Back to Journals » Journal of Inflammation Research » Volume 19
Narrative Review: Research Progress and Future Directions of Presepsin in Neurological Prognostication of Adult Post-Return of Spontaneous Circulation (Post-ROSC) Cardiac Arrest Survivors
Authors Liu M ![]() , Shao R, Liu B
, Shao R, Liu B ![]() , Tang Z
, Tang Z
Received 6 November 2025
Accepted for publication 19 January 2026
Published 28 January 2026 Volume 2026:19 571744
DOI https://doi.org/10.2147/JIR.S571744
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Dharmappa Krishnappa
Min Liu,1 Rui Shao,1 Bo Liu,2 Ziren Tang1
1Emergency Medicine Clinical Research Center, Beijing Chaoyang Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Department of Emergency Medicine, Beijing You’an Hospital, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Bo Liu; Email [email protected] Ziren Tang, Email [email protected]
Abstract: The assessment of neurological prognosis in patients after return of spontaneous circulation (ROSC) following cardiopulmonary resuscitation (CPR) is a critical challenge in critical care medicine. Current prognostic tools (eg, clinical scales, imaging, or traditional biomarkers) have limitations in early accuracy and specificity, leading to uncertainties in treatment decision-making and prognostic communication. Presepsin (soluble CD14 subtype), an emerging inflammation- and infection-related biomarker, has gained increasing attention due to its potential association with post-CPR neurological injury and functional recovery. To address the lack of a systematic synthesis of evidence in this field, this narrative review aims to summarize the biological characteristics of presepsin, its role in neurological prognostic assessment post-CPR, and the underlying mechanisms linking presepsin to neuroinflammation and brain injury. We conducted a narrative synthesis of clinical studies retrieved from PubMed, Embase, and Cochrane Library up to (December 2025, focusing on studies correlating presepsin levels with validated neurological outcome scales. Core findings from synthesized evidence indicate that elevated presepsin levels, particularly within 24– 72 hours after return of ROSC, show a consistent and significant association with poor neurological outcome (Cerebral Performance Category (CPC) 3– 5) and higher mortality, and presepsin may serve as an independent prognostic factor complementary to existing tools. Major clinical implications include presepsin’s potential utility in multimodal prognostic protocols, aiding in early and more accurate outcome prediction. However, significant research gaps persist, including a lack of large-scale, multicenter validation studies, standardized measurement timepoints, and consensus on optimal cutoff values. In conclusion, current evidence supports presepsin as a promising inflammatory biomarker for neurological prognostication after cardiac arrest (CA). Future research must prioritize prospective validation in diverse cohorts and investigate its dynamic changes to establish its definitive role in clinical decision-making.
Keywords: presepsin, cardiopulmonary resuscitation, neurological function, prognostic assessment, inflammatory marker
Introduction
Neurological dysfunction is the leading cause of long-term morbidity, disability, and mortality in patients who survive CA and successful CPR.1 Globally, over 340,000 out-of-hospital cardiac arrests (OHCAs) occur annually in the United States alone, with only 10% of patients surviving to discharge—and among survivors, 15–25% suffer permanent neurological impairment that compromises their quality of life and functional independence.2,3 Traditional methods of neurological function assessment, such as neuroimaging and clinical functional scoring, have certain reference value but often have limitations, especially in the early stages. Biomarkers have emerged as complementary tools to overcome these limitations, as they can objectively reflect the extent of brain injury and systemic pathophysiological responses. Historically, neuron-specific enolase (NSE) and S100 calcium-binding protein β (S100β) have been the most widely studied neurological biomarkers post-CA, but their sensitivity and specificity remain limited, and false negative or false positive results may occur in different situations.4 Other systemic markers, such as procalcitonin (PCT) and C-reactive protein (CRP), primarily reflect infection or general inflammation but do not specifically link to neurological injury mechanisms.5 Troponin, while useful for cardiac injury assessment, has no direct correlation with brain recovery.6 These limitations highlight the urgent need for a sensitive, specific, and mechanistically relevant biomarker to improve neurological prognostication post-CPR.
A core pathophysiological driver of post-CA neurological injury is global ischemia-reperfusion injury (IRI), which activates innate immunity by releasing damage-associated molecular patterns (DAMPs) that bind to TLR4 on monocytes.7 Presepsin, a soluble fragment of CD14 (sCD14-ST) first identified for sepsis diagnosis, is specifically released upon monocyte activation, directly reflecting this inflammatory cascade.8 As a biomarker of interest in recent years, it can reflect the body’s inflammatory response, and studies have shown it is associated with various acute brain injuries, especially in post-CPR patients. According to a systematic review, presepsin plays an important role in predicting neurological outcomes after CA, with its levels closely related to neurological recovery.9 Research has found that changes in presepsin levels at different time points are significantly correlated with clinical outcomes, laying the foundation for its application post-CPR.9–11
Notably, major guidelines such as the 2021/2023 European Resuscitation Council (ERC) Guidelines and 2020/2023 American Heart Association (AHA) Guidelines for post-cardiac arrest care do not yet recommend presepsin for routine neurological prognostication, citing inconsistent thresholds and limited comparative data with existing markers.12,13 This gap together with the need to clarify presepsin’s mechanistic link to neuroinflammation, warrants further exploration of its utility.
In summary, presepsin, as a potential biomarker reflecting monocyte activation and IRI-induced inflammation, may provide important reference for the neurological prognosis of post-CPR patients. This review aims to synthesize recent evidence on presepsin’s performance relative to traditional biomarkers, clarify its pathophysiological relevance to neurological injury, and evaluate its potential for integration into clinical practice. Future research will further explore presepsin’s application post-CPR brain function assessment and prognostic value, aiming to provide new ideas for improving post-CPR patient management and outcomes.
Biological Characteristics and Detection Methods of Presepsin
Molecular Structure, Source, and Physiological Function of Presepsin
Presepsin, also known as sCD14-ST, is an important biological marker primarily released by monocytes during infection and inflammatory states. Its molecular structure is a soluble fragment of the CD14 receptor, which has unique biological functions. CD14 is a pattern recognition receptor capable of recognizing bacterial lipopolysaccharides (LPS) and other pathogen-associated molecular patterns (PAMPs), thereby initiating the immune response of the body.14,15 During an infection, monocytes release presepsin through the phagocytosis of neutrophil extracellular traps (NETs), making presepsin an important indicator of the body’s immune response.16
Changes in the concentration of presepsin can sensitively reflect the body’s immune response and inflammation levels. Studies have shown that the levels of presepsin are significantly elevated in infected patients, particularly in cases of sepsis and severe infections.17 For example, in one study, when the concentration of presepsin exceeded 350 pg/mL, the sensitivity for diagnosing sepsis reached 80.2%, with even higher sensitivity for predicting 28-day mortality.18 Additionally, the concentration of presepsin is not only related to the severity of sepsis but is also closely linked to the patient’s pathological state and clinical outcomes, demonstrating its potential value in clinical applications.19
In vivo, the primary sources of presepsin are M1 macrophages in organs such as the lungs, liver, and kidneys, which significantly increase the production of presepsin during infection.16 Due to its sensitive response to bacterial infections, presepsin is widely used in the early diagnosis and assessment of various infections in clinical settings.20 Furthermore, presepsin has shown unique application potential under different infection conditions, such as neonatal sepsis, acute pancreatitis, and surgical site infections.21 Notably, recent studies have indicated that presepsin is not only involved in systemic inflammation but also closely associated with neurological injury. Its elevation can amplify the release of pro-inflammatory cytokines (eg, IL-6, TNF-α) that disrupt the blood-brain barrier and induce neuronal apoptosis, laying a pathological foundation for its role in post-CPR neurological prognostication.22
In summary, presepsin, as an emerging biological marker, plays an important role in the early diagnosis of infections and provides new means for evaluating inflammatory responses and prognostic judgments in clinical practice. In the future, with deeper research on presepsin, it is expected to find broader applications in various clinical scenarios.
Detection Technologies and Current Clinical Applications of Presepsin
Presepsin (sCD14-ST), as an emerging biological marker, is mainly detected through immunoassay methods, particularly enzyme-linked immunosorbent assay (ELISA) and chemiluminescent immunoassay (CLIA). These detection methods are widely used in clinical practice due to their rapidity and high accuracy, especially in the diagnosis of infectious diseases and sepsis. According to existing studies, the detection of presepsin can identify infections at an early stage, and its sensitivity and specificity are superior to traditional biological markers, such as CRP and PCT, in patients with liver disease.23 Research has shown significant correlations between presepsin levels and the severity of infections as well as clinical scores (such as SOFA and APACHE II scores), making presepsin a powerful tool for assessing infection risk and prognosis.
Presepsin has demonstrated broad clinical application potential in the diagnosis and prognostic evaluation of infectious diseases and sepsis. In a study involving patients with liver cirrhosis, it was found that presepsin outperformed traditional markers in the early detection of sepsis, particularly in patients with impaired liver function, maintaining its diagnostic value.23 Furthermore, presepsin has been used to monitor the occurrence of postoperative infections, such as in studies following esophagectomy, where levels of presepsin significantly increased in patients with anastomotic leaks, indicating its potential as an early infection indicator.24 In children and neonates, presepsin has also been shown to have good sensitivity and specificity in the early diagnosis of sepsis, especially when combined with other biomarkers (such as PCT and CRP), improving diagnostic accuracy.25 Notably, variability between detection platforms remains a non-negligible issue: ELISA offers lower cost but longer turnaround time (4–6 hours), while point-of-care (POC) systems enable rapid detection (30 minutes) but exhibit higher batch-to-batch variability (coefficient of variation [CV]: 8–12% vs 5–7% for ELISA) and are more susceptible to interference from hemolysis or lipidemia.26,27 This inconsistency may affect the comparability of results across studies and clinical institutions.
In conclusion, as a novel biological marker, the advancements in detection technology and widespread clinical applications of presepsin demonstrate its significant value in the early diagnosis and prognostic evaluation of infectious diseases and sepsis. Future research should continue to explore its application potential in various clinical scenarios.
Comparison of Presepsin with Other Inflammatory Markers
In recent years, presepsin has garnered attention as an emerging inflammatory marker for its performance in early diagnosis and dynamic monitoring. Traditional inflammatory markers, such as CRP and PCT, while widely used in clinical applications, still exhibit shortcomings in sensitivity and specificity in certain cases. For instance, CRP levels typically do not rise significantly until 24 hours post-infection, while PCT elevation may be influenced by non-infectious factors such as surgery or trauma.28
In contrast, presepsin’s superiority lies in its ability to rise significantly in the early stages of infection. Studies have shown that presepsin, as a soluble fragment of CD14, increases rapidly following bacterial infection, providing more timely diagnostic information in the early stages of infection.29 In a study involving patients with acute cholecystitis, presepsin was found to effectively differentiate between infected and non-infected states, with diagnostic accuracy significantly higher than that of CRP and PCT.30
Moreover, presepsin also outperforms traditional markers in dynamic monitoring. In a study of heart transplant recipients, presepsin levels could significantly increase in the early postoperative period, reflecting the occurrence of infection, while CRP and PCT showed significant changes only after a longer duration post-infection.31 This early responsiveness makes presepsin an important tool for monitoring infection progression and treatment effectiveness.
In comparison with other markers, presepsin also demonstrates good performance in specificity and sensitivity. For example, in a study involving COVID-19 patients, presepsin’s predictive capability ranked among the top of various inflammatory markers, indicating its significant value in assessing disease severity and prognosis. Additionally, when used in combination with CRP and PCT, Presepsin can enhance diagnostic accuracy for infectious diseases, especially in complex clinical situations where multiple inflammatory states coexist.32 However, presepsin exhibits notable limitations: its specificity is low in non-infectious inflammatory states (eg, sterile ischemia-reperfusion injury, postoperative aseptic inflammation), often leading to false-positive elevations that may mislead the judgment of neurological injury etiology post-CPR.33 Furthermore, its prognostic accuracy for pure neuronal damage is generally lower than that of neuro-specific biomarkers such as NSE and S100β.
In summary, presepsin’s superior performance in early diagnosis and dynamic monitoring marks it as a significant advancement in the field of inflammatory markers. Although traditional markers still hold important clinical application value, Presepsin’s unique advantages are gradually being recognized by the medical community, providing more precise tools for infection diagnosis and management in clinical practice. Future research should continue to explore the potential applications of Presepsin in different diseases and clinical contexts to promote its widespread use in clinical practice.
Supplementary Notes on Presepsin Detection Methods and Key Considerations
Presepsin (sCD14-ST) relies primarily on immunoassay techniques for serum detection, with ELISA and CLIA as the core methods, which are characterized by high sensitivity and specificity to effectively detect low concentrations of the marker in serum.34 Studies have shown that presepsin levels are significantly elevated in patients with sepsis, and measurements at different time points suggest that presepsin levels could serve as an early diagnostic indicator for sepsis.35 Notably, presepsin detection may help differentiate between bacterial and fungal infections, providing significant clinical guidance for treatment.
It is worth noting that renal dysfunction is a key confounder for presepsin detection, as presepsin is primarily excreted by the kidneys, and patients with acute or chronic kidney injury post-CA may present with falsely elevated levels independent of infection or neurological injury.36 This requires clinicians to integrate renal function assessment when interpreting presepsin results.
Overall, CLIA has become the preferred method for presepsin detection due to its high sensitivity, short detection time, and good specificity, demonstrating its potential value in clinical applications. With ongoing technological advancements, more improved detection methods may emerge in the future, providing clinicians with more accurate and efficient diagnostic tools.
Pathological Mechanisms of Brain Nerve Function Damage After CPR
Ischemia-Reperfusion Injury and Neuronal Death
Ischemia-reperfusion injury is a common pathological process following CPR, particularly affecting brain tissue. After CPR, brain tissue undergoes severe ischemia, followed by reperfusion, which triggers a series of pathophysiological reactions, including oxidative stress and apoptosis. These reactions not only cause direct damage to nerve cells but also exacerbate functional impairments in brain tissue following ischemia. In ischemic conditions, brain cells suffer from a lack of oxygen and nutrients, leading to impaired energy metabolism, compromised cell membrane integrity, and ultimately triggering cell death. After reperfusion, the sudden restoration of oxygen generates a substantial amount of reactive oxygen species (ROS), which further damages cells, leading to apoptosis and necrosis.37,38
Neuronal damage is considered the core pathological basis for brain dysfunction. Studies have shown that ischemia-reperfusion injury induces various mechanisms of cell death, including programmed cell death (such as apoptosis, necrosis, and autophagy).39,40 For example, following ischemia-reperfusion, intracellular calcium ion concentrations significantly increase, activating multiple apoptotic signaling pathways, ultimately leading to neuronal death.41 Additionally, extracellular inflammatory factors can exacerbate this process, further deteriorating the survival environment for nerve cells and creating a vicious cycle.
During ischemia-reperfusion, researchers have identified a new form of cell death—PANoptosis, which involves a complex process of apoptosis, necrosis, and inflammatory cell death.42 This pattern may play a significant role in neuronal ischemia-reperfusion injury, suggesting the need for in-depth research into different types of cell death mechanisms to find more effective treatment strategies.
Overall, ischemia-reperfusion injury following CPR is one of the primary causes of neuronal death. Understanding the pathological mechanisms involved in this process can provide new directions for clinical intervention. Future research should focus on the interactions between different cell death pathways and the potential role of targeted therapies in reducing neuronal damage.
The Role of Inflammatory Response in Brain Injury
In the pathological process of brain injury, the inflammatory response plays a crucial role. Following brain injury, the release of inflammatory mediators not only disrupts the blood-brain barrier but also exacerbates neuroinflammation. Research indicates that the initial stage of brain injury is accompanied by the release of numerous inflammatory factors, which activate local immune cells, forming a “cytokine storm.” For instance, in acute brain injury patients, elevated cytokine levels in cerebrospinal fluid correlate with poor neurological function, suggesting that the inflammatory response may be a key factor in the prognosis of brain injury.43 Additionally, inflammatory cytokines such as IL-1β and IL-6 are considered primary mediators of secondary injury, as they activate endogenous glial cells and exogenous immune cells, further aggravating neuronal damage.44,45 Notably, presepsin, as a downstream product of CD14/TLR4 activation during ischemia-reperfusion injury, directly amplifies this inflammatory cascade: it promotes monocytes/macrophages to secrete more IL-6, TNF-α, and IL-1β, which downregulate the expression of tight junction proteins (eg, occludin, claudin-5) in the blood-brain barrier, increasing its permeability.46 This allows peripheral inflammatory cells and harmful substances to infiltrate brain tissue, directly inducing neuronal apoptosis and exacerbating neuroinflammation.47
An important mechanism of the inflammatory response involves the activation of immune cells and their responses to neuronal injury. Studies have shown that the activation of microglia and macrophages significantly increases after brain injury, and the inflammatory mediators produced by these cells, such as tumor necrosis factor α (TNF-α) and interleukins (IL), lead to apoptosis and oxidative stress, thereby exacerbating neuronal damage.48 In ischemic brain injury models, therapeutic strategies targeting these inflammatory factors have been shown to improve neurological function and reduce mortality, such as alleviating the inflammatory response and cell death by inhibiting NLRP3 inflammasome activation.12
Moreover, following brain injury, the disruption of the blood-brain barrier allows peripheral immune cells to enter brain tissue, further exacerbating inflammation. The infiltration of peripheral immune cells is considered an important mechanism leading to secondary brain injury. Studies have found that the migration of peripheral immune cells is closely related to the inflammatory response after CPR, and the activation state of these cells is significantly correlated with patient prognosis.49,50 Therefore, the inflammatory response is not only a result of brain injury but also an important factor affecting the prognosis of brain injury.
In summary, the role of the inflammatory response in brain injury is complex and multifaceted, encompassing both protective effects against damage and exacerbating effects on the injury. Future research could focus on how to effectively regulate the inflammatory response to improve neurological functional prognosis after brain injury, exploring new therapeutic targets and strategies to provide more effective interventions for clinical practice.
The Balance Between Immune Regulation and Neural Repair
After CPR, the relationship between the patient’s immune response and neural repair becomes particularly complex. Specifically, the immune response can, to some extent, protect the body from infection and further damage, but it may also lead to tissue damage and functional impairment. Moreover, patients often experience a series of physiological and biochemical changes, including activation of inflammation. This inflammatory response is a natural reaction of the body to ischemia-reperfusion injury, which may initially have a protective effect but can cause secondary damage to the nervous system if it lasts too long or is too intense.51
The damaging effects of the immune response mainly manifest in the release of inflammatory mediators and the excessive production of cytokines. These inflammatory factors can affect the function of nerve cells through various mechanisms, leading to apoptosis, neuronal damage, and functional impairment. Additionally, the inflammatory response may trigger the disruption of the blood-brain barrier, allowing harmful substances to enter the central nervous system, further exacerbating neural injury. In this case, dysregulation of the immune response can lead to poor neurological functional prognosis for patients and increase the risk of neurological complications.52
However, the immune response is not entirely negative. Under appropriate circumstances, the immune system can also promote neural repair. Studies have shown that certain immune cells, such as macrophages and T cells, can play a role in repair after neural injury. These cells help restore damaged neural function by releasing neurotrophic factors and promoting regeneration and repair processes.53 For example, macrophages can transform into a repair-functional phenotype after injury, releasing a variety of cytokines to promote neuronal survival and regeneration. Therefore, the immune system plays an important role not only in the occurrence of neural injury after CPR but also in the process of neural repair.54
Clinically, patients after CPR often face the challenge of balancing the immune response and neural repair. How to modulate this balance to reduce damage and promote repair is key to improving prognosis. Researchers are exploring various strategies, such as using immunomodulators, anti-inflammatory drugs, or cell therapies, in hopes of achieving this balance in early interventions after CPR.55 Through these interventions, it is possible to reduce the inflammatory response and enhance the ability for neural repair, thereby improving the neurological functional prognosis of patients. In summary, the immune response plays a dual role in the process of neural injury and repair after CPR. Presepsin may serve as a “switch” reflecting the balance of this immune response—moderate elevation indicates effective activation of the protective immune response, while excessive and persistent elevation suggests uncontrolled inflammation that hinders neural repair.56,57 Understanding its complex interrelationship can provide new ideas and directions for clinical treatment. Future research focusing on the balance between immune regulation and neural repair, as well as how to utilize this balance to improve patient prognosis, will be an important area of study.
Research Progress of Presepsin in Neurological Functional Prognosis After CPR
Current Status of Clinical Research and Data Analysis
In recent years, research on presepsin as a biomarker for neurological functional prognosis in patients after CPR has gradually gained attention. Some studies have indicated a possible negative correlation between plasma presepsin levels in patients after CPR and neurological functional scores. This suggests that higher presepsin levels may correlate with lower neurological functional scores, indicating its potential as an important indicator for assessing neurological functional prognosis after CPR. Researchers have monitored plasma presepsin levels at different time points after CPR and found that it can significantly increase in the early stages post-resuscitation, closely related to the patients’ neurological recovery.9
Specifically, some studies have utilized neurological functional scores such as CPC to assess patient prognosis and explored the relationship between presepsin levels and neurological functional scores through statistical analysis methods.58 Results showed a significant negative correlation between the elevation of presepsin levels and the decrease of CPC scores within 24 hours post-CPR.9 This finding provides new insights and evidence for clinicians in assessing patient prognosis after CPR, helping them identify potentially high-risk patients earlier.
Moreover, the elevation of presepsin levels is not only associated with poor neurological prognosis but is also closely related to increased mortality in patients. In a large-scale prospective study, researchers observed that presepsin levels in surviving patients after CPR were significantly lower than in those who unfortunately died, further emphasizing the importance of Presepsin in clinical applications.59 However, Some studies have raised critical concerns about its clinical utility. One study involving 277 OHCA patients reported that presepsin’s area under the curve (AUC) for predicting 12-month poor neurological outcomes (CPC 3–5) was only 0.72, significantly lower than that of PCT (0.76).58 Another unresolved issue is the lack of standardized cut-off values, making cross-study comparisons and clinical translation difficult.60
Through a comprehensive analysis of existing research data, it can be seen that presepsin can serve as a predictive indicator of neurological functional prognosis after CPR and may play an important role in the early identification of high-risk patients and guiding clinical decision-making. However, current studies still have certain limitations, such as small sample sizes and insufficiently rigorous study designs. Therefore, future research should further validate the clinical application value of presepsin on a large scale and in multi-center studies, as well as explore its applicability in different patient populations. Additionally, further investigation into the biological mechanisms of presepsin is needed to better understand its role in neurological functional prognosis after CPR.
Advantages of Presepsin as an Early Prognostic Indicator
In patients after CPR, prognosis assessment is a critical clinical decision-making process. Presepsin, as an emerging biomarker, has gained attention for its rapid detection and early reflection of inflammatory states. Presepsin is a precursor of soluble CD14 subtype, and its concentration significantly increases in infection states, with detection that can be completed in a short time, making it advantageous in clinical settings. For instance, one study pointed out that Presepsin demonstrated high sensitivity and specificity in diagnosing acute biliary infections, with an AUC reaching 0.823, showcasing its potential for prognostic assessment in severe infections.61 Additionally, the short detection time of presepsin can quickly provide essential information to medical personnel during clinical emergencies, allowing timely adjustments to treatment plans and improving patient survival chances.62
When combined with traditional neurological functional assessment tools, presepsin can significantly enhance the accuracy of prognostic judgments. Traditional indicators such as CRP and PCT have certain applications in inflammation assessment, but their response times are relatively long and may be affected by other factors in some cases.63 In contrast, presepsin not only reflects systemic inflammatory responses but can also be used in conjunction with other scoring systems (such as SOFA scores) to further improve prognostic judgment accuracy. One study showed that combining presepsin with SOFA scores significantly improved predictive capability for 28-day mortality, with an AUC value reaching 0.747, indicating its important role in clinical evaluation.64
In summary, the advantages of presepsin as an early prognostic indicator lie in its rapid detection, ability to early reflect inflammatory states, and enhanced accuracy when used in combination with traditional neurological functional assessments. These characteristics demonstrate presepsin’s immense potential in managing patients after CPR, particularly in assessing neurological functional prognosis, providing a more reliable basis for clinical decision-making. Future research should continue to explore the application of presepsin in different patient populations, evaluating its effectiveness and reliability in specific clinical contexts to further promote its widespread use in clinical practice.
Combined Application of Presepsin and Other Neurological Injury Biomarkers
In monitoring patients after CPR, prognostic assessment is a crucial aspect. In recent years, Presepsin has been widely studied as an emerging biomarker for its potential in assessing neurological injuries. Using Presepsin in conjunction with traditional neurological injury markers, such as NSE and S100β protein, can enhance the sensitivity and specificity of predicting patient prognosis. Presepsin levels have been found to significantly increase in severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)-related cardiovascular injuries, indicating its application potential in assessing neurological functional prognosis after CPR.65
NSE is a specific marker of neuronal injury, with elevations typically directly related to the severity of brain damage. S100β reflects damage to glial cells, with its level changes associated with inflammatory responses in the nervous system. By combining the detection results of presepsin with these biomarkers, it may be possible to improve the recognition rate of brain injuries, thereby enhancing patient prognostic assessments. The effectiveness of multi-biomarker combined detection strategies has been validated in multiple studies.66 This helps to overcome the limitations of single markers regarding specificity and sensitivity, forming a more reliable prognostic assessment model.65
To clarify the comparative characteristics of Presepsin and other common biomarkers in post-CPR neurological prognostication, Table 1 summarizes their key performance parameters:
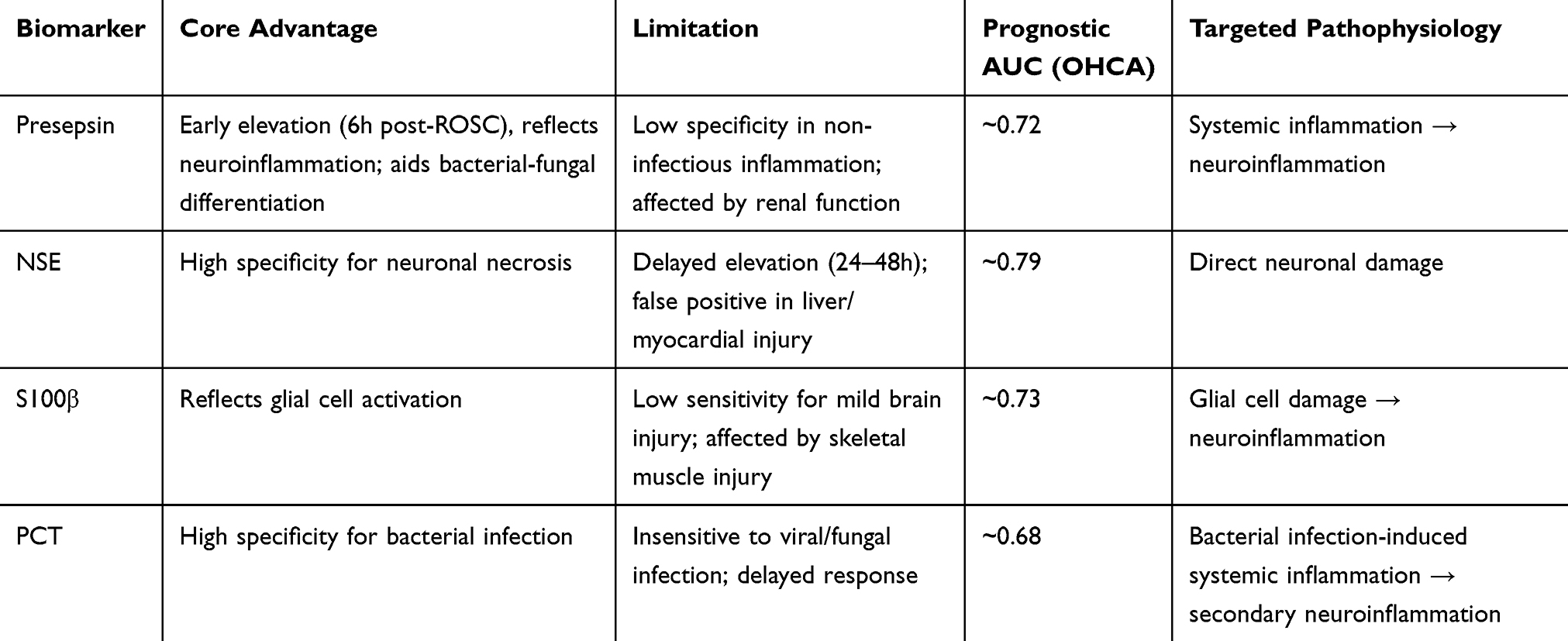 |
Table 1 Comparison of Presepsin with NSE, S100B, and PCT |
Future research directions should focus on further validating the joint application effectiveness of presepsin with other neurological injury biomarkers and exploring how to promote this multi-biomarker detection strategy as a clinical standard. Through large-scale clinical trials, assessing its application effects in different patient types can provide a more solid evidence base for clinical practice. Additionally, with advancements in detection technology, how to enhance the sensitivity and specificity of these biomarkers is also an important topic for future research. In summary, the combined application of presepsin with other neurological injury markers holds great promise for improving prognostic assessments in patients after CPR. The combined application of physical entities holds vast clinical application prospects and is expected to become a standardized strategy for the assessment of neurological prognosis in patients after CPR.
Limitations of Presepsin in Neurological Prognostication Post-CPR
Despite its potential, presepsin has several unresolved limitations that restrict its routine clinical application and require explicit recognition: Low specificity in non-infectious inflammation: Presepsin can be elevated in sterile ischemia-reperfusion injury, postoperative aseptic inflammation, or autoimmune diseases, leading to false-positive signals that may misclassify the etiology of neurological dysfunction post-CPR.64 Confounding by renal function: As a kidney-excreted biomarker, Presepsin levels are significantly elevated in patients with acute kidney injury or chronic renal insufficiency, independent of infection or neurological injury, which may interfere with prognostic judgment.67 Inferior specificity to neuro-specific biomarkers: For pure neuronal damage without systemic inflammation, its prognostic accuracy is lower than that of NSE and S100β.68
Future Research Directions and Clinical Application Prospects
Deepening Mechanism Research
Presepsin is a biomarker released during inflammatory responses, showing significant clinical relevance in assessing neurological prognosis in patients after CPR. To better understand the role of presepsin in neurological injury, it is crucial to delve into its specific mechanisms of action.
Furthermore, the role of presepsin is not limited to inflammatory responses; it may also be closely linked to the apoptosis of neural cells. Studies have found that ischemia-reperfusion injury following CPR can lead to the apoptosis of neural cells,69 and the elevation of presepsin may serve as an important marker of this process. By exploring apoptosis-related signaling pathways in depth, researchers can reveal how presepsin influences the survival and death of neural cells. For example, presepsin may affect the process of apoptosis by regulating the expression of Bcl-2 family proteins, which play a critical role in apoptosis. Investigating the interaction between Bcl-2 family proteins and presepsin will help elucidate its specific mechanisms in neurological injury.70
At the same time, the integrity of the blood-brain barrier is vital for maintaining normal neurological function. Following CPR, the disruption of the blood-brain barrier can allow harmful substances to enter the central nervous system, exacerbating neurological damage. The elevation of presepsin may be closely related to the disruption of the blood-brain barrier. Research indicates that inflammatory factors can increase the permeability of the blood-brain barrier,71 and as an inflammatory marker, presepsin may play a significant role in this process. Future research should focus on how presepsin affects the expression of tight junction proteins, such as occludin and claudin-5, thereby influencing the function of the blood-brain barrier. These studies will provide new insights for clinical applications and help develop interventions targeting presepsin to improve the neurological prognosis of patients after CPR. Notably, the interaction between presepsin and renal function requires further clarification, whether renal dysfunction simply affects its excretion or actively participates in presepsin-mediated neuroinflammation remains unclear.72 Resolving this issue will help optimize the interpretation of presepsin results in clinical practice.
In summary, the mechanisms of presepsin in neurological injury following CPR still require further investigation. By clarifying the specific roles of presepsin in inflammatory pathways, neural cell apoptosis, and blood-brain barrier disruption, researchers hope to identify new biomarkers and therapeutic targets for improving patient prognosis.
Large-Scale, Multi-Center Clinical Validation
Assessing the neurological prognosis after CPR is an essential part of clinical work. Presepsin, as an emerging biomarker, is gradually recognized for its potential in evaluating the prognosis of septic patients. To further validate the clinical value of presepsin in assessing neurological prognosis in patients after CPR, designing a prospective, multi-center clinical trial is particularly important. This study design can collect data from different hospitals and populations, thereby enhancing the generalizability and applicability of the research findings.
Firstly, the study should clearly define the inclusion criteria, including patients in various clinical statuses after ROSC, such as those with good recovery of consciousness, coma, or vegetative state. Secondly, the study needs to collect participants’ presepsin levels, clinical scores (eg, GCS scores), and other relevant biomarker values for comprehensive analysis. Studies have shown that presepsin levels are closely related to patient prognosis. For example, elevated presepsin levels may correlate with poorer outcomes,73 thus, in the multi-center trial, the relationship between different Presepsin levels and the final recovery of brain function can be assessed to evaluate its clinical value.
Additionally, determining the optimal detection window and critical value is also a key aspect of this study. Previous studies suggest that dynamic changes in presepsin may affect its effectiveness as a prognostic indicator.74 Therefore, the research should be designed to collect samples at different time points after CPR (eg, 0 hours, 6hours, 12hours, 24 hours, 48 hours, 72 hours after admission) to observe the changes in Presepsin levels over time and their impact on prognosis.
Finally, through data analysis, statistical models can be used to determine the optimal critical value for presepsin. For instance, ROC curve analysis can be utilized to assess the sensitivity and specificity of presepsin and compare it with other commonly used biomarkers (eg, CRP and PCT) to further evaluate its unique value in prognostic assessment.75 The results of this multi-center clinical trial can provide empirical support for the effectiveness of presepsin in clinical applications and lay the groundwork for future clinical guidelines.
At the same time, by comparing the results of presepsin detection across different time windows with clinical outcomes (such as neurological function scores, length of hospital stay, mortality, etc)., empirical evidence can be provided for determining the optimal detection window. Additionally, the study should consider the heterogeneity of different patient populations, such as age, underlying diseases, and methods of CPR, as these factors may influence presepsin levels and clinical significance.76
Regarding determining critical values, ROC curve analysis can be used to evaluate the sensitivity and specificity of different presepsin levels to find the optimal critical value. For example, one study found that presepsin at a specific level (eg, 600 pg/mL) could effectively distinguish between patients with good and poor clinical outcomes.77 Through this process, clear indicators can be provided for clinicians to better assess patient prognosis in practical applications.
In summary, through the design of prospective, multi-center clinical trials, combined with the clarification of optimal detection windows and critical values, the clinical application standardization of presepsin in assessing neurological prognosis in patients after ROSC can be effectively improved. This will provide a solid foundation for the widespread application of presepsin as a neurological prognosis indicator in future clinical practice.
Comprehensive Assessment Combined with Multi-Modal Monitoring Technologies
In managing patients after ROSC, accurately assessing neurological prognosis is a critical issue. In recent years, Presepsin, as a novel biomarker, has shown promising prospects in monitoring inflammation and infection. Combining presepsin detection with other neuroimaging and electroencephalography (EEG) multi-modal monitoring technologies is expected to establish a comprehensive multi-dimensional assessment system, thereby improving the predictive accuracy of neurological prognosis for patients and providing guidance for individualized treatment.
Firstly, neuroimaging techniques, such as magnetic resonance imaging (MRI) and computed tomography (CT), can provide detailed information about brain tissue structure and function. These imaging results can be correlated with presepsin levels to help doctors better understand the extent of potential brain injury in patients after CPR. By analyzing imaging data combined with the trends in presepsin levels, the biological mechanisms of brain injury can be revealed, optimizing treatment plans. For instance, high presepsin levels may correlate with the severity of brain ischemia or inflammatory responses, while imaging examinations can reveal the specific location and extent of brain tissue damage; the combination of these two will provide more comprehensive clinical information.
Secondly, EEG, as a non-invasive monitoring tool, can reflect the electrical activity state of the brain in real time. After CPR, patients’ EEGs often exhibit abnormal changes, such as low voltage or nonspecific waveforms, which may closely relate to neurological prognosis. By combining presepsin with EEG results, doctors can gain deeper insights into the electrophysiological changes of the brain during the resuscitation process, enabling more accurate prognostic assessments. For example, certain specific EEG patterns may coincide with higher presepsin levels, indicating a higher risk of neural damage in the patient.
Moreover, the integration of multiple monitoring technologies into a comprehensive assessment system can enhance the guidance capacity for individualized treatment. In clinical practice, patient responses may vary due to individual differences, and a single biomarker or detection method may not fully reflect the true situation of the patient. By integrating presepsin, neuroimaging, and EEG, doctors can tailor more precise treatment plans based on the specific conditions of patients. This individualized treatment strategy not only helps improve treatment outcomes but also reduces unnecessary medical costs and the psychological burden on patients.
To address the limitations of single biomarkers, we propose a preliminary “stepwise prognostication pathway” for post-ROSC patients: (1) Early screening (6h post-ROSC): Detect presepsin and assess renal function to identify high-risk patients with excessive inflammation, excluding renal-related false positives; (2) Prognostic refinement (24–48h post-ROSC): Combine with NSE/S100B to improve the specificity for neuronal damage; (3) Confirmation (72h post-ROSC): Integrate with MRI (diffusion-weighted imaging) and EEG to finalize prognosis stratification. This multi-step approach balances presepsin’s early warning advantage and the specificity of neuro-specific markers/imaging.
In summary, combining presepsin detection with multi-modal monitoring technologies provides new insights for the assessment of neurological prognosis in patients after CPR. Establishing this comprehensive assessment system not only enhances the accuracy of prognostic predictions but also aids in providing individualized guidance for clinical treatment, thus improving the overall prognosis of patients. Future research should further explore the joint application of presepsin with other biomarkers and the applicability of multi-modal monitoring technologies in different patient populations, which will be a worthwhile direction of study.
Exploration of Prognostic Interventions and Therapeutic Targets
Elevated levels of presepsin are typically closely associated with the activation of infection, inflammation, and immune responses, making it significant for prognostic assessment in patients after CPR. Research indicates that the inflammatory state of patients after CPR is directly related to the effectiveness of neurological recovery,11 hence exploring inflammation modulation intervention strategies based on presepsin levels may improve neurological recovery in patients following CPR.
Currently, studies show that presepsin levels positively correlate with changes in various inflammatory factors, such as C-reactive protein and IL-6.78 These increase in factors is often accompanied by the emergence of a cytokine storm, which causes secondary damage to neural tissues. Therefore, intervention strategies targeting presepsin levels may include the use of anti-inflammatory drugs or drugs that modulate immune responses to reduce inflammatory states, thereby facilitating the recovery of neural functions. For example, some studies have shown that in cases using anti-CD14 antibodies, presepsin levels can be significantly reduced, thereby inhibiting the activation of the inflammatory response.79
In addition, inflammation regulation strategies based on presepsin may also include individualized nutritional support and appropriate rehabilitation training, combined with clinical observation and dynamic monitoring of biomarkers. These comprehensive intervention measures aim to reduce the risk of neurological dysfunction in patients after CPR through early identification and optimized treatment, thereby improving overall prognosis.
Presepsin is not only a biomarker of inflammation, but its role in cellular signaling is also gradually being revealed. Research has found that presepsin can activate multiple signaling pathways, such as the NF-κB and MAPK pathways, after binding to the CD14 receptor, thereby triggering a series of inflammatory responses and cell death.80 Therefore, in-depth studies of presepsin-related signaling pathways can help us understand its mechanisms in inflammation and neural injury, and may provide new targets for the development of novel neuroprotective drugs.
Current research indicates that inhibiting presepsin-related signaling pathways may help reduce neural cell damage in patients after CPR. For example, by inhibiting the activation of the NF-κB pathway, the release of inflammatory factors can be reduced, thereby alleviating damage to the nervous system.81 Moreover, developing monoclonal antibodies or small molecule inhibitors targeting presepsin could achieve more precise interventions, minimizing secondary injuries caused by inflammatory responses, which is significant for improving the neurological functional prognosis of patients after CPR.
In conclusion, research based on presepsin not only provides a new biomarker for assessing the prognosis of patients after ROSC but also opens up new research directions for the development of novel neuroprotective drugs. Future research should focus on exploring the mechanisms of presepsin and its signaling pathways, aiming to provide more effective intervention strategies for clinical treatment.
Conclusion
As an emerging inflammatory biomarker, presepsin has shown promising but investigational value in assessing neurological prognosis after CA). Current evidence, predominantly from single-center studies, indicates a consistent association between elevated presepsin levels (especially within 48–72 hours post-ROSC) and poor neurological outcome, with predictive performance often comparable to that of NSE. This provides a compelling, though not yet definitive, rationale for its prognostic utility.
However, significant limitations preclude its current inclusion in clinical practice guidelines. Key constraints include the predominance of studies with small sample sizes, heterogeneity in sampling timing and assay methods, lack of standardized prognostic thresholds, and insufficient adjustment for major confounders such as renal function and the presence of concurrent infection. Crucially, its added value within established multimodal prognostication protocols (combining clinical examination, neurophysiology, and imaging) remains unproven.
Therefore, future research must prioritize specific, actionable steps to translate this potential into clinical practice: Standardization and Validation: Conduct large-scale, prospective multicenter studies to validate assay-specific cut-offs and define the optimal measurement timepoints, with separate analyses for OHCA and in-hospital (IHCA) cardiac arrest populations; Mechanistic and Comparative Clarity: Elucidate presepsin’s specific role in post-CA neuroinflammation versus systemic infection, and determine its independent prognostic contribution relative to and in combination with NSE, S100β, and other biomarkers; Integration into Clinical Pathways: Develop and test practical prognostic algorithms that integrate presepsin with multimodal parameters (eg, EEG, brain imaging, and clinical scores) to assess its ability to improve the accuracy and confidence of neuroprognostication.
In summary, presepsin is a promising candidate biomarker that may refine post-cardiac arrest neuroprognostication. Its path to routine clinical adoption, however, requires rigorous validation, standardization, and evidence of clear incremental value within the existing multimodal prognostic framework before it can be considered for guideline implementation.
Data Sharing Statement
Data sharing is not applicable to this article as no data were created or analysed in this study.
Author Contributions
All authors have made significant contributions to the work reported, Dr Ziren Tang contributed to conceptualization, funding acquisition, resources, and supervision. Dr Bo Liu was involved in methodology and investigation. Dr Rui Shao contributed to project administration, formal analysis, and verification. Dr Min Liu was responsible for visualization and writing. All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Beijing Hospitals Authority’s Ascent Plan (DFL20240302)and Beijing Municipal Science & Technology Commission, Administrative Commission of Zhongguancun Science Park (No.Z251100006025022).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Macherey-Meyer S, Heyne S, Meertens MM, et al. Restrictive versus high-dose oxygenation strategy in post-arrest management following adult non-traumatic cardiac arrest: a meta-analysis. Critical Care. 2023;27(1):387. doi:10.1186/s13054-023-04669-2
2. Jerkeman M, Sultanian P, Lundgren P, et al. Trends in survival after cardiac arrest: a Swedish nationwide study over 30 years. Eur Heart J. 2022;43:4817–14. doi:10.1093/eurheartj/ehac414
3. Virani SS, Alonso A, Aparicio HJ, et al. Heart disease and stroke statistics-2021 update: a report from the American heart association. Circulation. 2021;143:e254–e743. doi:10.1161/CIR.0000000000000950
4. Wang CH, Chang W-T, Su K-I, et al. Neuroprognostic accuracy of blood biomarkers for post-cardiac arrest patients: a systematic review and meta-analysis. Resuscitation. 2020;148:108–117. doi:10.1016/j.resuscitation.2020.01.006
5. Pink I, Raupach D, Fuge J, et al. C-reactive protein and procalcitonin for antimicrobial stewardship in COVID-19. Infection. 2021;49:935–943. doi:10.1007/s15010-021-01615-8
6. Prandin G, Furlanis G, Mancinelli L, et al. Stroke heart injury: the effect of cerebral reperfusion treatment. A 3-year retrospective study. J Neurol. 2024;271:5969–5975. doi:10.1007/s00415-024-12531-w
7. Wada T. Coagulofibrinolytic changes in patients with post-cardiac arrest syndrome. Front Med. 2017;4:156. doi:10.3389/fmed.2017.00156
8. Velissaris D, Zareifopoulos N, Karamouzos V, et al. Presepsin as a Diagnostic and Prognostic Biomarker in Sepsis. Cureus. 2021;13:e15019. doi:10.7759/cureus.15019
9. Qi Z, Zhang Q, Liu B, Shao F, Li C. Presepsin as a biomarker for evaluating prognosis and early innate immune response of out-of-hospital cardiac arrest patients after return of spontaneous circulation. Crit Care Med. 2019;47:e538–e546. doi:10.1097/CCM.0000000000003764
10. Popov D, Plyushch M, Ovseenko S, et al. Prognostic value of sCD14-ST (presepsin) in cardiac surgery. Kardiochirurgia i torakochirurgia polska. 2015;12:30–36. doi:10.5114/kitp.2015.50565
11. Masson S, Caironi P, Fanizza C, et al. Circulating presepsin (soluble CD14 subtype) as a marker of host response in patients with severe sepsis or septic shock: data from the multicenter, randomized ALBIOS trial. Intensive Care Med. 2015;41:12–20. doi:10.1007/s00134-014-3514-2
12. Soar J, Böttiger BW, Carli P, et al. European resuscitation council guidelines 2021: adult advanced life support. Resuscitation. 2021;161:115–151. doi:10.1016/j.resuscitation.2021.02.010
13. Perman SM, Elmer J, Maciel CB, et al. 2023 American Heart Association focused update on adult advanced cardiovascular life support: an update to the American heart association guidelines for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation. 2024;149:e254–e273. doi:10.1161/CIR.0000000000001194
14. Takahashi G, Hoshikawa K, Suzuki R, et al. Development of a newly immunoassay specific for mouse presepsin (sCD14-ST). Sci Rep. 2022;12:21724. doi:10.1038/s41598-022-22096-1
15. Luo R, Yao Y, Chen Z, Sun X. An examination of the LPS-TLR4 immune response through the analysis of molecular structures and protein-protein interactions. Cell Commun Signaling. 2025;23:142. doi:10.1186/s12964-025-02149-4
16. Kondo A, Morinishi T, Yamaguchi Y, Ikegame A. Identification of organs of origin of macrophages that produce presepsin via neutrophil extracellular trap phagocytosis. Sci Rep. 2024;14:16386. doi:10.1038/s41598-024-66916-y
17. Mussap M, Puxeddu E, Burrai P, et al. Soluble CD14 subtype (sCD14-ST) presepsin in critically ill preterm newborns: preliminary reference ranges. J Matern Fetal Neonatal Med. 2012;25:51–53. doi:10.3109/14767058.2012.717462
18. Kyriazopoulou E, Leventogiannis K, Tavoulareas G, et al. Presepsin as a diagnostic and prognostic biomarker of severe bacterial infections and COVID-19. Sci Rep. 2023;13:3814. doi:10.1038/s41598-023-30807-5
19. Carpio R, Zapata J, Spanuth E, Hess G. Utility of presepsin (sCD14-ST) as a diagnostic and prognostic marker of sepsis in the emergency department. Int J Clin Chem. 2015;450:169–175. doi:10.1016/j.cca.2015.08.013
20. Koizumi Y, Sakanashi D, Mohri T, et al. Can presepsin uniformly respond to various pathogens? - An in vitro assay of new sepsis marker. BMC Immunology. 2020;21:33. doi:10.1186/s12865-020-00362-z
21. Vicenti G, Solarino G, Bizzoca D, et al. The limits and potentials of presepsin in orthopaedic surgery: state of the art and future directions. J Biol Regul Homeost Agents. 2020;34:259–262.
22. Üstündağ H, Kara A, Gökhan Taş N, et al. Alleviation of LPS-induced acute lung injury by propolis-based nanocomposites through the TLR4/NFKB and P2X7/AKT pathways: randomized-controlled experimental study. Toxicon. 2025;258:108330. doi:10.1016/j.toxicon.2025.108330
23. Bilous DM, Ciocîrlan M, Vlăduț C, Fierbințeanu-Braticevici CG. Presepsin in hepatic pathology: bridging the gap in early sepsis detection. Diagnostics. 2025;15:1871. doi:10.3390/diagnostics15151871
24. Imai Y, Tanaka R, Matsuo K, et al. The usefulness of presepsin in the early detection of anastomotic leakage after esophagectomy. Surg Open Sci. 2025;23:75–80. doi:10.1016/j.sopen.2025.01.003
25. Piccioni A, Santoro MC, de Cunzo T, et al. Presepsin as early marker of sepsis in emergency department: a narrative review. Medicina. 2021;57:770. doi:10.3390/medicina57080770
26. Prat-Trunas J, Arias-Alpizar K, Álvarez-Carulla A, et al. Paper-based microfluidic electro-analytical device (PMED) for magneto-assay automation: towards generic point-of-care diagnostic devices. Biosens Bioelectron. 2024;246:115875. doi:10.1016/j.bios.2023.115875
27. Bonazzi E, Maniero D, Lorenzon G, et al. Comparing point-of-care technology to ELISA testing for infliximab and adalimumab levels in adult inflammatory bowel disease patients: a prospective pilot study. Diagnostics. 2024;14:2140. doi:10.3390/diagnostics14192140
28. Lee EH, Lee KH, Song YG, Han SH. Discrepancy of C-reactive protein, procalcitonin and interleukin-6 at hospitalization: infection in patients with normal C-reactive protein, procalcitonin and high interleukin-6 values. J Clin Med. 2022;11:7324. doi:10.3390/jcm11247324
29. Piccioni A, Baroni S, Rozzi G, et al. Evaluation of presepsin for early diagnosis of sepsis in the emergency department. J Clin Med. 2025;14:2480. doi:10.3390/jcm14072480
30. Gedik MS, Kilci AI, Hakkoymaz H, et al. The role of ischemia-modified albumin, presepsin, delta neutrophil index, and inflammatory markers in diagnosing acute cholecystitis. Ulusal Travma Acil Cerrahi Dergisi. 2024;30:242–247. doi:10.14744/tjtes.2024.67520
31. Giovannico L, Santobuono VE, Fischetti G, et al. Kinetics of procalcitonin, CRP, IL-6, and presepsin in heart transplant patients undergoing induction with thymoglobulin (rATG). J Clin Med. 2025;14:5369. doi:10.3390/jcm14155369
32. Ghenu MI, Dragoș D, Manea MM, et al. The pivotal role of presepsin in assessing sepsis-induced cholestasis. Diagnostics. 2024;14:1706. doi:10.3390/diagnostics14161706
33. Amanai E, Nakai K, Saito J, et al. Usefulness of presepsin for the early detection of infectious complications after elective colorectal surgery, compared with C-reactive protein and procalcitonin. Sci Rep. 2022;12:3960. doi:10.1038/s41598-022-06613-w
34. Ferrarese A, Frigo AC, Mion MM, et al. Diagnostic and prognostic role of presepsin in patients with cirrhosis and bacterial infection. Clin Chem Lab Med. 2021;59:775–782. doi:10.1515/cclm-2020-1212
35. Jereb M, Mavric M, Skvarc M, et al. Usefulness of presepsin as diagnostic and prognostic marker of sepsis in daily clinical practice. J Infect Developing Countries. 2019;13:1038–1044. doi:10.3855/jidc.11764
36. Saito J, Hashiba E, Kushikata T, Mikami A, Hirota K. Changes in presepsin concentrations in surgical patients with end-stage kidney disease undergoing living kidney transplantation: a pilot study. Journal of Anesthesia. 2016;30:174–177. doi:10.1007/s00540-015-2065-1
37. Yan WT, Zhao W-J, Hu X-M, et al. PANoptosis-like cell death in ischemia/reperfusion injury of retinal neurons. Neural Regen Res. 2023;18:357–363. doi:10.4103/1673-5374.346545
38. Meng Q, Ye C, Lu Y. miR-181c regulates ischemia/reperfusion injury-induced neuronal cell death by regulating c-Fos signaling. Die Pharmazie. 2020;75:90–93. doi:10.1691/ph.2020.9856
39. Yang Y, Li H, Yang C, et al. The potent inhibitory role of suppressing TBK1 in RIPK1 associated cerebral ischemia-reperfusion injury. Brain Res. 2022;1781:147813. doi:10.1016/j.brainres.2022.147813
40. He Y, Liu B, Yao P, et al. Adiponectin inhibits cardiac arrest/cardiopulmonary resuscitation‑induced apoptosis in brain by increasing autophagy involved in AdipoR1‑AMPK signaling. Mol Med Rep. 2020;22:870–878. doi:10.3892/mmr.2020.11181
41. Dai F, Hu C, Li X, et al. Cav3.2 channel regulates cerebral ischemia/reperfusion injury: a promising target for intervention. Neural Regen Res. 2024;19:2480–2487. doi:10.4103/1673-5374.390966
42. Patil N, Bhatt LK. Targeting Acyl-CoA synthetase long-chain family member 4: a potential approach for the treatment of cerebral ischemia/reperfusion injury. Metab Brain Dis. 2025;40:212. doi:10.1007/s11011-025-01638-2
43. Santacruz CA, Vincent J-L, Bader A, et al. Association of cerebrospinal fluid protein biomarkers with outcomes in patients with traumatic and non-traumatic acute brain injury: systematic review of the literature. Critical Care. 2021;25:278. doi:10.1186/s13054-021-03698-z
44. Angulo SL, Johnson TW, Hutchinson L, et al. Inflammation and neurological outcomes in cardiac arrest - a narrative review of serum biomarker investigations. J Intensive Care Med. 2025;8850666251357536.
45. Goebel U, Scheid S, Spassov S, et al. Argon reduces microglial activation and inflammatory cytokine expression in retinal ischemia/reperfusion injury. Neural Regen Res. 2021;16:192–198. doi:10.4103/1673-5374.290098
46. Chen X, Threlkeld SW, Cummings EE, et al. Ischemia-reperfusion impairs blood-brain barrier function and alters tight junction protein expression in the ovine fetus. Neuroscience. 2012;226:89–100. doi:10.1016/j.neuroscience.2012.08.043
47. Ma Y, Yang S, He Q, Zhang D, Chang J. The role of immune cells in post-stroke angiogenesis and neuronal remodeling: the known and the unknown. Front Immunol. 2021;12:784098. doi:10.3389/fimmu.2021.784098
48. Diao M, Xu J, Wang J, et al. Alda-1, an activator of ALDH2, improves postresuscitation cardiac and neurological outcomes by inhibiting pyroptosis in swine. Neurochem Res. 2022;47:1097–1109. doi:10.1007/s11064-021-03511-x
49. Lei Z, Ritzel RM, Li Y, et al. Old age alters inflammation and autophagy signaling in the brain, leading to exacerbated neurological outcomes after spinal cord injury in male mice. Brain Behav Immun. 2024;120:439–451. doi:10.1016/j.bbi.2024.06.023
50. deKay JT, Chepurko E, Chepurko V, et al. Delayed CCL23 response is associated with poor outcomes after cardiac arrest. Cytokine. 2024;176:156536. doi:10.1016/j.cyto.2024.156536
51. Eltzschig HK, Eckle T. Ischemia and reperfusion--from mechanism to translation. Nat Med. 2011;17:1391–1401. doi:10.1038/nm.2507
52. Campbell IL, Stalder AK, Chiang C-S, et al. Transgenic models to assess the pathogenic actions of cytokines in the central nervous system. Mol Psychiatry. 1997;2:125–129. doi:10.1038/sj.mp.4000225
53. Sprenger-Svačina A, Svačina MKR, Otlu HG, et al. Endoneurial immune interplay in peripheral nerve repair: insights and implications for future therapeutic interventions. Front Neurosci. 2025;19:1602112. doi:10.3389/fnins.2025.1602112
54. Jessen KR, Mirsky R. The repair Schwann cell and its function in regenerating nerves. J Physiol. 2016;594:3521–3531. doi:10.1113/JP270874
55. Jin Y, Song Y, Lin J, et al. Role of inflammation in neurological damage and regeneration following spinal cord injury and its therapeutic implications. Burns Trauma. 2023;11:tkac054. doi:10.1093/burnst/tkac054
56. Graber JJ, Dhib-Jalbut S. Protective autoimmunity in the nervous system. Pharmacol Ther. 2009;121:147–159. doi:10.1016/j.pharmthera.2008.10.001
57. Guo H, Liu WC, Sun YY, Jin XC, Geng PP. Neuroglia and immune cells play different roles in neuroinflammation and neuroimmune response in post-stroke neural injury and repair. Acta Pharmacol Sin. 2025:1–7.
58. Pekkarinen PT, Ristagno G, Wilkman E, et al. Procalcitonin and presepsin as prognostic markers after out-of-hospital cardiac arrest. Shock. 2018;50:395–400. doi:10.1097/SHK.0000000000001087
59. Ozkan S, Kahveci U, Hur I, Halici A. Prognostic importance of serum presepsin level in pneumonia focal sepsis and its relationship with other biomarkers and clinical severity scores. Saudi Med J. 2021;42:994–1001. doi:10.15537/smj.2021.42.9.20210163
60. Hessulf F, Bhatt DL, Engdahl J, et al. Predicting survival and neurological outcome in out-of-hospital cardiac arrest using machine learning: the SCARS model. EBioMedicine. 2023;89:104464. doi:10.1016/j.ebiom.2023.104464
61. Zhang HY, Xiao H-L, Wang G-X, et al. Predictive value of presepsin and acylcarnitines for severity and biliary drainage in acute cholangitis. World J Gastroenterol. 2023;29:2502–2514. doi:10.3748/wjg.v29.i16.2502
62. Luka S, Golea A, Tat RM, et al. The use of biomarkers testing in Emergency Department. J Critical Care Med. 2025;11:164–172. doi:10.2478/jccm-2024-0041
63. Formenti P, Gotti M, Palmieri F, et al. Presepsin in critical illness: current knowledge and future perspectives. Diagnostics. 2024;14:1311.
64. Park JE, Lee B, Yoon SJ, et al. Complementary use of presepsin with the sepsis-3 criteria improved identification of high-risk patients with suspected sepsis. Biomedicines. 2021;9.
65. Muthyala A, Sasidharan S, John KJ, Lal A, Mishra AK. Utility of cardiac bioenzymes in predicting cardiovascular outcomes in SARS-CoV-2. World J Virol. 2022;11:375–390. doi:10.5501/wjv.v11.i5.375
66. Sharma N, Das S, Nirmal K, et al. Diagnostic and prognostic evaluation of presepsin levels in neonatal septicemia: a hospital-based study. J Paediatr Child Health. 2025. doi:10.1111/jpc.70272
67. Kim CH, Kim EY. Prediction of postoperative sepsis based on changes in presepsin levels of critically ill patients with acute kidney injury after abdominal surgery. Diagnostics. 2021;11:2321. doi:10.3390/diagnostics11122321
68. Pluta MP, Czempik PF, Natorska J, Krzych ŁJ. Assessment of acute neuronal injury in critical illness: prognostication in septic shock patients - preliminary study in a Polish population. Neurologia i Neurochirurgia Polska. 2024;58:512–518. doi:10.5603/pjnns.99042
69. Ozbal S, Erbil G, Koçdor H, et al. The effects of selenium against cerebral ischemia-reperfusion injury in rats. Neurosci lett. 2008;438:265–269. doi:10.1016/j.neulet.2008.03.091
70. D’Orsi B, Mateyka J, Prehn JHM. Control of mitochondrial physiology and cell death by the Bcl-2 family proteins Bax and Bok. Neurochem Int. 2017;109:162–170. doi:10.1016/j.neuint.2017.03.010
71. Keep RF, Xiang J, Ennis SR, et al. Blood-brain barrier function in intracerebral hemorrhage. Acta Neurochirurgica Suppl. 2008;105:73–77.
72. Miyoshi M, Inoue Y, Nishioka M, et al. Usefulness of presepsin/creatinine ratio as a new index that corrects for renal function. J Med Invest. 2021;68:105–111. doi:10.2152/jmi.68.105
73. Yang HS, Hur M, Yi A, et al. Prognostic value of presepsin in adult patients with sepsis: systematic review and meta-analysis. PLoS One. 2018;13:e0191486. doi:10.1371/journal.pone.0191486
74. Wu J, Zhan X, Wang S, et al. The value of plasma presepsin as a diagnostic and prognostic biomarker for sepsis in Southern China. Inflammation Res. 2023;72:1829–1837. doi:10.1007/s00011-023-01787-z
75. Pietrasanta C, Ronchi A, Vener C, et al. Presepsin (Soluble CD14 Subtype) as an early marker of neonatal sepsis and septic shock: a prospective diagnostic trial. Antibiotics. 2021;10:580. doi:10.3390/antibiotics10050580
76. Xiao H, Wang G, Wang Y, et al. Potential value of presepsin guidance in shortening antibiotic therapy in septic patients: a multicenter, prospective cohort trial. Shock. 2022;57:63–71. doi:10.1097/SHK.0000000000001870
77. Parri N, Trippella G, Lisi C, et al. Accuracy of presepsin in neonatal sepsis: systematic review and meta-analysis. Exp Rev Anti-Infective Ther. 2019;17:223–232. doi:10.1080/14787210.2019.1584037
78. Rashwan NI, Hassan MH, El-Deen ZM, Ahmed A. Validity of biomarkers in screening for neonatal sepsis - A single center -hospital based study. Pediatr Neonatol. 2019;60:149–155. doi:10.1016/j.pedneo.2018.05.001
79. Morino G, Takahashi G, Kan S, et al. Antibody-mediated soluble CD14 stabilization prevents agitation-induced increases in presepsin levels in blood component specimens. BioTechniques. 2021;70:160–166. doi:10.2144/btn-2020-0136
80. Ikegame A, Kondo A, Kitaguchi K, Sasa K, Miyoshi M. Presepsin production in monocyte/macrophage-mediated phagocytosis of neutrophil extracellular traps. Sci Rep. 2022;12:5978. doi:10.1038/s41598-022-09926-y
81. Feng X, Ma W, Chen J, Jiao W, Wang Y. Ulinastatin alleviates early brain injury after traumatic brain injury by inhibiting oxidative stress and apoptosis. Acta Cir Bras. 2022;37:e370108. doi:10.1590/acb370108
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Combined Biomarker Panel of Presepsin, HE4, and Oxygenation Index for Sepsis Diagnosis and Prognosis in Intensive Care Unit Patients
Luo J, An S, Liao X, Wu J, Li L
Journal of Inflammation Research 2025, 18:14147-14159
Published Date: 10 October 2025