Back to Journals » International Journal of General Medicine » Volume 17
Neutrophil Lymphocyte Ratio Predicts Early Neurological Deterioration in Patients with Anterior Circulation Stroke
Authors Zhao L, Zhou S, Dai Q, Li J
Received 5 August 2024
Accepted for publication 8 November 2024
Published 16 November 2024 Volume 2024:17 Pages 5325—5331
DOI https://doi.org/10.2147/IJGM.S472316
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Woon-Man Kung
Lingling Zhao,1,* Shuyu Zhou,1,* Qiliang Dai,2 Junrong Li1
1Department of Neurology, The Affiliated Jiangning Hospital of Nanjing Medical University, Jiangning Clinical Medical School, Kangda College of Nanjing Medical University, Nanjing, People’s Republic of China; 2Department of Neurology, Jinling Hospital, Medical School of Nanjing University, Nanjing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Junrong Li, Department of Neurology, The Affiliated Jiangning Hospital of Nanjing Medical University,Jiangning Clinical Medical School, Kangda College of Nanjing Medical University, 169 Hushan Road, Nanjing, People’s Republic of China, 211100, Email [email protected]
Background: Early neurologic deterioration (END) in acute ischemic stroke could result in significant worsening of clinical prognosis. Neutrophil lymphocyte ratio (NLR) is related to stroke severity and might be a predictor of short-term mortality in acute ischemic stroke. This study investigated the relationship between NLR and END in anterior circulation stroke patients.
Methods: Consecutive patients with first-ever acute ischemic stroke admitted to hospital within 24-hour of symptom onset were analyzed. NLR was calculated according to the Laboratory parameters obtained during the first 24 hours after admission. The rate of the END was recorded during the first 72-hours of admission. Multivariate logistic regression was applied to investigate the relationship between NLR and END.
Results: We included 228 consecutive patients within 24-hours of symptom onset for the final analysis. In total, 64 (28.1%) experienced END during the first 72 hours after admission. Patients with END were more likely to have higher NLR (median NLR 3.8 vs 2.4; p< 0.001) compared with those without END. Multivariate logistic regression revealed that NLR> 2.65 (OR, 4.019; 95% CI, 1.937– 8.337; p< 0.001) was an independent predictor of END. Also, patients in high NLR subgroup (NLR> 2.65) at admission were more likely to have prolonged length of stays (median length of stays 12 vs 4; p< 0.001).
Conclusion: This study found NLR was an independent predictor of END in patients with anterior circulation stroke.
Keywords: neutrophil lymphocyte ratio, END, stroke
Introduction
END in patients with acute ischemic stroke could result in significant worsening of clinical prognosis. Several risk factors for END have been reported in previous studies, including age,1,2 female,3 stroke severity,2,4 internal carotid artery occlusion,2,3 leukocyte count,1,4 and C-Reactive Protein.3 In addition, patients with a history of atrial fibrillation,4 cigarette smoking,4 and heart failure1,2 were also related to END.
Brain tissue inflammation was a typical response to the vascular injury. It had been demonstrated that there was a causal relationship between the inflammatory response and stroke-induced brain dysfunction and tissue injury.5 Recent research suggested that inflammation was a possible mechanism leading to END.6 High neutrophil count in patients with acute stroke was related to stroke severity and poor prognosis at three months, while low lymphocyte count was predictive of poor neurologic improvement during the first week after admission.7 Neutrophil lymphocyte ratio (NLR) was related to stroke severity and might be a predictor of short-term mortality in acute ischemic stroke.8–10 Moreover, NLR was independently associated with the severity of coronary artery disease and progression of atherosclerosis in patients undergoing angiography.11,12
Whether high NLR independently predicts END, has not been reported. Therefore, the objective of the present study was to identify the possible relationship between NLR and END in patients with acute infarct of anterior circulation.
Methods
Patients
Consecutive patients with first-ever acute ischemic stroke who were admitted to Jinling hospital within 24-hours of symptom onset were analyzed. Acute ischemic stroke was diagnosed if there were new focal neurologic deficits explained by relevant lesions detected on diffusion weighted image (DWI) or computed tomography (CT). Subjects with anterior circulation infarction were eligible for inclusion. The exclusion criteria included patients who were (1) diagnosed with infection 72 hours pre or post admission, (2) presently using corticosteroids or other immunosuppressive drugs, (3) diagnosed with cancer or immune system disease, and (4) with incomplete medical records.
Demographic and Clinical Data Collection
The baseline data were collected from case database: demographic data (age and sex); vascular risk factors (hypertension, diabetes mellitus, hypercholesterolemia, atrial fibrillation, cigarette smoking, alcohol drinking, coronary heart disease and myocardial infarction); vital signs (blood pressure); time from stroke onset to admission; duration of hospitalization; laboratory parameters (total white blood cell count and subtypes, total cholesterol, LDL-cholesterol, HDL-cholesterol, triglycerides, creatinine, serum glucose, albumin, and hematocrit). Laboratory parameters were analyzed from fasting blood samples obtained during the first 24 hours after admission. NLR was calculated as the ratio of neutrophil count to lymphocyte count. Etiological classification of stroke was determined according to the Trial of Org 10172 in Acute Stroke Treatment (TOAST) criteria.13 The NIHSS scores were recorded by experienced neurologists immediately after admission, at 72h after hospitalization, and on discharge. Functional impairment was evaluated using the modified Rankin Scale (mRS) on discharge.
Treatment and Neurological Assessment
During the stay in hospital, patients treated with tissue plasminogen activator (tPA) or endovascular therapy were excluded. Guideline-based treatments14 were taken in the enrolled subjects. Other treatments such as expectant treatment and management of cardiovascular risk factors were implemented, as appropriate. We defined END as an increase of ≥2 points in the National Institutes of Health Stroke Scale (NIHSS) score after 72-hours of admission.
Ethics Statement and Patient Consents
The study was approved by the Clinical Trials Ethics Committee of Jinling Hospital. The guidelines outlined in the Declaration of Helsinki were followed. Informed consent was obtained from each of the study participants or their authorized delegators.
Statistical Analysis
Continuous data were presented as mean ± standard deviation (SD) or median value with interquartile ranges (IQR), and were evaluated using student t test or Mann–Whitney U-test. Categorical data were expressed as frequencies and percentage, and were assessed using chi-square test or Fisher exact test, as appropriate. Stepwise forward conditional process was applied on the multiple logistic regression model to analyze the correlation between the presence of END and other covariates. The results were expressed as odds ratios (OR) with 95% confidence intervals (CI). Receiver operating curve (ROC) analysis was drawn to calculate the optimal cut-off values of NLR to predict END. A 2-sided P<0.05 was considered statistically significant.
Results
A total of 228 consecutive patients were included in the analysis. The mean age was 61 years, of whom 67% were male. 64 (28.1%) experienced END during the first 72 hours after admission according to the definition. Two patients with END were dead during hospitalization. The median of the difference between the admission NIHSS score and 72 hours NIHSS score was 2 (IQR, 2 to 3) in the END group. Table 1 summarized the demographic and clinical characteristics in patients with END and without END. END was associated with systolic blood pressure, HDL-cholesterol level, serum glucose, neutrophil counts, lymphocyte counts, NLR and stroke severity at admission. NIHSS score at admission was significantly higher in patients with END than patients without END (median NIHSS score 5 vs 4; p=0.011). Subjects with END were more likely to have higher NLR (median NLR 3.8 vs 2.4; p<0.001), higher neutrophil counts (median neutrophil counts 5.3 vs 4.4; p=0.006), and lower lymphocyte counts (mean lymphocyte counts 1.6 vs 1.9; p=0.006) compared with subjects without END.
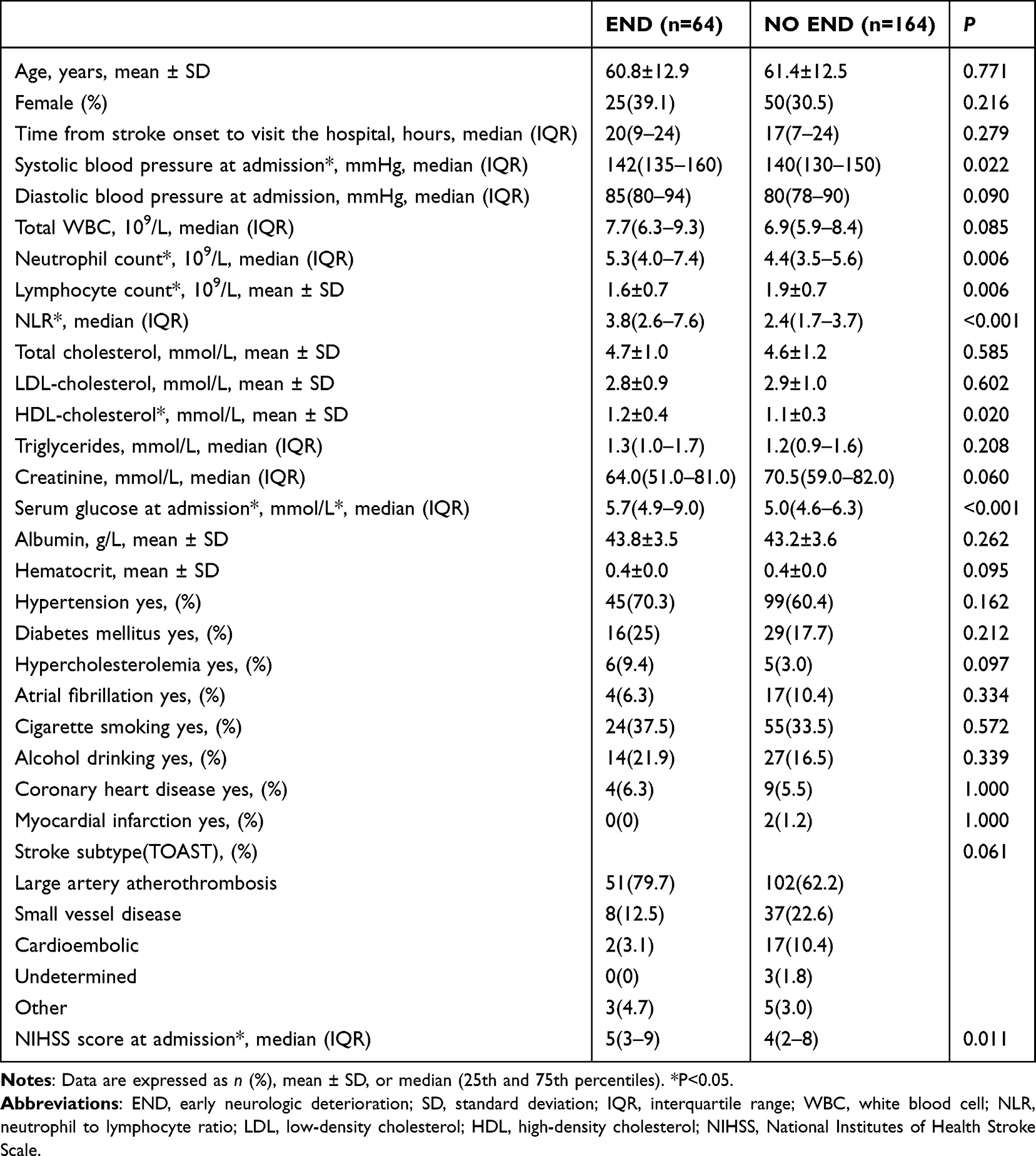 |
Table 1 Demographic Information and Clinical Characteristics |
Age, sex, and variables that were statistically significant (p<0.05) in univariate analyses were performed as covariates in multivariate logistic regression analysis. NLR was included in the logistic regression model as a dichotomous variable (above median, >2.65; below or equal to the median, ≤2.65), and NIHSS score at admission was also determined as a dichotomous variable (above median, >4; below or equal to the median, ≤4).
Multivariate logistic regression analysis revealed that NLR>2.65 (OR, 4.019; 95% CI, 1.937–8.337; p<0.001) HDL-cholesterol (OR, 3.140; 95% CI, 1.066–9.247; p=0.038) and serum glucose at admission (OR, 1.178; 95% CI, 1.021–1.359; p=0.025) were independent predictors of END (Table 2). Patients with a NLR>2.65 were almost 4 times more likely to develop END than patients with NLR≤2.65. In the ROC curve, the optimal cut-off value for NLR was determined as 2.68 to predict END with sensitivity of 75% and specificity of 60.98% (area under the ROC curve, 0.72; 95% CI, 0.657–0.777; P <0.001) (Figure 1).
 |
Table 2 Logistic Regression Model to Predict END |
 |
Figure 1 Receiver operating curves (ROC) of neutrophil lymphocyte ratio (NLR) to predict early neurologic deterioration (END) in patients with anterior circulation Stroke. |
We divided the study population into two group (high NLR group and low NLR group) based on the median (2.65) of NLR, finding that the patients in high NLR subgroup (NLR>2.65) at admission were more likely to have prolonged length of stays (median length of stays 12 vs 4; p<0.001), while patients in low NLR subgroup (NLR≤2.65) had a relationship with favorable outcome at discharge (MRS 0–2) (the percentage of patients in favorable outcome at discharge 80.7% vs 52.6%; p<0.001) (Table 3).
 |
Table 3 Short-Term Outcome Characteristics |
Discussion
The study found that NLR was an independent predictor of END in patients with anterior circulation stroke. Moreover, NLR>2.68 was determined to be an optimal cut-off value to predict END. As to the definition of END, different studies have used different diagnostic criteria and timeframes, resulting in inconsistent incidence rates and associated factors. The incidence of END in patients with ischemic stroke varies widely (13–37%).15 Present study showed END was presented in 28.1% of patients with anterior circulation stroke. In the study of patients with posterior circulation acute ischemic stroke, total white blood cell count (p=0.132) and NLR (p=0.863) were not significantly associated with END. It may be due to inappropriate assessment of the spectrum of posterior circulation-related neurologic deficits, using NIHSS score.16 Therefore, our study chose the subjects with anterior circulation lesion as inclusion criteria.
Inflammatory response was thought to be implicated in all stages of ischemic stroke, from brain cell necrosis of the early stage triggered by the interruption of blood supply, to the recovery and repair of post-ischemic tissue of the late stage. The inflammatory response to cerebral injury region resulted in the evolution of ischemic brain injury and the deterioration of neurological function.17 Through different approaches, as a marker of systemic inflammation, leukocytes further aggravated ischemic cerebral tissue injury.18 Neutrophils initially infiltrated ischemic brain at about 6–12 hours post-ischemia, while lymphocyte recruitment in the ischemic brain was relatively late, occurring within 3 to 6 days in stroke model.18 Lymphocytes play a protective role by releasing anti-inflammatory cytokines and repairing the inflamed tissues, at the same time they play a deleterious role associated with the development of inflammation, and different subtypes of lymphocytes play a different role in response to cerebral ischemia.18,19 Clinical evidence confirmed that early higher leukocytes and neutrophil counts were associated with larger infarct volumes and increased stroke severity in early stage of ischemia.20 In several studies, leukocytes had been found to be related with END in acute stroke patients.4,21 However, this relationship was not found in other studies.3,22 In our study, there was not a statistically significant relationship between leukocytes and END. Kim et al7 showed that patients with lower lymphocyte counts were more likely to have less improvement of neurological function during the first week after admission and worse long-term functional outcome. While studies on the evaluation of neutrophils and lymphocytes were insufficient, as an indicator of systemic inflammation,23 NLR integrated the information of two different and important immuno-inflammatory responses, and was more predictive than either parameter alone. Recently, studies have found the important role of NLR in predicting clinical prognosis in acute ischemic stroke.9,10 High NLR increased the size of infarct independent from the etiology,24 which may be associated with stroke severity and poor short-term clinical outcome.
In multiple logistic regression models with a stepwise forward conditional process, we respectively replaced NLR>2.65 with neutrophil count and lymphocyte count to predict END. We found that neutrophil count and lymphocyte count were not independent predictors of END. Systolic blood pressure at admission has been found to be associated with increased risk of progressing stroke.22 This was confirmed in our study. Systolic blood pressure in patients with END was higher than patients without END (median systolic blood pressure 142mmHg vs 140mmHg, p=0.022). We found high serum glucose level at admission was an independent risk of END in accordance with previous studies.2 It has been demonstrated that admission stress hyperglycemia was related to poor outcome after an ischemia stroke through exacerbation of cerebral ischemia damage.25 Contrary to our expectations, high levels of HDL-cholesterol was identified as a predictor of END. Using the same definition of END, Woo-Keun Seo3 obtained the consistent result. Woo-Keun Seo3 speculated that acute brain infarction contributed to an acute phase response, then converted HDL-cholesterol from anti-inflammatory to proinflammatory and can be associated with END, or the association might be a chance event. The HDL-cholesterol may link to the use of statin. Statin not only influence the lipid profile but also has a local anti-inflammatory effect. Also, statin withdrawal and adherence is associated with stroke outcomes.26 Although all patients were treated with statin after admission, data regarding statin use before admission was not analyzed in our study. This limitation should be noticed and may lead to further study. Several studies confirmed NIHSS score at admission could predict END,2,21,27 but not all.1,3,28,29 The risk of END associated with greater admission NIHSS score may be due to the consistency between NIHSS score and infarct volume, which was associated with great risk of developing edema in patients with acute stroke.2 In univariate logistic regression analysis, NIHSS score >4 (median NIHSS score) was an independent risk of END (OR, 1.993; 95% CI, 1.106–3.593; p=0.022). However, after adjusting for age, female, HDL-cholesterol, serum glucose, NLR, and systolic blood pressure at admission, we did not find NIHSS score >4 at admission was predictive of END.
Our study also had several limitations. First, the exact increase of the National Institutes of Health Stroke Scale (NIHSS) score to evaluate END is under discussion. At least one study recommended NIHSS score by ≥2 points as a sensitive indicator of death and major disability. There is no common consensus on the exact definition of END. The widely used definition is an increase of ≥2 or 4 points in NIHSS score after 48–120 hours of admission.15,30 In our study, we defined END as an increase of ≥2 points in NIHSS score after 72-hours of admission. The difference on the definition of END may lead to different results. Second, the data were collected from a retrospective stroke registry, and the limited number of study subjects may be subject to bias. Finally, several risks of END were not analyzed, such as the size of cerebral infarction area. Hence, large sample analysis and multi-center studies are needed to further explore the relationship between NLR and END.
In conclusion, NLR at admission was independently associated with END in patients with acute ischemic stroke of anterior circulation lesion. As an inexpensive and easy to obtain biomarker, NLR may serve as a clinically practical indicator for assessing risks of END after acute infarction.
Funding
This study was supported by Science Foundation of Kangda College of Nanjing Medical University (KD2022KYJJZD080) and Science Foundation of Nanjing Medical University (NMUB20220160).
Disclosure
Part of the data has been published as an abstract for Poster Presentations on the Asia Pacific Stroke Conference 2017. The study is also available on ResearchSquare. (https://www.researchgate.net/publication/321808744_DIFFUSION_TENSOR_IMAGING_IN_STROKE_FOLLOW_UP_OVER_1_YEAR_PRELIMINARY_STUDY). The authors report no conflicts of interest in this work.
References
1. Lin L-C, Lee T-H, Chang C-H, et al. Predictors of clinical deterioration during hospitalization following acute ischemic stroke. Eur Neurol. 2011;67(3):186–192. doi:10.1159/000334723
2. Siegler JE, Boehme AK, Kumar AD, et al. Identification of modifiable and nonmodifiable risk factors for neurologic deterioration after acute ischemic stroke. J Stroke Cerebrovascular Dis. 2013;22(7):e207–e13. doi:10.1016/j.jstrokecerebrovasdis.2012.11.006
3. Seo W-K, Seok H-Y, Kim JH, et al. C-reactive protein is a predictor of early neurologic deterioration in acute ischemic stroke. J Stroke Cerebrovascular Dis. 2012;21(3):181–186. doi:10.1016/j.jstrokecerebrovasdis.2010.06.002
4. Kwan J, Hand P. Early neurological deterioration in acute stroke: clinical characteristics and impact on outcome. Qjm. 2006;99(9):625–633. doi:10.1093/qjmed/hcl082
5. Rodrigues S, Granger D. Leukocyte-mediated tissue injury in ischemic stroke. Curr Med Chem. 2014;21(19):2130–2137. doi:10.2174/0929867321666131228192119
6. Serena J, Rodriguez-Yanez M, Castellanos M. Deterioration in acute ischemic stroke as the target for neuroprotection. Cerebrovascular Dis. 2006;21(Suppl 2):80–88. doi:10.1159/000091707
7. Kim J, Song T-J, Park JH, et al. Different prognostic value of white blood cell subtypes in patients with acute cerebral infarction. Atherosclerosis. 2012;222(2):464–467. doi:10.1016/j.atherosclerosis.2012.02.042
8. Gökhan S, Özhasenekler A, Durgun HM, Akil E, Üstündag M, Orak M. Neutrophil lymphocyte ratios in stroke subtypes and transient ischemic attack. Age. 2013;67:
9. Tokgoz S, Kayrak M, Akpinar Z, Seyithanoğlu A, Güney F, Yürüten B. Neutrophil lymphocyte ratio as a predictor of stroke. J Stroke Cerebrovascular Dis. 2013;22(7):1169–1174. doi:10.1016/j.jstrokecerebrovasdis.2013.01.011
10. Celikbilek A, Ismailogullari S, Zararsiz G. Neutrophil to lymphocyte ratio predicts poor prognosis in ischemic cerebrovascular disease. J Clin Lab Analysis. 2014;28(1):27–31. doi:10.1002/jcla.21639
11. Arbel Y, Finkelstein A, Halkin A, et al. Neutrophil/lymphocyte ratio is related to the severity of coronary artery disease and clinical outcome in patients undergoing angiography. Atherosclerosis. 2012;225(2):456–460. doi:10.1016/j.atherosclerosis.2012.09.009
12. Kalay N, Dogdu O, Koc F, et al. Hematologic parameters and angiographic progression of coronary atherosclerosis. Angiology. 2012;63(3):213–217. doi:10.1177/0003319711412763
13. Adams HP, Bendixen BH, Kappelle LJ, et al. Classification of subtype of acute ischemic stroke. definitions for use in a multicenter clinical trial. TOAST. trial of org 10172 in acute stroke treatment. Stroke. 1993;24(1):35–41. doi:10.1161/01.STR.24.1.35
14. Adams HP, Del Zoppo G, Alberts MJ, et al. Guidelines for the early management of adults with ischemic stroke a guideline from the American Heart Association/American Stroke Association Stroke Council, clinical cardiology council, cardiovascular radiology and intervention council, and the atherosclerotic peripheral vascular disease and quality of care outcomes in research interdisciplinary working groups: the American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Circulation. 2007;115(20):e478–e534. doi:10.1161/CIRCULATIONAHA.107.181486
15. Thanvi B, Treadwell S, Robinson T. Early neurological deterioration in acute ischaemic stroke: predictors, mechanisms and management. Postgraduate Medical Journal. 2008;84(994):412–417. doi:10.1136/pgmj.2007.066118
16. Lee JH, Han SJ, Yun YH, et al. Posterior circulation ischemic stroke in Korean population. Eur J Neurol. 2006;13(7):742–748. doi:10.1111/j.1468-1331.2006.01274.x
17. Chamorro A, Hallenbeck J. The harms and benefits of inflammatory and immune responses in vascular disease. Stroke. 2006;37(2):291–293. doi:10.1161/01.STR.0000200561.69611.f8
18. Kim JY, Kawabori M, Yenari MA. Innate inflammatory responses in stroke: mechanisms and potential therapeutic targets. Curr Med Chem. 2014;21(18):2076–2097. doi:10.2174/0929867321666131228205146
19. Jin R, Yang G, Li G. Inflammatory mechanisms in ischemic stroke: role of inflammatory cells. Journal of Leukocyte Biology. 2010;87(5):779–789. doi:10.1189/jlb.1109766
20. Buck BH, Liebeskind DS, Saver JL, et al. Early neutrophilia is associated with volume of ischemic tissue in acute stroke. Stroke. 2008;39(2):355–360. doi:10.1161/STROKEAHA.107.490128
21. Miyamoto N, Tanaka Y, Ueno Y, et al. Demographic, clinical, and radiologic predictors of neurologic deterioration in patients with acute ischemic stroke. J Stroke Cerebrovascular Dis. 2013;22(3):205–210. doi:10.1016/j.jstrokecerebrovasdis.2011.07.018
22. Barber M, Wright F, Stott DJ, Langhorne P. Predictors of early neurological deterioration after ischaemic stroke: a case-control study. Gerontology. 2003;50(2):102–109. doi:10.1159/000075561
23. Imtiaz F, Shafique K, Mirza SS, Ayoob Z, Vart P, Rao S. Neutrophil lymphocyte ratio as a measure of systemic inflammation in prevalent chronic diseases in Asian population. Int Arch Med. 2012;5(1):2. doi:10.1186/1755-7682-5-2
24. Ertaş G, Sönmez O, Turfan M, et al. Neutrophil/lymphocyte ratio is associated with thromboembolic stroke in patients with non-valvular atrial fibrillation. J Neurol Sci. 2013;324(1):49–52. doi:10.1016/j.jns.2012.09.032
25. Luitse MJ, Biessels GJ, Rutten GE, Kappelle LJ. Diabetes, hyperglycaemia, and acute ischaemic stroke. Lancet Neurol. 2012;11(3):261–271. doi:10.1016/S1474-4422(12)70005-4
26. Vitturi BK, Gagliardi RJ. The influence of statin withdrawal and adherence on stroke outcomes. Neurol Sci. 2021;42(6):2317–2323. doi:10.1007/s10072-020-04790-y
27. Lin LC, Yang J, Weng H, Hsiao C, Lai SL, Fann W. Predictors of early clinical deterioration after acute ischemic stroke. Am J Emergency Med. 2011;29(6):577–581. doi:10.1016/j.ajem.2009.12.019
28. Ntaios G, Lambrou D, Cuendet D, Michel P. Early major worsening in ischemic stroke: predictors and outcome. Neurocritical Care. 2013;19(3):287–292. doi:10.1007/s12028-013-9865-7
29. Kwon H-M, Lim J-S, Park H-K, Lee Y-S. Hypertriglyceridemia as a possible predictor of early neurological deterioration in acute lacunar stroke. J Neurol Sci. 2011;309(1):128–130. doi:10.1016/j.jns.2011.06.057
30. Siegler JE, Martin-Schild S. Early neurological deterioration (END) after stroke: the END depends on the definition. Int J Stroke. 2011;6(3):211–212. doi:10.1111/j.1747-4949.2011.00596.x
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.