Back to Journals » Cancer Management and Research » Volume 17

Neoadjuvant Docetaxel-Carboplatin-Trastuzumab Therapy in HER2-Positive Breast Cancer: A Single-Center Experience from Vietnam
Authors Nguyen Quang H, Dao Manh P, Nguyen Thi Hoa M, Tran Thi D
Received 1 May 2025
Accepted for publication 22 August 2025
Published 31 August 2025 Volume 2025:17 Pages 1851—1858
DOI https://doi.org/10.2147/CMAR.S537882
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sanjeev K. Srivastava
Hung Nguyen Quang,1,2 Phuong Dao Manh,1,2 Mai Nguyen Thi Hoa,1 Doan Tran Thi3
1Nuclear Medicine and Oncology Center, Bach Mai Hospital, Hanoi, Vietnam; 2Oncology Center, Phenikaa University Hospital, Hanoi, Vietnam; 3Department of Metabolic and Cardiovascular Disorders Treatment, National Hospital of Endocrinology, Hanoi, Vietnam
Correspondence: Hung Nguyen Quang, Oncology Center, Phenikaa University Hospital, Group 5 Xuan Phuong Ward, Hanoi, Vietnam, Tel +84 909 572 686, Email [email protected]
Purpose: To evaluate the efficacy of neoadjuvant therapy and identify associated factors influencing treatment response in patients with HER2-positive breast cancer.
Subjects and Methods: A prospective, longitudinal study of 40 women with a mean age of 50.68 ± 10.53 years diagnosed with HER2-positive breast cancer. All patients received neoadjuvant treatment using Docetaxel-Carboplatin-Trastuzumab (TCH) regimens. These patients were evaluated for treatment response based on the Response Evaluation Criteria In Solid Tumors (RECIST) after six 21-day treatment cycles.
Results: The proportion of good responders was 45.0% (18/40 patients). Younger age, earlier clinical stage, and lower baseline serum CA15-3 levels were significantly associated with a better response (p < 0.05). The incidence of adverse events was also significantly lower in good responders (p < 0.05). Multivariate analysis identified younger age and lower CA15-3 concentration as independent predictors of favorable response, with area under the Receiver Operating Characteristic (ROC) curves (AUC) of 0.758 and 0.821, respectively (p = 0.006 and p = 0.001).
Conclusion: Neoadjuvant treatment using the Docetaxel-Carboplatin-Trastuzumab regimen provides favorable clinical outcomes in HER2-positive breast cancer patients. Baseline CA15-3 levels may serve as a useful predictor of treatment response.
Keywords: breast cancer, HER2-positive, neoadjuvant therapy, cancer antigen 15-3
Introduction
Breast cancer is a heterogeneous group of malignant tumors originating in the mammary gland and remains a significant global health burden, particularly among women.1,2 According to a 2022 survey of 185 countries, there were 2.3 million new cases and 670,000 deaths due to breast cancer. Annual incidence rates increased by 1–5% in half of the surveyed countries, with projections indicating a 38% increase in new cases and a 68% increase in deaths by 2050.3 Some Asian countries, including Vietnam, lack comprehensive national data on breast cancer incidence and mortality, primarily due to the absence of large-scale epidemiological surveys.4,5
Breast cancer development involves a complex interplay of genetic predisposition, environmental exposures, lifestyle factors, chronic inflammation, and oxidative stress, all of which contribute to hormonal imbalance and immunosuppression.6,7 Early diagnosis and radical surgical resection remain the cornerstone of treatment. Multimodal approaches, including surgery, chemotherapy, radiation, and targeted therapies, are considered standard care based on disease subtype and stage.8–10
HER2-positive breast cancer, characterized by overexpression of the human epidermal growth factor receptor 2, accounts for approximately 15–20% of cases and is associated with aggressive behavior, increased cell proliferation, angiogenesis, and poor prognosis.11,12 Neoadjuvant therapy combining chemotherapy and HER2-targeted agents has demonstrated efficacy in downstaging tumors, facilitating curative surgery.13–15 However, implementation remains challenging in low-resource settings due to financial constraints. This study aimed to evaluate the clinical outcomes and predictive factors associated with the Docetaxel-Carboplatin-Trastuzumab (TCH) neoadjuvant regimen in Vietnamese patients with HER2-positive breast cancer.
Subjects and Methods
Study Design and Population
This was a prospective, longitudinal, non-interventional study involving female patients diagnosed with HER2-positive breast cancer who received neoadjuvant therapy with the TCH regimen at the Nuclear Medicine and Oncology Center, Bach Mai Hospital (Hanoi, Vietnam) from January 2023 to January 2024. Exclusion criteria included: age < 18 years; stage IV breast cancer; prior treatment for breast cancer; use of alternative neoadjuvant regimens; concurrent malignancies; acute infections; suspected surgical pathology; non-compliance with treatment protocol; pregnancy or lactation.
A total of 40 eligible patients provided informed consent and were enrolled in the study.
Neoadjuvant Treatment Protocol and Outcome Evaluation
Patients received the following regimen: Docetaxel 75 mg/m² and Carboplatin (AUC = 6 mg/mL/min) intravenously on day 1; Trastuzumab loading dose 8 mg/kg on day 1 of cycle 1, followed by 6 mg/kg in subsequent cycles. Treatment was administered every 21 days for a total of six cycles.
Baseline clinical and laboratory data were recorded prior to treatment initiation. Patients were re-evaluated every three cycles. Adverse events were monitored and recorded throughout the treatment period. Venous blood samples were collected at baseline and after completion of the sixth cycle to assess complete blood count, serum biochemistry, liver and renal function, and tumor markers. Additional assessments included liver ultrasound, ECG, echocardiography, and neuromuscular studies.
Treatment response was assessed according to RECIST criteria.16 Patients were categorized into two groups:
- Good responders (n = 18): patients achieving clinical complete response (cCR) and eligible for curative surgery.
- Poor responders (n = 22): patients with partial response, stable disease, or progressive disease without indication for radical surgery.
Statistical Analysis
Continuous variables with a normal distribution were presented as mean ± standard deviation and compared using the Student’s t-test or one-way ANOVA, as appropriate. Non-normally distributed variables were expressed as the median and interquartile range (IQR), with group comparisons conducted using the Mann–Whitney U-test or Kruskal–Wallis test. Categorical variables were summarized as frequencies and percentages and analyzed using the Chi-square test or Fisher’s exact test, as appropriate.
Multivariate logistic regression was employed to identify independent predictors of treatment response. The predictive performance was assessed using receiver operating characteristic (ROC) curve analysis, and the area under the curve (AUC) was reported.
All statistical analyses were conducted using SPSS version 22.0 (Chicago, IL, USA), with a p-value of < 0.05 considered statistically significant.
Results
Table 1 shows that 45.0% of patients achieved a good response to treatment. Compared to the poor response group, patients with a good response had a lower mean age, a lower menopausal rate, a lower incidence of stage 2 and 3 disease, and lower serum CA15-3 levels. These differences were statistically significant (p < 0.05).
 |
Table 1 Clinical and Paraclinical Comparison Between Good and Poor Treatment Response Groups |
Table 2 presents a comparative analysis of adverse event incidence between patients with good and poor treatment responses. A wide range of side effects was observed, with 100% of patients experiencing anorexia and alopecia and 95% reporting nausea and vomiting. Regarding organ-specific toxicity, 100% of patients experienced at least one manifestation of hematologic toxicity, while neurotoxicity and hepatotoxicity were observed in 80% and 15% of patients, respectively. No instances of renal or cardiac toxicity were reported. Notably, the frequency of both side effects and hematologic toxicity was significantly lower in the good response group compared to the poor response group (p < 0.05).
 |
Table 2 Comparison of Patient Rates According to Adverse Events Between the Good and Poor Response Groups |
Among the variables analyzed, younger age (OR = 0.815; 95% CI: 0.701–0.949; p = 0.008) and lower CA15-3 levels (OR = 0.890; 95% CI: 0.798–0.992; p = 0.036) were found to be statistically significant independent predictors of good response to treatment (p < 0.05). Other variables, including Stage III disease and decreased neutrophil count, did not reach statistical significance.
Figure 1 illustrates that age and CA15-3 levels are potential predictors of favorable treatment response in patients with HER2-positive breast cancer. Notably, CA15-3 demonstrated high predictive value, with an area under the curve (AUC) of 0.821 and a statistically significant p-value < 0.001.
 |
Figure 1 ROC curves of some tumor factors predict a good treatment response (Blue line: Age; Red line: CA15-3; Black line: Reference line). Notes: Age: AUC = 0.758; p = 0.006; cut-off value = 48.5 years; sensitivity = 77.3%; specificity = 66.7%; CA15-3: AUC = 0.821; p = 0.001; cut-off value = 17.75 U/mL; sensitivity = 77.3%; specificity = 88.9%. |
Discussion
Outcomes of Neoadjuvant Treatment with the Docetaxel-Carboplatin-Trastuzumab Regimen in Patients with HER2-Positive Breast Cancer
Radical surgery remains the cornerstone in the management of breast cancer. Depending on the stage of the disease, patients may undergo lumpectomy, lumpectomy combined with mastectomy, or lumpectomy/mastectomy with regional lymph node dissection.17,18 In some instances, patients may present with locally advanced disease at the time of initial diagnosis, necessitating tumor downstaging prior to surgery. Neoadjuvant therapy has been widely adopted to achieve this goal and increase the rate of breast conservation. Adding trastuzumab to neoadjuvant therapy has demonstrated significant clinical benefits, including the pathological complete response (pCR) rate, promoting tumor shrinkage, and improving breast-conservation outcomes in HER2-positive breast cancer.13,19,20 Targeting the HER2 pathway with trastuzumab has increased the pathological complete response rate. The Docetaxel-Carboplatin-Trastuzumab (TCH) regimen demonstrates high efficacy and safety, with favorable 5-year disease-free survival and overall survival outcomes in patients with HER2-positive breast cancer.21 Trastuzumab is now established as a key therapeutic agent in both early-stage and metastatic HER2-positive breast cancer due to its capacity to disrupt HER2 signaling and modulate the tumor immune microenvironment.22,23 Carboplatin, a platinum-based agent, enhances the immunogenic effects of chemotherapy and provides clinical benefit in early HER2-positive breast cancer.24,25 Docetaxel is frequently employed as part of first-line combination therapy for patients with HER-2-positive metastatic breast cancer, attributed to its potent antitumor activity.26
Our study supports these findings, reporting a clinical complete response (cCR) rate of 45.0% (18 out of 40 patients; Table 1). Regarding toxicity, both systemic and organ-specific adverse events were observed, with a safety profile consistent with previously published studies.21,27 Our results confirm that neoadjuvant therapy with the Docetaxel-Carboplatin-Trastuzumab regimen yields favorable efficacy and safety outcomes in HER2-positive breast cancer. We believe that this treatment approach demonstrates promising outcomes and may serve as a valuable reference for clinicians worldwide, particularly in Vietnam, in the management of patients with HER2-positive breast cancer.
Predictive Factors Associated with Good Treatment Response
Despite the clinical benefits of the Docetaxel-Carboplatin-Trastuzumab regimen, its use in Vietnam remains limited due to the high cost. In our study, 45.0% (18/40) of patients responded favorably (Table 1). Upon comparing clinical characteristics between responders and non-responders, we found that the good response group was characterized by younger age, earlier disease stage, fewer hematologic toxicities, and lower serum CA15-3 levels (Tables 1 and 2).
Multivariate analysis identified younger age and reduced CA15-3 levels as independent predictors of favorable response (Table 3). Specifically, patients aged < 48 years (p = 0.006) or with CA15-3 levels < 17.75 U/mL (p = 0.001) were significantly more likely to benefit from neoadjuvant treatment with this regimen (Figure 1).
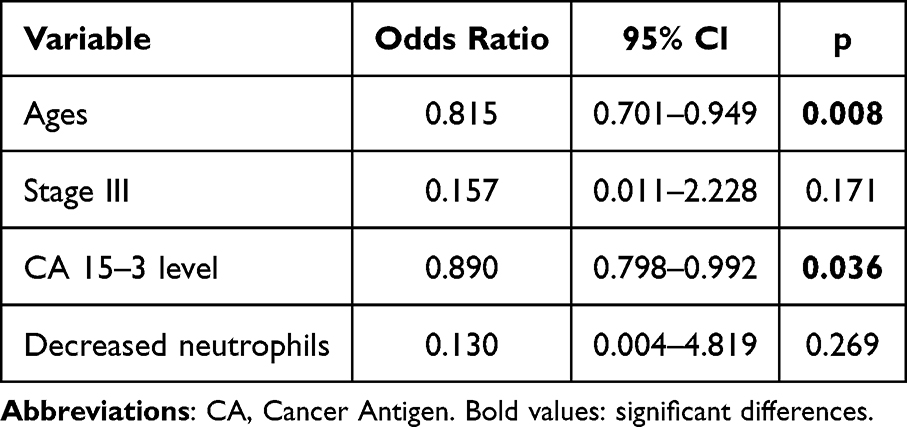 |
Table 3 Multivariate Analysis of Independent Tumor Factors Associated with Good Treatment Response |
Various clinical and paraclinical markers have been explored as predictors of treatment response. For instance, Wang L. et al identified elevated IL-6, NK-T cells, the CD4+/CD8+ T-cell ratio, and tumor-infiltrating lymphocytes as predictive markers for response to six cycles of neoadjuvant docetaxel, carboplatin, and trastuzumab in 42 HER2-positive patients.28 More recently, Bion M. et al suggested Trop-2 expression as a potential biomarker of resistance to neoadjuvant chemotherapy with dual HER2 blockers in a cohort of 41 HER2-positive breast cancer patients.29 Our findings suggest that serum CA15-3 levels and patient age can serve as accessible, cost-effective indicators for predicting response to neoadjuvant therapy with Docetaxel-Carboplatin-Trastuzumab regimen in HER2-positive breast cancer patients.
Our study results have achieved the objectives, however, the study has some limitations as follows: The sample size was relatively small, comprising only 40 cases from a single center, which limits the generalizability of the findings. Furthermore, the follow-up duration was short, and pathological complete response (pCR) was not assessed, preventing an evaluation of disease recurrence.
Conclusion
Neoadjuvant therapy with the Docetaxel-Carboplatin-Trastuzumab regimen in 40 patients with HER2-positive breast cancer demonstrated favorable clinical outcomes. The overall good response rate was 45.0% (18/40 patients). A lower plasma CA15-3 level was significantly associated with treatment efficacy, with an AUC of 0.821 and a p-value of 0.001.
Data Sharing Statement
The data presented in this study are available on request from the corresponding author.
Ethics Approval
This study was approved by the Ethical Committee of Bach Mai Hospital (No: 4676/QĐ-BVBM).
Animals did not participate in this research. All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2008.
Consent for Publication
Informed consent was obtained from all the participants.
Acknowledgments
In this study, we were strongly supported by our local Hospital and university to complete our research.
Funding
No funds, grants, or other support was received.
Disclosure
The authors have no relevant financial or non-financial interests to disclose.
References
1. Veronesi U, Boyle P, Goldhirsch A, et al. Breast cancer. Lancet. 2005;365(9472):1727–1741. doi:10.1016/S0140-6736(05)66546-4
2. Merino Bonilla JA, Torres Tabanera M, Ros Mendoza LH. Breast cancer in the 21st century: from early detection to new therapies. Radiologia. 2017;59(5):368–379. doi:10.1016/j.rx.2017.06.003
3. Kim J, Harper A, McCormack V, et al. Global patterns and trends in breast cancer incidence and mortality across 185 countries. Nat Med. 2025;31:1154–1162. doi:10.1038/s41591-025-03502-3
4. Ngan TT, Jenkins C, Minh HV, et al. Breast cancer screening practices among Vietnamese women and factors associated with clinical breast examination uptake. PLoS One. 2022;17(5):e0269228. doi:10.1371/journal.pone.0269228
5. A KCB, Htay ZW, Parvin R, et al. Prevalence of breast cancer screening in alia: systematic review and meta-analysis. Asian Pac J Cancer Prev. 2024;25(10):3379–3391. doi:10.31557/APJCP.2024.25.10.3379
6. Harbeck N, Gnant M. Breast cancer. Lancet. 2017;389(10074):1134–1150. doi:10.1016/S0140-6736(16)31891-8
7. Xiong X, Zheng LW, Ding Y, et al. Breast cancer: pathogenesis and treatments. Signal Transduct Target Ther. 2025;10(1):49. doi:10.1038/s41392-024-02108-4
8. Smith BD, Bellon JR, Blitzblau R, et al. Radiation therapy for the whole breast: executive summary of an American Society for Radiation Oncology (ASTRO) evidence-based guideline. Pract Radiat Oncol. 2018;8(3):145–152. doi:10.1016/j.prro.2018.01.012
9. McGuire KP, Mamounas EP. Management of hereditary breast cancer: ASCO, ASTRO, and SSO Guideline. Ann Surg Oncol. 2020;27(6):1721–1723. doi:10.1245/s10434-020-08396-8
10. Korde LA, Somerfield MR, Carey LA, et al. Neoadjuvant chemotherapy, endocrine therapy, and targeted therapy for breast cancer: ASCO guideline. J Clin Oncol. 2021;39(13):1485–1505. doi:10.1200/JCO.20.03399
11. Puglisi F, Fontanella C, Amoroso V, et al. Current challenges in HER2-positive breast cancer. Crit Rev Oncol Hematol. 2016;98:211–221. doi:10.1016/j.critrevonc.2015.10.016
12. Pan L, Li J, Xu Q, et al. HER2/PI3K/AKT pathway in HER2-positive breast cancer: a review. Medicine. 2024;103(24):e38508. doi:10.1097/MD.0000000000038508
13. Takada M, Toi M. Neoadjuvant treatment for HER2-positive breast cancer. Chin Clin Oncol. 2020;9(3):32. doi:10.21037/cco-20-123
14. Stanowicka-Grada M, Senkus E. Anti-HER2 drugs for the treatment of advanced her2 positive breast cancer. Curr Treat Options Oncol. 2023;24(11):1633–1650. doi:10.1007/s11864-023-01137-5
15. Li X, Zhang X, Yin S, et al. Challenges and prospects in HER2-positive breast cancer-targeted therapy. Crit Rev Oncol Hematol. 2025;207:104624. doi:10.1016/j.critrevonc.2025.104624
16. Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–247. doi:10.1016/j.ejca.2008.10.026
17. Bertozzi N, Pesce M, Santi PL, et al. Oncoplastic breast surgery: comprehensive review. Eur Rev Med Pharmacol Sci. 2017;21(11):2572–2585.
18. Gilmour A, Cutress R, Gandhi A, et al. Oncoplastic breast surgery: a guide to good practice. Eur J Surg Oncol. 2021;47(9):2272–2285. doi:10.1016/j.ejso.2021.05.006
19. Wuerstlein R, Harbeck N. Neoadjuvant therapy for HER2-positive breast cancer. Rev Recent Clin Trials. 2017;12(2):81–92. doi:10.2174/1574887112666170202165049
20. Sheikh F, Nazir A, Yasmeen S, et al. Pathologic complete response in HER2-positive breast cancer patients receiving trastuzumab in neoadjuvant setting. J Coll Physicians Surg Pak. 2019;29(2):159–163. doi:10.29271/jcpsp.2019.02.159
21. Wu D, Xiong L. Efficacy analysis of trastuzumab, carboplatin and docetaxel in HER-2-positive breast cancer patients. Oncol Lett. 2020;19(3):2539–2546. doi:10.3892/ol.2020.11277
22. Shi SJ, Wang LJ, Yu B, et al. LncRNA-ATB promotes trastuzumab resistance and invasion-metastasis cascade in breast cancer. Oncotarget. 2015;6:11652–11663. doi:10.18632/oncotarget.3457
23. Perez EA, Barrios C, Eiermann W, et al. Trastuzumab emtansine with or without pertuzumab versus trastuzumab plus taxane for human epidermal growth factor receptor 2-positive, advanced breast cancer: primary results from the Phase III MARIANNE study. J Clin Oncol. 2017;35:141–148. doi:10.1200/JCO.2016.67.4887
24. von Minckwitz G, Schneeweiss A, Loibl S, et al. Neoadjuvant carboplatin in patients with triple-negative and HER2-positive early breast cancer (GeparSixto; GBG 66): a randomised Phase 2 trial. Lancet Oncol. 2014;15(7):747–756. doi:10.1016/S1470-2045(14)70160-3
25. Ho GY, Woodward N, Coward JI. Cisplatin versus carboplatin: comparative review of therapeutic management in solid malignancies. Crit Rev Oncol Hematol. 2016;102:37–46. doi:10.1016/j.critrevonc.2016.03.014
26. Leung HW, Chan AL, Muo CH, et al. Cost-effectiveness of pertuzumab combined with trastuzumab and docetaxel as a first-line treatment for HER-2 positive metastatic breast cancer. Expert Rev Pharmacoecon Outcomes Res. 2018;18:207–213. doi:10.1080/14737167.2018.1386559
27. Feng QZ, Chen XZ, Sun J, et al. Analysis of the effect of trastuzumab combined with docetaxel on serum tumor markers in the treatment of HER-2 positive breast cancer and factors influencing therapeutic efficacy. Cancer Manag Res. 2021;13:8077–8084. doi:10.2147/CMAR.S334680
28. Wang L, Zhang X, Ma X, et al. Elevated Sera IL-6 and NK-T cells associated with increased pathological complete response in her2-positive breast cancer with carboplatin-based neoadjuvant therapy. Altern Ther Health Med. 2023;29(3):246–253.
29. Gion M, García-Mosquera JJ, Pérez-García JM, et al. Correlation between trophoblast cell-surface antigen-2 (Trop-2) expression and pathological complete response in patients with HER2-positive early breast cancer treated with neoadjuvant docetaxel, carboplatin, trastuzumab, and pertuzumab. Breast Cancer Res Treat. 2024;205(3):589–598. doi:10.1007/s10549-024-07292-z
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.