Back to Journals » Open Access Emergency Medicine » Volume 13
New Horizons in Understanding Appropriate Prehospital Identification and Trauma Triage for Older Adults
Authors Alshibani A ![]() , Banerjee J, Lecky F
, Banerjee J, Lecky F ![]() , Coats TJ
, Coats TJ ![]() , Alharbi M
, Alharbi M ![]() , Conroy S
, Conroy S
Received 17 December 2020
Accepted for publication 26 February 2021
Published 26 March 2021 Volume 2021:13 Pages 117—135
DOI https://doi.org/10.2147/OAEM.S297850
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hans-Christoph Pape
Abdullah Alshibani,1,2 Jay Banerjee,1,3 Fiona Lecky,4 Timothy J Coats,3,5 Meshal Alharbi,2,5 Simon Conroy1
1Department of Health Sciences, College of Life Sciences, University of Leicester, Leicester, UK; 2Emergency Medical Services Department, College of Applied Medical Sciences, King Saud Bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia; 3University Hospitals of Leicester NHS Trust, Leicester, UK; 4Centre for Urgent and Emergency Care Research, University of Sheffield, Sheffield, UK; 5Department of Cardiovascular Sciences, University of Leicester, Leicester, UK
Correspondence: Abdullah Alshibani
Department of Health Sciences, College of Life Sciences, George Davies Centre, University of Leicester, 15 Lancaster Road, Leicester, LE1 7HA, UK
Email [email protected]
Abstract: Caring for older people is an important part of prehospital practice, including appropriate triage and transportation decisions. However, prehospital triage criteria are designed to predominantly assess injury severity or high-energy mechanism which is not the case for older people who often have injuries compounded by multimorbidity and frailty. This has led to high rates of under-triage in this population. This narrative review aimed to assess aspects other than triage criteria to better understand and improve prehospital triage decisions for older trauma patients. This includes integrating frailty assessment in prehospital trauma triage, which was shown to predict adverse outcomes for older trauma patients. Furthermore, determining appropriate outcome measures and the benefits of Major Trauma Centers (MTCs) for older trauma patients should be considered in order to direct accurate and more beneficial prehospital trauma triage decisions. It is still not clear what are the appropriate outcome measures that should be applied when caring for older trauma patients. There is also no strong consensus about the benefits of MTC access for older trauma patients with regards to survival, in-hospital length of stay, discharge disposition, and complications. Moreover, looking into factors other than triage criteria such as distance to MTCs, patient or relative choice, training, unfamiliarity with protocols, and possible ageism, which were shown to impact prehospital triage decisions but their impact on outcomes has not been investigated yet, should be more actively assessed and investigated for this population. Therefore, this paper aimed to discuss the available evidence around frailty assessment in prehospital care, appropriate outcome measures for older trauma patients, the benefits of MTC access for older patients, and factors other than triage criteria that could adversely impact accurate prehospital triage decisions for older trauma patients. It also provided several suggestions for the future.
Keywords: undertriage, geriatrics, injury, emergency, paramedics, frailty
Introduction
The population of older adults has increased worldwide over the last years. More people in the world currently live into or beyond 60 years of age.1 The number of older adults aged 60 years and over has projected by 48% from 607 million in 2000 to 901 million in 2015.1 The number of this population (60 years and over) is expected to reach a total of 2.1 billion by 2050.1 This means the rates of older adults requiring health care including trauma care will increase. Therefore, high-quality trauma care for this population is needed including that of prehospital trauma care.
Prehospital care represents an essential and important part of the patient’s journey and plays a significant role in determining outcomes. One of the main principles of prehospital care is to get the right patient, to the right place, at the right time.2 This means prehospital assessment should accurately identify complaint(s), nature, and severity enabling appropriate triage decisions. This article aims to highlight and investigate the issues around prehospital trauma triage of older patients, discuss the current evidence, and provide recommendations for future improvement of prehospital care for older people.
Scope of the Problem
Many triage tools have been developed to aid prehospital care providers to make appropriate and accurate triage decisions for patients. However, this is far from true when it comes to the prehospital triage of people aged ≥55 years, especially for trauma. The literature from the United States of America (USA) and Australia show increased rates of under-triage among this population.3–15 Under-triage is simply defined as the transportation of severely injured patients to lower-level Trauma Centers (TCs) or other Acute Care (AC) facilitates, as opposed to Major Trauma Centers (MTCs) (equivalent to major trauma service or Level I or II TCs).16 A number of recent studies in the USA developed trauma triage tools specific for older adults in order to improve early identification and appropriate triage and transportation decisions.8,12–14,17 Although most of these tools had better sensitivity than the current adult trauma triage tools, they had sub-optimal specificity.12–14 Only one recently developed triage tool has a better sensitivity with an acceptable reduction in the specificity when compared to current triage tool for adult trauma patients in predicting the need of MTC care (sensitivity: 93% vs 61%, and specificity: 49% vs 61%).8 Furthermore, the performance of this tool among older trauma patients is similar to the performance of the current triage tool in younger trauma patients (sensitivity: 93% vs 87%, and specificity: 49% vs 44%, respectively).8 However, using the cut-off point of ≥70 years in this study represents a major limitation as a previous study from the USA has shown that the issue of under-triage can begin as early as the age of 50 years.4
Current triage tools predominantly assess injury severity or high-energy mechanism. However, older people usually have injuries compounded by multimorbidity and frailty. They also exhibit age-related anatomical and physiological changes,18–24 which could adversely affect the accuracy of the triage tool. This in turn risks inappropriate prehospital identification and transportation decisions. Therefore, applying traditional trauma triage criteria only, for the assessment of older adults, may not be effective. However, integrating additional assessment tools such as frailty assessment into prehospital trauma tirage may improve early identification of older patients who are at high risk of adverse outcomes.
Frailty assessment has been embedded in routine care for patients requiring emergency care in the United Kingdom (UK). Applying simple frailty assessment tools using, for example, the Clinical Frailty Scale (CFS) was shown recently to independently predict 30-day mortality, inpatient delirium, and increased care level at discharge in trauma patients aged ≥65 years.25 The application of the CFS in emergency care was determined to be feasible, reliable, and accurate.26 However, compliance to frailty attuned scores in prehospital care may impact their effectiveness in such setting as previous evidence showed that paramedics’ compliance with trauma triage tools varied from a rate of 21% to 93%.27
Whilst there is reasonable evidence that care in MTCs benefits younger patients with severe injuries, it is uncertain whether or not the same benefits will accrue to injured older adults. This could be partially due to the lack of trauma-specific outcome measures for older people,28 thereby limiting the determination of benefits of MTC access. It also results from differences in aetiology - whereby high energy transfer (road traffic collisions, sport, assault) is usually required to injure a young adult. However, from the seventh decade of life onwards, major injury is most likely to result from fall from a standing height.29 Older people are more likely to have low-level falls (ie, <2 meters) and when they occur, major injury is more likely to result compared to younger adults.29 The less robust injured structures may not respond to aggressive treatments (organ surgery and critical care) employed in MTCs. Hence, there is a need to clarify the optimal level of care that should be provided to older people to support Emergency Medical Service (EMS) personnel decision-making.
Little is known about factors other than triage criteria that could affect the triage decisions of older trauma patients including patient (or relative) choice, paramedics’ training and familiarity with protocols, and their impact on outcomes.
The aim of this article is to provide an overview on prehospital frailty assessment, appropriate outcome measures for older trauma patients, the benefits of MTC access for older patients, and factors other than triage criteria that could impact accurate triage decisions for older trauma patients, discuss the evidence base surrounding these issues, and recommend possible solutions that require further scrutiny from prehospital care providers and policymakers within the healthcare system.
Frailty Assessment in Prehospital Care
Frailty is known to be an independent predictor of mortality, morbidity, and hospitalizations among older adults from studies including older trauma patients.30,31 The “frailty index” has been shown to be an independent predictor of poor health outcomes, in-hospital complications, and adverse discharge disposition among older trauma patients.32–34 Hitherto, no frailty assessment tool has been used for older trauma patients as a method of prehospital triage.
With respect to applying frailty assessment in prehospital care, there is a limited evidence on the feasibility of assessing frailty and the validation of frailty assessment tools (Table 1).35–37 Two studies from Canada investigated the feasibility of the Care Partner – Comprehensive Geriatric Assessment (CP-CGA) and validity of the Care Partner-derived Frailty Index based upon Comprehensive Geriatric Assessment (CP-FI-CGA) to measure frailty in the prehospital phase by paramedics and in busy clinical practice (Table 1).35,36 One recent study from Australia assessed the perceptions of paramedic students about the application of the Edmonton Frail Scale (EFS) and the Groningen Frailty Index (GFI) for assessing and screening older adults in the prehospital phase (Table 1).37 Overall, frailty assessment and screening in the prehospital phase was recognised to be important and feasible.
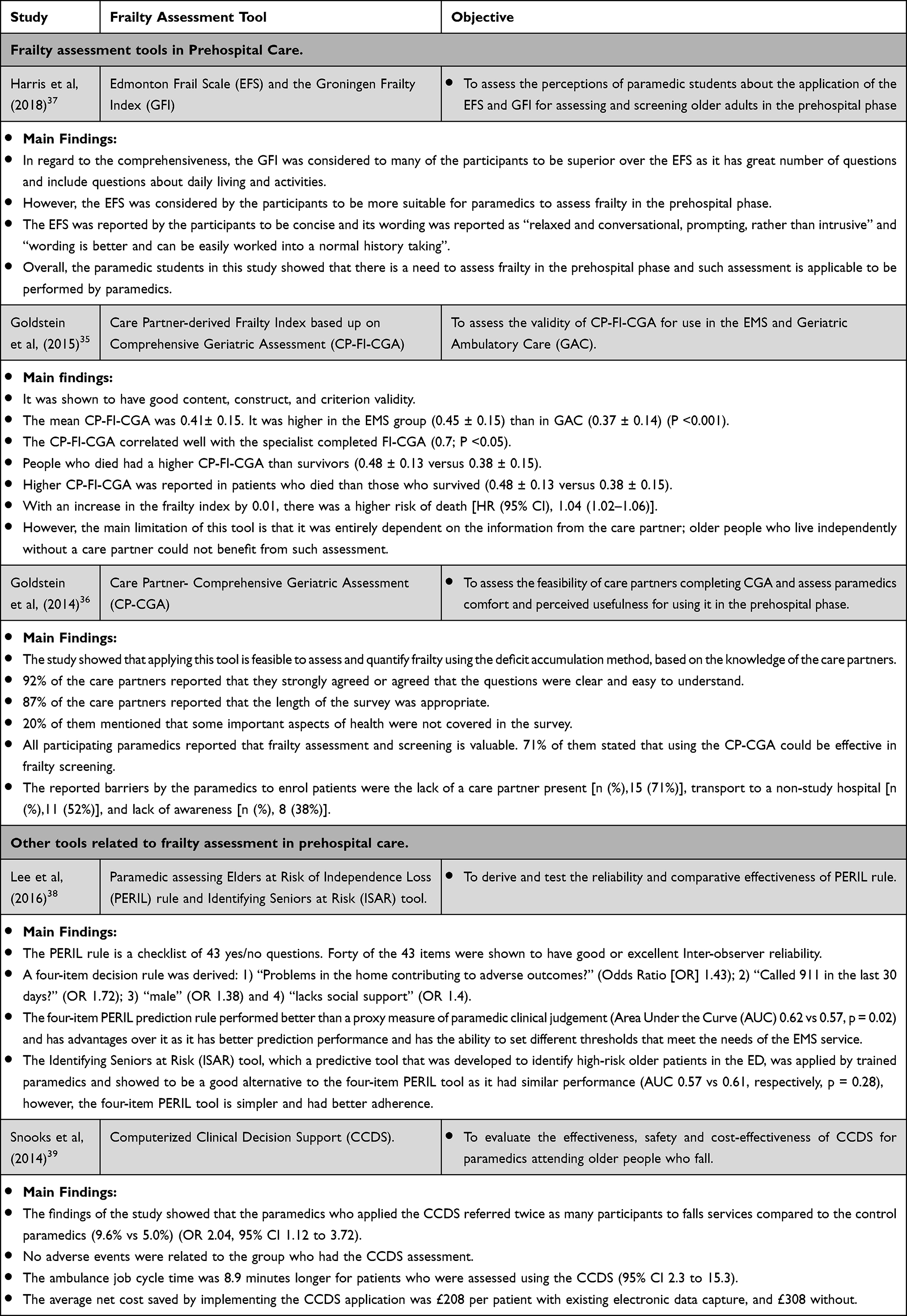 |
Table 1 The Use of Frailty Assessment Tools in Prehospital Care |
Furthermore, two studies have investigated the application of clinical decision rules by paramedics to determine which older person should stay at home or be transported to the Emergency Department (ED).38,39 Although neither of these studies explicitly assessed frailty among older adults, the outcomes of these studies were relevant to frail patients.38,39 One study from Canada assessed the performance of the Paramedic assessing Elders at Risk of Independence Loss (PERIL) rule which is a checklist of 43 yes/no questions for all older patients and not specific to trauma or fall mechanisms38 (Table 1). The study showed that the four-item PERIL prediction rule performed better than a proxy measure of paramedic clinical judgement and has more advantages over it as it has better prediction performance and has the ability to set different thresholds that meet the needs of the EMS service38 (Table 1). The Identifying Seniors at Risk (ISAR) tool, which is a screening tool that was developed to identify high-risk older patients in the ED, was applied by trained paramedics and showed to be a good alternative to the four-item PERIL tool as it had similar performance (AUC 0.57 vs 0.61, respectively, p = 0.28), however, the four-item PERIL tool is simpler and had better adherence.38 The other study from the UK evaluated the effectiveness, safety, and cost-effectiveness of the Computerized Clinical Decision Support (CCDS) for paramedics attending older people who fall.39 The study showed that the use of CCDS is safe, effective in referring older people who fall to community falls services and potentially cost-effective39 (Table 1).
Overall, frailty assessment in prehospital care was shown to be important, feasible, and maybe cost-effective. This suggests that Integrating frailty assessment in prehospital triage could improve the accuracy of appropriate triage decisions and be more beneficial in terms of outcomes.
Determining Appropriate Outcome Measures
An outcome measure is referred to any measure that is chosen to assess the impact of interventions.40 It is a supposition that is the end point of an intervention.40 Therefore, it is important to measure the impact of interventions on outcomes. Mortality is an important Clinician Reported Outcome Measure (CROM) to improve trauma care for patients. It should be the primary focus when assessing trauma outcomes. For example, changing the trauma care system in the UK was shown to improve survival rates.41 However, reliance mostly on mortality as the primary outcome measure and not looking for other important secondary outcomes especially for older people seems to be inappropriate and could lead away from a focus on patient-centred care. A global health standard set of outcome measures in older persons which was relevant for people in the last 10 years of life was developed.42 It showed that older adults and their carers perceived survival to be less crucial than other outcome measures.42 In fact, they consider mortality as an inevitable and expected outcome.42 Outcomes that were considered important by older persons and their carers included:
- independence and living at own home,
- participation in social and community activities,
- quality of life and wellbeing,
- the avoidance of inappropriate discharge and readmission,
- isolation,
- loneliness and friendship,
- physical disabilities,
- hobbies and activities,
- access to 24 hours healthcare and social services,
- avoiding falls,
- delaying frailty,
- care and respite for the carer,
- malnutrition,
- physical symptom burden,
- pain,
- and sleep quality.42
In terms of outcomes following major trauma, an expert panel, which determined research priorities for older trauma patients, highlighted the need to determine appropriate outcome measures specifically for older people.28 They mentioned, for example, that the identification of polytrauma in older people living with frailty does not always change their outcomes, so in young trauma patients, we usually expect them to walk out of hospital and regain their full functional ability, while in these patients, we may rather look at their comfort and palliation.28
Previous reviews showed that many outcome measurement tools are used in trauma registries to assess patient outcomes following trauma.43–46 For example, a recent scoping review showed that more than 100 unique measurement tools were used to assess Patient-Reported Outcome Measures (PROMs) for hospitalized trauma patients.45 However, no study, to date, has investigated and validated the use of already existing outcome measure or developed an outcome measure specifically for older trauma patients. In the UK, a consensus study made recommendations on appropriate outcome measures for adults in general and pediatrics following major trauma, but no consensus has been made specifically for older adults.47
Therefore, it is important to assess CROMs and PROMs for older trauma patients as we need to look at both outcome measures in order to strike an ethical balance between paternalism (in healthcare provision) and autonomy (of the patient in what they expect and seek) when caring for this population.
Outcomes Beyond Mortality for Older Trauma Patients
For the assessment of outcomes beyond mortality for older trauma patients, outcomes including frailty, mental health, quality of life, overall health status, complications, use of healthcare services, in-hospital Length of Stay (LOS), readmission, functional status, and level of independence are all reported to be important (Table 2).
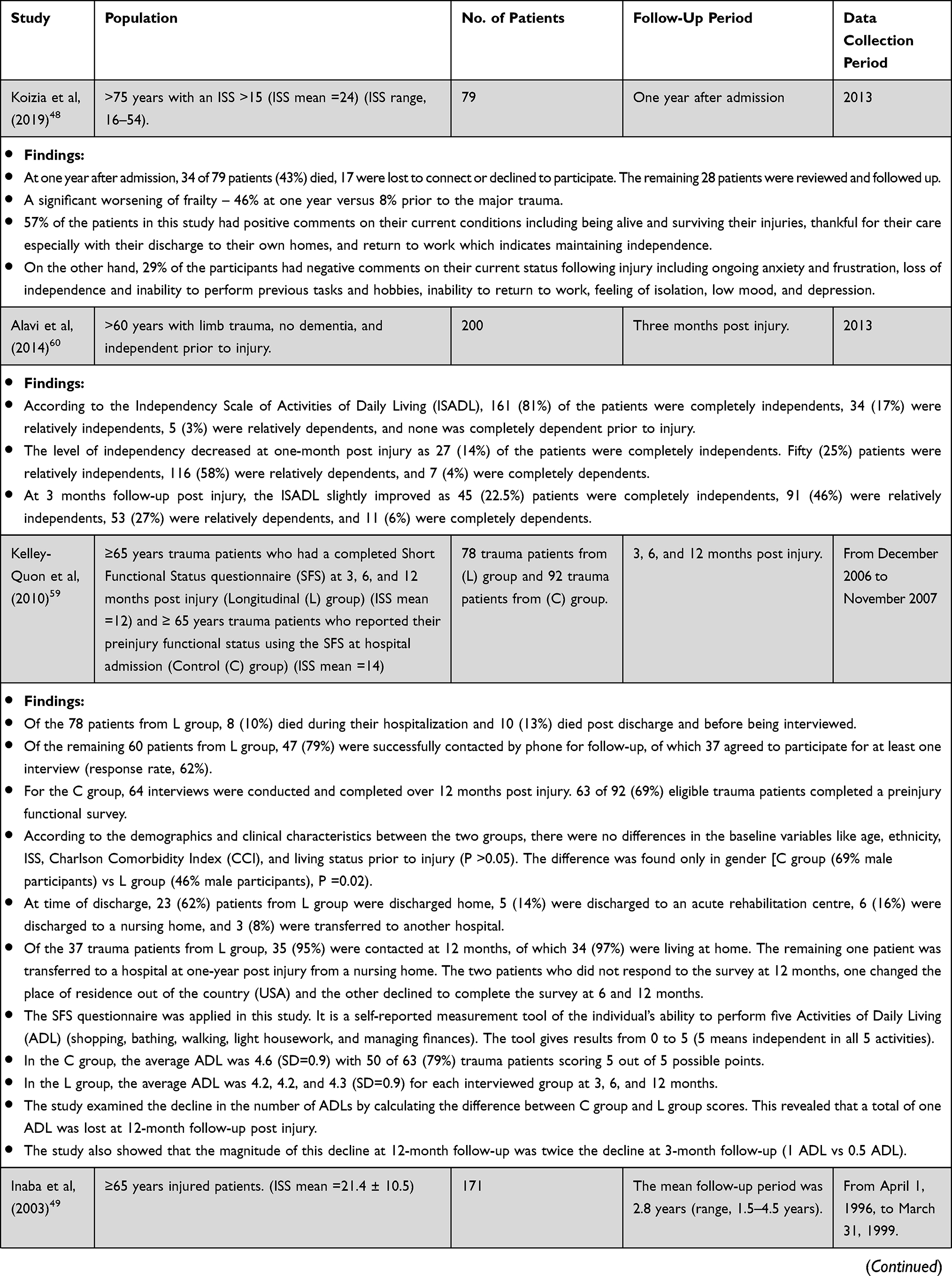 | 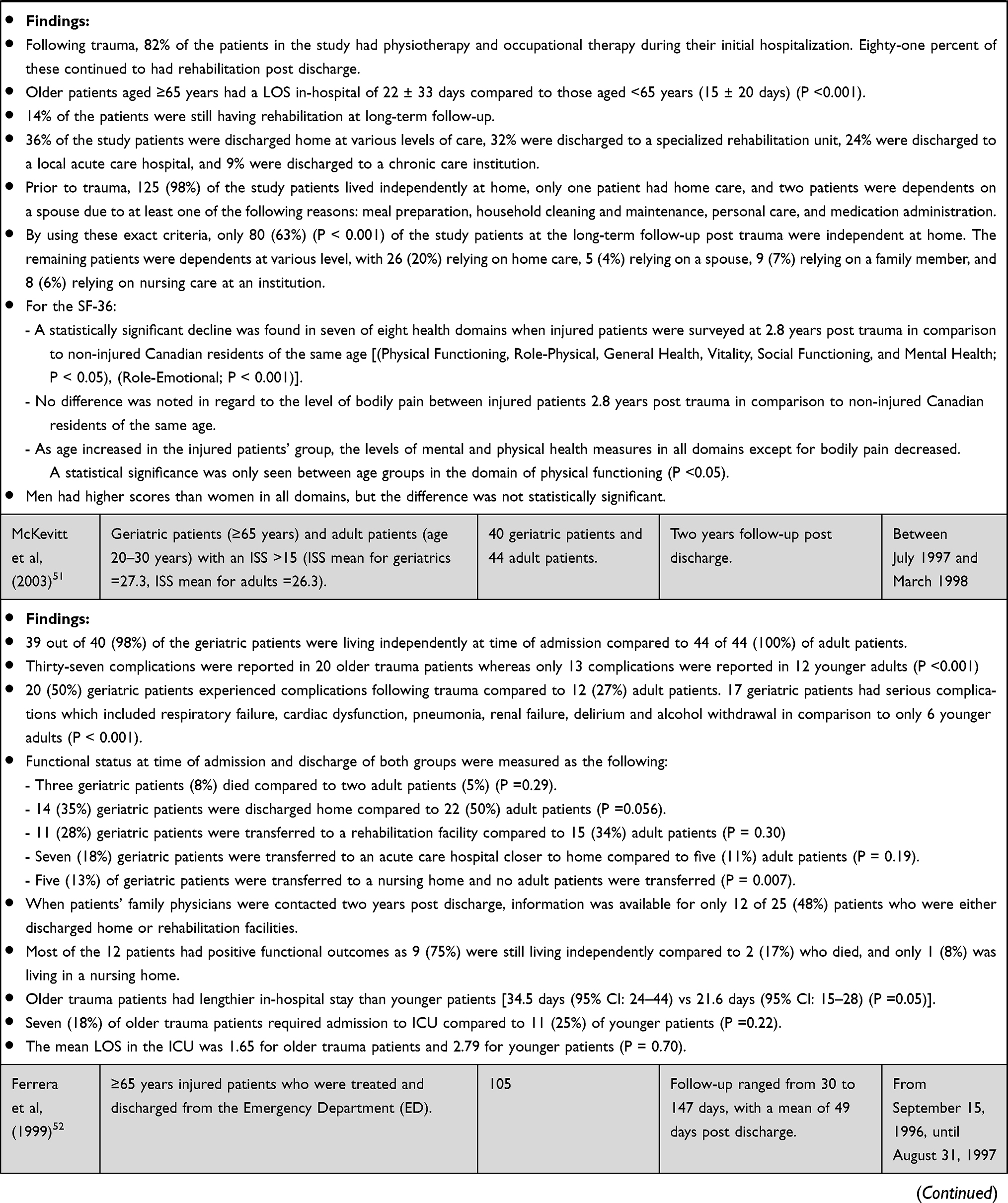 | 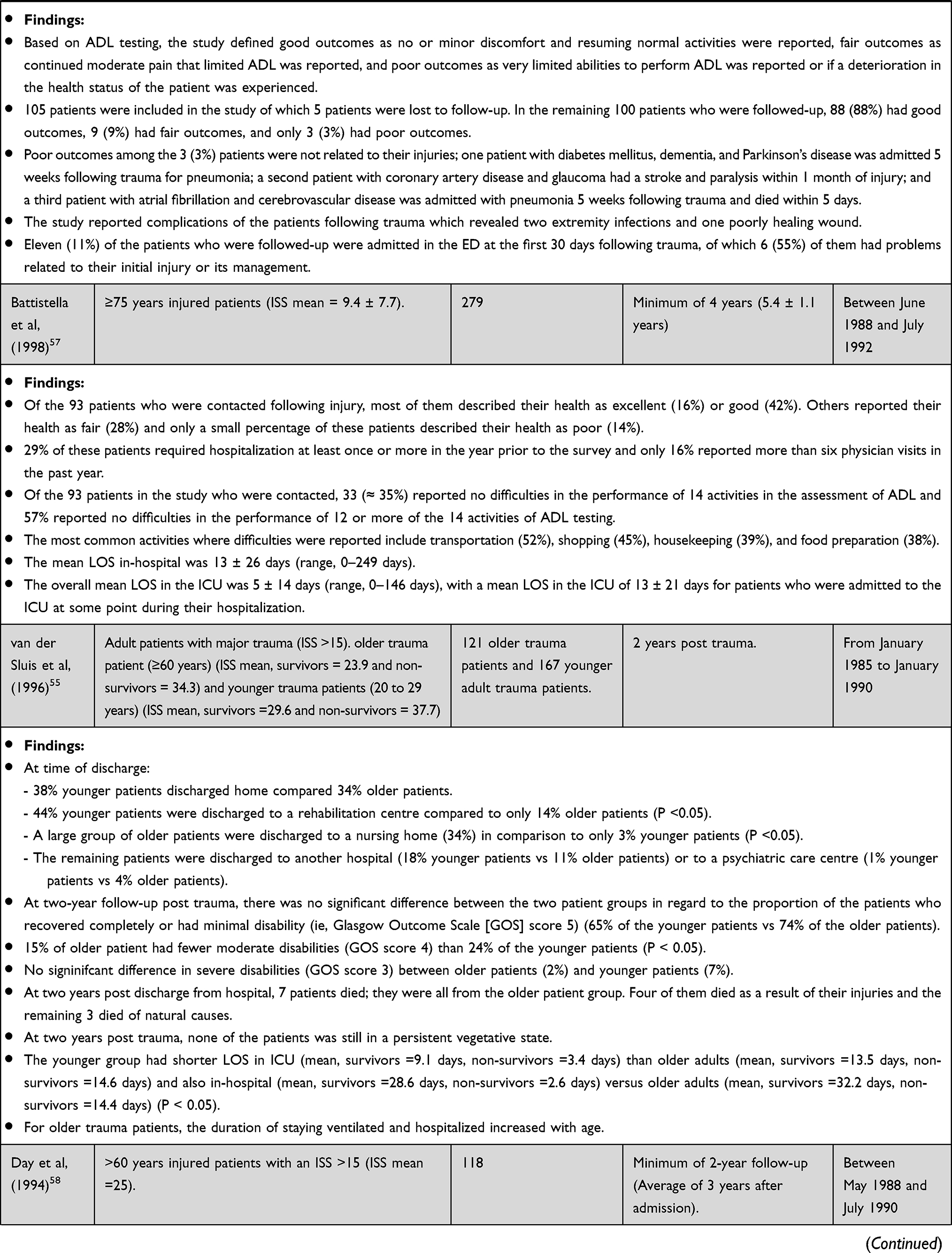 | 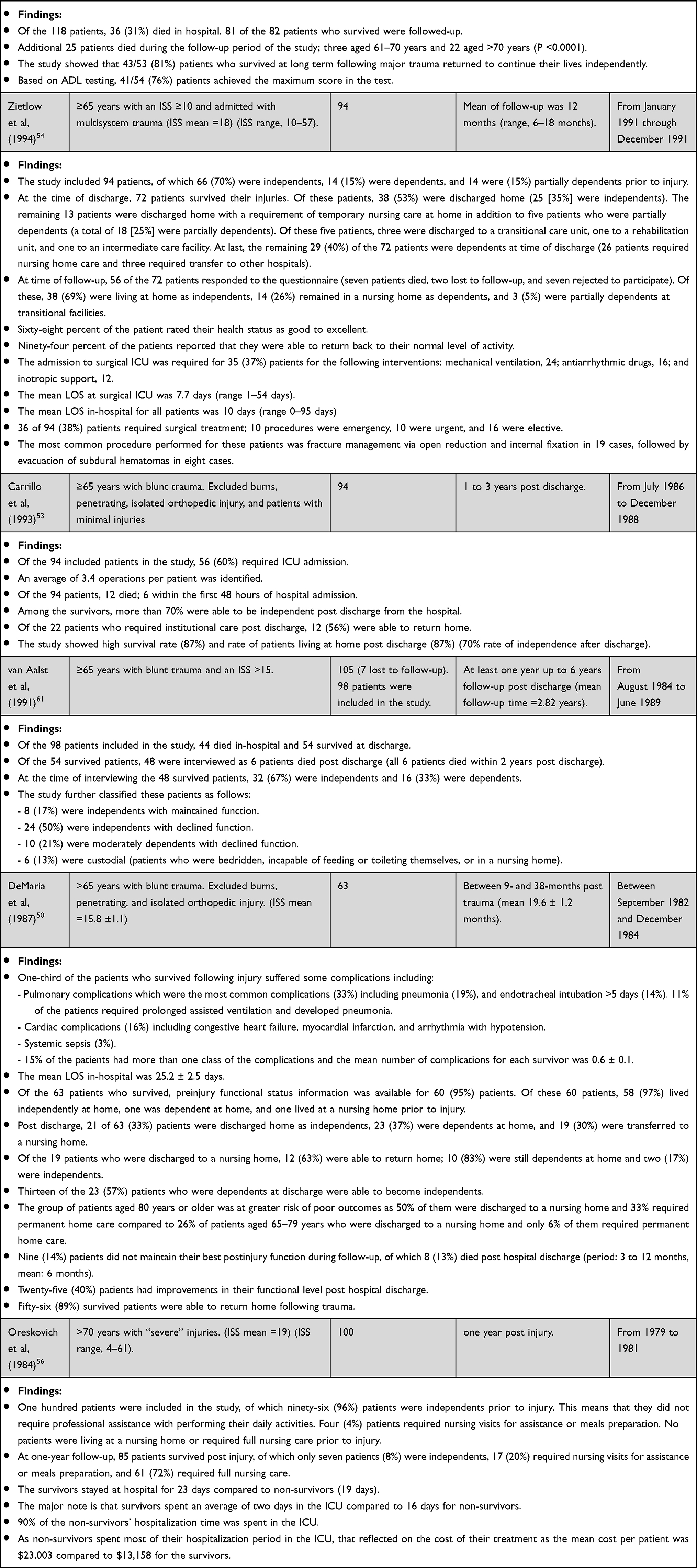 |
Table 2 Outcomes Beyond Mortality for Older Trauma Patients |
Frailty and Overall Health Status
Only one study from the UK assessed frailty during follow-up period and showed that patients aged >75 years with major trauma (Injury Severity Score [ISS] >15) had significant worsening of frailty at one-year after injury compared to pre-injury (8% of the study group were frail at pre-injury phase compared to 46% at one-year post injury).48 It also reported that 57% had positive comments on their mental health, quality of life, and functional status whereas 29% of the participants have negative comments on the same aspects at one-year following major trauma.48 Inaba et al49 showed a significant decline in seven of eight health domains using the 36-item Short Form survey (SF-36) at 2.8 years after trauma for trauma patients aged ≥65 years compared to non-injured residents of the same age (Table 2).
Complications
Few studies reported serious complications of older patients following trauma including pulmonary complications, cardiac complications, systematic sepsis, renal failure, delirium, and alcohol withdrawal (Table 2).50,51 When compared to younger adults, older trauma patients who survived following trauma had significantly higher serious complication rates.51 Lower rates of complications related to injury were reported for older patients discharged from the ED including extremity infection and poorly healing wounds (Table 2).52
Use of Healthcare Services
With regard to the use of healthcare services, more than 80% of the older trauma patients required rehabilitation (physiotherapy or occupational therapy) extending beyond discharge from the hospital.49 An average of 3.4 operations were performed per patient for trauma patients aged ≥65 years.53 Thirty-eight percent of trauma patients with ISS ≥10 required surgical treatment (Table 2).54 The most common performed procedure for these patients was fracture management via open reduction and internal fixation (Table 2).54
Sixty percent of trauma patients aged ≥65 years required Intensive Care Unit (ICU) admission.53 Previous evidence showed no significant change in ICU admission between older and younger trauma patients51,55 (Table 2). Older adults with major trauma (ie, ISS >15) stayed ventilated in the ICU for longer periods than younger patients and the duration of staying ventilated increased with age55 (Table 2). For the use of surgical ICU, 37% of trauma patients aged ≥65 years with an ISS ≥10 were admitted for the following interventions: mechanical ventilation, antiarrhythmic drugs, and inotropic support.54
An earlier study showed that 90% of hospitalization time for non-survivor older trauma patients aged >70 years was spent in the ICU.56 This reflected on the cost of their treatment as the mean cost per patient was $23,003 compared to $13,158 for the survivors.56
Length of Stay
Variation in hospital LOS for older trauma patients ranges from a mean of 10 days to 35 days (Table 2).49–51,54–57 Older trauma patients significantly stayed for longer period in-hospital than younger patients even after major trauma (ie, ISS >15) (Table 2).49,51,55 Furthermore, older patients with an ISS >15 who survived had lengthier in-hospital stay than younger adults and also the same is true for those who did not survive55 (Table 2). For patients aged >70 years, those who survived had a mean LOS of 23 days compared to 19 days for non-survivors.56
Differences in ICU LOS were identified in the literature ranging from a mean of 2 days to 16 days51,54–57 (Table 2). One study showed that patients aged ≥65 years with an ISS >15 had shorter LOS in ICU than younger patients aged 20–30 years old (P =0.70).51 However, another study showed significantly increased LOS in ICU for older patients who survived and who did not survive compared to younger patients after major trauma (ie, ISS >15) (P <0.05)55 (Table 2). Older trauma patients aged >70 years who survived spent an average of two days in the ICU compared to 16 days for those who did not survive.56
Readmission and Hospitalization
A previous study, which followed-up older trauma patients for a mean length of 5.4 (SD ± 1.1) years, found that 29% of trauma patients aged ≥75 years required hospitalization at least once in the year preceding the survey.57 It also showed that 16% of the patients reported more than six physician visits in the previous year.57 Of injured patients aged ≥65 years and discharged from the ED, 11% were admitted to the ED at the first 30 days following trauma, of which 55% had problems related to their initial injury or its management (Table 2).52
Functional Status and Level of Independence
For the assessment of functional status, Oreskovich et al56 showed that more than 90% of trauma patients aged >70 years with “severe” injuries (ISS mean =19) required nursing care at home or in a nursing care facility. The studies published after that, however, showed more promising results, with 70% or more of older patients with different ISS means returning to live independently at home (Table 2).50,51,55,58,59 Others also reported much higher rates of independence and living at home than the earlier study by Oreskovich et al56 (Table 2).48,49,52–54,57,60,61 Although improvements in the level of independence and living at home were reported at different follow-up periods, it did not reach the pre-injury level (Table 2).49–51,54,60 Progressive deterioration in functional ability for older trauma patients at one-year follow-up was reported59 (Table 2). However, comparing the results of functional status for older trauma patients is difficult due to the recruitment of different patient populations (age group, pattern of injury, and injury severity), applying different follow-up periods (ranging from a mean of 49 days up to 5 years), not using standardized measures, variable definitions of “independence”, and many studies were published more than a decade ago (Table 2).
Overall, the findings of these studies indicate the importance of measuring outcomes other than mortality for older trauma patients. These could include outcome measures looking into independence and living at own home, frailty, cognition and mood, social networking and support, complications, and use of healthcare services, LOS, and readmissions.
Prehospital Triage and Outcomes
The impact of prehospital triage decisions on outcomes of older trauma patients is still uncertain.3,5,10,15 Most of current prehospital triage tools were assessed for their accuracy in identifying major trauma among older people4,6,8,9,11,12,14,17,62 and only few were assessed for their effects on the outcomes, with mortality used as the main outcome measure.3,5,7,10,13,15,63,64 Other outcomes including disability, complications, costs, LOS, and discharge to home were rarely captured in the assessment of triage tools.7,10,15,63 No standardized patient outcome measures regarding functional status, quality of life, and well-being for older trauma patients were reported in these studies.
Determining the Benefits of Major Trauma Centres Access
There is still no strong consensus if triaging older trauma patients to MTCs is beneficial (Table 3). In terms of mortality, a recent evidence showed that older trauma patients were under-triaged, ie, had lower odds of MTC transport (adjusted OR 0.52, 95% CI 0.35–0.78) than younger adults and this was associated with 1.7 times increase in their in-hospital mortality (95% CI 1.04–2.7).3 Furthermore, a previous study showed that under-triaged older trauma patients had higher mortality than under-triaged younger patients (21% vs 6.0%, respectively).10 However, Staudenmayer et al15 investigated the unadjusted 60-day mortality rate for older trauma patients with an ISS >15 and found no significant difference between patients who were transported to non-MTCs compared to those transported to MTCs (16% vs 17%, p=0.87). They also showed that the transportation of this population to MTCs is associated with higher costs [Total costs, $, median (Interquartile Range [IQR]): 35,069 (19,321–88,357) vs 14,332 (5112–29,321)] and prolonged in-hospital LOS [LOS, days, median (IQR): 6.0 (3.0–14.0) vs 5.0 (1.5–8.0)].15 The study, however, did not adjust for comorbidities and there was no consideration of specific patterns of injury such as head injury.15 The study also performed mortality analysis based on only 41 deaths which may have impacted the precision of the estimated effect.15
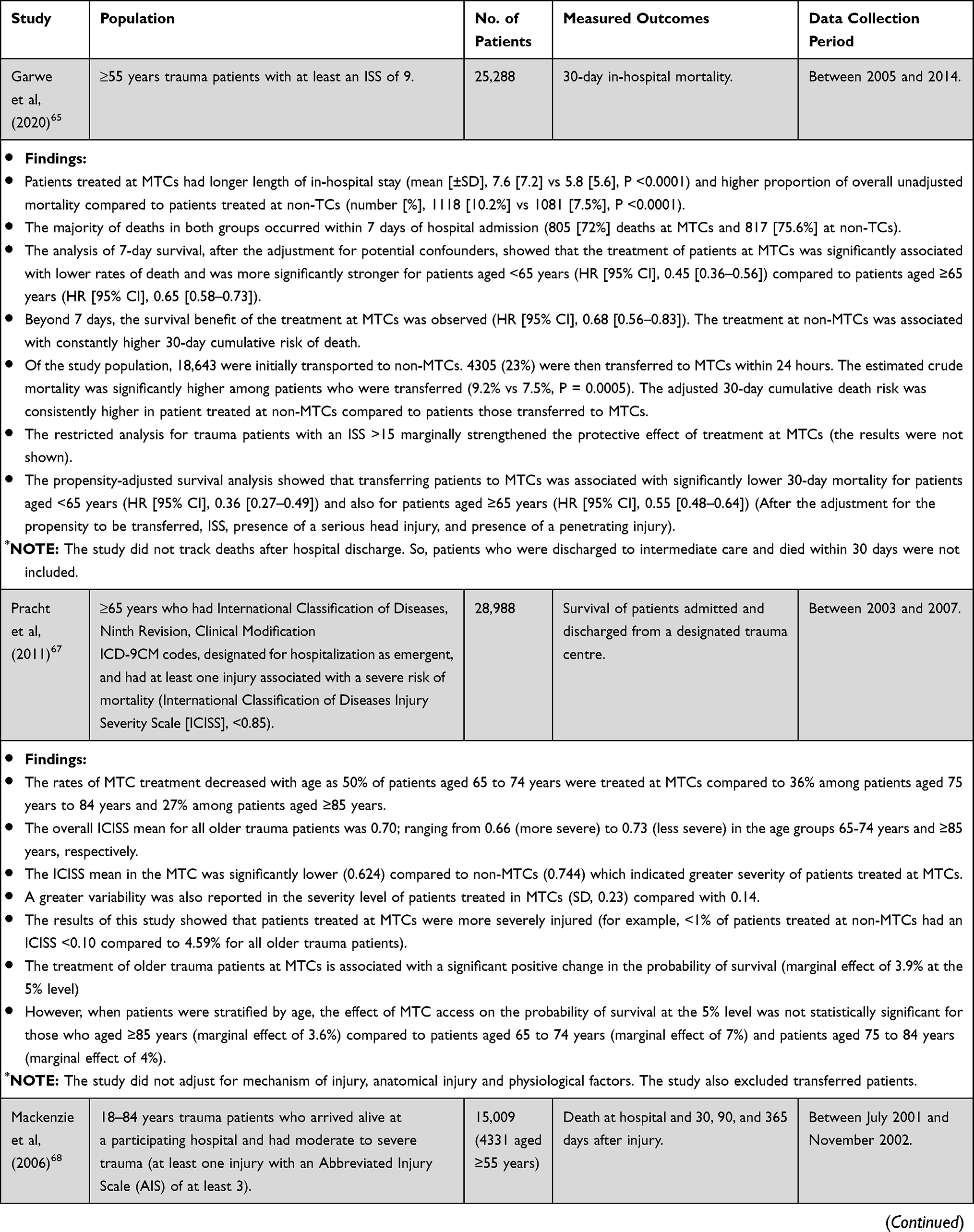 | 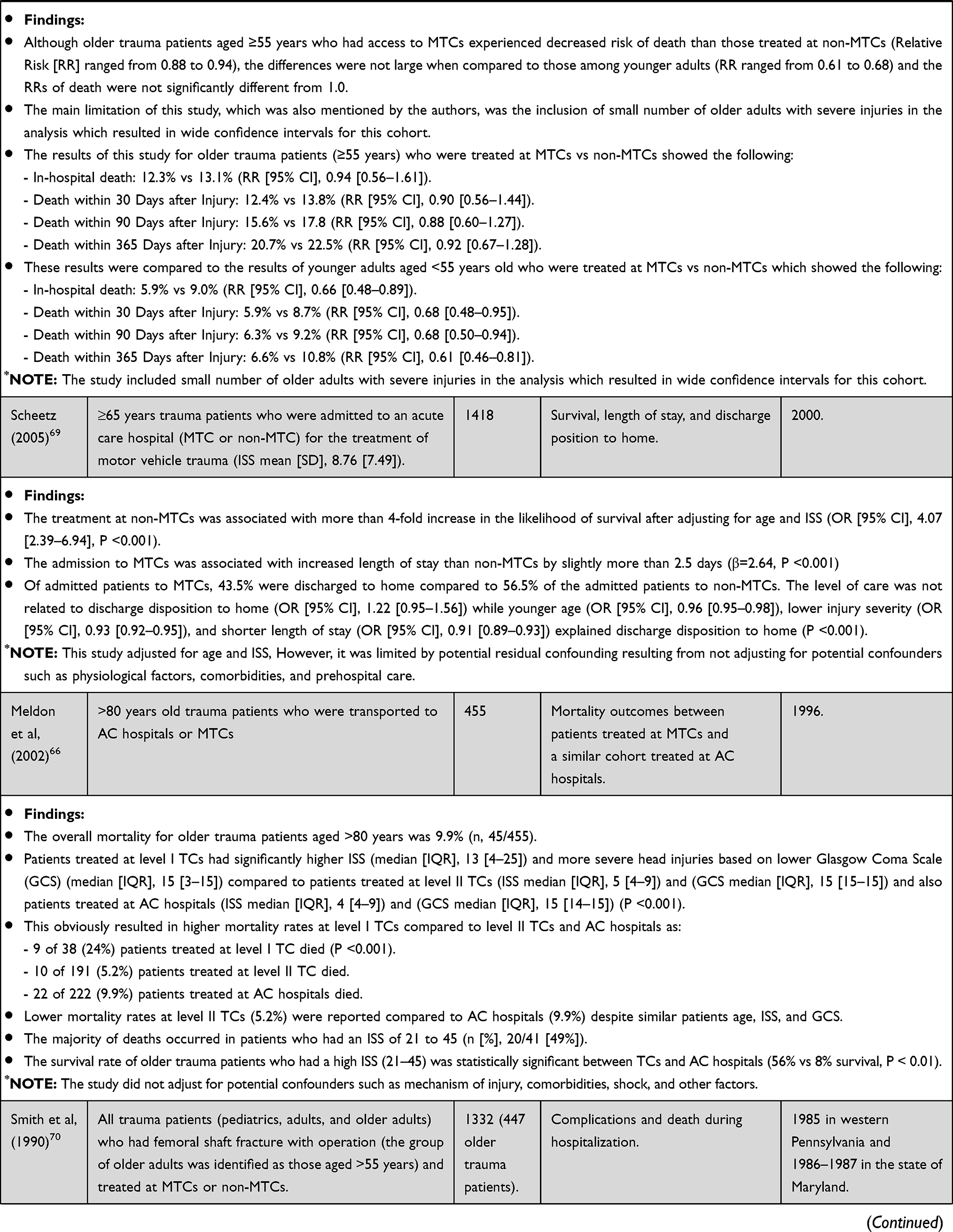 | 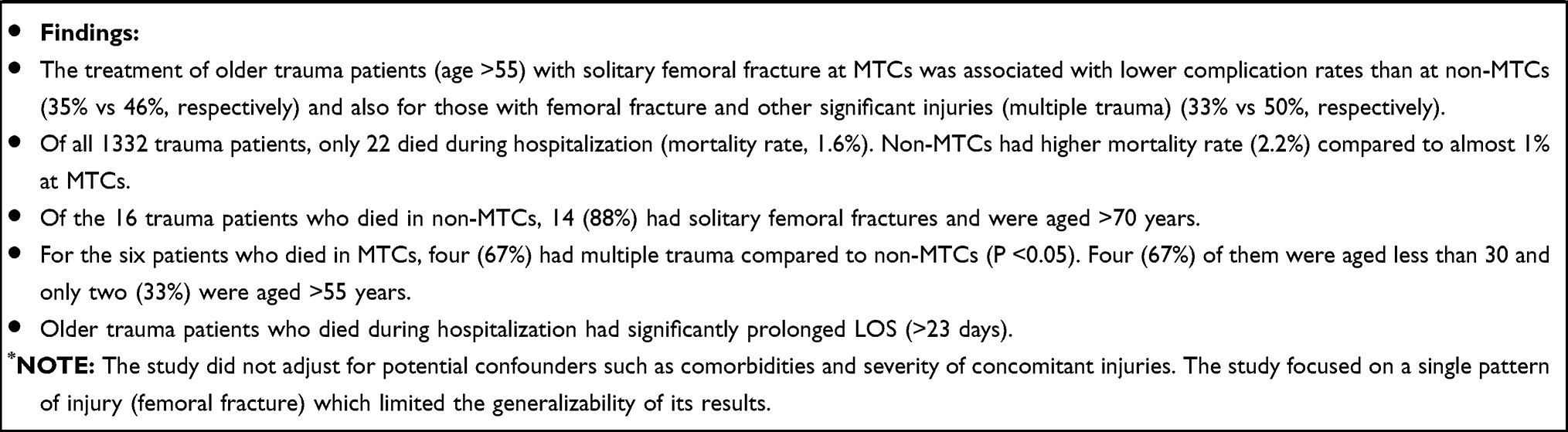 |
Table 3 Benefits of MTC Access for Older Trauma Patients |
A recent study, which assessed the impact of specific geriatric trauma triage criteria on outcomes found no significant difference in mortality rate before its application (7.1%) (95% CI, 6.6–7.4%) compared to post application (6.6%) (95% CI, 5.9–6.6%) despite identifying more older trauma patients who required MTC transport (improved sensitivity from 61% to 93% after applying the criteria).63 It also showed minimal increase in the rate of older trauma patients discharged home from 34% (95% CI 33–35%) to 35% (95% CI, 35–35%) (difference 1.2%, 95% CI of the difference 0.2–2.2%).63 However, the results of this study may have been influenced by destination compliance as initial transportation to MTCs improved by only 1% after the application of the developed triage tool (45% vs 44%).63 “Destination compliance” is simply defined as access to the highest level of trauma services for patients who meet the prehospital trauma triage criteria. Another study showed higher disability rates (22% vs 6.0%) and complication rates (39% vs 23%) in older trauma patients triaged to lower MTCs in comparison with their younger counterparts.10
As previous literature looking into the benefits of prehospital triage of older trauma patients to MTCs showed conflicting findings, these findings echo the broader literature, which showed no strong consensus about the impact of conveyance to MTCs for older people with trauma (Table 3). The literature review showed that most of the previous evidence investigated the benefits of older trauma patients’ access to MTCs with regards to their survival or mortality. Other outcomes that were rarely measured regarding the benefits of MTC access for older trauma patients included LOS, complications, and discharge to home. No patient outcomes were measured in the previous literature to assess the benefits of MTC access including outcomes related to mental health, functional ability, and quality of life. Such outcomes were shown in the previous section to be important to measure when caring for older trauma patients.
Previous evidence showed survival benefit for the treatment of older trauma patients of different age groups at MTCs compared to non-MTCs (Table 3).65–67 However, some other studies showed no significant advantage of such access for older trauma patients68 and that the treatment at non-MTC was associated with more than 4-fold increase in the likelihood of survival (Table 3).69 It was shown that the admission of older trauma patients to MTCs was associated with lengthier in-hospital stay than non-MTCs (Table 3).69 Smith et al70 showed that the treatment of patients aged >55 years at MTCs was associated with lower rates of complications than those treated at non-MTCs (Table 3). The level of care, however, was not associated with discharge to home rates (Table 3).69
Although most of these studies showed some benefit of MTC access for older adults, generalizing these results may not be appropriate as these studies had variations in the datasets that were used for analysis, included different patient populations in different trauma systems, and assessed different outcome measures. Furthermore, some of these studies did not adjust for some important confounders such as physiological factors, comorbidities, and mechanism of injury,66,67,69,70 included small number of patients,68 excluded transfers,67 focused on single pattern of injury,70 and did not track deaths post hospital discharge within a defined period65 - all of which make comparisons difficult.
Factors Affecting Appropriate Triage Decisions
There are several unique factors that could adversely affect accurate prehospital trauma triage decisions for older patients. Some of which could directly affect meeting the thresholds of the existing triage criteria for direct transportation to an MTC including anatomical and physiological changes with age, comorbidities, and medication use.71 The efforts in recent research tried to overcome these challenges by developing geriatric-specific trauma triage criteria that are accurate enough to capture severely injured older patients.71 However, no geriatric-specific trauma triage criteria have achieved acceptable sensitivity and/or specificity71 and some were not applied to all older trauma patients.8
Despite these factors, there are other important factors that are not related to triage criteria and could significantly affect prehospital trauma triage decisions for older patients. Previous studies have consistently shown decreased rates of destination compliance among injured patients with increasing age.5,12,62 For instance, a study from Australia showed that nearly 67% of the older trauma patients who met the triage criteria were transported to MTCs in contrast to almost 88% of the injured younger patients.5 This finding is consistent with other studies from the USA even when a specific triage tool for older adults was developed.4,14,62,63 In this regard, there is limited evidence that factors other than the triage criteria have been assessed in relation to their effect on prehospital triage decisions for older trauma patients (Table 4). No study has assessed the impact of such factors on outcomes. These initial findings showed that such factors could impact prehospital triage decisions for these patients and may, consequently, affect their outcomes.
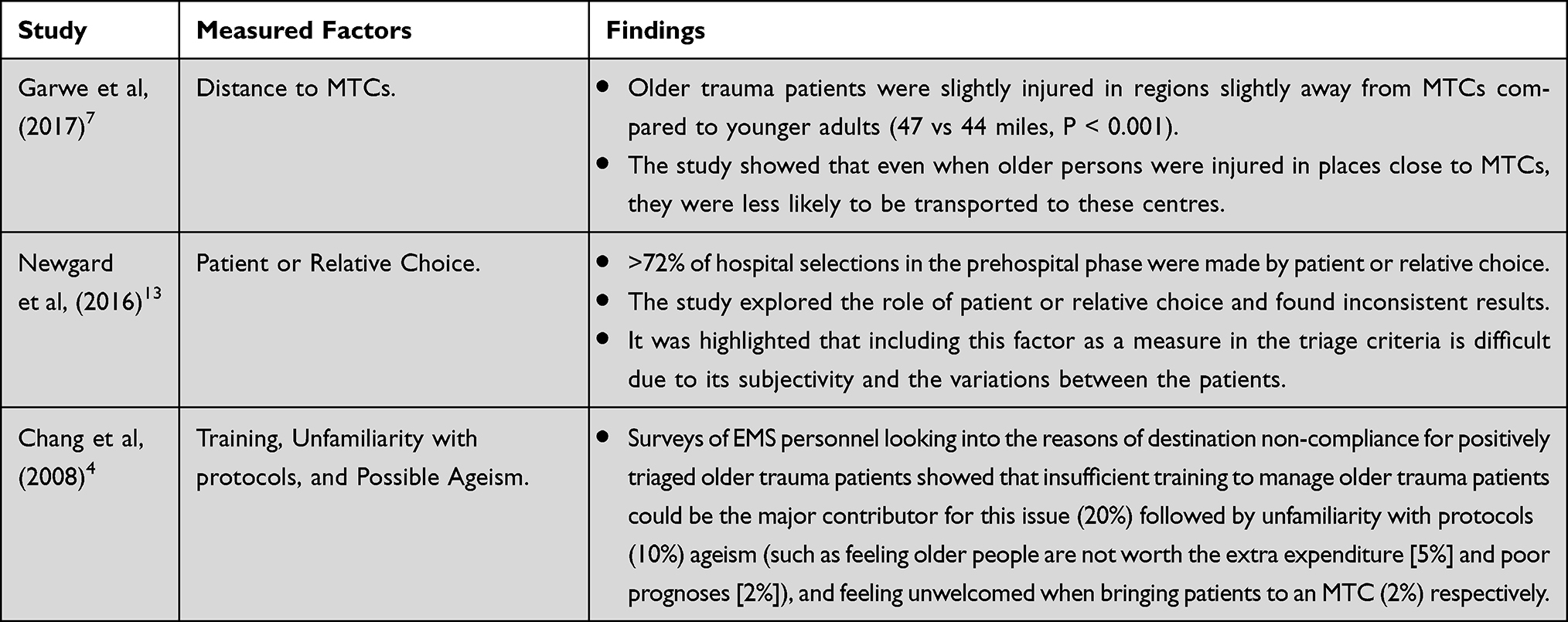 |
Table 4 Assessment of Other Factors Not Related to Prehospital Trauma Triage Criteria |
The Future
- There is a paucity of information, worldwide, on the use of frailty assessment tools by paramedics and trauma outcomes in older people. Therefore, further efforts in future research are required to assess the feasibility and validity of frailty assessment for use in the prehospital environment.
- More studies are also required to assess the benefits of access to MTCs for older trauma patients.
- Appropriate patient- and clinician-reported, short-term and long-term outcome measures would also need to be determined for older trauma patients.
- It seems that there are other factors such as distance to MTCs, patient or relative choice, training, unfamiliarity with protocols, and possible ageism that affect prehospital triage of older trauma patients which require further investigation and assessment.
- More focus is also needed to ensure that EMS personnel have adequate education and training to assess and treat older trauma patients and be more familiar with their protocols.
- Overall, future research in this field could significantly improve prehospital triage decisions and the transition of care from prehospital to in-hospital setting which could, consequently, reduce patients’ complications and improve their quality of life and healthcare use and experience.
Conclusion
Prehospital care of older trauma patients represents a major part of the EMS service. This includes accurate identification and triage of this population followed by appropriate transportation to a designated facility. Prehospital triage criteria were found to be inaccurate in identifying high-risk older trauma patients. Applying other assessment tools, such as frailty identification, could be helpful. Furthermore, determining the appropriate outcome measures for older trauma patients and the benefits that they can get from their access to MTCs could improve triage and appropriate prehospital transportation which, consequently, could be positively reflected on their outcomes. Moreover, investigating factors other than triage criteria that could impact prehospital destination compliance will enhance high-quality prehospital care for this population.
Abbreviations
USA, United States of America; TCs, Trauma Centers; AC, Acute Care; MTC, Major Trauma Centers; UK, United Kingdom; CFS, Clinical Frailty Scale; EMS, Emergency Medical Service; CP-CGA, Care Partner – Comprehensive Geriatric Assessment; CP-FI-CGA, Care Partner-derived Frailty Index based up on Comprehensive Geriatric Assessment; EFS, Edmonton Frail Scale; GFI, Groningen Frailty Index; GAC, Geriatric Ambulatory Care; HR, Hazard Ratio; CI, Confidence Interval; ED, Emergency Department; PERIL, Paramedic assessing Elders at Risk of Independence Loss; OR, Odds Ratio; AUC, Area Under the Curve; ISAR, Identifying Seniors at Risk; CCDS, Computerized Clinical Decision Support; CROM, Clinician Reported Outcome Measure; PROMs, Patient Reported Outcome Measures; LOS, Length of Stay; ISS, Injury Severity Score; SF-36, 36-item Short Form survey; ICU, Intensive Care Unit; SD, Standard Deviation; ADL, Activities of Daily Living; ISADL, Independency Scale of Activities of Daily Living; SFS, Short Functional Status questionnaire; CCI, Charlson Comorbidity Index; GOS, Glasgow Outcome Scale; IQR, Interquartile Range; ICISS, International Classification of Diseases Injury Severity Scale; ICD-9CM, International Classification of Diseases, Ninth Revision, Clinical Modification; AIS, Abbreviated Injury Scale; RR, Relative Risk; GCS, Glasgow Coma Scale.
Ethics Approval and Informed Consent
This article does not contain any studies with human participants or animals performed by any of the authors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, literature review, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
AA is funded by King Saud bin Abdulaziz University for Health Sciences, Riyadh, Saudi Arabia. The role of this funding is to publish the study as open access.
Disclosure
Professor Simon Conroy reports the receipt of NIHR grant funding to study emergency care. The authors declare that they have no other competing interests.
References
1. United Nations, Department of Economic and Social Affairs, Population Division. World Population Ageing 2015 (ST/ESA/Ser.a/390). New York: United Nations; 2015.
2. Trauma Trunkey D. Accidental and intentional injuries account for more years of life lost in the U.S. than cancer and heart disease. Among the prescribed remedies are improved preventive efforts, speedier surgery and further research. Sci Am. 1983;249(2):28–35.
3. Brown E, Tohira H, Bailey P, Fatovich D, Pereira G, Finn J. Older age is associated with a reduced likelihood of ambulance transport to a trauma centre after major trauma in Perth. Emerg Med Australas. 2019;31(5):763–771. doi:10.1111/1742-6723.13244
4. Chang DC, Bass RR, Cornwell EE, MacKenzie EJ. Undertriage of elderly trauma patients to state-designated trauma centers. Arch Surg. 2008;143(8):776–781. doi:10.1001/archsurg.143.8.776
5. Cox S, Morrison C, Cameron P, Smith K. Advancing age and trauma: triage destination compliance and mortality in Victoria, Australia. Injury. 2014;45(9):1312–1319. doi:10.1016/j.injury.2014.02.028
6. Davis JS, Allan BJ, Sobowale O, Ivascu F, Orion K, Schulman CI. Evaluation of a new elderly trauma triage algorithm. South Med J. 2012;105(9):447–451. doi:10.1097/SMJ.0b013e318261f6f4
7. Garwe T, Stewart K, Stoner J, et al. Out-of-hospital and inter-hospital under-triage to designated tertiary trauma centers among injured older adults: a 10-year statewide geospatial-adjusted analysis. Prehosp Emerg Care. 2017;21(6):734–743. doi:10.1080/10903127.2017.1332123
8. Ichwan B, Darbha S, Shah MN, et al. Geriatric-specific triage criteria are more sensitive than standard adult criteria in identifying need for trauma center care in injured older adults. Ann Emerg Med. 2015;65(1):92–100. doi:10.1016/j.annemergmed.2014.04.019
9. Kodadek LM, Selvarajah S, Velopulos CG, Haut ER, Haider AH. Undertriage of older trauma patients: is this a national phenomenon? J Surg Res. 2015;199(1):220–229. doi:10.1016/j.jss.2015.05.017
10. Lehmann R, Beekley A, Casey L, Salim A, Martin M. The impact of advanced age on trauma triage decisions and outcomes: a statewide analysis. Am J Surg. 2009;197(5):571–575. doi:10.1016/j.amjsurg.2008.12.037
11. Meyers MH, Wei TL, Cyr JM, et al. The triage of older adults with physiologic markers of serious injury using a state-wide prehospital plan. Prehosp Disaster Med. 2019;34(5):497–505. doi:10.1017/S1049023X19004825
12. Nakamura Y, Daya M, Bulger EM, et al. Evaluating age in the field triage of injured persons. Ann Emerg Med. 2012;60(3):335–345. doi:10.1016/j.annemergmed.2012.04.006
13. Newgard CD, Holmes JF, Haukoos JS, et al. Improving early identification of the high-risk elderly trauma patient by emergency medical services. Injury. 2016;47(1):19–25. doi:10.1016/j.injury.2015.09.010
14. Newgard CD, Lin A, Eckstrom E, et al. Comorbidities, anticoagulants, and geriatric-specific physiology for the field triage of injured older adults. J Trauma Acute Care Surg. 2019;86(5):829–837. doi:10.1097/TA.0000000000002195
15. Staudenmayer KL, Hsia RY, Mann NC, Spain DA, Newgard CD. Triage of elderly trauma patients: a population-based perspective. J Am Coll Surg. 2013;217(4):569–576. doi:10.1016/j.jamcollsurg.2013.06.017
16. Rotondo M, Cribari C, Smith R; American College of Surgeons Committee on Trauma. Resources for Optimal Care of the Injured Patient. Vol. 6. Chicago, USA: American College of Surgeons; 2014.
17. Brown JB, Gestring ML, Forsythe RM, et al. Systolic blood pressure criteria in the National Trauma Triage Protocol for geriatric trauma: 110 is the new 90. J Trauma Acute Care Surg. 2015;78(2):352–359. doi:10.1097/TA.0000000000000523
18. Doherty TJ. Invited review: aging and sarcopenia. J Appl Physiol. 2003;95(4):1717–1727. doi:10.1152/japplphysiol.00347.2003
19. Ferrara N, Komici K, Corbi G, et al. β-adrenergic receptor responsiveness in aging heart and clinical implications. Front Physiol. 2014;4:396. doi:10.3389/fphys.2013.00396
20. Gerstenblith G, Frederiksen J, Yin F, Fortuin NJ, Lakatta EG, Weisfeldt ML. Echocardiographic assessment of a normal adult aging population. Circulation. 1977;56(2):273–278. doi:10.1161/01.CIR.56.2.273
21. Hedman AM, van Haren NE, Schnack HG, Kahn RS, Hulshoff Pol HE. Human brain changes across the life span: a review of 56 longitudinal magnetic resonance imaging studies. Hum Brain Mapp. 2012;33(8):1987–2002. doi:10.1002/hbm.21334
22. Janssen I, Heymsfield SB, Ross R. Low relative skeletal muscle mass (sarcopenia) in older persons is associated with functional impairment and physical disability. J Am Geriatr Soc. 2002;50(5):889–896. doi:10.1046/j.1532-5415.2002.50216.x
23. Sharma G, Goodwin J. Effect of aging on respiratory system physiology and immunology. Clin Interv Aging. 2006;1(3):253–260. doi:10.2147/ciia.2006.1.3.253
24. Xu X, Wang B, Ren C, et al. Age-related impairment of vascular structure and functions. Aging Dis. 2017;8(5):590–610. doi:10.14336/AD.2017.0430
25. Rickard F, Ibitoye S, Deakin H, et al. The Clinical Frailty Scale predicts adverse outcome in older people admitted to a UK major trauma centre. Age Ageing. 2020;2020:1–7.
26. O’Caoimh R, Costello M, Small C, et al. Comparison of frailty screening instruments in the emergency department. Int J Environ Res Public Health. 2019;16(19):3626. doi:10.3390/ijerph16193626
27. van Rein EA, van der Sluijs R, Raaijmaakers AM, Leenen LP, van Heijl M. Compliance to prehospital trauma triage protocols worldwide: a systematic review. Injury. 2018;49(8):1373–1380. doi:10.1016/j.injury.2018.07.001
28. Alshibani A, Banerjee J, Lecky F, et al. A consensus building exercise to determine research priorities for silver trauma. BMC Emerg Med. 2020;20(1):1–8. doi:10.1186/s12873-020-00357-4
29. Trauma Audit and Research Network (TARN). Major Trauma in Older People. Salford/United Kingdom; April 04, 2017:1.
30. Joosten E, Demuynck M, Detroyer E, Milisen K. Prevalence of frailty and its ability to predict in hospital delirium, falls, and 6-month mortality in hospitalized older patients. BMC Geriatr. 2014;14(1):1. doi:10.1186/1471-2318-14-1
31. Pecheva M, Phillips M, Hull P, O’Leary RCA, Queally J. The impact of frailty in major trauma in older patients. Injury. 2020;51(7):1536–1542. doi:10.1016/j.injury.2020.04.045
32. Curtis E, Romanowski K, Sen S, Hill A, Cocanour C. Frailty score on admission predicts mortality and discharge disposition in elderly trauma patients over the age of 65 y. J Surg Res. 2018;230:13–19. doi:10.1016/j.jss.2018.04.017
33. Joseph B, Pandit V, Zangbar B, et al. Superiority of frailty over age in predicting outcomes among geriatric trauma patients: a prospective analysis. JAMA Surg. 2014;149(8):766–772. doi:10.1001/jamasurg.2014.296
34. Sadarangani T, Squires A. Frailty as a predictive factor in geriatric trauma patient outcomes. J Clin Outcomes Manag. 2014;21(9):396–397.
35. Goldstein J, Hubbard RE, Moorhouse P, Andrew MK, Mitnitski A, Rockwood K. The validation of a care partner-derived frailty index based upon comprehensive geriatric assessment (CP-FI-CGA) in emergency medical services and geriatric ambulatory care. Age Ageing. 2015;44(2):327–330. doi:10.1093/ageing/afu161
36. Goldstein J, Travers A, Hubbard R, Moorhouse P, Andrew MK, Rockwood K. Assessment of older adults by emergency medical services: methodology and feasibility of a care partner Comprehensive Geriatric Assessment (CP-CGA). CJEM. 2014;16(5):370–383.
37. Harris W, Lucas PV, Eyles H, Parker L. Paramedic assessment of frailty: an exploratory study of perceptions of frailty assessment tools. Ir J Paramed. 2018;3(1):1–10. doi:10.32378/ijp.v3i1.80
38. Lee JS, Verbeek PR, Schull MJ, et al. Paramedics assessing Elders at Risk for Independence Loss (PERIL): derivation, reliability and comparative effectiveness of a clinical prediction rule. CJEM. 2016;18(2):121–132. doi:10.1017/cem.2016.14
39. Snooks HA, Carter B, Dale J, et al. Support and Assessment for Fall Emergency Referrals (SAFER 1): cluster randomised trial of computerised clinical decision support for paramedics. PLoS One. 2014;9(9):e106436. doi:10.1371/journal.pone.0106436
40. Smith PG, Morrow RH, Ross DA. Field Trials of Health Interventions: A Toolbox. OUP Oxford; 2015.
41. Moran CG, Lecky F, Bouamra O, et al. Changing the system-major trauma patients and their outcomes in the NHS (England) 2008–17. EClinicalMedicine. 2018;2:13–21. doi:10.1016/j.eclinm.2018.07.001
42. Akpan A, Roberts C, Bandeen-Roche K, et al. Standard set of health outcome measures for older persons. BMC Geriatr. 2018;18(1):36. doi:10.1186/s12877-017-0701-3
43. Gabbe BJ, Williamson OD, Cameron PA, Dowrick AS. Choosing outcome assessment instruments for trauma registries. Acad Emerg Med. 2005;12(8):751–758. doi:10.1197/j.aem.2005.03.527
44. Hoffman K, Cole E, Playford ED, Grill E, Soberg HL, Brohi K. Health outcome after major trauma: what are we measuring? PLoS One. 2014;9(7):e103082. doi:10.1371/journal.pone.0103082
45. Rosenberg GM, Stave C, Spain DA, Weiser TG. Patient-reported outcomes in trauma: a scoping study of published research. Trauma Surg Acute Care Open. 2018;3(1):e000202. doi:10.1136/tsaco-2018-000202
46. Sleat GK, Ardolino AM, Willett KM. Outcome measures in major trauma care: a review of current international trauma registry practice. Emerg Med J. 2011;28(12):1008–1012. doi:10.1136/emermed-2011-200326
47. Ardolino A, Sleat G, Willett K. Outcome measurements in major trauma—results of a consensus meeting. Injury. 2012;43(10):1662–1666. doi:10.1016/j.injury.2012.05.008
48. Koizia L, Kings R, Koizia A, et al. Major trauma in the elderly: frailty decline and patient experience after injury. Trauma. 2019;21(1):21–26. doi:10.1177/1460408618783221
49. Inaba K, Goecke M, Sharkey P, Brenneman F. Long-term outcomes after injury in the elderly. J Trauma Acute Care Surg. 2003;54(3):486–491. doi:10.1097/01.TA.0000051588.05542.D6
50. DeMaria EJ, Kenney PR, Merriam MA, Casanova LA, Gann DS. Aggressive trauma care benefits the elderly. J Trauma Acute Care Surg. 1987;27(11):1200–1206. doi:10.1097/00005373-198711000-00002
51. McKevitt EC, Calvert E, Ng A, et al. Geriatric trauma: resource use and patient outcomes. Can J Surg. 2003;46(3):211–215.
52. Ferrera PC, Bartfield JM, D’Andrea CC. Geriatric trauma: outcomes of elderly patients discharged from the ED. Am J Emerg Med. 1999;17(7):629–632. doi:10.1016/S0735-6757(99)90146-8
53. Carrillo EH, Richardson JD, Malias MA, Cryer H, Miller FB. Long term outcome of blunt trauma care in the elderly. Surg Gynecol Obstet. 1993;176(6):559–564.
54. Zietlow SP, Capizzi PJ, Bannon MP, Farnell MB. Multisystem geriatric trauma. J Trauma Acute Care Surg. 1994;37(6):985–988. doi:10.1097/00005373-199412000-00020
55. van der Sluis CK, Klasen H, Eisma W, Ten Duis H. Major trauma in young and old: what is the difference? J Trauma Acute Care Surg. 1996;40(1):78–82. doi:10.1097/00005373-199601000-00015
56. Oreskovich MR, Howard JD, Copass MK, Carrico CJ. Geriatric trauma: injury patterns and outcome. J Trauma. 1984;24(7):565–572. doi:10.1097/00005373-198407000-00003
57. Battistella FD, Din AM, Perez L. Trauma patients 75 years and older: long-term follow-up results justify aggressive management. J Trauma. 1998;44(4):618–624. doi:10.1097/00005373-199804000-00010
58. Day RJ, Vinen J, Hewitt-Falls E. Major trauma outcomes in the elderly. Med J Aust. 1994;160(11):675–678.
59. Kelley-Quon L, Min L, Morley E, Hiatt JR, Cryer H, Tillou A. Functional status after injury: a longitudinal study of geriatric trauma. Am Surg. 2010;76(10):1055–1058. doi:10.1177/000313481007601006
60. Alavi NM, Safa A, Abedzadeh-Kalahroudi M. Dependency in activities of daily living following limb trauma in elderly referred to shahid beheshti hospital, kashan-Iran in 2013. Arch Trauma Res. 2014;3(3):e20608.
61. van Aalst J, Morris JJ, Yates H, Miller R, Bass S. Severely injured geriatric patients return to independent living: a study of factors influencing function and independence. J Trauma. 1991;31(8):1096–1101. doi:10.1097/00005373-199131080-00008
62. Amoako J, Evans S, Brown NV, Khaliqdina S, Caterino JM. Identifying predictors of undertriage in injured older adults after implementation of statewide geriatric trauma triage criteria. Acad Emerg Med. 2019;26(6):648–656. doi:10.1111/acem.13695
63. Caterino JM, Brown NV, Hamilton MW, et al. Effect of geriatric-specific trauma triage criteria on outcomes in injured older adults: a statewide retrospective cohort study. J Am Geriatr Soc. 2016;64(10):1944–1951. doi:10.1111/jgs.14376
64. Phillips S, Rond PC, Kelly SM, Swartz PD. The failure of triage criteria to identify geriatric patients with trauma: results from the Florida Trauma Triage Study. J Trauma Acute Care Surg. 1996;40(2):278–283. doi:10.1097/00005373-199602000-00018
65. Garwe T, Stewart KE, Newgard CD, et al. Survival benefit of treatment at or transfer to a tertiary trauma center among injured older adults. Prehosp Emerg Care. 2020;24(2):245–256. doi:10.1080/10903127.2019.1632997
66. Meldon SW, Reilly M, Drew BL, Mancuso C, Fallon JW
67. Pracht EE, Langland-Orban B, Flint L. Survival advantage for elderly trauma patients treated in a designated trauma center. J Trauma Acute Care Surg. 2011;71(1):69–77. doi:10.1097/TA.0b013e31820e82b7
68. MacKenzie EJ, Rivara FP, Jurkovich GJ, et al. A national evaluation of the effect of trauma-center care on mortality. N Engl J Med. 2006;354(4):366–378. doi:10.1056/NEJMsa052049
69. Scheetz LJ. Differences in survival, length of stay, and discharge disposition of older trauma patients admitted to trauma centers and nontrauma center hospitals. J Nurs Scholarsh. 2005;37(4):361–366. doi:10.1111/j.1547-5069.2005.00062.x
70. Smith JS, Martin LF, Young WW, Macioce DP. Do trauma centers improve outcome over non-trauma centers: the evaluation of regional trauma care using discharge abstract data and patient management categories. J Trauma. 1990;30(12):1533–1538. doi:10.1097/00005373-199012000-00017
71. Alshibani A, Singler B, Conroy S. Towards improving prehospital triage for older trauma patients. Z Gerontol Geriatr. 2021. doi:10.1007/s00391-021-01844-4
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.