Back to Journals » International Journal of General Medicine » Volume 19
Necessity of Percutaneous Coronary Intervention Evaluated by Low-Pressure Balloon Occlusion and Improvement of Postoperative Clinical Symptoms in Patients with Intermediate Lesions
Received 6 March 2026
Accepted for publication 30 June 2026
Published 9 July 2026 Volume 2026:19 602037
DOI https://doi.org/10.2147/IJGM.S602037
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Jun Wang,1 Yuan Liu,2 Guo-Zhen Jin3
1Department of Cardiology, Hongze District People’s Hospital, Huaian, 223100, People’s Republic of China; 2Department of General Practice, Huaihai Road Community Health Service Center, Nanjing, 210002, People’s Republic of China; 3Department of Cardiology, Nanjing First Hospital, Nanjing Medical University, Nanjing, 210006, People’s Republic of China
Correspondence: Guo-Zhen Jin, Email [email protected]
Objective: The value of low-pressure balloon occlusion (LPBO) technology was investigated to evaluate the necessity of percutaneous coronary intervention (PCI) and the improvement of postoperative clinical symptoms in patients with intermediate lesions. Furthermore, the feasibility and safety of this technique were validated.
Methods: Forty-eight patients with intermediate lesions identified during angiography at the Department of Cardiology, Nanjing First Hospital, Nanjing Medical University, were enrolled and randomly assigned to the treatment group and the control group. In the treatment group, PCI was guided by LPBO. In the control group, PCI was guided by intravascular ultrasound (IVUS) or optical coherence tomography (OCT). Symptom intensity, symptom similarity scores, and PCI implantation rates were collected during the procedure. The clinical symptom improvement rate and the incidence of major adverse cardiovascular events (MACE) were observed during hospitalization and follow-up.
Results: In the treatment group (n=24), 10 patients experienced symptoms similar to their pre-hospitalization condition during LPBO and subsequently underwent PCI, resulting in symptom resolution. The remaining 14 patients with low symptom similarity scores showed good prognosis after intensive medical therapy. In the control group (n=24), 18 patients met the minimum lumen area (MLA) criteria via IVUS/OCT and received PCI. The PCI implantation rate in the treatment group was significantly lower than that in the control group (P < 0.05). Significant improvement in Seattle Angina Questionnaire (SAQ) scores was observed in 18 patients (75%) in the treatment group compared to 8 patients (33.3%) in the control group (P < 0.05). At the 6-month follow-up, no MACE occurred in the treatment group (n=24, 0.0%). In the control group, 2 cases of target vessel revascularization (TVR) occurred (2/24, 8.3\%), with no cardiac deaths or non-fatal myocardial infarctions. No significant difference in MACE incidence was found between the two groups. No complications related to LPBO, such as dissection or plaque rupture, were observed.
Conclusion: LPBO technology effectively correlates coronary stenosis with clinical symptoms. It provides a reliable basis for PCI decision-making in patients with intermediate lesions. This technique is safe and feasible. It has the potential to reduce unnecessary stent implantation and improve patient prognosis.
Keywords: low-pressure balloon occlusion, intermediate lesions, percutaneous coronary intervention, clinical symptom improvement
Introduction
Cardiovascular disease (CVD) has become the leading cause of death among chronic non-communicable diseases in China. There are 11.39 million patients with coronary heart disease (CHD), and the number of patients undergoing percutaneous coronary intervention (PCI) reached 1.636 million in 2023.1–4 As an important method for revascularization in CHD, PCI effectively improves patient symptoms and prognosis. However, residual chest pain after the procedure remains a prominent issue, with an incidence ranging from 14.2% to 59%.5,6 Postoperative chest pain increases the risk of cardiovascular events. It also leads to negative emotions such as anxiety and depression, which seriously affect treatment outcomes and quality of life.
Patients with intermediate lesions are a high-risk group for residual symptoms after PCI. Coronary intermediate lesions refer to lesions with a lumen diameter stenosis of 50% to 70% as shown by angiography. Due to anatomical diversity, evidence-based medical data for these lesions are insufficient, making clinical treatment decisions difficult. Currently, methods such as intravascular ultrasound (IVUS), optical coherence tomography (OCT), and fractional flow reserve (FFR) are commonly used. These methods can evaluate the anatomical or functional status of lesions. However, they cannot directly establish a correlation between stenosis and clinical symptoms. Consequently, some patients experience recurrent symptoms even after undergoing ineffective PCI. Therefore, a new evaluation method is urgently needed to accurately link coronary stenosis with symptoms and guide treatment decisions.
Transient low-pressure balloon occlusion (LPBO) induces controlled, reversible myocardial ischemia by temporarily obstructing coronary blood flow with a non-compliant balloon inflated at low pressure (2–4 atm) to occlude the target vessel. This brief ischemia can precisely reproduce the patient’s baseline clinical symptoms (eg, chest pain, chest tightness) if the stenosis is functionally significant, directly linking anatomical narrowing to symptomatic ischemia. As validated in the ORBITA-STAR trial, the symptom similarity score derived from LPBO-induced symptoms strongly predicts PCI-related symptom relief, confirming the causal relationship between stenosis and symptoms.7 Based on previous clinical observations, this study found that patients with severe coronary stenosis can experience ischemic symptoms similar to their preoperative symptoms during short-term expansion with a small balloon. Accordingly, the use of low-pressure balloon occlusion (LPBO) technology is proposed. Ischemic symptoms are induced and compared with preoperative symptoms to evaluate the necessity of PCI in patients with intermediate lesions. This study provides a new perspective for clinical treatment.
Subjects and Methods
Study Subjects
Forty-eight patients with intermediate lesions were selected. These patients were hospitalized in the Department of Cardiology at Nanjing First Hospital, Nanjing Medical University, between January 2025 and June 2025. The lesions were identified during coronary angiography. Intermediate lesions were defined as lumen diameter stenosis ≥50% and ≤70% as shown by coronary angiography. The patients were scheduled for PCI evaluation. Informed consent forms were signed by the patients and their relatives. The experiment followed guidelines outlined in the Declaration of Helsinki and obtained written informed consent from participants. The study was approved by Nanjing First Hospital, Nanjing Medical University (20180517).
Sample Size Calculation
Based on preliminary data and relevant literature reports, the PCI implantation rate for patients with intermediate lesions guided by traditional IVUS/OCT is approximately 80%. It was hypothesized that LPBO technology could reduce the PCI implantation rate to 40%. The parameters were set as α = 0.05 and β = 0.2. The sample size was calculated using the formula for comparing two independent sample rates:

where p = (0.8 + 0.4) / 2 = 0.6, and p1 - p2 = 0.4. The calculated sample size was 20 cases per group. A dropout rate of 10% was considered. Finally, 48 patients were included, with 24 patients in each group.
Research Methods
Patients were divided into a treatment group and a control group using a random number table method, with 24 cases in each group. The treatment group underwent PCI guided by LPBO. The control group underwent PCI guided by IVUS or OCT.
Treatment Group (LPBO-Guided PCI)
Routine Coronary Angiography: Left and right coronary angiography was performed using the Judkins technique to determine the lesion location and the degree of stenosis.
Low-pressure Balloon Occlusion: A semi-compliant balloon (balloon-to-artery ratio of 1:1) was placed at the stenosis. The balloon was inflated to the minimum pressure required to occlude the distal vessel (usually 2–4 atm). Complete vessel occlusion was confirmed by angiography showing no blood flow distal to the occlusion. The occlusion time was calculated using the Digital Subtraction Angiography (DSA) screen display. Generally, the occlusion lasted at least 60s and up to 180 s. After 60s, the patient was asked about their symptoms and the similarity to their pre-admission symptoms. Electrocardiogram (ECG) and hemodynamic changes were observed. If similar symptoms were induced or blood pressure dropped, the occlusion was stopped immediately.
Scoring System: Pain intensity and similarity were assessed using a numeric rating scale. Intensity Score (0–10): 0 indicates no sensation perceived; 10 indicates the worst pain imaginable. Similarity Score (0–10): This measures the similarity between the characteristics of the induced sensation and the patient’s daily symptoms. 0 indicates not similar; 10 indicates identical to daily symptoms.
PCI Decision: If similar symptoms appeared, PCI was performed (drug-eluting stent implantation). If similar symptoms did not appear or the similarity score was low, PCI was abandoned. Conservative medical therapy was administered (aspirin and statins; beta-blockers or nitrates were added if necessary). The specific procedure is illustrated in Case 1.
Case 1: The patient was a 58-year-old male. He was admitted due to “recurrent chest tightness for 1 year, aggravated for 1 month”. He was diagnosed with CHD and unstable angina. Coronary angiography showed intermediate stenosis in the left anterior descending artery (LAD). A 3.0×12 mm pre-dilation balloon was used for occlusion at 4 atm. Symptoms appeared after 90s. The symptom similarity score was 2. Consequently, PCI was not performed. Intensive medical therapy was recommended. Repeated IVUS showed no dissection or plaque rupture at the site of low-pressure dilation, as shown in Figure 1.
 |
Figure 1 IVUS. (A) Intermediate stenosis in the middle segment of the LAD; (B) Low-pressure balloon occlusion; (C) IVUS examination; (D) IVUS revealed no dissection or plaque rupture at the occlusion site. |
Control Group (IVUS/OCT-Guided PCI)
Routine Coronary Angiography: The procedure was identical to that in the treatment group.
Intravascular Imaging: IVUS or OCT examinations were performed on the intermediate lesions. The Minimum Lumen Area (MLA) was evaluated by IVUS and OCT. PCI was recommended if the MLA was < 2.4 mm2 in vessels with a diameter < 3.0 mm2, or if the MLA was < 2.8 mm2 in vessels with a diameter > 3.0 mm2.8
PCI Decision: The decision to perform PCI was based on the IVUS/OCT results. The PCI procedure and postoperative medication were identical to those in the treatment group. The specific process is illustrated in Case 2.
Case 2: The patient was a 72-year-old male. He was admitted due to “recurrent chest pain for six months, aggravated for one week”. He was diagnosed with CHD and unstable angina. Coronary angiography showed intermediate stenosis in the LAD and the diagonal branch. OCT examination revealed an MLA of 0.8 mm2 in the LAD. Consequently, PCI was performed on both the LAD and the diagonal branch. Angina attacks persisted during the follow-up period, as shown in Figure 2.
 |
Figure 2 Angina attacks persisted. (A) Intermediate stenosis in the middle segment of the LAD and the proximal segment of the diagonal branch; (B) OCT examination; (C) OCT revealed fibrous plaque with an MLA of 0.8 mm2, arrow: guidewire artifact, the white line: the measurement line; (D) Angiography after PCI. |
Primary Endpoints
PCI Implantation Rate: The proportion of patients who finally received PCI treatment in both groups.
Six-month Postoperative Chest Pain Improvement Rate: This was evaluated using the Seattle Angina Questionnaire (SAQ). The assessment included four dimensions: degree of physical limitation, angina stability, angina frequency, and treatment satisfaction. A score increase of ≥ 20 points from baseline was defined as “significant improvement”. The proportion of patients with significant improvement was calculated.9
Secondary Endpoints
Incidence of MACE at 6 months post-procedure: MACE included cardiac death, non-fatal myocardial infarction (defined as Troponin I elevation ≥ 5 times the Upper Limit of Normal [ULN] accompanied by ischemic symptoms or ECG changes), and Target Vessel Revascularization (TVR, defined as repeat PCI or Coronary Artery Bypass Grafting [CABG] due to target vessel stenosis ≥ 50%).
Incidence of procedure-related complications: This included coronary dissection (NHLBI classification type ≥ B), vessel perforation, and contrast-induced nephropathy (defined as a serum creatinine increase ≥ 25% from baseline or an absolute increase ≥ 44 μmol/L within 48 hours post-procedure).
Success rate of LPBO technology: This was defined as the proportion of patients in the treatment group who successfully completed LPBO and obtained definitive ischemia evaluation results (absence of severe complications and ability to clearly determine the presence or absence of ischemia).
Follow-Up Protocol
1 month post-procedure: Outpatient follow-up was conducted. SAQ scores were completed. ECG, myocardial enzymes, and liver and renal function were reviewed.
3 months post-procedure: Outpatient follow-up was conducted. ECG and echocardiography (evaluating Left Ventricular Ejection Fraction [LVEF]) were reviewed.
6 months post-procedure: Outpatient follow-up was conducted. SAQ scores were completed. Coronary angiography (if necessary), ECG, and myocardial enzymes were reviewed. The occurrences of MACE and complications were recorded.
Statistical Analysis
Data analysis was performed using SPSS 26.0 software. Continuous variables were expressed as mean ± standard deviation (x±s). Comparisons between groups were performed using the independent samples t-test. Categorical variables were expressed as frequency (percentage) [n (%)]. Comparisons between groups were performed using the Chi-square (χ2) test or Fisher’s exact test (when the theoretical frequency was < 5). A P-value < 0.05 was considered statistically significant.
Results
Comparison of Baseline Characteristics
Baseline characteristics were compared between the two groups. These included age, gender, history of hypertension, history of diabetes, history of hyperlipidemia, history of smoking, distribution of target vessels (Left Anterior Descending artery [LAD], Left Circumflex artery [LCX], Right Coronary Artery [RCA]), and baseline SAQ scores. No statistically significant differences were found (all P > 0.05). The two groups were comparable (Table 1).
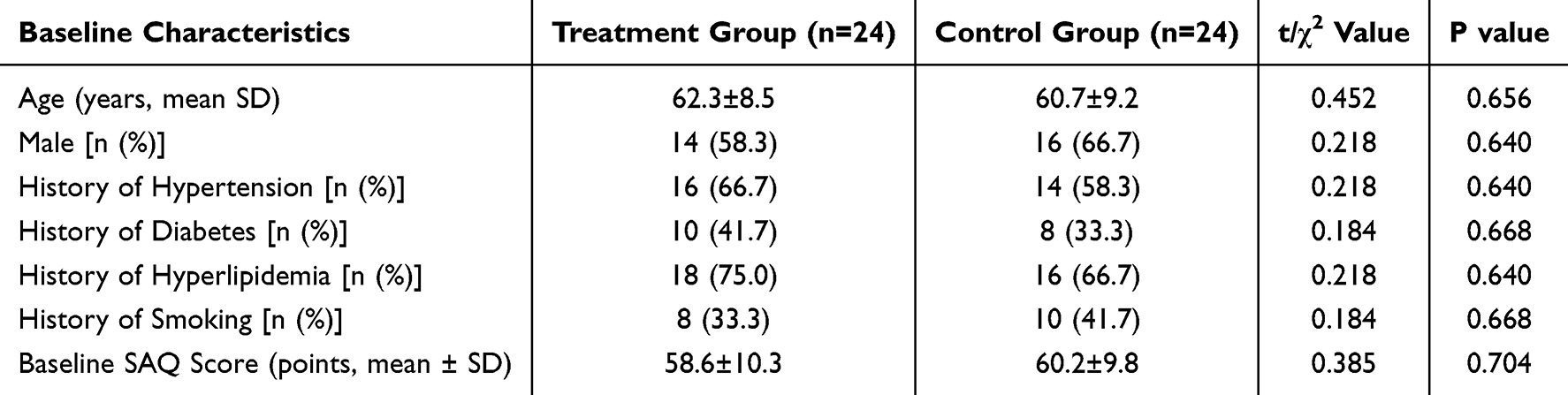 |
Table 1 Baseline Characteristics |
Comparison of Primary Endpoints
PCI Implantation Rate: In the treatment group (n=24), 10 patients (41.7%) were indicated for ischemia by LPBO assessment and underwent PCI. In the control group (n=24), 20 patients (83.3%) met the MLA criteria assessed by IVUS/OCT and underwent PCI. The PCI implantation rate in the treatment group was significantly lower than that in the control group (χ2 = 4.44, P = 0.038).
Improvement Rate of Chest Pain Symptoms at 6 Months Post-procedure: In the treatment group (n=24), significant improvement in SAQ scores compared to baseline was observed in 18 patients (75%). In the control group (n=24), significant improvement was observed in 8 patients (33.3%). The difference between the two groups was statistically significant (χ2 = 4.20, P = 0.041).
Comparison of Secondary Endpoints
Incidence of MACE at 6 months post-procedure: No MACE occurred in the treatment group (n=24, 0.0%). In the control group, 2 cases of Target Vessel Revascularization (TVR) occurred (2/24, 8.3%); no cardiac deaths or non-fatal myocardial infarctions occurred. No statistically significant difference was found in the incidence of MACE between the two groups (Fisher’s exact test, P = 1.000).
Incidence of procedure-related complications: No coronary dissection or vessel perforation occurred in either group. Contrast-induced nephropathy occurred in 2 patients (8.3%) in the treatment group and in 2 patients (8.3%) in the control group. No statistically significant difference was found in the incidence of complications between the two groups (Fisher’s exact test, P = 1.000).
Success rate of LPBO technology: All 24 patients in the treatment group successfully completed the LPBO assessment. No procedural failures or severe complications occurred. The technical success rate was 100.0% (24/24). Details are shown in Table 2.
 |
Table 2 Comparison of Primary and Secondary Endpoints |
Discussion
Intermediate coronary lesions are usually defined as lesions with coronary artery lumen diameter stenosis of ≥ 50% and ≤ 70% as evaluated by coronary angiography. Although coronary angiography is the “gold standard” for anatomical evaluation of coronary arteries, it has significant limitations in judging lesion severity and identifying vulnerable plaques. Currently, it is generally considered that coronary artery stenosis greater than 70% accompanied by evidence of myocardial ischemia is an indication for coronary stent implantation. Epidemiological data show that among patients with acute coronary syndrome (ACS), 60% to 70% have underlying lesion stenosis between 30% and 70%.10,11 Given the anatomical diversity of intermediate lesions, evidence-based medical data are scarce. Furthermore, clinical management tends to be individualized. Considering the invasive nature of PCI and the potential risk of complications, defining intermediate lesions, evaluating their significance, and deciding on intervention are difficult challenges for interventional cardiologists. Decisions must be made after careful consideration, weighing of pros and cons, and comprehensive evaluation. Current methods for evaluating intermediate lesions include imaging techniques (IVUS, OCT) and functional assessment (FFR). However, these results cannot directly indicate the relationship between lesions and symptoms, and they are expensive. Therefore, a more prudent management strategy should be adopted for intermediate lesions.
Consequently, for patients with intermediate lesions, there is an urgent need for a method to link stenosis with symptoms. In previous PCI procedures, it was observed that patients with severe coronary stenosis experienced ischemic symptoms similar to their pre-operative symptoms even during short-term expansion with a small balloon. Therefore, the following question arises: can active balloon occlusion be performed in patients with intermediate lesions to induce relevant ischemic symptoms? By judging whether the induced symptoms are similar to the patient’s pre-operative symptoms, the necessity of PCI and the possibility of symptom recurrence after PCI can be evaluated. This approach aims to reduce patient suffering, anxiety, and potential doctor-patient disputes.
The results of this study showed that LPBO technology significantly reduced the PCI implantation rate in patients with atypical chest pain and intermediate lesions (41.7% vs 83.3%, P = 0.038). Simultaneously, it significantly increased the improvement rate of chest pain symptoms at 6 months post-procedure (75.0% vs 33.3%, P = 0.041). No significant differences were found in the incidence of MACE and complications between the two groups. This result validates the core value of LPBO technology: by directly assessing the correlation between myocardial ischemia and clinical symptoms, patients who will truly benefit from PCI are screened, and stent treatment is avoided for patients without evidence of ischemia.
Mechanistically, the correlation between symptoms and coronary lesions in patients with intermediate lesions is weak. In some patients, symptoms may be caused by non-cardiac factors. Even if intermediate anatomical stenosis exists, it does not necessarily lead to myocardial ischemia.12 Through the direct evidence of “symptom reproduction”, LPBO technology clarifies the functional significance of the lesion. This approach fits clinical needs better than the morphological assessment of IVUS/OCT. In this study, ischemia was not detected by LPBO assessment in 58.3% (14/24) of patients in the treatment group, thus avoiding unnecessary stent implantation. This is consistent with the concept of “functional revascularization” guided by FFR. However, LPBO does not require special equipment and is more suitable for promotion in primary hospitals.13 This study is the first to apply LPBO technology to PCI decision-making in patients with atypical chest pain and intermediate lesions. It fills the technical gap for simple functional assessment in such patients and provides a new “symptom-oriented” evaluation method. This not only reduces medical costs and the risk of stent-related complications but also saves medical resources, aligning with the development direction of “precision medicine” and “value-based medicine”. It lays the foundation for the subsequent development of standardized ischemia assessment processes and related devices, while providing clinical data support for the construction of ischemia models.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Boden WE, O’Rourke RA, Teo KK, et al. Optimal medical therapy with or without percutaneous coronary intervention for stable coronary disease: the COURAGE trial. N Engl J Med. 2007;356(15):1503–7. doi:10.1056/NEJMoa070829
2. Tonino PA, De Bruyne B, Pijls NH, et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med. 2009;360(21):213–224. doi:10.1056/NEJMoa0807611
3. Maron DJ, Hochman JS, Reynolds HR, et al. Initial invasive or conservative strategy for stablecoronary disease. N Engl J Med. 2020;382(15):1395–1407. doi:10.1056/NEJMoa1915922
4. Chacko L, P Howard J, Rajkumar C, et al. Effects of percutaneous coronary intervention on death and myocardial infarction stratified by stable and unstable coronary artery disease: a meta-analysis of randomized controlled trials. Circ Cardiovasc Qual Outcomes. 2020;13(2):e006363. doi:10.1161/CIRCOUTCOMES.119.006363
5. Bai Y, Li Y. Analysis of causes of chest pain after PCI in coronary heart disease. Chinese J Mod Drug App. 2012;6(1):31–32.
6. Rajkumar CA, Foley MJ, Ahmed-Jushuf F, et al. A placebo-controlled trial of percutaneous coronaryintervention for stable angina. N Engl J Med. 2023;389(25):23192330. doi:10.1056/NEJMoa2310610
7. Rajkumar CA, Foley MJ, Ahmed-Jushuf F, et al. N-of-1 trial of angina verification before percutaneous coronary intervention. J Am Coll Cardiol. 2024;84(1):1–12. doi:10.1016/j.jacc.2024.04.001
8. Bu J, Wang W. Chinese expert consensus on the application of intravascular ultrasound in coronary artery disease 2018. Chinese J Cardiol. 2018;46(5):344–351.
9. Sullivan MJ, Rogers WJ, Rosati RA, et al. Development and evaluation of the Seattle angina questionnaire: a new functional status measure for coronary artery disease. Am Heart J. 1996;131(2):221–229.
10. Welén Schef K, Tornvall P, Alfredsson J, et al. Prevalence of angina pectoris and association with coronary atherosclerosis in a general population. Heart. 2023;109(19):1450–1459. doi:10.1136/heartjnl-2023-322345
11. Huo Y, Fang W. Evaluation, treatment decision and interventional therapy of intermediate lesions. Train Mater Coronary Intervent. 2018;1:364–367.
12. Douglas PS, Grines CL, Brindis RG, et al. 2021 ACC/AHA/SCAI guideline for coronary artery revascularization. Circulation. 2021;144(15):e754–e831.
13. Dehbi HM, Sen S, Neumann FJ, et al. Fractional flow reserve-guided PCI versus medical therapy in stable coronary disease. N Engl J Med. 2020;382(19):1829–1838.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.