Back to Journals » Risk Management and Healthcare Policy » Volume 16
Needle-Stick Injuries in Ophthalmic Practice
Authors Alfarhan A ![]() , Al-Swailem S
, Al-Swailem S ![]() , Alobaid M, Ahmad K
, Alobaid M, Ahmad K ![]() , Khan R
, Khan R ![]()
Received 24 March 2023
Accepted for publication 4 August 2023
Published 23 August 2023 Volume 2023:16 Pages 1667—1677
DOI https://doi.org/10.2147/RMHP.S409326
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Abdulrahman Alfarhan,1 Samar Al-Swailem,2,3 Mohannad Alobaid,4 Khabir Ahmad,3 Ruhi Khan5
1Fellowship and Residency Training Program, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia; 2Anterior Segment Division, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia; 3Research Department, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia; 4Department of Ophthalmology, King Saud Medical City, Riyadh, Saudi Arabia; 5Medicine Department, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia
Correspondence: Abdulrahman Alfarhan, King Khaled Eye Specialist Hospital, Riyadh, 14611, Saudi Arabia, Email [email protected]
Purpose: Needle-stick injuries (NSI) are a prominent route by which blood-borne infections are transmitted. The unique microsurgical nature of ophthalmic practice constitutes an additional risk to sustain injury. This study aimed to identify the epidemiological profile of needle-stick injuries in a tertiary eye center and to evaluate the implemented safety policy in preventing sharp injuries.
Methods: This was a retrospective cross-sectional study of all sharp injuries that occurred at King Khalid Eye Specialist Hospital (KKESH). Data on all reported sharp injury incidents from 2013 to 2021 were collected. The mechanisms of injury, context, location, and type of prick were collected and analyzed. Also, this study involved an institution-based survey for all ophthalmic staff.
Results: Two hundred and one sharp injury incidents were reported over 9 years. Physicians sustained 46.8% (n=94) of injuries, followed by nurses and ophthalmic technicians, 40.8% (n=82) and 7% (14); respectively. Operating and treatment rooms were the locations of 60.7% of incidents, whereas outpatient clinics and emergency rooms accounted for 19.4% and 13.4% of injuries, respectively.
Conclusion: The current findings add to the growing body of literature on the importance of NSI prevention and reporting strategies. In the present study, sharp injuries were most commonly encountered by ophthalmic staff in the operating rooms. Continuous staff education on handling sharp instruments, encouraging anonymous reporting, and up-to-date revisions of guidelines and policies are of paramount importance to lessen the burden of sharp injuries.
Keywords: needle stick injury, sharp injury, occupational exposure, ophthalmology
Background
Sharp injuries are a prime concern for occupational injuries in the health care sector. Despite the worldwide recognition of their hazards, these injuries can have serious medical and psychological repercussions with a high risk for transmission of blood-borne pathogens and long-lasting stress even when an infection is not present. There are at least more than twenty different microbial agent that can be transmitted by sharp injuries such as human immunodeficiency virus (HIV), hepatitis B virus (HBV), hepatitis C virus (HCV).1 It is also estimated that the attributable fractions for percutaneous exposure incidents among health care workers (HCWs) to HIV, HCV, HBV are 4.4%, 39%, and 37%, respectively.2 Sharp injuries are relatively common, with three million such incidents reported annually around the world.3 A nation-wide study showed that the rate of percutaneous exposure per 100 hospital beds was 3.2, for which the authors believed the exact incidence to be underreported.4 Another recent study reported that almost two-thirds of university surgical residents (58.9%) have sustained sharp injuries at one time during training.5
In the operating theater, health care workers are being placed under increased occupational risk of blood-borne viruses (BBVs).6 Given the fact that surgical settings are more blood and fluid intensive, requires manipulation of sharp objects, chaotic in emergent cases, and demand harmonized member–member interaction, percutaneous exposure incident rates significantly decreased outside the surgical scenes.7
The field of ophthalmology has always been at the forefront of science and innovation. Advancement in ophthalmic practices have introduced unique microsurgical procedures that additionally increase the risk of sustaining sharp injuries.7 A risk of instrument mishandling is further exacerbated when visual cues are compromised under high magnification fields combined with minimal room lightning. Medical and nursing professionals may experience such incidents while focusing on the microscope, administering ophthalmic injections, recapping needle, discarding needle, and other related activities.
Although occupational exposure hazards are relatively common, it is not known to what extent risk adjustment policies are effective in reducing the risk of BBV. Furthermore, the reported data on sharp injuries in an ophthalmic setup in Saudi Arabia has not yet been examined and explored.5,8,9 This study therefore attempts to identify the epidemiological profile of sharp injuries in the largest tertiary eye-care center in Saudi Arabia. This study also aims to evaluate the implemented safety policy in preventing sharp injuries.
Methods
This was a retrospective cross-sectional study of all incidents of sharp injuries that occurred in King Khaled Eye Specialist Hospital (KKESH), Saudi Arabia. This public sector institute offers a comprehensive eye care and is equipped with operating rooms, inpatient and outpatient facilities, and an emergency department. It also provides teaching and practical training for residents, fellows, and nursing staff. In this study, the term “needlestick injuries” and “sharp injuries” are used interchangeably and were defined as an incidental penetration of the skin by a suture needle, hypodermic syringes, or any other needle devices. The study was approved by the Institutional Review Board at King Khaled Eye Specialist Hospital (RP-21091-R) and adhered to the tenets of the Declaration of Helsinki.
Data for all reported anonymized sharp injury incidents from 2013 to 2021 were obtained from the electronic hospital information system and from incident report forms. Incomplete or vague reports were excluded from the study. Hospital protocol necessitates reporting of all sharp injury incidents to the employee-health clinic within 60 minutes of occurrence. Reported information includes mechanism and location of injury, a description of the context and the type of instrument involved in the injury. Self-inflicted injuries are identified when a health care professional unintentionally causes an injury to him or herself. Second- and third-party injuries are recognized when two or more parties are involved in the incident, respectively. An example of second- party injury is when a scrubbed nurse injures the surgeon while passing a needle, while a third-party injury refers to situations where an individual inadvertently disrupts another practitioner, leading to an injury inflicted upon a third person. NSI injuries occurring right before or during the use of a sharp instrument were defined as injuries that happen in close proximity to or during the actual manipulation or preparation of a sharp instrument. For example, a surgeon accidentally pricking their finger with a needle while suturing a surgical wound. In the realm of instrument-related injuries, they were divided into three categories; solid needle including suture needles; hollow bore needles which have a channel through which medications are administered such as intravitreal injections; other sharp instruments such as surgical blades and scissors. All near misses are reported on different forms and therefore were not included in this study. In addition, this study involved an institution-based survey which was sent to through e-mail to all health care professionals at the study’s workplace. Informed consent was electronically obtained from all participants after explaining the aims of the study. The survey tool was a web-based questionnaire, which was designed by an investigator and research coordinator using a Google form. The survey comprises demographics and information related to practice of using needles. This online form was opened for a period of three weeks, after which all responses were enrolled. To enhance response rates, three reminder emails were sent to participants during the survey period, to encourage survey completion.
Statistical Analysis
Data were entered using Microsoft Access 2010 (Microsoft Corporation, Redmond, Washington) and analyzed using STATA 17.0 (StataCorp LLC, College Station, TX, USA). Categorical data were presented as counts and percentages. The determinants of “ever having had an NSI” and “having received training in sharp injuries prevention after induction” were examined using Poisson regression with robust error variance. Incidence ratios and 95% confidence intervals were calculated as measures of association. A p-value <0.05 was considered statistically significant.
Results
Two hundred and one incidents of sharp injuries were reported over a period of 9 years from 2013 to 2021 (Table 1). Out of the reported incidents, 95 (47.2%) occurred among eye care physicians (including attendings, fellows, and residents), 82 (40.7%) among nursing staff while 14 (7%) among ophthalmic technicians (Figure 1). None of the involved health care workers had seroconversion to HIV, HBC, or hepatitis B surface antigen. Self-induced injury was the most frequent form of injury (84.6%), followed by second-party injury (14.9%), and only one incident reported three party involvement (0.5%). Operating room and treatment room were the most reported location of injury (60.7%). Thirty-nine (19.4%) incidents took place in outpatient clinics, and 27 (13.4%) in the emergency room. Eight injuries (4%) occurred in laboratory and pharmaceutical facilities. The most frequent site of injury was hands (98%) (Table 2).
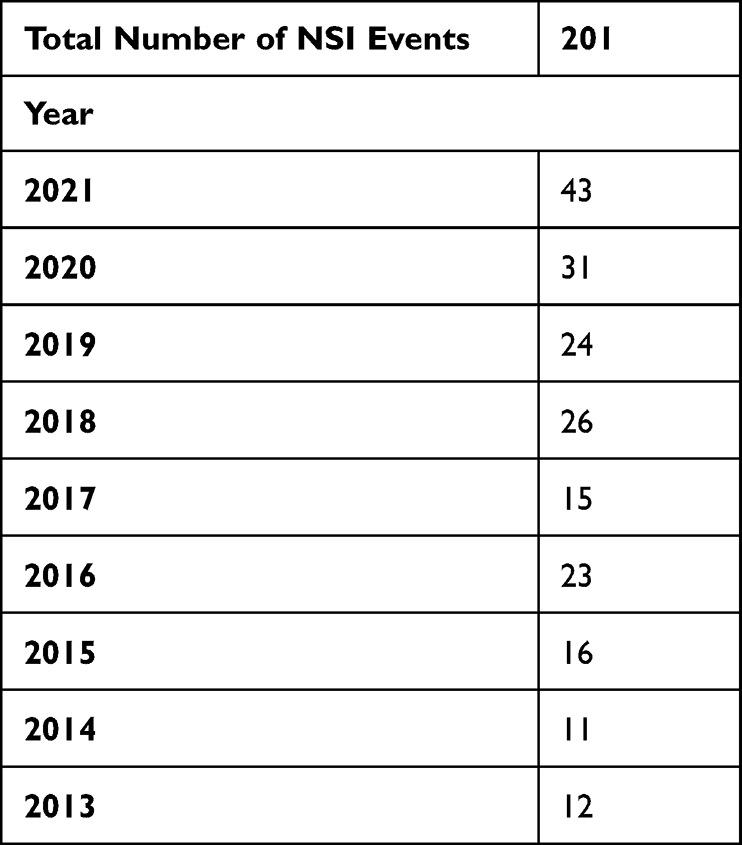 |
Table 1 Number of Needle-Stick Injuries Events per Year |
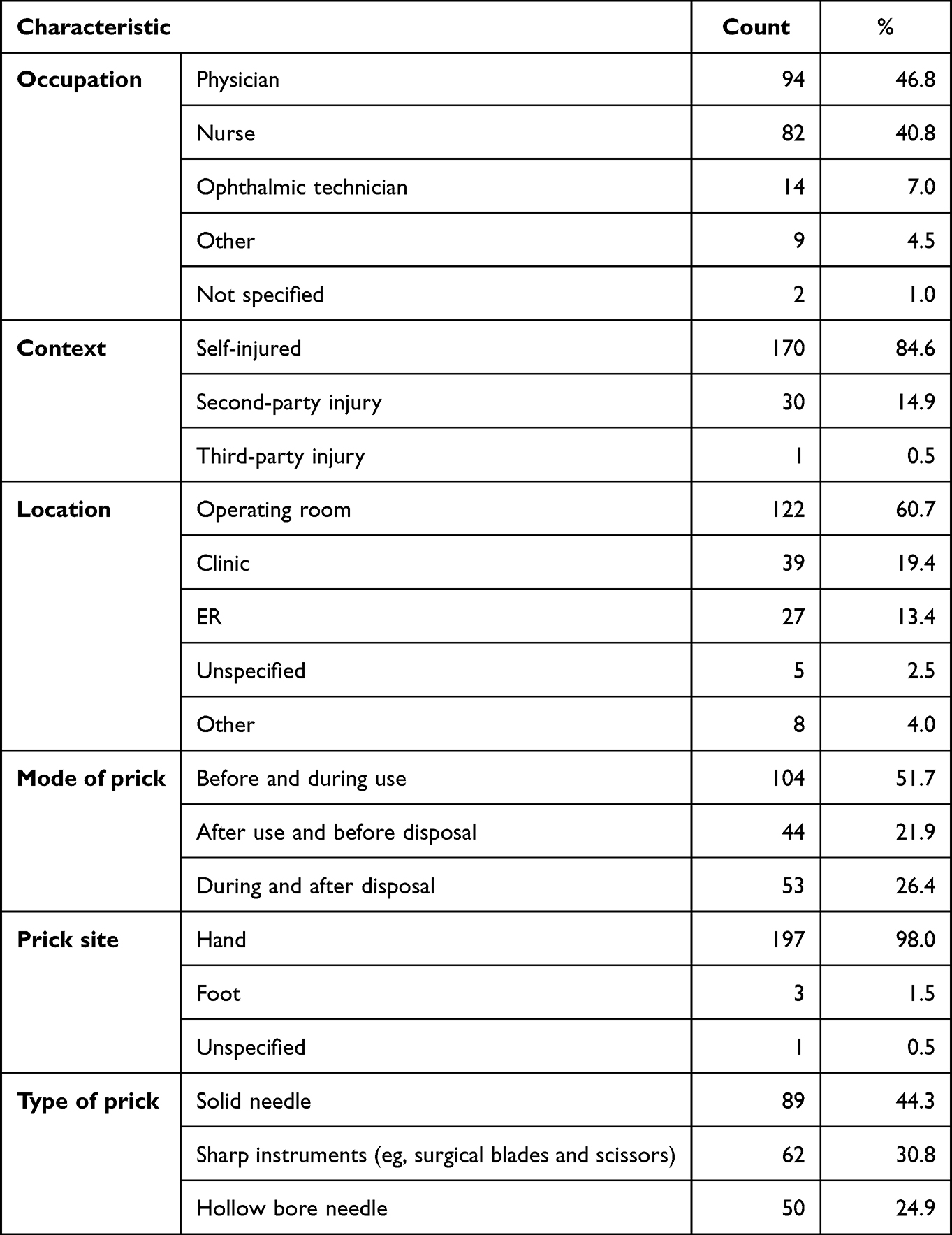 |
Table 2 Distribution of Injuries by Occupation, Context of Injury, Location of Injury and Mode of Prick, Prick Site, and Type of Prick (2013–2021) |
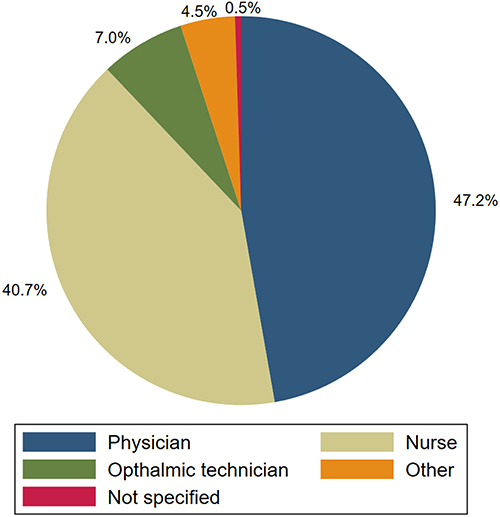 |
Figure 1 Percentage of sharp injuries by occupation of injured personal (2013–2021). |
There was a total of 104 (51.7%) injuries occurring right before or during the use of a sharp instrument. After use and before disposal injuries occurred in 44 (21.9%), and 53 (26.4%) incidents reported injuries during the act of disposal or right afterwards. Of notable injury, a scrub nurse felt pain in her toe which was ignored until late in the day when she found a needle imbedded in her left toe. Eighty-nine (44.3%) injuries were attributable to solid needles, 62 (30.8%) to sharp instruments (eg, surgical blade or scissors), and 50 (24.9%) to hollow-bore instruments (eg, injections and uncapped needles). Injuries related to hollow-bore needles were most commonly in the operating rooms (34%) and 28% were in outpatient clinics.
Of all the medical staff who voluntarily participated in the survey, 108 (response rate 25%) completed the survey (Table 3). Majority of respondents (58.3%) were aged less than 40 years, and 64.8% were of female gender. They included 63 (58.3%) nurses, 34 (31.5%) physicians, and 10.2% other healthcare professionals. More than half of the respondents had more than 5 years’ work experience in clinical practice. Thirty-three percent (36) did not receive any training in preventing sharp injuries when starting their position in the current workplace. Participants who self-reported ever having had an incident with sharp instruments were 21 (19.4%) (Table 4). Multivariable Poisson regression with robust error variances revealed that females were approximately 2-times more likely to have had a self-reported needle-stick injury in the past compared to males (IR=1.95, CI: 0.91–4.18); however, this difference was only marginally significant (p = 0.086). Eye physicians were 3-times more likely to have ever had an injury compared to nurses (IR=2.92, CI: 1.18–7.24, p=0.021). Our analysis also showed that physicians were less likely to have had a training in sharp injuries prevention (p = 0.008) (Table 5). Those who have a clinical experience between 5 and 9 years in the current workplace are more likely to have received training in sharp injuries compared to those with less experience (p = 0.002).
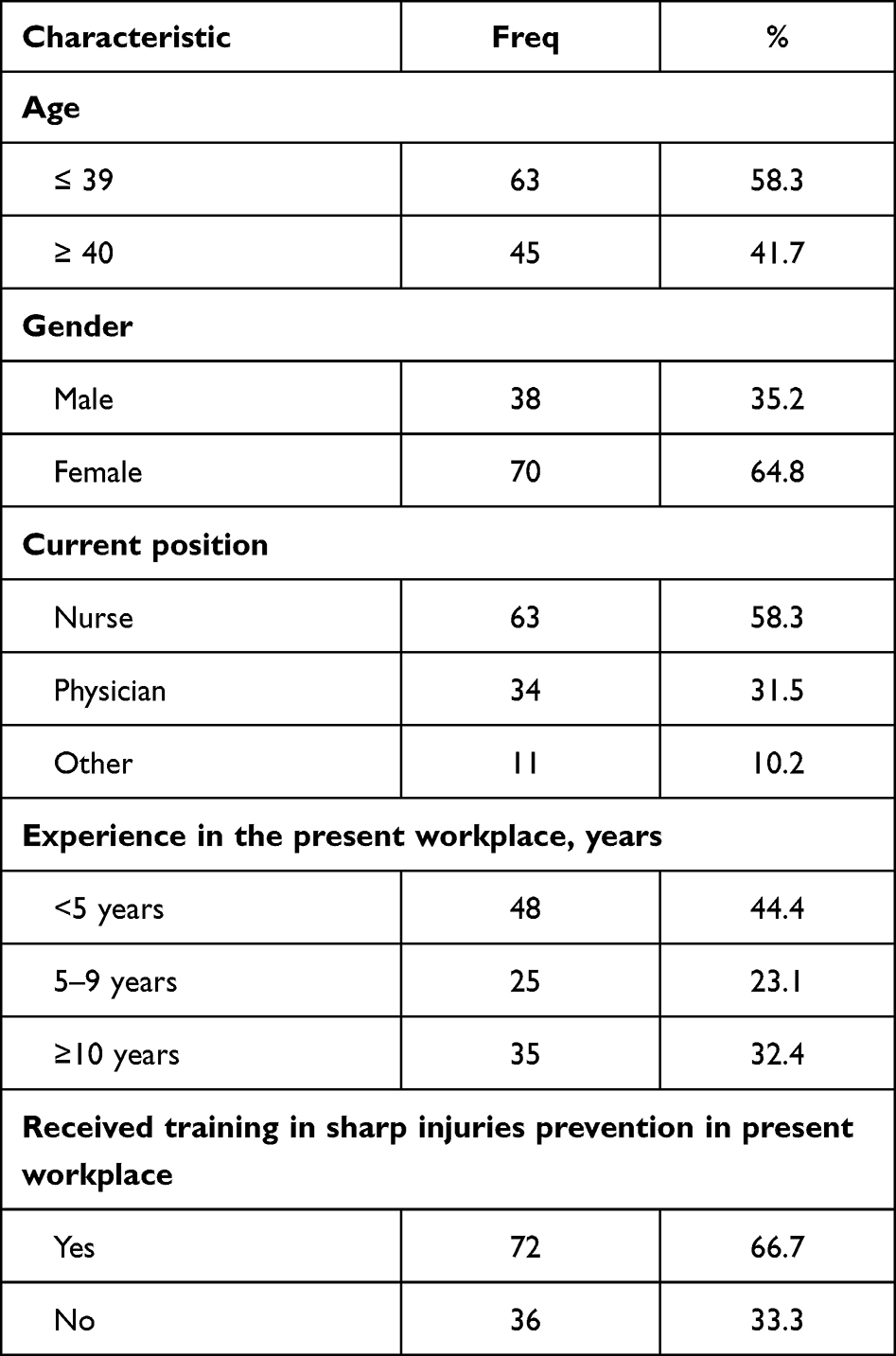 |
Table 3 Characteristics of Survey Participants (n=108) |
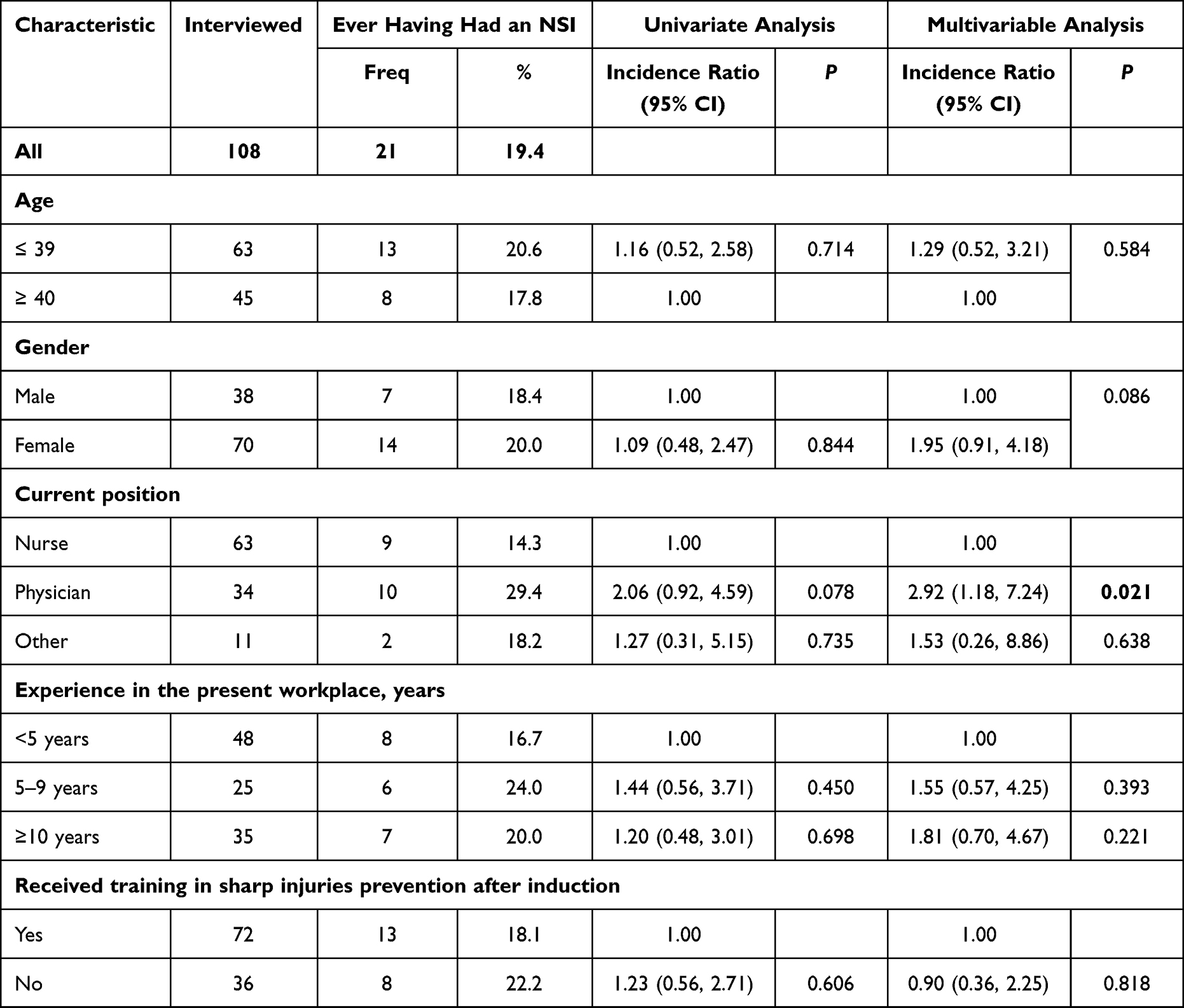 |
Table 4 The Incidence and Determinants of Ever Having Had an NSI Among Eye Care Workers |
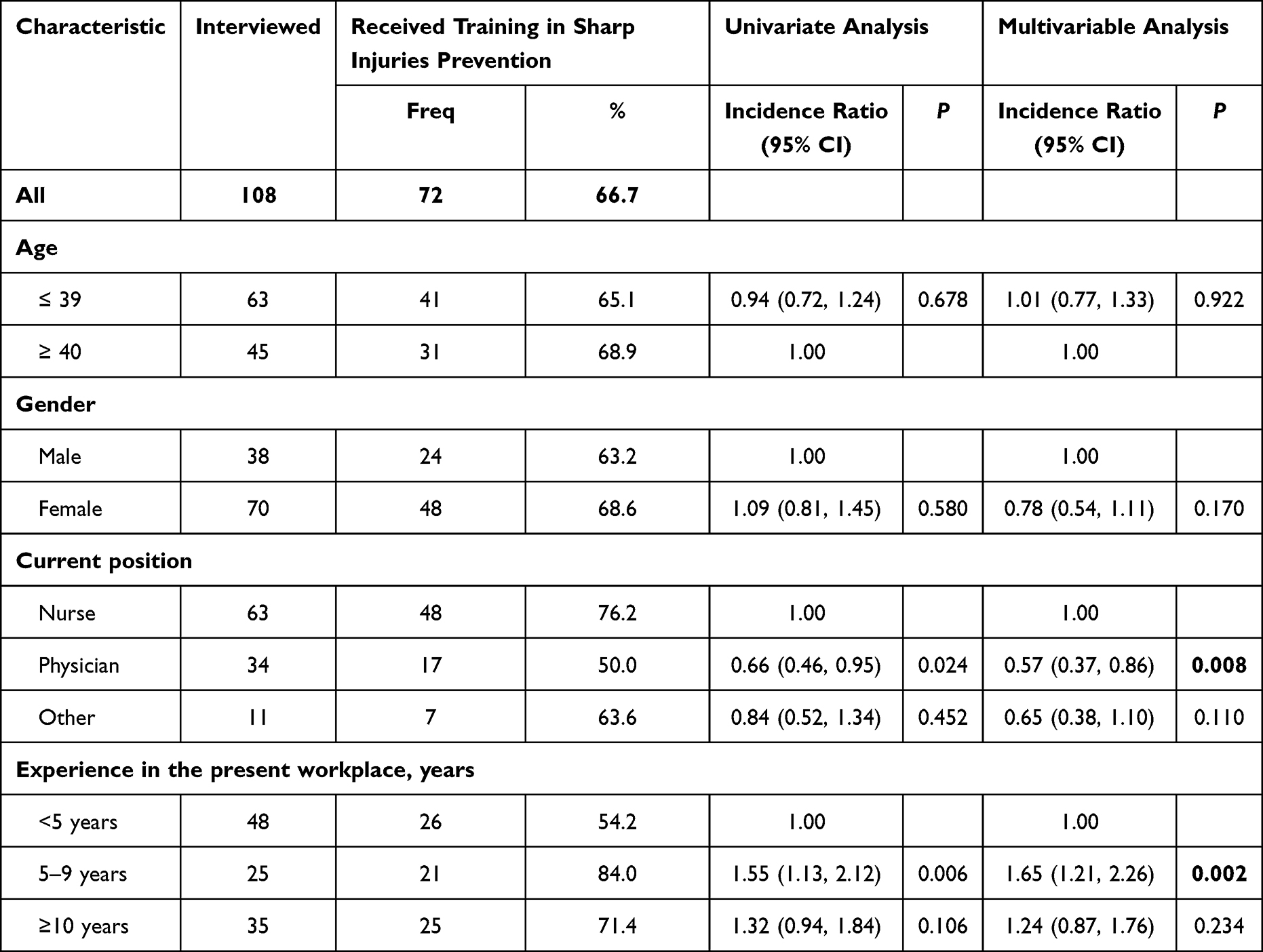 |
Table 5 The Determinants of Having Received Training in Sharp Injuries Prevention After Induction |
Discussion
Sustaining sharp injury at some point in the career of a healthcare worker is a serious event. Although preventable on most occasions, suffering from at least one injury is widely considered inevitable, particularly in surgical environments. This study found that over the span of nine years, 201 incidents of needlestick injuries were reported. The highest occurrence of injuries was observed among ophthalmic surgeons who were responsible for 94 (46.8%) of the reported incidents. A similar study reported that the highest number of sharp injuries was noted among physicians under training (24%), followed by nursing staff (23%).10 Another study found that 54.4% of nurses are at risk of sustaining an injury compared to ophthalmic surgeons (39.7%).11 Most incidences of needlestick injury reported were from operating rooms (60.7%). Reported incidents in outpatient clinics and the emergency room were 15% and 13%, respectively, while only 4% occurred in laboratories and other hospital facilities. This largely explained by the high volume of surgeries performed in ophthalmic practice. At this study’s institute, a total number of 89,733 surgeries (excluding refractive surgeries) performed from 2013 to 2021 (unpublished data). Also, ophthalmic surgery generally does not require hospital stay overnight, and the average number of days patients spend in hospital compared to other surgical specialties tends to be the lowest.12 Statistics from the United Kingdom reported that 90% of ophthalmic surgical procedures are one-day surgery.12 Ophthalmologists often do not perform procedures in inpatient settings or at bed side. With the exception of running sutures after strabismus surgery where sutures may be removed at bed side to control diplopia postoperatively. On the contrary, many invasive procedures are frequently performed in outpatient settings including the removal of corneal sutures and intravitreal injections. With the introduction of anti-vascular endothelial growth factor (anti-VEGF) therapy, intravitreal injections use has significantly increased in recent years.13 Though this modality of treatment is in its infancy, it is the most commonly performed ophthalmic procedure for many retinal diseases.14 Data record form our institute in 2021 estimates that 1700 eyes have received anti-VEGF injection in injection clinic and operating rooms (unpublished data). Although the handling and administration of injections are more commonly performed in clinical settings compared to operating rooms, in this current investigation, 34% of hollow-bore, including intravitreal injections, occurred in OR settings. This raises the concern of the limited visibility under microscopic settings as a potential concealed factor in the increased incidence of NSI.
Reported incident forms form the year 2021 have revealed 43 incidents. This noticeable rise in numbers can potentially be explained by the fact that the implementation of strict infection-control measures, due to COVID-19 pandemic, may have encouraged medical staff to be more vigilant, leading to more capture of incidents. Also, following the relaxation of lockdown measures, there may have been a surge in surgical procedures as deferred surgeries were rescheduled. This increase in volume during this period could have contributed to a proportional rise in reported injuries.
In the operating room, the majority of injuries occurred while passing of a sharp instrument from the scrubbed nurse to the surgeon and vice versa. These observations are recognized in Alshihry’s et al who reported that the most common circumstance of injury is while handling a sharp instrument (47%).15 This is also consistent with data from other medical specialties as evident by the 2021 The International Safety Center EPINet report, which has estimated that 57.5% of injuries happened during the use of a sharp item.16 Injuries occurring before disposal of a sharp device were 21.9%. These include instrument which were left in the sterilized surgical tray before being disposed of in the sharp container. In an emergency room of a tertiary health care facility, patients often flock with a plethora of variable ophthalmic conditions. In a busy setting, a slit lamp table may be used as a temporary transition station for sharp instruments before discarding them into the waste bin. One may argue that physicians should dispose of the instrument immediately, others may argue that this would present as a huge wastage of time in a typical busy practice. Therefore, when practicing any interventional procedure, all HCW must develop the habit of practicing the universal preventative measures with sharp instrument as evident in operative settings.
In this study, injuries reported during/after disposal are comparable to Alshihry et al (21%), lower than the one reported in Ghauri et al (46%), but significantly higher than the 4% reported in EPINet.11,15,16 Injuries in this context are largely observed with hollow-bore needles such as intravitreal injections. Ophthalmologists perform dozens of intravitreal injections on a daily basis. In one survey, 8% of retinal specialist have had needle stick injury after Avastin injections.17 This study also shed some light on the importance of the packaging design and the possibility of needle stick injury with the exposed labeling adhesive stickers on the Avastin syringe. Also, due to its funnel-shaped design and often lack of safety lids, standard sharp containers are filled quickly leading to overflow if not replaced in a timely manner. HCW, especially physician, should be aware that a sharp container should be replaced if filled to 75% of its capacity. Overfilling containers with additional sharp waste does not necessarily put physicians in danger, instead it is risky for other health care professionals including housekeepers who are trying to empty the containers.
Several methods have been proposed in the literature to minimize the incidence of sharp injury.18–20 One of the widely established methods is hands-free passing, in which a neutral zone is employed as an intermediary area rather than hand-to-hand passing. Several studies have assessed the effectiveness of minimizing simultaneous handling of sharp instrument (ie hands-free passing).18,20 Stringer et al reported a 60% decrease in incidence rate in operating rooms where hands-free passing method was used.18 A recent study also showed 35% reduction in injuries when the technique is used during ≥75% of the surgery’s duration.19 While this strategy can be applied to some ophthalmic procedures, it is limited by the fact that surgeons under microscope require direct visualization of the surgical field during critical steps of certain procedures. However, surgical loupes, which are often used in strabismus surgeries and oculoplastic procedures, provide an excellent magnification of the operative field while maintaining a wide peripheral view of the surgeon’s surrounding. In many surgical specialties, double-gloving technique is largely advocated.21 Blood-borne infections have been reduced by eight-fold after implementing this technique.22 However, particularly in ophthalmology, double gloves may adversely impact hand dexterity, palpation and final surgical outcomes. In fact, 73 out of 158 ophthalmologists surveyed do not wear protective gloves while administering intravitreal injections.17
Under-reporting of needlestick injuries is widely recognized in the literature.23–25 The rate of under-reported injuries was estimated to be as much as 50% in the United States.26 The authors of this study could not find local data estimating the rate of underreported incidents. However, a study reported significantly lower rates of NSIs per hundred beds compared to similar settings in the United States (12.3 vs 33.6).26 One of the main reasons responsible for such lower rates was suggested to be under-reporting.26 In this study, a trending increase in the number of incidents was observed. Year 2021 has almost quadruple the number of self-reported injuries in year 2013. Several factors such as disruption to the operating room workflow and a complicated incidents form were proposed to be responsible for under-reporting rates.23 It is also possible that some ophthalmologist are desensitized to an injury knowing that the instrument device is not contaminated with the patient’s blood and are therefore considered a low transmission risk of infectious disease. Importantly, all eye care providers must know that periocular and ocular fluid can transmit as much infections as exposure to blood.27,28 It is reported in the literature that surgeons in training seem to have lower rate of reporting.23,29 Residents in training can feel embarrassed when reporting an injury to an attending physician. In addition, they are usually responsible for ordering the lab workup themselves. Moreover, the lengthy and complicated process of following hospital protocols is a frequently encountered reporting barrier met by many surgeons.23,24
The fact that one-third did not receive any training on preventing sharp injuries upon entering their present workplace highlights a concerning gap in healthcare practices. In another study, logistic regression analysis on nursing staff revealed a strong association between insufficient training and an elevated risk magnitude (IR = 5.72).30 Obviously, organizational policies and practices are variable and subjected to change, leading to inconsistencies in the implementation of training programs. Resource constraints and time limitations could also hinder the provision of comprehensive training for all healthcare professionals. Additionally, high staff turnover rates or a lack of standardized onboarding processes might contribute to some individuals not receiving adequate training. The impact of this training gap cannot be understated. Several studies have shown that education programs lead to a reduction in the number of sharp injuries.31–33 A Chinese study reported that healthcare workers were more likely to sustain NSI if they do not attend bloodborne transmission prevention programs (IR = 2.59).31 The authors believe that developing an education program aimed at decreasing the risks of NSI is a cornerstone of any effective policy. Without proper training, healthcare professionals may be unaware of best practices for sharp injury prevention, increasing their vulnerability to potential harm. Possible health risks associated with these injuries should be made fully clear to every healthcare worker. Performing sharpless procedures can dramatically reduce the number of injuries. For instance, when complete eye akinesia is not essential in surgery, topical anesthesia can be an alternative to peri or retrobulbar injections. Also, scrapping corneal infiltrate can be performed using Weck-Cel eye spears, Kimura platinum spatula or calcium alginate swab instead of scalpel blades.
Despite the best efforts to lessen the burden of NSIs by education and training, some injuries are inevitable. Therefore, up-to-date guidelines and clear policies are necessary. Our hospital policy regarding occupational exposure to blood and/or body fluids is implemented in all ophthalmic settings (Figure 2). These indicate that an employee must follow the standardized process in case of exposure, immediately notify their supervisor, and begin the process of initiating an incident report. After notifying their superior, the employee must immediately start cleaning the wound with soap and water. In case of an exposure to a mucous membrane, the area must be thoroughly flushed with water. The protocol also dictates that the exposed employee must report to the Employee Health department immediately or within a maximum of one hour. Afterwards, the source patient will be tested for Hepatitis B, Human Immunodeficiency Virus, Hepatitis C, and Syphilis. This protocol is in accordance with the Centers of Disease Control and Prevention (CDC) recommendations and the Occupational Safety and Health Standards.33
 |
Figure 2 Flowchart diagram demonstrating the hospital protocol following needle-stick injury. Abbreviations: EH, Employee health; ER, Emergency room; HBV, Hepatitis B virus; HIV, Human immunodeficiency virus; HCV, hepatitis C virus; VDRL, Venereal Disease Research Laboratory test; HBAg, Hepatitis B surface antigen; Anti-HCV, HCV antibody test. |
This study design is not exempt from certain inherent limitations that should be acknowledged. The reliance on participants’ subjective recollection of past events, which may be influenced by various factors such as time elapsed since the event or personal interpretations introduces the possibility of recall bias. In addition, the absence of a controlled experimental setting limits the ability to determine a temporal sequence of relation. Despite these limitations, this research offers valuable findings into past events and behaviors, serving as a foundation for generating hypotheses and guiding future prospective investigations.
This study provides insights into the incidence, contributing factors, and consequences of needle-stick injuries among all medical staff within an ophthalmic center. With a particular emphasis on ophthalmologists, we shed light on their specific experiences and highlight the challenges faced daily. Ophthalmologists encounter unique risks due to their use of sharp instruments both inside and outside operative settings. This study highlights the importance of understanding these risks and implementing targeted interventions to ensure the safety and well-being. Staff training and continued education on sharp injury policy is of paramount importance to enhance adherence to safe needle use and to improve reporting rates. Robust hospital policies and protocols should advocate for establishing a safety program to regularly monitor high-risk procedure, determining the exact cause of each injury and how it could have been prevented. Efforts should be made to minimize needle use where possible and to adhere to safe use precautions when handling sharp devices. Decision-makers should also seek to create a safe culture that encourages reporting without fear of retribution. Audits could be randomly conducted to make sure policies are being followed and assessment of outcomes is carried out periodically. Given the unique challenges encountered in ophthalmic practice, specialty-specific guidelines should be developed to decrease sharp injuries in the field of ophthalmology. Further prospective research is needed to accurately assess the incidence of sharp injuries and evaluate the compliance of hospital personnel to reporting.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Whitby M, Slater K, McLaws ML, et al. Needlestick injuries in a major teaching hospital: the worthwhile effect of hospital-wide replacement of conventional hollow-bore needles. Am J Infect Control. 2008;36(3):180–186. doi:10.1016/j.ajic.2007.07.009
2. Rapiti E, Pruss-Ustun A, Hutin YJ. Sharps injuries assessing the burden of disease from sharps injuries to health-care workers at national and local levels. Geneva, World Health Organization. Environ Burd Dis Ser. 2005;11:1–58.
3. Rapiti E. Aide-Memoire for a Strategy to Protect Health Workers from Infection with Bloodborne Viruses. World Health Organization; 2003:5–9.
4. Memish ZA, Assiri AM, Eldalatony MM, et al. Benchmarking of percutaneous injuries at the ministry of health hospitals of Saudi Arabia in comparison with the United States hospitals participating in exposure prevention information network (epinetTM). Int J Occup Environ Med. 2015;6:26–33. doi:10.15171/ijoem.2015.467
5. Singh AP, Tanger R, Mathur V, et al. Sharp injuries in the operative room among residents in surgical specialties: a cross-sectional study. Saudi Surg J. 2018;6:11–15. doi:10.4103/ssj.ssj_43_17
6. Jagger J, Berguer R, Phillips EK, et al. Increase in sharps injuries in surgical settings versus nonsurgical settings after passage of national needlestick legislation. J Am Coll Surg. 2010;210:496–502. doi:10.1016/j.jamcollsurg.2009.12.018
7. Mansour AMansour A. Needlestick injuries in ophthalmology. Ophthalmic Surg. 1989;20(5):367–369.
8. Abalkhail A, Kabir R, Elmosaad YM, et al. Needle-stick and sharp injuries among hospital healthcare workers in Saudi Arabia: a cross-sectional survey. Int J Environ Res Public Health. 2022;19(10):6342. doi:10.3390/ijerph19106342
9. Alsabaani A, Alqahtani NSS, Alqahtani SSS, et al. Incidence, knowledge, attitude and practice toward needle stick injury among health care workers in Abha City, Saudi Arabia. Front Public Heal. 2022;10:1–11.
10. Rishi E, Shantha B, Dhami A, Rishi P, Rajapriya HC. Needle stick injuries in a tertiary eye-care hospital: incidence, management, outcomes, and recommendations. Indian J Ophthalmol. 2017;65(10):999–1003. doi:10.4103/ijo.IJO
11. Ghauri AJ, Amissah-Arthur KN, Rashid A, et al. Sharps injuries in ophthalmic practice. Eye. 2011;25(4):443–448. doi:10.1038/eye.2011.13
12. Health and Social Care Information Centre. Hospital episode statistics. 473 43:16 10; 2022. Available from: http://www.hesonline.org.uk/Ease/servlet/.
13. Seah I, Zhao X, Lin Q, et al. Use of biomaterials for sustained delivery of anti-VEGF to treat retinal diseases. Eye. 2020;34:1341–1356. doi:10.1038/s41433-020-0770-y
14. Tah V, Orlans HO, Hyer J, et al. Anti-VEGF therapy and the retina: an update. J Ophthalmol. 2015;2015:1–13. doi:10.1155/2015/627674
15. Alshihry AM. Pattern of sharps injuries in ophthalmic practice. Epidemiol. 2013;3:128. doi:10.4172/2161-1165.1000128
16. International Safety Center. EPINet Report for Needlestick and Sharp Object Injuries. International Safety Center; 2014:5–9.
17. Shah SU, Koenig MJ, Dacquay Y, et al. Assessment of the risk of needlestick injuries associated with intravitreal injections. Retina. 2014;34:781–784. doi:10.1097/IAE.0b013e3182a2f523
18. Stringer B, Infante-Rivard C, Stringer B, Hanley JA. Effectiveness of the hands-free technique in reducing operating theatre injuries. Occup Environ Med. 2002;59:703–707. doi:10.1136/oem.59.10.703
19. Stringer B, Haines T, Goldsmith CH, et al. Hands-free technique in the operating room: reduction in body fluid exposure and the value of a training video. Public Health Rep. 2009;124:169–179. doi:10.1177/00333549091244S119
20. Linzer PB, Linzer PB, Clarke SP. An integrative review of the hands-free technique in the OR. AORN J. 2017;106:211–218.e6. doi:10.1016/j.aorn.2017.07.004
21. Tanner J, Tanner J, Parkinson H. Double gloving to reduce surgical cross-infection (Review). Cochrane Database Syst Rev. 2006;3. doi:10.1002/14651858.CD003087.pub2
22. Berguer R, Berguer R, Heller PJ. Strategies for preventing sharps injuries in the operating room. Surg Clin North Am. 2005;85:1299–1305. doi:10.1016/j.suc.2005.09.012
23. Kennedy R, Kelly S, Gonsalves S, et al. Barriers to the reporting and management of needlestick injuries among surgeons. Ir J Med Sci. 2009;178:297–299. doi:10.1007/s11845-009-0359-8
24. Bahat H, Hasidov-Gafni A, Youngster I, et al. The prevalence and underreporting of needlestick injuries among hospital workers: a cross-sectional study. Int J Qual Heal Care. 2021;33:1–5.
25. Thomas WJC, Thomas WJC, Murray JRD. The incidence and reporting rates of needle-stick injury amongst UK surgeons. Ann R Coll Surg Engl. 2009;91:12–17. doi:10.1308/003588409X359213
26. Balkhy HH, El Beltagy KE, El-Saed A, et al. Benchmarking of percutaneous injuries at a teaching tertiary care center in Saudi Arabia relative to United States hospitals participating in the exposure prevention information network. Am J Infect Control. 2011;39:560–565. doi:10.1016/j.ajic.2010.10.022
27. Ciulla TA, Schnizlein-bick CT, Danis RP, et al. Comparison of intraocular to plasma HIV-1 viral burden in patients with cytomegalovirus retinitis. Am J Ophthalmol. 1999;127:221–223. doi:10.1016/S0002-9394(98)00345-6
28. Bourla DH, Wirthlin RS, Bourla N, et al. Risk for eye splash injury during administration of intraocular injections: a study of retina specialists and fellows. Retina. 2007;27:609–612. doi:10.1097/01.iae.0000249578.65443.27
29. Makary M, Al-Attar A, Holzmueller CG, et al. Needlestick injuries among surgeons in training. N Engl J Med. 2007;28:2693–2699. doi:10.1056/NEJMoa070378
30. Nsubuga FM, Nsubuga FM, Jaakkola MS. Needle stick injuries among nurses in sub-Saharan Africa. Trop Med Int Heal. 2005;10:773–781. doi:10.1111/j.1365-3156.2005.01453.x
31. Tang P, Jamulitrat S, Tang P. Incidence and risk factors for sharps injury among healthcare workers in three hospitals in Kunming, China. J Nurs Sci. 2009;27:42–48.
32. Holodnick CL, Barkauskas V, Holodnick CL, Barkauskas V. Reducing percutaneous injuries in the OR by educational methods. AORN J. 2000;72(3):461–464, 468–472, 475–476. doi:10.1016/s0001-2092(06)61278-7
33. Brusaferro S, Calligaris L, Farneti F, et al. Educational programmes and sharps injuries in health care workers. Occup Med. 2009;59:512–514. doi:10.1093/occmed/kqp112
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.