Back to Journals » Journal of Hepatocellular Carcinoma » Volume 9
Neoadjuvant Immunotherapy for Hepatocellular Carcinoma
Authors Marron TU ![]() , Schwartz M, Corbett V, Merad M
, Schwartz M, Corbett V, Merad M
Received 4 February 2022
Accepted for publication 23 June 2022
Published 30 June 2022 Volume 2022:9 Pages 571—581
DOI https://doi.org/10.2147/JHC.S340935
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ahmed Kaseb
Thomas U Marron,1– 7 Myron Schwartz,1– 4,6,7 Virginia Corbett,1,3,5– 7 Miriam Merad1– 7
1The neoAdjuvant Research Group to Evaluate Therapeutics (TARGET), Icahn School of Medicine at Mount Sinai, New York, NY, USA; 2Early Phase Trials Unit, Tisch Cancer Institute, Icahn School of Medicine at Mount Sinai, New York, NY, USA; 3Tisch Cancer Institute, Icahn School of Medicine at Mount Sinai, New York, NY, USA; 4Precision Immunology Institute, Icahn School of Medicine at Mount Sinai, New York, NY, USA; 5Division of Hematology and Medical Oncology, Icahn School of Medicine at Mount Sinai, New York, NY, USA; 6Center of Excellence for Liver and Bile Duct Cancer, Icahn School of Medicine at Mount Sinai, New York, NY, USA; 7Liver Cancer Program, Division of Liver Diseases and RM Transplant Institute, Icahn School of Medicine at Mount Sinai, New York, NY, USA
Correspondence: Thomas U Marron, Email [email protected]
Abstract: The treatment paradigm for hepatocellular carcinoma (HCC) had been stagnant until recently, with new combinations of targeted and immunotherapies entering the first- and second-line setting for patients with advanced disease. This improvement in therapeutic options is well timed given the rise in rates of HCC globally; additionally, screening high-risk patients has also led to an increase in detection of early HCC lesions, identifying patients who can be treated with curative intent approaches such as surgery. Unfortunately, the vast majority of patients who undergo surgical resection develop recurrent HCC, either due to disease recurrence from residual micrometastatic disease or de novo primaries, and there are no perioperative therapies that have demonstrated the ability to significantly improve survival for these patients. Given the survival benefit that immunotherapy has imparted to patients with advanced HCC, and recent studies in other tumor types demonstrating perioperative—in particular neoadjuvant—immunotherapy significantly improves outcomes, there is substantial interest in neoadjuvant immunotherapy for patients with resectable HCC. Three recently reported small studies looking at anti-PD-1 antibodies alone or in combination have demonstrated significant pathologic response to brief pre-operative interventions, and support exploring this approach in larger registrational studies. With these developments the clinical outlook for HCC patients, with both early and advanced disease, is rapidly improving.
Keywords: immunotherapy, neoadjuvant therapy, perioperative therapy
Introduction
Immunotherapy has revolutionized the treatment of many cancers including hepatocellular carcinoma (HCC). HCC is unique among cancers due to its resistance to chemotherapy; instead, tyrosine kinase inhibitors (TKIs) have been the mainstay of treatment for HCC for the past two decades.1 However, immunotherapy agents targeting programmed death receptor (PD-1) and its ligand (PD-L1) have shown significant clinical activity as a second-line therapy in patients whose disease had progressed following treatment with TKIs, and a potentially higher survival when combined with CTLA-4 blocking antibodies.2–4 More recently combination approaches with PD-(L)1 blocking antibodies given with either the VEGF antibody bevacizumab or lenvatinib, a multi-targeted TKI, have showed significant activity in the first-line setting far superior to the historic TKI comparator, sorafenib.5 While these agents have changed the treatment paradigm, the majority of patients with HCC still fail to respond to therapy, and we lack a firm understanding of the heterogeneity of clinical response as well as validated biomarkers to help define who will benefit from these therapies.
PD-L1 immunohistochemistry (IHC) has been used in other malignancies as a biomarker of response, though in most malignancies it has relatively poor predictive power, and in HCC it remains controversial whether it is useful in guiding therapy.6 Additionally, given that HCC can be diagnosed radiographically, the use of a tissue-based biomarker will require a paradigm shift in the clinical approach to diagnosing and treating HCC. Pre-treatment and on-treatment biopsies from patients receiving therapy in the context of a clinical trial is the ideal way to identify predictive biomarkers, though given the heterogeneous nature of tumors—particularly in tumors where there has been a response to therapy and significant intratumoral necrosis—the utility of small-bore needle biopsies in defining pre-treatment predictors of response, as well as dynamic changes induced by therapy, is questionable. Even in clinical trials with mandated biopsies, the tissue quality is often suboptimal, and typically high-quality pre- and on-treatment biopsies are successfully collected from only a minority of patients.
Neoadjuvant clinical trials offer a unique setting not only to improve outcomes for patients with localized HCC, but to better understand how novel therapies work in patients with HCC, which can inform biomarkers and identify optimal combinatorial therapeutic approaches. The standard approach for patients with localized disease and intact liver function is surgical resection; however, even in patients with tumors smaller than 2 cm the risk of recurrence nears 70%,7 and no perioperative therapy has demonstrated significant survival benefit to date.8 Given the success of immunotherapy in the advanced HCC setting,4,5 and the clinical efficacy of perioperative immunotherapy in other malignancies that has led to FDA approvals in the past year,9–13 we would hypothesize that perioperative immunotherapy may significantly benefit patients with resectable HCC, and recent trials support this hypothesis.14–16 Here we review the current understanding—and scientific and clinical promise—of perioperative immunotherapy in HCC.
The Clinical and Scientific Potential of Perioperative Therapy in HCC
Neoadjuvant trials offer a unique clinical setting to accurately define the mechanism of action of novel immunotherapies and combination approaches.17 In general, neoadjuvant therapy is used with two goals in mind: (1) reducing the chance of recurrence through elimination of micrometastatic disease not visualized on imaging, and (2) cytoreduction of the primary tumor to facilitate subsequent definitive therapy. Additionally, response to therapy may be used as a predictive and prognostic marker and to guide clinical decisions around adjuvant therapy. However, brief pre-operative therapeutic intervention trials, often termed “window-of-opportunity” trials, may be designed not necessarily with the intention of downstaging the tumor, but rather to study the effect of therapy. This said, these trials—and this therapeutic approach—do not represent an exploitation of humans for the purpose of research; they in fact may have the potential to improve recurrence-free survival while at the same time not significantly delaying surgery.14,18–22 Tumor shrinkage and/or frank necrosis prior to surgery is sometimes observed in this setting, but the primary target of therapy is micrometastatic disease that can seed eventual recurrence since the clinically evident tumor will be surgically removed.
Additionally, response rates to immunotherapy in the neoadjuvant setting across cancer types appear equivalent to, if not higher than, those observed in the unresectable and/or metastatic setting.14,18–23 Neoadjuvant immunotherapy alone or in combination with chemotherapy is now standard therapy for triple negative breast cancer, and promising phase 2 and phase 3 clinical trial data in multiple other tumor types will likely lead to broadening of this approach in the coming years.9–13 There are many reasons why operative candidates may be more responsive to immunotherapy than patients with more advanced disease. Operative candidates are typically treatment naïve and have more robust immune systems; not only does more advanced cancer potentially induce systemic immunosuppression through a variety of mechanisms, but immunotherapy is often given following many other lines of therapy that may have further taxed the immune system. Additionally, smaller resectable tumors typically demonstrate less intratumoral heterogeneity (including mutational/neoantigen heterogeneity) and less loss of heterozygosity that may enable immune evasion.24,25 Indeed, there are numerous clinical studies in many cancer types demonstrating that tumor burden inversely correlates with response to immunotherapy.26–28
With improving rates of screening of high-risk individuals, more HCC patients are being identified with early-stage HCC amenable to surgical resection, however, the vast majority of these patients’ tumors recur, and to date perioperative therapy has demonstrated enough of a significant survival advantage to warrant widespread adoption.8,29,30 A number of studies are underway assessing the efficacy of adjuvant immunotherapy following curative-intent treatment of HCC, including the registrational CheckMate 9DX study looking at the use of nivolumab after resection or ablation; clinical efficacy of adjuvant immunotherapy has already led to its approval by the FDA in multiple other cancers including non-small cell lung cancer and melanoma.31,32 However, neoadjuvant—which we can more accurately call “perioperative” immunotherapy since anti-PD-(L)1 antibodies have long half-lives and will remain in circulation post-operatively—is posited to be superior to adjuvant immunotherapy alone. Use of immunotherapy preoperatively augments anti-tumor immunity, likely due to priming of new T cell responses against tumor neoantigens while the tumor still remains in vivo, while in the adjuvant setting the only neoantigens that remain are from micrometastatic disease, which may translate to less immune priming and activation.11,33 Pre-clinical modeling lends credence to this argument, with improved survival and enhanced tumor-specific CD8+ T cell activation in mice administered PD-1 blockade pre-operatively compared with those that received only post-operative therapy.34 Limited clinical evidence in melanoma and lung cancer also supports the use of neoadjuvant over adjuvant immunotherapy and, in an albeit small cohort, there are data showing augmented T cell clonal expansion when immunotherapy is administered pre-operatively.11,18
Additionally, neoadjuvant treatment therapy may be superior to treatment in the adjuvant setting, as surgery itself can be an insult to systemic immunity. Post-operative immunosuppression, associated with surgical stress, is mediated by elevated alarmins such as damage-associated molecular patterns (DAMPs) and peripheral cytokines including IL-8 and IL-6, leading to local and systemic inflammation.35,36 This suppresses cellular immunity, hindering both de novo T cell priming and activation and potentially further limiting efficacy of adjuvant immunotherapy with checkpoint blockade.37–39 Resection and disruption of the tumor microenvironment and associated draining lymph nodes may also impact the efficacy of immunotherapy, as PD-1 targeting agents may in part act to aid in T cell expansion at the site of tumor-draining lymph nodes, and surgical disruption of normal lymphatics may decrease the efficacy of adjuvant immunotherapy compared with neoadjuvant.
In addition to providing potential clinical benefit, neoadjuvant trials provide a unique window to characterize the dynamic effect of immunotherapy in vivo. As opposed to the scant biospecimens available from clinical trials in the metastatic setting, neoadjuvant trials provide blood and tissue specimens pre-treatment and post-treatment (time of resection), greatly facilitating characterization of the effect of an intervention.40 Using emerging immune monitoring capabilities including platforms such as multiplex IHC and spatial transcriptomics, we can characterize the changes induced in the three-dimensional interface between tumor, stroma and immune infiltrate at baseline and post-treatment, so as to understand predictors of response and spatial determinants of resistance that may be targeted by more optimal combination approaches.41–47 Additionally, single-cell technologies enable us to characterize at the transcriptomic level the complex heterogeneity within the intratumoral lymphoid and myeloid cell lineages, enabling us to resolve very small subpopulations, such as the stem-like T cell populations that we now believe are responsible for the efficacy of PD-1 blockade.48–51 Additionally, through neoantigen calling and incorporation of T cell receptor (TCR) sequencing, we can resolve the tumor-specific T cells from the conglomerate of tumor-infiltrating T cells, the majority of which are bystanders and not reactive to tumor neoantigen.18,52 Resolving and phenotyping the pre-existing T cells, as well as those de novo clones induced by therapy, will enable us to more precisely target our immune modulation to activate this all-important subset, with the aim to increase response to therapy while decreasing toxicity associated with pan-activation of the immune system.
There is increasing understanding of the key role myeloid cells have in promoting a permissive immune milieu to grow, and determining response to immunotherapy. It has long been known that myeloid cells—specifically macrophages and granulocytes—comprise a large portion of the cellular composition of tumors of multiple tumor histologies.48,53,54 Recent deep profiling of the immune compartment within HCC lesions has demonstrated that Kupffer cells, the tissue resident macrophage within the liver, are lacking from the tumor microenvironment, and rather macrophages derived from inflammatory monocytes recruited to the tumor make up the majority of the intratumoral macrophage population.53 These macrophages have a resolutely immunosuppressive phenotype and likely aid in promoting tumor growth, and potentially resistance to therapy. There are numerous agents in clinical development targeting intratumoral macrophages, but many of these agents (e.g. antibodies targeting the CSF1-R receptor present on all macrophages) deplete the entire lineage rather than the specific subset of immunosuppressive monocyte-derived macrophages. Depletion of macrophages capable of priming anti-cancer immunity along with the suppressive subsets is likely one reason for the net neutral benefit that these therapies have demonstrated in clinical trials to date.55
Neoadjuvant Therapies Demonstrate Early Signs of Efficacy
Neoadjuvant as well as adjuvant TKI administration has failed to show benefit in the randomized phase 3 setting.8,56 There is, however, a strong pre-clinical rationale for the combination of TKI with immunotherapy, and this has shown efficacy in the advanced setting.57 One of the first published reports of the use of neoadjuvant immunotherapy in HCC was from a cohort of patients with locally advanced disease, where nivolumab was given in conjunction with the TKI cabozantinib to assess the potential to downstage tumors in order to enable curative-intent resection.16 This trial enrolled 15 patients with HCC for whom upfront surgical resection was not recommended due to high-risk features such as multifocal disease, portal vein invasion, or tumor diameter >10 cm. Patients received a 2-week lead-in with the TKI cabozantinib, followed by 4 treatments with nivolumab added to the TKI, and initial restaging was performed at 10 weeks. Twelve patients successfully underwent resection; in five a major pathologic response (defined as ≥90% necrosis) was noted, with one achieving a pathologic complete response. Patients in this study underwent biopsies at the beginning and end of the 2-week cabozantinib run-in period, enabling assessment of the effect of cabozantinib monotherapy prior to adding PD-1 blockade. After 2 weeks on TKI there was an expansion of peripheral blood effector and memory T cells, and biopsies demonstrated transcriptomic evidence of a more activated immune milieu induced by cabozantinib. After the addition of nivolumab and subsequent resection, the tumors in responders showed a robust immune infiltrate and a preponderance of tertiary lymphoid structures, B cells, and plasma cells when compared with the tumors in patients who failed to achieve a pathologic response.
While the trial with cabozantinib was for patients who were deemed poor resection candidates at presentation, two window-of-opportunity trials for patients deemed resection candidates up-front were recently reported that showed promising pathologic and immunological response to more brief interventions.14,15 One trial treated patients with two doses of the anti-PD-1 antibody cemiplimab, administered 3 weeks apart, followed by surgery as soon as 22 days following the initiation of immunotherapy; all patients underwent pre-treatment biopsies and regular blood collection, and following surgery patients received an additional 8 cycles of adjuvant therapy.14 Notably this trial mandated that patients be up-front surgical candidates; though these were not small isolated lesions, 62% were BCLC-A while the remainder had multifocal disease or other high-risk features. The primary endpoint of this trial was significant tumor necrosis (STN), defined as necrosis of 70% or more of the tumor at time of resection. As with the prior trial, therapy was well tolerated, and all patients went to the operating room; only one experienced a 2-week delay due to the emergence of immunotherapy-related pneumonitis prior to initial planned day of resection. The trial enrolled 21 patients, and 20 tumors were successfully resected; 4 (20%) had achieved STN, with 3 of those 4 achieving a pathologic complete response (pCR). Three additional patients had between 50–70% necrosis of the resected tumor, while the remaining 13 patients had 30% or less necrosis, so an exploratory analysis was pursued looking at patients who had more or less than 50% necrosis. Mandatory core-needle biopsies on this trial enabled direct comparison between pre- and post-treatment tissue. Similar to the data from the trial of nivolumab and cabozantinib, a significant immune infiltrate was seen in responders compared with non-responders, and this increased immune infiltrate was also noted at baseline among responders, suggesting that a pre-existing immune infiltrate—so-called “hot” tumors—may be predictive of rapid response to immunotherapy. Also similar to the previous study, an enrichment in B cells and plasma cells was seen among responders, recapitulating findings from many studies in the advanced setting which have seen a correlation between the presence of B cells and response to checkpoint blockade.15
In this trial the primary endpoint was safety and tolerability; all 27 patients enrolled received 3 pre-operative infusions of nivolumab, administered every 2 weeks, and patients randomized to the combination arm received a single infusion of pre-operative ipilimumab. Following surgery nivolumab was administered every 2 weeks, with those in the combination arm continuing to receive ipilimumab every 6 weeks. Therapy was overall well tolerated, though, as has been seen in the advanced setting, patients receiving the ipilimumab combination had nearly double the rate of serious immunotherapy-related adverse events (irAEs). In this study a major pathologic response (MPR) was also defined as 70% or more necrosis, which was seen in 6 of the 20 patients who underwent resection; 5 of these showed a pCR. Of the 7 patients who did not undergo surgery, the majority were due to disease progression, and none of these cancellations was due to irAEs. This trial had the longest follow-up of the three trials discussed here, and notably, after a median follow-up of 2 years there had been no recurrences seen in patients with MPR, while half of the remaining patients had developed recurrence. This trial similarly found a higher immune infiltrate and increased B cells in MPR patients compared with those without significant pathologic response. Interestingly, similar to the trial with cemiplimab, preexisting immune infiltrate appeared to predict response to nivolumab monotherapy without a significant increase in the number of T cells following therapy, whereas in the nivolumab/ipilimumab combination cohort there was a notable increase in the T and NK cell infiltrate following therapy in the MPR patients that was not seen in non-responders. While this is a small cohort, these data suggest that PD-1 monotherapy may benefit only patients who have pre-existing immune infiltrate, while patients with “cold” tumors may stand to benefit from the more toxic combination with ipilimumab.15 This is notable given the data supporting the potential of CTLA-4 blockade to induce de novo T cell clones.19 Beyond PD-1 and CTLA-4 blockade, there are numerous trials looking at other combinations, including combination therapies often used in the metastatic setting, incorporating antibodies or TKIs targeting VEGF, and novel combinations of PD-1 and targets such as LAG-3 which have shown synergistic efficacy in melanoma (Table 1). These trials and others will enable us to better understand the efficacy of these combinations in the advanced setting, where there is a significant need for biomarkers and more optimized combinations given that no combined therapy to date shows response rates over 50%.
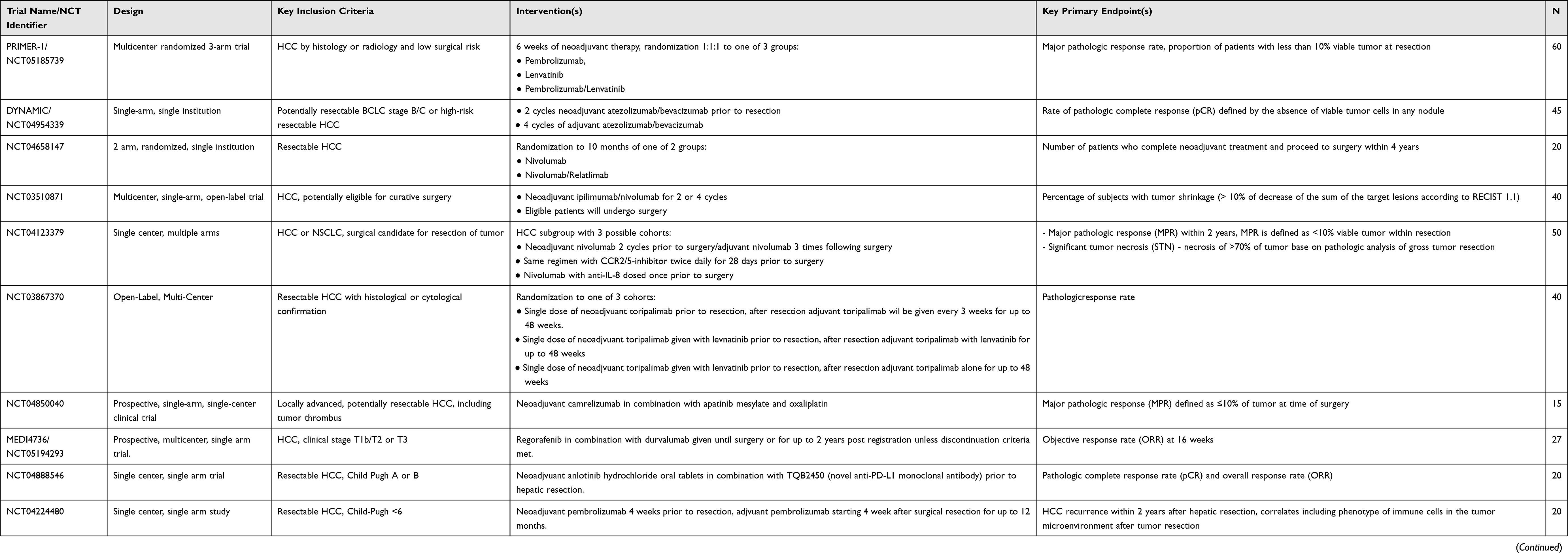 |
Table 1 Neoadjuvant Immunotherapy Trials Underway in HCC |
Challenges in the Neoadjuvant Space
These three trials highlight both the potential of immunotherapy to prolong recurrence-free survival, and the limitations in this approach. One pressing issue that must be resolved to make way for regulatory approval of neoadjuvant agents for HCC is the lack of a validated endpoint. Pathologic endpoints have been validated in tumors such as breast and lung cancer where neoadjuvant chemotherapy is standard, but extrapolating response to cytotoxic therapy to immunotherapy is a stretch. Validating pathologic endpoints such as pCR and MPR anew in the age of immunotherapy will be required. In HCC there is no validated endpoint from previous TKI or chemotherapy trials, so it is not surprising that early trials have disparate endpoints. The cemiplimab trial and the nivolumab±ipilimumab trials chose 70% necrosis as cutoffs, extrapolating from a case series in with patients underwent resection following locoregional therapy with chemoembolization.58 The cabozantinib trial, conversely, borrowed the commonly used MPR definition of 90% or more necrosis seen in NSCLC trials.59 For exploratory purposes the cemiplimab trial noted that 7 patients had 50% or more necrosis while the remaining patients had 30% or less necrosis in the post-treatment tumors, and explored that as a potential cutoff; this 50% cutoff has been used as the definition of MPR in other studies reported in abstract form.60 Traditional radiographic responses are sometimes used in the clinical setting to identify when patients receiving neoadjuvant therapy should proceed to the operating room, but when we are considering very brief interventions, where pseudoprogression is a real possibility, the two neoadjuvant papers’ response data highlight how this type of radiographic assessment must be refined.14,15 The cemiplimab trial had multiple patients who had pathologic responses and evidence on contrast-enhanced MRI of necrosis without significant response as per standard RECIST criteria which rely on tumor size alone. The nivolumab±ipilimumab trial similarly had one patient with frank progression by RECIST on imaging who was found on pathologic assessment to have a pCR with growth of the tumor bed associated with immune infiltrate. Larger trials are warranted to define and validate clinically significant pathologic and/or radiographic responses.
The optimal duration of therapy is also a key question. In the three reports we highlight here, using the respective pathologic endpoints identified, there was an inverse correlation between the time that people received therapy prior to surgery and the rate of pathologic response. Since the aim of neoadjuvant therapy is not so much to kill the tumor as to prime an immune response against micrometastatic disease, a briefer intervention may not only be equally beneficial but also decrease the risk of a pre-operative irAE derailing the scheduled surgery. With PD-1 blockade alone toxicities typically show up after a month or more of therapy, so a brief intervention may mean that should a patient develop a toxicity it would happen after surgery and not risk delaying surgery, while ipilimumab-containing regimens often result in toxicity developing earlier on during treatment. As was the case with one patient in the cemiplimab trial, an early case of pneumonitis immediately prior to surgery delayed resection significantly, and such delays in certain circumstances may lead to patients no longer being surgical candidates. Conversely, in the nivolumab±ipilimumab trial 4 of the 7 patients who did not have surgery were found to have progressive disease on imaging prior to surgery, suggesting that a longer treatment provides a “biological test of time” enabling identification of patients who will rapidly recur, and should therefore be spared the morbidity of a hepatectomy. Some have expressed concern about the use of immunotherapy in HCC patients who may subsequently undergo transplant, as may occur in a patient who is found to have additional small lesions upon reimaging following induction immunotherapy. However, while there is valid concern for complications, the highly immunosuppressive lymphodepleting regimens used in the post-transplant setting will likely abrogate any concern for increased toxicity, and small case series to date have supported the use of immunotherapy in HCC patients who may subsequently undergo transplantation.61
The use of immunotherapy based on biomarkers and/or underlying etiology of HCC must also be investigated to see if these factors should guide decisions about whether to use immunotherapy in the pre-operative setting, and if so which therapy is best. In other malignancies tumor size, histologic classification, and/or lymph node metastasis guides stage and treatment decision in the neoadjuvant space, but in HCC we know that the vast majority of patients with even the smallest tumors (less than 2 cm) with no radiographic evidence will recur postoperatively, and may therefore benefit from perioperative therapy that may help eradicate micrometastatic disease. While a recent report suggested that in patients with advanced non-alcoholic steatohepatitis (NASH)-related HCC, immunotherapy is significantly less efficacious than in patients with other etiologies, this finding has not been fully supported in these albeit small neoadjuvant trials.14,62 In the cemiplimab trial there was significant necrosis seen in tumors resected from both viral (HBV and/or HCV-related) and non-viral (alcohol and/or NASH-related) tumors, suggesting that etiology alone does not define the immune response to cancer, though again, larger trials must be performed to support either conclusion.
While standard biomarkers, such as size or underlying etiology may not prove helpful, in-depth analysis of tissue from these trials will aid in identifying biomarkers, such as baseline T cell infiltration, described in the setting of the ipilimumab trial. These findings support the increased use of diagnostic biopsies not only to confirm the radiographic finding of HCC but also to inform development and personalization of therapeutic approach. There are numerous clinical trials now looking at combining these standard immunotherapies with radiation (e.g. NCT03916627), myeloid modifying agents (e.g. NCT04123379) and dozens of other approaches, and given the vast number of agents in development in the immunotherapy space, in-depth understanding of how these agents work and for whom will be key to tailoring therapy to individual patients.
The Unique Potential to Learn in the Neoadjuvant Setting
While the studies discussed here support the idea that, for at least a subset of patients, preoperative therapy likely portends significant clinical benefit, these studies in which pre- and post-treatment biospecimens are available offer a unique setting to investigate the dynamic effects of these therapies. Groups leading similar trials in other fields have already spearheaded revolutionary characterization of tumor-specific immune cells that will inform our development of immunotherapies that target only the minute subset of lymphocytes capable of tumor-recognition while avoiding the toxicity associated with pan-immune activation.18,52 Through use of spatial transcriptomics and multiplex IHC we will garner further understanding of the immune-tumor-stroma interface which is the target of numerous novel cancer therapeutics. The insights from these trials will benefit development of therapies not only for the minority of patients who are surgical candidates, but also the majority of patients for whom curative intent surgery is not an option.
Conclusion
In conclusion, neoadjuvant immunotherapy is a promising clinical approach for the treatment of resectable HCC, and also offers the opportunity to characterize how novel therapies work in vivo in humans. Trials of adjuvant immunotherapy will read out in the coming year, and this will further help define the optimal perioperative therapy, given that many neoadjuvant trials opt to continue immunotherapy following resection. These perioperative trials will aid us in defining the optimal duration of therapy and biomarkers to guide therapeutic decisions to improve both progression-free and overall survival in HCC patients across stages.
Disclosure
Thomas U Marron reports grants and personal fees from Regeneron, Boehringer Ingelheim, Bristol-Myers Squibb, grants from Merck, and personal fees from AstraZeneca, Celldex, Chimeric Therapeutics, Genentech, Surface, NGMbio, DBV Technologies, and Glenmark Pharma, outside the submitted work. Virginia Corbett reports holding equity in prior 36 months in Pfizer, BristolMyers Squibb, Seagen, and Viatris, outside the submitted work. Miriam Merad reports grants from Regeneron, Inc, outside the submitted work. The authors report no other potential conflicts of interest in relation to this work.
References
1. Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359(4):378–390. doi:10.1056/NEJMoa0708857
2. El-Khoueiry AB, Sangro B, Yau T, et al. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): an open-label, non-comparative, Phase 1/2 dose escalation and expansion trial. Lancet. 2017;389(10088):2492–2502. doi:10.1016/S0140-6736(17)31046-2
3. Yau T, Kang Y-K, Kim T-Y, et al. Efficacy and safety of nivolumab plus ipilimumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib: the CheckMate 040 randomized clinical trial. JAMA Oncol. 2020;6(11):e204564–e204564. doi:10.1001/jamaoncol.2020.4564
4. Zhu AX, Finn RS, Edeline J, et al. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): a non-randomised, open-label phase 2 trial. Lancet Oncol. 2018;19(7):940–952. doi:10.1016/S1470-2045(18)30351-6
5. Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382(20):1894–1905. doi:10.1056/NEJMoa1915745
6. Pinato DJ, Mauri FA, Spina P, et al. Clinical implications of heterogeneity in PD-L1 immunohistochemical detection in hepatocellular carcinoma: the Blueprint-HCC study. Br J Cancer. 2019;120(11):1033–1036. doi:10.1038/s41416-019-0466-x
7. Roayaie S, Obeidat K, Sposito C, et al. Resection of hepatocellular cancer≤ 2 cm: results from two Western centers. Hepatology. 2013;57(4):1426–1435. doi:10.1002/hep.25832
8. Bruix J, Takayama T, Mazzaferro V, et al. Adjuvant sorafenib for hepatocellular carcinoma after resection or ablation (STORM): a phase 3, randomised, double-blind placebo-controlled trial. Lancet Oncol. 2015;16(13):1344–1354. doi:10.1016/S1470-2045(15)00198-9
9. Schmid P, Cortes J, Dent R, et al. VP7-2021: KEYNOTE-522: phase III study of neoadjuvant pembrolizumab+ chemotherapy vs. placebo+ chemotherapy, followed by adjuvant pembrolizumab vs. placebo for early-stage TNBC. Ann Oncol. 2021;32(9):1198–1200. doi:10.1016/j.annonc.2021.06.014
10. Topalian SL, Bhatia S, Amin A, et al. Neoadjuvant nivolumab for patients with resectable Merkel cell carcinoma in the CheckMate 358 trial. J Clin Oncol. 2020;38(22):2476–2487. doi:10.1200/JCO.20.00201
11. Blank CU, Rozeman EA, Fanchi LF, et al. Neoadjuvant versus adjuvant ipilimumab plus nivolumab in macroscopic stage III melanoma. Nat Med. 2018;24(11):1655–1661. doi:10.1038/s41591-018-0198-0
12. Forde PM, Anagnostou V, Sun Z, et al. Durvalumab with platinum-pemetrexed for unresectable pleural mesothelioma: survival, genomic and immunologic analyses from the phase 2 PrE0505 trial. Nat Med. 2021;27(11):1910–1920. doi:10.1038/s41591-021-01541-0
13. Forde PM, Spicer J, Lu S, et al. Abstract CT003: nivolumab (NIVO)+ platinum-doublet chemotherapy (chemo) vs chemo as neoadjuvant treatment (tx) for resectable (IB-IIIA) non-small cell lung cancer (NSCLC) in the phase 3 CheckMate 816 trial. Cancer Res. 2021;81(13_Supplement):CT003–CT003. doi:10.1158/1538-7445.AM2021-CT003
14. Marron TU, Fiel MI, Hamon P, et al. Neoadjuvant cemiplimab for resectable hepatocellular carcinoma: a single-arm, open-label, phase 2 trial. Lancet Gastroenterol Hepatol. 2022;7(3):219–229. doi:10.1016/S2468-1253(21)00385-X
15. Kaseb AO, Hasanov E, Cao HST, et al. Perioperative nivolumab monotherapy versus nivolumab plus ipilimumab in resectable hepatocellular carcinoma: a randomised, open-label, phase 2 trial. Lancet Gastroenterol Hepatol. 2022;7(3):208–218. doi:10.1016/S2468-1253(21)00427-1
16. Ho WJ, Zhu Q, Durham J, et al. Neoadjuvant cabozantinib and nivolumab converts locally advanced HCC into resectable disease with enhanced antitumor immunity. Nat Cancer. 2021;2(9):891–903. doi:10.1038/s43018-021-00234-4
17. Pinato DJ, Fessas P, Sapisochin G, Marron TU. Perspectives on the neoadjuvant use of immunotherapy in hepatocellular carcinoma. Hepatology. 2020;74(1):483–490.
18. Forde PM, Chaft JE, Smith KN, et al. Neoadjuvant PD-1 blockade in resectable lung cancer. N Engl J Med. 2018;378(21):1976–1986. doi:10.1056/NEJMoa1716078
19. Cascone T, William WN, Weissferdt A, et al. Neoadjuvant nivolumab or nivolumab plus ipilimumab in operable non-small cell lung cancer: the phase 2 randomized NEOSTAR trial. Nat Med. 2021;27(3):504–514. doi:10.1038/s41591-020-01224-2
20. Huang AC, Orlowski RJ, Xu X, et al. A single dose of neoadjuvant PD-1 blockade predicts clinical outcomes in resectable melanoma. Nat Med. 2019;25(3):454–461. doi:10.1038/s41591-019-0357-y
21. Rusch VW, Chaft JE, Johnson B, et al. Neoadjuvant atezolizumab in resectable non-small cell lung cancer (NSCLC): initial results from a multicenter study (LCMC3). Am Soc Clin Oncol. 2018;36(15_suppl):8541. doi:10.1200/JCO.2018.36.15_suppl.8541
22. Uppaluri R, Campbell KM, Egloff AM, et al. Neoadjuvant and adjuvant pembrolizumab in resectable locally advanced, human papillomavirus-unrelated head and neck cancer: a multicenter, Phase 2 trial. medRxiv. 2020;26:5140–5152.
23. Schmid P, Cortes J, Pusztai L, et al. Pembrolizumab for early triple-negative breast cancer. N Engl J Med. 2020;382(9):810–821. doi:10.1056/NEJMoa1910549
24. Losic B, Craig AJ, Villacorta-Martin C, et al. Intratumoral heterogeneity and clonal evolution in liver cancer. Nat Commun. 2020;11(1):291. doi:10.1038/s41467-019-14050-z
25. Nault JC, Villanueva A. Intratumor molecular and phenotypic diversity in hepatocellular carcinoma. Clin Cancer Res. 2015;21(8):1786–1788. doi:10.1158/1078-0432.CCR-14-2602
26. Topalian SL, Hodi FS, Brahmer JR, et al. Five-year survival and correlates among patients with advanced melanoma, renal cell carcinoma, or non-small cell lung cancer treated with nivolumab. JAMA Oncol. 2019;5(10):1411. doi:10.1001/jamaoncol.2019.2187
27. Huang AC, Postow MA, Orlowski RJ, et al. T-cell invigoration to tumour burden ratio associated with anti-PD-1 response. Nature. 2017;545(7652):60–65. doi:10.1038/nature22079
28. Robert C, Ribas A, Hamid O, et al. Durable complete response after discontinuation of pembrolizumab in patients with metastatic melanoma. J Clin Oncol. 2018;36(17):1668–1674. doi:10.1200/JCO.2017.75.6270
29. Tabrizian P, Jibara G, Shrager B, et al. Recurrence of hepatocellular cancer after resection: patterns, treatments, and prognosis. Ann Surg. 2015;261(5):947–955. doi:10.1097/SLA.0000000000000710
30. Roayaie S, Jibara G, Tabrizian P, et al. The role of hepatic resection in the treatment of hepatocellular cancer. Hepatology. 2015;62(2):440–451. doi:10.1002/hep.27745
31. Wakelee HA, Altorki NK, Zhou C, et al. IMpower010: primary results of a phase III global study of atezolizumab versus best supportive care after adjuvant chemotherapy in resected stage IB-IIIA non-small cell lung cancer (NSCLC). J Clin Oncol. 2021;39(15_suppl):8500. doi:10.1200/JCO.2021.39.15_suppl.8500
32. Zimmer L, Livingstone E, Hassel JC, et al. Adjuvant nivolumab plus ipilimumab or nivolumab monotherapy versus placebo in patients with resected stage IV melanoma with no evidence of disease (IMMUNED): a randomised, double-blind, placebo-controlled, phase 2 trial. Lancet. 2020;395(10236):1558–1568. doi:10.1016/S0140-6736(20)30417-7
33. Garris CS, Arlauckas SP, Kohler RH, et al. Successful anti-PD-1 cancer immunotherapy requires T cell-dendritic cell crosstalk involving the cytokines IFN-gamma and IL-12. Immunity. 2018;49(6):1148–1161 e7. doi:10.1016/j.immuni.2018.09.024
34. Liu J, Blake SJ, Yong MCR, et al. Improved efficacy of neoadjuvant compared to adjuvant immunotherapy to eradicate metastatic disease. Cancer Discov. 2016;6(12):1382–1399. doi:10.1158/2159-8290.CD-16-0577
35. Tang F, Tie Y, Tu C, et al. Surgical trauma-induced immunosuppression in cancer: recent advances and the potential therapies. Clin Transl Med. 2020;10(1):199–223. doi:10.1002/ctm2.24
36. Jia R, Zhou M, Tuttle CSL, et al. Immune capacity determines outcome following surgery or trauma: a systematic review and meta-analysis. Eur J Trauma Emerg Surg. 2020;46(5):979–991. doi:10.1007/s00068-019-01271-6
37. Fitzgerald BG, Galsky MD, Marron TU. The cutting edge: leveraging pre-surgical immunotherapy trials to understand therapeutic mechanisms. Immuno-Oncol Insights. 2022;3(3):81–91. doi:10.18609/ioi.2022.011
38. Cheng X, Zhang H, Hamad A, et al. Surgery-mediated tumor-promoting effects on the immune microenvironment. Semin Cancer Biol. 2022. doi:10.1016/j.semcancer.2022.01.006
39. Bakos O, Lawson C, Rouleau S, et al. Combining surgery and immunotherapy: turning an immunosuppressive effect into a therapeutic opportunity. J Immunother Cancer. 2018;6(1):86. doi:10.1186/s40425-018-0398-7
40. Topalian SL, Taube JM, Pardoll DM. Neoadjuvant checkpoint blockade for cancer immunotherapy. Science. 2020;367:6477. doi:10.1126/science.aax0182
41. Remark R, Merghoub T, Grabe N, et al. In-depth tissue profiling using multiplexed immunohistochemical consecutive staining on single slide. Sci Immunol. 2016;1(1):aaf6925. doi:10.1126/sciimmunol.aaf6925
42. Goltsev Y, Samusik N, Kennedy-Darling J, et al. Deep profiling of mouse splenic architecture with CODEX multiplexed imaging. Cell. 2018;174(4):968–981. e15. doi:10.1016/j.cell.2018.07.010
43. Giesen C, Wang HAO, Schapiro D, et al. Highly multiplexed imaging of tumor tissues with subcellular resolution by mass cytometry. Nat Methods. 2014;11(4):417–422. doi:10.1038/nmeth.2869
44. Lin J-R, Izar B, Wang S, et al. Highly multiplexed immunofluorescence imaging of human tissues and tumors using t-CyCIF and conventional optical microscopes. Elife. 2018;7. doi:10.7554/eLife.31657
45. Zhuang X. Spatially resolved single-cell genomics and transcriptomics by imaging. Nat Methods. 2021;18(1):18–22. doi:10.1038/s41592-020-01037-8
46. Merritt CR, Ong GT, Church SE, et al. Multiplex digital spatial profiling of proteins and RNA in fixed tissue. Nat Biotechnol. 2020;38(5):586–599. doi:10.1038/s41587-020-0472-9
47. Ståhl PL, Salmén F, Vickovic S, et al. Visualization and analysis of gene expression in tissue sections by spatial transcriptomics. Science. 2016;353(6294):78–82. doi:10.1126/science.aaf2403
48. Lavin Y, Kobayashi S, Leader A, et al. Innate immune landscape in early lung adenocarcinoma by paired single-cell analyses. Cell. 2017;169(4):750–765. e17. doi:10.1016/j.cell.2017.04.014
49. Leader AM, Grout JA, Chang C, et al. CITEseq analysis of non-small-cell lung cancer lesions reveals an axis of immune cell activation associated with tumor antigen load and TP53 mutations. bioRxiv. 2020. doi:10.1101/2020.07.16.207605
50. Giladi A, Cohen M, Medaglia C, et al. Dissecting cellular crosstalk by sequencing physically interacting cells. Nat Biotechnol. 2020;38(5):629–637. doi:10.1038/s41587-020-0442-2
51. Rose SA, Wroblewska A, Dhainaut M, et al. A microRNA expression and regulatory element activity atlas of the mouse immune system. Nat Immunol. 2021;22(7):914–927. doi:10.1038/s41590-021-00944-y
52. Caushi JX, Zhang J, Ji Z, et al. Transcriptional programs of neoantigen-specific TIL in anti-PD-1-treated lung cancers. Nature. 2021;596(7870):126–132. doi:10.1038/s41586-021-03752-4
53. Hamon P, Magen A, Cohen M, et al. Characterization of molecular and spatial diversity of macrophages in hepatocellular carcinoma. Cancer Res. 2021;81:64.
54. Hegde S, Leader AM, Merad M. MDSC: markers, development, states, and unaddressed complexity. Immunity. 2021;54(5):875–884. doi:10.1016/j.immuni.2021.04.004
55. Ordentlich P. Clinical evaluation of colony-stimulating factor 1 receptor inhibitors. Semin Immunol. 2021;54:101514. doi:10.1016/j.smim.2021.101514
56. Williet N, Dubreuil O, Boussaha T, et al. Neoadjuvant sorafenib combined with gemcitabine plus oxaliplatin in advanced hepatocellular carcinoma. World J Gastroenterol. 2011;17(17):2255. doi:10.3748/wjg.v17.i17.2255
57. Zhu AX, Finn RS, Ikeda M, et al. A phase Ib study of lenvatinib (LEN) plus pembrolizumab (PEMBRO) in unresectable hepatocellular carcinoma (uHCC). Am Soc Clin Oncol. 2020;30:v286–v287.
58. Allard MA, Sebagh M, Ruiz A, et al. Does pathological response after transarterial chemoembolization for hepatocellular carcinoma in cirrhotic patients with cirrhosis predict outcome after liver resection or transplantation? J Hepatol. 2015;63(1):83–92. doi:10.1016/j.jhep.2015.01.023
59. Hellmann MD, Chaft JE, William WN, et al. Pathological response after neoadjuvant chemotherapy in resectable non-small-cell lung cancers: proposal for the use of major pathological response as a surrogate endpoint. Lancet Oncol. 2014;15(1):e42–e50. doi:10.1016/S1470-2045(13)70334-6
60. Xia Y, Wang P, Pu L, et al. Preliminary Efficacy and Safety of Perioperative Treatment of Camrelizumab Combined With Apatinib in Resectable Hepatocellular Carcinoma (HCC): A Prospective Phase II Study. Wolters Kluwer Health; 2021.
61. Tabrizian P, Florman SS, Schwartz ME. PD-1 inhibitor as bridge therapy to liver transplantation? Am J Transplant. 2020;20(1):220–230. doi:10.1111/ajt.15576
62. Pfister D, Núñez NG, Pinyol R, et al. NASH limits anti-tumour surveillance in immunotherapy-treated HCC. Nature. 2021;592(7854):450–456. doi:10.1038/s41586-021-03362-0
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.