Back to Journals » Journal of Healthcare Leadership » Volume 17
Nature and Outcomes of Longitudinal Authentic Leadership Profiles
Authors Cougot B ![]() , Gillet N, Gauvin J, Ollierou F, Le Saout A, Moret L, Tripodi D
, Gillet N, Gauvin J, Ollierou F, Le Saout A, Moret L, Tripodi D
Received 20 November 2024
Accepted for publication 16 March 2025
Published 25 May 2025 Volume 2025:17 Pages 189—209
DOI https://doi.org/10.2147/JHL.S486730
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Baptiste Cougot,1– 3 Nicolas Gillet,1,4,5 Jules Gauvin,2,3 Florian Ollierou,2,3 Alice Le Saout,2,3 Leïla Moret,6,7 Dominique Tripodi2,8
1QualiPsy UR 1901, Université de Tours, Tours, F37000, France; 2Department of Occupational Medicine and Environmental Health, Nantes University Hospital, Nantes, F-44000, France; 3Santé Psychosociale & Santé au Travail, Igéia, Nantes, F-44000, France; 4Institut Universitaire de France (IUF), Paris, F-75000, France; 5Oxford Business College, Oxford, OX1 2AA, United Kingdom; 6Methods in Patients-Centered Outcomes and HEalth Research (SPHERE) Inserm UMR 1246, Nantes and Tours University, Nantes, F-44000, France; 7Department of Public Health, Nantes University Hospital, Nantes, F-44000, France; 8Laboratoire de Psychologie Des Pays de la Loire (LPPL) UR 4638, Nantes and Angers University, Nantes, F-44000, France
Correspondence: Baptiste Cougot, Email [email protected]
Purpose: Although authentic leadership is known to improve caregivers’ functioning, health, and quality of care, information is lacking about whether the authentic leadership subdimensions may be distinguished from an overarching authentic leadership global construct, and how these global and specific factors can combine within various profiles to explain outcomes over time. Relying on an integration of person- and variable-centered perspectives, this study aims to provide a deeper understanding of the dimensionality of the authentic leadership construct. Specifically, it aims to examine the profiles taken by authentic leadership dimensions, document their stability over time, and explore the associations between these profiles and outcomes (need satisfaction, anhedonia, and safety of care).
Methods: A questionnaire was completed twice over a one-year period by 750 healthcare professionals. Latent transition analysis was the primary method of analysis.
Results: Our results showed that employees’ perceptions of authentic leadership behaviors reflected an overarching construct simultaneously coexisting with four specific dimensions (self-awareness, internalized moral perspective, relational transparency, and balanced processing). We identified four profiles highly stable over time: Low Global Authentic, Normative, Low Specific Self-Awareness, and High Specific Balanced Processing. Finally, employees’ global and specific (relatedness, competence, and autonomy) levels of need satisfaction as well as perceptions of safety of care and anhedonia differed as a function of their profile, with the most positive outcomes associated with the Normative profile.
Conclusion: In addition to confirming that authentic leadership may be studied as a global construct, this study highlights the importance of considering the combinations of global and specific factors in explaining variations in caregivers’ need satisfaction, anhedonia, and quality of care over a one year-period. Our findings suggest that managers should strive to implement a complete array of authentic leadership behaviors at a balanced level to ensure positive outcomes.
Keywords: authentic leadership, latent transition analyses, need satisfaction, safety, ill-being, bifactor models
Introduction
Authentic leadership has garnered significant interest in the organizational and managerial sciences (eg, Hoch et al1 and Zhang et al)2 due to its positive outcomes for healthcare organizations and employees.3 For instance, authentic leadership has been found to promote an error management culture and to reduce errors in healthcare settings.4 Additionally, authentic leadership was found to enhance employees’ functioning, particularly by satisfying their psychological needs,5 and to decrease their levels of ill-being.6 In sum, these findings suggest that authentic leadership could be considered as an important factor in ensuring both performance and safety of care, as well as employees’ functioning and health.3 However, several questions remain unanswered, regarding (1) the dimensionality of authentic leadership, (2) the combinations between the global and specific factors of authentic leadership within various profiles, and (3) how these configurations could lead to distinct performance and health-related outcomes. We elaborate on these issues in the following paragraphs.
Authentic leadership, as defined by Walumbwa et al,7 is a constructive leadership behavior encompassing four distinct yet complementary components. In this model, self-awareness reflects leaders who are able to assess their own weaknesses, strengths, and values in order to be more authentic with their employees. Such leaders are thus capable of processing their own perspective while considering others. Balanced processing involves that leaders consider both supporting and opposing opinions before making a decision. Relational transparency refers to transparent relationships between leaders and their employees, and honesty when leaders share their own thoughts and feelings. Finally, internalized moral perspective describes leaders who maintain consistency between their internalized values and their behaviors. There is a general recognition (eg, Schoofs et al8 and Song et al)9 that a thorough examination of authentic leadership should encompass all four components.
Nevertheless, some studies have indicated that employees might perceive authentic leadership behaviors as a global construct.1,2 This global representation is supported by the evidence of stronger correlations with outcomes when authentic leadership is measured as a global factor,10 and by the high correlations reported between the different authentic leadership components.7,11 Nonetheless, previous research has also demonstrated that each of these dimensions has distinct relationships with outcomes (eg, Walumbwa et al,7 Puni & Hilton)12 suggesting that these dimensions can be considered independently. Such considerations raise several important questions: (a) Does the specification of an overarching authentic leadership construct still allow the authentic leadership facets to maintain their specificity; and (b) does such overarching construct encompass the specificities represented by the facets, or do these facets represent separate related factors without any overarching core?13,14 Answering such questions is critical to characterize authentic leadership and to ground its theoretical foundation and dimensionality. For instance, finding that the four authentic leadership facets are no longer identified when considering a global factor of authentic leadership would challenge the current consensus on the four-factor model proposed by Walumbwa et al7 and would invite a reconsideration of previous conclusions about the differential effects of these components. From a practical viewpoint, it could prompt a redesign of authentic leadership counseling and training, encouraging managers to see authentic leadership as a holistic set of behaviors that need to be implemented as a whole to warrant positive effects. Conversely, finding that the facets represent separate related factors without any overarching core would challenge the very existence of an authentic leadership construct as a whole. More generally, it could lead to questioning the dimensionality of authentic leadership, and spur new directions on the effects of authentic leadership as well as the design of interventions and training.
These questions are not clear-cut because research investigating the structure of authentic leadership has primarily relied on the classic confirmatory factor analytic (CFA) method (eg, Walumbwa et al)7 that has limitations restricting its usefulness.15 More precisely, within this framework, an overarching construct can be estimated directly from item information (ie, a one-factor CFA model) or as a higher-order factor derived from a set of factors estimated from item information representing the different facets (ie, hierarchical CFA model). Although the one-factor CFA solution makes it possible to identify a global construct, it prevents the estimation of specific factors. Furthermore, the hierarchical CFA model allows identifying both an overarching construct and specific factors, but does not make possible to know whether the various components retain their specificity once an overarching construct is considered.15 In other words, estimating the global construct as a higher-order factor allows the easy identification of both global and specific factors without providing evidence on the potential co-existence of globality and specificity.13,15,16
Furthermore, beyond clarifying the authentic leadership dimensionality, questions remain about the global and specific factors of authentic leadership combine within profiles, and the effects of such configurations on performance and health-related outcomes. Indeed, research on authentic leadership has generally taken a variable-centered approach, focused on the independent, additive, or interactive effects of authentic leadership on outcomes, thus assuming that these relations would generalize to the whole sample. Fortunately, beyond considering the unique role of different global and specific factors of authentic leadership, person-centered studies allow examination of the various combinations of authentic leadership dimensions within different profiles of workers.17 By considering the unique authentic leadership configurations observed among distinct profiles of employees, this approach will allow us to better understand the authentic leadership profiles that are most optimal for employees and their organizations. For instance, do employees need to simultaneously perceive high levels of authentic leadership across dimensions to maximally benefit from authentic leadership behaviors? In contrast, are specific authentic leadership facets (eg, balanced processing) more critical than others (eg, relational transparency) from an outcome perspective?
Previous research has used a person-centered perspective to examine how components of empowering leadership18 or leader-member exchange19 (LMX) combine within employees. These studies showed that distinct managerial profiles with different global and specific leadership facets could be identified, and that these profiles were associated with differentiated performance and health-related outcomes.14,15 However, no person-centered research has considered the authentic leadership facets proposed by Walumbwa et al.7 Furthermore, no studies have done so while accounting for both the global aspects (common across all components) and the specific (particular to each component and not captured by the overarching construct) aspects of authentic leadership.19,20 Given the potential implications for employees’ performance and health, investigating this question appears important. Moreover, research has yet to examine the temporal evolution of these combinations of authentic leadership dimensions as a cross-sectional research design makes it impossible to assess whether the identified profiles will be replicated over time (within-sample stability) and to assess the stability of these profiles at the employee level (within-person stability).21 Evidence of within-sample stability is a key requirement to ensure that the identified profiles generalize over time rather than to capture ephemeral phenomena likely to reflect random sampling variations and to guide the development of intervention efforts (eg, Sandrin et al).22 Indeed, interventions rely on the assumption that profiles can be changed rather than reflecting rigid psychological traits but also that employees’ profiles are unlikely to change on their own over short periods of time (ie, ideally evidence of stability should be moderate).23
In this study, we explore these questions by examining the authentic leadership profiles (or configurations) that most accurately represent a sample comprising professionals who filled out the Authentic Leadership Questionnaire.7 Furthermore, we estimated these profiles, while incorporating both global and specific (self-awareness, internalized moral perspective, relational transparency, and balanced processing) factors to capture the multidimensionality of authentic leadership.19,20 Importantly, we also investigate how these profiles change over a one-year period in terms of their nature and prevalence, as well as employees’ profile membership. Finally, we also examine how these profiles are related to outcomes and the extent to which these associations are maintained over time in order to investigate the criterion-related validity of these authentic leadership profiles. More specifically, we investigate profile associations with employees’ global and specific (relatedness, competence, and autonomy) levels of need satisfaction as well as perceptions of safety of care and anhedonia (a depressive symptom). Beyond the construct validity perspective, this study should help shed light on how global and specific authentic leadership dimensions can combine to explain safety of care, as well as employees’ functioning and mental health. From a managerial viewpoint, these results should lead to practical recommendations about the implementation of authentic leadership behaviors aimed at fostering positive outcomes.
Co-Existing Global and Specific Authentic Leadership Dimensions
Anchored in Walumbwa et al’s definition of authentic leadership,7 the Authentic Leadership Questionnaire is arguably the most common measure of authentic leadership. Supporting the distinctiveness of the four dimensions (self-awareness, internalized moral perspective, relational transparency, and balanced processing), Guenter et al10 showed that each of them exhibited distinct relationships with outcomes. While recognizing the importance of viewing authentic leadership as a multidimensional construct, research has also indicated that professionals might perceive authentic leadership behaviors as a holistic global dimension.1,2 When considering the Authentic Leadership Questionnaire, these two possibilities suggest that specific levels of self-awareness, relational transparency, internalized moral perspective, and balanced processing could remain unexplained by, and co-exist with, the global levels of authentic leadership. Recent research19,20 has suggested the idea that authentic leadership may exist both as a global construct, capturing what is common among ratings of specific dimensions (ie, self-awareness, internalized moral perspective, relational transparency, and balanced processing), which, in themselves, encompass relevant specifics that remain unexplained by this global entity.
For example, Chénard-Poirier et al20 successfully used a bifactor model of transformational leadership behaviors comprising one transformational leadership global factor and four specific factors representing the individualized consideration, inspirational motivation, intellectual stimulation, and idealized influence facets. Nevertheless, they found weak composite reliability for the idealized influence specific factor, which suggests that this dimension could be largely captured by the global factor, resulting in a specific factor not retaining much specificity. Similar conclusions were reported by Mitropoulou et al24 with a measure of ethical leadership, although they also found evidence that all components shared meaningful associations with covariates. Finally, Gillet et al19 also found support for the need to disaggregate a LMX global factor from four specific factors (loyalty, affect, contribution, and professional respect) in a series of three studies. However, contrasting with previous conclusions, they found that all five factors maintained a significant specificity and played a role in covariate associations. However, it is still unclear whether these results would generalize to new samples and to an authentic leadership measure. Further research is needed to confirm whether sufficient specificity exists at the subscale level in the Authentic Leadership Questionnaire,7 especially when accounting for global levels of authentic leadership. One of the main objectives of this research is to examine whether these results may be generalized to another leadership behavior, namely authentic leadership.
A Person-Centered Perspective on Authentic Leadership
Although substantial research highlights the positive effects of authentic leadership dimensions,1,2 there is a need for a thorough investigation of their combined effects. Two complementary statistical approaches may be used to achieve this objective. First, the disaggregation of the variance attributed to participants’ global and specific levels of authentic leadership, along with the assessment of their unique and complementary impact, can be properly conducted using variable-centered bifactor analyses. However, these analyses summarize data in a single set of “average” parameters, based on the assumption that all employees are drawn from a homogeneous population. Conversely, person-centered statistical approaches are tailored to distinct sub-populations of professionals who display unique configurations of perceived authentic leadership components.19,20 Specifically, person-centered analyses allow for capturing the combined effects of various components of authentic leadership, while excluding the assumption that these effects apply to the entire population. In this research, we rely on this approach to investigate the nature of authentic leadership profiles, using the best-fitting measurement structure identified in preliminary analyses, thus allowing us to combine a bifactor variable-centered method with a person-centered perspective. In sum, this combination of approaches will allow for (1) disaggregating global and specific levels of authentic leadership and (2) capturing the combined effects of its various components. Person-centered findings better align with the way managers and practitioners typically view workers as belonging to distinct categories, rather than focusing on the dominant relationships between variables, as in variable-centered approaches.25 As such, our results are expected to carry significant practical consequences. For example, outlining the outcomes associated with these profiles should aid in identifying which one ought to be targeted for intervention.
Research has begun exploring how various perceived leadership behavior components integrate within workers from a person-centered perspective (eg, Chénard-Poirier et al,20 Dahling et al,26 Gillet et al19 and Stadnick et al).27 Regrettably, many studies have considered leadership behaviors along with other variables as profile indicators (eg, goal orientations: Bae et al;28 self-esteem: Galante & Ward),29 thus hindering the ability to distinguish the effects of perceived leadership behaviors in characterizing the profiles. Among the limited studies focusing exclusively on leadership behaviors, Klug et al30 found four profiles based on the health-oriented leadership components: (1) High care; (2) Low care; (3) Follower sacrifice; and (4) Leader sacrifice. Nonetheless, this research relies on a sample of German white-collar employees in the public sector, suggesting the need for further studies to determine whether these results can be generalized to other sectors, occupations, countries, and leadership behaviors. Likewise, Arnold et al31 found four profiles among a sample of employees belonging to diverse occupations and organizations: (1) Disengaged; (2) Passive; (3) Optimal; and (4) Comprehensive. Although this second study relied on laissez-faire, transformational, and transactional leadership behaviors that are significantly related to authentic leadership behaviors,1 these findings imply that there may be a limited value in differentiating these leadership components.
Nonetheless, this previous research has relied on leadership behaviors other than authentic leadership, and above all without considering both the global and specific components of authentic leadership. Yet, previous research13,14,32 has demonstrated that person-centered analyses can result in an inaccurate estimation of profiles when relying on indicators that do not capture global and specific components (eg, similar levels across indicators, such as the profiles identified by Chénard-Poirier et al).18 Indeed, while relying on a questionnaire assessing three types of empowering leadership (ie, delegation, coaching, and recognition), Chénard-Poirier et al18 found four distinct profiles exhibiting varying levels of empowering leadership: (1) Optimal (23% of the sample with high levels of coaching, recognition, and delegation); (2) Moderately Empowered Task-Focused (21% of the sample with average levels of coaching, recognition, and delegation); (3) Moderately Empowered Social-Focused (32% of the sample with slightly above average levels of coaching, recognition, and delegation); and (4) Non-Empowered (24% of the sample with low levels of coaching, recognition, and delegation). Although several profiles could be identified, they exhibited similar levels across dimensions, implying that this set of profiles reflects more global levels of empowering leadership rather than distinct combinations with varying levels of empowering leadership across dimensions. This is potentially due to the failure to estimate the empowering leadership global factor that coexists with specific dimensions.13 In such cases, controlling for global levels is recommended to identify clearly distinct profiles.13,32 More generally, these findings have not yet been confirmed using a combination of bifactor models and person-centered approach, nor have they been expanded in relation to the model of authentic leadership proposed by Walumbwa et al.7
Considering the lack of prior person-centered research disaggregating global and specific components in identifying authentic leadership profiles,7 we propose as an open question the number and structure of profiles that would best represent workers’ perceptions of authentic leadership configurations. Nevertheless, given that previous research was based on a variety of indicators, methods, and samples, the majority of evidence leads us to expect three profiles: Low Authentic Leadership, Moderate Authentic Leadership, and High Authentic Leadership configurations. In contrast, given that the bifactor method we used here facilitates the identification of profiles with more distinct qualitative differences,19,20 anticipating additional profiles defined by a clearer differentiation among the specific and global authentic leadership factors seems reasonable.
A Longitudinal Person-Centered Perspective
Another objective of this study is to examine the stability of the authentic leadership profiles over a one-year period. Based on previous research,33,34 this time lag is expected to be long enough to surpass daily fluctuations (eg, Yagil & Medler-Liraz),35 yet short enough to account for changes that might be missed over longer intervals (eg, Baron).36 As mentioned above, confirming the stability of person-centered configurations is essential to support their usefulness in guiding the design of specific interventions targeting distinct profiles of employees.17
It is important to consider two different types of longitudinal stability.22,37 Within-sample stability, the first type of longitudinal stability, refers to the fact that the nature of the profiles themselves may evolve throughout the study period. For instance, the structure or number of profiles might evolve, indicating that the group of participants has undergone significant external or internal transformations, or that the profiles may have limited value in guiding intervention design, as they appear to represent transient phenomena. Changes in structure and number of profiles refer to two subtypes of within-sample profile stability: structural (same nature of profiles) and configural similarity (same number of profiles).21 In contrast, contextual transformations can have effects on profile size (distributional similarity), or change the extent to which members within specific profiles are similar (dispersion similarity). The non-confirmation of these two subtypes of within-sample profile stability does not rule out the use of profile solutions in guiding intervention design; rather, it suggests that the profiles exhibit a certain level of sensitivity to external or internal transformations. The second form of longitudinal stability is called within-person stability. It reflects the extent to which workers transition from one profile to another over time.22,37 Such changes can occur without any within-sample changes.
Up to now, investigations on perceived leadership behavior profiles have been cross-sectional. However, a longitudinal study38 of employees’ perceptions of authentic leadership showed a moderately high level of stability over fourteen months (r = 0.62). Kinnunen et al33 also demonstrated similar results over periods of eight to 22 months (r = 0.59 to 0.79). Based on these observations, we anticipate finding a moderately high level of within-person stability, along with clear indications of dispersion, structural, and configural within-sample similarity. Nevertheless, we leave open the questions of whether the predominant transition from one profile to another (within-person transition), will be downward (toward less authentic profiles), lateral (toward distinct profiles exhibiting similar levels of authentic leadership) or upward (toward more authentic profiles), and whether the relative size of the profiles (distributional similarity) will change over time.
A Construct Validation Perspective
An additional crucial step in assessing the construct validity of profile configurations, particularly when using a primarily inductive method like the one used in this study,32 is to investigate their implications (both theoretical and practical) by examining the relationships between profile membership and outcomes.17,39,40 Without information on the outcomes of authentic leadership profiles, it is not possible to accurately determine the actual value of the various profiles, thus complicating the decision of which profile should be targeted for intervention. As mentioned above, we consider the role of workers’ global and specific (autonomy, competence, and relatedness) levels of need satisfaction as well as perceptions of safety of care and anhedonia as outcomes of the authentic leadership profiles. This set of variables was retained for its complementarity, aiming to reflect employees’ health and performance within care domains, as well as well-known psychological mechanisms associated with optimal functioning, namely need satisfaction.41 First, anhedonia is a central symptom of depression (eg, De Beer et al)42 and represents a loss of interest and pleasure for ordinary aspects of life, including pleasant events such as work.43 Beyond health, it can provide insight into how authentic leadership profiles may prevent negative experiences and loss of interest in both work and personal lives. Second, safety of care is directly related to the core mission of healthcare organizations that aim to provide high-quality care, and thus serves as a key indicator of organizational performance.44 Third, according to self-determination theory,41 three psychological needs – relatedness, competence, and autonomy –must be fulfilled to facilitate effective functioning at work and ensure psychological health. More precisely, need satisfaction mediates the effects of the working environment on employees’ health and performance, and thus can be seen as a necessary condition for employees’ optimal functioning.41 In sum, by considering these outcomes, we will be able to identify the most adaptive profiles of authentic leadership for employees’ functioning, health, and performance that should thus be targeted for interventions.
Previous variable-centered research has already demonstrated positive effects of authentic leadership on these outcomes. According to self-determination theory,41 employees’ psychological needs are met in an environment that supports their autonomy. Leroy et al5 considered that authentic leadership represented behaviors facilitating the development of employees’ autonomy. More specifically, authentic leaders take employees’ opinions into account, give them constructive feedback without any manipulative intent, and encourage initiative-taking, thus resulting in higher levels of employees’ psychological need satisfaction. Authentic leaders may also reduce the likelihood that their employees will feel disinterest in their work since authentic leadership is related to employees’ motivation for self-development and personal growth.45 In such environments, employees are interested and stimulated by their work because they can develop their intuition, improve their knowledge, and acquire new skills.46 Finally, authentic leadership may be related to an increase in healthcare workers’ quality of care as it facilitates team effectiveness.47 Authentic leadership also facilitates the development of an error management culture (eg, better communication, encouraging practices for early detection and monitoring), which in turn is negatively related to the frequency of errors.4
Considering these results, we can generally expect profiles with higher global and specific levels of authentic leadership to be associated with the most positive outcomes – namely, lower levels of anhedonia and higher levels of need satisfaction and safety of care. However, formulating accurate hypotheses about the relationships between authentic leadership profiles and outcomes is challenging, given the lack of prior person-centered studies on authentic leadership, as addressed in this study (ie, proposing a relevant disaggregation of the global and specific factors of the Authentic Leadership Questionnaire). Nevertheless, previous findings from variable-centered research and observations from the few previous person-centered studies of leadership behaviors can be informative.
Previous investigations have shown that higher global levels of authentic leadership or specific levels of self-awareness, internalized moral perspective, relational transparency, and balanced processing tend to be related to lower levels of stress and cynicism, and to higher levels of autonomy and performance.1,2 Other studies have also shown that global levels of authentic leadership were positively associated with psychological need satisfaction8,9 and psychological empowerment.46 In addition, Chénard-Poirier et al18 demonstrated that the most negative outcomes (ie, the lowest degrees of behavioral empowerment) were observed in the Non-Empowered profile, followed by the Moderately Empowered Task-Focused profile, by the Moderately Empowered Social-Focused profile, and, lastly, by the Optimal profile. Similarly, Gillet et al19 demonstrated that the most adaptive functioning (eg, the highest levels of job satisfaction and well-being) was associated with the profile exhibiting the highest global levels of LMX, coupled with aligned specific levels of LMX across dimensions (Normative profile). In sum, these prior results lead us to expect that profiles exhibiting higher global levels of authentic leadership (eg, High Authentic Leadership) will be associated with higher levels of perceived safety of care, higher global and specific (relatedness, competence, and autonomy) levels of need satisfaction, and lower levels of anhedonia, than profiles with lower global levels of authentic leadership (eg, Low Authentic Leadership).
Beyond the positive effects of global levels of authentic leadership, previous findings also revealed that the balance across the global and specific levels of authentic leadership within profiles might be important in explaining positive outcomes. For instance, although Gillet et al19 demonstrated that the most adaptive functioning was associated with the profile exhibiting the highest global levels of LMX, they also showed that the least desirable outcomes (eg, the highest levels of emotional exhaustion, and the lowest levels of job satisfaction and positive affect) were associated with the profile exhibiting the lowest global levels of LMX, coupled with a generally misaligned configuration (Low Exchange profile). More generally, when considering the profiles exhibiting various global and specific levels of LMX, global levels of LMX were not sufficient to explain the effects of profiles on outcomes. For example, workers characterized by a Moderate Exchange with Low Loyalty and High Respect profile and a Moderate Exchange with Low Affect profile displayed similar levels of well-being and job satisfaction but higher levels of affective commitment than those characterized by a Moderate Exchange with High Affect and Low Respect profile and a Moderately Low Exchange with High Loyalty and Low Respect profile. Considering these results, we also expect that balanced profiles across global and specific levels of authentic leadership (eg, Normative profile) would be related to more positive outcomes than unbalanced ones. This is in line with the within-domain exacerbation phenomenon suggesting that exposure to inconsistent interactions with supervisors (eg, combining high and low authentic leadership across dimensions) is stressful for employees.20
Research Methodology
Participants and Procedures
Employees working in two sub-centers of a large French university hospital complex were invited to complete an electronic questionnaire in 2018 and 2019. Each sub-center comprised 20 to 25 care units spanning various medical and surgical specialties (eg, nephrology, neurology, cancerology, traumatology), making the targeted population representative of the French hospital setting. The targeted sub-centers were selected based on (1) their wide variety of medical and surgical specialties; (2) their large size that allowed for the recruitment of a substantial sample; (3) their accessibility, making data collection convenient; and (4) their agreement to participate in this research.
We invited all employees of the two sub-centers to participate in the present research during their mandatory medical checkup in the hospital’s occupational health department. Each employee was informed of this data collection by their managers and invited to contact the occupational health department. To improve participation, the coordination team sent a letter and made up to three phone calls to all potential participants at their workplace inviting them to participate and setting up an appointment to begin data collection. After three phone calls (including a message on the answering machine) without any response, an Email was sent inviting employees to call back one of the members of the research team.
Welcome and study explanation were performed by a clinical research nurse. Participants were included based on the following criteria: (1) working in a care unit within the two targeted sub-centers, and (2) providing written informed consent to participate in the study. After questionnaire filling on tablet, participants were received by the occupational physician for the medical check-up. Sociodemographic data, authentic leadership, safety of care, and need satisfaction were collected with a self-report questionnaire. Anhedonia was assessed with a structured clinical interview performed by the occupational physician during the medical check-up. In the event of refusal to participate, professionals were seen for their medical checkup without any data collection.
A total of 750 participants completed the questionnaire at Time 1 (T1), with a follow-up rate of 72% (539 participants) at Time 2 (T2). The sample at T1 represented 48.22% of the total targeted population within the two sub-centers. More precisely, 77% of the nurses, 74% of the nurse assistants, 80% of the secretaries, 43% of the hospital service agents (eg, cleaning, meal delivery), and 41% of the physicians working in the two sub-centers agreed to participate, making the sample broadly representative of the variety of occupations in the hospital. Baseline sample characteristics are detailed in Table S1. In accordance with the characteristics of the target population, most of the participants were women (87.2%), and the mean age was 40.40 years old (SD = 9.71). In addition, 66.7% of the participants worked full time, and 91.4% worked as civil servants, with 5.2% of them on probation. Other participants worked on permanent (0.4%) or fixed-term (8.1%) contracts. Finally, 77.1% of the sample worked during day, 13.7% at night, and 9.2% with a rotating day/night schedule.
Research Instruments
All questionnaires were displayed in French language. Considering that the authentic leadership questionnaire had not been translated and validated in French, a translation back-translation process was performed prior to the study by members of the research team and professional translators.48
Employees’ authentic leadership perceptions were assessed using the Authentic Leadership Questionnaire (ALQ)7 which comprises 16 items measuring: Self-awareness (eg, “My manager seeks feedback to improve interactions with others”; αt1 = 0.81; αt2 = 0.85), relational transparency (eg, “My manager says exactly what he or she means”; αt1 = 0.83; αt2 = 0.86), internalized moral perspective (eg, “My manager demonstrates beliefs that are consistent with actions”; αt1 = 0.81; αt2 = 0.84), and balanced processing (eg, “My manager solicits views that challenge his or her deeply held positions”; αt1 = 0.73; αt2 = 0.76). Participants were invited to answer on a 5-point scale ranging from “not at all” to “frequently, if not always”.
Need satisfaction was assessed with the nine-item questionnaire developed and validated by Gillet et al49 in the professional context. The scale measures relatedness (eg, “I have a lot of sympathy for the people I interact with”; αt1 = 0.74; αt2 = 0.80), competence (eg, “I often feel very competent”; αt1 = 0.74; αt2 = 0.78), and autonomy (eg, “I generally feel free to express my ideas and opinions”; αt1 = 0.57; αt2 = 0.75) need satisfaction. Participants were invited to answer on a 7-point scale ranging from “strongly disagree” to “strongly agree”.
Workers’ safety of care perceptions were assessed with a single item proposed within the Hospital Survey on Patient Safety Culture (HSOPSC):44 “Please give your unit an overall grade on patient safety”. Participants were invited to answer on a 5-point scale ranging from “poor” to “excellent”.
Anhedonia was assessed with the SDI.43 The occupational physician conducted the interview with the four questions devoted to the assessment of loss of interest or pleasure (eg, “Do you enjoy ordinary things in life and pleasant events less than usual”) and the evaluation of frequency and duration (eg, “Has this been the case nearly every day and most of the day for two weeks or more”). The participants were considered to exhibit anhedonia if they experienced loss of interest or pleasure every day and most of the day for two weeks or more, based on the criteria specified in the fourth edition of the Diagnostic and Statistical Manual (DSM-IV).43
Analyses
Preliminary Analyses
Preliminary factor analyses were conducted to assess the psychometric properties of all multi-item measures (factor structure, composite reliability, factor correlations, and measurement invariance over time). Supplementary Material 1 and Tables S2–S6 display these analyses in the online supplements. Factor scores (derived from the preliminary analyses) were used to conduct the main analyses,17,21,50 as they facilitate partial control of unreliability51 while preserving the configuration of the measurement model (eg, invariance; Morin et al).13
Model Estimation
The maximum likelihood robust (MLR) estimator was used for models estimation, as implemented in Mplus 8.7.52 Mplus is considered a robust statistical software for conducting factor analyses and latent profile analyses,53 and is commonly used in person-centered studies (eg, Caesens et al;54 Gillet et al).19 The full information maximum likelihood (FIML) method was used to handle missing responses. This procedure allows for the inclusion of all available information in model estimation (without any missing data imputation), ensuring that all participants who completed the questionnaire at least once (n = 750) could be considered. Therefore, there was no need for the suboptimal listwise deletion strategy, which would have limited analyses to participants (n = 540) who responded at both time points. FIML is as effective as the multiple imputation strategy, but more efficient in terms of computational resources.55 Considering that the start values impact model estimation within latent profile analyses (LPA), all models were estimated with 5000 sets of random start values, allowing 1000 iterations each, and final stage optimization was conducted on the 200 best solutions. These numbers were changed to 10000, 1000, and 500 for the longitudinal analyses.
Latent Profile Analyses (LPA)
LPA models summarize the multivariate distribution of scores on profile indicators by identifying a finite number of latent profiles or subpopulations of participants. These profiles are defined by distinct configurations on these indicators, while also accounting for within-profile variability across all indicators.56 These profiles are called latent to indicate their probabilistic nature.32 Specifically, a probability of belonging to each of the latent profiles is given to each participant, allowing for the estimation of the LPA model and accounting for classification errors. For this study, we used the five authentic leadership factors as indicators to estimate the time-specific LPA models. Profile solutions were estimated at each time point, including one to eight profiles with the means of the indicators freely estimated (global levels of authentic leadership, and specific levels of internalized moral perspective, balanced processing, relational transparency, and self-awareness).53
Model Comparison and Selection
The decision on the number of profiles to select depends on an assessment of profiles in terms of meaningfulness, alignment with theory, and statistical adequacy.39,57 Some statistical indicators56 may support the decision: a lower value on the sample-size Adjusted BIC (ABIC), Bayesian Information Criterion (BIC), Consistent AIC (CAIC), and Akaïke Information Criterion (AIC) indicate better fitting models. In addition, a better fit relative to a model with one fewer profile can be indicated by significant p-values on the Bootstrap Likelihood Ratio Test (BLRT) and the adjusted Lo, Mendell and Rubin’s Likelihood Ratio Test (aLMR).58
Based on statistical research, the BLRT, ABIC, CAIC, and BIC, but not the aLMR and AIC, can be regarded as effective in determining the number of latent profiles.59,60 Therefore, we will not use the aMLR and AIC for model comparison and selection; they are reported for transparency. Because all these tests are highly dependent on sample size,39 they frequently struggle to identify a definitive number of profiles. For this reason, it is generally advised to use a graphical representation of these indicators, known as an elbow plot. Using this plot, the optimal solution can be identified by detecting a plateau in the decrease in the statistical indicators values.25 Lastly, we report the entropy, which summarizes the classification accuracy (from 0 to 1), for transparency purposes. However, this should not be used to choose the optimal profile solution.61
Longitudinal Tests of Profile Similarity
The two time-specific LPA solutions will be combined to estimate a longitudinal LPA, assuming the same number of profiles is extracted at each measurement point.62 This longitudinal LPA will allow for tests of within-sample profile similarity over time. These tests were conducted according to the recommendations of Morin et al,21 with further optimizations for the longitudinal context by Morin and Litalien.63 To begin with, this sequential approach examines whether the same number of profiles is found at each measurement point. Then, a longitudinal model of configural similarity, combining the two time-specific solutions, can be estimated. Next, equality constraints can be applied to the within-profile means (for structural similarity), variances (for dispersion similarity), and size (for distributional similarity). In order to contrast these models, the ABIC, BIC, and CAIC can be used; each type of profile similarity is considered supported if at least two of these indices decrease after the application of equality constraints.21
Latent Transition Analyses (LTA)
Then, in order to examine transitions in profile belonging and within-person stability, the most similar longitudinal LPA solution will be specified as an LTA solution.64 The manual three-step approach65 will be used to guide the specification of this LTA model and all subsequent analyses, following the guidelines set by Morin and Litalien.63 For a comprehensive overview of the technical and practical aspects of estimating LPA and LTA, readers are invited to consult Morin and Litalien.53
Predictors and Outcomes of Profile Membership
We examined the degree to which the relationships between profiles, predictors (for predictive similarity), and outcomes (for explanatory similarity) were stable over time. Multinomial logistic regression link function was used to specify the association between demographics (sex, age, status, and position) and profile membership across four models. A null effects model was first estimated, assuming no relations between the profiles and these variables. A second model was then specified, freely estimating the effects of these demographic variables, which were allowed to vary over time and as a function of T1 profile membership. This model allows for the assessment of the effects on specific profile transitions. A third model was then estimated, in which predictions were specified to differ over time only. Finally, a fourth model was estimated, imposing equality constraints on these associations over time (a model of predictive similarity).
We included the time-specific outcome measures (psychological need satisfaction, safety of care, and anhedonia) and allowed them to vary according to profile membership at each time point. Since they were jointly included, outcomes’ levels at T2 are statistically controlled for their shared variance with the levels at T1 (ie, stability). Explanatory similarity was evaluated by imposing equality constraints on these associations over time. The statistical significance of between-profile differences in outcome levels was assessed using the multivariate delta method.66
Results
Latent Profile Analyses (LPA)
Table S7, along with Figures S1 and S2, presents each of the time-specific LPA solutions with their statistical indicators in the online supplements. A clear dominant solution could not be identified using these indicators at both time points. Fortunately, a plateau was observed at both time points between three and five profiles, as indicated by the elbow plots. A careful examination of these solutions revealed that they were highly similar across time points. In addition, it was revealed that the adding profiles enhanced the model’s meaning up to four profiles. A split of one profile into smaller ones, representing a similar configuration, was observed when a fifth profile was added. The decision was made to select the four-profile solution at both time points, on the basis of this examination, for further analyses.
Table 1 displays the fit indices from all longitudinal models. Beginning with a model of configural similarity that included four profiles at each time point, equality constraints were gradually introduced. Lower BIC and CAIC values were observed for the second model, thus supporting structural similarity. Higher values on BIC, CAIC, and ABIC were observed for the third model, leading to the rejection of dispersion similarity. Finally, a comparison of the model of distributional similarity with the model of structural similarity revealed lowest values on BIC and CAIC, supporting distributional similarity. The model of distributional similarity was retained for interpretation. It is graphically displayed in Figure 1. Tables S8 and S9 present the detailed parameter estimates in the online supplements. The model of distributional similarity is associated with a high level of classification accuracy across profiles at T1 (74.9% to 92.2%) and at T2 (83.9% to 91.6%).
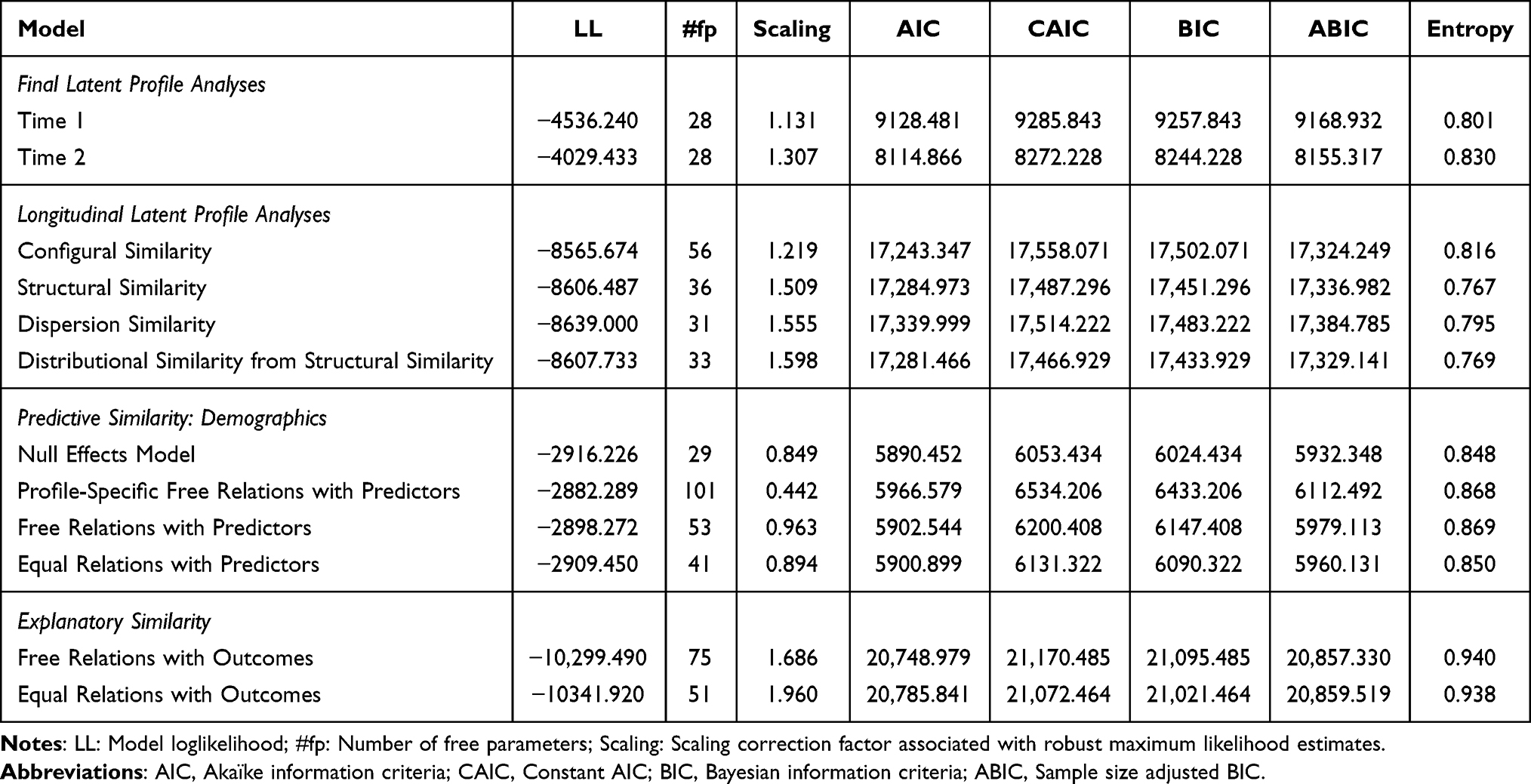 |
Table 1 Results From the Time-Specific and Longitudinal Models |
 |
Figure 1 Graphical Representation of the Final Four-Profile Solution. |
Profile 1 exhibits very low global levels of authentic leadership, moderately low specific levels of balanced processing, and average specific levels of transparency, moral perspective, and self-awareness. This Low Global Authentic profile characterizes 12.44% of the participants. Profile 2 represents workers reporting average global levels of authentic leadership and specific levels of self-awareness, moral processing, transparency, and balanced processing. This Normative profile characterizes 73.83% of the workers. Profile 3 represents workers reporting very low specific levels of self-awareness, average global levels of authentic leadership and specific levels of transparency and moral perspective, and moderately high specific levels of balanced processing. This Low Specific Self-Awareness profile characterizes 9.39% of the workers. Finally, Profile 4 represents workers reporting very high specific levels of balanced processing, high specific levels of self-awareness, average global levels of authentic leadership and specific levels of moral perspective, and moderately low specific levels of transparency. This High Specific Balanced Processing profile represents 4.35% of the workers.
Latent Transitions Analyses (LTA)
Table 2 displays the transition probabilities estimated within the LTA solution. Membership into Profiles 1 (Low Global Authentic: Stability of 91.7%), 2 (Normative: Stability of 97.0%), 3 (Low Specific Self-Awareness: Stability of 85.0%), and 4 (High Specific Balanced Processing: Stability of 100.0%) were very stable over time. Participants exhibiting very low global levels of authentic leadership at T1 (Low Global Authentic profile), when they shift to another profile at T2, they transition to the Normative (2.7%) and Low Specific Self-Awareness (5.6%) profiles. For members of the Normative profile at T1, transitions seem to mainly involve the Low Global Authentic profile at T2 (3.0%). Finally, when shifting to another profile at T2, members of the Low Specific Self-Awareness profile seem to transition to the Normative (10.8%), Low Global Authentic (2.8%), and High Specific Balanced Processing (1.4%) profiles at T2.
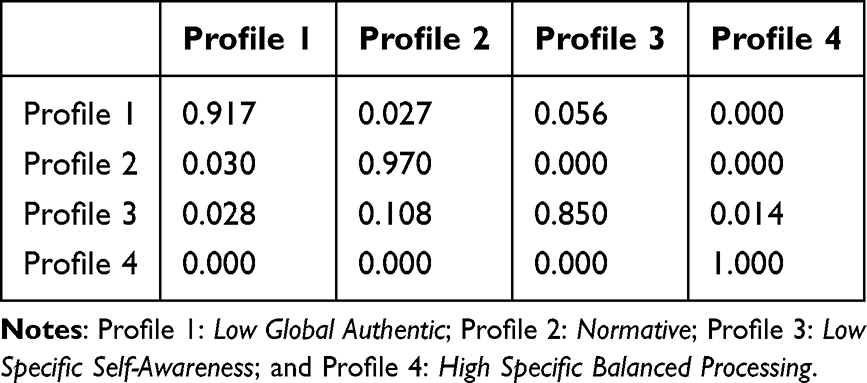 |
Table 2 Transitions Probabilities |
Predictors of Profile Membership
Congruent with the absence of associations between the demographic variables and profile membership, the null effects model exhibited the lowest values on all information criteria (Table 1). The absence of associations between the profiles and these variables was also confirmed through the examination of parameter estimates.
Outcomes of Profile Membership
The lowest values on the BIC and CAIC were observed for the model of explanatory similarity (see Table 1), which was thus supported by the data. Table 3 displays the average levels of each outcome across profiles. Clear differentiations were found across all profiles. Profile 2 (Normative) was associated with the highest global levels of need satisfaction, followed equally by Profiles 1 (Low Global Authentic) and 3 (Low Specific Self-Awareness), and finally by Profile 4 (High Specific Balanced Processing). Profile 4 (High Specific Balanced Processing) was associated with the highest specific levels of relatedness need satisfaction, followed equally by Profiles 2 (Normative) and 3 (Low Specific Self-Awareness), and finally by Profile 1 (Low Global Authentic). Profile 4 (High Specific Balanced Processing) was associated with the highest specific levels of competence need satisfaction, followed equally by Profiles 1 (Low Global Authentic) and 2 (Normative), and finally by Profile 3 (Low Specific Self-Awareness). Profiles 3 (Low Specific Self-Awareness) and 4 (High Specific Balanced Processing), which did not differ between them, were associated with higher specific levels of autonomy need satisfaction than Profiles 1 (Low Global Authentic) and 2 (Normative), which did not differ between them. Profiles 2 (Normative) and 3 (Low Specific Self-Awareness), which did not differ between them, were associated with higher levels of safety of care than Profiles 1 (Low Global Authentic) and 4 (High Specific Balanced Processing), which did not differ between them. Finally, Profiles 1 (Low Global Authentic) and 4 (High Specific Balanced Processing), which did not differ between them, were associated with higher levels of anhedonia than Profile 2 (Normative).
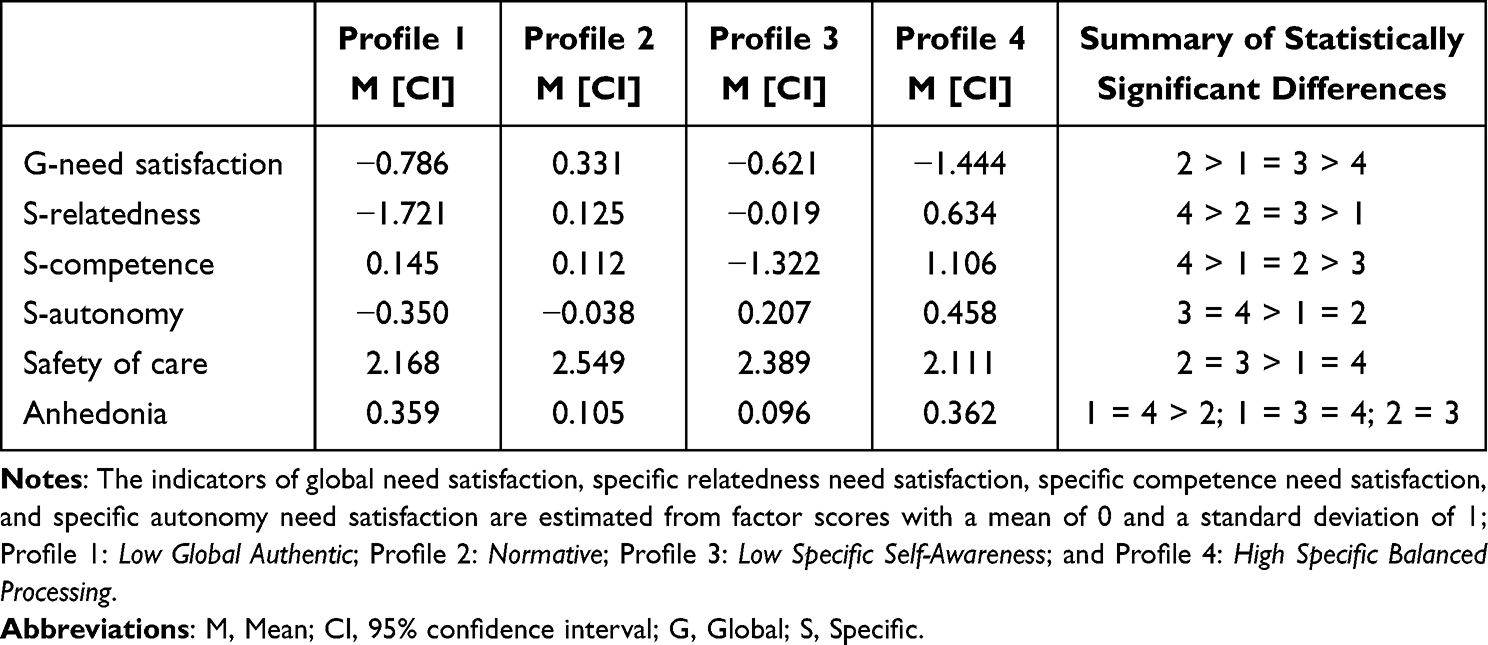 |
Table 3 Associations Between Profile Membership and the Outcomes Taken From the Model of Explanatory Similarity (Equal Across Time Points) |
Discussion
Authentic Leadership Profiles
Four distinct authentic leadership profiles were identified in the present research: (1) Low Global Authentic, (2) Normative, (3) Low Specific Self-Awareness, and (4) High Specific Balanced Processing. These results are consistent with those found in previous studies relying on other conceptualizations of leadership behaviors (eg, Chénard-Poirier et al;20 Gillet et al).19 Indeed, as expected, we identified a profile with low global levels of authentic leadership (Low Global Authentic profile). This profile was also characterized by moderately low specific levels of balanced processing, and average specific levels of transparency, moral processing, and self-awareness. As expected, we also identified not one but three profiles (Normative, Low Specific Self-Awareness, and High Specific Balanced Processing profiles) with average global levels of authentic leadership. The Normative profile was characterized by similarly average specific levels across dimensions. Unlike the two other profiles with average global levels of authentic leadership, this profile still reflects consistent leadership behaviors that are not dominated by a specific behavior.19 Interestingly, this profile was the largest and covers almost three-quarters of employees (73.83%), suggesting that a majority of employees perceive their supervisor as someone who generally demonstrates balanced authentic leadership behaviors towards them.
We also identified a Low Specific Self-Awareness profile and a High Specific Balanced Processing profile with different levels across the specific leadership behaviors, thus confirming the need to take into account specific self-awareness, balanced processing, moral perspective, and transparency leadership behaviors rather than only focusing on some specific behaviors (eg, moral perspective; Alavi et al)67 or on global authentic leadership behaviors.1,2
Nevertheless, these two profiles were the smallest in terms of size and concerned only 9.39% (Low Specific Self-Awareness profile) and 4.35% (High Specific Balanced Processing profile) of the participants. From a practical point of view, such results suggest that few employees ultimately perceive their supervisor as inconsistent across specific authentic leadership behaviors, as such a posture is probably difficult to manage over time for both supervisors (who may feel uncomfortable and lost in the way they act) and employees (who may feel deprived and suffer from this ambiguity).20 More surprisingly, we did not identify, as expected, a profile with high global levels of authentic leadership. Interestingly, Gillet et al19 also did not identify a profile with high or very high global levels of LMX, but rather a Normative profile with moderately high levels on this dimension. Further research relying on bifactor models of leadership should be conducted to examine whether we could identify such profiles with high global levels of leadership. Additional studies will also have to be carried out in order to discover the working conditions or individual characteristics that could contribute to the development of such profiles.
Outcomes of Authentic Leadership Profiles
Our results showed numerous associations between profile membership and the outcomes. In the following paragraphs, we detail the benefits and disadvantages of each of the four profiles identified. First, our results revealed that the most positive outcomes (eg, the highest levels of global need satisfaction and safety of care, and the lowest levels of anhedonia) were associated with the Normative profile followed by the Low Specific Self-Awareness profile. Not surprisingly, the most favorable profile for employees’ functioning is the one with the highest global levels of authentic leadership.3,7 This suggests that employees seem to experience the most optimal functioning when their supervisor is perceived as having integrity, not shirking their responsibilities, and making rational decisions.
Interestingly, the Normative and Low Specific Self-Awareness profiles were both characterized by average specific levels of transparency and moral perspective. These results are thus consistent with those already demonstrated in previous person-centered research emphasizing the positive effects of balanced levels of leadership behaviors.19,20 Of particular importance is that the Low Specific Self-Awareness profile was also characterized by higher specific levels of balanced processing and much lower specific levels of self-awareness. First, these results are consistent with the positive effects of balanced processing found in previous studies (eg, Rego et al).68 They may also suggest that moderately high specific levels of balanced processing may compensate for lower global levels of authentic leadership to achieve equivalent levels of safety of care. Nevertheless, when comparing the differences between the Low Specific Self-Awareness and High Specific Balanced Processing profiles, what seems to be most important are the low specific levels of self-awareness.
More specifically, the Low Specific Self-Awareness and High Specific Balanced Processing profiles have radically different levels of self-awareness (low vs high) and this difference appears to lead to very differentiated effects on global need satisfaction and safety of care. Indeed, the Low Specific Self-Awareness profile was associated with higher levels of global need satisfaction and safety of care than the High Specific Balanced Processing profile. These results thus suggest that low specific levels of self-awareness may compensate for lower global levels of authentic leadership to lead to positive outcomes at least when they are coupled with average specific levels of transparency and moral perspective, and moderately high specific levels of balanced processing. In this sense, one can imagine that leaders who share information (transparency), ask for opinions before making a decision (balanced processing), and do what they say (moral perspective) could foster employees’ global need satisfaction, even if they lack awareness about their impact on followers (self-awareness). According to authentic leadership theory,7 we can suppose that such settings already give employees the opportunity to get information (through transparency), express themselves (through balanced processing), and exert an impact on their work (though moral perspective), which in turn allows them to fulfill their needs, and handle their work efficiently.3
Although self-awareness implies that leaders have a significant impact on their staff, it may also reflect the leaders’ decision flexibility insofar as it involves the ability to know when to re-evaluate their position.7 From this perspective, the Low Specific Self-Awareness profile could reflect an authentic yet directive leadership style, combining moderate transparency, balanced processing, and moral perspective with strong inflexibility concerning the decisions they made. Such practices could have positive outcomes as authoritative forms of leadership help employees cope with ambiguity or uncertainty at work, and prevent the burden of communication and decision-making, particularly when employees have no time to communicate (eg, due to workload).69
In contrast, similar levels of global authentic leadership and specific moral perspective combined with higher specific levels of self-awareness and balanced-processing (and to a lesser extent with lower specific levels of transparency) within the High Specific Balanced Processing profile did not lead to the same benefits. First, high to very high specific levels of self-awareness and balanced-processing can intrinsically induce negative outcomes that cannot be compensated for. On the one hand, although a low specific level of self-awareness could represent decision inflexibility, a high level could represent strong decision flexibility, characterized by the leaders’ tendency to frequently re-evaluate their position. On the other hand, such behaviors could make organizations and decisions unstable and ambiguous, thwart need satisfaction, and lead to lower pleasure and efficacy at work.69,70
Furthermore, a very high specific level of balanced-processing could reinforce this mechanism. In fact, although moderate levels of balanced-processing can be considered as a resource,3,7 very high levels could reflect leaders’ excessive tendency to ask for opinions and information. Such behaviors could thus represent an additional burden for employees, requiring frequent decision-making and information processes in addition to their regular workload.71,72 In this sense, leaders’ incentives towards employees to foster decision-making and innovation have been found to be associated with increased employees’ perceived stress.73
Very high specific levels of balanced-processing, combined with high specific levels of self-awareness, could lead employees to perceive their supervisors as ineffective or unqualified. Indeed, one can imagine that leaders’ frequent self-re-evaluation of their position (self-awareness), combined with frequent requests for opinions and information to make decision (balanced processing), could lead employees to perceive that their leader is unable to make decisions and expects them to provide direction.74 In turn, such situations could foster ambiguity and uncertainty at work as suggested above, as well as poor trust in the leader,74 resulting in poor leader-member exchange and negative outcomes.75,76 Such negative feelings could also be reinforced within the High Specific Balanced Processing profile due to the lower specific levels of transparency, which could induce imbalance or inequity in information sharing and access (ie, although employees are invited to share their views and information, leaders lack of transparency). In this sense, informational justice has been found to moderate the effect of job insecurity, such that a lack of informational justice reinforces the negative effect of job insecurity on performance because employees lack the resources they need to cope efficiently with ambiguity.77
Nevertheless, despite these potential explanations, it should be stressed that the results differed according to the outcomes considered. More specifically, although the High Specific Balanced Processing profile was associated with adverse outcomes for the majority of the dimensions considered, it was still associated with the highest specific levels of relatedness, competence, and autonomy (together with the Low Specific Self-Awareness profile) need satisfaction. Such results suggest that what differentiates this High Specific Balanced Processing profile from the others, namely higher specific levels of balanced processing and self-awareness are beneficial at least for employees’ feelings of relatedness and competence. They have important practical implications, suggesting that employees can benefit, at least for a limited number of outcomes, from exposure to specific balanced processing and self-awareness leadership behaviors, as long as global levels of authentic leadership remain average. In fact, according to authentic leadership theory,7 balanced processing and self-awareness can generally be considered as resources that help empower employees and foster self-development, as well as foster identification and trust in the leaders, both of which lead to positive outcomes.3 Moreover, as expression of leader authentic functioning, balanced processing and self-awareness are thought to promote followers’ expression of their true selves at work,7 leading them to experience strong feelings of autonomy, competence, and relatedness.5 A combination of high to very high levels of specific self-awareness and balanced processing (within the High Specific Balanced Processing profile) may thus be associated with higher specific levels of autonomy, competence, and relatedness. Interestingly, it should be noted that the High Specific Balanced Processing and Low Specific Self-Awareness profiles, both of which present the highest specific levels of balanced processing, were associated with the highest level of specific autonomy need satisfaction. This result suggests that balanced processing, specifically calling for alternative views to make decision, may be particularly important in fostering employees’ autonomy experiences at work. Although we have attempted to provide potential explanations for these double-edged sword effects associated with the High Specific Balanced Processing profile, additional research is needed to better understand the mechanisms underlying these effects.
The effects associated with the Low Global Authentic profile were also not fully in line with our expectations. On the one hand, as expected, this profile was associated with the lowest levels of specific relatedness need satisfaction, specific autonomy need satisfaction (together with the Normative profile), and safety of care (together with the High Specific Balanced Processing profile), and the highest levels of anhedonia (together with the High Specific Balanced Processing profile). These results confirm that low global of authentic leadership are generally associated with adverse outcomes.3,7 On the other hand, and more surprisingly, the Low Global Authentic profile was also associated with higher global levels of need satisfaction than the High Specific Balanced Processing profile, and with higher specific levels of competence need satisfaction than the Low Specific Self-Awareness profile. If we refer specifically to global levels of need satisfaction, the rather balanced levels of specific leadership behaviors observed in the Low Global Authentic profile might be more beneficial than the much more differentiated specific levels within the High Specific Balanced Processing profile.
Nevertheless, as mentioned above, balanced levels of specific leadership behaviors alone are not sufficient to produce positive effects, as evidenced by the higher global levels of need satisfaction displayed by employees within the Normative profile (also characterized by balanced levels of specific behaviors but by significantly higher global levels of authentic leadership) compared to those within the Low Global Authentic profile. Furthermore, employees who perceive their supervisor simply as unauthentic and as someone they cannot rely on might see their sense of competence increase because they have a higher self-esteem and know that they can only rely on their expertise and know-how to perform well in their work.78 Employees faced with such unauthentic leadership behaviors could also implement effective coping strategies such as avoidance, social support, or resistance in order to limit their stress levels and compensate for their supervisors’ suboptimal leadership in order to maintain high levels of work performance.79,80
Theoretical Implications
In sum, our results make a significant contribution to the authentic leadership literature by highlighting the value of using a person-centered approach coupled with bifactor models. We identified different combinations of global authentic leadership and specific self-awareness, balanced processing, moral perspective, and transparency leadership behaviors confirming that supervisors may tap into different types of leadership behaviors when interacting with their subordinates.19,20 Specifically, these results make a real contribution to the literature by demonstrating that supervisors can exhibit, at the same time, average global levels of authentic leadership and low (Low Specific Self-Awareness profile) or high (High Specific Balanced Processing profile) specific levels of self-awareness. Interestingly, prior research had already identified profiles with different specific levels of leadership behaviors (eg, Chénard-Poirier et al18 and Gillet et al)19 but without relying on supervisors’ authentic leadership behaviors7 as in the present study.
In addition to gaining a better comprehension of the characteristics of different profiles of authentic leadership behaviors, this study also provides insight into the implications of these profiles in terms of positive (need satisfaction and safety of care) and negative (anhedonia) outcomes for employees and their organization. First, in line with prior studies, the most positive outcomes were experienced by the employees with the highest global level of authentic leadership (Normative profile).3,7 Similarly, our findings revealed that the profiles with more balanced levels across dimensions were associated with more positive outcomes.19,20 This supports the idea that consistent managers may reduce employees’ feelings of ambiguity and uncertainty while fostering more adaptive coping and outcomes. In contrast, inconsistent managers may lead employees to feel uncertain because they cannot anticipate and control their environment, their relations with supervisor, and their own perceptions of themselves.81,82
More surprisingly, the more negative outcomes associated with the High Specific Balanced Processing (relative to the Low Specific Self-Awareness profile) suggest that self-awareness may have contrasting effects, particularly when combined with high balanced processing. As mentioned above, several hypotheses can be formulated. For example, a high level of self-awareness could reflect the managers’ excessive tendency to reevaluate their position and frequently seek opinions and information (especially when combined with high balanced processing). This may contribute to organizational and decision-making instability, creating ambiguity that hinders need satisfaction and ultimately reduces pleasure and efficacy at work.69,70 Although self-awareness is generally considered as an occupational resource (as indicated by the positive outcomes associated with the Normative profile characterized by average levels of specific self-awareness), our results highlight the importance of considering the combined effects of authentic leadership behaviors to better understand their impact on employees and organizations. More generally, our results have both theoretical and practical implications by showing, for the first time, the need to consider specific self-awareness, balanced processing, moral perspective, and transparency leadership behaviors as a complement to global authentic leadership behaviors. These specific behaviors play a major role in defining the profiles, with quite different levels within some identified profiles.
Implications for Practice
According to the present findings, managers should try to increase their global authentic leadership behaviors and to display balanced specific behaviors as the Normative profile was associated with positive outcomes. In other words, our results indicate that managers should adopt the full set of authentic leadership behaviors to ensure the most positive outcomes among their subordinates. On the contrary, managers who exhibit low levels of both global and specific authentic leadership behaviors, as well as those who behave in an unbalanced manner, may lead their employees to experience negative outcomes.
More specifically, our results suggest that managers should avoid a specific combination of high to very high specific self-awareness and balanced processing coupled with moderate levels of global authentic leadership and moderate to low levels of specific transparency and morale perspective behaviors (ie, the High Specific Balanced Processing profile). Although our results revealed that this profile could facilitate specific relatedness and competence need satisfaction, the negative effects of this profile on global need satisfaction and safety of care, as well as the positive association found with anhedonia, suggest that the combination of these authentic leadership behaviors may be particularly harmful. Informing healthcare managers about such results appears particularly critical as the High Specific Balanced Processing profile initially seems to be aligned with common recommendations from authentic leadership theory. Yet, although this profile is characterized by high to very high scores on two of the four specific authentic leadership behaviors, its development should not necessarily be promoted and encouraged. Rather, managers should rely on the full range of authentic leadership behaviors and try to maintain a balance across dimensions to ensure positive effects.
Interestingly, authentic leadership interventions have been successfully implemented and can be useful in reinforcing supervisors’ training and development. For instance, Dirik and Intepeler23 found that authentic leadership training increased head nurses’ and nurses’ perceptions of global authentic leadership behaviors. Organizational factors may also facilitate or hinder the implementation of authentic leadership behaviors.83 For instance, if supervisors face too many hindrances in their daily work and are under a great deal of pressure from their healthcare organization, they will find it difficult to behave as an authentic leader and will tend to turn instead to abusive leadership practices in order to regain control84 or to laissez-faire leadership behaviors to escape their demanding leadership responsibilities.85 In this case, it might be useful to encourage them to proactively identify the occupational situations in which such behaviors might occur.86
More generally, our results suggest that supervisors should give priority to their overall mode of functioning toward their subordinates,87 since it appears that global levels of authentic leadership play an important role in predicting employees’ functioning, regardless of the specificity of authentic leadership behaviors. Such an approach does not mean, however, that specific transparency, moral perspective, balanced processing, and self-awareness leadership behaviors should be totally banished, as the present findings revealed that certain combinations of specific authentic leadership behaviors may have positive effects on certain outcomes, even more so when global levels of authentic leadership remain dominant.
Limitations and Suggestions for Future Research
Limitations of the current research must be highlighted. First, we relied solely on self-report questionnaires, which implies that social desirability biases may play a role in our results. To reduce this concern, future research should include informant ratings (eg, supervisor, customers, colleagues) and objective measures (eg, official data about turnover, absenteeism, performance). Second, this study only covered healthcare workers who lived and worked in France. Additional studies will be needed to test the replicability of the current findings to a variety of work settings, cultures, languages, and countries. Finally, we only considered the predictive role of demographics (sex, age, status, and position). Future research may investigate how other job (eg, challenge and hindrance demands, organizational dehumanization) and personal (eg, workaholism, proactive personality) characteristics predict authentic leadership behaviors profiles (eg, Gillet et al88 and Sandrin et al).89 Likewise, other negative (eg, counterproductive behaviors, absenteeism) and positive (eg, creativity, organizational citizenship behaviors) outcomes, coupled with psychological mechanisms (eg, work engagement, recovery experiences), could be included to better understand the implications of these authentic leadership profiles (eg, Drouin Rousseau et al90 and Huyghebaert-Zouaghi et al).91
Conclusion
This person-centered research makes it possible to consider the full range of authentic leadership behaviors7 perceived by followers and shows how important it is to take into account these different types of leadership behaviors in order to better understand the complexity of the nature of authentic leadership profiles and their effects on outcomes. However, further studies are needed to confirm whether the profiles identified in this study can be replicated across different conceptualizations of leadership behaviors, as well as in diverse occupations, cultures, and countries.
Abbreviations
ABIC, sample-size Adjusted Bayesian Information Criterion; aLMR, Lo, Mendell and Rubin’s Likelihood Ratio Test; AIC, Akaïke Information Criterion; ALQ, Authentic Leadership Questionnaire; CAIC, Consistent Akaïke Information Criterion; BLRT, Bootstrap Likelihood Ratio Test; BIC, Bayesian Information Criterion; CFA, Confirmatory Factor Analyses; DSM-IV, Diagnostic and Statistical Manual; HSOPSC, Hospital Survey on Patient Safety Culture; FIML, Full Information Maximum Likelihood; LMX, Leader-Member Exchange; LPA, Latent Profile Analyses; LTA, Latent Transition Analyses; MLR, Maximum Likelihood Robust estimator; SDI, Short Depression Interview.
Data Sharing Statement
Our dataset will be accessible upon reasonable request, commencing three years following the conclusion of the study, through the corresponding author.
Ethical Statement
The research protocol, identified as GNEDS02122018 and reviewed and approved by the Nantes University Hospital Ethics Committee (GNEDS), is registered with the reference number NCT04010773 on ClinicalTrials.gov. All procedures adhered to the guidelines outlined in the Declaration of Helsinki. This study is a component of the Chrysalide research project (Cougot et al, 2019).
Acknowledgments
In addition to the authors listed, the project benefitted from the involvement and contributions of various professionals and individuals. These include research nurses (Annaïs Thureau, Solenn Renault, Jeremy Thureau), physicians from the Occupational Medicine Department who assisted in data collection (Guerric Fourneau, Claire Gordeeff, Mickael Humilier, François Léger, Loïc Louisy, Amélie Mear, Pierre-Alban Pioch, Stéphanie Grégoire), psycho-sociologists (Marine Robert, Thomas Sterchi, Arnaud Lecun), and psychology students (Arthur Peltier, Antoine Tastayre, Annaël Joubert, Lucille Boulery, Kiliane Chabonnel, Mélanie Gendron, Lola Garcia Dupuis, Hugo Normand) supervised by the coordination team.
Funding
This research received full financial support from the French Ministry of Health (Direction Générale de l’Offre de Soin) totaling €498,180, as part of the PREPS (Programme de Recherche sur la Performance du Système de soin) under the grant number PREPS-16-681. The allocation of the grant underwent peer review by an independent scientific committee. The funder was not involved in the formulation of the protocol, execution of the study, data collection, analysis, interpretation, or selection of results for presentation, nor in the chosen methods of publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hoch JE, Bommer WH, Dulebohn JH, Wu D. Do ethical, authentic, and servant leadership explain variance above and beyond transformational leadership? A meta-analysis. J Manage. 2018;44(2):501–529. doi:10.1177/0149206316665461
2. Zhang Y, Guo Y, Zhang M, Xu S, Liu X, Newman A. Antecedents and outcomes of authentic leadership across culture: a meta-analytic review. Asia Pac J Manag. 2022;39(4):1399–1435. doi:10.1007/s10490-021-09762-0
3. Alilyyani B, Wong CA, Cummings G. Antecedents, mediators, and outcomes of authentic leadership in healthcare: a systematic review. Int J Nurs Stud. 2018;83:34–64. doi:10.1016/j.ijnurstu.2018.04.001
4. Farnese ML, Zaghini F, Caruso R, Fida R, Romagnoli M, Sili A. Managing care errors in the wards: the contribution of authentic leadership and error management culture. Leadersh Organ Dev J. 2018;40(1):17–30. doi:10.1108/LODJ-04-2018-0152
5. Leroy H, Anseel F, Gardner WL, Sels L. Authentic leadership, authentic followership, basic need satisfaction, and work role performance: a cross-level study. J Manage. 2015;41(6):1677–1697. doi:10.1177/0149206312457822
6. Laschinger BL, Consiglio C, Read E. The effects of authentic leadership, six areas of worklife, and occupational coping self-efficacy on new graduate nurses’ burnout and mental health: a cross-sectional study. Int J Nurs Stud. 2015;52(6):1080–1089. doi:10.1016/j.ijnurstu.2015.03.002
7. Walumbwa FO, Avolio BJ, Gardner WL, Wernsing TS, Peterson SJ. Authentic leadership: development and validation of a theory-based measure. J Manage. 2008;34(1):89–126. doi:10.1177/0149206307308913
8. Schoofs LK, Maunz LA, Glaser J. Multi-level effects of authentic leadership on self-actualization at work – the mediating roles of authentic followership and basic psychological need satisfaction. Curr Psychol. 2024;43(16):14494–14505. doi:10.1007/s12144-023-05480-6
9. Song L, Zhou Y, Wang Y, Feng X, Xiang L. Investigating the antecedents of employee authenticity from the organizational context: the mediating role of basic psychological need satisfaction. Curr Psychol. 2024;43(17):15352–15365. doi:10.1007/s12144-023-05479-z
10. Guenter H, Gardner WL, Davis McCauley K, Randolph-Seng B, Prabhu VP. Shared authentic leadership in research teams: testing a multiple mediation model. Small Group Res. 2017;48(6):719–765. doi:10.1177/1046496417732403
11. Levesque-Côté J, Fernet C, Austin S, Morin AJS. New wine in a new bottle: refining the assessment of authentic leadership using exploratory structural equation modeling (ESEM). J Bus Psychol. 2018;33(5):611–628. doi:10.1007/s10869-017-9512-y
12. Puni A, Hilton SK. Dimensions of authentic leadership and patient care quality. Leadersh Health Serv. 2020;33(4):365–383. doi:10.1108/LHS-11-2019-0071
13. Morin AJS, Boudrias JS, Marsh HW, Madore I, Desrumaux P. Further reflections on disentangling shape and level effects in person-centered analyses: an illustration exploring the dimensionality of psychological health. Struct Equ Model. 2016;23(3):438–454. doi:10.1080/10705511.2015.1116077
14. Morin AJS, Boudrias JS, Marsh HW, et al. Complementary variable- and person-centered approaches to the dimensionality of psychometric constructs: application to psychological wellbeing at work. J Bus Psychol. 2017;32(4):395–419. doi:10.1007/s10869-016-9448-7
15. Morin A, Arens AK, Marsh HW. A bifactor exploratory structural equation modeling framework for the identification of distinct sources of construct-relevant psychometric multidimensionality. Struct Equ Model Multidiscip J. 2016;23(1):116–139. doi:10.1080/10705511.2014.961800
16. Markon KE. Bifactor and hierarchical models: specification, inference, and interpretation. Annu Rev Clin Psychol. 2019;15(1):51–69. doi:10.1146/annurev-clinpsy-050718-095522
17. Meyer JP, Morin AJS. A person-centered approach to commitment research: theory, research, and methodology. J Organ Behav. 2016;37(4):584–612. doi:10.1002/job.2085
18. Chénard Poirier LA, Morin AJS, Boudrias JS. On the merits of coherent leadership empowerment behaviors: a mixture regression approach. J Vocat Behav. 2017;103(Part B):66–75. doi:10.1016/j.jvb.2017.08.003
19. Gillet N, Morin AJS, Cougot B, Fouquereau E. A person-centered perspective on the combined effects of global and specific lmx components for employees. Int J Stress Manag. 2022;29(1):14–30. doi:10.1037/str0000230
20. Chénard-Poirier LA, Morin AJS, Boudrias JS, Gillet N. The combined effects of destructive and constructive leadership on thriving at work and behavioral empowerment. J Bus Psychol. 2022;37(1):173–189. doi:10.1007/s10869-021-09734-7
21. Morin A, Meyer JP, Creusier J, Biétry F. Multiple-group analysis of similarity in latent profile solutions. Organ Res Methods. 2016;19(2):231–254. doi:10.1177/1094428115621148
22. Sandrin E, Morin AJS, Fernet C, Gillet N. A longitudinal person-centered perspective on positive and negative affect at work. J Psychol. 2020;154(7):499–532. doi:10.1080/00223980.2020.1781033
23. Dirik HF, Seren Intepeler S. An authentic leadership training programme to increase nurse empowerment and patient safety: a quasi-experimental study. J Adv Nurs. 2024;80(4):1417–1428. doi:10.1111/jan.15926
24. Mitropoulou EM, Tsaousis I, Xanthopoulou D, Petrides KV. Development and psychometric evaluation of the questionnaire of ethical leadership (QueL). Eur J Psychol Assess. 2020;36(4):635–645. doi:10.1027/1015-5759/a000533
25. Morin AJS, Morizot J, Boudrias JS, Madore I. A multifoci person-centered perspective on workplace affective commitment: a latent profile/factor mixture analysis. Organ Res Methods. 2011;14(1):58–90. doi:10.1177/1094428109356476
26. Dahling JJ, Gabriel AS, MacGowan R. Understanding typologies of feedback environment perceptions: a latent profile investigation. J Vocat Behav. 2017;101:133–148. doi:10.1016/j.jvb.2017.05.007
27. Stadnick NA, Meza RD, Suhrheinrich J, et al. Leadership profiles associated with the implementation of behavioral health evidence-based practices for autism spectrum disorder in schools. Autism. 2019;23(8):1957–1968. doi:10.1177/1362361319834398
28. Bae CL, Hayes KN, DeBusk-Lane M. Profiles of middle school science teachers: accounting for cognitive and motivational characteristics. J Res Sci Teach. 2020;57(6):911–942. doi:10.1002/tea.21617
29. Galante M, Ward RM. Female student leaders: an examination of transformational leadership, athletics, and self-esteem. Personal Individ Differ. 2017;106:157–162. doi:10.1016/j.paid.2016.11.017
30. Klug K, Felfe J, Krick A. Caring for oneself or for others? How consistent and inconsistent profiles of health-oriented leadership are related to follower strain and health. Front Psychol. 2019;10. doi:10.3389/fpsyg.2019.02456
31. Arnold KA, Connelly CE, Gellatly IR, Walsh MM, Withey MJ. Using a pattern-oriented approach to study leaders: implications for burnout and perceived role demand. J Organ Behav. 2017;38(7):1038–1056. doi:10.1002/job.2182
32. Morin AJS, Bujacz A, Gagné M. Person-centered methodologies in the organizational sciences: introduction to the feature topic. Organ Res Methods. 2018;21(4):803–813. doi:10.1177/1094428118773856
33. Kinnunen U, Feldt T, Mauno S. Authentic leadership and team climate: testing cross-lagged relationships. J Manag Psychol. 2016;31(2):331–345. doi:10.1108/JMP-12-2014-0362
34. Read EA, Laschinger HKS. The influence of authentic leadership and empowerment on nurses’ relational social capital, mental health and job satisfaction over the first year of practice. J Adv Nurs. 2015;71(7):1611–1623. doi:10.1111/jan.12625
35. Yagil D, Medler-Liraz H. Feel free, be yourself: authentic leadership, emotional expression, and employee authenticity. J Leadersh Organ Stud. 2014;21(1):59–70. doi:10.1177/1548051813483833
36. Baron L. Authentic leadership and mindfulness development through action learning. J Manag Psychol. 2016;31(1):296–311. doi:10.1108/JMP-04-2014-0135
37. Gillet N, Caesens G, Morin AJS, Stinglhamber F. Complementary variable- and person-centred approaches to the dimensionality of work engagement: a longitudinal investigation. Eur J Work Organ Psychol. 2019;28(2):239–258. doi:10.1080/1359432X.2019.1575364
38. Perko K, Kinnunen U, Tolvanen A, Feldt T. Investigating occupational well-being and leadership from a person-centred longitudinal approach: congruence of well-being and perceived leadership. Eur J Work Organ Psychol. 2016;25(1):105–119. doi:10.1080/1359432X.2015.1011136
39. Marsh HW, Lüdtke O, Trautwein U, Morin AJS. Classical latent profile analysis of academic self-concept dimensions: synergy of person- and variable-centered approaches to theoretical models of self-concept. Struct Equ Model Multidiscip J. 2009;16(2):191–225. doi:10.1080/10705510902751010
40. Woo SE, Hofmans J, Wille B, Tay L. Person-centered modeling: techniques for studying associations between people rather than variables. Annu Rev Organ Psychol Organ Behav. 2024;11(1):453–480. doi:10.1146/annurev-orgpsych-110721-045646
41. Ryan RM, Deci EL. Self-Determination Theory: Basic Psychological Needs in Motivation, Development, and Wellness. The Guilford Press; 2017:xii,756. doi:10.1521/978.14625/28806
42. De Beer LT, Hakanen JJ, Schaufeli WB, et al. The burnout-depression conundrum: investigating construct-relevant multidimensionality across four countries and four patient samples. Psychol Health. 2024:1–28. doi:10.1080/08870446.2024.2321358
43. Terluin B, van Hout HPJ, van Marwijk HWJ, et al. Reliability and validity of the assessment of depression in general practice: the short depression interview (SDI). Gen Hosp Psychiatry. 2002;24(6):396–405. doi:10.1016/S0163-8343(02)00211-6
44. Occelli P, Quenon JL, Kret M, et al. Validation of the French version of the hospital survey on patient safety culture questionnaire. Int J Qual Health Care. 2013;25(4):459–468. doi:10.1093/intqhc/mzt047
45. Ilies R, Morgeson FP, Nahrgang JD. Authentic leadership and eudaemonic well-being: understanding leader–follower outcomes. Leadersh Q. 2005;16(3):373–394. doi:10.1016/j.leaqua.2005.03.002
46. Joo BK, Jo SJ. The effects of perceived authentic leadership and core self-evaluations on organizational citizenship behavior: the role of psychological empowerment as a partial mediator. Leadersh Organ Dev J. 2017;38(3):463–481. doi:10.1108/LODJ-11-2015-0254
47. Alilyyani B, Kerr MS, Wong C, Wazqar DY. The influence of authentic leadership on nurses’ turnover intentions and satisfaction with quality of care in Saudi Arabia: a structural equation modelling study. J Nurs Manag. 2022;30(8):4262–4273. doi:10.1111/jonm.13895
48. Vallerand R. Vers une méthodologie de validation trans-culturelle de questionnaires psychologiques: implications pour la recherche en langue française. Can Psychol. 1989;30(4):662–680. doi:10.1037/h0079856
49. Gillet N, Fouquereau E, Huyghebaert T, Colombat P. Effets du soutien organisationnel perçu et des caractéristiques de l’emploi sur l’anxiété au travail et l’épuisement professionnel: le rôle médiateur de la satisfaction des besoins psychologiques. Psychol Fr. 2016;61(2):73–81. doi:10.1016/j.psfr.2014.05.004
50. Millsap RE. Statistical Approaches to Measurement Invariance. Routledge; 2012; doi:10.4324/9780203821961
51. Skrondal A, Laake P. Regression among factor scores. Psychometrika. 2001;66(4):563–575. doi:10.1007/BF02296196
52. Muthén LK, Muthén B. Mplus user’s guide. 2021.
53. Morin AJS, Litalien D. Mixture modeling for lifespan developmental research. 2019. Available from: https://corpus.ulaval.ca/jspui/handle/20.500.11794/34673.
54. Caesens G, Morin AJS, Gillet N, Stinglhamber F. Perceived Support Profiles in the Workplace: a Longitudinal Perspective. Group Organ Manag. 2021;10596011211044580. doi:10.1177/10596011211044581
55. Enders CK. Applied Missing Data Analysis, 2nd Ed. The Guilford Press; 2022:ix,546.
56. McLachlan G, Peel D. Finite Mixture Models. Wiley; 2000.
57. Morin AJS. Person-centered research strategies in commitment research. In: Handbook of Employee Commitment. Edward Elgar Publishing; 2016:490–508.
58. Lo Y, Mendell NR, Rubin DB. Testing the number of components in a normal mixture. Biometrika. 2001;88(3):767–778. doi:10.1093/biomet/88.3.767
59. Diallo TMO, Morin AJS, Lu H. Impact of misspecifications of the latent variance–covariance and residual matrices on the class enumeration accuracy of growth mixture models. Struct Equ Model Multidiscip J. 2016;23(4):507–531. doi:10.1080/10705511.2016.1169188
60. Diallo TMO, Morin AJS, Lu H. The impact of total and partial inclusion or exclusion of active and inactive time invariant covariates in growth mixture models. Psychol Methods. 2017;22(1):166–190. doi:10.1037/met0000084
61. Lubke G, Muthén BO. Performance of factor mixture models as a function of model size, covariate effects, and class-specific parameters. Struct Equ Model. 2007;14(1):26–47. doi:10.1207/s15328007sem1401_2
62. Morin AJS, Wang JCK. A gentle introduction to mixture modeling using physical fitness performance data. John Wiley & Sons; 2016. Available from: https://acuresearchbank.acu.edu.au/item/89944/a-gentle-introduction-to-mixture-modeling-using-physical-fitness-performance-data.
63. Morin AJS, Litalien D. Webnote: longitudinal tests of profile similarity and latent transition analyses. 2017.
64. Collins LM, Lanza ST. Latent Class and Latent Transition Analysis: With Applications in the Social, Behavioral, and Health Sciences. John Wiley and Sons Inc.; 2010; doi:10.1002/9780470567333
65. Asparouhov T, Muthén B. Auxiliary variables in mixture modeling: three-step approaches using Mplus. Struct Equ Model. 2014;21(3):329–341. doi:10.1080/10705511.2014.915181
66. Raykov T, Marcoulides GA. Using the delta method for approximate interval estimation of parameter functions in sem. Struct Equ Model Multidiscip J. 2004;11(4):621–637. doi:10.1207/s15328007sem1104_7
67. Alavi SB. The making of an authentic leader’s internalized moral perspective: the role of internalized ethical philosophies in the development of authentic leaders’ moral identity. J Bus Ethics. 2024;190(1):77–92. doi:10.1007/s10551-023-05442-9
68. Rego A, Cunha MP, Simpson AV. The perceived impact of leaders’ humility on team effectiveness: an empirical study. J Bus Ethics. 2018;148(1):205–218. doi:10.1007/s10551-015-3008-3
69. Harms PD, Wood D, Landay K, Lester PB, Vogelgesang Lester G. Autocratic leaders and authoritarian followers revisited: a review and agenda for the future. Leadersh Q. 2018;29(1):105–122. doi:10.1016/j.leaqua.2017.12.007
70. Huyghebaert T, Gillet N, Lahiani FJ, Dubois-Fleury A, Fouquereau E. Psychological safety climate as a human resource development target: effects on workers functioning through need satisfaction and thwarting. Adv Dev Hum Resour. 2018;20(2):169–181. doi:10.1177/1523422318756955
71. Bawden D, Robinson L. The dark side of information: overload, anxiety and other paradoxes and pathologies. J Inf Sci. 2009;35(2):180–191. doi:10.1177/0165551508095781
72. Cheong M, Spain SM, Yammarino FJ, Yun S. Two faces of empowering leadership: enabling and burdening. Leadersh Q. 2016;27(4):602–616. doi:10.1016/j.leaqua.2016.01.006
73. Cougot B, Gillet N, Moret L, et al. Relationship between empowering leadership and stress in a French university hospital: a cross-sectional study combining the measurement of perceived stress and salivary cortisol. J Nurs Manag. 2024;2024:e8839893. doi:10.1155/2024/8839893
74. Wong SI, Giessner SR. The thin line between empowering and laissez-faire leadership: an expectancy-match perspective. J Manage. 2018;44(2):757–783. doi:10.1177/0149206315574597
75. Dulebohn JH, Bommer WH, Liden RC, Brouer RL, Ferris GR. A meta-analysis of antecedents and consequences of leader-member exchange: integrating the past with an eye toward the future. J Manage. 2012;38(6):1715–1759. doi:10.1177/0149206311415280
76. Legood A, van der Werff L, Lee A, Den Hartog D. A meta-analysis of the role of trust in the leadership- performance relationship. Eur J Work Organ Psychol. 2021;30(1):1–22. doi:10.1080/1359432X.2020.1819241
77. Schumacher D, Schreurs B, De Cuyper N, Grosemans I. The ups and downs of felt job insecurity and job performance: the moderating role of informational justice. Work Stress. 2021;35(2):171–192. doi:10.1080/02678373.2020.1832607
78. Vogel RM, Mitchell MS. The motivational effects of diminished self-esteem for employees who experience abusive supervision. J Manage. 2017;43(7):2218–2251. doi:10.1177/0149206314566462
79. Harvey P, Stoner J, Hochwarter W, Kacmar C. Coping with abusive supervision: the neutralizing effects of ingratiation and positive affect on negative employee outcomes. Leadersh Q. 2007;18(3):264–280. doi:10.1016/j.leaqua.2007.03.008
80. Tepper BJ, Simon L, Park HM. Abusive supervision. Annu Rev Organ Psychol Organ Behav. 2017;4(1):123–152. doi:10.1146/annurev-orgpsych-041015-062539
81. Itzchakov G, Amar M, Van Harreveld F. Don’t let the facts ruin a good story: the effect of vivid reviews on attitude ambivalence and its coping mechanisms. J Exp Soc Psychol. 2020;88:103938. doi:10.1016/j.jesp.2019.103938
82. Lind EA, van den Bos K. When fairness works: toward a general theory of uncertainty management. Res Organ Behav. 2002;24:181–223. doi:10.1016/S0191-3085(02)24006-X
83. Tate K, Penconek T, Dias BM, Cummings GG, Bernardes A. Authentic leadership, organizational culture and the effects of hospital quality management practices on quality of care and patient satisfaction. J Adv Nurs. 2023;79(8):3102–3114. doi:10.1111/jan.15663
84. Lavoie-Tremblay M, Fernet C, Lavigne GL, Austin S. Transformational and abusive leadership practices: impacts on novice nurses, quality of care and intention to leave. J Adv Nurs. 2016;72(3):582–592. doi:10.1111/jan.12860
85. Berger R, Glazer S, Leiva D. Leaders condition the work experience: a test of a job resources-demands model invariance in two countries. J Nurs Manag. 2023;2023:1–11. doi:10.1155/2023/1353289
86. Kowalski MO, Basile C, Bersick E, Cole DA, McClure DE, Weaver SH. What do nurses need to practice effectively in the hospital environment? An integrative review with implications for nurse leaders. Worldviews Evid Based Nurs. 2020;17(1):60–70. doi:10.1111/wvn.12401
87. Huyghebaert‐Zouaghi T, Morin AJS, Ntoumanis N, Berjot S, Gillet N. Supervisors’ interpersonal styles: an integrative perspective and a measure based on self‐determination theory. Appl Psychol Int Rev. 2023;72(3):1097–1133. doi:10.1111/apps.12423
88. Gillet N, Morin AJS, Fernet C, Austin S, Huyghebaert-Zouaghi T. A longitudinal person-centered investigation of the multidimensional nature of employees’ perceptions of challenge and hindrance demands at work. Anxiety Stress Coping Int J. 2024;NoPaginationSpecified–NoPaginationSpecified. doi:10.1080/10615806.2024.2324252
89. Sandrin É, Gillet N, Fernet C, Depint-Rouault C, Leloup M, Portenard D. Effects of workaholism on volunteer firefighters’ performance: a moderated mediation model including supervisor recognition and emotional exhaustion. Anxiety Stress Coping Int J. 2019;32(5):568–580. doi:10.1080/10615806.2019.1638683
90. Drouin‐Rousseau S, Morin AJS, Fernet C, Blechman Y, Gillet N. Teachers’ profiles of work engagement and burnout over the course of a school year. Appl Psychol Int Rev. 2024;73(1):57–92. doi:10.1111/apps.12465
91. Huyghebaert-Zouaghi T, Berjot S, Gillet N. Benefits of psychological detachment from work in a digital era: how do job stressors and personal strategies interplay with individual vulnerabilities? Scand J Psychol. 2022;63(4):346–356. doi:10.1111/sjop.12810
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.