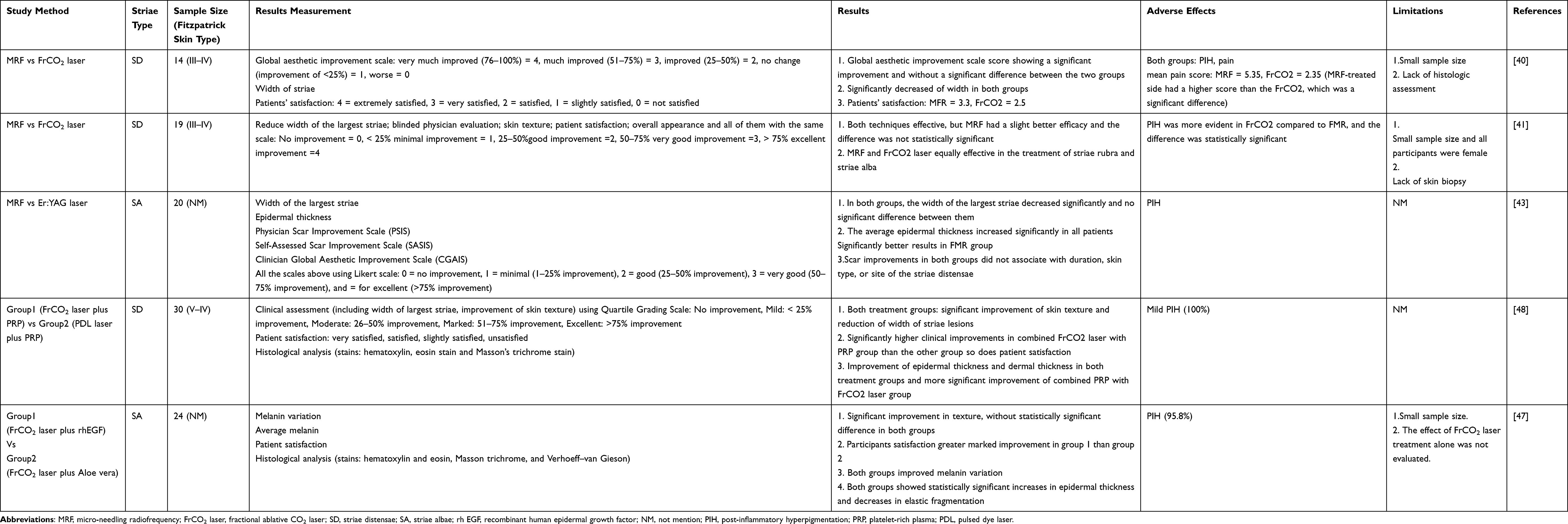 |
Table 2 Clinical Trials of Combined Treatment Modalities |
Conclusion
Different skin types have different reactions and side effects to the same treatment. Despite some positive results, the treatment of SD is still a great challenge, especially for SA (end-stage of SD). Despite the limitations of the existing literature, combined treatment is generally more effective than single treatment. Tretinoin, FrCO2 laser, Er:YAG laser, radiofrequency and microneedling were clinically responsive to proper settings or concentrations in single treatment. FrCO2 laser remains the most popular and effective treatment, but the side effects of PIH deserve our attention, especially in dark-skinned people. The combination of radiofrequency and microneedling was the most common treatment with good clinical response and fewer side effects. In the future, a universal SD grading scale and a standardized way of assessing post-treatment outcomes are expected to be established before definitive conclusions can be obtained for more accurate comparative treatment. Combining therapy is currently a hot topic in SD treatment and more combinations can be tried to improve the efficacy, reduce side effects to achieve a better treatment effect and increase patient compliance. The study’s design requires samples for different skin types, optimal parameters, and protocols for various treatment modalities, and follow-up of long-term results are directions that can be worked on in the future.
Consent for Publication
All authors have read and approved the final manuscript for submission.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ud-Din S, McGeorge D, Bayat A. Topical management of striae distensae (stretch marks): prevention and therapy of striae rubrae and albae. J Eur Acad Dermatol Venereol. 2016;30(2):211–222. doi:10.1111/jdv.13223
2. Seirafianpour F, Sodagar S, Mozafarpoor S, et al. Systematic review of single and combined treatments for different types of striae: a comparison of striae treatments. J Eur Acad Dermatol Venereol. 2021;35(11):2185–2198. doi:10.1111/jdv.17374
3. Hague A, Bayat A. Therapeutic targets in the management of striae distensae: a systematic review. J Am Acad Dermatol. 2017;77(3):559–568. doi:10.1016/j.jaad.2017.02.048
4. Osman H, Rubeiz N, Tamim H, et al. Risk factors for the development of striae gravidarum. Am J Obstet Gynecol. 2007;196(1):61–62. doi:10.1111/dsu.12460
5. Watson W, Parry P, Humphries H, et al. Fibrillin microfibrils are reduced in skin exhibiting striae distensae. Br J Dermatol. 1998;138(6):931–937. doi:10.1046/j.1365-2133.1998.02257.x
6. Wang F, Calderone K, Smith NR, et al. Marked disruption and aberrant regulation of elastic fibres in early striae gravidarum. Br J Dermatol. 2015;173(6):1420–1430. doi:10.1111/bjd.14027
7. Wang F, Calderone K, Do TT, et al. Severe disruption and disorganization of dermal collagen fibrils in early striae gravidarum. Br J Dermatol. 2018;178(3):749–760. doi:10.1111/bjd.15895
8. Ash K, Lord J, Zukowski M, et al. Comparison of topical therapy for striae alba (20% glycolic acid/0.05% tretinoin versus 20% glycolic acid/10% L-ascorbic acid). Dermatol Surg. 1998;24(8):849–856. doi:10.1111/j.1524-4725.1998.tb04262.x
9. Rangel O, Arias I, Garcia E, et al. Topical tretinoin 0.1% for pregnancy-related abdominal striae: an open-label, multicenter, prospective study. Adv Ther. 2001;18(4):181–186. doi:10.1007/BF02850112
10. Hexsel D, Soirefmann M, Porto MD, et al. Superficial dermabrasion versus topical tretinoin on early striae distensae: a randomized, pilot study. Dermatol Surg. 2014;40(5):537–544.
11. Pribanich S, Simpson FG, Held B, et al. Low-dose tretinoin does not improve striae distensae: a double-blind, placebo-controlled study. Cutis. 1994;54(2):121–124.
12. Mazzarello V, Farace F, Ena P, et al. A superficial texture analysis of 70% glycolic acid topical therapy and striae distensae. Plast Reconstr Surg. 2012;129(3):589e–590e. doi:10.1097/PRS.0b013e3182419c40
13. Crocco EI, Muzy G, Schowe NM, et al. Fractional ablative carbon-dioxide laser treatment improves histologic and clinical aspects of striae gravidarum: a prospective open label paired study. J Am Acad Dermatol. 2018;79(2):363–364. doi:10.1016/j.jaad.2017.12.041
14. Guida S, Losi A, Greco M, et al. Reflectance confocal microscopy for striae distensae treatment monitoring after CO2 fractional laser. Dermatol Ther. 2020;33(6):e14318. doi:10.1111/dth.14318
15. Saki N, Rahimi F, Pezeshkian FS, et al. Comparison of the efficacy of microneedling versus CO2 fractional laser to treat striae alba: a randomized clinical trial. Dermatol Ther. 2022;35(1):e15212. doi:10.1111/dth.15212
16. Shen J, Lu XG, Jin JJ, et al. Combination of a 2940 nm Er: yAGlaser with recombinant bovine basic fibroblast growth factor (rb-bFGF) and light-emitting diode-red light (LED-RL) for the treatment of striae alba: a pilot study. J Cosmet Dermatol. 2018;17(2):176–183. doi:10.1111/jocd.12376
17. Wanitphakdeedecha R, Meeprathom W, Manuskiatti W. A pilot study of treatment of striae distensae with variable square pulse Erbium: YAG laser resurfacing. J Cosmet Dermatol. 2017;16(4):466–470. doi:10.1111/jocd.12391
18. Meningaud JP, SidAhmed-Mezi M, Billon R, et al. Clinical benefit of using a multifractional Er: yAGlaser combined with a spatially modulated ablative (SMA) module for the treatment of striae distensae: a prospective pilot study in 20 patients. Lasers Surg Med. 2019;51(3):230–238. doi:10.1002/lsm.23042
19. de Angelis F, Kolesnikova L, Renato F, et al. Fractional nonablative 1540-nm laser treatment of striae distensae in Fitzpatrick skin types II to IV: clinical and histological results. Aesthet Surg J. 2011;31(4):411–419. doi:10.1177/1090820X11402493
20. Zaleski-Larsen LA, Jones IT, Guiha I, et al. A comparison study of the nonablative fractional 1565-nm Er: glass and the picosecond fractional 1064/532-nm Nd: YAG lasers in the treatment of striae alba: a split body double-blinded trial. Dermatol Surg. 2018;44(10):1311–1316. doi:10.1097/DSS.0000000000001555
21. Fusano M, Galimberti MG, Bencini M, et al. Picosecond laser treatment of striae distensae: in vivo evaluation of results by 3D analysis, reflectance confocal microscopy, and patient’s satisfaction. Lasers Surg Med. 2021;53(9):1180–1185. doi:10.1002/lsm.23401
22. Kaewkes A, Manuskiatti W, Cembrano KA, et al. Treatment of abdominal striae distensae in Fitzpatrick skin types IV to V using a 1064-nm picosecond laser with a fractionated microlens array. Lasers Surg Med. 2022;54(1):129–137. doi:10.1002/lsm.23471
23. Shokeir H, El BA, Sayed S, et al. Efficacy of pulsed dye laser versus intense pulsed light in the treatment of striae distensae. Dermatol Surg. 2014;40(6):632–640. doi:10.1111/dsu.0000000000000007
24. Jimenez GP, Flores F, Berman B, et al. Treatment of striae rubra and striae alba with the 585-nm pulsed-dye laser. Dermatol Surg. 2003;29(4):362–365. doi:10.1046/j.1524-4725.2003.29086.x
25. Elsaie ML, Hussein MS, Tawfik AA, et al. Comparison of the effectiveness of two fluences using long-pulsed Nd: yAGlaser in the treatment of striae distensae. Histological and morphometric evaluation. Lasers Med Sci. 2016;31(9):1845–1853. doi:10.1007/s10103-016-2060-2
26. Al-Dhalimi MA, Abo NA. A comparative study of the effectiveness of intense pulsed light wavelengths (650 nm vs 590 nm) in the treatment of striae distensae. J Cosmet Laser Ther. 2013;15(3):120–125. doi:10.3109/14764172.2012.748200
27. Harmelin Y, Boineau D, Cardot-Leccia N, et al. Fractionated bipolar radiofrequency and bipolar radiofrequency potentiated by infrared light for treating striae: a prospective randomized, comparative trial with objective evaluation. Lasers Surg Med. 2016;48(3):245–253. doi:10.1002/lsm.22458
28. Manuskiatti W, Boonthaweeyuwat E, Varothai S. Treatment of striae distensae with a TriPollar radiofrequency device: a pilot study. J Dermatolog Treat. 2009;20(6):359–364. doi:10.3109/09546630903085278
29. Alster TS, Li MK. Microneedling treatment of striae distensae in light and dark skin with long-term follow-up. Dermatol Surg. 2020;46(4):459–464. doi:10.1097/DSS.0000000000002081
30. West L, He B, Vandergriff T, et al. The use of microneedling to treat striae distensae. Dermatol Surg. 2021;47(10):1407–1408. doi:10.1097/DSS.0000000000003151
31. Naspolini AP, Boza JC, Da SV, et al. Efficacy of microneedling versus fractional non-ablative laser to treat striae alba: a randomized study. Am J Clin Dermatol. 2019;20(2):277–287. doi:10.1007/s40257-018-0415-0
32. Abdel-Motaleb AA, Zedan H, Mostafa MM, et al. Combined microneedling with topical application of platelet-rich plasma versus microneedling alone in the treatment of stria distensae: clinicopathological analysis. J Dermatolog Treat. 2022;33(2):836–847. doi:10.1080/09546634.2020.1782323
33. Hodeib AA, Hassan G, Ragab M, et al. Clinical and immunohistochemical comparative study of the efficacy of carboxytherapy vs platelet-rich plasma in treatment of stretch marks. J Cosmet Dermatol. 2018;17(6):1008–1015. doi:10.1111/jocd.12481
34. Gamil HD, Ibrahim SA, Ebrahim HM, et al. Platelet-rich plasma versus tretinoin in treatment of striae distensae: a comparative study. Dermatol Surg. 2018;44(5):697–704. doi:10.1097/DSS.0000000000001408
35. Ebrahim HM, Salem A, Salah T, et al. Subcision, chemical peels, and platelet-rich plasma: combination approaches for the treatment of striae distensae. Dermatol Ther. 2022;35(2):e15245. doi:10.1111/dth.15245
36. Ferreira A, Guida A, Piccini AA, et al. Galvano-puncture and dermabrasion for striae distensae: a randomized controlled trial. J Cosmet Laser Ther. 2019;21(1):39–43. doi:10.1080/14764172.2018.1444777
37. Elmorsy EH, Elgarem YF, Sallam ES, et al. Fractional carbon dioxide laser versus carboxytherapy in treatment of striae distensae. Lasers Surg Med. 2021;53(9):1173–1179. doi:10.1002/lsm.23418
38. Podgorna K, Kolodziejczak A, Rotsztejn H. Cutometric assessment of elasticity of skin with striae distensae following carboxytherapy. J Cosmet Dermatol. 2018;17(6):1170–1174. doi:10.1111/jocd.12465
39. Ahmed NA, Mostafa OM. Comparative study between: carboxytherapy, platelet-rich plasma, and tripolar radiofrequency, their efficacy and tolerability in striae distensae. J Cosmet Dermatol. 2019;18(3):788–797. doi:10.1111/jocd.12685
40. Al-Muriesh M, Huang CZ, Ye Z, et al. Dermoscopy and VISIA imager evaluations of non-insulated microneedle radiofrequency versus fractional CO2 laser treatments of striae distensae. J Eur Acad Dermatol Venereol. 2020;34(8):1859–1866. doi:10.1111/jdv.16266
41. Sobhi RM, Mohamed IS, El SD, et al. Comparative study between the efficacy of fractional micro-needle radiofrequency and fractional CO2 laser in the treatment of striae distensae. Lasers Med Sci. 2019;34(7):1295–1304. doi:10.1007/s10103-019-02792-7
42. Seong GH, Jin EM, Ryu TU, et al. Fractional radiofrequency microneedling combined with fractional carbon dioxide laser treatment for striae distensae. Lasers Surg Med. 2021;53(2):219–226. doi:10.1002/lsm.23264
43. Nada HA, Sallam MA, Mohamed MN, et al. Optical coherence tomography-assisted evaluation of fractional Er: yAGLaser versus fractional microneedling radiofrequency in treating striae alba. Lasers Surg Med. 2021;53(6):798–805. doi:10.1002/lsm.23349
44. Tang Z, Wen S, Liu T, et al. Comparative study of treatment for striae alba stage striae gravidarum: 1565-nm non-ablative fractional laser versus fractional microneedle radiofrequency. Lasers Med Sci. 2021;36(9):1823–1830. doi:10.1007/s10103-020-03203-y
45. Issa MC, de Britto PKL, Chevrand NS, et al. Transepidermal retinoic acid delivery using ablative fractional radiofrequency associated with acoustic pressure ultrasound for stretch marks treatment. Lasers Surg Med. 2013;45(2):81–88. doi:10.1002/lsm.22105
46. Tian T, Luo Y, Wang H, et al. Efficacy and safety of a sublative bipolar fractional radiofrequency system combined with topical tretinoin in treating striae gravidarum: a randomized pilot study. Dermatol Surg. 2019;45(10):1245–1252. doi:10.1097/DSS.0000000000001933
47. Disphanurat W, Kaewkes A, Suthiwartnarueput W. Comparison between topical recombinant human epidermal growth factor and Aloe vera gel in combination with ablative fractional carbon dioxide laser as treatment for striae alba: a randomized double-blind trial. Lasers Surg Med. 2020;52(2):166–175. doi:10.1002/lsm.23052
48. Neinaa Y, Gheida SF, Mohamed D. Synergistic effect of platelet-rich plasma in combination with fractional carbon dioxide laser versus its combination with pulsed dye laser in striae distensae: a comparative study. Photodermatol Photoimmunol Photomed. 2021;37(3):214–223. doi:10.1111/phpp.12636
49. Preclaro I, Tianco E, Buenviaje-Beloso M. Efficacy of ablative fractional carbon dioxide laser combined with autologous platelet-rich plasma versus ablative fractional carbon dioxide laser and placebo in the treatment of striae gravidarum: a randomized clinical trial. J Cosmet Dermatol. 2022. doi:10.1111/jocd.14791
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.