Back to Journals » International Journal of Nanomedicine » Volume 19
Natural Products-Based Inhaled Formulations for Treating Pulmonary Diseases
Authors Yong J, Shu H, Zhang X, Yang K, Luo G, Yu L, Li J, Huang H
Received 22 November 2023
Accepted for publication 1 February 2024
Published 23 February 2024 Volume 2024:19 Pages 1723—1748
DOI https://doi.org/10.2147/IJN.S451206
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yan Shen
Jiangyan Yong,1,* Hongli Shu,1,* Xiao Zhang,2,* Kun Yang,3 Guining Luo,3 Lu Yu,3 Jiaqi Li,3 Hong Huang4
1Department of Clinical Laboratory, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, 610072, People’s Republic of China; 2Department of Clinical Laboratory, Chengdu Children Special Hospital, Chengdu, Sichuan, 610031, People’s Republic of China; 3Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, 611137, People’s Republic of China; 4Department of Clinical Laboratory, the People’s Hospital of Chongqing Liang Jiang New Area, Chongqing, 401121, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hong Huang, Email [email protected]
Abstract: Given the unique physiological and pathological characteristics of the lung, the direct, inhalable route is more conducive to pulmonary drug delivery and disease control than traditional systemic drug delivery, significantly circumventing drug loss, off-target effects, systemic and organ toxicity, etc., and is widely regarded as the preferred regimen for pulmonary drug delivery. However, very few lung diseases are currently treated with the preferred inhaled formulations, such as asthma, chronic obstructive pulmonary disease and pulmonary hypertension. And there is a lack of appropriate inhaled formulations for other critical lung diseases, such as lung cancer and pulmonary fibrosis, due to the fact that the physicochemical properties of the drugs and their pharmacokinetic profiles do not match the physiology of the lung, and conventional inhalation devices are unable to deliver them to the specific parts of the lung. Phytochemicals of natural origin, due to their wide availability and clear safety profile, hold great promise for the preparation of inhalable formulations to improve the current dilemma in the treatment of lung diseases. In particular, the preparation of inhalable formulations based on nano- and microparticulate carriers for drug delivery to deep lung tissues, which overcome the shortcomings of conventional inhalation therapies while targeting the drug activity directly to a specific part of the lung, may be the best approach to change the current dilemma of lung disease treatment. In this review, we discuss recent advances in nano- and micron-carrier-based inhalation formulations for the delivery of natural products for the treatment of pulmonary diseases, which may represent an opportunity for practical clinical translation of natural products.
Keywords: inhaled nanoformulations, inhalation therapy, natural products, nanomedicine, pulmonary diseases
Introduction
Globally, pulmonary diseases, represented by acute respiratory infections, chronic obstructive pulmonary disease (COPD), bronchial asthma, and lung cancer, are characterized by high morbidity, mortality, disability, and treatment costs.1 With changing lifestyles, increasing environmental pollution, unavoidable occupational exposures, the continued prevalence of tobacco use, and an aging population, the morbidity, mortality and associated disease burden of pulmonary disease are increasing year by year. There is an urgent need to discover new therapeutic approaches applicable to the physiology, pathology and anatomy of the lung to transform the current global public health challenge of preventing and treating pulmonary disease.1,2
Conventional modes of drug delivery inevitably limit efficacy due to degradation of the active fraction in the gastrointestinal tract or first-pass metabolism in the liver, and this systemic mode of drug delivery increases non-specific toxicity due to high drug exposure to other organs.3 The lung is an excellent organ for drug absorption. Given its natural advantages, such as its large absorptive surface area (100–200 m2), abundant capillaries, very short transit distance, thin alveolar epithelial layer, and slow cell surface clearance, inhalation therapy is widely recognized as the preferred regimen for pulmonary drug delivery.4 Pulmonary delivery devices, such as dry powder inhalers (DPIs), pressurized metered dose inhalers (PMDIs), nebulizers, etc., are able to deliver medications locally to the lungs, dramatically improving the bioavailability of medications while fully exploiting their efficacy.5,6 Currently, inhaled formulations have become the first-line treatment for asthma and COPD, but there are no corresponding inhaled formulations for other lung diseases, including lung cancer and pulmonary fibrosis.
Phytochemicals of natural origin hold promise for inhaled formulations to improve the current dilemma of lung disease treatment due to their wide availability and clear safety profile.5 Given the low bioavailability of natural products and the inability of existing drug dosage forms to be delivered to the lungs in their natural form by inhalation, the use of appropriate drug delivery systems to create inhalable formulations that match the physiopathological characteristics of the lungs would be a potential solution for a wide range of lung diseases.7 Nano-/micron-sized carriers will undoubtedly be the best choice due to their smaller size and superior aerodynamic properties, enabling site-specific release for targeted drug delivery and higher retention and lower drug loss after delivery.8,9 In this review, we systematically summarize new ideas and approaches for the treatment of lung diseases, with a focus on lung cancer, using inhalation formulations of natural products delivered by nano-/microparticle carriers. Our goal is to draw more and more research attention to the potential and great value of natural products and inhalation therapies in the treatment of lung diseases, which promises to become a focus of translational new drug development and a new trend in clinical applications in the future.
Pharmacokinetic Process of Inhaled Formulations
The first process after inhalation is drug deposition, which can occur in the oropharynx, large airways or alveoli, and determines the site of drug action. Therefore, a key measure to improve the pulmonary bioavailability of inhaled formulations is to increase the pulmonary deposition rate, which depends on their aerodynamic equivalent diameter (Dae), inhalation flow rate, inhaler device characteristics and disease-related factors.10 Dae has a significant impact on respiratory deposition and subsequent drug absorption: particles with a Dae of 5–10 μm are retained in the upper respiratory tract; particles in the range of 1–5 μm have excellent pulmonary deposition and distribution properties and can be deposited in the secondary bronchioles (small airways and fine bronchioles); and particles in the range of 1–3 μm are suitable for deposition in the distal part of the fine bronchioles; smaller particles, about 1 μm, can accumulate in the alveoli; however, particles smaller than 0.5 μm are not deposited in the lungs and often diffuse into the bloodstream and are expelled via the respiratory airflow.11,12 After deposition in various parts of the lungs, the drug is either cleared, absorbed into the blood or lymphatic circulation, or metabolized.13,14 There are several clearance mechanisms depending on the site of drug deposition, including mechanical clearance, mucociliary clearance, macrophage degradation, and metabolic clearance. In the upper respiratory tract, mucociliary clearance is the primary mode of drug removal. This mechanism is more prevalent and faster for larger particles, which are usually completely cleared within 24 hours. In the lower respiratory tract, however, alveolar macrophage uptake plays a more dominant role in limiting the efficacy of inhaled preparations. Macrophages can also be targets for the delivery of certain inhaled drugs. For example, in the treatment of infectious diseases.14 Drug particles that successfully evade lung clearance mechanisms and dissolve in the epithelial lining fluid may subsequently be absorbed into lung tissue, with the rate of absorption depending on airway characteristics and drug properties.10 Drugs trapped in the lung tissue are metabolized by metabolic enzymes in the lung tissue after they have exerted their effect, and are released from the lung tissue into the blood circulation depending on the hyperperfusion of the lung.10
Therefore, given the pharmacokinetic characteristics of drugs in the lungs, inhalation formulations that match the anatomical and physiological characteristics of the lungs can achieve the desired therapeutic effect: the first aspect is to ensure that the inhaled formulation has excellent aerodynamic properties and is able to evade the lung clearance mechanism to reach the lung tissue; the second aspect to consider is the lung exposure time of the inhaled formulation; and then it is to ensure that the inhaled formulation is able to reach the target site to exert its effect and reduce the effect on the other sites, ie strike a balance between efficacy and safety.15 Considering the current state of medical care, drug delivery systems based on nanomaterials may be the optimal solution. Nanomaterials are characterized by their small size, large specific surface area, high surface reactivity and high adsorption capacity.16 Nanomaterials as drug carriers can improve drug pharmacokinetics and help drugs cross physiological and pathological barriers, thereby increasing bioavailability.17 Through active or passive targeting mechanisms, nanomaterials can increase the local concentration of drugs in lung tissue lesions, control drug release, prolong drug exposure time, and improve drug efficacy while reducing side effects.18 And through the delicate “camouflage” can reduce the body’s immune recognition and reticuloendothelial system clearance, nanomaterials can increase the retention time of the drug in vivo, prolong the half-life of the drug, and enhance the efficacy of the drug.19 Therefore, inhalable formulations based on nanomaterials are expected to have great potential in the treatment of lung diseases.
Determinant Characteristics of Inhaled Formulations
Inhaled drug delivery technology based on nano-/microcarriers skillfully combines aerosol technology and nanotechnology to prepare drugs into inhalation formulations that match the physiological and pathological characteristics of the lungs, and then deliver them directly to the site of action or absorption in the form of aerosols (eg powders, aerosols, inhalation mist droplets, etc.) with high speed and high efficiency.20 Therefore, considering the anatomical, physiological and pathological characteristics of the lung, the size, shape, surface properties and aerodynamic characteristics of nano-/micron-sized particle carriers determine the deposition and bioavailability of the drug in the lung.
Particle size is an important physical characteristic of inhaled formulations because it determines the properties of the aerosol as well as the site of particle action, and is classified as geometric diameter (physical diameter) and Dae (diameter of a spherical particle per unit density that settles in air at the same rate as a given particle).21 Nanomaterials can cross the mucosal barrier due to their small size, but the choice of specific size varies. In general, for pulmonary diseases such as asthma, COPD or pulmonary infections, carriers around 200–500 nm are appropriate, as they allow rapid delivery to deeper regions of the lung and thus to target cells such as alveolar macrophages for effective intracellular delivery. Sizes smaller than 200 nm or larger than 6 μm can avoid clearance by alveolar macrophages and are more suitable for non-obstructive lung diseases such as lung cancer.22
Particle morphology, ie the surface roughness and external shape of particles and the internal structure of porous particles, is another important factor affecting the performance of inhalation formulations. Large shape factor and low density reduce the Dae of particles, and in general, elongated particles have a larger shape factor, resulting in a smaller Dae than spherical particles of the same volume.21 Surface roughness or porous particles reduce interparticle cohesion, contact area and give the particles high dispersibility. In addition, the pollen-shaped particles exhibit better flowability, higher emitted dose, and higher fine particle fraction (FPF) than spherical, needle-like, plate-like, etc. particles due to their lower packing density as well as conical protrusions that increase the distance between particles, thereby minimizing interparticle forces and aggregation tendency.23
The surface properties of the particles are also a key determinant of the bioavailability of inhaled formulations. Nanoparticles with a high cationic surface charge have excellent stability and ability to penetrate the lung, but at the same time can cause toxic effects. Therefore, the toxicity of nanoparticles is generally avoided by using neutral or negative surface charges. Accordingly, materials such as chitosan can be used to surface modify nanoparticles to improve their ability to penetrate mucus and reduce lung clearance.24 Conversely, for infectious diseases such as tuberculosis or pneumonia, it is recommended that nanoparticles be modified with positively charged compounds to enhance macrophage uptake. In addition, particles can be modified with pulmonary surfactants, proteins or peptides to improve biocompatibility and efficiency of drug delivery to the lungs, particularly to target specific cells such as cancer cells.25,26
Natural Product Components in Inhaled Formulations
Pulmonary drug delivery has become a modality of administration that has received much attention, and a large number of clinical trials are attempting to convert existing orally or intravenously administered chemicals into inhaled formulations (Table 1). Although many diseases can be treated with the advantages of pulmonary drug delivery, currently only asthma and COPD can be treated with preferred inhaled formulations, such as inhaled glucocorticoids and bronchodilators. However, other critical lung diseases such as lung cancer, pulmonary fibrosis, tuberculosis and pneumoconiosis still lack appropriate inhaled formulations due to the fact that the physicochemical properties of conventional drug dosage forms and their pharmacokinetic profiles do not match the physiology of the lung and conventional inhalation devices are unable to deliver them to the specific parts of the lung. Therefore, there is a need to develop formulations specifically for inhalation, combining optimal inhaled drugs with well-designed inhalation devices to achieve efficient and safe lung-specific therapies.27 The use of nano- and microparticulate carriers to deliver drugs to their targets, especially in cancer, has gained unprecedented benefits over the past decades.20,28 Therefore, the development of inhaled formulations based on nano- and microparticulate carriers to deliver drugs to deep lung tissues, which overcome the shortcomings of traditional inhalation therapies while targeting drug activity directly to specific parts of the lung, may be the best way to change the current dilemma of lung disease treatment.29
 |
Table 1 Clinical Trials of Inhaled Chemical Formulations for Pulmonary Diseases |
Frustratingly, in today’s era of drug discovery, a large number of chemically synthesized molecules are approved and marketed by regulatory agencies that have good therapeutic value, but resistance, side effects, etc., remain unavoidable problems and are not always suitable for preparation into inhaled formulations. Unlike oral administration, inhaled formulations should have low oral bioavailability and high systemic clearance to maximize airway selectivity and minimize toxicity associated with systemic exposure after drug inhalation.36 Phytochemicals of natural origin may help to address these issues. Plants have been an important source for drug development and translational medicine since ancient times due to their abundance, high safety profile, and multiple mechanisms of action.37 However, the clinical applicability of phytochemicals is often hampered by their low bioavailability, which may be associated with their low solubility and/or susceptibility to degradation in aqueous media. For example, the bioavailability of quercetin in humans after oral administration was as low as 1%, which was attributed to poor aqueous solubility (2.84 mg/mL).38 In addition, the insoluble flavonoid silibinin is characterized by limited oral absorption (<50%), resulting in weak clinical efficacy.39 Therefore, the properties of natural products such as low oral bioavailability and high safety profile are the advantages for their preparation into inhaled formulations. Nano-delivery systems containing natural phytochemicals have no first-pass effect, rapid onset of action, high bioavailability, high local drug concentration at low dosage, enhanced pharmacological activity and higher safety margins (Figure 1). Consequently, pulmonary natural product delivery systems based on inhalable nano/micron carriers such as liposomes, nanoparticles, microparticles, nanocomposites, and nanoaggregates and (Figure 2) would be an attractive method of pulmonary drug delivery.
 |
Figure 1 Benefits of natural product-based inhaled nanoformulations in the treatment of pulmonary diseases. |
 |
Figure 2 Drug delivery nano/micron carriers for natural products. |
Inhaled Nanoformulations Based on Natural Products
Lipid-Based Inhaled Nanoformulations
Lipids are important components in living organisms, including fats, phospholipids, and sterols, of which phospholipids and sterols are the major components of biological membranes.40 Compared with other nanoformulations, it uses biocompatible lipid materials (eg, triglycerides and fatty acids) as carriers to dissolve or encapsulate the drug in the lipid core or adsorb it on the surface of the nanoparticles, including liposomes, solid lipid nanoparticles (SLNs), nanostructured lipid carriers (NLCs), etc., and it has good biocompatibility, complete biodegradability as well as low carrier toxicity and immunogenicity.41 Lipid-based nanomedicines are the forerunners in the clinical translation of nanomedicines, and most of the currently marketed nanomedicines are lipid-based nano-delivery systems represented by liposomes, which are widely used in the fields of cancer therapy, viral or fungal infections, analgesia, gene delivery, etc.42,43 Inhalable lipid nanoformulations based on natural products also show excellent potential in the treatment of pulmonary diseases (Table 2).
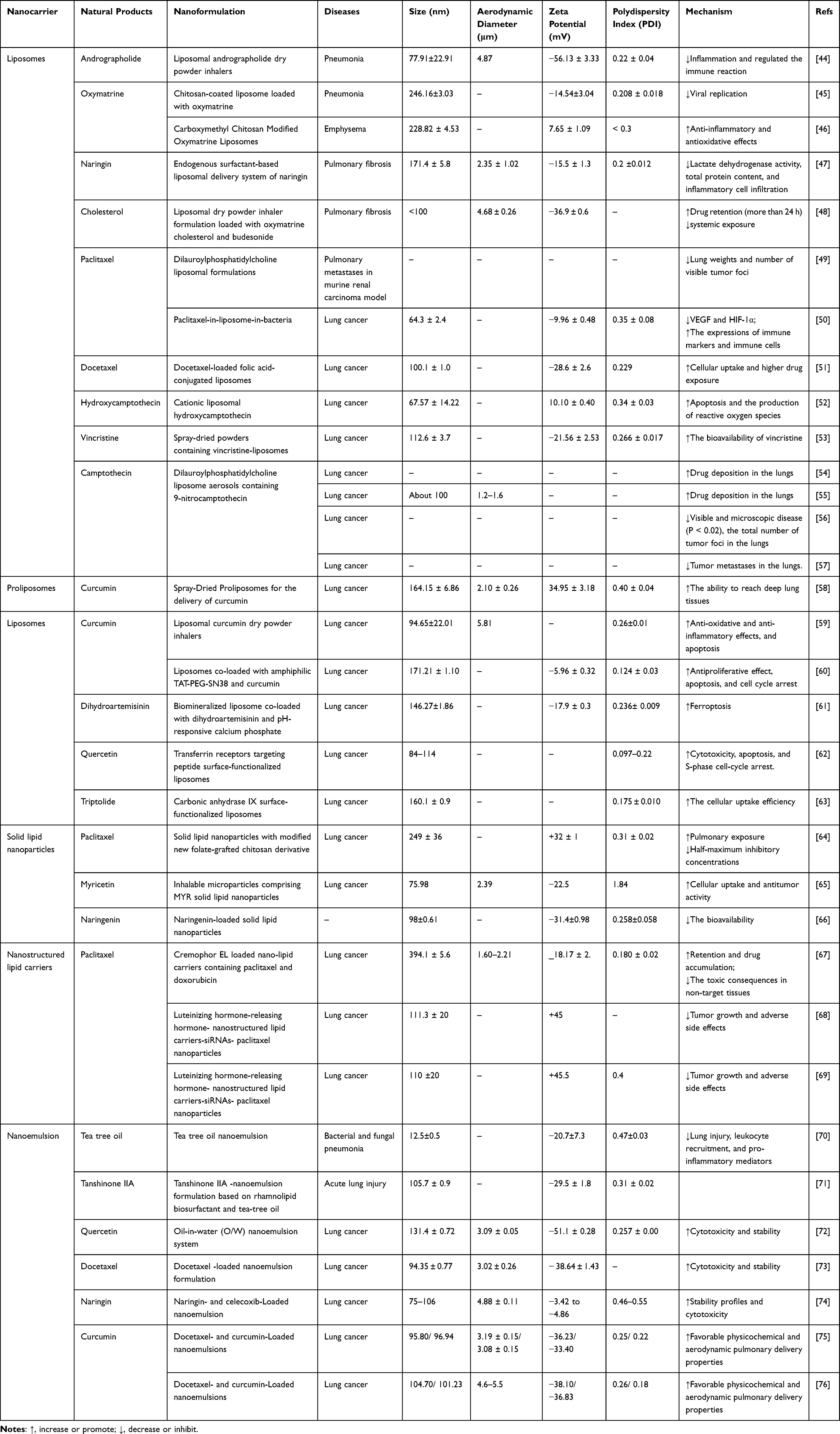 |
Table 2 Natural Products-Based Lipid Inhaled Nanoformulations for the Treatment of Pulmonary Diseases |
Liposomes
Liposomes are the earliest and most successful inhalable lipid nanocarriers, and liposomal formulations can be delivered to the lungs either by nebulizer atomization or as a dry powder via DPI.12 Liposomes are spherical vesicles (usually in the range of 20 nm to 20 μm) consisting of an aqueous core surrounded by one or more phospholipid bilayers of natural or synthetic origin, capable of encapsulating and carrying both hydrophilic (aqueous core) and lipophilic (lipophilic bilayers) drugs to achieve precise drug release at the site of the lesion.77 Enhanced pulmonary drug delivery through improved pharmacokinetics and pharmacodynamics, liposomes increase drug therapeutic index, improve patient compliance, reduce respiratory side effects and decrease drug toxicity.15 Liu78 et al demonstrated that liposomes promote rapid pulmonary distribution and cytoplasmic release of cyclic guanosine monophosphate-adenosine monophosphate, stimulate STING signaling and type I interferon production in pulmonary antigen-presenting cells, and induce systemic anticancer immunity and long-term inhibition of lung metastasis. A 2015 clinical study also found that cystic fibrosis patients who received a formulation of nebulized DNA plasmid-liposome complexes encoding the CFTR gene every 28 days for 12 months improved lung function with a 3.7% increase in forced expiratory volume in 1 s (0.07%-7.25%).79 In studies of inhaled formulations for the treatment of lung diseases, natural products have shown low side effects, stable anti-inflammatory and antifibrotic therapeutic effects, and no significant drug dependence due to their natural properties, making them promising therapeutic alternatives to inhaled therapies.5
Increasing respiratory infections and hard-to-beat pathogens (eg, multidrug-resistant strains) have become a challenge in clinical practice, and conventional antibiotic therapies are increasingly ineffective due to limitations in tissue penetration, toxicity, or drug resistance.77 In a mouse model of Staphylococcus aureus-induced pneumonia, DPI delivered andrographolide liposomes to the lungs, which inhibited lung inflammation, immune responses, and tissue damage by downregulating the NF-κB pathway and the release of pro-inflammatory cytokines such as TNF-α and IL-1. Moreover, andrographolide liposomes delivered to the lungs showed stronger antibacterial effects against pneumonia compared to tenfold doses of andrographolide or penicillin.44 Similarly, oxymatrine (OMT) derived from Sophora flavescens Ait has excellent anti-inflammatory, antioxidant, and antiviral activity. However, OMT is a hydrophilic natural phytochemical that tends to diffuse in the mucus layer and penetrate the air-blood barrier to rapidly enter the circulation, limiting its efficacy.45,46 Chitosan, which is highly biocompatible and biodegradable, and its encapsulated liposomes deliver OMT directly to the lungs, enhancing its distribution and retention in lung tissue without mucus restriction, thereby inhibiting the biosynthesis and penetration of human respiratory syncytial virus to exert its antiviral effects.45 Moreover, liposomes further enhanced the anti-inflammatory and antioxidant effects of OMT by down-regulating inflammatory cytokines and modulating the rebalancing antioxidant/oxidant Nrf2/HO-1 and NF-κB/IκB-α signaling pathways, which alleviated alveolar dilatation and destruction in emphysema model mice.46
Pulmonary fibrosis (PF) is a common, progressive, irreversible, and fatal chronic lung disease characterized by excessive structural remodeling of lung tissue due to myofibroblast proliferation and extracellular matrix deposition that impairs alveolar elasticity and lung function, ultimately leading to severe functional failure and even death.80 Kotta et al47 designed a liposomal naringin based on endogenous surfactant (phosphatidylcholine) to deliver naringin as an aerosol to the deep alveoli to attenuate inflammatory cell infiltration, oxidative stress, and collagen deposition to reduce alveolar surface tension thereby maintaining airway patency. In addition, the combination regimen may have a better antifibrotic effect. Co-loading of inhaled corticosteroid (budesonide) and antifibrotic natural product (colchicine) in liposomes and delivery to deep lung tissues as a dry powder using DPI, which can achieve site-specific delivery, reduce systemic exposure and prolong drug residence time in the lung (more than 24 hours), thus synergistically improving fibrotic lesions.48
Although conventional therapies have shown clear benefits in the treatment of cancer, a number of factors, including chemotherapy-induced toxicity and adverse effects, lack of target specificity, and most importantly, drug resistance during cancer progression, limit the clinical efficacy in lung cancer.81 Pulmonary delivery of natural products based on inhalable nanoformulations reduces drug dosage, decreases systemic toxicity and increases the actual local concentration of the drug in the lungs, ultimately resulting in better anti-tumor efficacy. Currently, marketed plant-derived chemotherapeutic agents such as paclitaxel,49,50 docetaxel,51 camptothecin,52,54–56 and vincristine53 have been prepared in their inhalable liposome nanoformulations for deep drug delivery and pulmonary therapy.
Paclitaxel is the most successfully developed plant-based chemotherapeutic agent, but its high lipophilicity limits its solubility in aqueous media, which in turn affects the efficacy of oral and intravenous administration. Liposomes can overcome this challenge by improving pharmacological properties and reducing toxicity.82 Paclitaxel was encapsulated in a liposomal formulation of dilauroylphosphatidylcholine, and pharmacokinetic studies showed that the area under the curve for inhalation administration was 26 times greater than that for intravenous tail vein administration. In an established mouse model of lung metastasis from renal cell carcinoma, inhalation of a liposomal formulation of paclitaxel via a nebulizer significantly reduced lung weight and the number of tumor foci in mice, while also demonstrating improved long-term survival.49 Interestingly, Zhang et al50 used live carrier bacteria for targeted delivery of paclitaxel. Liposomal paclitaxel was efficiently internalized into bacteria (Escherichia coli or Lactobacillus casei) by electroporation without affecting the growth of these bacteria. After intratracheal administration, the distribution of drug-carrying bacteria was much higher in the lung than in other organs, resulting in faster delivery of the carrier to lung cancer cells, which in turn downregulated vascular endothelial growth factor and HIF-1α and induced apoptosis. In addition, drug-carrying bacteria significantly increased the expression of immune markers (TNF-α, IL-4, and IFN-γ) and immune cells (leukocytes and neutrophils), resulting in superior anticancer activity.50
It has been found that aerosolized inhalation can disrupt the structure of liposomes and affect the final efficacy, which can be modified by preparing them as stable dry powder formulations by spray-drying, spray-freeze-drying and freeze-drying.12 Docetaxel is a natural antitumor compound similar in structure and efficacy to paclitaxel. Zhu et al51 first prepared folic acid-conjugated liposomes loaded with docetaxel, followed immediately by an inhalable dry powder using spray drying technique, which showed higher cellular uptake, cytotoxicity, tumor targeting properties and drug exposure accompanied by low drug exposure in other organs. Similarly, the use of spray-drying technology to produce liposomes of vincristine that can be administered via DPI to increase its exposure in the lungs and reduce clearance time imparts better anti-tumor properties to vincristine.53
Since camptothecins are alkaloids with excellent anticancer activity, and the potent anticancer agents irinotecan and topotecan are derivatives of these alkaloids, the continued development of comedones and their derivatives holds the promise of continued superior efficacy.83 9-Nitrocamptothecin (9-NC, a derivative of camptothecin) is a water-insoluble anticancer drug. After 30 min of inhalation of 9-NC liposomal aerosol, a large amount of the drug accumulated in the lungs (310 ng/g), while relatively little accumulated in other organs.54 Inhaled 9-NC liposome aerosol reduces lung weight, number of tumor foci and size of individual tumor nodules in mouse models of melanoma and osteosarcoma lung metastases.55,56 In contrast, oral 9-NC liposome had no detectable effect on cancer growth, suggesting that its therapeutic benefit is due to lung deposition.55 Mutations in the P53 oncogene have been found in most lung cancers, leading to increased drug resistance and tumor recurrence. Transfer of the P53 gene into tumor cells to induce apoptosis and increase cellular sensitivity to chemotherapeutic agents may be a potential solution. Aerosol pulmonary delivery of polyethyleneamine-p53-DNA (PEI-p53) complexes can achieve high levels of p53 gene expression to inhibit the growth of lung metastases.84,85 More importantly, the sequential aerosol delivery of PEI-p53 and 9-NC liposome showed significant synergistic efficacy in inhibiting the growth of established melanoma metastases in the lung, reducing the dose of drugs used and increasing the average survival time of the mice by 30–40%.57 This combination regimen also includes sonodynamic therapy. Xiao et al52 combined pulmonary delivery of cationic liposomal hydroxycamptothecin-based chemotherapy and 5-aminolevulinic acid-based sonodynamic therapy, again showing significant synergistic efficacy. This combined regimen showed enhanced cytotoxicity by inducing apoptosis and increasing reactive oxygen species (ROS) production in cancer cells, suggesting that inhaled therapies may be suitable for the development of combination regimens for lung cancer.
Curcumin is a naturally occurring polyphenol extracted from the rhizome of Curcuma longa, which limits its conversion into an anticancer agent due to its low hydrophilicity, poor bioavailability and rapid clearance from the body.86 Liposomal curcumin nanoformulations exhibit excellent atomization properties that promote the delivery of curcumin to deep lung tissues, increase the rate and extent of lung tissue uptake, and prolong exposure time in lung tissues.58 After freeze-drying, curcumin liposome dry powder was prepared, which was suitable for lung inhalation and selective targeting of lung cancer cells, and showed superior anticancer activity to gemcitabine and curcumin powders due to its high lung deposition with an average FPF of 46.71 and Dae of 5.81 μm.59 In addition, liposomes co-loaded with curcumin and 7-ethyl-10-hydroxyl camptothecin precursors showed enhanced anti-proliferative, pro-apoptotic and cell cycle inhibitory effects to synergistically inhibit lung cancer growth compared to the single agent.60
Ferroptosis therapy has been proposed as a promising strategy for lung cancer treatment by promoting intracellular ROS production and lipid peroxidation accumulation (LPO).87 However, insufficient intracellular ROS levels and suboptimal drug accumulation in cancer tissues hamper the effectiveness of iron death therapy, and the respirable biomineralized liposomes constructed by Fu et al helped to improve the situation through intracellular ROS and LPO accumulation-driven cell swelling and cell membrane disruption.61 The natural product dihydroartemisinin (DHA) was doped into the liposome core, while pH-responsive calcium phosphate (CaP) was coated on the liposome surface as a shell. Upon aerosolized delivery to lung tumors, the CaP shell disintegrates and releases a certain amount of Ca2+ into the cell, triggering an initial Ca2+ burst. Meanwhile, the intense endoplasmic reticulum stress induced by Ca2+, aided by DHA-mediated ROS generation and sarco-/endoplasmic reticulum calcium ATPase inhibition, can further promote LPO generation and ferroptosis, which in turn accelerates tumor elimination both in vitro and in vivo.61
To enhance antitumor drug-specific delivery and avoid off-target effects, active targeting is an effective strategy.88 T7 peptide is a cell-targeting peptide with specific binding affinity for the transferrin receptor (TFR), and targeting of the TFR, which is overexpressed and confined to tumor cells, may increase the therapeutic efficacy in lung cancer.89 The T7 surface is functionalized with loaded quercetin liposomes that are actively targeted for delivery to lung cancer cells, which in turn release quercetin to induce apoptosis, S-phase cell cycle arrest and growth inhibition of tumor tissue. Its accumulation and sustained release behavior in the lung lasted up to 96 hours without systemic toxicity.62 Similarly, Lin et al63 used carbonic anhydrase IX, an enzyme expressed on the surface of lung cancer cells, to surface-modify liposomes loaded with tretinoin lactone to specifically target and kill lung cancer cells.
Solid Lipid Nanoparticles (SLN)
SLN are colloidal dispersions of non-polar lipids (eg, triglycerides and fatty acids) composed of excipients that are “generally recognized as safe”. SLN are solid at both room and body temperatures, which reduces the mobility of the delivered drug in the lipid matrix and improves its stability and sustained release efficiency. In contrast, SLN have a greater affinity for lipophilic drugs.90 Rosière et al64 developed inhalable SLN highly loaded with paclitaxel and modified with folic acid and chitosan to improve surface properties. Lung exposure to paclitaxel was prolonged up to 6 h after inhalation administration with limited systemic distribution. In addition, folic acid-modified SLN enhanced the selectivity of SLN for lung cancer cells by actively targeting the folate receptor on the surface of lung cancer cells, which in turn penetrated and distributed throughout the lung tumors independently of the vasculature.64 This vascular low-dependence therapeutic regimen will have positive implications for poorly vascularized solid tumors such as lung cancer.
Attributed to its limited water solubility (2 mg / mL), the bioavailability of myricetin is poor, which restricts its further drug development and clinical application.91 Based on phospholipid complexes, SLN encapsulating myricetin were prepared, which could ensure the high stability of myricetin and at the same time endow myricetin with faster drug release and uptake as well as more significant antitumor activity against lung cancer cells. After spray drying, the aerodynamic particles were produced with an mass median aerodynamic diameter (MMAD) of 2.77 μm, indicating that they could be deposited in the target bronchial area for targeted treatment of lung cancer.65 Similarly, Peng et al66 successfully incorporated the poorly water-soluble drug naringenin into SLN for pulmonary delivery using emulsification and low-temperature hardening methods, significantly improving the bioavailability of naringenin by 2.53 times that of naringenin suspension.
Nanostructured Lipid Carrier (NLC)
NLC is a new type of nano-drug delivery system developed and formed on the basis of SLN. Through the introduction of liquid lipid carrier, compared with SLN, it has higher encapsulation rate, drug loading capacity and stability, which can effectively increase the solubility of drug, prolong the action time of drug in vivo, improve the bioavailability and reduce the adverse drug reactions.92 Inhalation of surfactant Cremophor EL-based NLCs enhances cellular uptake and drug accumulation of paclitaxel and doxorubicin in lung cancer cells, improving drug resistance while reducing toxicity to non-target tissues.67 Moreover, the use of NLC as a multifunctional nanomedicine platform can enable multiple mechanisms of lung cancer treatment.68,69 Garbuzenko et al68 fabricated a multifunctional delivery NLC co-loaded with paclitaxel and small interfering RNAs (siRNAs). The NLC enhances drug stability, solubility, and cellular penetration. The inhalation delivery technique delivers the drug to the lungs to promote passive targeting and uses luteinizing hormone-releasing hormone (LHRH) modification, a molecule specific for targeting receptors overexpressed in the plasma membrane of lung cancer cells, to actively target lung cancer cells. The system delivers paclitaxel to induce cancer cell death and a series of siRNAs to inhibit all four types of epidermal growth factor receptors - tyrosine kinases. In addition, the formulation exhibits desirable organ accumulation, superior anticancer activity and significantly fewer side effects than single agents or siRNA or non-targeted delivery.68 Similarly, Taratula et al69 developed multifunctional NLC for pulmonary co-delivery of chemotherapeutics and siRNAs. LHRH-modified NLC to actively target lung cancer cells, release anticancer drugs (paclitaxel/doxorubicin) after inhalation of the NLC to induce cancer cell death, and release siRNAs targeting MRP1 and BCL2 mRNAs to ameliorate resistance to the drugs, thus effectively inhibiting tumor growth and preventing adverse side effects on healthy organs.
Nanoemulsions (NEs)
Nanoemulsions(NEs) are biphasic dispersions of two immiscible liquids: water-in-oil (W/O) or oil-in-water (O/W) droplets stabilized by amphiphilic surfactants, with long-term kinetic and thermodynamic stability.93 NEs have been recognized by the US FDA as safe drug carriers capable of dissolving large quantities of hydrophobic drugs within their lipophilic cores and reducing enzymatic degradation and hydrolysis of the loaded drugs to achieve sustained drug release.94 In addition, its small size, typically averaging 20–200 nm in diameter, allows it to cross cellular barriers by diffusion, thus maintaining retention and deposition in lung tissue for extended periods of time, and has great potential in the treatment of lung diseases.12
Tea tree oil (TTO), a natural essential oil, has potent antimicrobial activity and is almost unlikely to develop antimicrobial resistance. However, allergic reactions, instability, and hydrophobicity limit its clinical application.95 Li et al prepared an inhalable TTO nanoemulsion (nanoTTO) consisting of TTO/Cremophor EL/water with an average size of 12.5 nm. In vitro, the nanoTTO was able to significantly inhibit Escherichia coli, Acinetobacter baumannii, Klebsiella pneumoniae, Staphylococcus aureus, and Candida albicans. In a rat model of fungal pneumonia, inhaled nanoTTO directly reaches microbially infected lung tissue, exhibits superior antifungal activity to fluconazole, and inhibits leukocyte recruitment and pro-inflammatory mediators to attenuate lung injury. In a rat model of bacterial pneumonia, the efficacy of nanoTTO, although slightly lower than that of penicillin, was achieved at a much lower dose and without significant adverse effects.70 Due to the current prevalence of microbial bacterial resistance, inhaled nanoTTO are expected to be the alternative nanomedicine of choice for the treatment of bacterial and fungal pneumonia. Degradation and shedding of the glycocalyx, the gel-like layer that lines the surface of the lumen of the vascular endothelium, has been implicated as an important mechanism in the pathogenesis of acute lung injury.96 El-Moslemany et al71 prepared a tanshinone IIA-loaded NEs formulation (TSIIA-NE) using ultrasound technology based on bioactive natural ingredients, rhamnolipid biosurfactant and TTO (as the oily phase). TSIIA-NE ameliorated LPS-induced pulmonary ventilatory dysfunction and pathological changes through antioxidant (up-regulation of superoxide dismutase, glutathione peroxidase, down-regulation of malondialdehyde), anti-inflammatory (up-regulation of IL-10, down-regulation of TNF-α and IL-17) and inhibition of glycocalyx degradation, as evidenced by a 1.4-fold and 1.9-fold increase in tidal volume and minute respiratory volume, respectively, a 32% decrease in the wet/dry lung weight ratio, and an improvement in arterial blood gas levels.71 Similarly, Arbain et al72 prepared an O/W NE formulation loaded with quercetin using palm oil ester/ricinoleic acid as the oil phase. The formulation had an acceptable MMAD (3.09 ± 0.05 μm), high FPF (90.52 ± 0.10%), and percent inhaled (81.26 ± 1.28%), which met the physicochemical and nebulization characteristics required for deep lung delivery applications. In addition, NEs impart high stability to natural products and can continuously deliver quercetin and docetaxel to act on lung cancer tissue even under extreme environmental conditions, making them promising inhalable agents for the treatment of lung cancer.72,73 In addition to demonstrating significant safety and bioaccumulation in lung tissue, NEs delivering naringin also accumulate in the brain, liver and bone, the major organs for lung cancer metastasis.74 Moreover, natural products, due to their excellent anticancer activity and potential as chemotherapeutic sensitizers, make their combination with chemotherapeutic agents a potential combination for lung cancer treatment.97 The synergistic effect of NEs-based formulations co-loaded with curcumin and docetaxel, which have good physicochemical and aerodynamic pulmonary delivery properties that can reduce docetaxel toxicity and improve bioavailability, will undoubtedly play an important role in the treatment of lung cancer.75,76
Polymeric Nanoparticles
Polymers are mainly classified as natural polymers (eg, chitosan nanoparticles) or synthetic polymers (eg, poly(lactic-co-glycolic acid, PLGA), which have good properties such as good biodegradability, biocompatibility, and controllable drug release profile. Drugs can be encapsulated within the polymer or coupled to the surface of the polymer, and further modification of the ligand on the surface allows for targeted delivery of the drug.29,98 In nanoformulations for inhalation drug delivery, polymeric nanoparticles help prevent the drug from being cleared by lung macrophages and ciliary mucus mechanisms, and are able to remain in the lungs longer to exert their effects (Table 3).
 |
Table 3 Natural Products-Based Inhaled Polymeric Nanoparticle Formulations for the Treatment of Pulmonary Diseases |
Antibiotic resistance is one of the most serious medical problems today, and urgent clinical needs require the timely discovery of alternative therapies for bacterial infections. Curcumin, a natural bacterial inhibitor, was prepared into pure curcumin nanoparticles by evaporative precipitation of nanosuspensions, solid dispersions and antisolvent precipitation, which in turn kills bacteria deep in the alveoli via inhaler without using any support or nano-carrier.8 PLGA nanoparticles co-loaded with antibiotics (tobramycin, ciprofloxacin or azithromycin), N-acetylcysteine and curcumin, resulting in a combination of antimicrobial, mucolytic and anti-inflammatory properties to improve antibiotic resistance for effective control of pulmonary infections.99 Moreover, as a naturally occurring photosensitizer, curcumin-based antimicrobial photodynamic therapy offers new options for improving drug-resistant bacterial pneumonia.109 Curcumin-loaded inhalable PLGA nanoparticles adhered tightly to the bacterial cell wall and stimulated antimicrobial phototoxicity under an applied low-energy light source, disrupted bacterial morphology and ultrastructure, and significantly inhibited the growth of Staphylococcus saprophyticus subsp. bovis (Gram-positive bacteria) and Escherichia coli DH5 alpha (Gram-positive bacteria).100,101
Silicosis, caused by excessive inhalation of dust containing crystalline silica, is a life-threatening disease of pulmonary fibrosis for which there is a lack of effective treatment.110 The natural product quercetin may be an effective strategy against fibrosis due to its antioxidant and anti-inflammatory activities. Quercetin encapsulated in chitosan-assisted manufactured nanoparticles (Qu/CS-NPs) facilitated the enhancement of quercetin’s antifibrotic activity by virtue of its excellent encapsulation ability, excellent hydrophilic stability, and outstanding controlled and slow release capabilities. Inhaled Qu/CS-NPs ameliorated silica-induced silicosis-associated fibrosis by reducing ROS and malondialdehyde production to attenuate oxidative stress, inhibiting IL-1β and TNF-α release to alleviate inflammation, and downregulating α-smooth muscle actin levels and inhibiting extracellular matrix deposition to improve lung histology.102 Given the negligible toxicity, inhalation of nanomodified natural products may be a viable therapeutic option for the treatment of silicosis.
Resveratrol, a natural polyphenol found in fruits, has excellent anticancer activity and low toxicity; however, its low water solubility and instability limit its clinical use.111 The loading of sulfobutylether-β-cyclodextrin onto PLGA polymers (CD-RES NPs) perfectly ameliorates the above-mentioned deficiencies of resveratrol, with a 66-fold increase in its water solubility. Moreover, the excellent aerodynamic properties of CD-RES NPs after inhalation endowed resveratrol with enhanced anticancer efficacy as evidenced by significantly increased cellular uptake, cytotoxicity, antioxidant and pro-apoptotic activities.103 Notably, tumor cells typically possess higher levels of ROS and glutathione (GSH) compared with normal cells, resulting in greater redox potentials.112 Based on this, Tian et al104 designed ROS/GSH-responsive paclitaxel dimer nanoparticles, which were able to rapidly decompose in the ROS- and GSH-rich tumor microenvironment thereby increasing local paclitaxel exposure and accumulation, exhibiting enhanced anticancer potential and reduced systemic toxicity. Metastasis is also a major threat to the treatment and prognosis of lung cancer. Hu et al105 designed Cholesterol-PEG Co-Modified Poly (n-Butyl) Cyanoacrylate Nanoparticles for sustained pulmonary delivery of docetaxel. The PEG modification could avoid docetaxel clearance by macrophages and prolong the lung uptake time. Cholesterol modification, on the other hand, promotes docetaxel diffusion across the blood-brain barrier and into the brain in a sustained release fashion, making it a promising and effective vehicle for the treatment of lung cancer brain metastases.105 In addition, bone and liver are common metastatic sites of lung cancer. Inhalation of naringin-encapsulated PLGA nanoparticles can not only accumulate in lung tissue, but also exist in large quantities in bone, liver, and brain, which will undoubtedly be an effective therapeutic strategy to control lung cancer metastasis.106
Inhaled nanoparticles deliver chemotherapy drugs deeper into the lungs than traditional intravenous drug delivery due to their smaller size and more localized drug delivery, which could significantly improve the efficacy of drugs such as paclitaxel.107 However, inhaled nanomedicines inevitably interact with surface-active substances in the lung, forming a “surfactant corona” that affects drug adhesion/penetration. Paclitaxel-loaded PLGA nanoparticles were modified with biomimetic endogenous lung surfactant phospholipids, such as phosphatidyl dipalmitoyl phosphatidylcholine. The different phospholipids conferred adhesion, mucus permeability and cellular uptake properties to the nanoparticles, respectively, and modulated their retention in bronchoalveolar lavage fluid, uptake by alveolar macrophages and uptake by lung tissues, providing a scientific rationale for improving the intrapulmonary distribution of inhaled formulations.108
Other Nanocarriers
Nanomicelles are thermodynamically stable systems composed of amphiphilic polymers with small particle size, strong adsorption capacity, good biocompatibility and targeting. The hydrophobic core can load insoluble drugs, which is an effective way to improve the oral absorption of insoluble drugs, while the hydrophilic shell can prevent the micelles from being recognized by the reticuloendothelial system, thus prolonging the circulation time of drugs in the body.113,114 Micelle-based delivery systems can be prepared that are both tissue-targeted and biologically active, delivering natural products to the deep lung for enhanced pharmacological activity.114,115 Mahajan et al116 prepared curcumin-loaded polymeric micelles based on l-lactide grafted xyloglucan and then used freeze-drying technique to prepare DPI formulations for pulmonary delivery of curcumin. The local concentration of curcumin was higher in deep lung tissues and was maintained at the effective drug concentration for a longer period of time. Matrix metalloproteinases (MMPs), specific markers of malignancy, are involved in malignant behaviors such as angiogenesis, invasion and metastasis in lung cancer.117 MMP2/9-triggered release micelles were developed for pulmonary delivery of paclitaxel. Upon nebulized inhalation, paclitaxel was released in a concentration-dependent MMP2/9-triggered release at the tumor site and was rapidly taken up by cancer cells to enhance anticancer activity and reduce toxicity to healthy lung cells.118
Nanogels are non-toxic and biocompatible porous carriers with large surface area and drug loading capacity, making them particularly suitable for clinical topical applications.119 For example, cholesteryl group-modified pullulan self-assembled polysaccharide nanogels for cancer vaccine delivery and enhancement of immune response against tumor cells.120 Chen et al121 designed an inhalable nanogel with a “material-drug” structure to improve the low solubility and bioavailability deficiencies of quercetin, a natural flavonoid with excellent antioxidant and anti-inflammatory properties. In this nanoformulation, quercetin and alginate are cross-linked by Ca2+ and stabilized by intermolecular hydrogen bonding, resulting in a “co-construct” water-soluble nanogel (QU-nanogel). In a rat model of acute lung injury, inhaled QU-nanogel provided targeted delivery of quercetin to the lung, attenuated lung inflammation and oxidative damage, and prevented subsequent lung fibrosis as evidenced by down-regulation of inflammatory cytokines (TNF-α, IL-6, and IL-1β) and up-regulation of antioxidant enzymes (SOD, catalase, and heme oxygenase-1).121
Exosomes, which are small lipid bilayer nanoparticles derived from many cell types, can deliver drugs to specific cell types or tissues for targeted drug delivery due to their stable structure and unique permeability.122 Zheng et al123 encapsulated paclitaxel using T cell-derived exosomes expressing chimeric antigen receptors (PTX@CAR-Exos). In a mouse model of orthotopic lung cancer, inhaled PTX@CAR-Exos accumulated in the tumor region by targeting the mesothelin-expressing Lewis lung cancer through the anti-mesothelin single-chain variable fragment of CAR-Exos, thereby reducing tumor volume and prolonging survival of the mice. In addition, PTX@CAR-Exos reprogrammed the tumor microenvironment and reversed the immunosuppression, as evidenced by CD8 T-cell infiltration and increased levels of IFN-γ and TNF-α.123
Nanocochleates, a new type of nanocarrier with a helical structure composed of soluble lipid molecules, have been prepared as oral formulations to improve the bioavailability of chemotherapeutic drugs such as paclitaxel.124 The surface activity of nanocochleates was found to be similar to that of endogenous lung surfactant, which is expected to be used as both a drug delivery vehicle and lung surfactant for lung diseases. Paclitaxel-loaded nanocochleates (PTX-CPTs) exhibited excellent lung surface activity and terminal airway patency. Inhaled PTX-CPTs were readily deposited in the deep alveoli, which in turn enhanced cellular uptake-mediated cytotoxicity via energy-dependent endocytosis. In a mouse model of melanoma lung metastasis, PTX-CPTs significantly inhibited the numbers of tumor nodules and percent metastasis area covered by melanoma cells in the lung, and reduced respiratory complications and side effects of chemotherapeutic agents.125
In addition, albumin nanoparticles,126,127 nano transfersome,128 and nanocapsules129 have been prepared to deliver natural compounds to the lungs as inhalable nanoformulations. Moreover, the preparation of natural phytochemicals into nanocrystals for pulmonary delivery using methods such as milling can also improve the bioavailability of natural phytochemicals130,131 (Table 4).
 |
Table 4 Natural Products-Based Other Inhaled Nanocarriers for the Treatment of Pulmonary Diseases |
Microparticles
Microparticles have excellent aerodynamic properties with an average size of about 5 μm, and spray drying produces inhalable formulations that effectively evade phagocytosis by alveolar macrophages and penetrate deep into the lungs.132,133 Using materials such as PLGA, alginate, chitosan and lipids, they can be easily atomized as dry powder formulations for sustained drug release in the lungs (Table 5).
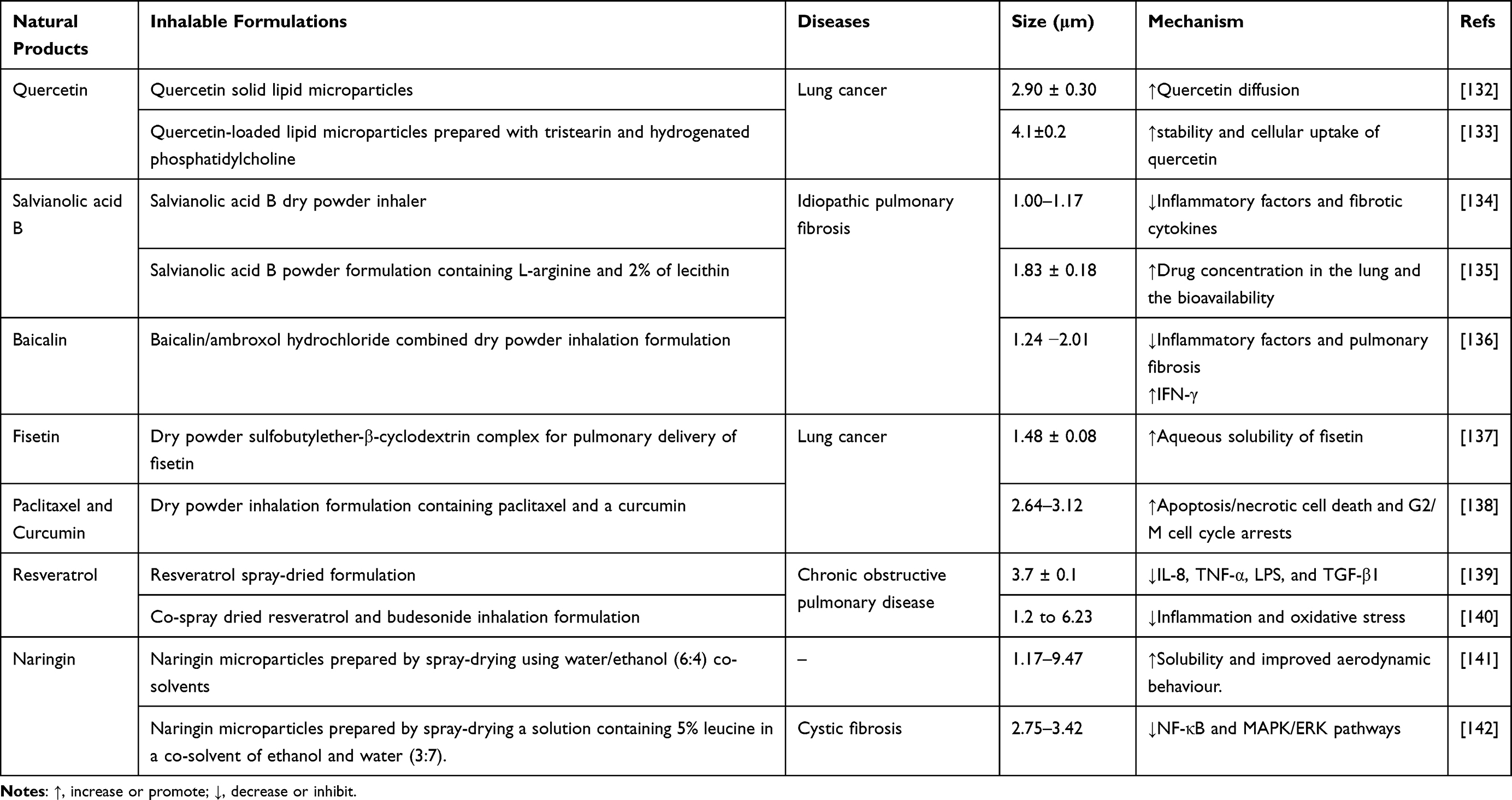 |
Table 5 Natural Products-Based Inhaled Microparticles for the Treatment of Pulmonary Diseases |
Salvianolic acid B (Sal B), a water-soluble component of Salvia miltiorrhiza Bunge, prevents or delays the onset and progression of idiopathic pulmonary fibrosis by modulating inflammatory cytokines and fibrosis-related cytokines. Its preparation as an inhalable dry powder formulation may overcome the limitations of oral and intravenous administration.134,135 Sal B-DPI was prepared by spray-drying using L-leucine as an excipient for targeted delivery to the deep lung as a dry powder.134 Similarly, Jiang et al135 prepared new Sal B powder formulations containing L-arginine and lecithin using ball milling technique. L-arginine was used to modulate the strong acidity of Sal B solution, and lecithin could improve the flowability and biocompatibility due to its similarity in composition to lung surfactants. These two dry powder formulations have good powder properties, low irritation, effective pulmonary delivery, high bioavailability and pulmonary drug concentration. By attenuating oxidative damage and modulating inflammatory factors and fibrotic cytokines (eg, I/III Collagen type α1, intercellular adhesive molecule-1, fibronectin, inducible nitric oxide synthase, and arginase type 1) during disease progression, Sal B-DPI significantly alleviated bleomycin-induced pulmonary fibrosis as evidenced by the reduction of alveolar wall congestion, inflammatory cell infiltration, emphysema extent, and lung ventilatory function.134,135 Moreover, the DPI co-loaded with baicalein/ambroxol hydrochloride demonstrated antifibrotic, anti-inflammatory, and antioxidant effects of pirfenidone due to its pulmonary targeting, rapid onset of action and high pulmonary bioavailability.136 These inhaled formulations will undoubtedly help to address the current dilemma of the extreme shortage of drugs for the treatment of pulmonary fibrosis.
Complexation of the natural flavonoid fisetin with sulfobutylether-β-cyclodextrin increased the solubility of fisetin while maintaining its antioxidant activity. Subsequently, it was fabricated into a low-density inhalable powder using a spray-drying method for delivery to deep lung tissues for therapeutic purposes.137 However, the dose of fisetin required for this formulation to achieve a significant degree of anticancer activity is relatively high, and thus co-delivery of natural products and chemotherapeutic agents to the particles may achieve superior efficacy. Curcumin and paclitaxel were homogeneously mixed and co-jet milled to form particles suitable for inhalation with a MMAD of 2.64–3.12 μm. This co-delivery regimen possessed, on the one hand, enhanced anticancer activity, inducing apoptosis/necrotic cell death, G2/M cell cycle arrests and oxidative stress (increase in ROS, mitochondrial depolarization and decrease in ATP content). On the other hand, the presence of curcumin attenuated the toxic effects of paclitaxel on healthy cells.138 This suggests that combination formulations of chemotherapeutic agents with chemoprotective agents (natural products) are a promising option.
Inhaled medications are already the first-line treatment for COPD, such as budesonide, but some airway inflammation is resistant to glucocorticoids, leading to treatment failure. Inhalable dry powder formulations of resveratrol with an MMAD of 3.7 ± 0.1 μm were prepared using a spray-drying method, showing excellent lung deposition, transport and cellular uptake, which in turn inhibited the production of multiple inflammatory mediators (eg, IL-8, TNF-α, and TGF-β1) is expected to be efficacious in inflammatory lung diseases such as COPD.139 In addition, the combination of resveratrol and budesonide to design inhalable microparticles holds promise for synergistic efficacy in the treatment of COPD. Budesonide reduced cohesion between resveratrol particles and reduced particle agglomeration, resulting in significantly improved aerosol properties suitable for inhaled drug delivery, which in turn synergistically inhibited alveolar macrophage inflammation and oxidative stress.140 Naringin is also a flavonoid with excellent antioxidant activity, and inhalable naringin microparticles were prepared by spray-drying method with higher solubility, lower density and improved aerodynamic properties.141 Next, the researchers used leucine to further enhance the aerosol properties of naringenin microparticles, which in turn enhanced the pharmacological activity of naringenin, inhibiting NF-κB and MAPK/ERK pathways to attenuate the hyperinflammatory state associated with cystic fibrosis.142
Nanocomposites and Nanoaggregates
Although nanocarriers are excellent carriers for targeted drug delivery, their size range (<1 μm) makes them easily exhaled before reaching the target. In general, particles in the size range of 1–5 μm can only be deposited at the lung base and reach the alveoli, thus fully utilizing the anti-cancer activity of the drug.143 Physical instability and low lung deposition efficiency of nanoparticles, particle-particle interactions also hinder drug delivery to the lungs. Despite overcoming this challenge, microparticles undergo pulmonary clearance via alveolar macrophages.12 Incorporating nanoparticles into inhalable micron-sized carriers combines the advantages of both micron and nanoparticle drug delivery systems and will likely offer unique advantages in pulmonary drug delivery,144 thus taking full advantage of natural products (Table 6).
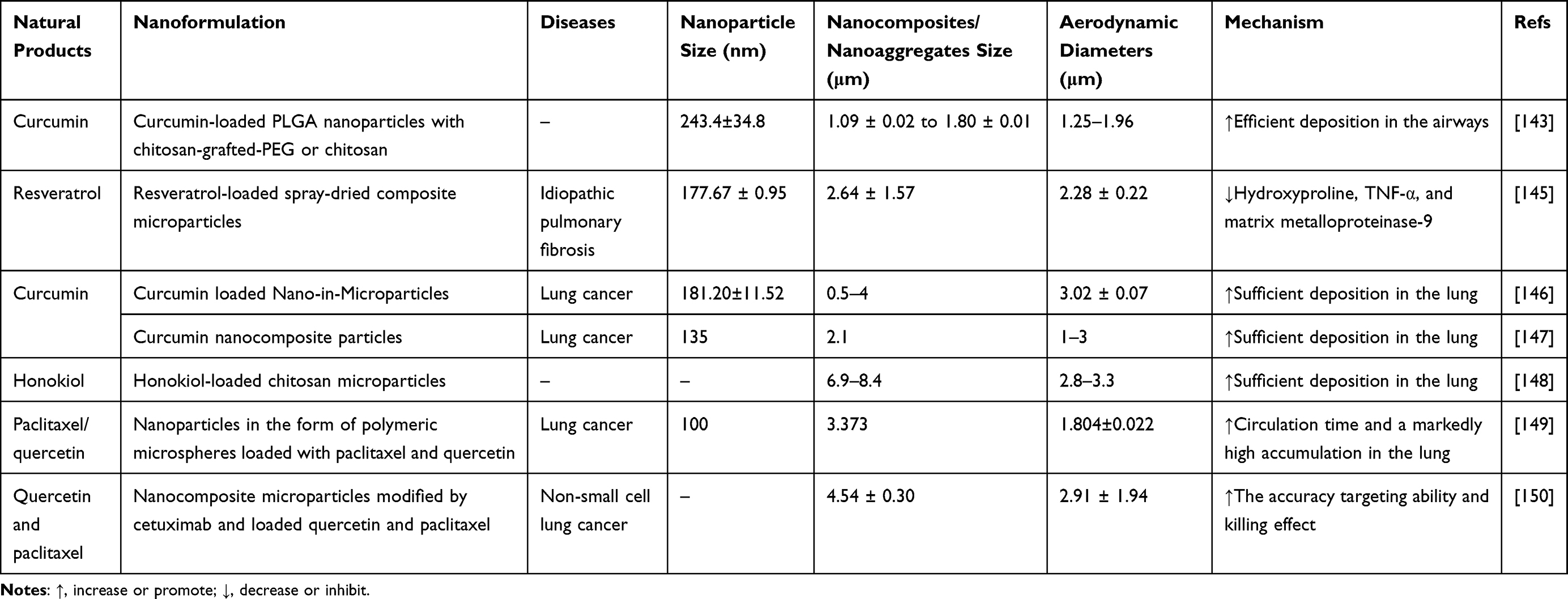 |
Table 6 Natural Products-Based Inhaled Nanocomposites and Nanoaggregates for the Treatment of Pulmonary Diseases |
Ahmed et al145 first prepared resveratrol-loaded bovine serum albumin nanoparticles (BSA NPs), and then the NPs were co-spray-dried into composite microparticles with different carriers including mannitol, dextran, trehalose, leucine, glycine, aspartic acid, and glutamic acid. Encouragingly, the MMAD of these microparticles was less than 5 μm, and all were suitable for deep lung deposition, especially leucine aerosolization was the most effective with an FPF of 75.74%. The composite microparticles released NPs upon contact with lung fluid and sustained the release of resveratrol, which successfully ameliorated bleomycin-induced pulmonary fibrosis in mice.145 Similarly, other natural products, such as curcumin146,147 and honokiol,148 could be prepared first as nanoparticles to enhance their therapeutic effects, followed by the use of chitosan as a material for encapsulating the nanoparticles and spray-drying to produce composite microparticles with appropriate aerodynamic properties to disintegrate into pristine nanoparticles to exert their medicinal effects when sufficiently deposited and redispersed in the lungs.
Inhalable nano-formulations with deformable size also contribute to lung retention and targeted drug accumulation.81 El-Sherbiny et al143 doped curcumin-loaded PLGA nanoparticles into amphiphilic PEG-chitosan copolymer hydrogel microspheres to develop swellable biocompatible microparticles. Upon inhalation, the formulation was able to rapidly expand under humid conditions, such as in the lung, and evade macrophage uptake, allowing for effective deposition in the airways and controlled release of curcumin over 24 hours.143
In addition, composite particles provide an optional option for drug co-loading. Liu et al149 prepared NPs loaded with paclitaxel and quercetin as polymeric microspheres (PMs). PMs are polymers formed from a large number of NPs with a uniform size ranging from 1 to 5 μm in diameter. PMs are inhaled deep into the lungs and redispersed into NPs with diameters ranging from 250 to 350 nm. This formulation prolongs drug release and increases the retention time of paclitaxel in the lungs. Quercetin inhibits the expression of the P-glycoprotein drug efflux pumps, which in turn improves the body’s sensitivity to paclitaxel.34 Cui et al150 fabricated cetuximab-modified nanoparticles loaded with paclitaxel and quercetin, respectively, and then used a spray-drying technique to composite these two nanoparticles into nanocomposite microparticles (P/Q@CNMPs). The P/Q@CNMPs had a suitable aerodynamic diameter and homogeneous morphology to meet the requirements for particle deposition in the lungs. The excipient mannitol, which is highly absorbent and easily disintegrated, ensures rapid decomposition of the nanocomposite microparticles in the moist environment of lung mucus and lung surface active substances to release drug-loaded nanoparticles. Cetuximab modification enhances the precise targeting and killing effect of the formulation on the surface high-expression EGFR lung cancer cells.150 These results show that nanocomposites and nanoaggregates combine the advantages of both nano- and micro-size particles and have great potential for targeted drug delivery in lung diseases.
Conclusion and Prospects
Although inhalable nanoformulations are still in the exploratory stage, it is clear that the direct, inhalable route is more favorable for pulmonary drug delivery and lung disease control than conventional systemic delivery, significantly avoiding drug loss, off-target effects, systemic and organ toxicity. The real clinical use of inhaled formulations currently faces a number of challenges: the first is to design a drug delivery system that matches the physiological-pathological characteristics of the lung. The size, surface properties, and aerodynamic characteristics of micro/nano carriers determine their ability to target deeper regions of the lung (alveoli) while safely crossing the mucosal barrier to avoid clearance by pulmonary macrophages. The second is potential toxicity. The drug delivery system itself may be potentially toxic, and the cumulative effect of prolonged use without timely pulmonary clearance may have unknown consequences, which is certainly contrary to the intended purpose. Even more critical is the return to nature. Medicinal plants are a promising source for inhalation formulations. More and more researchers and drug development companies should consider natural plant components when designing and developing novel dosage forms. How to optimize the bioavailability of natural products based on the full pharmacological activity of botanical ingredients is a current problem that needs to be solved. It can be expected that, along with the advances in nanomaterials and inhaled drug delivery technology, more and more new inhaled formulations will eventually be used in various lung diseases to change the current dilemma of lung disease prevention and control.
Funding
This work was supported by the Sichuan Provincial Science and Technology Innovation and Entrepreneurship Seedling Project (No. 2022JDRC0139) and Chongqing Science and Health Joint Medical Research Project (No. 2020FYYX024).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Soriano JB, Kendrick PJ, Paulson KR. Prevalence and attributable health burden of chronic respiratory diseases, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/S2213-2600(20)30105-3
2. Leiter A, Veluswamy RR, Wisnivesky JP. The global burden of lung cancer: current status and future trends. Nat Rev Clin Oncol. 2023;20(9):624–639. doi:10.1038/s41571-023-00798-3
3. Bai X, Zhao G, Chen Q, et al. Inhaled siRNA nanoparticles targeting IL11 inhibit lung fibrosis and improve pulmonary function post-bleomycin challenge. Sci Adv. 2022;8(25):eabn7162. doi:10.1126/sciadv.abn7162
4. Shen AM, Minko T. Pharmacokinetics of inhaled nanotherapeutics for pulmonary delivery. J Control Release. 2020;326:222–244. doi:10.1016/j.jconrel.2020.07.011
5. Mehta P, Bothiraja C, Mahadik K, et al. Phytoconstituent based dry powder inhalers as biomedicine for the management of pulmonary diseases. Biomed Pharmacother. 2018;108:828–837. doi:10.1016/j.biopha.2018.09.094
6. Hickey AJ. Emerging trends in inhaled drug delivery. Adv Drug Deliv Rev. 2020;157:63–70. doi:10.1016/j.addr.2020.07.006
7. Zhang Y, Lu P, Qin H, et al. Traditional Chinese medicine combined with pulmonary drug delivery system and idiopathic pulmonary fibrosis: rationale and therapeutic potential. Biomed Pharmacother. 2021;133:111072. doi:10.1016/j.biopha.2020.111072
8. Kanwal Q, Shahid S, Ahmad A, et al. Sustainable, economical and rapid treatment of multiple lung diseases using therapeutic potential of curcumin nanoparticles. Environ Res. 2023;233:116477. doi:10.1016/j.envres.2023.116477
9. Julia Altube M, Perez N, Romero EL, et al. Inhaled lipid nanocarriers for pulmonary delivery of glucocorticoids: previous strategies, recent advances and key factors description. Int J Pharm. 2023;642:123146. doi:10.1016/j.ijpharm.2023.123146
10. Borghardt JM, Kloft C, Sharma A. Inhaled Therapy in Respiratory Disease: the Complex Interplay of Pulmonary Kinetic Processes. Can Respir J. 2018;2018:2732017. doi:10.1155/2018/2732017
11. Danaei M, Dehghankhold M, Ataei S, et al. Impact of Particle Size and Polydispersity Index on the Clinical Applications of Lipidic Nanocarrier Systems. Pharmaceutics. 2018;10(2):57.
12. Gupta C, Jaipuria A, Gupta N. Inhalable Formulations to Treat Non-Small Cell Lung Cancer (NSCLC): recent Therapies and Developments. Pharmaceutics. 2022;15(1):548.
13. Pasqua E, Hamblin N, Edwards C, et al. Developing inhaled drugs for respiratory diseases: a medicinal chemistry perspective. Drug Discov Today. 2022;27(1):134–150. doi:10.1016/j.drudis.2021.09.005
14. Kukut Hatipoglu M, Hickey AJ, Garcia-Contreras L. Pharmacokinetics and pharmacodynamics of high doses of inhaled dry powder drugs. Int J Pharm. 2018;549(1–2):306–316. doi:10.1016/j.ijpharm.2018.07.050
15. Guo Y, Bera H, Shi C, et al. Pharmaceutical strategies to extend pulmonary exposure of inhaled medicines. Acta Pharm Sin B. 2021;11(8):2565–2584. doi:10.1016/j.apsb.2021.05.015
16. Liao W, Li Y, Wang J, et al. Natural Products-Based Nanoformulations: a New Approach Targeting CSCs to Cancer Therapy. Int J Nanomed. 2022;17:4163–4193. doi:10.2147/IJN.S380697
17. Shi J, Kantoff PW, Wooster R, et al. Cancer nanomedicine: progress, challenges and opportunities. Nat Rev Cancer. 2017;17(1):20–37. doi:10.1038/nrc.2016.108
18. Petros RA, DeSimone JM. Strategies in the design of nanoparticles for therapeutic applications. Nat Rev Drug Discov. 2010;9(8):615–627. doi:10.1038/nrd2591
19. Han J, Sheng T, Zhang Y, et al. Bioresponsive Immunotherapeutic Materials. Adv Mater;2023. e2209778. doi:10.1002/adma.202209778
20. Gandhi S, Roy I. Lipid-Based Inhalable Micro- and Nanocarriers of Active Agents for Treating Non-Small-Cell Lung Cancer. Pharmaceutics. 2023;15(5):658.
21. Ke WR, Chang RYK, Chan HK. Engineering the right formulation for enhanced drug delivery. Adv Drug Deliv Rev. 2022;191:114561. doi:10.1016/j.addr.2022.114561
22. Lee WH, Loo C-Y, Traini D, et al. Nano- and micro-based inhaled drug delivery systems for targeting alveolar macrophages. Expert Opin Drug Deliv. 2015;12(6):1009–1026. doi:10.1517/17425247.2015.1039509
23. Hassan MS, Lau RW. Effect of particle shape on dry particle inhalation: study of flowability, aerosolization, and deposition properties. AAPS Pharm Sci Tech. 2009;10(4):1252–1262. doi:10.1208/s12249-009-9313-3
24. Khutoryanskiy VV. Beyond PEGylation: alternative surface-modification of nanoparticles with mucus-inert biomaterials. Adv Drug Deliv Rev. 2018;124:140–149. doi:10.1016/j.addr.2017.07.015
25. García-Fernández A, Sancenón F, Martínez-Máñez R. Mesoporous silica nanoparticles for pulmonary drug delivery. Adv Drug Deliv Rev. 2021;177:113953. doi:10.1016/j.addr.2021.113953
26. Guagliardo R, Pérez-Gil J, De Smedt S, et al. Pulmonary surfactant and drug delivery: focusing on the role of surfactant proteins. J Control Release. 2018;291:116–126. doi:10.1016/j.jconrel.2018.10.012
27. Jin Z, Gao Q, Wu K, et al. Harnessing inhaled nanoparticles to overcome the pulmonary barrier for respiratory disease therapy. Adv Drug Deliv Rev. 2023;115111.
28. Zhu X, Yu Z, Feng L, et al. Chitosan-based nanoparticle co-delivery of docetaxel and curcumin ameliorates anti-tumor chemoimmunotherapy in lung cancer. Carbohydr Polym. 2021;268:118237. doi:10.1016/j.carbpol.2021.118237
29. Abdelaziz HM, Gaber M, Abd-Elwakil MM, et al. Inhalable particulate drug delivery systems for lung cancer therapy: nanoparticles, microparticles, nanocomposites and nanoaggregates. J Control Release. 2018;269:374–392. doi:10.1016/j.jconrel.2017.11.036
30. Panahi Y, Ghanei M, Rahimi M, et al. Evaluation the efficacy and safety of N-acetylcysteine inhalation spray in controlling the symptoms of patients with COVID-19: an open-label randomized controlled clinical trial. J Med Virol. 2023;95(1):e28393. doi:10.1002/jmv.28393
31. Waxman A, Restrepo-Jaramillo R, Thenappan T, et al. Long-term inhaled treprostinil for pulmonary hypertension due to interstitial lung disease: INCREASE open-label extension study. Eur Respir J. 2023;61(6):2202414. doi:10.1183/13993003.02414-2022
32. West A, Chaudhuri N, Barczyk A, et al. Inhaled pirfenidone solution (AP01) for IPF: a randomised, open-label, dose-response trial. Thorax. 2023;78(9):882–889. doi:10.1136/thorax-2022-219391
33. Karvouniaris M, Makris D, Zygoulis P, et al. Nebulised colistin for ventilator-associated pneumonia prevention. Eur Respir J. 2015;46(6):1732–1739. doi:10.1183/13993003.02235-2014
34. Middleton A, Robinson PD, McKay K, et al. A pilot study of inhaled dry-powder mannitol during cystic fibrosis-related pulmonary exacerbation. Eur Respir J. 2015;45(2):541–544. doi:10.1183/09031936.00137814
35. Wilson R, Welte T, Polverino E, et al. Ciprofloxacin dry powder for inhalation in non-cystic fibrosis bronchiectasis: a Phase II randomised study. Eur Respir J. 2013;41(5):1107–1115. doi:10.1183/09031936.00071312
36. Tayab ZR, Hochhaus G. Pharmacokinetic/pharmacodynamic evaluation of inhalation drugs: application to targeted pulmonary delivery systems. Expert Opin Drug Deliv. 2005;2(3):519–532. doi:10.1517/17425247.2.3.519
37. Liao W, Zhang L, Chen X, et al. Targeting cancer stem cells and signalling pathways through phytochemicals: a promising approach against colorectal cancer. Phytomedicine. 2023;108:154524. doi:10.1016/j.phymed.2022.154524
38. Kakran M, Shegokar R, Sahoo NG, et al. Fabrication of quercetin nanocrystals: comparison of different methods. Eur J Pharm Biopharm. 2012;80(1):113–121. doi:10.1016/j.ejpb.2011.08.006
39. Wu JW, Lin L-C, Hung S-C, et al. Analysis of silibinin in rat plasma and bile for hepatobiliary excretion and oral bioavailability application. J Pharm Biomed Anal. 2007;45(4):635–641. doi:10.1016/j.jpba.2007.06.026
40. Muller MP, Jiang T, Sun C, et al. Characterization of Lipid-Protein Interactions and Lipid-Mediated Modulation of Membrane Protein Function through Molecular Simulation. Chem Rev. 2019;119(9):6086–6161. doi:10.1021/acs.chemrev.8b00608
41. Tenchov R, Bird R, Curtze AE, et al. Lipid Nanoparticles─From Liposomes to mRNA Vaccine Delivery, a Landscape of Research Diversity and Advancement. ACS Nano. 2021;15(11):16982–17015. doi:10.1021/acsnano.1c04996
42. Hald Albertsen C, Kulkarni JA, Witzigmann D, et al. The role of lipid components in lipid nanoparticles for vaccines and gene therapy. Adv Drug Deliv Rev. 2022;188:114416. doi:10.1016/j.addr.2022.114416
43. Lam K, Schreiner P, Leung A, et al. Optimizing Lipid Nanoparticles for Delivery in Primates. Adv Mater. 2023;35(26):e2211420. doi:10.1002/adma.202211420
44. Li M, Zhang T, Zhu L, et al. Liposomal andrographolide dry powder inhalers for treatment of bacterial pneumonia via anti-inflammatory pathway. Int J Pharm. 2017;528(1–2):163–171. doi:10.1016/j.ijpharm.2017.06.005
45. Peng J, Wang Q, Guo M, et al. Development of Inhalable Chitosan-Coated Oxymatrine Liposomes to Alleviate RSV-Infected Mice. Int J Mol Sci. 2022;23(24):15909.
46. Peng J, Cai Z, Wang Q, et al. Carboxymethyl Chitosan Modified Oxymatrine Liposomes for the Alleviation of Emphysema in Mice via Pulmonary Administration. Molecules. 2022;27(11):3610.
47. Kotta S, Aldawsari HM, Badr-Eldin SM, et al. Aerosol Delivery of Surfactant Liposomes for Management of Pulmonary Fibrosis: an Approach Supporting Pulmonary Mechanics. Pharmaceutics. 2021;13(11):1851.
48. Chennakesavulu S, et al. Pulmonary delivery of liposomal dry powder inhaler formulation for effective treatment of idiopathic pulmonary fibrosis. Asian J Pharm Sci. 2018;13(1):91–100. doi:10.1016/j.ajps.2017.08.005
49. Koshkina NV, Waldrep JC, Roberts LE, et al. Paclitaxel liposome aerosol treatment induces inhibition of pulmonary metastases in murine renal carcinoma model. Clin Cancer Res. 2001;7(10):3258–3262.
50. Zhang M, Li M, Du L, et al. Paclitaxel-in-liposome-in-bacteria for inhalation treatment of primary lung cancer. Int J Pharm. 2020;578:119177. doi:10.1016/j.ijpharm.2020.119177
51. Zhu X, Kong Y, Liu Q, et al. Inhalable dry powder prepared from folic acid-conjugated docetaxel liposomes alters pharmacodynamic and pharmacokinetic properties relevant to lung cancer chemotherapy. Pulm Pharmacol Ther. 2019;55:50–61. doi:10.1016/j.pupt.2019.02.001
52. Xiao Z, Zhuang B, Zhang G, et al. Pulmonary delivery of cationic liposomal hydroxycamptothecin and 5-aminolevulinic acid for chemo-sonodynamic therapy of metastatic lung cancer. Int J Pharm. 2021;601:120572. doi:10.1016/j.ijpharm.2021.120572
53. Xu J, Lu X, Zhu X, et al. Formulation and Characterization of Spray-Dried Powders Containing Vincristine-Liposomes for Pulmonary Delivery and Its Pharmacokinetic Evaluation From In Vitro and In Vivo. J Pharm Sci. 2019;108(10):3348–3358. doi:10.1016/j.xphs.2019.05.009
54. Koshkina NV, Gilbert BE, Waldrep JC, et al. Distribution of camptothecin after delivery as a liposome aerosol or following intramuscular injection in mice. Cancer Chemother Pharmacol. 1999;44(3):187–192. doi:10.1007/s002800050966
55. Knight V, Kleinerman ES, Waldrep JC, et al. 9-Nitrocamptothecin liposome aerosol treatment of human cancer subcutaneous xenografts and pulmonary cancer metastases in mice. Ann N Y Acad Sci. 2000;922(1):151–163. doi:10.1111/j.1749-6632.2000.tb07033.x
56. Koshkina NV, Kleinerman ES, Waidrep C, et al. 9-Nitrocamptothecin liposome aerosol treatment of melanoma and osteosarcoma lung metastases in mice. Clin Cancer Res. 2000;6(7):2876–2880.
57. Gautam A, Waldrep JC, Densmore CL, et al. Growth inhibition of established B16-F10 lung metastases by sequential aerosol delivery of p53 gene and 9-nitrocamptothecin. Gene Ther. 2002;9(5):353–357. doi:10.1038/sj.gt.3301662
58. Adel IM, ElMeligy MF, Abdelrahim ME, et al. Design and Characterization of Spray-Dried Proliposomes for the Pulmonary Delivery of Curcumin. Int J Nanomed. 2021;16:2667–2687. doi:10.2147/IJN.S306831
59. Zhang T, Chen Y, Ge Y, et al. Inhalation treatment of primary lung cancer using liposomal curcumin dry powder inhalers. Acta Pharm Sin B. 2018;8(3):440–448. doi:10.1016/j.apsb.2018.03.004
60. Gao C, Zhang L, Xu M, et al. Pulmonary delivery of liposomes co-loaded with SN38 prodrug and curcumin for the treatment of lung cancer. Eur J Pharm Biopharm. 2022;179:156–165. doi:10.1016/j.ejpb.2022.08.021
61. Fu F, Wang W, Wu L, et al. Inhalable Biomineralized Liposomes for Cyclic Ca 2+ -Burst-Centered Endoplasmic Reticulum Stress Enhanced Lung Cancer Ferroptosis Therapy. ACS Nano. 2023;17(6):5486–5502. doi:10.1021/acsnano.2c10830
62. Riaz MK, Zhang X, Wong KH, et al. Pulmonary delivery of transferrin receptors targeting peptide surface-functionalized liposomes augments the chemotherapeutic effect of quercetin in lung cancer therapy. Int J Nanomed. 2019;14:2879–2902. doi:10.2147/IJN.S192219
63. Lin C, Li M, Du L, et al. Pulmonary delivery of triptolide-loaded liposomes decorated with anti-carbonic anhydrase IX antibody for lung cancer therapy. Sci Rep. 2017;7(1):1097. doi:10.1038/s41598-017-00957-4
64. Rosière R, Van Woensel M, Gelbcke M, et al. New Folate-Grafted Chitosan Derivative To Improve Delivery of Paclitaxel-Loaded Solid Lipid Nanoparticles for Lung Tumor Therapy by Inhalation. Mol Pharm. 2018;15(3):899–910. doi:10.1021/acs.molpharmaceut.7b00846
65. Nafee N, Gaber DM, Elzoghby AO, et al. Promoted Antitumor Activity of Myricetin against Lung Carcinoma Via Nanoencapsulated Phospholipid Complex in Respirable Microparticles. Pharm Res. 2020;37(4):82. doi:10.1007/s11095-020-02794-z
66. Ji P, Yu T, Liu Y, et al. Naringenin-loaded solid lipid nanoparticles: preparation, controlled delivery, cellular uptake, and pulmonary pharmacokinetics. Drug Des Devel Ther. 2016;10:911–925. doi:10.2147/DDDT.S97738
67. Kaur P, Mishra V, Shunmugaperumal T, et al. Inhalable spray dried lipidnanoparticles for the co-delivery of paclitaxel and doxorubicin in lung cancer. J Drug Delivery Sci Technol. 2020;56:101502. doi:10.1016/j.jddst.2020.101502
68. Garbuzenko OB, Kuzmov A, Taratula O, et al. Strategy to enhance lung cancer treatment by five essential elements: inhalation delivery, nanotechnology, tumor-receptor targeting, chemo- and gene therapy. Theranostics. 2019;9(26):8362–8376. doi:10.7150/thno.39816
69. Taratula O, Kuzmov A, Shah M, et al. Nanostructured lipid carriers as multifunctional nanomedicine platform for pulmonary co-delivery of anticancer drugs and siRNA. J Control Release. 2013;171(3):349–357. doi:10.1016/j.jconrel.2013.04.018
70. Li M, Zhu L, Liu B, et al. Tea tree oil nanoemulsions for inhalation therapies of bacterial and fungal pneumonia. Colloids Surf B Biointerfaces. 2016;141:408–416. doi:10.1016/j.colsurfb.2016.02.017
71. El-Moslemany RM, El-Kamel AH, Allam EA, et al. Tanshinone IIA loaded bioactive nanoemulsion for alleviation of lipopolysaccharide induced acute lung injury via inhibition of endothelial glycocalyx shedding. Biomed Pharmacother. 2022;155:113666. doi:10.1016/j.biopha.2022.113666
72. Arbain NH, Salim N, Masoumi HRF, et al. In vitro evaluation of the inhalable quercetin loaded nanoemulsion for pulmonary delivery. Drug Deliv Transl Res. 2019;9(2):497–507. doi:10.1007/s13346-018-0509-5
73. Asmawi AA, Salim N, Ngan CL, et al. Excipient selection and aerodynamic characterization of nebulized lipid-based nanoemulsion loaded with docetaxel for lung cancer treatment. Drug Deliv Transl Res. 2019;9(2):543–554. doi:10.1007/s13346-018-0526-4
74. Said-Elbahr R, Nasr M, Alhnan MA, et al. Simultaneous pulmonary administration of celecoxib and naringin using a nebulization-friendly nanoemulsion: a device-targeted delivery for treatment of lung cancer. Expert Opin Drug Deliv. 2022;19(5):611–622. doi:10.1080/17425247.2022.2076833
75. Asmawi AA, Salim N, Abdulmalek E, et al. Modeling the Effect of Composition on Formation of Aerosolized Nanoemulsion System Encapsulating Docetaxel and Curcumin Using D-Optimal Mixture Experimental Design. Int J Mol Sci. 2020;21(12):4357. doi:10.3390/ijms21124357
76. Asmawi AA, Salim N, Abdulmalek E, et al. Size-Controlled Preparation of Docetaxel- and Curcumin-Loaded Nanoemulsions for Potential Pulmonary Delivery. Pharmaceutics. 2023;15(2):652. doi:10.3390/pharmaceutics15020652
77. Bassetti M, Vena A, Russo A, et al. Inhaled Liposomal Antimicrobial Delivery in Lung Infections. Drugs. 2020;80(13):1309–1318. doi:10.1007/s40265-020-01359-z
78. Liu Y, Crowe WN, Wang L, et al. An inhalable nanoparticulate STING agonist synergizes with radiotherapy to confer long-term control of lung metastases. Nat Commun. 2019;10(1):5108. doi:10.1038/s41467-019-13094-5
79. Alton E, Armstrong DK, Ashby D, et al. Repeated nebulisation of non-viral CFTR gene therapy in patients with cystic fibrosis: a randomised, double-blind, placebo-controlled, phase 2b trial. Lancet Respir Med. 2015;3(9):684–691. doi:10.1016/S2213-2600(15)00245-3
80. Li J, Xiao Y, Zhang Y, et al. Pulmonary Delivery of Specialized Pro-Resolving Mediators-Based Nanotherapeutics Attenuates Pulmonary Fibrosis in Preclinical Animal Models. ACS Nano. 2023;17:15354.
81. Ma S, et al. Pulmonary delivery of size-transformable nanoparticles improves tumor accumulation and penetration for chemo-sonodynamic combination therapy. J Control Release. 2022;350:132–145. doi:10.1016/j.jconrel.2022.08.003
82. Zhu T, Chen Z, Jiang G, et al. Sequential Targeting Hybrid Nanovesicles Composed of Chimeric Antigen Receptor T-Cell-Derived Exosomes and Liposomes for Enhanced Cancer Immunochemotherapy. ACS Nano. 2023;17(17):16770–16786. doi:10.1021/acsnano.3c03456
83. Pommier Y. Topoisomerase I inhibitors: camptothecins and beyond. Nat Rev Cancer. 2006;6(10):789–802. doi:10.1038/nrc1977
84. Gautam A, Densmore CL, Waldrep JC. Inhibition of experimental lung metastasis by aerosol delivery of PEI-p53 complexes. Mol Ther. 2000;2(4):318–323. doi:10.1006/mthe.2000.0138
85. Densmore CL, Kleinerman ES, Gautam A, et al. Growth suppression of established human osteosarcoma lung metastases in mice by aerosol gene therapy with PEI-p53 complexes. Cancer Gene Ther. 2001;8(9):619–627. doi:10.1038/sj.cgt.7700343
86. Nelson KM, Dahlin JL, Bisson J, et al. The Essential Medicinal Chemistry of Curcumin. J Med Chem. 2017;60(5):1620–1637. doi:10.1021/acs.jmedchem.6b00975
87. Zhang W, Sun Y, Bai L, et al. RBMS1 regulates lung cancer ferroptosis through translational control of SLC7A11. J Clin Invest. 2021;131(22):548.
88. Lim SB, Banerjee A, Önyüksel H. Improvement of drug safety by the use of lipid-based nanocarriers. J Control Release. 2012;163(1):34–45. doi:10.1016/j.jconrel.2012.06.002
89. Han L, Huang R, Liu S, et al. Peptide-conjugated PAMAM for targeted doxorubicin delivery to transferrin receptor overexpressed tumors. Mol Pharm. 2010;7(6):2156–2165. doi:10.1021/mp100185f
90. Mirchandani Y, Patravale VB. Solid lipid nanoparticles for hydrophilic drugs. J Control Release. 2021;335:457–464. doi:10.1016/j.jconrel.2021.05.032
91. Dang Y, Lin G, Xie Y, et al. Quantitative determination of myricetin in rat plasma by ultra performance liquid chromatography tandem mass spectrometry and its absolute bioavailability. Drug Res (Stuttg). 2014;64(10):516–522. doi:10.1055/s-0033-1363220
92. Costa CP, Moreira JN, Sousa Lobo JM, et al. Intranasal delivery of nanostructured lipid carriers, solid lipid nanoparticles and nanoemulsions: a current overview of in vivo studies. Acta Pharm Sin B. 2021;11(4):925–940. doi:10.1016/j.apsb.2021.02.012
93. Singh Y, Meher JG, Raval K, et al. Nanoemulsion: concepts, development and applications in drug delivery. J Control Release. 2017;252:28–49. doi:10.1016/j.jconrel.2017.03.008
94. Ashaolu TJ. Nanoemulsions for health, food, and cosmetics: a review. Environ Chem Lett. 2021;19(4):3381–3395. doi:10.1007/s10311-021-01216-9
95. Muta T, Parikh A, Kathawala K, et al. Quality-by-Design Approach for the Development of Nano-Sized Tea Tree Oil Formulation-Impregnated Biocompatible Gel with Antimicrobial Properties. Pharmaceutics. 2020;12(11):1091. doi:10.3390/pharmaceutics12111091
96. Iba T, Levy JH, Hirota T, et al. Protection of the endothelial glycocalyx by antithrombin in an endotoxin-induced rat model of sepsis. Thromb Res. 2018;171:1–6. doi:10.1016/j.thromres.2018.09.042
97. van Drooge DJ, Hinrichs WLJ, Dickhoff BHJ, et al. Spray freeze drying to produce a stable Delta(9)-tetrahydrocannabinol containing inulin-based solid dispersion powder suitable for inhalation. Eur J Pharm Sci. 2005;26(2):231–240. doi:10.1016/j.ejps.2005.06.007
98. Lai SK, Wang YY, Hanes J. Mucus-penetrating nanoparticles for drug and gene delivery to mucosal tissues. Adv Drug Deliv Rev. 2009;61(2):158–171. doi:10.1016/j.addr.2008.11.002
99. Lababidi N, Montefusco-Pereira CV, de Souza Carvalho-Wodarz C, et al. Spray-dried multidrug particles for pulmonary co-delivery of antibiotics with N-acetylcysteine and curcumin-loaded PLGA-nanoparticles. Eur J Pharm Biopharm. 2020;157:200–210. doi:10.1016/j.ejpb.2020.10.010
100. Agel MR, Baghdan E, Pinnapireddy SR, et al. Curcumin loaded nanoparticles as efficient photoactive formulations against gram-positive and gram-negative bacteria. Colloids Surf B Biointerfaces. 2019;178:460–468. doi:10.1016/j.colsurfb.2019.03.027
101. Preis E, Baghdan E, Agel MR, et al. Spray dried curcumin loaded nanoparticles for antimicrobial photodynamic therapy. Eur J Pharm Biopharm. 2019;142:531–539. doi:10.1016/j.ejpb.2019.07.023
102. Yao J, Li Y, Meng F, et al. Enhancement of suppression oxidative stress and inflammation of quercetin by nano-decoration for ameliorating silica-induced pulmonary fibrosis. Environ Toxicol: Int J. 2023;38(7):1494–1508. doi:10.1002/tox.23781
103. Wang X, et al. Inhalable resveratrol-cyclodextrin complex loaded biodegradable nanoparticles for enhanced efficacy against non-small cell lung cancer. Int J Biol Macromol. 2020;164:638–650. doi:10.1016/j.ijbiomac.2020.07.124
104. Tian X, Bera H, Guo X, et al. Pulmonary Delivery of Reactive Oxygen Species/Glutathione-Responsive Paclitaxel Dimeric Nanoparticles Improved Therapeutic Indices against Metastatic Lung Cancer. ACS Appl Mater Interfaces. 2021;13(48):56858–56872. doi:10.1021/acsami.1c16351
105. Hu X, Yang F, Liao Y, et al. Docetaxel-Loaded Cholesterol-PEG Co-Modified Poly (n-Butyl) Cyanoacrylate Nanoparticles for Antitumor Drug Pulmonary Delivery: preparation, Characterization, and in vivo Evaluation. Int J Nanomed. 2020;15:5361–5376. doi:10.2147/IJN.S249511
106. Said-Elbahr R, Nasr M, Alhnan MA, et al. Nebulizable colloidal nanoparticles co-encapsulating a COX-2 inhibitor and a herbal compound for treatment of lung cancer. Eur J Pharm Biopharm. 2016;103:1–12. doi:10.1016/j.ejpb.2016.03.025
107. Meenach SA, Anderson KW, Zach Hilt J, et al. Characterization and aerosol dispersion performance of advanced spray-dried chemotherapeutic PEGylated phospholipid particles for dry powder inhalation delivery in lung cancer. Eur J Pharm Sci. 2013;49(4):699–711. doi:10.1016/j.ejps.2013.05.012
108. Liu Q, Xue J, Zhang X, et al. The influence of a biomimetic pulmonary surfactant modification on the in vivo fate of nanoparticles in the lung. Acta Biomater. 2022;147:391–402. doi:10.1016/j.actbio.2022.05.038
109. Trigo-Gutierrez JK, Vega-Chacón Y, Soares AB, et al. Antimicrobial Activity of Curcumin in Nanoformulations: a Comprehensive Review. Int J Mol Sci. 2021;22(13):7130. doi:10.3390/ijms22137130
110. Fazio JC, Gandhi SA, Flattery J, et al. Silicosis Among Immigrant Engineered Stone (Quartz) Countertop Fabrication Workers in California. JAMA Intern Med. 2023;183(9):991–998. doi:10.1001/jamainternmed.2023.3295
111. Zhou F, Peterson T, Fan Z, et al. The Commonly Used Stabilizers for Phytochemical-Based Nanoparticles: stabilization Effects, Mechanisms, and Applications. Nutrients. 2023;15(18):3881. doi:10.3390/nu15183881
112. Luo C, Sun J, Liu D, et al. Self-Assembled Redox Dual-Responsive Prodrug-Nanosystem Formed by Single Thioether-Bridged Paclitaxel-Fatty Acid Conjugate for Cancer Chemotherapy. Nano Lett. 2016;16(9):5401–5408. doi:10.1021/acs.nanolett.6b01632
113. Wang X, Zhang M, Li Y, et al. Research Status of Dendrimer Micelles in Tumor Therapy for Drug Delivery. Small. 2023;19(50):e2304006. doi:10.1002/smll.202304006
114. Jin M, Liu B, Zhang Z, et al. Catechin-functionalized Cationic Lipopolymer Based Multicomponent Nanomicelles for Lung-Targeting Delivery. Adv Mater;2023. e2302985. doi:10.1002/adma.202302985
115. Rezazadeh M, Davatsaz Z, Emami J, et al. Preparation and Characterization of Spray-Dried Inhalable Powders Containing Polymeric Micelles for Pulmonary Delivery of Paclitaxel in Lung Cancer. J Pharm Pharm Sci. 2018;21(1s):200s–214s. doi:10.18433/jpps30048
116. Mahajan HS, Mahajan PR. Development of grafted xyloglucan micelles for pulmonary delivery of curcumin: in vitro and in vivo studies. Int J Biol Macromol. 2016;82:621–627. doi:10.1016/j.ijbiomac.2015.09.053
117. Cox TR. The matrix in cancer. Nat Rev Cancer. 2021;21(4):217–238. doi:10.1038/s41568-020-00329-7
118. Wang X, Chen Q, Zhang X, et al. Matrix metalloproteinase 2/9-triggered-release micelles for inhaled drug delivery to treat lung cancer: preparation and in vitro/in vivo studies. Int J Nanomed. 2018;13:4641–4659. doi:10.2147/IJN.S166584
119. Pavelić K, Kraljević Pavelić SK, Bulog A, et al. Nanoparticles in Medicine: current Status in Cancer Treatment. Int J Mol Sci. 2023;24(16):12827. doi:10.3390/ijms241612827
120. Muraoka D, Harada N, Shiku H, et al. Self-assembled polysaccharide nanogel delivery system for overcoming tumor immune resistance. J Control Release. 2022;347:175–182. doi:10.1016/j.jconrel.2022.05.004
121. Chen YB, Zhang Y-B, Wang Y-L, et al. A novel inhalable quercetin-alginate nanogel as a promising therapy for acute lung injury. J Nanobiotechnology. 2022;20(1):272. doi:10.1186/s12951-022-01452-3
122. Liang Y, Duan L, Lu J, et al. Engineering exosomes for targeted drug delivery. Theranostics. 2021;11(7):3183–3195. doi:10.7150/thno.52570
123. Zheng W, Zhu T, Tang L, et al. Inhalable CAR-T cell-derived exosomes as paclitaxel carriers for treating lung cancer. J Transl Med. 2023;21(1):383. doi:10.1186/s12967-023-04206-3
124. Shanmugam T, Joshi N, Ahamad N, et al. Enhanced absorption, and efficacy of oral self-assembled paclitaxel nanocochleates in multi-drug resistant colon cancer. Int J Pharm. 2020;586:119482. doi:10.1016/j.ijpharm.2020.119482
125. Shanmugam T, Joshi N, Kaviratna A, et al. Aerosol Delivery of Paclitaxel-Containing Self-Assembled Nanocochleates for Treating Pulmonary Metastasis: an Approach Supporting Pulmonary Mechanics. ACS Biomater Sci Eng. 2021;7(1):144–156. doi:10.1021/acsbiomaterials.0c01126
126. Pápay ZE, Kósa A, Böddi B, et al. Study on the Pulmonary Delivery System of Apigenin-Loaded Albumin Nanocarriers with Antioxidant Activity. J Aerosol Med Pulm Drug Deliv. 2017;30(4):274–288. doi:10.1089/jamp.2016.1316
127. Hanafy NAN, El-Kemary MA. Silymarin/curcumin loaded albumin nanoparticles coated by chitosan as muco-inhalable delivery system observing anti-inflammatory and anti COVID-19 characterizations in oleic acid triggered lung injury and in vitro COVID-19 experiment. Int J Biol Macromol. 2022;198:101–110. doi:10.1016/j.ijbiomac.2021.12.073
128. Khan I, Apostolou M, Bnyan R, et al. Paclitaxel-loaded micro or nano transfersome formulation into novel tablets for pulmonary drug delivery via nebulization. Int J Pharm. 2020;575:118919. doi:10.1016/j.ijpharm.2019.118919
129. Hureaux J, Lagarce F, Gagnadoux F, et al. Lipid nanocapsules: ready-to-use nanovectors for the aerosol delivery of paclitaxel. Eur J Pharm Biopharm. 2009;73(2):239–246. doi:10.1016/j.ejpb.2009.06.013
130. Zhang J, Lv H, Jiang K, et al. Enhanced bioavailability after oral and pulmonary administration of baicalein nanocrystal. Int J Pharm. 2011;420(1):180–188. doi:10.1016/j.ijpharm.2011.08.023
131. Hu L, Kong D, Hu Q, et al. Evaluation of High-Performance Curcumin Nanocrystals for Pulmonary Drug Delivery Both In Vitro and In Vivo. Nanoscale Res Lett. 2015;10(1):381. doi:10.1186/s11671-015-1085-y
132. Scalia S, Haghi M, Losi V, et al. Quercetin solid lipid microparticles: a flavonoid for inhalation lung delivery. Eur J Pharm Sci. 2013;49(2):278–285. doi:10.1016/j.ejps.2013.03.009
133. Scalia S, Trotta V, Traini D, et al. Incorporation of quercetin in respirable lipid microparticles: effect on stability and cellular uptake on A549 pulmonary alveolar epithelial cells. Colloids Surf B Biointerfaces. 2013;112:322–329. doi:10.1016/j.colsurfb.2013.07.067
134. Lu P, Li J, Liu C, et al. Salvianolic acid B dry powder inhaler for the treatment of idiopathic pulmonary fibrosis. Asian J Pharm Sci. 2022;17(3):447–461. doi:10.1016/j.ajps.2022.04.004
135. Jiang L, Li Y, Yu J, et al. A dry powder inhalable formulation of salvianolic acids for the treatment of pulmonary fibrosis: safety, lung deposition, and pharmacokinetic study. Drug Deliv Transl Res. 2021;11(5):1958–1968. doi:10.1007/s13346-020-00857-7
136. Qi D, Jia B, Peng H, et al. Baicalin/ambroxol hydrochloride combined dry powder inhalation formulation targeting lung delivery for treatment of idiopathic pulmonary fibrosis: fabrication, characterization, pharmacokinetics, and pharmacodynamics. Eur J Pharm Biopharm. 2023;188:243–253. doi:10.1016/j.ejpb.2023.05.017
137. Mohtar N, Taylor KMG, Sheikh K, et al. Design and development of dry powder sulfobutylether-β-cyclodextrin complex for pulmonary delivery of fisetin. Eur J Pharm Biopharm. 2017;113:1–10. doi:10.1016/j.ejpb.2016.11.036
138. Lee WH, Loo C-Y, Traini D, et al. Development and Evaluation of Paclitaxel and Curcumin Dry Powder for Inhalation Lung Cancer Treatment. Pharmaceutics. 2020;13(1):9. doi:10.3390/pharmaceutics13010009
139. Trotta V, Lee W-H, Loo C-Y, et al. In vitro biological activity of resveratrol using a novel inhalable resveratrol spray-dried formulation. Int J Pharm. 2015;491(1–2):190–197. doi:10.1016/j.ijpharm.2015.06.033
140. Trotta V, Lee W-H, Loo C-Y, et al. Co-spray dried resveratrol and budesonide inhalation formulation for reducing inflammation and oxidative stress in rat alveolar macrophages. Eur J Pharm Sci. 2016;86:20–28. doi:10.1016/j.ejps.2016.02.018
141. Sansone F, Aquino RP, Gaudio PD, et al. Physical characteristics and aerosol performance of naringin dry powders for pulmonary delivery prepared by spray-drying. Eur J Pharm Biopharm. 2009;72(1):206–213. doi:10.1016/j.ejpb.2008.10.007
142. Prota L, Santoro A, Bifulco M, et al. Leucine enhances aerosol performance of naringin dry powder and its activity on cystic fibrosis airway epithelial cells. Int J Pharm. 2011;412(1–2):8–19. doi:10.1016/j.ijpharm.2011.03.055
143. El-Sherbiny IM, Smyth HD. Controlled release pulmonary administration of curcumin using swellable biocompatible microparticles. Mol Pharm. 2012;9(2):269–280. doi:10.1021/mp200351y
144. Alhajj N, O’Reilly NJ, Cathcart H. Nano-in-Microparticles for Pulmonary Drug Delivery. In: Mehta PP, Dhapte-Pawar V, editors. Pulmonary Drug Delivery Systems: Material and Technological Advances. Singapore: Springer Nature Singapore; 2023:91–129.
145. Ahmed S, Mansour M, Ishak RAH, et al. Customizable resveratrol spray-dried micro-composites for inhalation as a promising contender for treatment of idiopathic pulmonary fibrosis. Int J Pharm. 2023;642:123117. doi:10.1016/j.ijpharm.2023.123117
146. Baghdan E, Duse L, Schüer JJ, et al. Development of inhalable curcumin loaded Nano-in-Microparticles for bronchoscopic photodynamic therapy. Eur J Pharm Sci. 2019;132:63–71. doi:10.1016/j.ejps.2019.02.025
147. Taki M, Tagami T, Fukushige K, et al. Fabrication of nanocomposite particles using a two-solution mixing-type spray nozzle for use in an inhaled curcumin formulation. Int J Pharm. 2016;511(1):104–110. doi:10.1016/j.ijpharm.2016.06.134
148. Li X, Guo Q, Zheng X, et al. Preparation of honokiol-loaded chitosan microparticles via spray-drying method intended for pulmonary delivery. Drug Deliv. 2009;16(3):160–166. doi:10.1080/10717540902738341
149. Liu K, Chen W, Yang T, et al. Paclitaxel and quercetin nanoparticles co-loaded in microspheres to prolong retention time for pulmonary drug delivery. Int J Nanomed. 2017;12:8239–8255. doi:10.2147/IJN.S147028
150. Cui X, Zhang F, Zhao Y, et al. A novel ligand-modified nanocomposite microparticles improved efficiency of quercetin and paclitaxel delivery in the non-small cell lung cancer. Drug Deliv. 2022;29(1):3123–3133. doi:10.1080/10717544.2022.2120567
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.