Back to Journals » International Journal of Nanomedicine » Volume 21
Natural Polymers Based Biocompatible Nanomedicines for Targeting Colon Cancer: Prospects and Challenges
Received 16 November 2025
Accepted for publication 6 March 2026
Published 30 March 2026 Volume 2026:21 581940
DOI https://doi.org/10.2147/IJN.S581940
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Kamakhya Misra
Qi Wang,1 Zhendong Liu,2 Ketao Jin3
1Department of Colorectal Surgery, Shaoxing People’s Hospital, Shaoxing, Zhejiang, 312000, People’s Republic of China; 2Department of Medical Oncology, The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Chinese Medicine), Hangzhou, Zhejiang, 310003, People’s Republic of China; 3Department of Colorectal and Anal Surgery, The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Chinese Medicine), Hangzhou, Zhejiang, 310003, People’s Republic of China
Correspondence: Ketao Jin, Department of Colorectal and Anal Surgery, The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Chinese Medicine), No. 54, Youdian Road, Hangzhou, Zhejiang, 310003, People’s Republic of China, Email [email protected] Zhendong Liu, Department of Medical Oncology, The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Chinese Medicine), No. 54, Youdian Road, Hangzhou, Zhejiang, 310003, People’s Republic of China, Email [email protected]
Abstract: Natural polymers have gained significant attention as materials for the development of biocompatible nanomedicines, offering promising potential for the targeted treatment of colon cancer. These biopolymers are derived out of renewable resources and possess many beneficial characteristics such as biodegradability, low immunogenicity and easy functionalisation to allow precise targeting, making them highly applicable to nanomedicine applications. They can be used to prepare nanoparticles that can effectively deliver therapeutic agents to tumor sites, improving therapeutic effects and reducing systemic toxicity. In addition, the versatile chemical structures of natural polymers allow conjugation with targeting ligands, which allows increased specificity in colon cancer therapy. However, despite these benefits, there are still a number of challenges in the development and clinical translation of natural polymer-based nanomedicines. The complexity of nanoparticles design, including careful control of particle size, physicochemical properties of the surface, and drug-loading capacity, makes the synthesis process and scale-up difficult. Moreover, the realization of consistent and reproducible production at an industrial level is a significant obstacle. Also, although the phenomenon of enhanced permeability and retention (EPR) increases passive tumour targeting, its heterogeneity in colorectal cancer patients compromises predictability of therapeutic responses, which necessitates individualised treatment plans. The possible cytotoxicity of nanoparticles, especially those with complex structures, highlights the need to have more realistic preclinical models to carefully test safety and therapeutic efficacy. The review provides an in-depth evaluation of the present situation of natural polymer-based nanomedicines in the treatment of colon cancer, their unique properties, therapeutic potential, and the challenges that need to be overcome to achieve clinical success. Novel technologies, including microfluidic systems and individualised treatment plans, are given particular focus as they are likely to reduce these challenges and open the path to safer, more effective, and scalable nanomedicine solutions to colon cancer.
Keywords: natural polymers, nanomedicine, biocompatability, targeted delivery, colon cancer
Introduction
Colorectal cancer (CRC) is one of the strongest malignancies in the world, which has ensured that it has been ranked as the third most frequently diagnosed cancer and as the second-most frequent cancer-related mortality in the world.1,2 The latest epidemiological evidence is specifically frightening, and reports show an annual burden of more than 1.9 million new cases and almost 1 million deaths, and the estimates project that the number of new cases will go to 3.2 million, and the number of deaths will reach 1.6 million by 2040.3 Although the overall incidence and mortality rates among the elderly population in developed countries are steadily decreasing, and in most cases, it can be explained by effective screening techniques, there is a worrying pattern that the prevalence of CRC among the population that are younger than 50 years of age has been steadily increasing.4 This early-onset CRC is often found at an advanced age, which also adds to the reason as to why CRC is the leading cancer killer of men under 50 in the United States.1 The growing epidemic in the domain of public health, as well as the complexity of the disease, which is conditioned by both modifiable (diet, physical activity, obesity) and non-modifiable (genetic) risk factors, requires a paradigm shift in the approach to its treatment,5 as illustrated in Figure 1.
 |
Figure 1 Factors associated to cause colon cancer. Adapted from 6 under a creative common license. |
The contemporary standard of care of CRC is a multimodal strategy that incorporates surgery, chemotherapy (CT), and, in the case of rectal cancer, radiotherapy (RT) and includes target agents or immunotherapy as adding supplements.7 Even though these traditional treatments have increased the general survival rates, they essentially have extreme gross weaknesses that cannot achieve full recovery of a considerable proportion of patients.8 The most severe and general disadvantage is the lack of specificity in the systemic distribution of conventional cytotoxic agents such as 5-Fluorouracil (5-FU), Oxaliplatin and Irinotecan.9 These agents act without selectiveness attacking fast dividing cells such as normal proliferating cells in the bone marrow, hair follicles, and the gastrointestinal tract causing dose-limiting systemic toxicities;10 comparative overview of general solid tumour characteristics is mentioned in Table 1. The most common adverse effects are myelosuppression (neutropenia), disabling gastrointestinal toxicity, and peripheral neuropathy that substantially diminishes health-related quality of life (HRQoL) in patients, and often requires a reduction in dose or discontinuing the treatment, thus weakening treatment efficacy.11
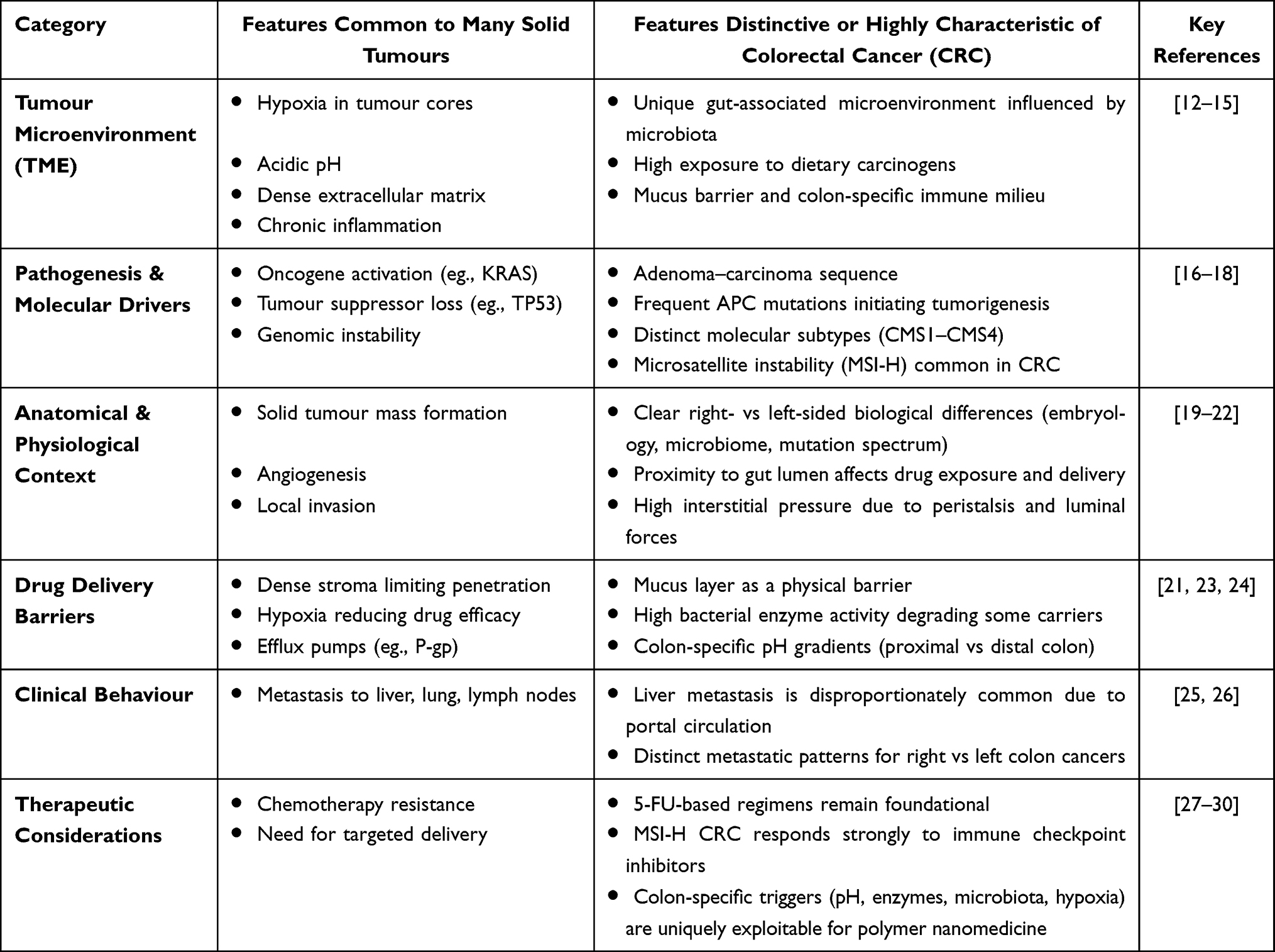 |
Table 1 Comparative Overview of General Solid Tumour Characteristics versus Features Specific to CRC, Highlighting Key Biological and Clinical Distinctions Across Major Domains |
In addition to systemic toxicity, Multi-Drug Resistance (MDR) is one of the leading causes of failed treatment and cancer recurrence, which cause cancer-related deaths up to 90%.31 MDR in CRC is a multifactorial phenomenon and a complex phenomenon with both cell-intrinsic and tumor microenvironment (TME)-tied mechanisms.32 One of the significant cell-intrinsic processes is the up-regulation of ATP-binding cassettes (ABC) transporter proteins, including P-glycoprotein (P-gp/MDR1) and Breast Cancer Resistance Protein (BCRP).33 Such efflux pumps are actively engaged in ejection of a broad spectrum of chemotherapeutic agents out of the cancer cell, before they can reach their intracellular targets, radically reducing the concentration of effective drugs.33 Moreover, CRC cells may resist due to a change in drug metabolism (eg., increased inactivation of drugs by enzymes such as glutathione S-transferases), increase in DNA repair capability, and dys-regulation of apoptotic processes.31,32
Traditional surgical and radiation techniques also have unique constraints that do not allow the full elimination of the illness. Surgery is the primary method to get rid of CRC, but the minimal residual disease (MRD) in most cases complicates the use of surgery, and the risk of local or distant tumor recurrence, especially in intestinal obstructions.34 Also, radiotherapy which is used in most cases of rectal tumors is characterized by the occurrence of radio resistance in cancerous cells and the emergence of serious long-term repercussions on healthy tissues within the area that remains observable in the lives of the patients years after the administration of radiotherapy.35,36 Together, the high incidence, growing prevalence among the younger age groups, and the inheritable, unresolved shortcomings of traditional therapies, ie., systemic toxicity, lack of specificity, and deep-rooted multi-drug resistance, spawn a strong need to develop new, targeted therapeutic platforms. This is the critical gap that is being increasingly being bridged by the state-of-art nanomedicine, more so systems by which biocompatible natural polymers are used to deliver drugs precisely and specifically to the tumor site within the colorectum.
The Emergence of Nanomedicine in Cancer Therapy
The pitfalls of traditional cancer treatment, especially the problem of non-specific systemic toxicity and the widespread effect of multi-drug resistance (MDR), have inherently predetermined a rational change in strategy towards precision medicine.9,31 This is the urgent need that has led to nanomedicine taking the center stage in the study of oncology. Nanomedicine is a new, interdisciplinary specialty that utilizes the physical, chemical, and biological characteristics of nanoscale (1–100nm) materials to diagnose, monitor, prevent, and treat the disease.37,38 Nanomedicine, especially in cancer therapy, entails utilization of nanocarriers, which may be liposomes, polymeric nanoparticles, solid lipid nanoparticles, and inorganic nanoparticles, to deliver therapeutic agents.39 These nanosystems are designed to address the shortcomings of small-molecule drugs by modulating their pharmacokinetics and biodistribution, radically redesigning the interactions of anticancer drugs with the body and the tumor microenvironment (TME).8
The inherent benefit of nanomedicines is that they can be used to achieve high tumor selectivity based on two main concepts: passive and active targeting.40 Passive targeting takes advantage of a physiological process occurring in solid tumors, called the Enhanced Permeability and Retention (EPR) effect.41 Moreover, poor lymphatic drainage is common in the tumor tissue. Because of size, nanoparticles can easily extravasate (leak) out of the blood through these permeable abnormal vessels and thereafter, accumulate in the interstitial space of the tumor as a result of inefficient lymphatic clearance.42 The above mechanism inherently focuses the drug-loaded nanocarriers into the tumor site with minimal exposure to healthy organs directly to the site of systemic toxicity.43 This accumulation is further enhanced by the fact that the nanocarriers ensure that the encapsulated drug is not prematurely degraded and also increases the half-life of the accumulation in the bloodstream, giving the EPR effect a chance to take place.44
Besides passive accumulation, nanomedicines also allow complex active targeting by strategic surface functionalization. It entails conjugation of certain targeting ligands, including antibodies, peptides, aptamers, or small molecules onto the surface of the nanocarrier.45 These ligands are constructed to specifically target overexpressed receptors on the surface of colorectal cancer cells or the cells in the TME, including the folate receptor, epidermal growth factor receptor (EGFR) or integrins.46 Active targeting offers a second-level specificity to enable receptor-mediated endocytosis and allow the therapeutic payload to be internalized by the malignant cells themselves, which is especially important to overcome the heterogeneous nature of the EPR effect between tumors and stages.47 Moreover, the nano-formulation as such is a source of vital physicochemical benefits: it can elevate aqueous solubility of low-solubility chemotherapy agents (eg., paclitaxel or Curcumin) to a clinically viable level and can increase the stability of the drug - payload against enzyme degradation in the biological fluids.48 Stimuli-responsive nanocarriers that can release their cargo when exposed to specific TME conditions are also desirable - the reason why nanomedicine should be focused on Colorectal Cancer (CRC) treatment is overwhelmingly strong, and the solution to all the main therapeutic constraints of the disease is provided on a case-by-case basis.
Nanocarriers are uniquely designed to achieve high local concentrations of cytotoxic agents at the primary tumor and metastatic foci of disease, thereby increasing treatment efficacy and radically lowering the systemic side effects of the traditional chemotherapy regimen eg., FOLFOX or FOLFIRI.49,50 The distribution of the drug in the nanocarrier physically isolates the drug against action by ABC efflux pumps (eg., P-gp) until the entire nanoparticle is internalized through endocytosis, and the drug effectively avoids the efflux mechanism.31 More than the straightforward delivery of chemotherapy, complex nanomedicine enables the simultaneous co-delivery of synergistic payloads, eg., using a chemotherapy agent together with gene-silencing payload (eg., siRNA), to silence MDR-related genes and thereby re-sensitize cancer cells that have developed resistance to therapy.51,52 This also finds additional support in the possibilities of theranostic uses, in which the same nanocarrier can contain both a therapeutic agent as well as a diagnostic imaging agent (eg., a magnetic resonance imaging contrast agent), allowing real-time tracking of drug delivery and treatment response.53
Natural Polymers in Nanomedicine
The move to safer, more efficient nanocarriers has driven the interest in biologically derived materials, which are more generally referred to as natural polymers or biopolymers.54 Living organisms synthesize these macromolecules, which are mainly classified as Polysaccharides (eg., chitosan, alginate, hyaluronic acid, starch) and proteins (eg., gelatin, collagen).55 The clear superiority of biopolymers over synthetic materials is mainly attributed to the high biocompatibility and low toxicity.56 Their natural chemical analogy with the native biological entities guarantees positive contact with the cellular and host surroundings, reducing immunogenicity, systemic adverse effects, which go a long way to facilitate regulatory acceptance and clinical safety.57 This inherent safety profile is combined with a high level of biodegradability; natural enzymes and hydrolysis can readily convert them into harmless, easily excretable compounds, eliminating accumulation in the long term, which is the bane of non-degradable nanoparticles.58 Moreover, natural polymers have highly chemically active hydroxyl, amine, and carboxyl groups in their molecular structures, which offers an easy platform to functionalize.59 This chemical versatility is most important in conjugation of targeting ligands, which allows development of active-targeted and stimuli-responsive nanocarriers.
This review has a specific focus on natural-based polymer nanomedicines in the targeting of colon cancer (CRC). This specificity is strategically decided since the unique anatomical and physiological characteristics of the lower gastrointestinal tract, especially the high levels of microbial enzyme activity and the unique pH gradients in the colon, can be exploited spectacularly by some biopolymers. The polysaccharides such as pectin, guar gum and certain dextran derivatives are largely degraded by the abundant colonic microflora, providing an inbuilt system of localized, enzyme-mediated release of drugs only upon reaching the target site.60 Therefore, the purpose of the review is to analyse the engineering of these natural polymers in detail such as core-shell structures, mucoadhesive nanogels and hybrid conjugates to improve oral bioavailability, protect the drug payload through the upper GI tract, and release a concentrated therapeutic dose directly to the CRC lesion and its microenvironment.
Natural versus Synthetic Polymers: Comparative Advantages and Limitations
Natural polymers like chitosan, alginate, hyaluronic acid and pectin are well valued in colon cancer nanomedicine because of their natural biodegradability, biocompatibility, and biological functionality such as receptor affinity and microbiota-responsive degradation.61–64 Hyaluronic acid, for instance, is used to allow CD44 feasible targeting without the need for intensive chemical modification.65 Additionally, polysaccharide matrices can be selectively degraded by colonic bacterial enzymes, and this promotes colonic-specific drug release strategies.66 However, compared to synthetic polymers (eg., PLGA or PEG), natural polymers can exhibit structural heterogeneity, batch-to-batch variability, inferior mechanical robustness and less predictable degradation kinetics, all of which can impact reproducibility and long-term stability.67,68 Some positive aspects are that synthetic systems allow for precise control of molecular weight and tunable release properties, as well as scalable consistency for malabrication, but also often times additional functionalisation is needed to deliver similar bioactivity as could be found in natural polymers.69–71 Accordingly, in the present instance, the manuscript underscored how hybrid systems that consist of both natural and synthetic polymers could serve as an optimal balance of biological compatibility and tunable structure for translational nanomedicine for colon cancer.
Biological and Physiological Barriers for Colon Cancer Targeting
Delivery of therapeutic agents to the colon is extremely attractive in the management of colorectal cancer (CRC) to improve both therapeutic and reduce systemic toxicity, but it encounters many biological and physiological challenges, which require sophisticated drug delivery methods.72
The Gastrointestinal Tract (GIT) Environment
The passage through the upper GIT is the initial significant obstacle of orally taken drugs.73 Low pH in the stomach (pH 1.0–3.0) is immediately destructive to acid-sensitive drugs, particularly large biomolecules such as peptides and proteins, which become denatured and inactive.74 It is further destabilized by the enzymatic breakdown along the stomach and small intestine which is primarily catalyzed by proteins such as pepsin and pancreatic enzymes. Small intestine has a large surface area that is meant to absorb nutrients and, therefore, non-specifically uptakes drugs or breaks them down before the compound can reach the colon.75 The intestinal mucus barrier is a critical physical barrier that is a size-exclusion barrier, a dense and viscoelastic layer, the major component of which is composed of mucins that is a critical physical barrier, trapping and clearing large therapeutic agents and conventional drug carriers in large quantities and, therefore, severely restricting drug bioavailability.73,76 Moreover, the tight junctions between intestinal epithelial cells (IECs), which inhibit paracellular transport, and the lipophilic properties of the cell membranes, which inhibit passive diffusion of hydrophilic drugs, inhibit drug absorption.72 The short transit time in the small intestine (usually 3–4 hrs) also leaves a small-time frame in which drug release can occur and in most cases results in premature drug absorption or clearance.77
The Colonic Microenvironment
The colonic microenvironment provides special physiological conditions which can be used to target drugs with high localization, however, which also present new challenges.75 The most important feature is the presence of the gradient of the pH: the small intestine is about neutral (6.5–7.4) whereas the colon has a slightly lower or variable pH (6.0–7.0) because of the presence of fermentation products of bacteria.75,78 This is the main triggering shift in the controlled drug delivery system (CDDS), which makes use of the pH-responsive polymers, which will dissolve only when reaching the colon.79 The greatest concentration of the microflora in the whole GIT is in the colon with up to 1012 CFU/mL of the microflora.77 These bacteria have reductive and proteolytic enzymes, namely azoreductases and glycosidases (such as -galactosidase and -glucuronidase), which are practically absent in the upper GIT.75 To eliminate the active drug payload of prodrugs or polymeric coats, these enzymes are used to break the specific chemical bonds in the drugs and trigger the release of the drug payload only when the drug reaches the targeted colonic location.80 In addition to this enzymatic capacity, the microenvironment of colon cancer is highly endowed with distinct receptors/biomarkers, including those of folate uptake or unique tumor-associated antigens (TAAs), which can be exploited with functionalized nanocarriers.43 Other novel targets are the hyaluronan-rich extracellular matrix (ECM) which physically hinders the absorption of drugs into solid tumors and necessitates the co-delivery of agents such as hyaluronidase to degrade the hyaluronan.81
Tumor Microenvironment (TME) Barriers
Biological and physical barriers in the Tumor Microenvironment (TME) seriously limit the efficacy of nanomedicines in colon cancer, even when they have successfully traversed the gastrointestinal tract,82 the difference between the physiological and tumour microenvironment is presented in Figure 2. The most common physical barrier is the thick Extracellular Matrix (ECM), in the case of colorectal cancer (CRC), it is frequently highly enriched with such components as hyaluronan (HA) and collagen and creates a hard desmoplastic stroma.81,83 This ECM is thick, forming physical mesh which can limit the convection and diffusion of nanocarriers into the tumor core creating uneven distribution of the drugs and lowering the therapeutic concentration.43,72
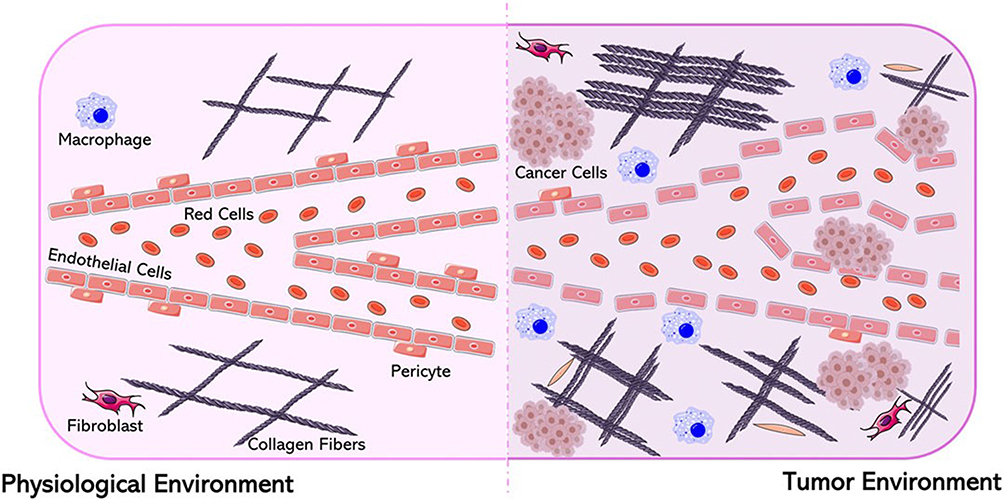 |
Figure 2 Difference between physiological and tumour micro-environment adapted from 84 under a Creative common license. |
 |
Figure 3 The schematic illustration of the natural polymers in biocompatible nanomedicines to deliver drugs into cancerous colon using targeted methods. The figure underlines the theme of employing different polysaccharides, proteins, peptides and chemically modified natural polymers to improve therapeutic targeting, circulation, mucosal adhesion and controlled release using effective treatment of colon cancer. |
 |
Figure 4 Schematic illustration of various targeting approaches (passive and active) to nanomedicine in drug delivery to the treatment of colon cancer. |
Moreover, the high rate of proliferation of the tumor, as well as the disorganized vascular structures, causes inadequate lymphatic drainage, which causes the Interstitial Fluid Pressure (IFP) to increase in the solid mass of the tumor.72,83 Such a high IPF causes the pressure gradient to the outside, which resists the convective delivery of nanomedicines across the bloodstream into the tumor tissue, which in effect pushes drugs away being repulsive to the cancer cells.43,85 Making things worse, there is poor and disorganized vascularization; the malformed blood vessels of the TME tend to be tortuous, structurally and functionally impaired and have lower blood flow rates. This hypoperfusion causes severe hypoxia (low oxygen levels) in large tumor areas that, in addition to conferring resistance to traditional chemotherapy and radiotherapy, restricts the number of nanocarriers to reach the tumor via the circulation as well as allows spreading of nanocarriers into the tumor area is limited by hypoxia.86 All these TME barriers contribute to the development of multidrug resistance (MDR), ie., restricted therapeutic penetration and facilitated efflux of internalised drugs, highlighting the importance of TME-responsive delivery systems that can break down the ECM or react to low pH and hypoxia to treat CRC effectively.
Despite being widely accepted for several decades as a cornerstone in passive tumour targeting, the EPR effect has been increasingly questioned with regard to its clinical relevance. Quantitative analyses show that on average, less than one percent of the administered nanoparticles dose is delivered to tumour tissue using preclinical models.87 Moreover, there is a noteworthy heterogeneity of the magnitude of the EPR effect, and significant attenuation in human tumours compared to murine xenograft models, which is largely due to differences in vascular architecture, stromal density, and the interstitial fluid pressure.88,89 Recent analyses highlight that nanoparticle tumour accumulation remains highly heterogeneous in human cancers, underscoring the need for delivery strategies beyond sole reliance on the EPR effect.90
Importantly, whilst ligand mediated active targeting can enhance cellular internalisation after nanoparticle extravasation into tumour tissue, there is no clear benefit on overall tumour accumulation at the systemic level.91,92 These observations suggest that active targeting does not preferentially increase intracellular delivery as compared to bypassing the constraints associated with vascular delivery. As such, the use of EPR alone may prove insufficient for effective clinical translation, especially in colorectal cancer given the heterogeneous tumour perfusion and stromal heterogeneity that relates to the pathway of nanoparticle distribution.
Natural Polymers Used in Biocompatible Nanomedicines
Nanomedicines that have been made from natural polymers are emerging as a significant approach in the management of colon cancer. Natural polymers offer a few advantages in drug delivery systems such as biocompatibility, biodegradability and their capacity to further differentiate malignant cells makes them a good choice in the treatment of colon cancer, as illustrated via Figure 3 and some examples are mentioned in Table 2. Polysaccharides are among other natural polymers making them especially appealing with their distinct structural and functional characteristics.
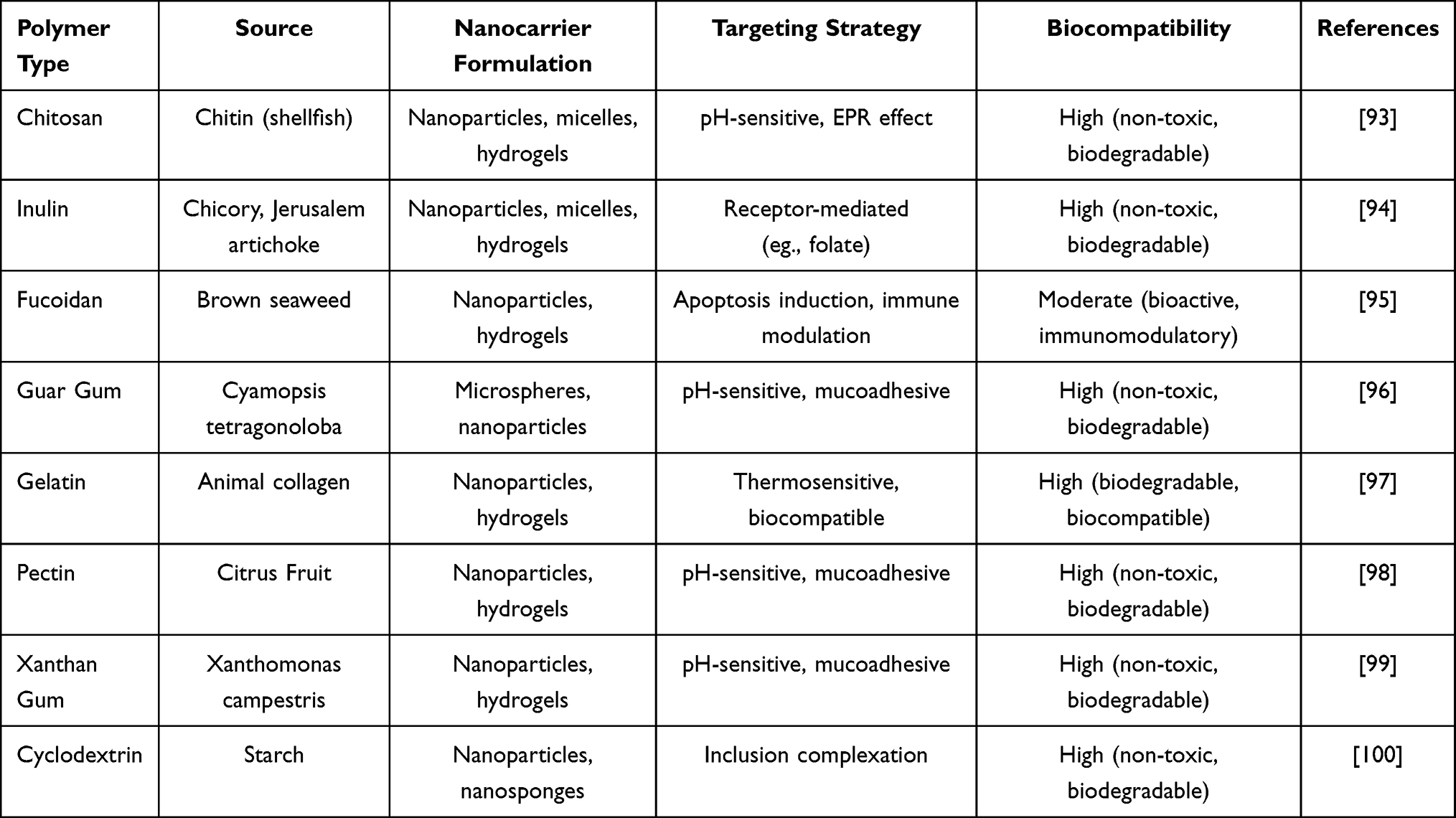 |
Table 2 Comprehensive Overview of Natural Polymer-Based Nanomedicines for Colon Cancer Targeting |
Polysaccharides
Chitosan
Chitosan is a polysaccharide of chitin, and it is one of the most commonly used natural polymers in drug delivery systems, especially the treatment of colon cancer. It has a positive charge, is pH sensitive, and mucoadhesive, which makes it extremely effective in targeting the colon. The positive charge helps the drug to interact with the negatively charged cell membranes and facilitate uptake by colon cancer cells.101,102 The mucoadhesive characteristic of chitosan helps the drug to remain in the target site longer, and the pH-sensitive characteristic enables the drug to release drugs according to the pH levels in the gastrointestinal tract especially in the colon where the pH is more alkaline.103 This is a controlled release system that improves the delivery of the drug to colon cancer cells, thereby improving therapeutic effects and reducing side effects on the body. It has been shown that nanoparticles prepared using chitosan are effective in improving oral absorption and colonic delivery of anticancer agents, thus chitosan-based nanoparticles have huge potential in the treatment of colon cancer.104
Alginate (AG)
Another significant substance in nanomedicine that is utilized in the treatment of colon cancer is alginate, which is a natural polysaccharide obtained by extracting it out of brown seaweed.105,106 Its ability to entrap divalent cations like calcium form gels makes it a very great material in preserving drug-packed nanoparticles against acid environment in the stomach. This characteristic enables the agents that are made of algae to release the drug specifically in the colon where gel is more favorable to form and release the drug.107 Alginate is biocompatible, thus making it even more attractive as a drug carrier of oral colon-targeted delivery systems.108 The use of alginate based nanocarriers to deliver anticancer drugs orally has been reported by several studies with promising outcomes in increasing the efficacy of the colon cancer treatments by providing a controlled, sustained release of the drugs in the colon.109,110
Pectin and Dextran
Natural polysaccharides such as pectin or dextran have been of interest in colon-targeted drug delivery systems because of their properties of being enzymatically degraded by the colonic microbiota.111,112 The site-specific release of drugs is best achieved with this form of degradation because they are enzyme-responsive in the colon, where they may disintegrate and release the therapeutic agents to the exact location of the tumor.113,114 An example is pectin which has been found to release drugs based on the enzymatic activity of pectinase which is an enzyme present in large amounts in the colon.113,115 On the same note, colon-specific release of dextran-based nanoparticles can be developed to increase the targeting and therapeutic efficacy of colon cancer treatment.116 Pectin and dextran are both promising agents in pacing the release of drugs, making them more precise and reducing the side effects associated with treating colon cancer.
Hyaluronic Acid
Hyaluronic acid (HA) is a naturally occurring glycosaminoglycan that is largely important in tumor biology particularly in the targeting of colon cancer. The cell surface glycoprotein binding HA, called CD44, is overexpressed in most cancerous cells, such as those in colon cancer.117,118 HA and CD44 interaction led to a range of cell responses, including cell migration, adhesion, and survival which are vital in cancer progression, and metastasis.119 This binding enables HA to serve as a good ligand to attack cancer cells because it can specifically bind to tumor cells that express CD44 and deliver drugs.
Recent research has drawn attention into the application of HA-functionalized nanoparticles as better ways of delivering and targeting anticancer drugs. HA-coated NPs are better targeted to colon cancer cells and therefore increase drug concentration at the tumour location with minimal systemic toxicity.120 HA-based nanocarriers are especially beneficial due to using the CD44 receptor overexpression of cancer cells to cause receptor-mediated endocytosis and the drug-delivery efficacy.121 Moreover, the capacity of HA to alter the tumor microenvironment and influence the extracellular matrix (ECM) has an extra therapeutic advantage because interplay between tumor cell and the surrounding matrix is essential in movement and metastasis of cancerous cells.122
Besides improving the delivery of drugs, HA-based NP can resolve challenges like multidrug resistance (MDR) in colon cancer. MDR is a major challenge to cancer treatment as it is the overexpression of efflux pumps that shrink drugs out of cancer cells. HA-coated NPs can avoid these pumps by attacking CD44, thus allowing the drug to be kept within the tumor cells and have its therapeutic effect.123 Consequently, HA-targeted nanomedicines form one of the potential ways of making the process of colon cancer treatment more efficient and resolving the issue of overcoming the difficulties of traditional chemotherapy.
Proteins and Peptides
Gelatin and Albumin
Two natural polymers that have been promising in the creation of biocompatible nanocarriers for treatment of colon cancer are albumin and gelatin. Gelatin is a collagen derivative which is especially useful because of its thermoresponsive behavior, large drug loading capacity, and biodegradation. Gelatin nanoparticles (GNPs) can encapsulate both hydrophilic and hydrophobic drugs so that they can have diverse therapeutic applications.124,125 The ability of loading large doses of anticancer drugs like paclitaxel and doxorubicin into GNPs increases the bioavailability and stability of the drug consequently increasing its effectiveness in fighting colon cancer cells.126,127
Equally so, another natural polymer which has attracted interest in nanomedicine is albumin, which is highly abundant plasma protein. Albumin nanoparticles (ANPs) have a number of advantages such as having the properties of being biocompatible, low immunogenicity and the capacity to entrap hydrophobic and hydrophilic drugs.128,129 Naturally, the tumor cells absorb albumin, as the permeability and retention (EPR) effect can be used to passively accumulate nanoparticles in the tumor microenvironment.130 The property is specifically useful in the targeting of solid tumors such as colon cancer whereby conventional chemotherapies are not always successful in attaining sufficient level of drugs at the location of the tumor. Also, the inherent capacity of albumin to bind certain receptors, including the albumin-binding receptor, can further target the drug delivery of therapeutic agents to cancer cells to further therapeutic results.131 Nanocarriers based on gelatin and albumin can provide an attractive platform on which targeted drug delivery systems can be developed to enhance the pharmacokinetics of the chemotherapeutic agent and to minimize the side effects of systemic drug delivery methods. They are natural and biocompatible that makes them the perfect choice in designing nanomedicines to enhance the cure of colon cancer.
Chemically Modified Natural Polymers
Natural polymers HA, gelatin and albumin have many benefits in drug delivery, but when it comes to nanomedical applications, they are frequently modified chemically to enhance their efficacy in treating colon cancer. PEGylation, which refers to the addition of polyethylene glycol (PEG) molecules to the polymer backbone, is one of the most widespread alterations. PEGylation enhances the stability, solubility and circulation of nanoparticles hence lowering their rapid clearance of the immune system and increasing their bioavailability.132,133 Such modification assists the nanoparticles to stay longer in the blood, and this is especially needed to enhance the concentration of drugs in the tumor tissues by the EPR effect.134
Thiolation is another modification that includes the inclusion of thiol groups to the polymer structure. Thiolated polymers are also better in mucoadhesive properties and therefore long-term retention of drug-loaded nanoparticles at the site of action, especially in the gastrointestinal tract which is important in treating colon cancer.135 Also, the nanocarrier stability of thiolation may be improved in the harsh microenvironment of tumor, which is often low pH, high enzyme conditions.136 It is also established that thiolated polymers enhance the efficiency of cellular uptake, which occurs by interacting with cell surface receptors, and may further increase drug delivery specificity to colon cancer cells.137
Moreover, natural polymers can be crosslinked or grafted with other materials like peptides or other functional groups that may be of great significance to the targeting ability and the drug release profile of the nanocarriers. As an example, it is possible to graft HA onto the nanoparticles to increase the specificity of the carriers on the CD44-positive cancer cells, whereas the pH-sensitive groups can be grafted to release the drugs in the acidic tumors on demand.138 These modifications assist in addressing certain limitations of natural polymers, including their rather fast clearance and inadequate targeting capabilities.
Design Strategies for Targeted Colon Cancer Nanomedicines
Passive Targeting Mechanisms
In passive targeting, the abnormal attributes of tumor vessel, namely the vessels being dilated and leaky because of the high and disorganized angiogenesis, are used,139 the features are mentioned in flow chart via Figure 4. This creates gaps among the endothelial cells in the blood vessels whose diameter varies between 100 nm and 1 µm through which the nanoparticles can extravasate passively into the tumor interstitium.140 The presence of these large gaps in the vasculature is not common in normal vasculature, and it gives the nanoparticles a selective route of accumulating in tumor tissues. Moreover, tumors in most cases have poor lymphatic drainage, thus, making it hard to remove nanoparticles in the tumor site effectively. This causes the nanoparticles to remain in the tumor thereby increasing the exposure of the drug to the cancer cells.141
Nanoparticles’ size and characteristics determine how to passive target. Nanoparticles between 10 and 200 nm are the best since they are large enough to build up in the tumor via the leaky vasculature yet small enough not to be cleared out by the renal system too quickly.142 The nanoparticles can be modified on their surface which can inhibit their rapid recognition and clearance by the immune system and improve their circulation time and ability to concentrate at the tumor site.143 PEGylation is now an established method of nanoparticle-based passive targeting, which has greatly enhanced the pharmacokinetics of nanoparticles.144
Passive targeting techniques are used in colon cancer exploiting the EPR effect, which also increases the uptake of chemotherapeutic agents by tumors. Taking advantage of the EPR effect, nanoparticles have the potential to preferentially target colon cancer tissues, further enhancing the delivery of drugs to the tumor with reduced systemic toxicity.145 This has been applied to several types of nanoparticles such as liposomes, polymeric nanoparticles and mesoporous silica nanoparticles that have garnered preclinical and clinical trial successes in the treatment of colon cancer.43,146,147
Active Targeting
Ligand-modified nanoparticles have selective accumulation at tumour sites by ligand -receptor interactions, thus enabling targeted delivery of therapeutic agents; the nature of these interactions is modelled in Figure 4. These nanostructures are normally termed as actively targeting nanoparticles.148 Cancer cells often overexpress certain receptors and release biomolecules that stimulate the growth of tumorous and surrounding tissues, often through paracrine or autocrine signalling pathways.149 There are two major methods of conjugating ligands to nanoparticles, one is a chemical functionalisation of nanoparticles in the synthesis step and the other is a ligand conjugation to polymers before nanoparticles are produced.150,151 Passive accumulation in tumour tissue can also be realised using ligand-modified nanoparticles and then these particles can be internalised by cancer cells through active targeting, which increases the specificity and therapeutic efficacy of the intervention.
In the last three years, nanodrug delivery systems against colorectal cancer have been developed with the primary emphasis on receptor-ligand binding approaches with the use of receptors that are highly expressed in colorectal cancer, including the folate receptor,152 epidermal growth factor receptor (EGFR),153 CD44, epithelial cell adhesion molecule (EpCAM),154 nucleolin,155 hyaluronic acid receptor,61 and many more. Among these, nanoparticles targeting EpCAM, folate receptor, EGFR, and CD44 have been the subject of extensive research. For instance, to enhance CRC targeting following systemic administration, DNA aptamers specific to EpCAM (eg., SYL3C), which exhibit a strong affinity for EpCAM proteins on cancer cells, have been conjugated to nanoparticles. To minimize drug toxicity and improve therapeutic outcomes, Ge et al154 synthesized biological conjugates loaded with celastrol, which were effectively captured by CRC cells overexpressing EpCAM. These conjugates consisted of EpCAM aptamers, polyethylene glycol (PEG), and dendrimers, resulting in extensive apoptosis in SW620 cells upon exposure. Moreover, in both xenograft mouse and zebrafish models, the biological conjugates demonstrated low toxicity. The dendrimer component of the study, composed of biocompatible materials, also exhibited a multivalent effect, thereby enhancing the safety profile of the chemotherapeutic drugs.154
In another study, miR-139-5p was delivered to colorectal carcinoma (CRC) cells using cationic liposomes. The liposomal preparation was a mixture of HSPC, DOTAP, Chol, and DSPEPEG2000COOH lipids. The nanoparticle surface was functionalised with an EpCAM aptamer to provide colorectal-specific targeting. The resultant construct exhibited a high level of inhibitory action against HCT cells and in vivo pharmacodynamic evaluation of murine models showed a strong inhibitory effect of tumor growth in CRC mice inoculated with HCT8 cells subcutaneously.156
Along with targets that are distinctly specific to CRC, several antigens that are commonly overexpressed in other neoplasma are also expressed in colorectal carcinoma and can therefore be utilized to deliver nanotherapeutic agents with specificity. Folate receptor is a membrane-bound glycoprotein that is typically absent or lowly expressed in normal tissues but highly up-regulated in a range of malignant cells, such as CRC.148 It, therefore, forms a logical object of therapeutic exploitation. Self-assembled nanoparticles based on biocompatible and biodegradable biopolymers, such as chitosan and chondroitin sulfate, have been used to entrap the hydrophobic proteasome inhibitor bortezomib. These particles were modified on the surface to obtain active folate receptor targeting. Soe et al152 conjugated folate to DSPEPEG which was then conjugated to the nanoparticles. This adjustment did not only increase the stability of the particles and the efficiency of drug loading but also promoted prolonged systemic circulation. The nanomedicines showed strong antitumour effects in animal models with little toxicity to non-tumour tissues.152
Design Strategies for Targeted Colon Cancer Nanomedicines
While nanoparticle size has been widely acknowledged as being a critical determinant of passive tumour accumulation, exclusive consideration of average particle diameter can present a confusing picture of the challenges of translating nanoparticle technology from bench to bedside because of size polydispersity. Polymeric nanoparticle preparations, especially those from natural polymers like chitosan, alginate, or gelatin, often have a measurable size distribution instead of monodisperse population. Consequently, the polydispersity index (PDI) has a direct influence on circulation half-life, biodistribution and clearance kinetics.157–159
Smaller hence nanoparticle fractions (<50nm) are susceptible to rapid renal clearance and thus reduce effective exposure to tumour, while larger fractions (>200nm) are more vulnerable to the mononuclear phagocyte system (MPS) – particularly in the liver and spleen.87,160 In contrast, heterogeneous size distributions may lead to divergent biological behaviour within a single formulation of the therapeutic element and hence inconsistent tumour accumulation profiles and variable therapeutic outcomes. Importantly, tumour extravasation is very size sensitive, and nanoparticles ranging in diameter of ca. 50–150 nm tend to show an optimal balance between prolonged circulation and effective tumour penetration, with broader size distributions lowering the predictability of EPR-mediated localisation.87,161–163 Moreover, advanced nanoparticle engineering increasingly focuses on precise control of physicochemical properties and structural uniformity to improve translational performance.164
Aside from biological performance, size polydispersity poses challenges in both manufacturing and regulatory perspectives. Batch-to-batch variation in polymer crosslinking, kinetics, and the solvent diffusion rates can cause a shift in size distribution profiles, affecting the reproducibility and scalability of the natural polymers nanoparticles systems.165 In addition, small changes in PDI can affect the dynamics of protein corona formation, which influences clearance behaviour and tumour-targeting efficiency.166 Accordingly, optimisation of the natural-polymer nanoparticle synthesis should be prioritised not only for the desired mean size but also for tight control on the size distribution (PDI <0.2 where possible and scalable fabrication protocols, robust physicochemical characterisation). Addressing heterogeneity in size at the formulation stage is vital to achieving predictable pharmacokinetics, reproducible tumour accumulation and successful clinical translation of nanotherapies. Moreover, pH-responsive drug delivery systems take advantage of small but biologically relevant pH-gradients, which occur along the gastrointestinal tract and in the tumour microenvironment. In colorectal cancer, luminal pH goes from very acidic in the stomach (pH (1–3)) to almost neutral in the colon (pH (6–7)), whereas tumour extracellular pH is generally slightly acidic (pH (6.5–6.8)) compared to normal tissue.167,168
Natural polymer-based systems are based on several molecular mechanisms for pH-responsive release. Polymers that contain ionisable functional groups, eg., carrier containing carboxyl or amine group, undergo protonation/deprotonation due to the local pH value, leading to electrostatic repulsion, the relaxation of polymer chains and the swelling of the polymer matrix allows the drug to diffuse faster.169,170 For example, chitosan can become protonated under acidic conditions affecting its solubility and permeability behaviour, while alginate exhibits pH dependent swelling and dissolution behaviour under near neutral colonic conditions.171,172 Acid-labile linkages, such as hydrazone bonds, acetal or Schiff base bonds can be introduced between the polymer backbone and the therapeutic payload. These covalent bonds are stable at physiological pH but are cleaved in slightly acidic tumour conditions to allow for controlled and selective intracellular drug-release.173,174
Mechanistic Pathways of Natural Polymer Nanocarriers Overcoming Biological Barriers
Natural polymer based nanocarriers for colon specific drug delivery natural polymer based nanocarriers exploit their inherent physicochemical characteristics to pass through hostile gastrointestinal milieu and the dense TME for colon specific drug delivery. Different therapeutic agents are susceptible to degradation within the acidic gastric compartment, nevertheless, polymeric carriers such as chitosan and alginate provide protective matrices which enhance the stability of the drug.175 The pH responsive behaviour of chitosan allows its integrity to be preserved in the presence of acidity in the stomach, to swell up or dissolve only under the high pH typically found in the intestine and colon, preventing premature drug release and/or degradation by the proteins of gastric proteases.176,177 Similarly, Alginate, a pH responsive polysaccharide, forms ionically crosslinked gels that resist acidic degradation and undergo controlled swelling with a rise in pH to induce controlled drug release at the desired site.178–180
Enzymatic catabolism is another challenge to be overcome since the degradation of sensitive therapeutic compounds by proteolytic and pancreatic enzymes in the upper gastrointestinal tract may occur. Polysaccharides such as pectin and dextran are designed to resist hydrolysis in the gastric and jejunal portions but are selectively hydrolyzed by gut-releasing enzymes by the gut microbiota in the colon. Consequently, the enzymatic degradation of these polymers in the colonic environment causes the release of the drug payload only at the target site and therefore increases the site specificity and reduces the systemic adverse effects.181,182
The thick layer of mucus on the intestinal epithelium forms a strong barrier to drug permeation and absorption. Natural polymers often have inherent mucoadhesive properties which allow nanocarriers to bind to mucus, prolonging the time of residence at the site of action and enhancing local drug absorption. Notably, chitosan, due to its cationic nature, electrostatically interacts with the anionic components of mucus, namely mucins, to promote an adhesion, and promotes the sustained release of drugs.104,183 In addition, techniques of surface engineering, like grafting of hydrophilic polymers, can attenuate unspecific mucoadhesion and deeper diffusion through the mucus network.184,185
Once it reaches the colon, more challenges are encountered in the tumoral microenvironment. The extracellular matrix of colorectal neoplasms is often enriched with hyaluronan and collagen and provide a compact stroma which limits nanoparticle infiltration into the neoplasm. Nanocarriers assembled from HA take advantage of overexpression of CD44 receptors on colon carcinoma cells which promote receptor mediated endocytosis with enhancing tumour specificity. HA functionalisation has the added benefit of facilitating deeper tumoral penetration through interaction with the constituents of the ECM and transient matrix modulation for improved delivery efficacy.186,187 Moreover, hybrid systems that combine chitosan with HA have shown synergistic effect in colon targeting by combining pH responsiveness and receptor-mediated uptake and thus improve treatment.188
Coordinated Multi-Component Integration in Natural Polymer Matrices
Recent developments in the field of natural polymer-based nanomedicine have helped to co-encapsulate the chemotherapeutic agents, imaging modalities and gene - regulatory payloads in a single multifunctional platform. Nevertheless, the successful transfer of such systems to clinical use requires more than simple co-encapsulation; more than that, it requires that the polymeric matrix has structural integrity and biological activity and orchestrates a temporally controlled release of therapeutics.
Natural polymers such as chitosan, HA, alginate and gelatin form hierarchical structural networks, which can segregate multiple functional agents. Possessing directly cross linked ionic and cross conjugated spherically discrete microdomains by utilizing hydrogen bonding strategies of an ionic cross-linking polymer and covalent conjugation strategies of a covalent cross-linking polymer, these matrices prevent premature interactions between sensitive payloads like nucleic acids and small molecule chemotherapeutics.189–191 Furthermore, stimuli-responsive polymeric nanosystems integrating therapeutic and diagnostic elements have emerged as promising precision platforms.192
Stimuli-responsible linkers built in the natural polymer frameworks enable the sequential or environment-trigger release of the therapeutic constituents. For example, pH-sensitive or enzyme cleavable linkages are used to allow the delivery of chemotherapeutics in the acidic environment of tumours while protecting siRNA or miRNA constructs from exposure until they are taken up into cells.193,194 In addition, hyaluronic acid-based matrices exhibit receptor-mediated endocytosis by targeting CD44 to deliver the coordinated intracellular trafficking of both imaging and therapeutic modules without compromising the functional integrity of gene-regulatory elements.176,195 The preservation of biological activity is of particular importance in the case of nucleic acids and imaging probes. Natural polymers offer soft fabrication conditions which reduce the risk of denaturation compared to synthetic polymer systems. Apart from this, electrostatic complexation within nanostructures built on Chitosan is shown to stabilize RNA payloads against enzymatic degradation until they are released into the cytosol.196,197 Consequently, multifunctional carrier natural polymer matrices possess not only a carrier function but also the capability of acting as dynamic structural frameworks that include spatial isolation, stimuli triggered activation, and synchronized payload release.
Optimizing Mucoadhesion–Penetration Balance in Natural Polymer Nanocarriers
The strong mucoadhesive properties of natural polymers may lead to an extension in the residence time at the mucosal surfaces and thus enhance the local drug retention, however too high adhesion may hinder deeper diffusion through the tumour-associated mucous and stromal barriers. Mucoadhesion is the outcome of specific polymer-mucin interactions, such as hydrogen bonding and electrostatic forces, which can improve carrier residence but may adversely affect nanoparticle mobility within thick mucus layers, which in turn limit the access to underlying tumour tissues.198,199 Chitosan is one of the most widely used natural polymers, with intrinsic mucoadhesive behaviour due to its positive charge, which allows for the interaction with mucins with a negative charge, but can also increase the sequestration if not optimised.104,200
For example, in order to improve this inherent trade-off, rational design strategies are focused on modulating polymer composition, hydration kinetics and surface chemistry. Reducing excessive surface charge density or mixing with neutral polymers can reduce mucin binding that would otherwise be too strong while retaining a level of adhesion that results in controlled release. Surface engineering techniques include the partial protection with hydrophilic layers or with motifs that can be infiltrated by mucus, which can interact with the mucus transiently and then with tumour tissue, ie., they diffuse deeper.199 Moreover, adjusting the hydration behaviour by a controlled cross-linking and controlled network density can be used to avoid overly dense gel layers hindering the transport, not to mention that regulated swelling promotes the gradual relaxation of polymers and favours the penetration of viscous mucus structures.198 Emerging dual functional strategies combine both mucoadhesive and mucopenetrating components into one formulation to balance the state of retention as well as mobility. By adding mucolytic constituents or surface ligands that limit the interaction between irreversible mucin and these systems, enhanced mucosal contact without compromising deeper tumour accessibility is achieved.199
Intelligent Tumour Microenvironment-Responsive Natural Polymer Nanocarriers
The colorectal tumour microenvironment is characterised by a compact and rigid ECM, high interstitial fluid pressure (IFP), abnormal vasculature and areas of profound hypoxia, all of which are associated with metastasis and invasion.23 These features are not independent, but are mechanistically interlinked, and this collectively limits the penetration of nanocars carrying drugs and the nanocarrier uniform drug distribution. Rational engineering of natural polymer-based nanomedicines is increasingly directed towards such pathological cues used as triggering activation rather than only being a barrier.
Stiff ECMs with natural polymer collagen and hyaluronan limit convective transport and diffusion. Natural polymer nanocarriers can be engineered with enzyme-responsible breakdown connections, for example, matrix metalloproteinase (MMP)-degradable peptides or hyaluronidase-sensitive components to make it possible for selective matrix reconfiguration when they reach tumour tissue. Such strategies allow controlled structural loosening and better intratumoral penetration while maintaining systemic stability.201,202
Increased interstitial pressure also acts to restrict the inward diffusion flow and promote peripheral accumulation of nanoparticles. Stress-responsive polymer networks with mechano-adaptive deformation have manifested potential in modulating release profiles in compressive forces as too characteristic of solid tumours. Hydrogels and cross-linked polysaccharide systems in which structural relaxation is controlled through mechanical stressing can be used to facilitate better deeper penetration and longer-lasting release.203–205
A further exploitable trigger is hypoxia, which is characteristic of a far-advanced colorectal tumour. Hypoxia responsive moieties such as azobenzene linkers, nitroimidazole derivatives and reductively cleavable bonds can be incorporated into natural polymer matrices. When starved of oxygen, these linkers become bioreduced, destabilising the formation of the nanostructure and releasing the drug in a localised manner, specifically in hypoxic tumour cores.206–208 Importantly, by incorporating several tumour-responsive elements into the same natural polymer matrix, it is possible to achieve hierarchical modes of activation, with ECM-sensitive degradation aiding penetration with subsequent hypoxia-triggered release inside the tumour core. Such multitargeted systems increase the therapeutic specificity with minimum premature systemic release. Therefore, natural polymer nanocarriers can be conceptualised not simply as passive delivery systems but as intelligent biomaterials that can dynamically respond to the heterogeneity of the tumour microenvironment, in terms of mechanical, enzymatic and metabolic heterogeneity.
Microbiota-Triggered Release: Managing Inter-Patient Variability
Polysaccharide-based colon delivery systems that are based on commensal bacterial degradation (eg., pectin, dextran, inulin or azobond linkers) are attractive as they can be relatively stable in the proximal gastrointestinal tract and to be cleaved in the colon. This strategy, though, relies inherently on the capacity of the microbes involved, which will vary substantially across individuals because of diet, age, disease state, antibiotic exposure and other host related factors.112,209 Inter- patient variations in the abundance and activity of bacterial enzymes involved in colonic activation including glycosidases, azoreductases and beta glucuronidase-related activities may thus be translated into clinically meaningful changes in polymer degradation and drug release timing. These shifts can be either delayed or inadequate liberation resulting in the risk of under exposure or premature cleavage resulting in the risk of premature release with altered profiles of local concentrations.210,211
Importantly, although taxonomic compositions can differ, in many gut communities there is functional redundancy, in that similar metabolic capabilities may be preserved although any taxa producing them may differ. However, functional production is not uniform across patients and dysbiosis may affect or redirect important enzymatic activities relevant in microbiota triggered delivery.212,213
To increase translational robustness, microbiota-based polysaccharide systems can be designed with attributes that minimize the need for a single patient-specific microbial step. Practical strategies involve integrating microbiota sensitivity with an added independent trigger, such as pH responsive outer coatings or time controlled matrices, to guarantee colon localisation even when decomposition of the polymer is not as fast as expected; to prioritise polymer chemstries that rely on cleavage by broadly distributed enzymatic functions; and to control cross linkage density, substitution pattern and layer thickness to increase the “activation window” and avoid sharp dependence on a particular microbiome state.112,214 From the translation perspective, ex vivo fecal fermentation or enzyme-activity assays can be incorporated into the development process to help quantify variability in release kinetics and serve as a guide to formulate parameter ranges that can be used to ensure a maintenance of efficacy across patient populations.
Molecular and Microbiome Signatures for Patient-Tailored Nanomedicine Design
Beyond the conventional ligand-receptor targeting, tumour-specific molecular and microbiome signatures are a tantalizing way forward for personalization of polymer-based formulations. The integration of patient-derived multi-omics (ie., genomics, transcriptomics, proteomics and metabolomics) data sets enables the determination of idiosyncratic expression patterns, such as receptor over-protection, tumour subtypes, metabolic dependencies and immune modulators. The resultant molecular atlas can be used to inform the optimisation of both targeting ligands and stimuli-responsive chemistries that have the greatest potential of being suited to an individual patient’s tumour, thereby augmenting specificity and clinical efficacy.215
Contemporary frameworks encourage the use of machine - learning approaches in tumour -omics profiles, which have made it possible to transfer heterogeneous biological aspects into quantitative design rules for nanocarrier optimisation. These rules include using a smart choice of ligand, composition of polymer and release triggers calibrated to the biochemistry of individual tumours. Empirical evidence has shown that such data-driven design enhances the performance of nanomedicine in patient-derived organoid models that can be seen as a paradigm shift from empirical approaches to precision nanotherapeutic design.
Simultaneously, the tumour-associated microbiome has emerged as a key player in colorectal cancer progression and responsive therapy. Specific microbial communities are associated with different tumour subtypes, tumour stages and immune phenotypes with influence on drug metabolism, immune activity and local inflammation (Long et al manage Theoretical Bayes CC, 2024). Intratumoural microbiota can affect epithelial signalling pathways, influence the state of the immune microenvironment and induce therapeutic resistance mechanisms, therefore requiring the design of nanocarriers that can either make use of or counter-act specific microbial interactions for improved clinical outcomes.
Personalised nanomedicine strategies additionally recognize receptor heterogeneity haunting traditional paradigms of targets. Tumours with unique expression profiles for integrins, growth factor receptors, immune checkpoints or stemness markers can be paired with polymers functionalised with ligands with the capacity to preferentially bind these markers and enhance cellular uptake and delivery of a therapeutic payload. Recent investigations show that the combination of molecular profiling and targeted design of nanocarriers will improve tumour selectivity and potentially overcome the problem of resistance due to receptor variability.
Isoform-Specific CD44 Targeting in HA-Based Nanomedicines
CD44 is not a homogeneous receptor, but rather a family of alternatively spliced receptors including the standard form (CD44s) and several variant forms (CD44v) including CD44v3 and CD44v6. The above-mentioned variants show structural disparities within their extracellular domains and are implicated in various biological processes which influence colorectal cancer development, metastasis, and regulation of stemness.216,217 Importantly, several CD44 variant isoforms, and in particular CD44v6, have been found to strongly correlate with aggressive tumour phenotypes and enhanced metastatic potential in colorectal cancer.218,219
Hyaluronic acid-based nanomedicines take advantage mainly of the conserved hyaluronan-binding domain found among the CD44 isoforms that permit receptor-mediated uptake in tumour cells that express larger numbers of CD44 receptors. However, this approach fails to distinguish between the standard and variant isoforms, although there is a growing body of evidence suggesting that CD44 variants exhibit distinct clustering behaviour, co-receptor interactions and downstream signalling properties that may affect nanoparticle internalisation as well as intracellular trafficking.218,220
Given the heterogeneous expression of CD44 variants across tumour subtypes and within tumour microenvironments, incorporating isoform-aware targeting strategies may significantly enhance precision. Potential approaches include combining HA with isoform-specific antibodies or peptide ligands targeting CD44v6-enriched tumour populations, thereby improving selectivity toward invasive or stem-like cancer cell subsets while reducing off-target interactions.221,222 Such refinement moves HA-based systems beyond general receptor targeting toward tumour isoform-specific precision medicine, improving translational relevance in heterogeneous colorectal cancers.
Natural Polymer Nanomedicine Formulations for Colon Cancer
Polymeric Nanoparticles
To achieve the best therapeutic effects in colorectal cancer (CRC), nanoparticle engineering must be advanced significantly. This advancement requires accurate control of the size, morphology and surface ligands of nanoparticles, which are central to improving drug delivery systems. Close assessment of synthesis guidelines is essential to produce the desired nanostructures, along with the rational choice of polymers to produce nanocarriers, covalent coupling methods, and targeting ligands.223,224 Moreover, polymeric systems provide significant flexibility in customization and optimization of nanoparticles to enable effective drug delivery, which is a requirement to translate these technologies into clinical practice; examples are given in Table 3. However, due to the large number of parameters that can be adjusted, strategic and thought-over design of nanoparticle systems is essential to achieve the required therapeutic effects.225
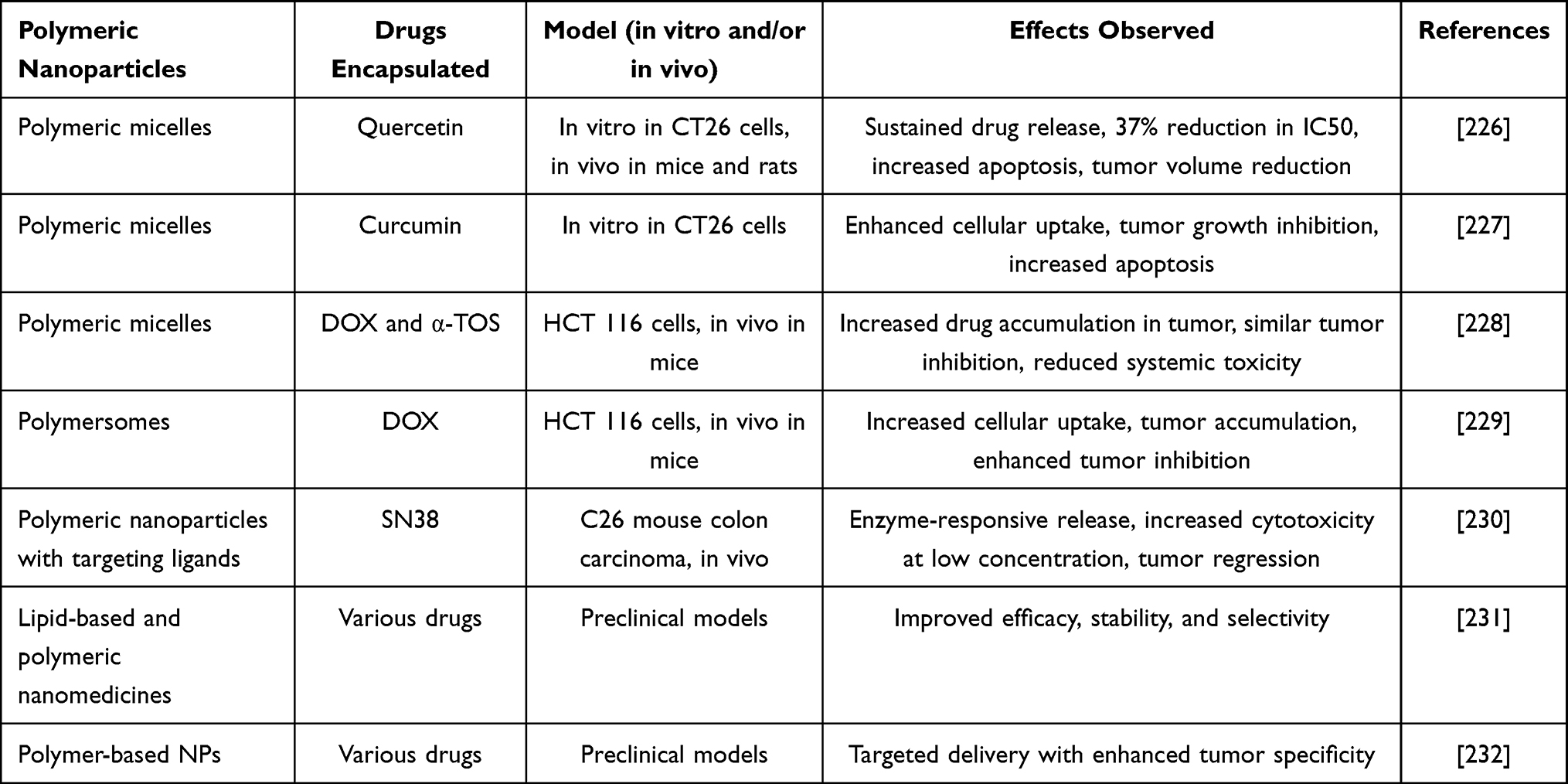 |
Table 3 Polymeric Nanoparticle for Colon Cancer Therapy |
Polymeric nanoparticles are usually solid in shape, in the form of a sphere, which is formed by self-assembly. Nanospheres and nanocapsules are two major subclasses that are formed through different mechanistic routes. The active agents are uniformly distributed in the polymeric structure of nanospheres, but in nanocapsules the drug is encased in a core that is surrounded by a single polymeric membrane.233 Polymeric nanoparticles of different kinds have been investigated in the treatment of CRC. As an example, Shashank Tummala et al designed a 5-fluorouracil (5-FU) enteric-coated polymeric nanoparticle that targets the colon and maintains the concentration of the drug in the tumour tissues, significantly shrinking the size of the tumour compared to the unencapsulated 5-FU controls.234
Polymeric nanoparticles of different kinds have been investigated in the treatment of colorectal cancer (CRC). As an example, Shashank Tummala et al designed a 5-fluorouracil (5-FU) enteric-coated polymeric nanoparticle that targets the colon and maintains the concentration of the drug in the tumour tissues, significantly shrinking the size of the tumour compared to the unencapsulated 5-FU controls.235 In the case of CRC management, Yishan Chen et al prepared a monomethyl poly(ethylene glycol) poly(epsilon-caprolactone) (MPEG-PCL) copolymer to encapsulate fisetin in a self-assembled micelle with an average diameter of 22 +3nm. Compared to unencapsulated fisetin, the micellar formulation had sustained and prolonged release in vitro, increased cytotoxicity and cellular uptake. In vivo studies demonstrated that there were a major tumour-growth inhibition and prolonged survival in the CT26 tumour model.236
Shin-Yu Lee et al utilized cationic PDMA-block-poly(ε-caprolactone) (PDMA-b-PCL) micelles to load SN-38, ultra-small superparamagnetic iron oxide (USPIO) nanoparticles, and small interfering RNA (siRNA) to create a multifunctional micellar drug delivery system. Their results demonstrated that SN-38/USPIO-loaded siRNA–PEG mixed micelles could passively target tumor sites, suppress VEGF action, and simultaneously deliver chemotherapy. This multi-dose therapy significantly reduced tumor growth.237
Polymersomes, another class of self-assembled polymer vesicles, are also employed for encapsulating and protecting sensitive molecules such as drugs, enzymes, and nucleic acids. Although similar in structure to liposomes, polymersomes exhibit enhanced stability and higher loading efficiency.238,239 Matthew A. Petersen et al developed PR_b-functionalized, bioresorbable polymersomes for the targeted delivery of cisplatin to human colon cancer cells. PR_b is a peptide targeting the a5b1 integrin, which is overexpressed on human colon cancer cells. Their findings demonstrated that this delivery system minimized side effects, extended circulation time, and improved the survival of mice. These advanced nanostructures exhibit tremendous potential for improving the therapeutic efficacy of CRC treatments, thus opening new avenues for cancer therapy.240
Other Drugs for Colon Therapy
5-Fluorouracil (5-FU) is widely utilized in the treatment of breast, colorectal, gastric, and pancreatic cancers. Although 5-FU activates multiple pathways, its primary mechanism of action involves inhibition of thymidylate synthase (TS), a critical enzyme in DNA synthesis, thereby limiting excessive DNA proliferation. Nonetheless, the combination of 5-FU with folinic acid has demonstrated improved therapeutic outcomes in colon cancer, as folinic acid enhances the effect of 5-FU by further inhibiting thymidylate synthase. Capecitabine, an oral prodrug of 5-FU, is metabolized in vivo to release the active drug. This compound increases the bioavailability of 5-FU and inhibits the synthesis of thymidine monophosphate, which is essential for de novo DNA synthesis. Numerous studies have demonstrated that capecitabine induces a higher tumor response rate compared to intravenous 5-FU. Furthermore, capecitabine has a more favorable side-effect profile and improved tolerability, offering significant clinical benefits over 5-FU.241 Oxaliplatin is a third-generation platinum analogue that differs with cisplatin and carboplatin by having a 1, 2-diaminocyclohexane ligand instead of two monodentate amine ligands. Irinotecan, a semi-synthetic analogue of camptothecin, is a topoisomerase I inhibitor, which hinders the replication of DNA and reduces the stress of superhelix. Its active metabolite, 7-ethyl-10-hydroxy-camptothecin (SN −38), is approximately a thousand times more cytotoxic than irinotecan. Even though the bioconversion of orally or intravenously administered irinotecan in humans is only 2–8% into SN-38, the drug is still an important chemotherapeutic, especially when used in optimized vehicle preparations.242 Cyclooxygenase-2 selective, non-steroidal anti-inflammatory agent (celecoxib) has shown a strong antineoplastic effect in preclinical models. The drug regulates key genes and signalling pathways involved in tumour-related inflammation, thus suppressing the development of colonic polyp. However, its use in clinical practice is limited by severe adverse events, including hypersensitivity reactions, cardiovascular events, including myocardial infarction and cerebrovascular accident, and high plasma clearance, which all reduces its clinical efficacy.243
Prospects and Future Directions
The prospects for natural polymer-based biocompatible nanomedicines in targeting colon cancer are highly promising, driven by advancements in nanotechnology and a growing understanding of tumor biology. Natural polymers eg., chitosan, alginate, dextran and hyaluronic acid have inherent biocompatibility, biodegradability and low toxicity which make them the best carriers of colon cancer therapeutics. The ability to functionalise these polymers with targeting ligands enables specific accumulation of drug-laden nanoparticles in tumour locations thereby increasing therapeutic effect whilst reducing systemic side effects. Future directions in this area are concerned with the development of multifunctional nanomedicines, which combine diagnostic and therapeutic properties, and hence allow real-time monitoring of therapeutic response. Stimuli-responsive natural polymer nanocarriers can be used to control and release drugs site-specifically through innovations in stimulus-responsive nanoparticles based on changes in pH, enzymatic activity, or redox conditions within the tumour microenvironment. The use of colon cancer specific biomarkers and active targeting receptors is expected to further improve the precision of delivery. Combining natural polymer nanomedicines with novel immunotherapeutic approaches has significant potential in overcoming tumour immune evasion and improving clinical outcomes. Also, the personalised nanomedicine plans, which will depend on individual tumour genotypes and microenvironmental features, will help streamline therapeutic regimens. However, there are still several issues, such as the mass reproducible production of these nanomaterials, their stability, and regulatory approval. To enhance the speed of translating these technologies into clinical practice, comprehensive preclinical studies based on advanced patient-derived models are needed. Interdisciplinary teams involving materials scientists, oncologists, and the pharmaceutical industry are essential to the promotion of innovation and a faster process of creating safe and effective polymer-based nanomedicines. In conclusion, natural polymer chemistry, nanotechnology, and tumour biology convergence offer strong prospects of transforming colon cancer treatment using safer, more targeted and highly effective nanomedicine platforms. Further interdisciplinary studies and stringent clinical validation are essential in order to realise the clinical potential of these biocompatible nanotherapeutics to the fullest.
Challenges and Clinical Translation
The translation of nanoparticles into clinical practice is highly successful because of the efficacy of nanoparticles that has been observed in preclinical models of CRC. Nevertheless, nano-drug delivery systems have several problems that persist in their development. The most difficult task is associated with the mass production of nanoparticle formulations and stringent testing of their preclinical safety and effectiveness. Currently, nanoplatforms, which are to be used in the treatment of a specific cancer type (CRC), are becoming increasingly complex in terms of design and composition, and production is becoming more challenging, as well as it is impossible to achieve the consistency of synthesis at large scale. In addition, physical and chemical characteristics of these nanoplatforms must be strictly regulated throughout the production procedure, which places an additional burden on the manufacturing facilities and causes the large-scale manufacturing to be even more complicated and costly. In this respect, microfluidic technology has attracted much interest. Indicatively, Valencia et al have shown successful self-assembly of lipid-polymer and lipid-quantum dot (QD) nanoparticles by microfluidics and the particles formed were stable, uniform.244 It is important to note, however, that the complicated structure of nanoparticles poses a possible risk of toxicity to patients, which makes the need to have models that better reflect the pathogenesis of human CRC in toxicity assessment in preclinical trials a necessity.245 Besides, clinical trials have shown that, although nanoplatforms usually decrease drug toxicity, they do not always increase therapeutic efficacy.245 It has been observed by scholars that even though most nanoparticles can localise at tumour sites due to the enhanced permeability and retention (EPR) effect- and even actively targeted particles are also dependent upon the same effect, the EPR effect is predictable in animal models but not in CRC patients. Such inconsistency of the EPR effect in patients can significantly affect the efficacy of nanoparticle-based therapies.246 Consequently, personalized treatment approaches are required, wherein nanoparticles are employed in patients exhibiting a strong EPR effect for optimal efficacy, or alternative formulations that can accumulate in tumors independently of the EPR effect, such as temperature-responsive hydrogels for localized CRC treatment, may be considered. Shelf-life limitations arise from the potential for drug leakage or premature release from the nanoparticle matrix before reaching the tumor site. Natural polymers might also undergo physicochemical changes during long-term storage, including changes in crystallinity or molecular weight distribution, leading to diminished performance. Furthermore, maintaining sterility and preventing microbial contamination pose additional challenges for shelf-stable formulations of natural polymer-based nanomedicines.247
Although the enhanced EPR effect is an appropriate mechanism for accumulation, a growing body of evidence shows that many human tumours have limited endothelial interstitial volumes and heterogeneous vascular permeability, which compromises the passive accumulation of certain broad classes of patients and lesions.41,248 Within settings of low EPR microenvironments, natural polymer-based nanomedicines may be designed with the prevailing objective of maintaining therapeutic efficacy by focusing on mechanisms that do not require significant vascular “leakiness”. First, active targeting strategies can be used to potentially augment cellular engagement and uptake following the contact with the tumour. In view of the colorectal cancer, the HA based systems are of particular relevance as they are able to bind to CD44 and RHAMM mediated pathways, which have been characterised in CRC and integrated with protective or colon specific designs of delivery systems.118,249
Second, tumour access may be improved by taking advantage of the transendothelial transport processes, such as transcytosis, combined with access facilitating strategies. These approaches are increasingly recognised as complementary to, or as replacement of, conventional EPR-mediated extravasation in a variety of solid tumours.41,250
Third, intratumoural dispersion, which is often limited by compactness and extracellular matrix architecture of the stroma, may be enhanced using multistage and stimuli-responsive polymer constructs for example size or charge switching designs and tumour microenvironment induced drug release mechanisms.251 Additionally, the incorporation of penetration promotional moieties, such as tumour penetrating peptides such as the iRGD when applicable, can improve more profound drug dissemination beyond perivascular zones.252,253 Taken together, these design considerations provide a pragmatic framework for improving the resilience of nanocarriers based on natural polymer materials against heterogeneous tumour vascular phenotypes.
Molecular Ageing and Release-Phase Instability of Natural-Polymer Carriers
Beyond macroscopic “shelf-life” considerations, the question of functional longevity of nanocarriers formed using natural polymers is often hampered by sluggish, coupled molecular phenomena which occur during storage and go on to modulate the release of the drug. In hydrated or partially hydrated conditions, relaxation of polymer chains re-organises the network over time - a process called physical ageing-, which can thus alter mesh size, permeability and mechanical integrity and so the kinetics of drug release over time. Concurrently, swelling by moisture-induced can plasticise polysaccharide matrices, increasing the rate of diffusion-driven drug escape, and can also provoke structural rearrangements that may not be apparent by routine sizing and evaluation techniques, and yet yield significant difference in performance in vivo.254,255
During extended storage or sustained release, the progressive hydrolytic and enzymatic breakage of glycosidic bonds or labile points of crosslinking (as well as, in some formulation, oxidative chain damage) may result in decreased molecular weight and decreased degree of cohesive strength and increase the premature drug leakage. These phenomena of degradation - relaxation are formulation - dependent (influenced eg., by polymer source, crosslink density, ionic milieu) and are strongly affected by the residual water content. Consequently, stabilisation strategies regularly use freeze - drying or lyophilisation with suitable protectants and strict moisture - control protocols once the biological activity structure have to be preserved upon reconstitution.256,257
Microfluidic Control of Flow Regime and Shear in Scalable Nanoparticle Fabrication
Microfluidic manufacturing has become an attractive platform for synthesis of natural polymer nanoparticles for better batch-to-batch reproducibility and better structural precision. In contrast with conventional bulk mixing strategies, microfluidic devices largely fall in the field of laminar flow regime (Reynolds number < 100), where the fluids stream parallel to one another and the mixing is achieved by controlled diffusion across sharply defined interfaces. Within this regime nucleation and growth of the nanoparticle are determined by rapid and reproducible solvent-anti-solvent interactions, allowing precise control of size and polydispersity of the finally obtained particles.258–260
More careful control of shear gradients within microchannels further affects the assembly of polymer chains and cross-linking kinetics. In natural polymer systems like chitosan or alginate nanoparticles, the ionic cross link formation can be controlled through shear-controlled mixing which limits uncontrolled aggregation and heterogeneity in size.261,262 It should also be noted that high shear rates can promote homogeneous supersaturation and binding uniform nucleation while poorly controlled gradients could result in wider size distributions and irregular structures.263,264
On one hand, rapid mixing times, often on the millisecond time, are particularly important in the definition of particle morphology and internal architecture. Short mixing times minimise uncontrolled growth phases and favour kinetically trapped and structurally uniform nanoparticles. This has direct implications for reproducibility, as by reducing this variability in clearance kinetics and tumor accumulation profiles improving distributions in size are less variable265,266 From an industrial point of view microfluidic platforms also provide scalability via parallelisation (“numbering-up”) as opposed to traditional scale - up approaches. By insuring identical hydrodynamic problems in replicated channels, structural porosity can be maintained at higher production rates, which overcomes a key limitation of classical bulk nanoprecipitation techniques.267,268 Consequently, a deep understanding of how the laminar flow condition, shear gradients, and mixing kinetics interact for preserving the structural fidelity and segregation of the therapeutic load through from laboratory synthesis to industrial manufacture is required for translating natural polymers nanoparticle systems.
Translational Limitations of Preclinical Tumour Models
The translation of preclinical efficacy of treatment is limited by biological differences between animal tumour models and human colorectal tumours, which by their nature is a limitation. Common murine models such as syngeneic and xenograft systems often do not match human cancers in terms of vascular architecture and stromal composition. Preclinical tumours are often characterized by an increased vessel density and more homogeneous perfusion (this can increase nanoparticle extravasation and retention in comparison with human tumours with more chaotic and heterogeneous vasculature - a factor which is directly relevant to nanocarrier accumulation by the EPR effect).269
In addition, the density of stroma and the composition of extracellular matrices (ECM) differ dramatically from one model to the next. For example, models of murine pancreatic and breast carcinoma display harder ECM with higher levels of collagen and hyaluronic acid which changes the diffusion of nanoparticles versus colon carcinoma models; this variation indicates that data obtained from one murine model may not be generalizable across tumour types or across to human disease.270 Moreover, patient-derived xenografts (PDX) have been widely used to maintain the human tumour histology, but the human stroma and immune cells are gradually replaced by host murine cells, and the microenvironment within the PDX develops differently from the original tumour with different cellular interactions, different enzymatic profile and the matrix dynamics.271
These discrepancies highlight that structural and functional attribute of tumours, including endothelial fenestration, interstitial pressure profiles, and the host enzymatic repertoires, can have differential effects on nanomedicine delivery, clearance and activation. Therefore, although data generated from preclinical models are still invaluable, the extent to which they are predictive in comparison with human CRC needs careful consideration. Complementary use of advanced models (eg., organoids, humanised animals and patient derived (humanised) systems) may enhance translational relevance through better recapitulating key aspects of human tumour biology.
Conclusion
Natural polymer-based nanomedicines represent a promising frontier in the targeted treatment of colon cancer, offering numerous advantages such as biocompatibility, biodegradability, and the ability to be functionalized for precise targeting. These nanomedicines have the potential to improve therapeutic efficacy while reducing systemic toxicity, making them a favorable alternative to traditional treatment modalities. Despite these promising prospects, significant challenges remain in the widespread clinical application of natural polymer-based nanoparticles. Issues related to the complexity of synthesis, scale-up production, and precise control over nanoparticle characteristics continue to hinder their commercialization. Additionally, the variability of the EPR effect in colon cancer patients underscores the need for personalized therapeutic approaches to optimize nanoparticle-based treatments. Addressing these challenges will require continued advancements in nanotechnology, manufacturing techniques, and the development of more predictive preclinical models. Innovative strategies, such as microfluidics for nanoparticle synthesis and the use of targeted formulations independent of the EPR effect, hold the potential to overcome some of the current limitations. Furthermore, personalized treatment regimens, tailored to the individual patient’s tumor characteristics and response profiles, will be essential in maximizing the clinical efficacy of natural polymer-based nanomedicines. While several hurdles remain, the continued development of natural polymer-based nanomedicines for colon cancer offers significant promise. With ongoing research and technological advancements, these nanomedicines could play a pivotal role in the future of targeted cancer therapy, offering more effective, safer, and personalized treatment options for colon cancer patients.
Funding
This work was supported by Science and Technology Department of the State Administration of Traditional Chinese Medicine of China - Zhejiang Province Joint Construction Project (grant no. GZY-ZJ-KJ-24098 to KTJ).
Disclosure
The authors declare that they have no competing interests, financial or non-financial or any other interests that might be perceived to influence the results and/or discussion reported in this paper.
References
1. ACS. ACS releases colorectal cancer estimates for 2024. 2024. Available from: https://colorectalcancer.org/article/acs-releases-colorectal-cancer-estimates-2024.
2. WHO. Colorectal cancer. 2024; Available from: https://www.who.int/news-room/fact-sheets/detail/colorectal-cancer.
3. Zhang T, Guo Y, Qiu B, et al. Global, regional, and national trends in colorectal cancer burden from 1990 to 2021 and projections to 2040. Front Oncol. 2025;14:1466159. doi:10.3389/fonc.2024.1466159
4. Tashkandi E. The Rise of Early-Onset Colorectal Cancer: clinical Characteristics and Outcomes in a Young Patient Population. Cancer Manage Res. 2025;17:2417–30. doi:10.2147/CMAR.S554044
5. Mehmood A. Epidemiological Trends and Risk Factors of Non-Communicable Diseases: a Global Perspective. Non-Communicable Diseases Care. 2025;2(1):12–22.
6. Farooqi MA, Mahnoor M, Delgado KM, et al. Focused Ultrasound as targeted therapy for colorectal cancer: a comprehensive review. Gastrointestinal Disorders. 2024;6(2):380–401. doi:10.3390/gidisord6020026
7. Zafar A, Khatoon S, Khan MJ, et al. Advancements and limitations in traditional anti-cancer therapies: a comprehensive review of surgery, chemotherapy, radiation therapy, and hormonal therapy. Discover Oncol. 2025;16(1):607. doi:10.1007/s12672-025-02198-8
8. Ashique S, Bhowmick M, Pal R, et al. Multi drug resistance in Colorectal Cancer-approaches to overcome, advancements and future success. Adv Cancer Biol. 2024;10:100114. doi:10.1016/j.adcanc.2024.100114
9. Puzzo M, De Santo M, Morelli C, et al. Colorectal cancer: current and future therapeutic approaches and related technologies addressing multidrug strategies against multiple level resistance mechanisms. Int J Mol Sci. 2025;26(3):1313. doi:10.3390/ijms26031313
10. Han CJ, Ning X, Burd CE, et al. Chemotoxicity and associated risk factors in colorectal cancer: a systematic review and meta-analysis. Cancers. 2024;16(14):2597. doi:10.3390/cancers16142597
11. Jiang Y, Zhao M, Tang W, et al. Impacts of systemic treatments on health-related quality of life for patients with metastatic colorectal cancer: a systematic review and network meta-analysis. BMC Cancer. 2024;24(1):188. doi:10.1186/s12885-024-11937-z
12. Vaupel P, Mayer A. Hypoxia in cancer: significance and impact on clinical outcome. Cancer Metastasis Rev. 2007;26(2):225–239. doi:10.1007/s10555-007-9055-1
13. Hockel M, Vaupel P. Tumor hypoxia: definitions and current clinical, biologic, and molecular aspects. J National Cancer Inst. 2001;93(4):266–276. doi:10.1093/jnci/93.4.266
14. Wong SH, Yu J. Gut microbiota in colorectal cancer: mechanisms of action and clinical applications. Nat Rev Gastroenterol Hepatol. 2019;16(11):690–704.
15. Pandey H, Tang DWT, Wong SH, et al. Gut microbiota in colorectal cancer: biological role and therapeutic opportunities. Cancers. 2023;15(3):866. doi:10.3390/cancers15030866
16. Fearon ER, Vogelstein B. A genetic model for colorectal tumorigenesis. Cell. 1990;61(5):759–767. doi:10.1016/0092-8674(90)90186-I
17. Guinney J, Dienstmann R, Wang X, et al. The consensus molecular subtypes of colorectal cancer. Nat Med. 2015;21(11):1350–1356. doi:10.1038/nm.3967
18. Network CGA. Comprehensive molecular characterization of human colon and rectal cancer. Nature. 2012;487(7407):330.
19. Sachdeo RA, Charde MS, Chakole RD. Colorectal cancer: an overview. Asian J Res Pharm Sci. 2020;10(3):211–223.
20. Puccini A, Marshall JL, Salem ME. Molecular variances between right-and left-sided colon cancers. Curr Colorectal Cancer Rep. 2018;14(5):152–158. doi:10.1007/s11888-018-0411-z
21. Zhang Y, Wang Y, Lu Y, et al. Advanced oral drug delivery systems for gastrointestinal targeted delivery: the design principles and foundations. J Nanobiotechnol. 2025;23(1):400. doi:10.1186/s12951-025-03479-8
22. Chuang L, Qifeng J, Shaolei Y. The tumor immune microenvironment and T-cell-related immunotherapies in colorectal cancer. Discover Oncol. 2024;15(1):244. doi:10.1007/s12672-024-01117-7
23. Pieniądz P, Pięt M, Paduch R. Characteristics of the colorectal cancer Microenvironment—Role in cancer progression and therapeutic possibilities. Appl Sci. 2024;14(7):2930. doi:10.3390/app14072930
24. Broesder A, Woerdenbag HJ, Prins GH, et al. pH-dependent ileocolonic drug delivery, part I: in vitro and clinical evaluation of novel systems. Drug Discovery Today. 2020;25(8):1362–1373. doi:10.1016/j.drudis.2020.06.011
25. Kridis WB, Mnif A, Khmiri S, et al. Right-sided versus left-sided metastatic colorectal cancer. Ann Oncol. 2019;30:iv68. doi:10.1093/annonc/mdz155.248
26. He X, Xie T, Shi L, et al. Research hotspots and frontiers in the tumor microenvironment of colorectal cancer: a bibliometric study from 2014 to 2024. Front Oncol. 2025;15:1525280. doi:10.3389/fonc.2025.1525280
27. Cervantes B, André T, Cohen R. Deficient mismatch repair/microsatellite unstable colorectal cancer: therapeutic advances and questions. Therapeut Adv Med Oncol. 2024;16:17588359231170473. doi:10.1177/17588359231170473
28. Azwar S, Seow HF, Abdullah M, et al. Recent updates on mechanisms of resistance to 5-fluorouracil and reversal strategies in colon cancer treatment. Biology. 2021;10(9):854. doi:10.3390/biology10090854
29. Sahin IH, Akce M, Alese O, et al. Immune checkpoint inhibitors for the treatment of MSI-H/MMR-D colorectal cancer and a perspective on resistance mechanisms. Br J Cancer. 2019;121(10):809–818. doi:10.1038/s41416-019-0599-y
30. Guo Y, Wang M, Zou Y, et al. Mechanisms of chemotherapeutic resistance and the application of targeted nanoparticles for enhanced chemotherapy in colorectal cancer. J Nanobiotechnol. 2022;20(1):371. doi:10.1186/s12951-022-01586-4
31. Haynes J, Manogaran P. Mechanisms and strategies to overcome drug resistance in colorectal cancer. Int J Mol Sci. 2025;26(5):1988.
32. Bukowski K, Kciuk M, Kontek R. Mechanisms of multidrug resistance in cancer chemotherapy. Int J Mol Sci. 2020;21(9):3233. doi:10.3390/ijms21093233
33. Albadari N, Xie Y, Li W. Deciphering treatment resistance in metastatic colorectal cancer: roles of drug transports, EGFR mutations, and HGF/c-MET signaling. Front Pharmacol. 2024;14:1340401. doi:10.3389/fphar.2023.1340401
34. Qiu J, Wu J-Z, Gu Z-G, et al. Influencing factors and predictive model of the early postoperative recurrence of colorectal cancer with obstruction. World J Gastrointest Surg. 2025;17(10). doi:10.4240/wjgs.v17.i10.110695.
35. Jain SM, Nagainallur Ravichandran S, Murali Kumar M, et al. Understanding the molecular mechanism responsible for developing therapeutic radiation-induced radioresistance of rectal cancer and improving the clinical outcomes of radiotherapy-A review. Cancer Biol Ther. 2024;25(1):2317999. doi:10.1080/15384047.2024.2317999
36. Wang L. Some People with Rectal Cancer Can Skip Radiation before Surgery. Available from: https://www.cancer.gov/news-events/cancer-currents-blog/2023/rectal-cancer-skip-radiation-before-surgery.
37. Arafat M, Sakkal M, Beiram R, et al. Nanomedicines: emerging platforms in smart chemotherapy treatment—a recent review. Pharmaceuticals. 2024;17(3):315. doi:10.3390/ph17030315
38. Mao Y, Xie J, Yang F, et al. Advances and prospects of precision nanomedicine in personalized tumor theranostics. Front Cell Develop Biol. 2024;12:1514399. doi:10.3389/fcell.2024.1514399
39. Pagar N, Shewale N, Patil P, et al. Nanomedicine In Cancer Therapy: targeted Approach For Improved Efficacy. IJSAT. 2025;16(1):5.
40. Zhang J, Ali K, Wang J. Research advances of lipid nanoparticles in the treatment of colorectal cancer. Int J Nanomed. 2024;19:6693–6715. doi:10.2147/IJN.S466490
41. Wu J. The enhanced permeability and retention (EPR) effect: the significance of the concept and methods to enhance its application. J Personalized Med. 2021;11(8):771. doi:10.3390/jpm11080771
42. Kim J, Cho H, Lim D-K, et al. Perspectives for improving the tumor targeting of nanomedicine via the EPR effect in clinical tumors. Int J Mol Sci. 2023;24(12):10082. doi:10.3390/ijms241210082
43. Hasan M, Evett CG, Burton J. Advances in Nanoparticle-Based Targeted Drug Delivery Systems for Colorectal Cancer Therapy: a Review. arXiv preprint arXiv:2409.05222. 2024.
44. Razzaq S, I Fatima, Z Moafian, et al. Nanomedicine innovations in colon and rectal cancer: advances in targeted drug and gene delivery systems. Med Oncol. 2025;42(4):1–35.
45. Ly P-D, Ly K-N, Phan H-L, et al. Recent advances in surface decoration of nanoparticles in drug delivery. Front Nanotechnol. 2024;6:1456939. doi:10.3389/fnano.2024.1456939
46. Roma-Rodrigues C, Mendes R, Baptista PV, et al. Targeting tumor microenvironment for cancer therapy. Int J Mol Sci. 2019;20(4):840. doi:10.3390/ijms20040840
47. Subhan MA, Yalamarty SSK, Filipczak N, et al. Recent advances in tumor targeting via EPR effect for cancer treatment. J Personalized Med. 2021;11(6):571. doi:10.3390/jpm11060571
48. Liu Y, Liang Y, Yuhong J, et al. Advances in nanotechnology for enhancing the solubility and bioavailability of poorly soluble drugs. Drug Design. Develop Ther. 2024;18:1469–1495. doi:10.2147/DDDT.S447496
49. Xin H, Chang Z, Niu M. Multifaceted Applications of Nanomaterials in Colorectal Cancer Management: screening, Diagnostics, and Therapeutics. Int J Nanomed. 2025;20:7271–7294. doi:10.2147/IJN.S520616
50. Cruz-Nova P, Ancira-Cortez A, Ferro-Flores G, et al. Controlled-release nanosystems with a dual function of targeted therapy and radiotherapy in colorectal cancer. Pharmaceutics. 2022;14(5):1095. doi:10.3390/pharmaceutics14051095
51. Xiao B, Ma L, Merlin D. Nanoparticle-mediated co-delivery of chemotherapeutic agent and siRNA for combination cancer therapy. Expert Opin Drug Delivery. 2017;14(1):65–73. doi:10.1080/17425247.2016.1205583
52. Creixell M, Peppas NA. Co-delivery of siRNA and therapeutic agents using nanocarriers to overcome cancer resistance. Nano Today. 2012;7(4):367–379. doi:10.1016/j.nantod.2012.06.013
53. Siafaka PI, Okur NÜ, Karantas ID, et al. Current update on nanoplatforms as therapeutic and diagnostic tools: a review for the materials used as nanotheranostics and imaging modalities. Asian J Pharm Sci. 2021;16(1):24–46. doi:10.1016/j.ajps.2020.03.003
54. Monia T. Sustainable natural biopolymers for biomedical applications. J Thermoplast Compos Mater. 2024;37(7):2505–2524. doi:10.1177/08927057231214468
55. Yadav P, Yadav H, Shah VG, et al. Biomedical biopolymers, their origin and evolution in biomedical sciences: a systematic review. J Clin Diagn Res. 2015;9(9):ZE21. doi:10.7860/JCDR/2015/13907.6565
56. Gowthaman N, Lim HN, Sreeraj TR, et al. Advantages of biopolymers over synthetic polymers: social, economic, and environmental aspects. In: Biopolymers and Their Industrial Applications. Elsevier; 2021:351–372.
57. Wu X, Xin Y, Zhang H, et al. Biopolymer-based nanomedicine for cancer therapy: opportunities and challenges. Int J Nanomed. 2024;19:7415–7471. doi:10.2147/IJN.S460047
58. Martínez G, Merinero M, Pérez-Aranda M, et al. Environmental impact of nanoparticles’ application as an emerging technology: a review. Materials. 2020;14(1):166. doi:10.3390/ma14010166
59. Zhao L, Zhou Y, Zhang J, et al. Natural polymer-based hydrogels: from polymer to biomedical applications. Pharmaceutics. 2023;15(10):2514. doi:10.3390/pharmaceutics15102514
60. Sarkar R, Biswas P, Mukherjee DR, et al. Chrono-Colonic Delivery in Engineering Time-Responsive Systems for Site-Specific Therapy. J Drug Delivery Ther. 2025;15(10):148–171. doi:10.22270/jddt.v15i10.7398
61. Pan DC, Krishnan V, Salinas AK, et al. Hyaluronic a cid–doxorubicin nanoparticles for targeted treatment of colorectal cancer. Bioeng Transl Med. 2021;6(1):e10166. doi:10.1002/btm2.10166
62. Chen E, Han S, Song B, et al. Mechanism investigation of hyaluronidase-combined multistage nanoparticles for solid tumor penetration and antitumor effect. Int J Nanomed. 2020;15:6311–6324. doi:10.2147/IJN.S257164
63. Satchanska G, Davidova S, Petrov PD. Natural and synthetic polymers for biomedical and environmental applications. Polymers. 2024;16(8):1159. doi:10.3390/polym16081159
64. Ganie SA, Rather LJ, Li Q. Recent innovations in the strategies for the functionalization of chitosan, pectin, alginate, hyaluronic acid, dextran and inulin biomaterials for anticancer applications-a review. J Polym Environ. 2023;31(1):13–35. doi:10.1007/s10924-022-02547-6
65. Hou X, Zhang H. Research progress of hyaluronic acid-coated nanocarriers in targeted cancer therapy. Cancer Biother Radiopharm. 2025;40(4):231–243. doi:10.1089/cbr.2024.0143
66. Sinha VR, Kumria R. Polysaccharides in colon-specific drug delivery. Int J Pharm. 2001;224(1–2):19–38. doi:10.1016/S0378-5173(01)00720-7
67. Ponnusamy PG, Mani S. Material and environmental properties of natural polymers and their composites for packaging applications—A review. Polymers. 2022;14(19):4033. doi:10.3390/polym14194033
68. Ramful R. Mechanical performance and durability attributes of biodegradable natural fibre-reinforced composites—A review. J Mater Sci. 2024;19(1):50.
69. Hua Y, Su Y, Zhang H, et al. Poly (lactic-co-glycolic acid) microsphere production based on quality by design: a review. Drug Delivery. 2021;28(1):1342–1355. doi:10.1080/10717544.2021.1943056
70. Khan MS, Rehman U, Alqahtani T, et al. Advances in PLGA-based polymeric nanocarriers for colorectal cancer therapy: overcoming chemoresistance through controlled delivery strategies. Mol Cancer. 2025;24(1):288. doi:10.1186/s12943-025-02435-2
71. Wang Y, Huang P, Li C, et al. PLGA-based nanoparticles in colorectal cancer immunotherapy: current concepts and future perspectives. Front Pharmacol. 2025;16:1714460. doi:10.3389/fphar.2025.1714460
72. Wang N, Chen L, Huang W, et al. Current advances of nanomaterial-based oral drug delivery for colorectal cancer treatment. Nanomaterials. 2024;14(7):557. doi:10.3390/nano14070557
73. Guduganahalli Manjunath P, Ravi NK, Sridhar SK, et al. Innovative strategies and nanocarrier approaches for enhancing the oral bioavailability of macromolecular therapeutics. Iran J Basic Med Sci. 2025;28(12):1607–1619. doi:10.22038/ijbms.2025.87167.18839
74. Lee SH, Bajracharya R, Min JY, et al. Strategic approaches for colon targeted drug delivery: an overview of recent advancements. Pharmaceutics. 2020;12(1):68. doi:10.3390/pharmaceutics12010068
75. Geetha K, Akshitha S, Rao TR. A Review on Colon Drug Delivery Systems. Int J Pharm Sci Rev Res. 2023;82(2):25–35. doi:10.47583/ijpsrr.2023.v82i02.004
76. Xu C, Xu H, Zhu Z, et al. Recent advances in mucus-penetrating nanomedicines for oral treatment of colonic diseases. Expert Opin Drug Delivery. 2023;20(10):1371–1385. doi:10.1080/17425247.2023.2242266
77. Philip AK, Philip B. Colon targeted drug delivery systems: a review on primary and novel approaches. Oman Med J. 2010;25(2):79. doi:10.5001/omj.2010.24
78. Yamamura R, Inoue KY, Nishino K, et al. Intestinal and fecal pH in human health. Front Microbiomes. 2023;2:1192316. doi:10.3389/frmbi.2023.1192316
79. Singh J, Solanki A, Sikarwar GS, et al. Advances in Colon-Targeted Drug Delivery Systems: innovative Strategies for Treating Colonic Disorders and Prospects for the Future. Curr Pharm Biotechnol. 2024;2024:1.
80. Guo Y, Zong S, Pu Y, et al. Advances in pharmaceutical strategies enhancing the efficiencies of oral colon-targeted delivery systems in inflammatory bowel disease. Molecules. 2018;23(7):1622. doi:10.3390/molecules23071622
81. Zhou F, Mu G, Bi H, et al. Targeted Hyaluronan Degradation Enhanced Tumor Growth Inhibition in Gastrointestinal Cancer Models. Cancers. 2025;17(21):3411. doi:10.3390/cancers17213411
82. Zheng G, Zhang B, Yu H, et al. Therapeutic applications and potential biological barriers of nano-delivery systems in common gastrointestinal disorders: a comprehensive review. Adv Compos Hybrid Mater. 2025;8(2):1–22. doi:10.1007/s42114-025-01292-3
83. Chai M, Wang S, Chen Y, et al. Targeted and intelligent nano-drug delivery systems for colorectal cancer treatment. Front Bioeng Biotechnol. 2025;13:1582659. doi:10.3389/fbioe.2025.1582659
84. Gagliardi A, Giuliano E, Venkateswararao E, et al. Biodegradable polymeric nanoparticles for drug delivery to solid tumors. Front Pharmacol. 2021;12:601626. doi:10.3389/fphar.2021.601626
85. Widiani Batubara R, Saputri FC, Iswandana R. Current Update of Clinical Therapeutic Strategies for Colon-Targeted Delivery Systems. Pharma Sci Res. 2024;11(1):1.
86. Chen Z, Han F, Du Y, et al. Hypoxic microenvironment in cancer: molecular mechanisms and therapeutic interventions. Signal Transduc Target Ther. 2023;8(1):70. doi:10.1038/s41392-023-01332-8
87. Wilhelm S, Tavares AJ, Dai Q, et al. Analysis of nanoparticle delivery to tumours. Nat Rev Mater. 2016;1(5):16014. doi:10.1038/natrevmats.2016.14
88. Sindhwani S, Syed AM, Ngai J, et al. The entry of nanoparticles into solid tumours. Nature Mater. 2020;19(5):566–575. doi:10.1038/s41563-019-0566-2
89. Danhier F. To exploit the tumor microenvironment: since the EPR effect fails in the clinic, what is the future of nanomedicine? J Control Release. 2016;244:108–121. doi:10.1016/j.jconrel.2016.11.015
90. Dilliard SA, Siegwart DJ. Passive, active and endogenous organ-targeted lipid and polymer nanoparticles for delivery of genetic drugs. Nature Rev Mater. 2023;8(4):282–300. doi:10.1038/s41578-022-00529-7
91. Bi Y, Hao F, Yan G, et al. Actively targeted nanoparticles for drug delivery to tumor. Curr Drug Metabol. 2016;17(8):763–782. doi:10.2174/1389200217666160619191853
92. Nguyen LN, Ngo W, Lin ZP, et al. The mechanisms of nanoparticle delivery to solid tumours. Nat Rev Bioeng. 2024;2(3):201–213. doi:10.1038/s44222-024-00154-9
93. Mukhtar M, Fényes E, Bartos C, et al. Chitosan biopolymer, its derivatives and potential applications in nano-therapeutics: a comprehensive review. Eur Polym J. 2021;160:110767. doi:10.1016/j.eurpolymj.2021.110767
94. Akram W, Mishra N, Haider T. Inulin for Pharmaceutical Applications: A Versatile Biopolymer. Springer Nature; 2025.
95. Somasundaram SN, Shanmugam S, Subramanian B, et al. Cytotoxic effect of fucoidan extracted from Sargassum cinereum on colon cancer cell line HCT-15. Int J Biol Macromol. 2016;91:1215–1223. doi:10.1016/j.ijbiomac.2016.06.084
96. Chaurasia M, Chourasia MK, Jain NK, et al. Cross-linked guar gum microspheres: a viable approach for improved delivery of anticancer drugs for the treatment of colorectal cancer. AAPS Pharm Sci Tech. 2006;7(3):74. doi:10.1208/pt070374
97. Kondiah PPD, Rants’o TA, Makhathini SS, et al. An oral 3D printed PLGA-tocopherol PEG succinate nanocomposite hydrogel for high-dose methotrexate delivery in maintenance chemotherapy. Biomedicines. 2022;10(7):1470. doi:10.3390/biomedicines10071470
98. Iskandar A, Zaiki Y, Wong TW. Pectin as cancer targeting nano-vehicle and therapeutic — physicochemical-biological perspectives: a review. Biomater Adv. 2026;180:214562. doi:10.1016/j.bioadv.2025.214562
99. Jadav M, Pooja D, Adams DJ, et al. Advances in Xanthan Gum-Based Systems for the Delivery of Therapeutic Agents. Pharmaceutics. 2023;15(2):402. doi:10.3390/pharmaceutics15020402
100. Raza MA, Sharma MK, Nagori K, et al. Recent trends on polycaprolactone as sustainable polymer-based drug delivery system in the treatment of cancer: biomedical applications and nanomedicine. Int J Pharm. 2024;666:124734. doi:10.1016/j.ijpharm.2024.124734
101. Bhattacharya S, Singh D. Chitosan Approaches in Colon Cancer Therapy: understanding its Macromolecular Interactions and Structure-Property Relationships. J Macromol Sci. 2025;Part B:1–12.
102. Bose A, Wong TW. Oral colon cancer targeting by chitosan nanocomposites. In: Applications of Nanocomposite Materials in Drug Delivery. Elsevier; 2018:409–429.
103. Stefanache A, Lungu II, Anton N, et al. Chitosan Nanoparticle-Based Drug Delivery Systems: advances, Challenges, and Future Perspectives. Polymers. 2025;17(11):1453. doi:10.3390/polym17111453
104. Choukaife H, Seyam S, Alallam B, et al. Current advances in chitosan nanoparticles based oral drug delivery for colorectal cancer treatment. Int J Nanomed. 2022;17:3933–3966. doi:10.2147/IJN.S375229
105. Zhang S, Qamar SA, Junaid M, et al. Algal polysaccharides‐based nanoparticles for targeted drug delivery applications. Starch - Stärke. 2022;74(7–8):2200014. doi:10.1002/star.202200014
106. Bhuyan PP, Nayak R, Patra S, et al. Seaweed-derived sulfated polysaccharides; the new age chemopreventives: a comprehensive review. Cancers. 2023;15(3):715. doi:10.3390/cancers15030715
107. Lai J, Azad AK, Sulaiman WMAW, et al. Alginate-based encapsulation fabrication technique for drug delivery: an updated review of particle type, formulation technique, pharmaceutical ingredient, and targeted delivery system. Pharmaceutics. 2024;16(3):370. doi:10.3390/pharmaceutics16030370
108. Agüero L, Zaldivar-Silva D, Peña L, et al. Alginate microparticles as oral colon drug delivery device: a review. Carbohydr Polym. 2017;168:32–43. doi:10.1016/j.carbpol.2017.03.033
109. Chiu HI, Lim V. Wheat germ agglutinin-conjugated disulfide cross-linked alginate nanoparticles as a docetaxel carrier for colon cancer therapy. Int J Nanomed. 2021;16:2995–3020. doi:10.2147/IJN.S302238
110. Alallam B, Abdkadir E, Hayati A, et al. Alginate coated mesoporous silica nanoparticles as oral delivery carrier of curcumin and quercetin to colon cancer: preparation, optimization, characterization, and anticancer activity. Drug Delivery Transl Res. 2025;15:1–42.
111. De Anda-Flores Y, Carvajal-Millan E, Campa-Mada A, et al. Polysaccharide-based nanoparticles for colon-targeted drug delivery systems. Polysaccharides. 2021;2(3):626–647. doi:10.3390/polysaccharides2030038
112. Ibrahim IM. Advances in polysaccharide-based oral colon-targeted delivery systems: the journey so far and the road ahead. Cureus. 2023;15(1):e33636.
113. Wong TW, Colombo G, Sonvico F. Pectin matrix as oral drug delivery vehicle for colon cancer treatment. AAPS Pharm Sci Tech. 2011;12(1):201–214.
114. Huang S, Huang G. Preparation and drug delivery of dextran-drug complex. Drug Delivery. 2019;26(1):252–261. doi:10.1080/10717544.2019.1580322
115. Khotimchenko M. Pectin polymers for colon-targeted antitumor drug delivery. Int J Biol Macromol. 2020;158:1110–1124.
116. Abid M, Naveed M, Azeem I, et al. Colon specific enzyme responsive oligoester crosslinked dextran nanoparticles for controlled release of 5-fluorouracil. Int J Pharm. 2020;586:119605. doi:10.1016/j.ijpharm.2020.119605
117. Yang B, Mao Y, Zhang Y, et al. HA-coated PLGA nanoparticles loaded with apigenin for colon cancer with high expression of CD44. Molecules. 2023;28(22):7565. doi:10.3390/molecules28227565
118. de Paula MC, Carvalho SG, Silvestre ALP, et al. The role of hyaluronic acid in the design and functionalization of nanoparticles for the treatment of colorectal cancer. Carbohydr Polym. 2023;320:121257.
119. Misra S, Heldin P, Hascall VC, et al. Hyaluronan–CD44 interactions as potential targets for cancer therapy. FEBS J. 2011;278(9):1429–1443. doi:10.1111/j.1742-4658.2011.08071.x
120. Mattheolabakis G, Milane L, Singh A, et al. Hyaluronic acid targeting of CD44 for cancer therapy: from receptor biology to nanomedicine. J Drug Targeting. 2015;23(7–8):605–618. doi:10.3109/1061186X.2015.1052072
121. Li Y, Duy Le TM, Nam Bui Q, et al. Tumor acidity and CD44 dual targeting hyaluronic acid-coated gold nanorods for combined chemo-and photothermal cancer therapy. Carbohydr Polym. 2019;226:115281. doi:10.1016/j.carbpol.2019.115281
122. Negi LM, Jaggi M, Joshi V, et al. Hyaluronic acid decorated lipid nanocarrier for MDR modulation and CD-44 targeting in colon adenocarcinoma. Int J Biol Macromol. 2015;72:569–574. doi:10.1016/j.ijbiomac.2014.09.005
123. Saneja A, Nayak D, Srinivas M, et al. Development and mechanistic insight into enhanced cytotoxic potential of hyaluronic acid conjugated nanoparticles in CD44 overexpressing cancer cells. Eur J Pharm Sci. 2017;97:79–91.
124. Madkhali OA. Drug delivery of gelatin nanoparticles as a biodegradable polymer for the treatment of infectious diseases: perspectives and challenges. Polymers. 2023;15(21):4327. doi:10.3390/polym15214327
125. Jiang X, Du Z, Zhang X, et al. Gelatin-based anticancer drug delivery nanosystems: a mini review. Front Bioeng Biotechnol. 2023;11:1158749. doi:10.3389/fbioe.2023.1158749
126. Raza F, Siyu L, Zafar H, et al. Recent advances in gelatin-based nanomedicine for targeted delivery of anti-cancer drugs. Curr Pharm Des. 2022;28(5):380–394. doi:10.2174/1381612827666211102100118
127. Hussain A, Hasan A, Babadaei MMN, et al. Application of gelatin nanoconjugates as potential internal stimuli-responsive platforms for cancer drug delivery. J Mol Liq. 2020;318:114053. doi:10.1016/j.molliq.2020.114053
128. Hassanin I, Elzoghby A. Albumin-based nanoparticles: a promising strategy to overcome cancer drug resistance. Cancer Drug Resistance. 2020;3(4):930. doi:10.20517/cdr.2020.68
129. Meng R, Zhu H, Wang Z, et al. Preparation of drug‐loaded albumin nanoparticles and its application in cancer therapy. J Nanomater. 2022;2022(1):3052175. doi:10.1155/2022/3052175
130. Cho H, Jeon SI, Ahn C-H, et al. Emerging albumin-binding anticancer drugs for tumor-targeted drug delivery: current understandings and clinical translation. Pharmaceutics. 2022;14(4):728. doi:10.3390/pharmaceutics14040728
131. Ishima Y, Maruyama T, Otagiri M, et al. The new delivery strategy of albumin carrier utilizing the interaction with albumin receptors. Chem Pharm Bull. 2022;70(5):330–333. doi:10.1248/cpb.c21-01024
132. Mun EA, Zhaisanbayeva BA. The role of nanoparticle PEGylation in drug delivery. Adv Mat & Tech. 2020;2020(2):10–18. doi:10.17277/amt.2020.02.pp.010-018
133. Suk JS, Xu Q, Kim N, et al. PEGylation as a strategy for improving nanoparticle-based drug and gene delivery. Adv Drug Delivery Rev. 2016;99:28–51. doi:10.1016/j.addr.2015.09.012
134. Acharya S, Sahoo SK. PLGA nanoparticles containing various anticancer agents and tumour delivery by EPR effect. Adv Drug Delivery Rev. 2011;63(3):170–183. doi:10.1016/j.addr.2010.10.008
135. Leonard TE, Liko AF, Gustiananda M, et al. Thiolated pectin-chitosan composites: potential mucoadhesive drug delivery system with selective cytotoxicity towards colorectal cancer. Int J Biol Macromol. 2023;225:1–12. doi:10.1016/j.ijbiomac.2022.12.012
136. Hock N, Racaniello GF, Aspinall S, et al. Thiolated nanoparticles for biomedical applications: mimicking the workhorses of our body. Adv Sci. 2022;9(1):2102451. doi:10.1002/advs.202102451
137. Grosso R, de-Paz M-V. Thiolated-polymer-based nanoparticles as an avant-garde approach for anticancer therapies—reviewing thiomers from chitosan and hyaluronic acid. Pharmaceutics. 2021;13(6):854. doi:10.3390/pharmaceutics13060854
138. Curcio M, Vittorio O, Bell JL, et al. Hyaluronic acid within self-assembling nanoparticles: endless possibilities for targeted cancer therapy. Nanomaterials. 2022;12(16):2851. doi:10.3390/nano12162851
139. Syed SA, Murthannagari VR, Venkatachalam S, et al. Precisive Colon Cancer Treatment: exploring Novel Avenues Of Cancer Treatment Through Multistage Nanocarriers. J Res Pharm. 2023;27(3):1096–1119. doi:10.29228/jrp.402
140. Belyaev IB, Griaznova OY, Yaremenko AV, et al. Beyond the EPR effect: intravital microscopy analysis of nanoparticle drug delivery to tumors. Adv. Drug Delivery Rev. 2025;219:115550. doi:10.1016/j.addr.2025.115550
141. Lin Q, Choyke PL, Sato N. Visualizing vasculature and its response to therapy in the tumor microenvironment. Theranostics. 2023;13(15):5223. doi:10.7150/thno.84947
142. Chehelgerdi M, Chehelgerdi M, Allela OQB, et al. Progressing nanotechnology to improve targeted cancer treatment: overcoming hurdles in its clinical implementation. Mol Cancer. 2023;22(1):169. doi:10.1186/s12943-023-01865-0
143. Patel JK, Patel AP. Passive targeting of nanoparticles to cancer. In: Surface Modification of Nanoparticles for Targeted Drug Delivery. Springer; 2019:125–143.
144. Vagena I-A, Malapani C, Gatou M-A, et al. Enhancement of EPR Effect for Passive Tumor Targeting: current Status and Future Perspectives. Appl Sci. 2025;15(6):3189. doi:10.3390/app15063189
145. Islam W, Niidome T, Sawa T. Enhanced permeability and retention effect as a ubiquitous and epoch-making phenomenon for the selective drug targeting of solid tumors. J Personalized Med. 2022;12(12):1964. doi:10.3390/jpm12121964
146. Cisterna BA, Kamaly N, Choi WI, et al. Targeted nanoparticles for colorectal cancer. Nanomedicine. 2016;11(18):2443–2456. doi:10.2217/nnm-2016-0194
147. Jain A, Bhattacharya S. Recent advances in nanomedicine preparative methods and their therapeutic potential for colorectal cancer: a critical review. Front Oncol. 2023;13:1211603. doi:10.3389/fonc.2023.1211603
148. Hu Y, He Y, Ji J, et al. Tumor targeted curcumin delivery by folate-modified MPEG-PCL self-assembly micelles for colorectal cancer therapy. Int J Nanomed. 2020;15:1239–1252. doi:10.2147/IJN.S232777
149. Dabkeviciene D, Jonusiene V, Zitkute V, et al. The role of interleukin-8 (CXCL8) and CXCR2 in acquired chemoresistance of human colorectal carcinoma cells HCT116. Med Oncol. 2015;32(12):258. doi:10.1007/s12032-015-0703-y
150. Jain AK, Massey A, Yusuf H, et al. Development of polymeric–cationic peptide composite nanoparticles, a nanoparticle-in-nanoparticle system for controlled gene delivery. Int J Nanomed;2015. 7183–7196. doi:10.2147/IJN.S95245
151. Yu D-H, Lu Q, Xie J, et al. Peptide-conjugated biodegradable nanoparticles as a carrier to target paclitaxel to tumor neovasculature. Biomaterials. 2010;31(8):2278–2292. doi:10.1016/j.biomaterials.2009.11.047
152. Soe ZC, Poudel BK, Nguyen HT, et al. Folate-targeted nanostructured chitosan/chondroitin sulfate complex carriers for enhanced delivery of bortezomib to colorectal cancer cells. Asian J Pharm Sci. 2019;14(1):40–51. doi:10.1016/j.ajps.2018.09.004
153. Bhattacharya S. Anti-EGFR-mAb and 5-fluorouracil conjugated polymeric nanoparticles for colorectal cancer. Recent Patents Anti-Cancer Drug Disc. 2021;16(1):84–100. doi:10.2174/1574892815666201221121859
154. Ge P, Niu B, Wu Y, et al. Enhanced cancer therapy of celastrol in vitro and in vivo by smart dendrimers delivery with specificity and biosafety. Chem Eng J. 2020;383:123228. doi:10.1016/j.cej.2019.123228
155. Khatami F, Matin MM, Danesh NM, et al. Targeted delivery system using silica nanoparticles coated with chitosan and AS1411 for combination therapy of doxorubicin and antimiR-21. Carbohydr Polym. 2021;266:118111. doi:10.1016/j.carbpol.2021.118111
156. Zhao Y, Xu J, Le VM, et al. EpCAM aptamer-functionalized cationic liposome-based nanoparticles loaded with miR-139-5p for targeted therapy in colorectal cancer. Mol Pharmaceut. 2019;16(11):4696–4710. doi:10.1021/acs.molpharmaceut.9b00867
157. Elmowafy M, Shalaby K, Elkomy MH, et al. Polymeric nanoparticles for delivery of natural bioactive agents: recent advances and challenges. Polymers. 2023;15(5):1123. doi:10.3390/polym15051123
158. Nair A, Chandrashekhar H R, Day CM, et al. Polymeric functionalization of mesoporous silica nanoparticles: biomedical insights. Int J Pharm. 2024;660:124314. doi:10.1016/j.ijpharm.2024.124314
159. Danaei M, Dehghankhold M, Ataei S, et al. Impact of particle size and polydispersity index on the clinical applications of lipidic nanocarrier systems. Pharmaceutics. 2018;10(2):57. doi:10.3390/pharmaceutics10020057
160. Blanco E, Shen H, Ferrari M. Principles of nanoparticle design for overcoming biological barriers to drug delivery. Nature Biotechnol. 2015;33(9):941–951. doi:10.1038/nbt.3330
161. Tang L, Gabrielson NP, Uckun FM, et al. Size-Dependent Tumor Penetration and in Vivo Efficacy of Monodisperse Drug–Silica Nanoconjugates. Mol Pharmaceut. 2013;10(3):883–892. doi:10.1021/mp300684a
162. Cabral H, Matsumoto Y, Mizuno K, et al. Accumulation of sub-100 nm polymeric micelles in poorly permeable tumours depends on size. Nature Nanotechnol. 2011;6(12):815–823. doi:10.1038/nnano.2011.166
163. Sykes EA, Chen J, Zheng G, et al. Investigating the impact of nanoparticle size on active and passive tumor targeting efficiency. ACS Nano. 2014;8(6):5696–5706. doi:10.1021/nn500299p
164. Lee B, Lee Y, Lee N, et al. Design of oxide nanoparticles for biomedical applications. Nature Rev Mater. 2025;10(4):252–267. doi:10.1038/s41578-024-00767-x
165. Kaialy W, Shafiee MA. Recent advances in the engineering of nanosized active pharmaceutical ingredients: promises and challenges. Adv Colloid Interface Sci. 2016;228:71–91. doi:10.1016/j.cis.2015.11.010
166. Monopoli MP, Aberg C, Salvati A, et al. Biomolecular coronas provide the biological identity of nanosized materials. Nano-Enabled Med Applications. 2020;205–229.
167. Bae YH, Park K. Targeted drug delivery to tumors: myths, reality and possibility. J Control Release. 2011;153(3):198–205.
168. Strambi A, De Milito A. Contribution of pH alterations to the tumor microenvironment. In: Tumor Cell Metabolism: Pathways, Regulation and Biology. Springer; 2015:173–196.
169. Kawamura A, Miyata T. pH-Responsive polymer. Encycl Polym Nanomater. 2021;2021:1–9.
170. Yusa S-I. Development and application of pH-responsive polymers. Polym J. 2022;54(3):235–242. doi:10.1038/s41428-021-00576-x
171. Khatibi N, Naimi-Jamal MR, Balalaie S, et al. Development and evaluation of a pH-sensitive, naturally crosslinked alginate-chitosan hydrogel for drug delivery applications. Front Biomater Sci. 2024;3:1457540. doi:10.3389/fbiom.2024.1457540
172. Moreno-Rivas SC, Ibarra-Gutiérrez MJ, Fernández-Quiroz D, et al. pH-responsive alginate/chitosan gel films: an alternative for removing cadmium and lead from water. Gels. 2024;10(10):669. doi:10.3390/gels10100669
173. Fu D, Zhong L, Xu J, et al. Hydrazone-functionalized nanoscale covalent organic frameworks as a nanocarrier for pH-responsive drug delivery enhanced anticancer activity. RSC Adv. 2024;14(29):20799–20808. doi:10.1039/D4RA01955E
174. Qin J, Zhu Y, Zheng D, et al. pH-sensitive polymeric nanocarriers for antitumor biotherapeutic molecules targeting delivery. Bio-Des Manuf. 2021;4(3):612–626. doi:10.1007/s42242-020-00105-4
175. Musa N, Layas NA, Zin NZM. Polysaccharides carrier as oral colon-specific drug delivery for colon cancer treatment. Nano Trends. 2025;10:100102. doi:10.1016/j.nwnano.2025.100102
176. Piotrowska U, Szatko J, Nowakowska A, et al. Chitosan-Based Drug Delivery Systems for Targeted Chemotherapy in Colorectal Cancer: a Scoping Review. Mar Drugs. 2025;23(12):467. doi:10.3390/md23120467
177. Kumar A, Singh NK, Wadhwa S, et al. Advancing colon targeting: natural polymer systems for drug delivery. Eur Polym J. 2025;2025:114459.
178. Dodero A, Alberti S, Gaggero G, et al. An up‐to‐date review on alginate nanoparticles and nanofibers for biomedical and pharmaceutical applications. Adv Mater Interfaces. 2021;8(22):2100809. doi:10.1002/admi.202100809
179. Liu Y, Kang W, Nie L, et al. Alginate/methacrylic acid/calcium ion-based pH-sensitive drug delivery hydrogel for the treatment of ulcerative colitis. React Funct Polym. 2024;204:106025. doi:10.1016/j.reactfunctpolym.2024.106025
180. Foroutan R, Mohammadzadeh A, Javanbakht S, et al. Alginate/magnetic hydroxyapatite bio-nanocomposite hydrogel bead as a pH-responsive oral drug carrier for potential colon cancer therapy. Res Chem. 2025;15:102177. doi:10.1016/j.rechem.2025.102177
181. Muhammed RA, Mohammed S, Visht S, et al. A review on development of colon targeted drug delivery system. Int J Appl Pharm. 2024;16(2):12–27. doi:10.22159/ijap.2024v16i2.49293
182. Shao H, Liu M, Jiang H, et al. Polysaccharide-based drug delivery targeted approach for colon cancer treatment: a comprehensive review. Int J Biol Macromol. 2025;302:139177. doi:10.1016/j.ijbiomac.2024.139177
183. Hasnain MS, Nayak AK. Chitosan as mucoadhesive polymer in drug delivery. In: Chitosan in Drug Delivery. Elsevier; 2022;2022:225–246.
184. Huckaby JT, Lai SK. PEGylation for enhancing nanoparticle diffusion in mucus. Adv Drug Delivery Rev. 2018;124:125–139. doi:10.1016/j.addr.2017.08.010
185. Nunes R, Araújo F, Tavares J, et al. Surface modification with polyethylene glycol enhances colorectal distribution and retention of nanoparticles. Eur J Pharm Biopharm. 2018;130:200–206. doi:10.1016/j.ejpb.2018.06.029
186. Shah D, Thakkar A, Bhattacharya S. Hyaluronic Acid-Polyethylene Glycol-Polycaprolactone Nanocarriers: accurate Targeting and Multimodal Treatment for Aggressive Cancers. J Macromol Sci. 2025;Part B:1–27. doi:10.1080/00222348.2025.2537449
187. Liu S, Tong S, Liu G, et al. Hyaluronic acid-functionalized nanoparticles enable enhanced chemo/chemodynamic therapy for the targeted treatment of colon cancer. Int J Biol Macromol. 2025;303:140553. doi:10.1016/j.ijbiomac.2025.140553
188. Puluhulawa LE, Joni IM, Elamin KM, et al. Chitosan–hyaluronic acid nanoparticles for active targeting in cancer therapy. Polymers. 2022;14(16):3410. doi:10.3390/polym14163410
189. Roope LS. The economic challenges of new drug development. J Control Release. 2022;345:275–277. doi:10.1016/j.jconrel.2022.03.023
190. Kabir SMF, Sikdar PP, Haque B, et al. Cellulose-based hydrogel materials: chemistry, properties and their prospective applications. Progress Biomater. 2018;7(3):153–174. doi:10.1007/s40204-018-0095-0
191. Baysal K, Aroguz AZ, Adiguzel Z, et al. Chitosan/alginate crosslinked hydrogels: preparation, characterization and application for cell growth purposes. Int J Biol Macromol. 2013;59:342–348. doi:10.1016/j.ijbiomac.2013.04.073
192. Wei D, Sun Y, Zhu H, et al. Stimuli-responsive polymer-based nanosystems for cancer theranostics. ACS Nano. 2023;17(23):23223–23261. doi:10.1021/acsnano.3c06019
193. Naeem M, Kim W, Cao J, et al. Enzyme/pH dual sensitive polymeric nanoparticles for targeted drug delivery to the inflamed colon. Colloids Surf B. 2014;123:271–278. doi:10.1016/j.colsurfb.2014.09.026
194. Joseph SK, Sabitha M, Nair SC. Stimuli-responsive polymeric nanosystem for colon specific drug delivery. Adv Pharm Bull. 2019;10(1):1. doi:10.15171/apb.2020.001
195. Pandey S, Joshi S, Tripathi P, et al. A review on targeting tunable nanocarrier interaction, physiochemical properties, and futuristic nanocarrier. Biochim Biophys Acta -Mol Basis Dis. 2025;1871(7):167956.
196. Grewal AK, Salar RK. Chitosan nanoparticle delivery systems: an effective approach to enhancing efficacy and safety of anticancer drugs. Nano Trans Med. 2024;3:100040. doi:10.1016/j.ntm.2024.100040
197. Bhatia S. Natural polymers vs synthetic polymer. In: Natural Polymer Drug Delivery Systems: Nanoparticles, Plants, and Algae. Springer; 2016:95–118.
198. Vasquez-Martínez N, Guillen D, Moreno-Mendieta SA, et al. The role of mucoadhesion and mucopenetration in the immune response induced by polymer-based mucosal adjuvants. Polymers. 2023;15(7):1615. doi:10.3390/polym15071615
199. Zheng B, Liu D, Qin X, et al. Mucoadhesive-to-mucopenetrating nanoparticles for mucosal drug delivery: a mini review. Int J Nanomed. 2025;20:2241–2252. doi:10.2147/IJN.S505427
200. Mura P, Maestrelli F, Cirri M, et al. Multiple roles of chitosan in mucosal drug delivery: an updated review. Mar Drugs. 2022;20(5):335. doi:10.3390/md20050335
201. Zong L, Xu H, Zhang H, et al. A review of matrix metalloproteinase-2-sensitive nanoparticles as a novel drug delivery for tumor therapy. Int J Biol Macromol. 2024;262:130043. doi:10.1016/j.ijbiomac.2024.130043
202. Kalli M, Poskus MD, Stylianopoulos T, et al. Beyond matrix stiffness: targeting force-induced cancer drug resistance. Trends Cancer. 2023;9(11):937–954.
203. Yao Q, Shi Y, Yao Y, et al. In situ forming hydrogels for colorectal cancer therapy. Mater Today Bio. 2025;35:102456. doi:10.1016/j.mtbio.2025.102456
204. Ivey JW, Bonakdar M, Kanitkar A, et al. Improving cancer therapies by targeting the physical and chemical hallmarks of the tumor microenvironment. Cancer Lett. 2016;380(1):330–339.
205. Sarwar S, Bashir S, Asim MH, et al. In-depth drug delivery to tumoral soft tissues via pH responsive hydrogel. RSC Adv. 2022;12(48):31402–31411.
206. Tahir H, Alanazi AK, Ahmad Z. Exploring the Functional Diversity of Hypoxia-Responsive Polymers in Drug Delivery: a Comparative Analysis. J Drug Delivery Sci Technol. 2026;117:108026. doi:10.1016/j.jddst.2026.108026
207. Zeng Y, Ma J, Zhan Y, et al. Hypoxia-activated prodrugs and redox-responsive nanocarriers. Int J Nanomed. 2018;13:6551–6574. doi:10.2147/IJN.S173431
208. Zhao D, Zhang Y, Yan Z, et al. Hypoxia-responsive polymeric nanoprodrugs for combo photodynamic and chemotherapy. ACS Omega. 2023;9(1):1821–1826. doi:10.1021/acsomega.3c08504
209. Gomaa EZ. Human gut microbiota/microbiome in health and diseases: a review. Antonie van Leeuwenhoek. 2020;113(12):2019–2040. doi:10.1007/s10482-020-01474-7
210. Zhang X, Han Y, Huang W, et al. The influence of the gut microbiota on the bioavailability of oral drugs. Acta Pharm Sin B. 2021;11(7):1789–1812. doi:10.1016/j.apsb.2020.09.013
211. Carrette O, Favier C, Mizon C, et al. Bacterial enzymes used for colon-specific drug delivery are decreased in active Crohn’s disease. Dig Dis Sci. 1995;40(12):2641–2646. doi:10.1007/BF02220454
212. Zalila-Kolsi I, Dhieb D, Osman HA, et al. The gut microbiota and colorectal cancer: understanding the link and exploring therapeutic interventions. Biology. 2025;14(3):251. doi:10.3390/biology14030251
213. Sánchez-Alcoholado L, Ramos-Molina B, Otero A, et al. The role of the gut microbiome in colorectal cancer development and therapy response. Cancers. 2020;12(6):1406. doi:10.3390/cancers12061406
214. Yeung C, McCoubrey LE, Basit AW. Advances in colon-targeted drug technologies. Curr Opin Gastroenterol. 2025;41(1):9–15. doi:10.1097/MOG.0000000000001064
215. Younas A, Wang S, Asad M, et al. Recent advances in cancer nanomedicine: from smart targeting to personalized therapeutics-pioneering a new era in precision oncology. Mater Today Bio. 2025;36:102660. doi:10.1016/j.mtbio.2025.102660
216. Ponta H, Sherman L, Herrlich PA. CD44: from adhesion molecules to signalling regulators. Nat Rev Mol Cell Biol. 2003;4(1):33–45. doi:10.1038/nrm1004
217. Ziranu P, Pretta A, Aimola V, et al. CD44: a new prognostic marker in colorectal cancer? Cancers. 2024;16(8):1569. doi:10.3390/cancers16081569
218. Todaro M, Gaggianesi M, Catalano V, et al. CD44v6 is a marker of constitutive and reprogrammed cancer stem cells driving colon cancer metastasis. Cell Stem Cell. 2014;14(3):342–356. doi:10.1016/j.stem.2014.01.009
219. Nicolazzo C, Loreni F, Caponnetto S, et al. Baseline CD44v6-positive circulating tumor cells to predict first-line treatment failure in patients with metastatic colorectal cancer. Oncotarget. 2020;11(45):4115. doi:10.18632/oncotarget.27794
220. Orian-Rousseau V. CD44 acts as a signaling platform controlling tumor progression and metastasis. Front Immunol. 2015;6:154. doi:10.3389/fimmu.2015.00154
221. Ma L, Dong L, Chang P. CD44v6 engages in colorectal cancer progression. Cell Death Dis. 2019;10(1):30. doi:10.1038/s41419-018-1265-7
222. Du W, Yang X, He S, et al. Novel hyaluronic acid oligosaccharide-loaded and CD44v6-targeting oxaliplatin nanoparticles for the treatment of colorectal cancer. Drug Delivery. 2021;28(1):920–929. doi:10.1080/10717544.2021.1914777
223. Petros RA, DeSimone JM. Strategies in the design of nanoparticles for therapeutic applications. Nat Rev Drug Discov. 2010;9(8):615–627. doi:10.1038/nrd2591
224. Nicolas J, Mura S, Brambilla D, et al. Design, functionalization strategies and biomedical applications of targeted biodegradable/biocompatible polymer-based nanocarriers for drug delivery. Chem Soc Rev. 2013;42(3):1147–1235. doi:10.1039/c2cs35265f
225. Wicki A, Witzigmann D, Balasubramanian V, et al. Nanomedicine in cancer therapy: challenges, opportunities, and clinical applications. J Control Release. 2015;200:138–157. doi:10.1016/j.jconrel.2014.12.030
226. Xu G, Shi H, Ren L, et al. Enhancing the anti-colon cancer activity of quercetin by self-assembled micelles. Int J Nanomed. 2015;10:2051–2063. doi:10.2147/IJN.S75550
227. Tiwari A, Saraf S, Jain A, et al. Basics to advances in nanotherapy of colorectal cancer. Drug Delivery Transl Res. 2020;10(2):319–338. doi:10.1007/s13346-019-00680-9
228. Debele TA, Lee K-Y, Hsu N-Y, et al. A pH sensitive polymeric micelle for co-delivery of doxorubicin and α-TOS for colon cancer therapy. J Mat Chem B. 2017;5(29):5870–5880. doi:10.1039/C7TB01031A
229. Wei Y, Gu X, Sun Y, et al. Transferrin-binding peptide functionalized polymersomes mediate targeted doxorubicin delivery to colorectal cancer in vivo. J Control Release. 2020;319:407–415. doi:10.1016/j.jconrel.2020.01.012
230. Ramezani P, Abnous K, Taghdisi SM, et al. Targeted MMP-2 responsive chimeric polymersomes for therapy against colorectal cancer. Colloids Surf B. 2020;193:111135. doi:10.1016/j.colsurfb.2020.111135
231. Asgharzadeh F, Moradi Binabaj M, Fanoudi S, et al. Lipid-based nanomedicine for colorectal cancer: progress and prospects. Alexandria Eng J. 2025;122:385–398. doi:10.1016/j.aej.2025.02.023
232. Al-Sahlawi F, Alabdali AY, Chinnappan S, et al. Polymer-based nanoparticles in targeted cancer therapy: a review. J Appl Pharm Sci. 2024;14(9):057–068.
233. Rao JP, Geckeler KE. Polymer nanoparticles: preparation techniques and size-control parameters. Prog Polym Sci. 2011;36(7):887–913. doi:10.1016/j.progpolymsci.2011.01.001
234. Tummala S, Kuppusamy G, Satish Kumar MN, et al. 5-Fluorouracil enteric-coated nanoparticles for improved apoptotic activity and therapeutic index in treating colorectal cancer. Drug Delivery. 2016;23(8):2902–2910. doi:10.3109/10717544.2015.1116026
235. Cabral H, Kataoka K. Progress of drug-loaded polymeric micelles into clinical studies. J Control Release. 2014;190:465–476. doi:10.1016/j.jconrel.2014.06.042
236. Chen Y, Wu Q, Song L, et al. Polymeric micelles encapsulating fisetin improve the therapeutic effect in colon cancer. ACS Appl Mater Interfaces. 2015;7(1):534–542. doi:10.1021/am5066893
237. Lee S-Y, Yang C-Y, Peng C-L, et al. A theranostic micelleplex co-delivering SN-38 and VEGF siRNA for colorectal cancer therapy. Biomaterials. 2016;86:92–105. doi:10.1016/j.biomaterials.2016.01.068
238. Ahmed F, Discher DE. Self-porating polymersomes of PEG–PLA and PEG–PCL: hydrolysis-triggered controlled release vesicles. J Control Release. 2004;96(1):37–53. doi:10.1016/j.jconrel.2003.12.021
239. Levine DH, Ghoroghchian PP, Freudenberg J, et al. Polymersomes: a new multi-functional tool for cancer diagnosis and therapy. Methods. 2008;46(1):25–32. doi:10.1016/j.ymeth.2008.05.006
240. Petersen MA, Hillmyer MA, Kokkoli E. Bioresorbable polymersomes for targeted delivery of cisplatin. Bioconjugate Chem. 2013;24(4):533–543. doi:10.1021/bc3003259
241. Longley DB, Harkin DP, Johnston PG. 5-fluorouracil: mechanisms of action and clinical strategies. Nat Rev Cancer. 2003;3(5):330–338. doi:10.1038/nrc1074
242. Köhne C-H, Bedenne L, Carrato A, et al. A randomised Phase III intergroup trial comparing high-dose infusional 5-fluorouracil with or without folinic acid with standard bolus 5-fluorouracil/folinic acid in the adjuvant treatment of stage III colon cancer: the Pan-European Trial in Adjuvant Colon Cancer 2 study. Eur J Cancer. 2013;49(8):1868–1875. doi:10.1016/j.ejca.2013.01.030
243. Schmoll H, Tabernero J, Maroun J, et al. Capecitabine plus oxaliplatin compared with fluorouracil/folinic acid as adjuvant therapy for stage iii colon cancer: final results of the NO16968 randomized controlled phase III trial. J Clin Oncol. 2015;33(32):3733–3740. doi:10.1200/JCO.2015.60.9107
244. Valencia PM, Basto PA, Zhang L, et al. Single-step assembly of homogenous lipid− polymeric and lipid− quantum dot nanoparticles enabled by microfluidic rapid mixing. ACS Nano. 2010;4(3):1671–1679. doi:10.1021/nn901433u
245. Choi SYC, Lin D, Gout PW, et al. Lessons from patient-derived xenografts for better in vitro modeling of human cancer. Adv Drug Delivery Rev. 2014;79–80:222–237. doi:10.1016/j.addr.2014.09.009
246. Bertrand N, Wu J, Xu X, et al. Cancer nanotechnology: the impact of passive and active targeting in the era of modern cancer biology. Adv Drug Deliv Rev. 2014;66:2–25.
247. Dhilip Kumar SS, Abrahamse H. Recent advances in the development of biocompatible nanocarriers and their cancer cell targeting efficiency in photodynamic therapy. Front Chem. 2022;10:969809.
248. Shi Y, van der Meel R, Chen X, et al. The EPR effect and beyond: strategies to improve tumor targeting and cancer nanomedicine treatment efficacy. Theranostics. 2020;10(17):7921. doi:10.7150/thno.49577
249. Phatak N, Bhattacharya S, Shah D, et al. CD44 targeted delivery of hyaluronic acid-coated polymeric nanoparticles against colorectal cancer. Nanomedicine. 2023;18(23):1613–1634. doi:10.2217/nnm-2023-0145
250. Liu X, Jiang J, Meng H. Transcytosis-An effective targeting strategy that is complementary to “EPR effect” for pancreatic cancer nano drug delivery. Theranostics. 2019;9(26):8018. doi:10.7150/thno.38587
251. Chen B, Dai W, He B, et al. Current multistage drug delivery systems based on the tumor microenvironment. Theranostics. 2017;7(3):538. doi:10.7150/thno.16684
252. Kang S, Lee S, Park S. iRGD peptide as a tumor-penetrating enhancer for tumor-targeted drug delivery. Polymers. 2020;12(9):1906. doi:10.3390/polym12091906
253. Ruoslahti E. Tumor penetrating peptides for improved drug delivery. Adv Drug Delivery Rev. 2017;110–111:3–12. doi:10.1016/j.addr.2016.03.008
254. Dikpati A, Maio VDP, Ates E, et al. Studying the stability of polymer nanoparticles by size exclusion chromatography of radioactive polymers. J Control Release. 2024;369:394–403. doi:10.1016/j.jconrel.2024.03.053
255. Yavari N, Azizian S. Mixed diffusion and relaxation kinetics model for hydrogels swelling. J Mol Liq. 2022;363:119861. doi:10.1016/j.molliq.2022.119861
256. Gatto MS, Najahi-Missaoui W. Lyophilization of nanoparticles, does it really work? Overview of the current status and challenges. Int J Mol Sci. 2023;24(18):14041. doi:10.3390/ijms241814041
257. Thang NH, Chien TB, Cuong DX. Polymer-based hydrogels applied in drug delivery: an overview. Gels. 2023;9(7):523. doi:10.3390/gels9070523
258. Vannoy CH, Tavares AJ, Noor MO, et al. Biosensing with quantum dots: a microfluidic approach. Sensors. 2011;11(10):9732–9763. doi:10.3390/s111009732
259. Neerooa BNHM, Ooi L-T, Shameli K, et al. Development of polymer-assisted nanoparticles and nanogels for cancer therapy: an update. Gels. 2021;7(2):60. doi:10.3390/gels7020060
260. Nunziata G, Borroni A, Rossi F. Advanced microfluidic strategies for core-shell nanoparticles: the next-generation of polymeric and lipid-based drug nanocarriers. Chem Eng J Adv. 2025;22:100759. doi:10.1016/j.ceja.2025.100759
261. Niculescu A-G, Grumezescu AM. Applications of chitosan-alginate-based nanoparticles—An up-to-date review. Nanomaterials. 2022;12(2):186. doi:10.3390/nano12020186
262. Jayan JS, Madhavikutty AS, Kumbhakar P, et al. Synthesis methods of chitosan nanoparticles: a review. Fundament Biomed Applicat Chitosan Nanoparticles. 2025;53–94.
263. Basu T, Goswami D, Majumdar S. Fabrication of crosslinker free hydrogels with diverse properties: an interplay of multiscale physical forces within polymer matrix. iscience. 2024;27(11):111227. doi:10.1016/j.isci.2024.111227
264. Sun F, Li Z, Kong S, et al. Linear and nonlinear interfacial rheology of responsive microgels at the oil-water interface. Food Hydrocoll. 2025;158:110479. doi:10.1016/j.foodhyd.2024.110479
265. Yang M, Yang L, Zheng J, et al. Mixing performance and continuous production of nanomaterials in an advanced-flow reactor. Chem Eng J. 2021;412:128565. doi:10.1016/j.cej.2021.128565
266. Maher S, Santos A, Kumeria T, et al. Multifunctional microspherical magnetic and pH responsive carriers for combination anticancer therapy engineered by droplet-based microfluidics. J Mat Chem B. 2017;5(22):4097–4109. doi:10.1039/C7TB00588A
267. Liu Y, Yang G, Hui Y, et al. Microfluidic nanoparticles for drug delivery. Small. 2022;18(36):2106580. doi:10.1002/smll.202106580
268. Donno R, Gennari A, Lallana E, et al. Nanomanufacturing through microfluidic-assisted nanoprecipitation: advanced analytics and structure-activity relationships. Int J Pharm. 2017;534(1–2):97–107. doi:10.1016/j.ijpharm.2017.10.006
269. Rizzo LY, De Lorenzi F, von Stillfried S, et al. Analysis of nanomedicine primary tumor vs. metastasis targeting using clinical-stage core-crosslinked polymeric micelles. Cell Rep. 2025;44(8):116086. doi:10.1016/j.celrep.2025.116086
270. Einen C, Snipstad S, Wesche HF, et al. Impact of the tumor microenvironment on delivery of nanomedicine in tumors treated with ultrasound and microbubbles. J Control Release. 2025;378:656–670. doi:10.1016/j.jconrel.2024.12.037
271. Zhang G, Liang Q, Wu Y, et al. Insights on the differences between two-and three-dimensional culture systems in tumor models. Int J Mol Med. 2025;56(5):185. doi:10.3892/ijmm.2025.5626
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.