Back to Journals » Neuropsychiatric Disease and Treatment » Volume 14
Neuropsychiatric assessments in patients with multiple sclerosis in early phases and with low disability
Authors Schmidt SL ![]() , Santos da Silva M, Schmidt JJ, Carvalho ALN, Vasconcelos CCF
, Santos da Silva M, Schmidt JJ, Carvalho ALN, Vasconcelos CCF ![]() , Paes RA, Boechat YEM
, Paes RA, Boechat YEM ![]() , Neder R, Alvarenga RP
, Neder R, Alvarenga RP
Received 23 January 2018
Accepted for publication 11 April 2018
Published 22 June 2018 Volume 2018:14 Pages 1665—1670
DOI https://doi.org/10.2147/NDT.S163480
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Roger Pinder
Sergio L Schmidt,1,2 Michele Santos da Silva,2 Juliana J Schmidt,2 Ana Lucia Novais Carvalho,3 Claudia Cristina Ferreira Vasconcelos,2 Renata Alves Paes,2 Yolanda EM Boechat,4 Rafael Neder,2 Regina P Alvarenga2
1Department of Neurophysiology, State University of Rio de Janeiro, RJ, Brazil; 2Neurology Department, Federal University of the State of Rio de Janeiro, RJ, Brazil; 3Department of Psychology, Fluminense Federal University, Niteroi, Brazil; 4Department of Internal Medicine, Fluminense Federal University, Niteroi, Brazil
Background: In the early phases of multiple sclerosis (MS), patients exhibit slight neuropsychiatric deficits that can only be detected using reliable tools.
Aim: The present investigation aimed to examine neuropsychological performance in 35 patients with incipient MS.
Patients and methods: For the MS group, the inclusion criteria included time of disease <3 years and low disability. The neuropsychological battery consisted of Rey Auditory Learning Test, Controlled Oral Word Association Test, Hooper Visual Organization Test, and Symbol Digit Modalities Test (SDMT).
Results: After correction for the educational level, no significant effect of MS on performance was found for all the tests except for the number of errors of the SDMT (NE-SDMT). Higher levels of education were associated with better performances in all tests, except for the NE-SDMT. MS patients made more errors than the controls.
Conclusion: The effect on the NE-SDMT may reflect difficulties in the ability to inhibit inadequate responses. Patients may exhibit impulsive control disorders in incipient MS, independent of their educational level.
Keywords: processing speed, cognitive impairments, neuropsychology
Introduction
Multiple sclerosis (MS) is a chronic neurological disease associated with both white matter and cortical lesions.1 It is estimated that cognitive and psychiatric impairments affect up to 65% of patients with MS.2,3 For the evaluation of the neurologic disability, the Expanded Disability Status Scale (EDSS) is commonly used.4 Higher EDSS scores reflect central nervous system (CNS) dysfunctions and progressive walking impairments.4 However, the scale is insensitive to changes in cognitive and behavioral dysfunctions.5 Since the neuropsychological symptoms are not related to physical disability, it has been proposed that they can be used to evaluate disease progression despite stable physical symptoms.6,7 In this regard, Rao demonstrated the clinical utility of the brief repeatable battery of neuropsychological tests in patients with MS.8 Langdon et al recommended the Symbol Digit Modalities Test (SDMT) if only 5 minutes were available for the cognitive assessment.9 Benedict et al reinforced the use of the SDMT.10 More recently, it was suggested that assessing information processing speed could be easily and quickly evaluated with the SDMT in MS patients.11
It should be mentioned that studies about neuropsychiatric impairments in MS patients mostly come from North America and Western Europe.12 Previous studies in South America described the frequency and the clinical characteristics of MS patients in different countries, including Brazil.13,14 These studies have stressed the importance and the specificities of MS and related disorders in South America. Therefore, there is a need for clinically valid measures of cognitive and behavioral performance in this population. In this regard, previous investigations on the Brief International Cognitive Assessment for MS (BICAMS)15,16 have reported excellent test–retest reliability of the Portuguese16 and the Spanish12 translations of tests such as the SDMT. However, the neuropsychological profile of Brazilian MS patients is relatively unknown.17 Unfortunately, the clinical utility of these tests remains to be demonstrated in the incipient phases of MS especially in patients from Latin-American countries.
In the early phases of MS, the patients may exhibit slight deficits that can only be detected using valid and reliable assessment tools.18 In Latin America, there is an additional problem related to the possible effect of educational background on test performance because the grouping of subjects based on years of formal education is particularly difficult in Brazil and other Latin American countries. Indeed, years of education cannot be directly compared among the subjects unless they come from the same region of the country and have same socioeconomic status. In the present study, we used years of formal education as a cofactor because the MS patients and their relatives (control group) lived in the same region of the country. Therefore, MS patients and controls could be directly compared in terms of years of education.
As mentioned, cognitive impairments are frequent in MS patients. However, most studies of cognitive dysfunction examined MS patients in later stages. There are only a few studies of cognitive impairments in the early stages of MS, all of them done in North America and Europe. The cognitive performance of Latin American subjects may be particularly affected by cultural and socioeconomic variables. The present investigation aimed to examine the cognitive performance of Brazilian MS patients in the early stages of the disease and with low functional disability. A brief battery was used to verify which test variables were affected by the disease. Age, gender, and years of education were used as cofactors.
Patients and methods
The MS subjects were sampled from patients of a reference hospital for MS located in the city of Rio de Janeiro, Brazil. The comparison group (control) consisted of healthy subjects paired by gender, age, and years of formal education. An experienced neurologist, who was blinded to the neuropsychological findings, assessed disability using the EDSS scale. A clinical neuropsychologist, administered the neuropsychological battery for the two groups (MS and healthy control groups). For the MS group, the inclusion criteria were age >18 years, relapsing remitting MS (RRMS), time of disease <3 years, and EDSS ≤3; exclusion criteria were patients with other idiopathic demyelinating diseases, history or evidence of delusions or head trauma in the last year, uncorrected visual deficit, and motor abnormalities. The ethical review committee of the Federal University of the State of Rio de Janeiro approved the research protocol. All participants provided signed written informed consent.
All subjects had visual acuity equal to or better than 20/30 in both eyes (glasses were used when needed). Testing sessions were noninvasive and were carried out in a quiet room: only the subject and the examiner were allowed to stay in the room during the testing session. The test session took approximately 35 minutes to complete.
The neuropsychological battery consisted of the following tests: Rey Auditory Learning Test (RAVLT),19,20 Controlled Oral Word Association Test (COWAT),21,22 Hopper Visual Organization Test (VOT),23,24 and the SDMT.16,25
The inclusion of the SDMT is strongly recommended by several investigators.10 The selection of the other three tests took into consideration that a previous study showed that the profile of MS-related cognitive dysfunctions includes memory and learning deficits, attention deficits, executive dysfunctions and visuo-spatial deficits.11 Negreiros et al developed a neuropsychological battery to identify cognitive impairment in Brazilian patients with RRMS and concluded that the COWAT and the RAVLT had adequate sensitivity and specificity to discriminate RRMS patients from controls.17 Here, the visuo-spatial domain was assessed with the aid of the VOT, because this test was validated in Brazil.24
Nine variables were directly derived from the RAVLT (trials 1 to 5, immediate recall list B, trial 6, delayed recall or trial 7, and recognition of words). Regarding the COWAT, eight variables were directly measured: number of animals (na); number of fruits (nf); total category fluency (na+nf); words with the letters F, A, and S (nF, nA, and nS); total phonetic fluency (nF+nA+nS); total fluency (sum of the seven variables). For the VOT, one variable was used: number of correct responses. Finally, from the SDMT two variables could be directly derived from the test: number of correct responses and number of errors.
Multivariate analysis of covariance (MANCOVA) tests were conducted to verify if there were significant changes in performance on each test between MS group and the control group using gender, age, and years of formal education as covariates. Between-subjects factor: disease (two levels, MS and absence of disease). Dependent variables: defined for each neuropsychological test as explained above. When the MANCOVA showed a significant effect of disease, subsequent univariate tests were conducted to verify the effect of disease (MS) on each variable of the test. Sidak correction was applied for multiple comparisons. Significance was set at P≤0.05. For the MANCOVAs and for each one of the univariate ANCOVAS, η2 was computed to calculate the effect size of the results.
The relationship between years of education and the depending variables was analyzed with the aid of Person correlation coefficients (significance set at P<5%).
Results
We evaluated 35 patients, 80% females, aged between 21 years and 53 years old (mean age 35 years ± 8.8 years), time of onset of disease: 21.2 months ± 11.7 months, and 15.4 years ± 4.3 years of education. Among the 35 MS patients, seven were found to be using a specific drug indicated for the treatment of MS (three on interferon-β1a and four on glatiramer acetate), and the other 28 were not taking any medication at the time of the neuropsychological test. Controls were selected among patient’s relatives to match age, gender, and years of education (Table 1).
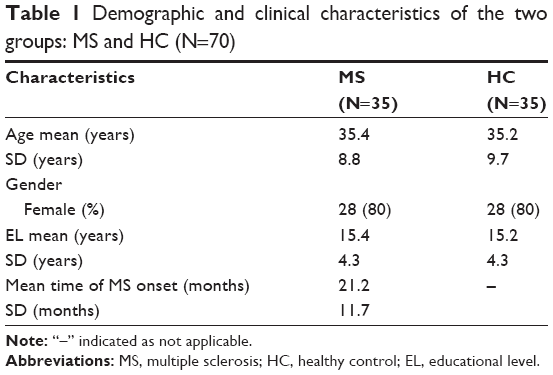 | Table 1 Demographic and clinical characteristics of the two groups: MS and HC (N=70) |
The MANCOVA(s) indicated that years of education reached significant levels for all the variables, except NE-SDMT (Table 2). In general, for all the variables the mean raw score of MS patients was found to be worse than the corresponding controls. For the RAVLT, VOT, and COWAT, the MANOVAS showed that there was no significant effect of MS on performance. In contrast, there was a significant effect of disease (MS vs controls) on performance of the SDMT (F=14.243, df=2/66, P=0.001, η2=0.301). The univariate tests (Table 3) showed a significant effect of disease (MS) on performance in the NE-SDMT (F=6.223 df=1/67, P<5%, η2=0.085). Analysis of the mean raw scores indicated that the MS patients made significantly more errors than the controls in the SDMT.
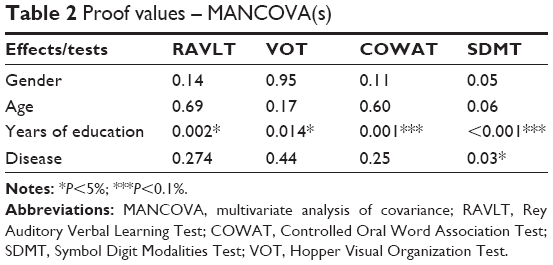 | Table 2 Proof values – MANCOVA(s) |
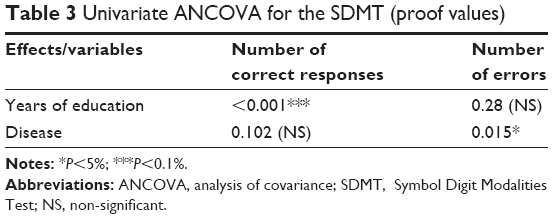 | Table 3 Univariate ANCOVA for the SDMT (proof values) |
Pearson’s correlation coefficients between years of formal education and performance (Table 4) reached significance for all the variables except for number of errors on the SDMT. For all the variables, the correlation coefficients indicate that a higher level of education is associated with a higher performance on the tests, except for the NE-SDMT.
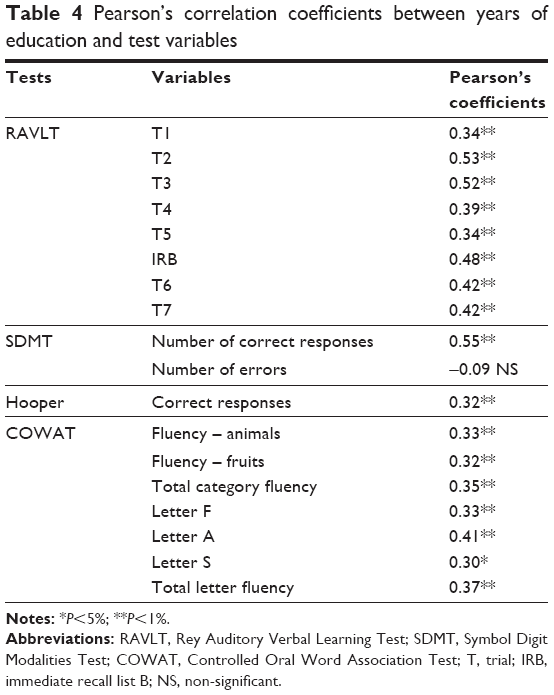 | Table 4 Pearson’s correlation coefficients between years of education and test variables |
Discussion
Among the four neuropsychological tests, only the SDMT was found to differ between MS patients and the controls after an adequate evaluation of level of education. The univariate analyses indicated that the number of correct answers on the SDMT did not differ between the controls and the MS patients. On the contrary, the number of errors on the SDMT reached significant levels. All variables of the four tests except the number of errors on the SDMT were found to be related to years of education. Higher education implied better performance in all variables except for the number of errors on the SDMT. There was a strong correlation between years of education and the number of correct answers on the SDMT in MS patients.
The finding here that deserves a more detailed explanation is the effect of years of education on cognitive performance in both controls and MS patients. Education level is a potential confounder of the performance in neuropsychological tests and thus normative data are needed to cope with different educational level. Educational level is commonly associated with years of formal education. In Brazil, the real meaning of years of formal education varies greatly across the different regions of the country: students in certain regions are required to attend school on a full-time basis, whereas in other regions of the country, the schools are only part-time. Thus, the same number of years of formal education does not necessarily indicate the same educational background across the country, since those in a full-time basis spent more time in the school as compared to those on a part-time basis even when they have the same number of years of education. Moreover, big social differences imply distinct types of schools for the rich and the poor people. In this regard, the variable denominated number of years does not adequately describe the true educational level when students from the richest areas of the country are compared to students attending public schools located in less favorable areas. The disparity reaches the university system. The ranking of the Brazilian Universities has an enormous deviation, and, again, the same years of graduate studies do not necessarily indicate the same level of formal education. For these reasons, norms based on years of education do not provide acceptable comparisons between controls and MS because most times these norms do not reflect the real educational background of the groups. It should be stressed that in the present study the controls were recruited using as many relatives of the patients as possible. This selected sample allowed us to use years of formal education as a cofactor. When adequately controlled for years of education, most of the tests did not show significant differences between controls and MS patients.
The data indicate that educational background may influence performance in a way that is stronger than the impact of the disease. This effect of the educational level obscured possible minor differences in performance between controls and patients. Our data disagree with a recent study conducted in Brazil by Spedo et al.16 These authors administered the Brazilian-Portuguese Brief International Cognitive Assessment for Multiple Sclerosis (BICAMS) test battery, which included the SDMT, the California Verbal Learning Test, and the Brief Visuospatial Memory Test-Revised. When controlling for age, gender, education, anxiety, and depression, they showed that MS patients differed against controls in all neuropsychological tests. One possible explanation, aside from our adequate control for educational level, might be the fact that we are working with incipient RRMS with low disability. Therefore, our sample was designed to capture subtle differences, and, consequently, only one subtest of the SDMT was able to detect the differences between patients and controls.
Among all test variables only the NE-SDMT was found to be significantly different between MS and controls. Although the number of errors is not commonly included as a variable in the SDMT, it is important to stress that it might be measuring an independent domain of attention. In analogy with the performance of attention deficits subjects in visual Continuous Performance Tests (CPTs), the number of errors might be related to the hyperactive/impulsivity domain of inattention.26–28 The present finding of an effect of the disease (MS) on the number of errors of the SDMT, in analogy with commission errors on CPT performance, reflects that MS patients with low disability exhibited significant impulse control problems. However, caution is necessary regarding the speculation that the effect on the errors of the SDMT is related to impulse control disorders because the SDMT was not designed to measure impulsivity. In fact, the SDMT evaluates information processing speed. Therefore, the number of correct responses is the only variable commonly considered for detecting cognitive abnormalities.
Previous investigators have reported that performance on complex processing tasks depends on the connectivity between the medial prefrontal cortex and the frontal poles in MS patients.29 Furthermore, cognitive performance has been found to be associated with frontal and parietal gray matter injury in RRMS patients.30 Considering the analogy between NE-SDMT and commission errors on visual CPTs, the same brain areas associated with performance on the CPTs may be affected in incipient MS. In this regard, a previous functional neuroimaging study using fluorodeoxyglucose positron emission tomography (FDG-PET) showed that the prefrontal and parietal cortices are activated during the performance of a visual attention test.31 Therefore, our data suggest that these cortical regions may be affected in MS patients with low disability.
Limitations
There are some limitations in the present study. First the sample size did not allow for the study of the effect of MS medication on the attentional performance. Further investigations with a larger sample are needed to address the question of treatments’ possible cognitive benefits. Another limitation is the absence of an adequate control of degree of depression. In RRMS patients, the prevalence of depression may reach 50%.3,32 Here, patients with major depression with psychotic symptoms were discarded. However, in the present study only one variable of the SDMT was affected in the MS patients. Therefore, it seems to be unlikely that even subclinical depression could bias only one variable of the SDMT. Further research is needed to include the effect of the disease over time and correlate the performance of the tests with the clinical data, the treatments, and the disability of the patients. In addition, it would be of interest to study the effect of education on the course of cognitive impairment. It should be stressed that this is a pilot study using all the variables derived from the tests. Each test was considered individually, and two tests seemed to be particularly important in the early phases of MS: SDMT and COWAT. Research using only psychologically meaningful variables is needed to confirm the hypothesis derived from this preliminary analysis.
Conclusion
Our data support that in the early phases of MS, patients may exhibit difficulties in the control of impulsive responses. However, the effect of the educational level on performance limits the use of most tests commonly administered in MS, at least in South American countries.
Acknowledgment
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
Kutzelnigg A, Lucchinetti CF, Stadelmann C, et al. Cortical demyelination and diffuse white matter injury in multiple sclerosis. Brain. 2005;128(Pt 11):2705–2712. | ||
McIntosh-Michaelis SA, Roberts MH, Wilkinson SM, et al. The prevalence of cognitive impairment in a community survey of multiple sclerosis. Br J Clin Psychol. 1991;30(Pt 4):333–348. | ||
Ghaffar O, Feinstein A. The neuropsychiatry of multiple sclerosis: a review of recent developments. Curr Opin Psychiatry. 2007;20(3):278–285. | ||
Kurtzke JF. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology. 1983;33(11):1444–1452. | ||
Chiaravalloti ND, DeLuca J. Cognitive impairment in multiple sclerosis. Lancet Neurol. 2008;7(12):1139–1151. | ||
Patti F. Treatment of cognitive impairment in patients with multiple sclerosis. Expert Opin Investig Drugs. 2012;21(11):1679–1699. | ||
Amato MP, Zipoli P. Clinical management of cognitive impairment in multiple sclerosis: a review of current evidence. Int MS J. 2003;10(3):72–83. | ||
Rao SM. A Manual for the Brief, Repeatable Battery of Neuropsychological Tests in Multiple Sclerosis. New York: National Multiple Sclerosis Society, 1991. Available from: www.nationalmssociety.org. Accessed January 23, 2018. | ||
Langdon DW, Amato MP, Boringa J, et al. Recommendations for a brief international cognitive assessment for multiple sclerosis (BICAMS). Mult Scler. 2012;18(6):891–898. | ||
Benedict RHB, DeLuca J, Phillpis G, et al. Validity of the symbol digit modalities test as a cognition performance outcome measure for multiple sclerosis. Mult Scler. 2017;23(5):721–733. | ||
Ruet A, Brochet B. Cognitive assessment in patients with multiple sclerosis: From neuropsychological batteries to ecological tools. Ann Phys Rehabil Med. Epub 2018 Feb 17. | ||
Vanotti S, Smerbeck A, Benedict RHB, Caceres F. A new assessment tool for patients with multiple sclerosis from Spanish speaking countries: Validation of the Brief International Cognitive Assessment for MS (BICAMS) in Argentina. Clin Neuropsychol. 2016;30(7):1023–1031. | ||
Papais-Alvarenga RM, Vasconcelos CC, Carra A, et al. Central nervous system idiopathic inflammatory demyelinating disorders in South Americans: A descriptive, multicenter, cross-sectional study. PLoS One. 2015;10:e0127757. | ||
Alvarenga MP, Schmidt S, Alvarenga RM. Epidemiology of neuromyelitis optica in Latin America. Mult Scler J Exp Transl Clin. 2017;3(3):1–8. | ||
Benedict RHB, Amato MP, Boringa J, et al. Brief International Cognitive Assessment for MS (BICAMS): International standards for validation. BMC Neurol. 2012;12:55. | ||
Spedo CT, Frndak SE, Marques VD, et al. Crosscultural adaptation, reliability, and validity of the BICAMS in Brazil. Clin Neuropsychol. 2015;29(6):836–846. | ||
Negreiros AA, Sousa-Munõz RL, Oliveira BE, Nobrega PV, Monteiro LL. Clinical and epidemiological profile of patients diagnosed with multiple sclerosis in João Pessoa, Paraíba, Brazil. Arq Neuropsiquiatr. 2015;73(9):741–745. | ||
Baysal KL, Ekmekçi Ö, Yüceyar N, Sagduyu Kocaman A. Assessment of early cognitive impairment in patients with clinically isolated syndromes and multiple sclerosis. Behav Neurol. Epub 2014 Apr 14. | ||
Wiens NA, McMinn MR, Crossen JR. Rey auditory-verbal learning test: development of norms for healthy young adults. Clin Neuropsychol.1988;2(1):67–87. | ||
Diniz LFM, Cruz MF, Torres VM, Cosenza RM. O teste de aprendizagem auditivo-verbal de Rey: normas para uma população brasileira. [Rey’s auditory-verbal learning test: norms for a Brazilian population]. Rev Bras Neurol. 2000;36(3):79–83. Portuguese. | ||
Tombaugh TN, Kozak J, Rees L. Normative data stratified by age and education for two measures of verbal fluency: FAS and animal naming. Arch Clin Neuropsychol. 1999;14(2):167–177. | ||
Brucki SMD, Malheiros SMF, Okamoto IH, Bertolucci PHF. Dados normativos para o teste de fluência verbal categoria animais em nosso meio. Arquivos de Neuro-Psiquiatria. 1997;55(1):56–61. | ||
Merten T. A short version of the Hooper Visual Organization Test: Development and validation. Clin Neuropsychol. 2002;16(2):136–144. | ||
Tosello DJT. Contribuição para o estudo normativo do Hooper Visual Organization Test (VOT). [Contribution to the normative study of the Hooper Visual Organization Test (VOT)]. Psicol Hosp. 2005;13(2):59–83. Portuguese. | ||
Smith A. Symbol Digit Modalities Test: Manual. Los Angeles, CA: Western Psychological Services, 1982. | ||
Schmidt SL, Simões EN, Novais Carvalho AL. Association between auditory and visual continuous performance tests in students with ADHD. J Atten Disord. Epub 2016 Nov 18. | ||
Simões EN, Carvalho ALN, Schmidt SL. What does handedness reveal about ADHD? An analysis based on CPT performance. Res Dev Disabil. 2017;65:46–56. | ||
Schmidt SL, Novais Carvalho AL, Simões EM. Effect of handedness on auditory attentional performace in ADHD students. Neuropsychiatr Dis Treat. 2017;13:2921–2924. | ||
Wojtowicz M, Omisade A, Fisk JD. Indices of cognitive dysfunction in relapsing-remitting multiple sclerosis: intra-individual variability, processing speed, and attention network efficiency. J Int Neuropsychol Soc. 2013;19(5):551–558. | ||
Jonkman LE, Rosenthal DM, Sornami MP, et al. Gray matter correlates of cognitive performance differ between relapsing-remitting and primary-progressive multiple sclerosis. PLoS One. 2015;10:e0129380. | ||
Schmidt SL, Correa P, Tolentino JC, et al. Value of combining activated brain FDG-PET and cardiac MIBG for the differential diagnosis of dementia. Clin Nucl Med. 2008;33:398–401. | ||
Cerqueira AC, Andrade PS, Barreiros JMG, Teixeira AL, Nardi AE. Psychiatric disorders in patients with multiple sclerosis. Compr Psychiatry. 2015;63:10–14. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.