Back to Journals » Clinical Ophthalmology » Volume 20
Near Fixation–Associated Intraocular Pressure Reduction in Intermittent Exotropia: Postoperative Changes After Strabismus Surgery
Authors Suzuki T ![]() , Fukutome T, Otaki C, Ueta Y, Suzuki T
, Fukutome T, Otaki C, Ueta Y, Suzuki T
Received 2 March 2026
Accepted for publication 18 May 2026
Published 28 May 2026 Volume 2026:20 606338
DOI https://doi.org/10.2147/OPTH.S606338
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sotiria Palioura
Takafumi Suzuki,1,2 Takao Fukutome,1 Chisato Otaki,1 Yoshiki Ueta,1 Tone Suzuki3,4
1Department of Ophthalmology, Shinseikai Toyama Hospital, Imizu, Toyama, Japan; 2Department of Ophthalmology, University of Tokyo Hospital, Bunkyo, Tokyo, Japan; 3Department of Ophthalmology, Dokkyo Medical University Saitama Medical Center, Koshigaya, Saitama, Japan; 4Hikari Eye Clinic, Yoshikawa, Saitama, Japan
Correspondence: Takafumi Suzuki, Department of Ophthalmology, University of Tokyo Hospital, 7-3-1 Hongō, Bunkyo, Tokyo, 113-8655, Japan, Tel +81 3 3815 5411, Email [email protected]
Purpose: To investigate changes in intraocular pressure (IOP) associated with accommodation in patients with intermittent exotropia (X(T)), and to evaluate how these changes are affected by strabismus surgery.
Patients and Methods: Thirty-one consecutive patients scheduled for strabismus surgery due to X(T) were retrospectively analyzed. IOP was measured using a rebound tonometer (iCare) during strabismus examinations under three conditions: binocular viewing at distance (bIOP-D), binocular viewing at near (bIOP-N), and monocular viewing at near (mIOP-N). Correlations were assessed between IOP changes and accommodation-related parameters, including patient age and the change in angle of deviation (AOD) from distance to near. Postoperative alterations in these IOP dynamics were also investigated.
Results: AOD at near was significantly greater than that at distance (p < 0.0001). bIOP-N was significantly lower than bIOP-D in both the non-fixation eyes (p = 0.017) and fixation eyes (p = 0.003). The decrease in IOP from distance to near under binocular viewing (Δd-nIOP) correlated significantly with age in fixation eyes (p = 0.007, r = − 0.473). Δd-nIOP was also significantly correlated with the increase in AOD from distance to near fixation in both non-fixation (p = 0.017, r = 0.424) and fixation eyes (p = 0.002, r = 0.544). Postoperatively, no significant differences between bIOP-D and bIOP-N were found at 1 month (p = 0.230) or 6 months (p = 0.309).
Conclusion: In patients with X(T) who exhibited a larger AOD at near than at distance, near fixation led to a significant IOP reduction. This near-fixation-associated IOP decrease was less evident after strabismus surgery, particularly in non-operated eyes. These findings suggest that ocular alignment and accommodative demand may interact to influence IOP, although confirmation in larger studies is warranted.
Keywords: intraocular pressure, accommodation, intermittent exotropia, strabismus surgery
Introduction
Intraocular pressure (IOP) is regulated by multiple physiological factors, including aqueous humor production, aqueous outflow, episcleral venous pressure, and biomechanical properties of the anterior segment.1 In addition to these intraocular factors, posture, gaze position, accommodation, and mechanical forces from periocular tissues and extraocular muscles may also influence IOP.2–14
iCare has gained broad clinical adoption and has enabled central corneal IOP measurement in a variety of postures,4 gaze positions,3,5 and even in strabismus patients.6,15 Studies on IOP variation with eccentric gaze in healthy eyes have yielded conflicting results. Using iCare, slight eccentric gaze positions (15° in four directions) have been associated with significantly lower IOP compared to primary gaze,3 whereas extreme gaze positions have been shown to cause IOP elevations in both glaucomatous and normal eyes, particularly in the order of temporal > superior > nasal > primary gaze.5 In contrast, studies using implantable IOP sensors have reported IOP reduction in inferonasal gaze at 10°, 20°, and 25°.2 These findings suggest that IOP is not a static parameter, but can be influenced by ocular position.
Furthermore, evidence exists that the extraocular muscle status influences IOP: a decrease in IOP immediately after lateral rectus muscle detachment during strabismus surgery for intermittent exotropia (X(T)) has been reported,8 as well as IOP elevation during upgaze in thyroid eye disease,9 and IOP increase during attempted abduction in patients with highly myopic strabismus.6 These observations suggest that mechanical forces related to extraocular muscles, orbital tissues, or abnormal ocular alignment may affect IOP. However, these studies primarily focused on gaze- or muscle-related mechanical effects, rather than accommodation-related IOP changes during physiological visual tasks.
Accommodation is another important physiological factor that may affect IOP. During accommodation, contraction of the ciliary muscle may alter the configuration of the trabecular meshwork and Schlemm’s canal, thereby influencing aqueous humor outflow.1 Consistent with this plausible mechanism, previous studies in eyes without strabismus have reported IOP reduction during near fixation,10–14 and a recent meta-analysis indicated that accommodation is associated with significant IOP reduction in normal eyes, regardless of the presence of convergence.7
Taken together, gaze position, accommodation, and extraocular muscle condition are intricately associated with IOP dynamics. Intermittent exotropia (X(T)), the most common form of pediatric strabismus, affecting up to 1% of children in their first decade,16 provides a clinically relevant model for investigating IOP dynamics related to accommodation, convergence effort, ocular alignment, and extraocular muscle status. In patients with X(T), the need to maintain phoria or binocular alignment during near fixation may impose additional convergence and accommodative demands, particularly when the angle of deviation (AOD) is larger at near than at distance. This feature allows evaluation of whether near-fixation–related IOP changes are associated not only with accommodation itself, but also with alignment-related convergence and accommodative demands in patients with X(T). In addition, strabismus surgery alters extraocular muscle status and ocular alignment, providing an opportunity to examine whether these IOP dynamics change after surgical correction.
To the best of our knowledge, no previous study has comprehensively examined IOP changes associated with distance fixation, near fixation, and postoperative changes in patients with X(T). Therefore, we retrospectively investigated IOP changes under different viewing conditions during strabismus examinations and after strabismus surgery. We hypothesized that near fixation would be associated with IOP reduction in patients with X(T), consistent with previous findings in non-strabismic eyes, and investigated whether this IOP response was related to accommodation- and convergence-related parameters and altered after strabismus surgery.
Materials and Methods
Ethics Statement
This study adhered to the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board of Shinseikai Toyama Hospital (approval number: 2025–005). Due to the retrospective nature of the study, an opt-out consent process was employed. The requirement for written informed consent was waived by the IRB; however, patients who declined the use of their medical records for research purposes were excluded from the study.
Patients
We retrospectively reviewed medical records from Shinseikai Toyama Hospital to identify consecutive patients diagnosed with X(T) who underwent surgical correction involving medial rectus muscle resection (MRRs) and/or lateral rectus muscle recession (LRRc) performed between September 2020 and January 2024. For postoperative analyses, only patients with a follow-up period of at least six months were included. Exclusion criteria included patients with incomitant strabismus, amblyopia, prior strabismus or intraocular surgery, ocular diseases other than strabismus or cataract, and systemic abnormalities. Additionally, patients with suspected or documented narrow angles were excluded based on slit-lamp and anterior segment evaluations.
Ophthalmic Examinations
Preoperative assessments included a comprehensive ophthalmologic examination: best-corrected visual acuity (BCVA) measured with a Landolt decimal chart (converted to the logarithm of the minimal angle of resolution), objective refraction using an autorefractor (Topcon KR-8100A, Tokyo or Nidek ARK-1, Aichi, Japan) or the Spot Vision Screener (SVS; Welch Allyn, NY, USA), subjective refraction, axial length measurement with OA2000 (Tomey, Nagoya, Japan), IOP using a rebound tonometer (iCare IC100; iCare Finland Oy, Helsinki, Finland), slit-lamp biomicroscopy, and fundus examination.
Postoperative follow-up included BCVA, IOP assessment using the same tonometer, and additional examinations as clinically indicated.
Comparisons were made between the non-fixating eye and the fixating eye for all parameters.
Assessment of Convergence Accommodation
Assessment of convergence accommodation was conducted using the SVS, exclusively in cases deemed clinically suspicious by the evaluating ophthalmologist. Refractive measurements were performed at a viewing distance of approximately 1 m using the internal fixation target of the device under two conditions: (1) binocular open viewing (bSVS) and (2) monocular viewing with occlusion of the fellow eye (mSVS).
Measurement of AOD
Pre- and postoperative angles of deviation (AOD) were measured using the alternate prism cover test (APCT) without prior occlusion adaptation. The fixation and non-fixation eyes were determined based on preoperative clinical assessment of fixation preference during manifest deviation. In patients with alternating fixation, the eye showing relatively weaker fixation tendency during tropia was designated as the non-fixation eye. Preoperatively, additional testing included (1) APCT after 60 minutes of occlusion of the non-fixating eye to elicit the maximum deviation and (2) prism adaptation testing (PAT), with each adaptation period lasting 15 minutes. All AOD measurements were taken in the primary gaze position at both distance (5 m; AOD-D) and near (33 cm; AOD-N). To uncover latent near deviation, a +3.00 diopter lens was placed over one eye during near fixation, and AOD was remeasured. If the AOD increased under this condition, the increased value was regarded as the true AOD at near. All AOD measurements were performed with full refractive correction.
IOP Measurements
Before AOD measurements, IOP was assessed during binocular fixation at distance using a 5-m target (bIOP-D) and at near using a 33-cm target (bIOP-N). During binocular viewing, patients were instructed to fixate on the target with both eyes open, and fixation behavior was clinically monitored by the examiner. Following 60 minutes of occlusion of the non-fixating eye to induce maximum deviation, IOP was measured under monocular fixation at near using a 33-cm target (mIOP-N). While maintaining monocular viewing, the occluded eye was alternated to measure IOP in the fellow eye as well. Postoperative mIOP-N was recorded without the prior 60-minute occlusion. All IOP values represent the average of three consecutive measurements. To reduce fatigue or accommodative aftereffects that could affect subsequent readings, a brief rest period of approximately 30 seconds was included between measurements. All IOP measurements were performed without refractive correction. These IOP measurements were routinely conducted at our institution since 2020 in X(T) patients as part of routine clinical assessment. All data were recorded in standardized templates within the electronic medical records, allowing for retrospective review.
Timing of Examinations
Baseline (Pre) evaluations were conducted 1 day to 2 months prior to surgery. Routine postoperative examinations were performed at 1 day, 1 week, 1 month (1M), 3 months, and 6 months (6M) after surgery. For this study, data from Pre, 1M, and 6M time points were used. All examinations were performed by experienced ophthalmologists and orthoptists. Although examiners differed among patients, each patient was assessed by the same examiner throughout the observation period. Although the exact time of day varied among patients, follow-up examinations for each patient were generally scheduled within the same outpatient session, such as morning or afternoon clinics, to minimize within-patient diurnal variation.
Evaluation of Changes in AOD, IOP, and SVS at Baseline
To assess the increase in AOD from distance to near fixation, AOD-D and AOD-N were compared. To evaluate the effect of accommodation on IOP under phoria-maintaining conditions, bIOP-D and bIOP-N were compared for each eye. To determine the influence of convergence accommodation on IOP, comparisons were made between mIOP-N and bIOP-N, as well as between mSVS and bSVS in each eye.
Correlation Between IOP Changes and Accommodation-Related Parameters
To investigate the relationship between standard accommodation or convergence accommodation and IOP under phoric conditions, we analyzed the correlation between the preoperative change in IOP from distance to near under binocular viewing (Δd-nIOP = bIOP-D – bIOP-N) and accommodation-related factors, including patient age and the change in AOD from distance to near (Δn-dAOD = AOD–N − AOD–D).
Surgical Protocol and Postoperative Care
All surgeries were performed by two experienced surgeons (YU and TKS) under local or general anesthesia. Standard unilateral MRRs and/or LRRc procedures for intermittent exotropia were performed on the non-fixation eye. The rectus muscles were directly reattached to the sclera using 6–0 absorbable suture (VSORB 6–0, double-armed; Kono Seisakusho Co., Ltd., Ichikawa, Japan), without employing adjustable suture techniques. Surgical procedures were standardized according to the institutional protocol for X(T). Postoperative treatment was initiated on the first postoperative day and included topical moxifloxacin 0.5% three times daily, fluorometholone 0.1% four times daily, and bromfenac 0.1% twice daily. These medications were tapered over the course of one month.
Postoperative Changes in AOD and IOP
Changes in AOD for each patient and IOP for each eye were assessed from Pre to 6M. To evaluate the effect of accommodation on IOP under phoria-maintaining conditions, bIOP-D and bIOP-N were compared for each eye at each time period.
Statistical Analysis
All values are presented as means ± standard deviations. Given the relatively small sample size and retrospective study design, non-parametric tests were primarily used. For comparisons between two values, the Wilcoxon signed-rank test was used to analyze changes in AOD within the same patients, changes in parameters within the same eye under different conditions, and differences between non-fixation (operated) eyes and fixation (fellow) eyes under identical conditions. For comparisons involving three parameters, analysis of variance (ANOVA) was performed first; if significant (p < 0.05), Dunnett’s multiple comparison test was subsequently applied as a post hoc analysis. Correlation analyses were conducted using Spearman’s rank correlation coefficient (r). No formal a priori sample size calculation was performed because of the retrospective nature of the study; therefore, the results should be interpreted as exploratory. A p-value of less than 0.05 was considered statistically significant. All statistical analyses were performed using JMP® 18 software (JMP Statistical Discovery LLC, Cary, NC, USA).
Results
Preoperative Analysis
Baseline Characteristics
Baseline demographic and clinical characteristics are summarized in Table 1. A total of 31 patients (14 men and 17 women; mean age, 27.0 ± 23.5 years) were included. No significant differences were observed in any of the preoperative parameters between the non-fixation and fixation eyes (all p > 0.05).
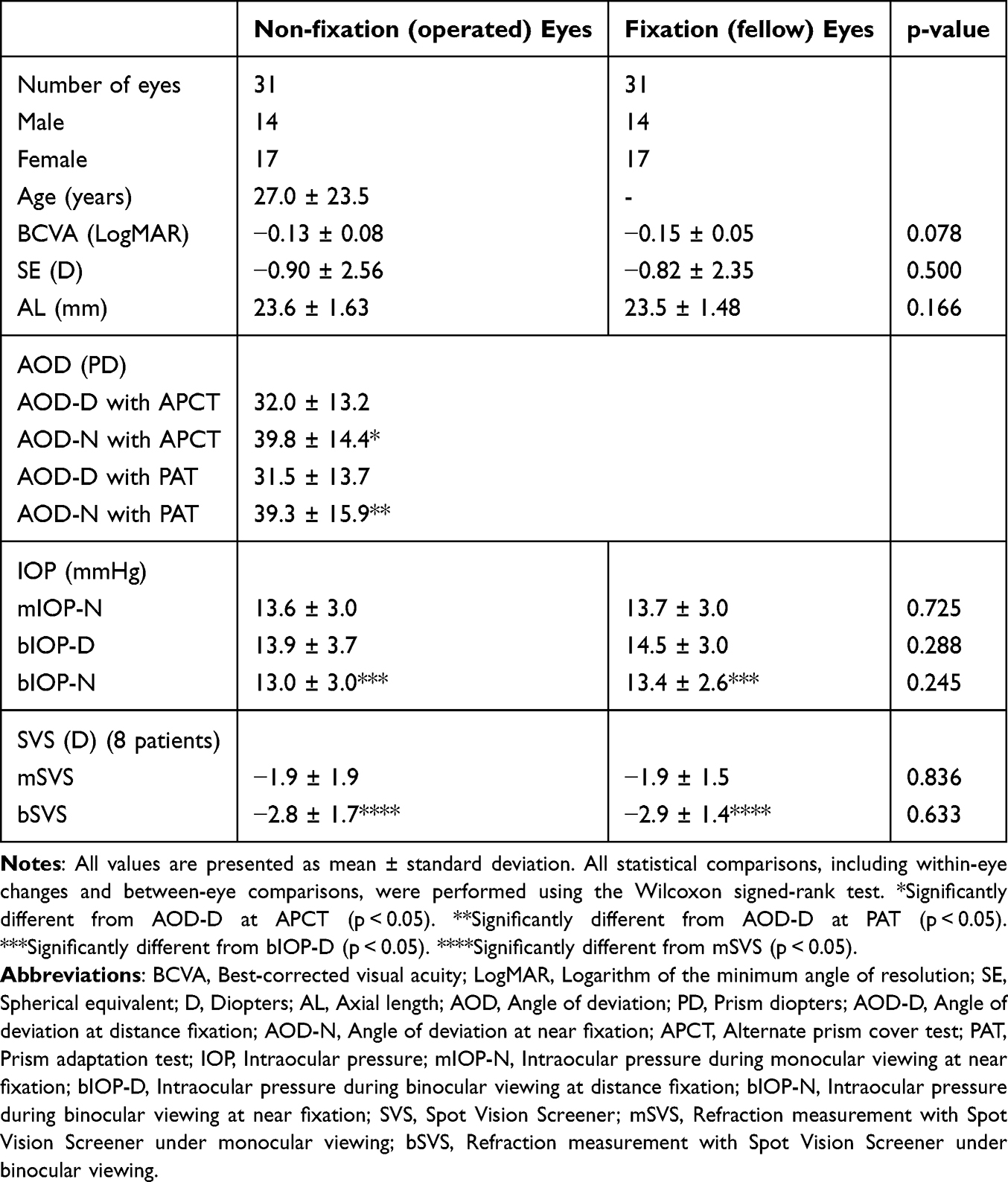 |
Table 1 Preoperative Patient Profiles (n=31) |
Preoperative Changes Under Different Viewing Conditions
AOD-N was significantly greater than AOD-D, both in the APCT and in the PAT (both p < 0.0001).
bIOP-N was significantly lower than bIOP-D in both the non-fixation eyes (p = 0.017) and fixation eyes (p = 0.003). No significant differences were found between bIOP-N and mIOP-N in either eye (non-fixation: p = 0.396; fixation: p = 0.794).
Due to the retrospective nature of the study, SVS measurements were available for only eight patients. In this subset, bSVS measurements were significantly more myopic than mSVS in both the non-fixation eyes (p = 0.016) and fixation eyes (p = 0.008).
Exploratory Correlation Analyses
Δd-nIOP showed a significant correlation with Δn-dAOD in both non-fixation (p = 0.017, r = 0.424) and fixation eyes (p = 0.002, r = 0.544). Δd-nIOP was significantly correlated with age in fixation eyes (p = 0.007, r = −0.473), but not in non-fixation eyes (p = 0.858) (Table 2, Figure 1).
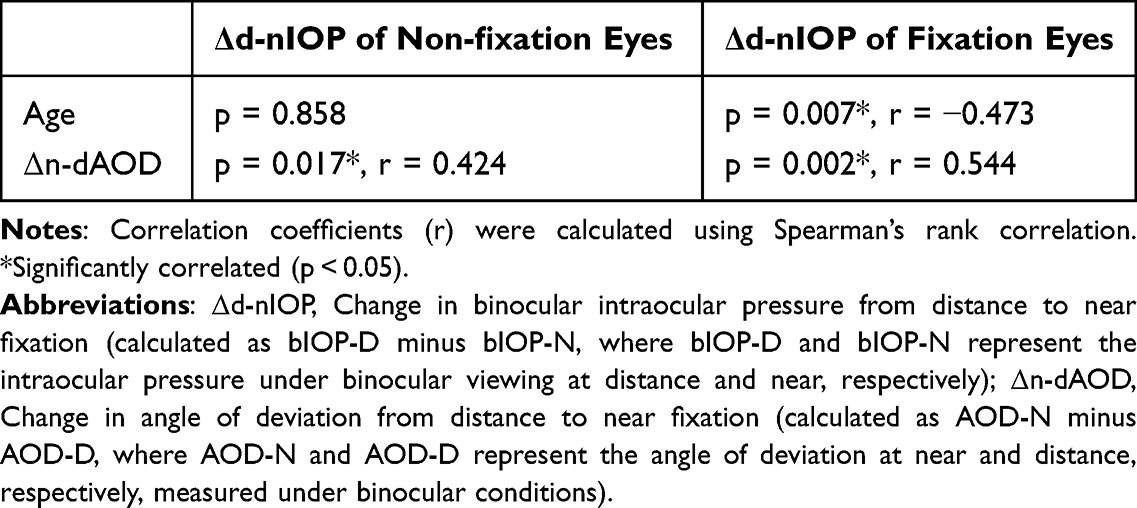 |
Table 2 Correlations of IOP Change with Accommodation-Related Factors |
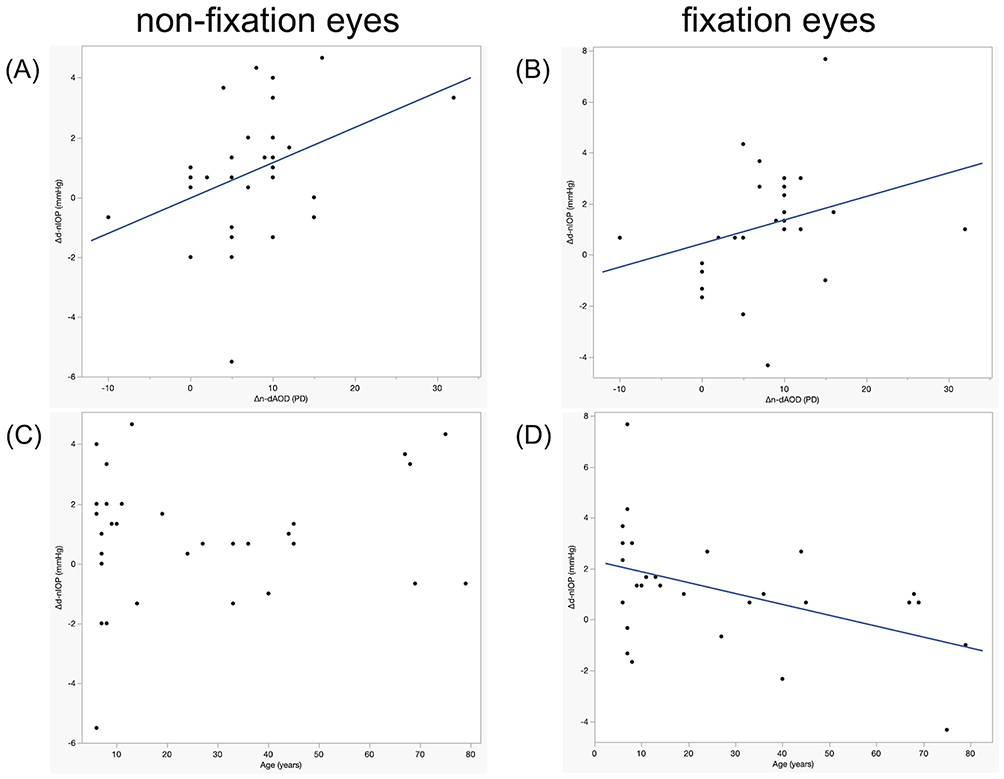 |
Figure 1 Correlation of Δd-nIOP with Δn-dAOD and Age. Correlation coefficients (r) were calculated using Spearman’s rank correlation. (A and B) Δd-nIOP showed a significant correlation with Δn-dAOD in both non-fixation eyes (p = 0.017, r = 0.424) (A) and fixation eyes (p = 0.002, r = 0.544) (B). (C and D) Δd-nIOP was not significantly correlated with age in non-fixation eyes (p = 0.858) (C), but was significantly correlated with age in fixation eyes (p = 0.007, r = −0.473) (D). Abbreviations: Δd-nIOP, Change in binocular intraocular pressure from distance to near fixation (calculated as bIOP-D minus bIOP-N, where bIOP-D and bIOP-N represent the intraocular pressure under binocular viewing at distance and near fixation, respectively); Δn-dAOD, Change in angle of deviation from distance to near fixation (calculated as AOD-N minus AOD-D, where AOD-N and AOD-D represent the angle of deviation at near and distance, respectively, measured under binocular conditions). |
Postoperative Analysis
Among the 31 patients, 17 were followed up for six months after strabismus surgery. The remaining 14 patients were not included in the postoperative analysis because complete 6-month follow-up data were not available. The results are summarized in Table 3. No significant differences in any parameter were observed between the operated eyes (preoperative non-fixation eyes) and the fellow eyes (preoperative fixation eyes) at each time period (all p > 0.05).
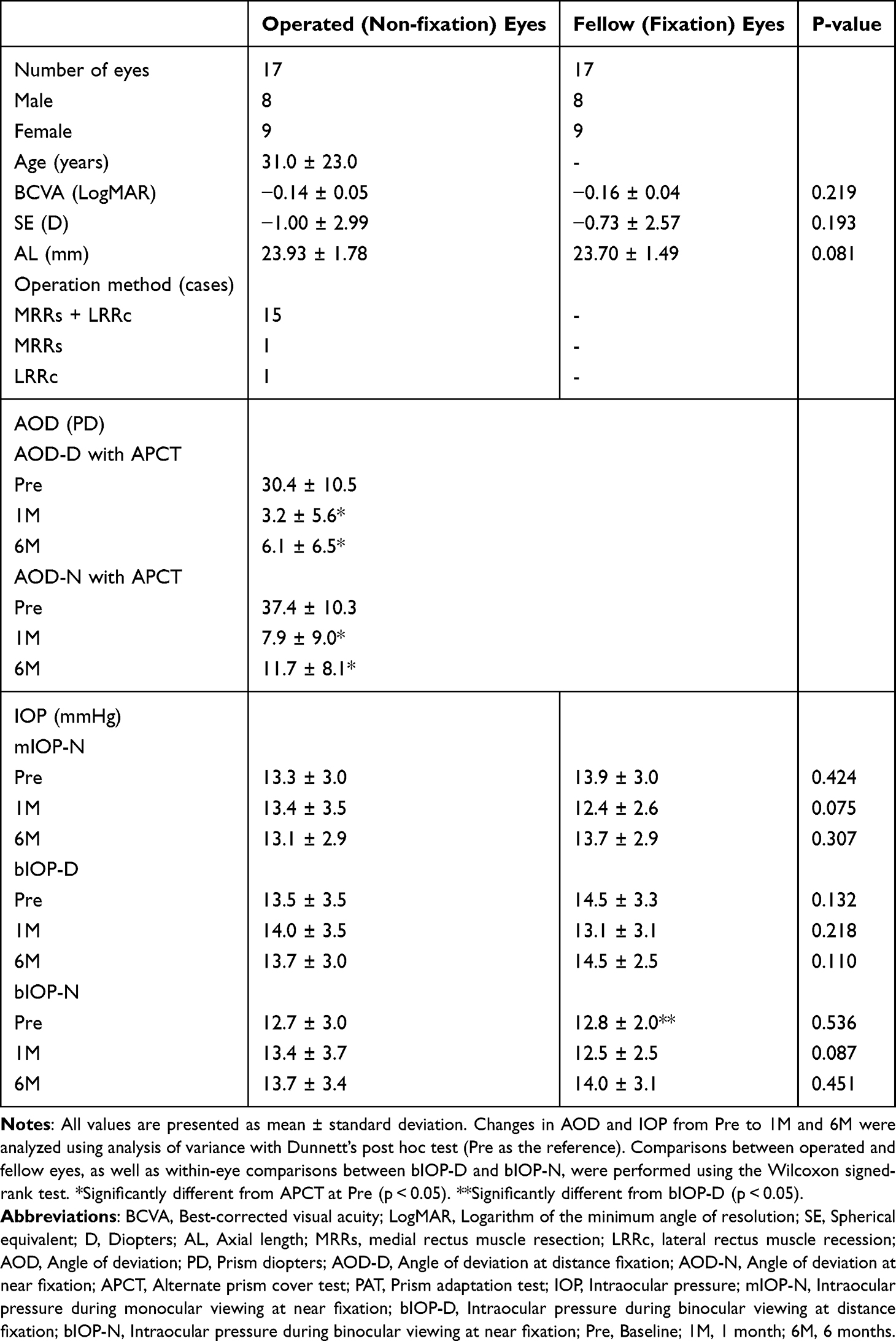 |
Table 3 Operation Methods and Shift in the Values of IOP and AOD from Pre to 6M (n=17) |
AOD-D at both 1M and 6M was significantly reduced compared to baseline (p < 0.0001 for both). Similarly, AOD-N at both time points was also significantly reduced (p < 0.0001 for both). There were no significant changes in mIOP-N, bIOP-D, or bIOP-N from Pre to 6M in either the operated eyes (p = 0.980, p = 0.927, and p = 0.737, respectively) or the fellow eyes (p = 0.277, p = 0.338, and p = 0.227, respectively) (Figure 2).
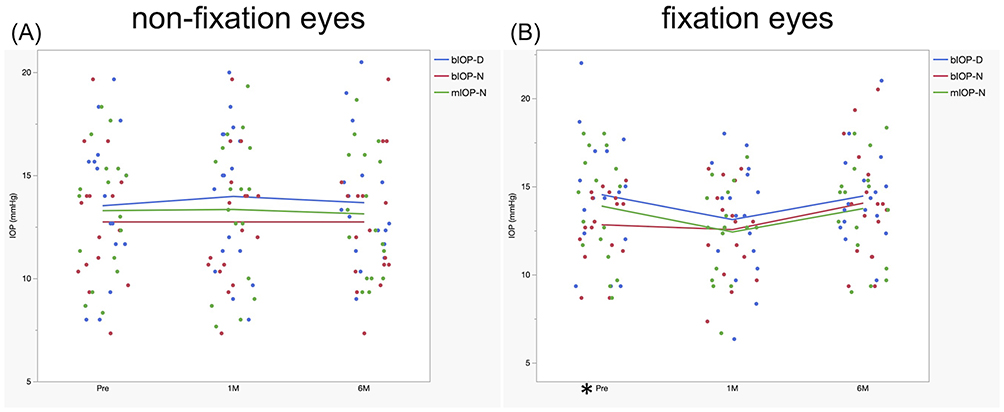 |
Figure 2 Shift of IOP in Operated (non-fixation) and Fellow (fixation) Eyes. IOP changes from Pre to 1M and 6M were analyzed using analysis of variance with Dunnett’s post hoc test (Pre as the reference). Within-eye comparisons between bIOP-D and bIOP-N at each time point were performed using the Wilcoxon signed-rank test. (A) In operated eyes, no significant difference was observed between bIOP-D and bIOP-N at Pre, 1M, or 6M. (B) In fellow eyes, bIOP-N was significantly lower than bIOP-D at Pre (p = 0.006), whereas no significant differences between bIOP-D and bIOP-N were observed at 1M or 6M. Asterisks indicate statistically significant differences (*p < 0.05). Abbreviations: IOP, Intraocular pressure; mIOP-N, Intraocular pressure during monocular viewing at near fixation; bIOP-D, Intraocular pressure during binocular viewing at distance fixation; bIOP-N, Intraocular pressure during binocular viewing at near fixation; Pre, Baseline; 1M, 1 month; 6M, 6 months. |
Preoperatively, bIOP-N was significantly lower than bIOP-D in fixation eyes (p = 0.006), with a mean bIOP-D minus bIOP-N difference of 1.7 mmHg, but the difference was not significant in non-fixation eyes (mean difference, 0.8 mmHg; p = 0.119). Postoperatively, no significant differences were observed between bIOP-D and bIOP-N at either 1M or 6M in the operated eyes (mean differences, 0.6 and 0.0 mmHg; p = 0.112 and p = 0.819, respectively) or fellow eyes (mean differences, 0.6 and 0.5 mmHg; p = 0.230 and p = 0.309, respectively) (Figure 2). Thus, the preoperative difference between bIOP-D and bIOP-N was not observed at postoperative follow-up.
Discussion
This study is the first to investigate the impact of near fixation on IOP and its postoperative changes in patients with X(T). The main finding was that near fixation was associated with a significant reduction in IOP compared with distance fixation. This IOP-lowering effect became less prominent after strabismus surgery, particularly in the non-operated eyes. In addition, greater IOP reduction during near fixation was observed in younger patients and in those with a greater increase in AOD from distance to near.
Preoperative Findings in Light of Previous Literature
Numerous studies have demonstrated IOP reduction during accommodation across various populations—normal eyes, myopic eyes, and eyes with glaucoma. In normal subjects, IOP reduction has been consistently reported during accommodation,10–13,17,18 and confirmed in meta-analyses.7 In myopic eyes, the level of myopia was not found to influence accommodation-induced IOP changes,18 and similar IOP reductions after accommodation were observed between emmetropic and progressive myopic patients.7 In glaucoma patients, results were more variable: for instance, in some cases of normal-tension glaucoma, IOP increased during accommodation, whereas post-trabeculectomy eyes showed negligible changes.19 Importantly, a decrease in IOP has been observed both during fixation on near targets10–13 and during fixation at distance with a −3.0 D lens to avoid convergence.14 These findings suggest that accommodation, rather than convergence, plays a primary role in the reduction of IOP. The principal mechanism is thought to involve increased aqueous humor outflow during ciliary muscle contraction. During accommodation, the longitudinal fibers of the ciliary muscle pull on the scleral spur, widening the trabecular meshwork and Schlemm’s canal, thereby enhancing outflow.1
A previous study has reported that a greater accommodative amplitude in younger individuals is associated with a more pronounced reduction in IOP during accommodation. This effect tends to diminish with age, likely due not only to a decline in accommodative amplitude but also to reduced responsiveness of the trabecular meshwork to ciliary muscle activity.20 In our X(T) cohort, similar trends were observed: younger age correlated with greater IOP reduction in fixation eyes. The absence of this correlation in the non-fixation eyes may be attributed to the limited sample size or to the inclusion of cases—particularly among elderly patients with difficulty maintaining stable phoria—in which IOP measurements were taken at positions deviating from the corneal apex.
In our X(T) patients who exhibited a larger AOD-N than AOD-D, near fixation likely demands greater convergence effort. Given that AOD increases more at near than at distance, and that younger individuals are generally known to exhibit stronger accommodation, including both standard accommodation and convergence accommodation, we believe that near fixation induced excessive accommodation, thereby resulting in a more pronounced IOP reduction compared to distance fixation. While mean bIOP-N appeared lower than mean mIOP-N, the lack of significant difference suggests that convergence accommodation contributed less than standard accommodation under these circumstances. Taken together, these findings support the notion that, as in normal subjects, accommodative stimuli are the primary drivers of IOP reduction in X(T) patients, with minimal contribution from anatomical or mechanical abnormalities of the extraocular muscles.
Postoperative Evaluation
Previous reports on strabismus surgery and IOP are limited. A study in pediatric XT patients noted a transient postoperative IOP increase due to topical steroids, which normalized by 1 month,21 without evaluating the roles of gaze or accommodation. Another study found no significant change in IOP following horizontal muscle surgery,22 consistent with our results.
In our study, although a significant reduction in IOP during near fixation was observed preoperatively, this effect diminished after surgery—most notably in the non-operated eyes, which were not directly affected by the surgical procedure. We interpret this finding to suggest that the excessive convergence accommodation present before surgery, which contributed to enhanced IOP reduction during near fixation, was mitigated postoperatively.
Limitations
This study has several limitations. Its retrospective design and relatively small sample size may limit statistical power. In addition, this study did not include a control group without strabismus, which limits direct comparison of near fixation–related IOP changes between patients with X(T) and non-strabismic individuals. We did not assess IOP under monocular distance fixation. Although patients with suspected narrow angles were excluded based on slit-lamp examination, gonioscopic confirmation of angle status was not available, which limits our ability to fully assess the impact of angle configuration on IOP changes. Central corneal thickness (CCT) was not measured due to the retrospective nature of the study. However, as all IOP comparisons were conducted either within the same eye under different viewing conditions or between both eyes of the same individual, the influence of CCT differences on our findings is expected to be minimal. Since IOP measurements were performed without refractive correction, the degree of standard accommodation and convergence accommodation at distance and near varied among individuals. However, given the consistent physiological principle that both standard accommodation and convergence accommodation are more active at near than at distance, this variability is unlikely to significantly affect the findings of this study. Additionally, the fixed order of IOP measurements may have introduced an order effect, potentially lowering IOP values in later measurements, despite efforts to mitigate this by including rest intervals between measurements and using the average of three readings for each condition. Although examinations for each patient were generally performed during the same outpatient session, such as morning or afternoon clinics, the exact time of day was not strictly standardized, and residual effects of diurnal IOP variation cannot be completely excluded. Not all patients underwent preoperative SVS or cycloplegic testing, and postoperative SVS evaluation was not performed. Despite careful measurement protocols, fixation behavior during binocular viewing was clinically monitored, and sensory status including suppression was assessed preoperatively using the Bagolini striated glasses test. However, fixation stability and suppression were not continuously or quantitatively assessed during IOP measurements, and some patients may not have maintained stable phoria throughout the measurements, potentially influencing central corneal IOP measurements.
Conclusions
In conclusion, near fixation was associated with IOP reduction in patients with X(T), consistent with previous observations in non-strabismic eyes. This response was less evident after strabismus surgery. These findings refine our understanding of the impact of ocular alignment and accommodative demand on IOP. In addition, although the magnitude of IOP change was modest, these results suggest that fixation distance and accommodative demand may be relevant when interpreting IOP measurements in patients with X(T), particularly in those with coexisting ocular conditions in which IOP assessment is clinically important. Future studies should incorporate prospective, large-cohort designs that include non-strabismic subjects as a control group.
Data Sharing Statement
The datasets used and analyzed in the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
This study adhered to the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board of Shinseikai Toyama Hospital (approval number: 2025-005). An opt-out consent process was used, and the requirement for written informed consent was waived.
Funding
No funding was received for this research.
Disclosure
All authors certify that they have no affiliations or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript.
References
1. McDougal DH, Gamlin PD. Autonomic control of the eye. Compr Physiol. 2015;5(1):439–11. doi:10.1002/cphy.c140014
2. van den Bosch JJON, Pennisi V, Invernizzi A, et al. Implanted microsensor continuous IOP telemetry suggests gaze and eyelid closure effects on IOP—a preliminary study. Invest Ophthalmol Vis Sci. 2021;62(6):8. doi:10.1167/iovs.62.6.8
3. Wongwanwatana S, Treesit I, Funarunart P, Iemsomboon W, Choontanom R. Intraocular pressure measurement using iCare rebound tonometer in different positions of eye and different locations on cornea. Med. 2023;102(36):e34874. doi:10.1097/MD.0000000000034874
4. Sang Q, Xin C, Yang D, Mu D, Wang N. Effect of different postures on intraocular pressure in open-angle glaucoma. Ophthalmol Ther. 2024;13(1):149–160. doi:10.1007/s40123-023-00845-3
5. Kim YJ, Moon Y, Kwon AM, Lim HW, Lee WJ. Intraocular pressure according to eye gaze by iCare rebound tonometry in normal participants and glaucoma patients. J Glaucoma. 2021;30(8):643–647. doi:10.1097/IJG.0000000000001883
6. Arai S, Suzuki H, Hayashi S, et al. Intraocular pressure at different gaze positions in patients with highly myopic strabismus. Jpn J Ophthalmol. 2022;66(6):572–578. doi:10.1007/s10384-022-00939-8
7. Ambrosini G, Poletti S, Roberti G, Carnevale C, Manni G, Coco G. Exploring the relationship between accommodation and intraocular pressure: a systematic literature review and meta-analysis. Graefes Arch Clin Exp Ophthalmol. 2025;263(1):3–22. doi:10.1007/s00417-024-06565-z
8. Yoo C, Chang MH, Song JS, Kim SH. Changes in intraocular pressure during strabismus surgery. Can J Ophthalmol. 2010;45(6):602–605. doi:10.3129/i10-049
9. Gomi CF, Yates B, Kikkawa DO, Levi L, Weinreb RN, Granet DB. Effect on intraocular pressure of extraocular muscle surgery for thyroid-associated ophthalmopathy. Am J Ophthalmol. 2007;144(5):654–657. doi:10.1016/j.ajo.2007.07.026
10. Read SA, Collins MJ, Becker H, et al. Changes in intraocular pressure and ocular pulse amplitude with accommodation. Br J Ophthalmol. 2010;94(3):332–335. doi:10.1136/bjo.2009.166355
11. Jenssen F, Krohn J. Effects of static accommodation versus repeated accommodation on intraocular pressure. J Glaucoma. 2012;21(1):45–48. doi:10.1097/IJG.0b013e31820277a9
12. Priluck AZ, Hoie AB, High RR, Gulati V, Ghate DA. Effect of near work on intraocular pressure in emmetropes. J Ophthalmol. 2020;2020:1352434. doi:10.1155/2020/1352434
13. Pakravan M, Samaeili A, Esfandiari H, et al. The influence of near vision tasks on intraocular pressure in normal subjects and glaucoma patients. J Ophthalmic Vis Res. 2022;17(4):497–504. doi:10.18502/jovr.v17i4.12350
14. Blake J, Horgan T, Carroll P, Stokes J, Fitzpatrick P. Effect of accommodation of the lens on ocular pressure. Ir J Med Sci. 1995;164(4):269–270. doi:10.1007/BF02967200
15. Arai S, Suzuki H, Hayashi S, et al. Intraocular pressure changes at different gaze positions after superior rectus muscle–lateral rectus muscle loop myopexy in highly myopic strabismus. Jpn J Ophthalmol. 2024;68(1):26–31. doi:10.1007/s10384-023-01032-4
16. Govindan M, Mohney BG, Diehl NN, Burke JP. Incidence and types of childhood exotropia: a population-based study. Ophthalmology. 2005;112(1):104–108. doi:10.1016/j.ophtha.2004.07.033
17. Yan L, Huibin L, Xuemin L. Accommodation-induced intraocular pressure changes in progressing myopes and emmetropes. Eye. 2014;28(11):1334–1340. doi:10.1038/eye.2014.208
18. Liu Y, Lv H, Jiang X, Hu X, Zhang M, Li X. Intraocular pressure changes during accommodation in progressing myopes, stable myopes and emmetropes. PLoS One. 2015;10(10):e0141839. doi:10.1371/journal.pone.0141839
19. Ha A, Kim YK, Kim JS, Jeoung JW, Park KH. Changes in intraocular pressure during reading or writing on smartphones in patients with normal-tension glaucoma. Br J Ophthalmol. 2020;104(5):623–628. doi:10.1136/bjophthalmol-2019-314467
20. Armaly MF, Rubin ML. Accommodation and applanation tonometry. Arch Ophthalmol. 1961;65:415–423. doi:10.1001/archopht.1961.01840020417016
21. Lee D, Kim MM, Kim WJ. Effect of strabismus surgery on ocular axial length, anterior chamber depth, and intraocular pressure. Med Baltim. 2019;98(22):e15812. doi:10.1097/MD.0000000000015812
22. Hayashi S, Sato M, Miura H, Sugano A, Yamazaki M, Yamashita H. Intraocular pressure decreases after muscle union surgery for highly myopic strabismus. Jpn J Ophthalmol. 2015;59(2):118–123. doi:10.1007/s10384-014-0364-y
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.