Back to Journals » International Journal of Women's Health » Volume 18
Network-Based Identification of Core Acupoints for Primary Dysmenorrhea: A Synthesis of Randomized Trial Prescriptions
Authors Lee IS ![]() , Park H
, Park H ![]() , Kim J
, Kim J
Received 24 January 2026
Accepted for publication 17 April 2026
Published 14 July 2026 Volume 2026:18 598657
DOI https://doi.org/10.2147/IJWH.S598657
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
In-Seon Lee,1 Hyunjun Park,2 Junsuk Kim2
1Department of Meridian and Acupoints, Kyung Hee University, Seoul, South Korea; 2School of Information Convergence, Kwangwoon University, Seoul, South Korea
Correspondence: Junsuk Kim, School of Information Convergence, Kwangwoon University, Seoul, 01897, South Korea, Tel +82-2-940-8477, Email [email protected]
Abstract: Primary dysmenorrhea is one of the most common gynecological conditions affecting women worldwide and a major indication for acupuncture treatment. Although numerous randomized controlled trials and systematic reviews have demonstrated the clinical effectiveness of acupuncture for primary dysmenorrhea, limited attention has been paid to how acupoint prescriptions are structured and which acupoints consistently play central roles across studies. In this paper, we present a network-based synthesis of acupoint prescription data extracted from 116 randomized controlled trials identified from three systematic reviews (2014– 2024). These reviews were selected through a systematic search of PubMed, EMBASE, and the Cochrane Library, specifically filtering for studies that provided granular acupoint prescriptions for primary dysmenorrhea to ensure data quality for network analysis. Using multiple network analytical approaches, including centrality measures, influence maximization, community detection, and structural role analysis, we identify a set of acupoints, CV4, CV6, SP8, ST36, and BL32, as core acupoints, with SP6 functioning as a central hub linking multiple functional clusters. This finding suggests that, despite substantial heterogeneity in individual acupuncture prescriptions, treatment for PD consistently converges on a relatively stable and structurally influential set of acupoints over time. We argue that network-based synthesis of existing trial data can complement conventional evidence by clarifying core treatment structures and reducing unwarranted variability in clinical practice. Because structural centrality does not inherently guarantee therapeutic superiority, future studies should integrate symptom severity, trial quality, and patient-level outcomes with structural analyses to better translate these network-based insights into standardized clinical guidelines.
Keywords: primary dysmenorrhea, acupuncture points, network analysis, women’s health, prescription structure
Introduction
Primary dysmenorrhea (PD) is one of the most prevalent gynecological conditions affecting women of reproductive age and represents a major cause of recurrent menstrual pain and reduced quality of life worldwide.1 Acupuncture is widely used as a non-pharmacological treatment option for PD, particularly among women seeking alternatives to long-term analgesic use.1 Over the past two decades, numerous randomized controlled trials (RCTs) and systematic reviews (SRs) have demonstrated the clinical effectiveness and safety of acupuncture for the management of PD.2–4
Despite this growing body of evidence, much of the existing literature has focused on whether acupuncture works, rather than on how acupuncture treatments are constructed in practice. In particular, relatively little attention has been paid to the structural characteristics of acupoint prescriptions used across clinical trials. Acupuncture interventions for PD often involve complex combinations of acupoints, yet it remains unclear which acupoints consistently play central roles, how these core elements are organized within prescriptions, and whether such patterns remain stable over time. For instance, a series of studies applying network analysis to pain diseases,5 skin disorders,6 functional gastrointestinal disorders7 successfully identified key acupoint combinations. The most recent study demonstrated that the most frequently prescribed acupoints do not always yield the largest clinical effect sizes.8 This precedent highlights the potential of clinical trial-based structural analyses to uncover which acupoints are commonly used versus which may offer the most substantial therapeutic benefits for various diseases. Although a clinical practice guideline for primary dysmenorrhea was published in 2015,9 there are still no specific guidelines that clearly dictate the optimal selection of acupoints and their expected therapeutic effects for acupuncture treatment.
Because traditional acupuncture relies heavily on the synergistic effects of multiple acupoints, analyzing them in isolation or merely counting their frequencies provides an incomplete picture. Network analysis serves as an optimal methodological framework to overcome this limitation by modeling the co-occurrence and topological influence of these points. This lack of structural insight in PD research contributes to substantial heterogeneity in both clinical practice and trial reporting, making it difficult to distinguish essential treatment components from optional or practitioner-specific choices. Ultimately, addressing this gap is clinically essential; clarifying the core prescription structure can reduce unwarranted variability, improve the reproducibility of future clinical trials, and provide a standardized, evidence-informed foundation for optimizing PD management.
To address this gap, we applied multiple network analytical approaches to acupoint prescription data extracted from RCTs included in recent systematic reviews. By examining acupoint co-occurrence patterns, structural influence, and community organization, this paper highlights recurring structural features of acupuncture prescriptions for PD and identifies acupoints that consistently occupy central positions across studies.
Methods
This study is a secondary analysis of previously published randomized controlled trials; therefore, no additional ethical approval was required. Acupoint data were extracted from RCTs included in three SRs on acupuncture for PD. To identify these SRs, we conducted a systematic search of PubMed, EMBASE, and the Cochrane Library for articles published through 2024 using keywords such as “primary dysmenorrhea,” “acupuncture,” and “systematic review”. The SRs were selected based on the following criteria: publication within the past 10 years (2014–2024), a specific focus on acupuncture-related interventions for PD, and reporting detailed acupoint prescriptions for each included study to ensure the availability of granular data for analysis. Three SRs were included,2–4 and all RCTs included in the selected SRs were identified. From each eligible RCT, publication year, intervention type (eg., manual acupuncture, electroacupuncture, or moxibustion), and the list of acupoints were extracted. Each unique acupuncture prescription was treated as an independent observation.
An undirected weighted acupoint co-occurrence network was constructed, with nodes representing individual acupoints and edges representing their co-prescription within the same treatment arm. Edge weights reflected co-occurrence frequency across all RCTs. Eigenvector centrality, degree centrality, betweenness centrality, and closeness centrality were calculated to assess nodal importance. Influence maximization analysis based on the Independent Cascade Model was performed using a single-seed approach to identify structurally influential acupoints. Main acupoints for PD were defined as the union of acupoints ranked within the top 10 across influence maximization and all four centrality measures. Community structures were identified using the Louvain algorithm to detect groups of frequently co-prescribed acupoints.10 Structural role analysis was conducted using the Role eXtraction (RolX) framework, with local and recursive features extracted via the recursive feature extraction algorithm to classify acupoints into distinct structural roles. A graph convolutional network (GCN) was applied to jointly model network topology and acupoint attributes.11 Temporal changes were examined by analyzing publication years across three predefined eras (1987–2010, 2011–2016, and 2017–2022).
All analyses were conducted in Python 3.12 via Google Colaboratory. The following libraries were used: NetworkX 3.6.1 for graph construction and analysis, PyTorch 2.10.0 for the GCN, scikit-learn 1.6.1 for clustering and t-SNE visualization, UMAP-learn 0.5.11 for dimensionality reduction, SciPy 1.16.3 for entropy and sparse matrix operations, python-louvain 0.16 for community detection, and a custom implementation of the Independent Cascade model for influence maximization. The GCN was implemented as a graph autoencoder with a two-layer architecture (hidden dimension = 32, latent dimension = 8) using ReLU activation, trained for 300 epochs with the Adam optimizer (learning rate = 0.01, weight decay = 5 × 10−4) and inner product decoding. A fixed random seed (42) was applied to ensure reproducibility. For influence maximization, edge transmission probabilities were derived from co-occurrence weights using square root scaling (p = (w/w_max)^0.5), and 1,000 Monte Carlo simulations were conducted per single-node seed. A total of 116 RCTs published between 1987 and 2023 were included. All code and analysis scripts are publicly available at https://github.com/hjun-park21/Acupuncture_Network_Analysis.
Results
In accordance with the inclusion criteria, acupoint data reported from 116 RCTs (after duplicates removed), identified through three SRs,2–4 were included in the analyses. The results show that five acupoints, CV (Conception Vessel) 4, CV6, SP (Spleen) 8, ST (Stomach) 36, and BL (Bladder) 32, consistently ranked among the top 10, indicating their robust and central roles in the treatment of PD (Table 1). Louvain clustering identified 11 distinct acupoint communities. The largest community, led by SP6, formed a core integrative module dominated by acupoints on the Conception Vessel and the spleen and kidney meridians, as well as acupoints located on the lower abdomen. Other communities corresponded to auricular points, limb- and system-regulatory groups, abdominal–pelvic modules, sacral clusters, and acupoints on the Governor Vessel meridian, indicating that PD prescriptions are organized into modular yet interconnected functional units (Figure 1A). GCN-based clustering identified five broader and inclusive acupoint clusters by integrating network topology and acupoint attributes. The largest cluster was again led by SP6, while the other clusters reflected limb–trunk regulation, a Governor Vessel–dominant cluster, and an auricular cluster (Figure 1B). Structural role analysis classified 87 acupoints into four roles. Role 0 (local cluster members, n = 61) showed moderate degree, low strength, and high clustering, suggesting dense local groupings around hubs. Role 1 included 13 core acupoints (eg. SP6, CV4, BL32, SP8, CV6, and ST36), and exhibited the highest degree and strength with moderate clustering. Role 2 (highly cohesive nodes, n =11) consisted mainly of Governor Vessel acupoints with low degree but extremely high clustering, forming tightly interconnected modules. Role 3 (bridges/pathways) included CV7 and KI5, which had minimal direct connections but exceptionally strong neighboring nodes.
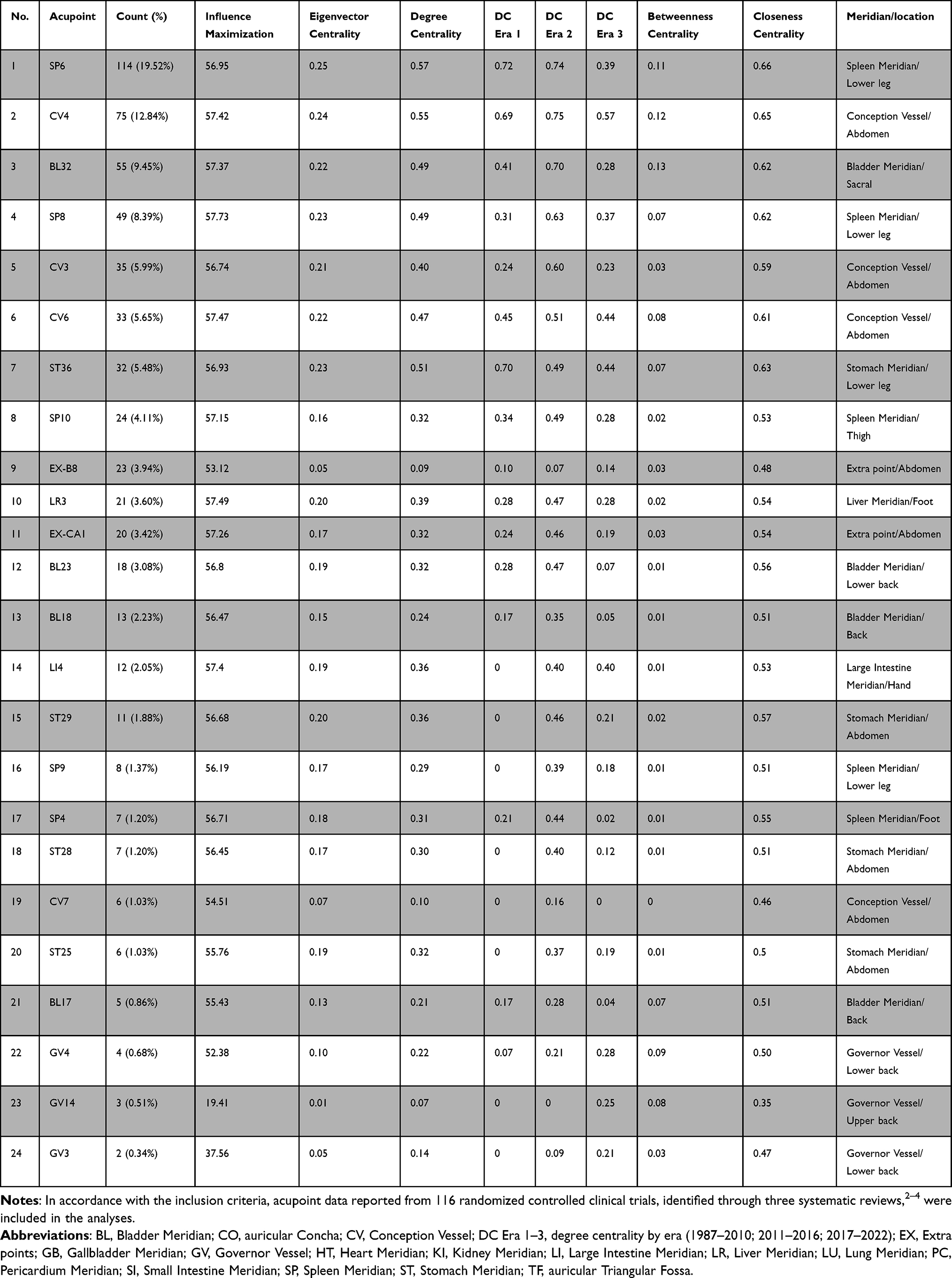 |
Table 1 Frequency, Influence Maximization, and Centrality Characteristics of Key Acupoints Identified from RCTs Within Selected Systematic Reviews |
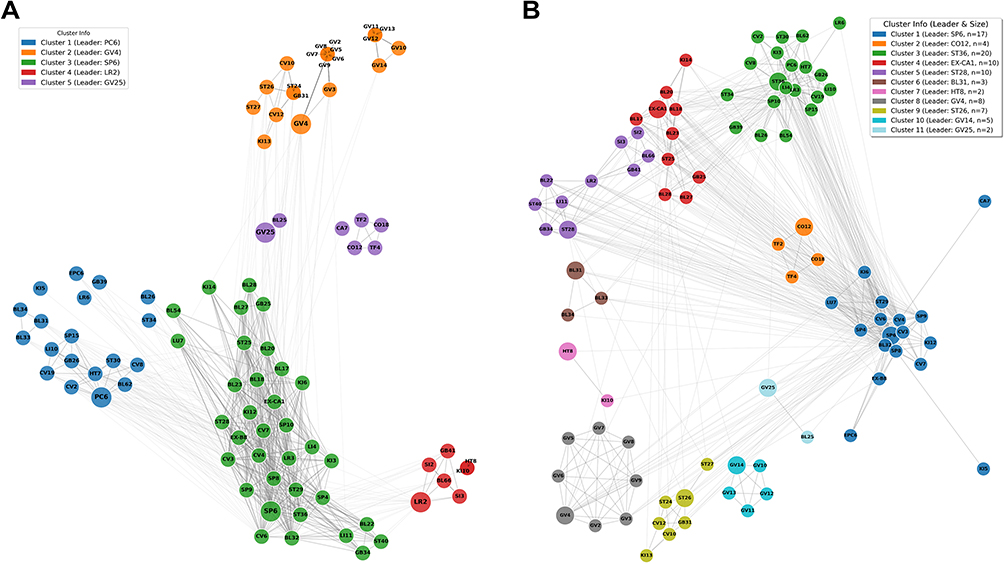 |
Figure 1 Network-based identification of acupoint communities for primary dysmenorrhea using Louvain and GCN clustering. (A) Louvain clustering identified 11 distinct acupoint communities within the dysmenorrhea treatment network. Cluster 1, led by SP6, comprised BL32, CA (Auricular Concha) 7, CV3, CV4, CV6, CV7, EPC (Ear point) 6, EX (Extra)-B8, KI12, KI5, KI6, LU (Lung) 7, SP4, SP6, SP8, SP9, and ST29. Cluster 2 was centered on the auricular point CO (Auricular Concha) 12 and included CO12, CO18, TF (Triangular Fossa) 2, and TF4. Cluster 3, with ST36 as the leader, consisted of BL26, BL54, BL62, CV19, CV2, CV8, GB (Gall Bladder) 26, GB39, HT (Heart) 7, KI3, LI (Large Intestine) 10, LI4, LR(Liver) 3, LR6, PC (Pericardium) 6, SP10, SP15, ST30, ST34, and ST36. Cluster 4 was led by EX-CA1 and included BL17, BL18, BL20, BL23, BL27, BL28, EX-CA1, GB25, KI(Kidney) 14, and ST25. Cluster 5, centered on ST28, comprised BL22, BL66, GB34, GB41, LI11, LR2, SI (Small Intestine) 2, SI3, ST28, and ST40. Cluster 6 consisted of sacral points BL31, BL33, and BL34, with BL31 as the leader. Cluster 7 was led by HT8 and included HT8 and KI10. Cluster 8, centered on GV (Governor Vessel) 4, comprised GV2, GV3, GV4, GV5, GV6, GV7, GV8, and GV9. Cluster 9, led by ST26, included CV10, CV12, GB31, KI13, ST24, ST26, and ST27. Cluster 10 was centered on GV14 and consisted of GV10, GV11, GV12, GV13, and GV14. Finally, Cluster 11, led by GV25, included BL25 and GV25. (B) GCN-based clustering identified five acupoint communities by integrating network topology and acupoint attributes. Cluster 1, led by PC6, included BL26, BL31, BL33, BL34, BL62, CV19, CV2, CV8, EPC6, GB26, GB39, HT7, KI5, LI10, LR6, PC6, SP15, ST30, and ST34. Cluster 2 was centered on GV4 and comprised CV10, CV12, GB31, GV2, GV3, GV4, GV5, GV6, GV7, GV8, GV9, GV10, GV11, GV12, GV13, GV14, KI13, ST24, ST26, and ST27. Cluster 3, the largest cluster, was led by SP6 and included BL17, BL18, BL20, BL22, BL23, BL27, BL28, BL32, BL54, CV3, CV4, CV6, CV7, EX-B8, EX-CA1, GB25, GB34, KI12, KI14, KI3, KI6, LI11, LI4, LR3, LU7, SP10, SP4, SP6, SP8, SP9, ST25, ST28, ST29, ST36, and ST40. Cluster 4, led by LR2, consisted of BL66, GB41, HT8, KI10, LR2, SI2, and SI3. Cluster 5 was centered on GV25 and comprised BL25, CA7, CO12, CO18, GV25, TF2, and TF4. |
Discussion
Using a comprehensive network-based analytical framework, we identified CV4, CV6, SP8, ST36, and BL32 as core acupoints, with SP6 serving as the central hub across multiple analytical approaches. The degree centrality of most acupoints tended to decrease in more recent periods, possibly due to the inclusion of a wider variety of acupoints in recent RCTs. Although network analyses offer a quantitative foundation for understanding core prescription structures, future studies should incorporate symptom- or severity-specific acupoint prescriptions and treatment effect (eg. effect size)–based analyses.8 Such integrative approaches may facilitate the development of evidence-based, standardized clinical decision support systems by combining these structural insights with actual clinical efficacy data, thereby guiding more consistent and reliable acupuncture care for PD.
A comparative analysis of the clustering results from the Louvain algorithm (Figure 1A) and the GCN (Figure 1B) underscores that both methodological approaches offer complementary insights into prescription structures. Methodologically, the Louvain algorithm strictly relies on topological edge weights, which resulted in 11 highly granular, densely connected communities. This approach excels at capturing empirical, micro-level clinical habits, identifying tightly knit co-prescription blocks such as distinct sacral or localized abdominal sub-groups. In contrast, by integrating topology with nodal attributes, the GCN yielded 5 broader, more macroscopic functional modules. While Louvain clustering reveals how practitioners specifically group acupoints in practice, the GCN uncovers the broader theoretical architecture, reflecting why these points are harmonized based on traditional meridian theory. Therefore, we believe that the concurrent use of both methods provides a more comprehensive understanding of primary dysmenorrhea treatments, effectively bridging the gap between empirical prescription patterns and underlying traditional mechanisms.
The structural importance of SP6 as the central hub in our network is further supported by a recent systematic review,12 which confirmed that SP6 stimulation alone is highly effective for pain management in PD. Specifically, their meta-analysis involving 1,171 patients with PD demonstrated that both acupuncture and acupressure at SP6 significantly reduce pain. Although their study focused strictly on single-point interventions, the results provide strong clinical validation for the central, integrative role of SP6 identified through our structural analysis. While Ravi et al12 clarified the independent efficacy of this hub, our network synthesis complements this by revealing how SP6 functions as a structural bridge, consistently co-occurring with other core elements such as CV4 and BL32 to form stable therapeutic modules. By bridging single-point efficacy with multi-point structural co-occurrence, we provide a more comprehensive understanding of how PD treatment is organized in clinical practice. For instance, future research could investigate the potential synergistic effects between SP6 and CV4 or BL32, to clarify both the common mechanisms shared across acupoint stimulations and the point-specific biological pathways underlying acupuncture’s efficacy in PD.
From a broader perspective, these observations address a long-standing challenge in acupuncture research and clinical practice: the lack of clarity regarding which acupoints are essential versus optional in treatment protocols. While systematic reviews and clinical trials have repeatedly demonstrated the effectiveness of acupuncture for PD, they have provided limited guidance on how acupoint prescriptions are structured or prioritized. By synthesizing prescription data across randomized trials using network-based approaches, this study offers a complementary form of evidence that goes beyond frequency counts and effect size estimates. Such structural insights may help reduce unwarranted variability in clinical practice, inform more consistent reporting of acupuncture interventions in future trials, and support the development of evidence-informed decision support tools for acupuncture care in women with PD.
A notable limitation of the current study is that the network synthesis relies strictly on structural co-occurrence, without weighting the data by the methodological quality of the included trials or the magnitude of their clinical effect sizes. Consequently, while our findings highlight core structural modules, high structural centrality does not inherently guarantee superior therapeutic efficacy, as shown in the previous study.8 Future studies should address this by integrating effect size calculations and rigorous trial quality assessments into the network models. By bridging topological importance with concrete clinical outcomes, such integrative approaches will translate these structural insights into truly actionable clinical strategies. Ultimately, this will enable practitioners to identify acupoint combinations that are not only structurally robust but also maximally effective for pain relief, thereby facilitating the development of optimized, evidence-based acupuncture protocols for PD. In addition, future research should extend this structural approach by incorporating symptom severity, menstrual pain phenotypes, and treatment responsiveness to examine whether core acupoints differ according to clinical presentation. In addition, integrating effect size estimates and dosage-related variables may help clarify how structural importance relates to therapeutic impact. Such efforts would strengthen the link between prescription structure and clinical outcomes, supporting more personalized and evidence-informed acupuncture care for women with PD.
Conclusion
In summary, we identified core acupoints that consistently occupy central structural roles in PD treatments. By employing multiple network approaches, this study extends beyond conventional systematic reviews to map the structural architecture of clinical practice, which can help reduce unwarranted prescription variability. However, because our analysis relies on unweighted trial data, frequent co-occurrence does not guarantee clinical effectiveness. Thus, this study provides a structural foundation rather than definitive protocols. Future research must integrate these findings with patient-level clinical outcomes to advance evidence-informed acupuncture strategies for PD.
Data Sharing Statement
The data supporting the findings of this study are available from the corresponding author, J. Kim, upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (RS-2023-00279315, RS-2025-22902971) and by the Research Grant of Kwangwoon University in 2025.
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
References
1. Zhang F, Sun M, Han S, et al. Acupuncture for primary dysmenorrhea: an overview of systematic reviews. Evidence Based Compl Alternat Med. 2018;2018(1):8791538. doi:10.1155/2018/8791538
2. Woo HL, Ji HR, Pak YK, et al. The efficacy and safety of acupuncture in women with primary dysmenorrhea: a systematic review and meta-analysis. Medicine. 2018;97(23):e11007. doi:10.1097/MD.0000000000011007
3. Liu W, Wang CC, Lee KH, Ma X, Kang TL. Efficacy and safety of acupuncture and or moxibustion for managing primary dysmenorrhea: a systematic review and meta-analysis. Clin Nurs Res. 2022;31(7):1362–7. doi:10.1177/10547738221086984
4. Chen S-C, Ruan J-Y, Zhang B, et al. Traditional Chinese medicine interventions based on Meridian theory for pain relief in patients with primary dysmenorrhea: a systematic review and network meta-analysis. Front Med. 2024;11:1453609. doi:10.3389/fmed.2024.1453609
5. Lee SH, Kim CE, Lee IS, et al. Network analysis of acupuncture points used in the treatment of low back pain. Evid Based Complement Alternat Med. 2013;2013:402180. doi:10.1155/2013/402180
6. Moon H, Chae Y, Lee I-S, Kim K. Identification of fundamental principles behind the treatment of skin diseases with acupuncture using network analysis. Indian J Tradit Knowl. 2025;24(3):211–218.
7. Moon H, Ryu Y, Lee I-S, Chae Y. Acupuncture treatment for functional gastrointestinal disorders: identification of major acupoints using network analysis. Integrat Med Res. 2023;12(3):100970. doi:10.1016/j.imr.2023.100970
8. Kim G, Kim D, Moon H, et al. Acupuncture and acupoints for low back pain: systematic review and meta-analysis. Am J Chin Med. 2023;51(2):223–247. doi:10.1142/S0192415X23500131
9. China Press of Traditional Chinese Medicine. Evidence-Based Acupuncture Clinical Practice Guidelines: Primary Dysmenorrhea. Beijing: China Press of Traditional Chinese Medicine; 2015.
10. Blondel VD, Guillaume J-L, Lambiotte R, Lefebvre E. Fast unfolding of communities in large networks. Statist Mech. 2008;2008(10):P10008. doi:10.1088/1742-5468/2008/10/P10008
11. Kipf TN, Welling M. Semi-supervised classification with graph convolutional networks. arXiv preprint arXiv:1609.02907. 2016.
12. Ravi P, Boopalan D, Vijayakumar V, et al. Effect of Sanyinjiao (Spleen-6) acupoint for pain management in primary dysmenorrhea: an updated systematic review and meta-analysis. Med Acupunct. 2024;36(4):178–188. doi:10.1089/acu.2023.0100
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Disease Burden of Dysmenorrhea: Impact on Life Course Potential
MacGregor B, Allaire C, Bedaiwy MA, Yong PJ, Bougie O
International Journal of Women's Health 2023, 15:499-509
Published Date: 3 April 2023