Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 16
Neurological and Psychiatric Comorbidities in Chronic Obstructive Pulmonary Disease
Authors Puteikis K, Mameniškienė R ![]() , Jurevičienė E
, Jurevičienė E
Received 12 November 2020
Accepted for publication 25 January 2021
Published 3 March 2021 Volume 2021:16 Pages 553—562
DOI https://doi.org/10.2147/COPD.S290363
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Kristijonas Puteikis,1 Rūta Mameniškienė,2 Elena Jurevičienė3
1Vilnius University, Faculty of Medicine, Vilnius, Lithuania; 2Vilnius University, Center for Neurology, Vilnius, Lithuania; 3Vilnius University, Center for Pulmonology and Allergology, Vilnius, Lithuania
Correspondence: Rūta Mameniškienė
Vilnius University, Center for Neurology, Vilnius, Lithuania
Tel +370 61153077
Email [email protected]
Background and Purpose: Chronic obstructive pulmonary disease (COPD) is often accompanied by different neurological and psychiatric comorbidities. The purpose of this study was to examine which of them are the most frequent and to explore whether their manifestation can be explained by underlying latent variables.
Methods: Data about patients with COPD and their neurological and psychiatric comorbidities were extracted from an electronic database of the National Health Insurance Fund of Lithuania for the period between January 1, 2012, and June 30, 2014. Exploratory factor analysis (EFA) was used to investigate comorbidity patterns.
Results: A study sample of 4834 patients with COPD was obtained from the database, 3338 (69.1%) of who were male. The most frequent neurological and psychiatric comorbidities were nerve, nerve root and plexus disorders (n=1439, 29.8%), sleep disorders (n=666, 13.8%), transient ischemic attack (n=545, 11.3%), depression (n=364, 7.5%) and ischemic stroke (n=349, 7.2%). The prevalence of ischemic stroke, transient ischemic attack, Parkinson’s disease, dementia and sleep disorders increased with age. One latent variable outlined during EFA grouped neurological disorders, namely ischemic stroke, transient ischemic attack, epilepsy, dementia and Parkinson’s disease. The second encompassed depression, anxiety, somatoform and sleep disorders. While similar patterns emerged in data from male patients, no clear comorbidity profiles among women with COPD were obtained.
Conclusion: Our study provides novel insights into the neurological and psychiatric comorbidities in COPD by outlining an association among cerebrovascular, neurodegenerative disorders and epilepsy, and psychiatric and sleep disorders. Future studies could substantiate the discrete pathological mechanism that underlie these comorbidity groups.
Keywords: chronic obstructive pulmonary disease, comorbidities, factor analysis, sleep impairment, stroke
Introduction
Chronic obstructive pulmonary disease (COPD) is one of the most frequent chronic respiratory conditions and a leading cause of death worldwide.1,2 Its prevalence, mortality and associated burden have been decreasing throughout the years when adjusted for population growth and ageing. However, COPD remains a major contributor to disease burden globally when measured in disability-adjusted life-years (DALYs). Among non-communicable diseases, COPD-related DALYs were surpassed only by ischemic heart disease and stroke, according to data from the Global Burden of Disease Study 2017.3 Patients suffering from COPD are also more likely to be diagnosed with various comorbidities, such as allergic, cardiovascular or cerebrovascular disease, different neurological and psychiatric conditions.4–8 Therefore, COPD can lead to high medical expenses and challenges in providing multidisciplinary care.9
Controlled studies provide information about the specific neurological or psychiatric risks that patients with COPD face (eg increased risk of stroke). However, the interpretation of reports addressing the increased prevalence of individual comorbidities is often limited because of methodological issues.10 Non-identical definitions of COPD, variability in data sources, selected patient samples and measured outcomes render very different comorbidity prevalence results. As current findings indicate that comorbidities in COPD tend to cluster in discrete groups, it might be thus more beneficial to examine multimorbidity patters among patients with COPD rather than the risks of the discrete comorbidities themselves.11–13 Further examination of such clustering may evade some of the limitations of prevalence studies by allowing qualitative analysis of the underlying multimorbidity profiles. A similar approach has already led to the identification of different clinical patterns of COPD.14–18 Outlining the comorbidity profiles in patients with COPD could help to acknowledge the additional health conditions that may be present in these individuals. This could improve personalization of care and facilitate a multidisciplinary approach in treatment protocols.19
Most studies exploring comorbidities in COPD include heterogeneous disorder groups and consequently report broad patterns of disease clustering (eg “cardiovascular” or “metabolic” profiles). This current study seeks to narrow the analysis down and focuses on neurological and psychiatric comorbidities in COPD. It is already known that psychiatric disorders (eg depression, anxiety), impaired cognition, poor sleep and an increased risk of stroke are relevant issues among patients with COPD.4,7,20–26 However, it is not entirely clear, whether different neurological and psychiatric comorbidities tend to manifest together and in what patterns they emerge among individuals with COPD. Such information could prove to be valuable for neurologists and psychiatrists when providing medical services to patients with COPD. The aims of this study were (1) to evaluate the frequency of neurological and psychiatric comorbidities in a sample of patients with COPD and (2) to explore the associations among the comorbidities by extracting underlying factors that are common for several comorbid disorders.
Materials and Methods
Data Sources
The data of this current study were part of a database from the project “The Joint Action on Chronic Diseases and Promoting Healthy Ageing Across the Life Cycle (JA-CHRODIS)” co-funded by the European Union. The initial project dealt with analyzing prevention and management of chronic diseases using data about chronic conditions from large populations by using national electronic health records. Selected variables (eg presence of different disorders, demographic variables, information about hospital admissions etc.) were extracted from electronic health records of the National Health Insurance Fund of Lithuania for the period from January 1, 2012, to June 30, 2014. The Lithuanian national healthcare system relies on compulsory health insurance and seeks to provide universal access for all country’s residents. Therefore, the records covered almost all primary care visits and up to 98% of all inpatient visits in the country’s territory during the study period. Comprehensive methods and results involving data from Lithuania have already been presented elsewhere.27 An approval from the Vilnius Regional Biomedical Research Ethics Committee has been acquired for this study (approval number 2020/3˗1207˗692) and it was conducted according to guidelines and principles outlined in the Declaration of Helsinki. No consent from individual participants was deemed necessary for the Committee’s approval, because all analysis was based on anonymous data from electronic health records. Researchers of this study received permission to use the database, which is comprised of anonymous data only.
Study Sample
The initial patient cohort consisted of 452 769 patients and was composed of all individuals (18 years or older) that had been diagnosed with at least one chronic condition from the 32 chronic diseases list used by Barnett et al and, thus, involved chronic diseases with the highest prevalence and the highest impact on patients.28 During the first step of patient selection for the current study, data of patients aged from 40 to 79 have been extracted, resulting in a sample of 353 780 individuals. The group of patients aged 80 and older was small; data variation in the group was high and many outliers were observed. Because of these reasons, we decided to exclude patients older than 79 years from the analysis. To include only patients with a reliable diagnosis of COPD, we used several criteria during the following step. To be regarded as having COPD, the patients had to be diagnosed with this disorder (code J44.8 in the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision, Australian Modification [ICD-10-AM], “Other specified chronic obstructive pulmonary disease”), have a record of being prescribed medication for COPD (for at least 6 months a year) and have had at least one consultation by a specialist in pulmonology. There were 4834 such individuals (1.37% of the initial sample aged 40 to 79) and only their data were used for further analysis. Among the excluded patients, 316 463 had no diagnosis of COPD, 17,466 had a diagnosis of COPD, but did not meet the required criteria and 15,017 had COPD codes that were not J44.8.
Variable Selection
To better differentiate among the conditions that co-occur with COPD during the second half of adulthood from those existing over the course of an individual’s life, all comorbid disorders had to be recorded during the study period (during medical visits or hospitalizations). All neurological and psychiatric comorbidities were identified only by diagnostic ICD-10-AM codes throughout the medical record data. Some disorders, however, were present in single cases (eg obsessive compulsive or eating disorders) and/or were judged to have too little value to be explored in the context of COPD (eg tic disorder). We chose to omit such disorders from the analysis. Stroke was classified as either ischemic or hemorrhagic by using codes I63-I64 and I60-I61, respectively, as proposed by Woodfield et al (presuming that most undetermined strokes are ischemic).29
Additional variables have been selected for context (eg as risks factors to be associated with stroke). They included diagnosis of tracheal or lung cancer (C33-C34), hypertension (I10-I15), type II diabetes mellitus (E11.01–E11.9, only with prescribed medication and a recorded endocrinologist consultation), ischemic heart disease (I20-I25, only with a recorded cardiologist consultation), arrhythmias (I44–I49, only with a recorded cardiologist consultation) or heart failure (I50.0–I50.9, only with a recorded cardiologist consultation). Information about the number of hospital admissions, total hospital stay and patient disability status was also available.
Statistical Analysis
Exploratory factor analysis (EFA) was performed in search of variables underlying the neurological and psychiatric multimorbidity profiles in COPD. EFA is the proposed method when it is assumed that distinct health conditions are causally related and represent a continuum of pathological processes.30 EFA was based on a tetrachoric correlation matrix from the binary comorbidity data (“1” – a condition is present, “0” – a condition is absent). To be included as variables, comorbidities had to be present in two or more percent of the patient sample or the patient subgroup in question. Being unaware of any existing guidelines for methods of selection of distinct diagnostic categories for EFA, we grouped diagnoses by ICD-10-AM codes according to two principles. First, if one condition was predominant in a group of ICD-coded disorders, we sought not to group it with other disorders that are heterogeneous in their etiology, mechanism and/or manifestation. For example, the group of different movement disorders was largely represented by Parkinson’s disease, which was thus selected for EFA. Secondly, we combined the coded disorders into groups if they have a similar impact on the patient’s health or have a similar etiology. For instance, nerve, nerve root or plexus disorders mostly manifest as pain or reduced mobility almost irrespectively of the affected region (eg whether they are cervical, thoracic or lumbar root disorders).
The number of factors extracted was based on Eigenvalues exceeding the value of 1.0 and the evaluation of a scree plot. The factor loadings were interpreted after performing an oblique oblimin rotation. A cutoff value of >0.30 was used to determine the inclusion of factor loadings into a comorbidity profile. If the Heywood phenomenon occurred (factor loading ≥1.00), the variable in question was eliminated and the procedure repeated to improve model fit. To state the obtained sampling adequacy, we employed the Kaiser-Meyer-Olkin (KMO) criterion (<0.50 being unacceptable).
The benefits of additional stratification by age in EFA of multimorbidity profiles is unclear.30 Given that the patient sample was already limited to ages between 40 and 79, we did not split the study sample into additional age groups. However, we anticipated variation in the discrete COPD comorbidities between genders. Therefore, additional EFA was performed for male and female subgroups.
Microsoft Excel 16.0 was used for descriptive statistics and the creation of graphs. IBM SPSS 23.0 was used for χ2 and Mann–Whitney U-tests. We employed STATA 13.0 for EFA.
Results
In the sample of 4834 patients with COPD, around two thirds were male. The number of patients in different age groups is seen in Figure 1. Patient characteristics and comorbidity data are presented in Table 1. We identified 2767 (57.2%) patients that had been diagnosed with at least one neurological or psychiatric disorder (including stroke). Among the neurological and psychiatric comorbidities, most prevalent were nerve, nerve root and plexus disorders (n=1439, 29.8%), sleep disorders (n=666, 13.8%), transient ischemic attack (n=545, 11.3%), depression (n=364, 7.5%) and ischemic stroke (n=349, 7.2%). Being diagnosed with a transient ischemic attack was associated with hypertension (OR=2.218, 95% CI from 1.429 to 3.443). Recorded ischemic stroke episodes were related to both hypertension (OR=2.117, 95% CI from 1.262 to 3.754) and arrhythmias (OR=1.343, 95% CI from 1.030 to 1.752). The rate of distinct neurological and psychiatric comorbidities varied between men and women, the former more frequently presenting with alcohol-use related disorders (p<0.0001) and ischemic stroke (p=0.001), the latter – with depression, anxiety and somatoform disorders, sleep, headache, nerve, nerve root and plexus disorders, and transient ischemic attack (p<0.0001 for all). Trends of comorbidity frequency and prevalence throughout age groups are presented in Table 2 and Figure 2, respectively.
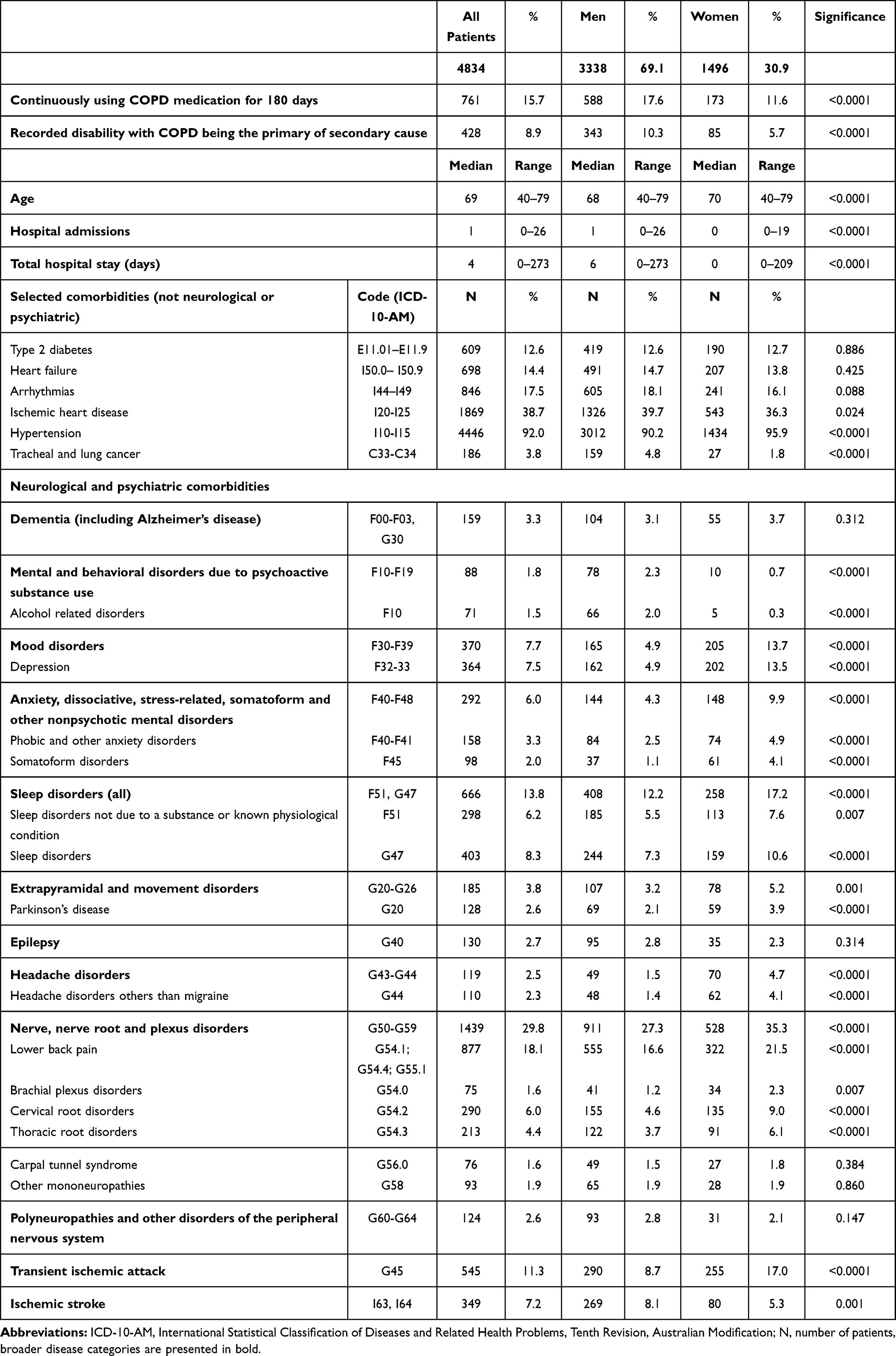 |
Table 1 Patient Characteristics and Comorbidity Data by Gender (Disorders with Prevalence <1% Have Been Omitted) |
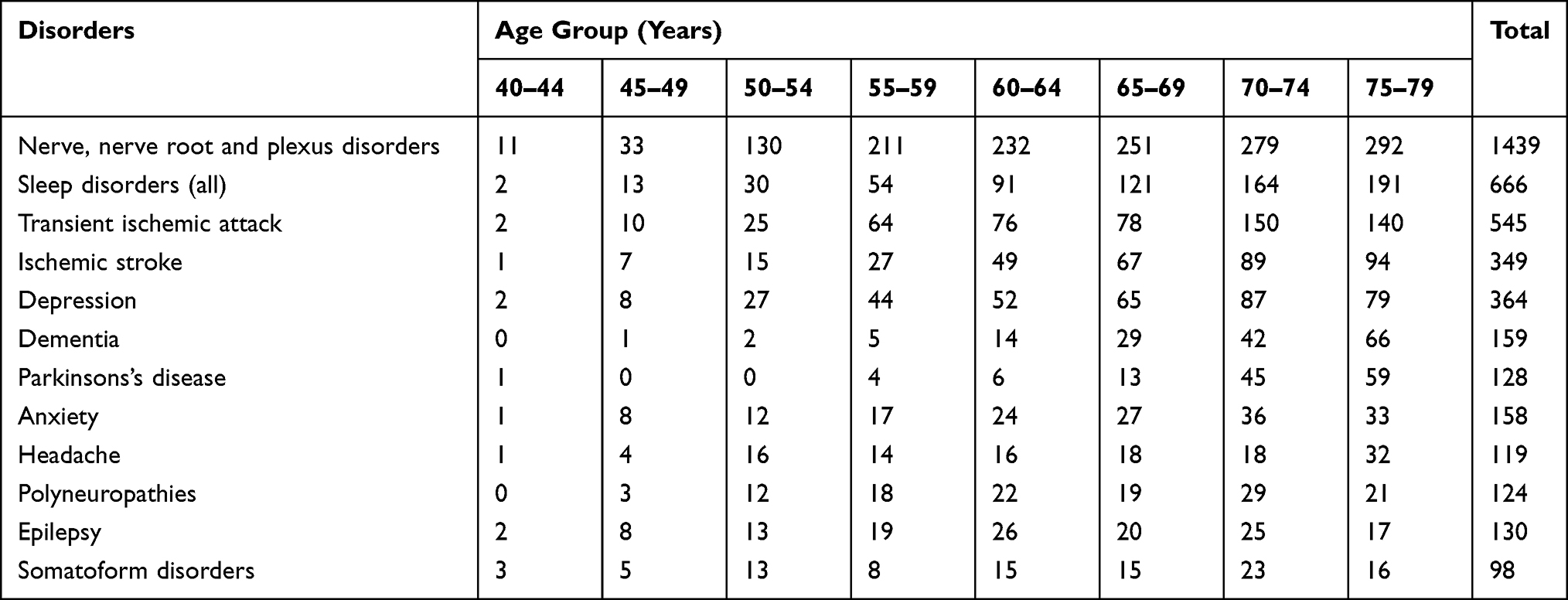 |
Table 2 Frequencies of the Selected Disorders (Overall Prevalence ≥ 2%) in Different Age Groups |
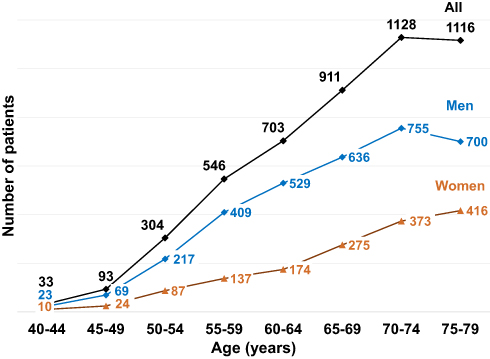 |
Figure 1 Patients with confirmed COPD in different age groups. |
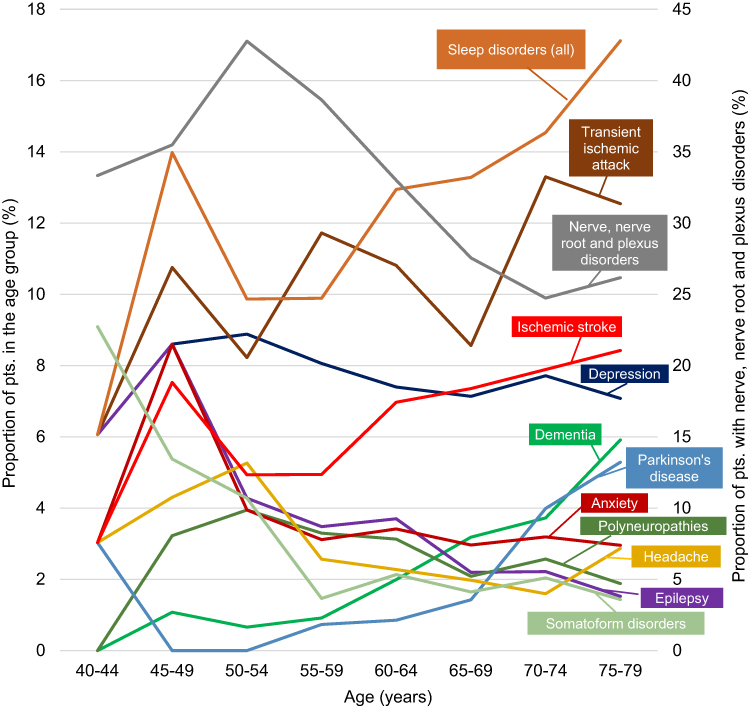 |
Figure 2 Prevalence of the selected disorders (overall prevalence ≥ 2%) in different age groups. Please note that nerve, nerve root and plexus disorders are plotted on a secondary axis. |
Results from EFA of comorbidity patterns based on data from all patients are seen in Table 3. The Kaiser-Meyer-Olkin (KMO) measure was 0.6738 (mediocre). Based on Eigenvalues, two factors have been extracted. The first factor groups disorders whose prevalence increases with age (except for epilepsy) and reveals a pattern of mostly neurodegenerative-cerebrovascular comorbidities. The second pattern matrix included psychiatric and sleep disorders. To better quantify the relationship between the neurodegenerative-cerebrovascular disorders and epilepsy (variables in the first factor), odds ratios were calculated. The odds ratios of being diagnosed with epilepsy were significantly increased with co-existent Parkinson’s disease (OR=3.624, 95% CI from 1.903 to 6.903), dementia (OR=4.130, 95% CI from 2.352 to 7.253), transient ischemic attack (OR=2.440, 95% CI from 1.606 to 3.707) and ischemic stroke (OR=3.051, 95% CI from 1.931 to 4.819).
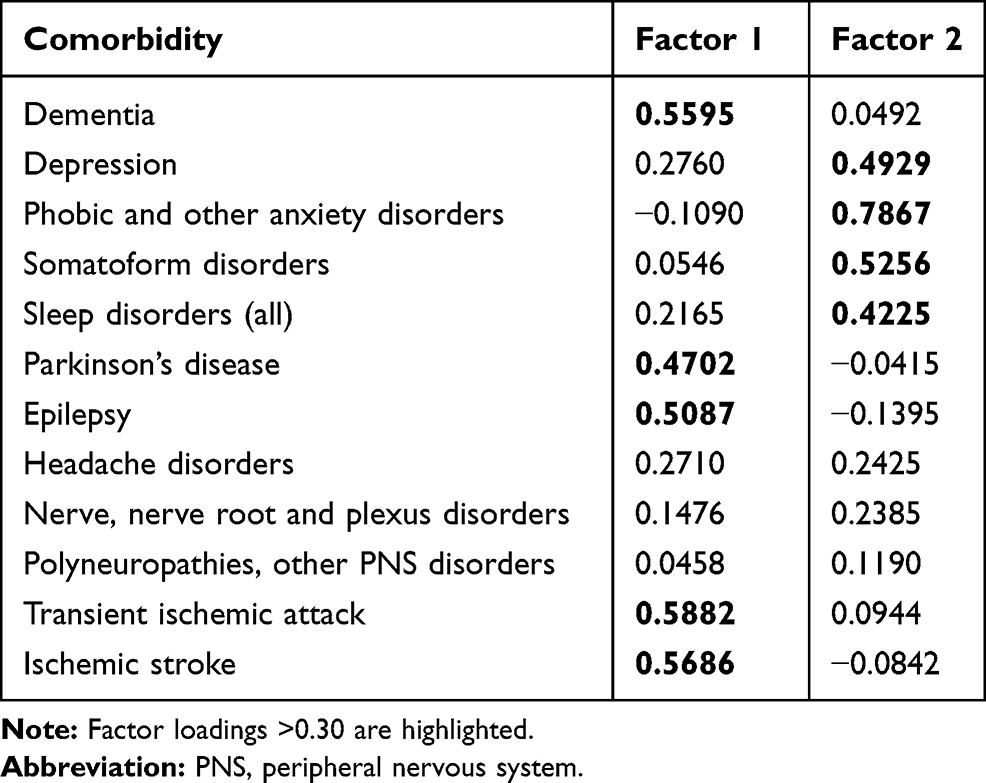 |
Table 3 Factor Loadings for the Selected Variables (Disorders with Prevalence ≥ 2%) When Analysis Was Performed with Data from All Patients in the Sample (KMO=0.6738) |
When performing EFA with data from male patients, a Heywood case was obtained for Parkinson’s disease. After omitting this variable, patterns of dementia-sleep-psychiatric comorbidities and dementia-epilepsy-cerebrovascular disease emerged with a KMO measure of 0.5923 (Table 4) and were similar to those obtained from EFA of all patient data. While EFA results from female individuals (Table 5) pointed to a mediocre sampling adequacy (KMO=0.6957), two variables had been excluded before the analysis. Besides, only one factor was extracted and factor loadings in the matrix did not outline a clear clinical profile.
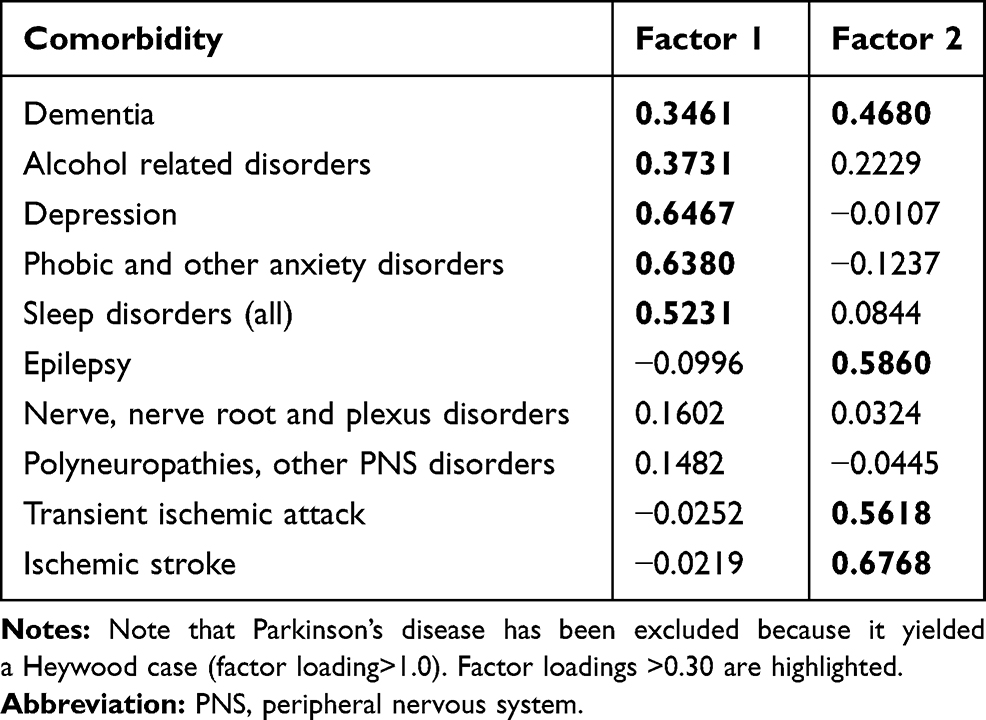 |
Table 4 Factor Loadings for the Selected Variables (Disorders with Prevalence ≥ 2% in the Group) When Analysis Was Performed with Data from Male Patients (KMO=0.5923) |
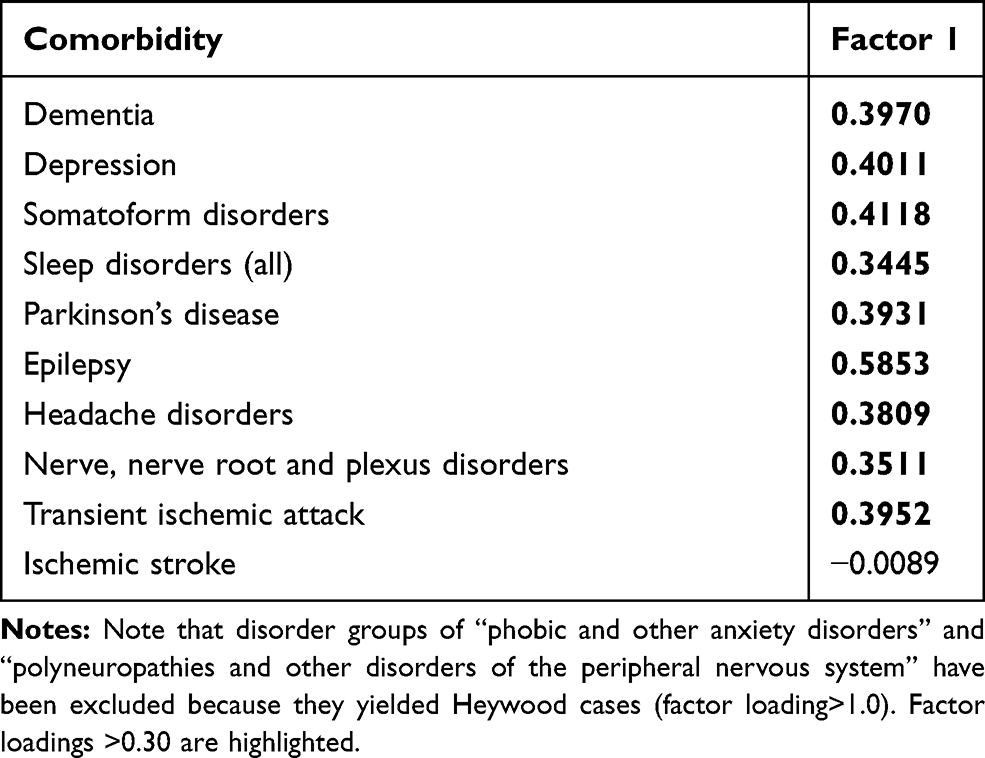 |
Table 5 Factor Loadings for the Selected Variables (Disorders with Prevalence ≥ 2% in the Group) When Analysis Was Performed with Data from Female Patients (KMO=0.6957) |
Discussion
General Findings
The prevalence of COPD (1.37%) was lower than could be expected from other reports, probably because of the conservative inclusion criteria in the current study.1,31 By including only patients who required medical consultations and treatment for COPD, we shifted the focus towards exploring comorbidities among individuals with more active forms of COPD. The male/female ratio was 2.2 – higher than that of around 1.5 observed in other studies and could also be partly explained by the sample selection strategy (ie more severe COPD).32,33 Our findings indicate a relatively sharp increase in both COPD and some of its neurological and psychiatric comorbidities with older age. Cerebrovascular, neurodegenerative and sleep disorders followed a positive trend when presented both in absolute estimates and in relative measures of prevalence among individuals in selected age groups. Gender differences were consistent with findings from other studies: women were more likely to suffer from sleep, anxiety problems, mood disorders and headaches.32,34 Evaluating the prevalence of the neurological and psychiatric disorders in COPD in comparison to a control group was beyond the scope of our study. Nevertheless, national prevalence data from the Health Statistics Portal of Institute of Hygiene of Lithuania from 2014 pointed to large differences in the rate of most neurological and psychiatric diseases between our sample and the general population of the same age. To name some, the estimates were 3.3% vs 0.8% for dementia, 7.5% vs 2.5% for depression, 2.7% vs 1.0% for epilepsy, 29.8% vs 8.5% for nerve, nerve root and plexus disorders, 2.6% vs 0.4% for polyneuropathies, 11.3% vs 1.8% for transient ischemic attack, 7.2% vs 0.9% for stroke, respectively.35 The extent of these dissimilarities indicates that disorders from the whole spectrum of neurological and psychiatric disease, rather than distinct conditions, can be relevant in COPD.
The Pattern of Epilepsy, Neurodegenerative and Cerebrovascular Disease
Exploratory factor analysis revealed two possible latent variables that underlie the neurological and psychiatric comorbidities in COPD. One of them grouped dementia, Parkinson’s disease, epilepsy, ischemic stroke and transient ischemic attack. A question regarding this factor could be whether it represents mainly the process of ageing with COPD or some discrete pathological mechanisms. The two explanations are probably interrelated, especially if ageing is understood as progressive decline in body function. In this sense, patients with COPD have been shown to age faster because of the earlier onset of COPD comorbidities.12,36 The specific pathways associating COPD and its comorbidities have not been fully elucidated. It is hypothesized that shared risk or genetic factors, chronic hypoxia, oxidative stress and systemic inflammation underlie the increased risk of co-occurring pathologies in COPD. The link between COPD and cerebrovascular disease is probably easier to explain because of the evidence of vascular impairment in COPD. Increase in molecules related to inflammation “spill-over” from the lungs (eg C reactive protein, interleukin-6) or reactive oxygen species might represent damage to the endothelium, which promotes atherosclerosis and results in an increased risk of stroke.37,38 It can only be speculated what groups ischemic stroke and transient ischemic attack with Parkinson’s disease, dementia and epilepsy. Systemic inflammation and a dysfunctional reaction to hypoxia (eg lower levels of hypoxia inducible factor-1) might contribute to the more frequent development of Parkinson’s disease in COPD.39 Similar pathological pathways, including systemic inflammation, oxidative stress, chronic hypoxia, hypercapnia, previous cerebrovascular events, could be important in developing dementia.40,41 Epilepsy may be thought to represent seizures associated with neurodegeneration, those secondary to cerebrovascular events or both (as in vascular dementia).42–46 Overall, the relationship between the discrete pathologies grouped under this factor is probably highly complex with multiple features causing vascular and neural impairment. Future research could investigate mitigation strategies for vascular damage and associated neurological outcomes in COPD.
The Pattern of Psychiatric and Sleep Comorbidities
Both anxiety and depression are known to be frequent in COPD. While being distinct psychiatric disorders, they are often present at the same time and have also been found to be related to the level of manifestation of somatic symptoms.20,47,48 Impaired sleep is also a significant comorbidity of COPD.22 An obstructive sleep apnea-COPD overlap syndrome can even be recognized as a separate diagnostic entity with effects common for both conditions, such as increased hypoxia and propagation of inflammatory processes.49 The link between sleep disorders, depression and anxiety in COPD has already been proven earlier and replicated in the exploratory analysis of this current study.50,51 Further, sleep disturbances in COPD can also be associated with cognitive deficits.25 We revealed the possibility of such a relationship only among men with COPD – in their case, dementia was included in both factor matrices (along both neurological and psychiatric conditions). The psychiatric-sleep pattern of COPD comorbidities could be relevant from a purely practical standpoint: targeting poor sleep in COPD might be directly beneficial in reducing the patient’s psychiatric symptoms.52
Study Limitations
Numerous limitations ought to be stated regarding our study. The source of our data consisted of medical records from the database of the National Health Insurance Fund of Lithuania, which had not been intentionally designed for observational studies. It is thus possible that some conditions were under- or overreported because of various reasons, including insurance policy to reimburse services only after a specific diagnosis is made, presumable stigmatization of some conditions (eg depression) and less accurate reporting in case of multimorbidity. The retrospective nature of our study did not allow selecting patients with COPD according to clinical criteria. Consequently, some patients with less severe forms of COPD had possibly been excluded from the sample. Associations between the various disorders in COPD should be regarded with caution as they depend on ad hoc grouping of nosological entities and a subjective interpretation of the possible underlying latent factors. That is, the statistical methods employed do not provide direct evidence of causative relationships between comorbidities.
Conclusion
This study reveals that the prevalence of ischemic stroke, transient ischemic attack, sleep disorders, dementia and Parkinson’s disease tends to increase with age in patients with COPD. There are two possible patterns grouping neurological and psychiatric comorbidities in COPD. One consists of cerebrovascular events, neurodegenerative disorders (dementia and Parkinson’s disease) and epilepsy, the other comprises psychiatric comorbidities and sleep disorders. While these comorbidity profiles were similar in the male subgroup, our study did not manage to prove their existence among women with COPD. Our findings point to the need for further evaluation, whether inflammatory determinants, reactive oxygen species, vascular damage or some other pathological mechanisms could be central to the co-occurrence of neurological disorders in COPD. Impaired sleep in COPD might influence worse psychiatric outcomes, although a bidirectional relationship between the two should be considered as well. Recognition of the neurological and psychiatric comorbidity patterns in neurological practice could direct care towards preventing vascular events and consider more attention to psychiatric conditions alongside complaints of impaired sleep (and vice versa).
Funding
The Joint Action CHRODIS has received funding from the European Union in the framework of the Health Programme (2008–2013) and provided primary data for this study. Sole responsibility lies with the authors and the Consumers, Health, Agriculture and Food Executive Agency is not responsible for any use that may be made of the information contained therein.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Soriano JB, Kendrick PJ, Paulson KR, et al. Prevalence and attributable health burden of chronic respiratory diseases, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/S2213-2600(20)30105-3
2. Li X, Cao X, Guo M, Xie M, Liu X. Trends and risk factors of mortality and disability adjusted life years for chronic respiratory diseases from 1990 to 2017: systematic analysis for the Global Burden of Disease Study 2017. BMJ. 2020;368. doi:10.1136/bmj.m234.
3. Kyu HH, Abate D, Abate KH, et al. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1859–1922. doi:10.1016/S0140-6736(18)32335-3
4. Yin H, Yin S, Lin Q, Xu Y, Xu H, Liu T. Prevalence of comorbidities in chronic obstructive pulmonary disease patients. Medicine. 2017;96(19):e6836. doi:10.1097/MD.0000000000006836
5. Matte DL, Pizzichini MMM, Hoepers ATC, et al. Prevalence of depression in COPD: a systematic review and meta-analysis of controlled studies. Respir Med. 2016;117:154–161. doi:10.1016/j.rmed.2016.06.006
6. Pelgrim CE, Peterson JD, Gosker HR, et al. Psychological co-morbidities in COPD: targeting systemic inflammation, a benefit for both? Eur J Pharmacol. 2019;842:99–110. doi:10.1016/j.ejphar.2018.10.001
7. Putcha N, Drummond MB, Wise RA, Hansel NN. Comorbidities and chronic obstructive pulmonary disease: prevalence, influence on outcomes, and management. Semin Respir Crit Care Med. 2015;36(4):575–591. doi:10.1055/s-0035-1556063
8. Söderholm M, Inghammar M, Hedblad B, Egesten A, Engström G. Incidence of stroke and stroke subtypes in chronic obstructive pulmonary disease. Eur J Epidemiol. 2016;31(2):159–168. doi:10.1007/s10654-015-0113-7
9. Rehman A, Hassali MAA, Muhammad SA, Harun SN, Shah S, Abbas S. The economic burden of chronic obstructive pulmonary disease (COPD) in Europe: results from a systematic review of the literature. Eur J Health Econ. 2020;21(2):181–194. doi:10.1007/s10198-019-01119-1
10. Houben-Wilke S, Triest FJJ, Franssen FME, Janssen DJA, Wouters EFM, Vanfleteren LEGW. Revealing methodological challenges in chronic obstructive pulmonary disease studies assessing comorbidities: a narrative review. COPD. 2019;6(2):166–177. doi:10.15326/jcopdf.6.2.2018.0145
11. Vanfleteren LEGW, Spruit MA, Groenen M, et al. Clusters of comorbidities based on validated objective measurements and systemic inflammation in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2013;187(7):728–735. doi:10.1164/rccm.201209-1665OC
12. Triest FJJ, Franssen FME, Reynaert N, et al. Disease-specific comorbidity clusters in COPD and accelerated aging. J Clin Med. 2019;8(4):511. doi:10.3390/jcm8040511
13. Faner R, Agustí A. Network analysis: a way forward for understanding COPD multimorbidity. Eur Respir J. 2015;46(3):591–592. doi:10.1183/09031936.00054815
14. Incalzi RA, Canonica GW, Scichilone N, Rizzoli S, Simoni L, Blasi F. The COPD multi-dimensional phenotype: a new classification from the STORICO Italian observational study. PLoS One. 2019;14(9). doi:10.1371/journal.pone.0221889
15. Siafakas N, Corlateanu A, Fouka E. Phenotyping before starting treatment in COPD? COPD. 2017;14(3):367–374. doi:10.1080/15412555.2017.1303041
16. Vazquez Guillamet R, Ursu O, Iwamoto G, Moseley PL, Oprea T. Chronic obstructive pulmonary disease phenotypes using cluster analysis of electronic medical records. Health Informatics J. 2018;24(4):394–409. doi:10.1177/1460458216675661
17. Postma DS, Anzueto AR, Jenkins C, et al. Factor analysis in predominantly severe COPD: identification of disease heterogeneity by easily measurable characteristics. Respir Med. 2013;107(12):1939–1947. doi:10.1016/j.rmed.2013.07.011
18. Yoon HY, Park SY, Lee CH, et al. Prediction of first acute exacerbation using COPD subtypes identified by cluster analysis. Int J COPD. 2019;14:1389–1397. doi:10.2147/COPD.S205517
19. Franssen FME, Alter P, Bar N, et al. Personalized medicine for patients with COPD: where are we? Int J COPD. 2019;14:1465–1484. doi:10.2147/COPD.S175706
20. Panagioti M, Scott C, Blakemore A, Coventry PA. Overview of the prevalence, Impact, And management of depression and anxiety in chronic obstructive pulmonary disease. Int J COPD. 2014;9:1289–1306. doi:10.2147/COPD.S72073
21. Yohannes AM, Junkes-Cunha M, Smith J, Vestbo J. Management of dyspnea and anxiety in chronic obstructive pulmonary disease: a critical review. J Am Med Dir Assoc. 2017;18(12):
22. McNicholas WT, Verbraecken J, Marin JM. Sleep disorders in COPD: the forgotten dimension. Eur Respir Rev. 2013;22(129):365–375. doi:10.1183/09059180.00003213
23. Owens RL, Macrea MM, Teodorescu M. The overlaps of asthma or COPD with OSA: a focused review. Respirology. 2017;22(6):1073–1083. doi:10.1111/resp.13107
24. McNicholas WT, Hansson D, Schiza S, Grote L. Sleep in chronic respiratory disease: COPD and hypoventilation disorders. Eur Respir Rev. 2019;28(153):190064. doi:10.1183/16000617.0064-2019
25. Olaithe M, Bucks RS, Hillman DR, Eastwood PR. Cognitive deficits in obstructive sleep apnea: insights from a meta-review and comparison with deficits observed in COPD, insomnia, and sleep deprivation. Sleep Med Rev. 2018;38:39–49. doi:10.1016/j.smrv.2017.03.005
26. DeJean D, Giacomini M, Vanstone M, Brundisini F. Patient experiences of depression and anxiety with chronic disease: a systematic review and qualitative meta-synthesis. Ont Health Technol Assess Ser. 2013;13(16):1–33.
27. Navickas R, Visockiene PR, Rukšeniene M, Kasiulevičius V, Jurevičiene E, Jurevičienė E. Prevalence and structure of multiple chronic conditions in Lithuanian population and the distribution of the associated healthcare resources. Eur J Intern Med. 2015;26(3):160–168. doi:10.1016/j.ejim.2015.02.015
28. Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet. 2012;380(9836):37–43. doi:10.1016/S0140-6736(12)60240-2
29. Woodfield R, Grant I, Sudlow CLM. Accuracy of electronic health record data for identifying stroke cases in large-scale epidemiological studies: a systematic review from the UK Biobank Stroke Outcomes Group. PLoS One. 2015;10(10). doi:10.1371/journal.pone.0140533
30. Busija L, Lim K, Szoeke C, Sanders KM, McCabe MP. Do replicable profiles of multimorbidity exist? Systematic review and synthesis. Eur J Epidemiol. 2019;34(11):1025–1053. doi:10.1007/s10654-019-00568-5
31. Diaz-Guzman E, Mannino DM. Epidemiology and prevalence of chronic obstructive pulmonary disease. Clin Chest Med. 2014;35(1):7–16. doi:10.1016/j.ccm.2013.10.002
32. Raghavan D, Varkey A, Bartter T. Chronic obstructive pulmonary disease: the impact of gender. Curr Opin Pulm Med. 2017;23(2):117–123. doi:10.1097/MCP.0000000000000353
33. Ntritsos G, Franek J, Belbasis L, et al. Gender-specific estimates of COPD prevalence: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2018;13:1507–1514. doi:10.2147/COPD.S146390
34. Grabicki M, Kuźnar-Kamińska B, Rubinsztajn R, et al. COPD course and comorbidities: are there gender differences? Adv Exp Med Biol. 2019;1113:43–51. doi:10.1007/5584_2018_160
35. Health statistics portal of institute of hygiene; 2021. Available from: https://stat.hi.lt/user-report-view.aspx?group_id=29.
36. Divo MJ, Celli BR, Poblador-Plou B, et al. Chronic Obstructive Pulmonary Disease (COPD) as a disease of early aging: evidence from the epichron cohort. PLoS One. 2018;13(2):e0193143. doi:10.1371/journal.pone.0193143
37. Lahousse L, Tiemeier H, Ikram MA, Brusselle GG. Chronic obstructive pulmonary disease and cerebrovascular disease: a comprehensive review. Respir Med. 2015;109(11):1371–1380. doi:10.1016/j.rmed.2015.07.014
38. Austin V, Crack PJ, Bozinovski S, Miller AA, Vlahos R. COPD and stroke: are systemic inflammation and oxidative stress the missing links? Clin Sci. 2016;130(13):1039–1050. doi:10.1042/CS20160043
39. Li C-H, Chen W-C, Liao W-C, et al. The association between chronic obstructive pulmonary disease and Parkinson’s disease: a nationwide population-based retrospective cohort study. QJM. 2015;108(1):39–45. doi:10.1093/qjmed/hcu136
40. Wang Y, Li X, Wei B, Tung T-H, Tao P, Chien C-W. Association between chronic obstructive pulmonary disease and dementia: systematic review and meta-analysis of cohort studies. Dement Geriatr Cogn Dis Extra. 2019;9(2):250–259. doi:10.1159/000496475
41. Tondo G, De Marchi F, Terazzi E, et al. Chronic obstructive pulmonary disease may complicate Alzheimer’s disease: a comorbidity problem. Neurol Sci. 2018;39(9):1585–1589. doi:10.1007/s10072-018-3470-7
42. Sen A, Capelli V, Husain M. Cognition and dementia in older patients with epilepsy. Brain. 2018;141(6):1592–1608. doi:10.1093/brain/awy022
43. Emsley HCA, Parkes LM. Seizures in the context of occult cerebrovascular disease. Epilepsy Behav. 2020;104:106396. doi:10.1016/j.yebeh.2019.06.039
44. Keret O, Hoang TD, Xia F, Rosen HJ, Yaffe K. Association of late-onset unprovoked seizures of unknown etiology with the risk of developing dementia in older veterans. JAMA Neurol. 2020;77(6):E1–E6. doi:10.1001/jamaneurol.2020.0187
45. De Reuck J, Proot P, Van Maele G. Chronic obstructive pulmonary disease as a risk factor for stroke-related seizures. Eur J Neurol. 2007;14(9):989–992. doi:10.1111/j.1468-1331.2007.01829.x
46. Wang JZ, Vyas MV, Saposnik G, Burneo JG. Incidence and management of seizures after ischemic stroke. Neurology. 2017;89(12):1220–1228. doi:10.1212/WNL.0000000000004407
47. Ferguson CJ, Stanley M, Souchek J, Kunik ME. The utility of somatic symptoms as indicators of depression and anxiety in military veterans with chronic obstructive pulmonary disease. Depress Anxiety. 2006;23(1):42–49. doi:10.1002/da.20136
48. Ouellette DR, Lavoie KL. Recognition, diagnosis, and treatment of cognitive and psychiatric disorders in patients with COPD. Int J COPD. 2017;2017:12–639. doi:10.2147/COPD.S123994
49. Mcnicholas WT. COPD-OSA overlap syndrome evolving evidence regarding epidemiology, clinical consequences, and management. Chest. 2017;152(6):1318–1326. doi:10.1016/j.chest.2017.04.160
50. Economou N-T, Ilias I, Velentza L, et al. Sleepiness, fatigue, anxiety and depression in Chronic Obstructive Pulmonary Disease and Obstructive Sleep Apnea – overlap – syndrome, before and after continuous positive airways pressure therapy. PLoS One. 2018;13(6):e0197342. doi:10.1371/journal.pone.0197342
51. Vanfleteren LE, Beghe B, Andersson A, Hansson D, Fabbri LM, Grote L. Multimorbidity in COPD, does sleep matter? Eur J Intern Med. 2020;73:7–15. doi:10.1016/j.ejim.2019.12.032
52. Gupta MA, Simpson FC, Lyons DCA. The effect of treating obstructive sleep apnea with positive airway pressure on depression and other subjective symptoms: a systematic review and meta-analysis. Sleep Med Rev. 2016;28:55–68. doi:10.1016/j.smrv.2015.07.002
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.