Back to Journals » International Journal of Nanomedicine » Volume 21
Nanotechnology-Enhanced Vaccines for Respiratory Infections: Opportunities and Challenges
Authors Wang K ![]() , Jiang Y, Zhou Y
, Jiang Y, Zhou Y
Received 26 March 2026
Accepted for publication 15 May 2026
Published 12 June 2026 Volume 2026:21 612148
DOI https://doi.org/10.2147/IJN.S612148
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Kamakhya Prakash Misra
Kaili Wang,1 Yushan Jiang,2 Yue Zhou3
1Nursing Department, Chun’an First People’s Hospital, Hangzhou, Zhejiang, 311700, People’s Republic of China; 2School of Nursing, Shaoxing University, Shaoxing, 312000, People’s Republic of China; 3Department of Respiratory Medicine, Chun’an First People’s Hospital, Hangzhou, Zhejiang, 311700, People’s Republic of China
Correspondence: Kaili Wang, Nursing Department, Chun’an First People’s Hospital, Hangzhou, Zhejiang, 311700, People’s Republic of China, Email [email protected] Yue Zhou, Department of Respiratory Medicine, Chun’an First People’s Hospital, No. 1869 Huanhubei Road, Hangzhou, Zhejiang, 311700, People’s Republic of China, Email [email protected]
Abstract: The continued global burden of the respiratory infections, despite availability of effective vaccines against major respiratory pathogens, represents the need to improve vaccination strategies. Although the conventional vaccines have shown effectiveness in many of the infectious diseases, they have serious limitations in developing the mucosal immunity and often fail to provide long-term protection against the rapidly mutating respiratory pathogens. In this area, nanotechnology offers novel solutions to enhance the potential of the respiratory vaccines. This review highlights recent advancements in the diverse nanotechnology platforms for respiratory vaccines, along with their transformative potentials, opportunities as well as challenges by covering the recent trends in the nanotechnology-based respiratory vaccines. Various nanotechnology platforms for respiratory vaccines include lipid nanoparticles (LNPs), polymeric nanoparticles, inorganic nanoparticles, biomimetic and self-assembling nanoplatforms. These platforms potentially address the key limitations of the traditional respiratory vaccines by improving the stability and targeted delivery of antigens, mucosal and cellular immune responses and flexible formulations against the evolving pathogens. However, challenges related to safety, scalability and real world applicability remain. The increasing research endeavors are gradually addressing the longstanding challenges and limitations of the nanotechnological measures in the respiratory vaccination and advancing this field with new opportunities for preventing the respiratory infections.
Keywords: nanotechnology, vaccines, respiratory infections, mucosal immunity, viruses
Introduction
Microbial respiratory infections caused by viral and bacterial pathogens pose a major health challenge across the globe.1,2 Particularly, the lower respiratory infections (LRIs), for example pneumonia, cause about 2.5 million mortalities every year.1,3,4 In 2023, the LRIs were reported as one of the deadliest infections on the global burden of disease.3,5 For example, Streptococcus pneumoniae caused about 25% of mortality cases due to the LRI in 2023.5 Similarly, the deadliest respiratory viruses also pose a significant threat, among which the respiratory syncytial virus (RSV) is one of the most contributing viral pathogens in the childhood pneumonia cases.6 Likewise, the seasonal influenza also leads to the annual epidemics of 3–5 million severe cases.7,8 On a global scale, the influenza virus causes about a billion infections in the people every year.7,9 Among the very recent pandemics, COVID-19 caused over 7 million deaths by end of 2024, which demonstrated how fast the new respiratory viruses can spread worldwide.1,8 This pandemic highlighted that the viruses transmitted by the respiratory route eg, coronaviridae, orthomyxoviridae, paramyxoviridae, pose global pandemic risks.10
Although, there have been considerable improvements in the vaccination approaches, yet the global trends of mortality due to these respiratory infections still remain alarming. For example, the LRIs have caused about 2.38 million deaths in 2016 and about 2.50 million in 2023, with a consequence of around 98.7 million disability adjusted life years in 2023.3 Particularly, the children and the elderly people face the highest risk due to LRIs.3 A survey conducted by World Health Organisation reported that 129 of 204 countries still cannot meet the goal of less than 60 deaths under the age of five per 100,000 people.3 These epidemics and pandemics demand improvements in the global standards of prevention towards the respiratory pathogenic viruses.10
To combat these respiratory pathogenic infections, the conventional injected vaccination strategies have shown great success but have many limitations.11,12 The available options of intramuscularly delivered vaccines are commonly prone to the systemic immunity.1,13 Although they can induce the serum IgG responses, they may generate limited mucosal IgA immunity, without which the respiratory pathogens can cause infection.1,13,14 Hence, the conventional methods of vaccination can provide protection against the disease but not against the infection or long term transmission at the mucosal membranes.1,14 Additionally, many of these vaccines need refrigeration at low temperature for their transport and storage,15–17 while maintaining a continuously cold chain is challenging for the low income and remote areas where there is unreliable electrical supply, extreme climates, and long travel times which can degrade the vaccines before their use.15–17 Furthermore, the inactivated and the subunit vaccines, for example including influenza, hepatitis, and pertussis vaccines, develop strong antibody response but poor response of the T cells because such vaccines do not replicate like the pathogens and lack intracellular presentation of antigen that drives the CD8+ cytotoxic T cells.14,18 As a result, these vaccine types can only stimulate weaker cellular immune response and need multiple doses to develop proper immunity, which limits their efficacy.14,18 Many of the conventional vaccination approaches need to be reformulated again and again for the circulating viral strains. Also, these vaccines develop on short lived immunity that fades with time, eg, the dead viral vaccines often require multiple booster doses to develop effective prevention, representing another gap to be filled by novel vaccine platforms.14,19,20
In light of the above limitations of the conventional vaccination strategies, novel nanoscale delivery systems offer promising solutions to address these challenges.21,22 Nanotechnology presents transformative avenues for the design of novel nanovaccines, which are formulations with antigen or adjuvant or both, carried by nanoscale particles.22 The particles in the nanovaccines can be liposomes, polymeric nanoparticles, virus like particles (VLPs), or lipid nanoparticles (LNPs), which mimic the size of viruses and can be designed with desired surface properties.22 Owing to their size and surface charge, the nanoparticles can efficiently target the lymphoid tissues and have the potential to be readily taken up by dendritic cells and other antigen presenting cells.22 Interestingly, the nanoparticle carriers in the nanovaccines can sometimes also act as adjuvants, eg, the lipid or polymer matrices can stimulate innate immune sensors to enhance the response of both the antibodies and the T cells.22
The challenges posed by the conventional vaccines and the need to overcome the gaps of these vaccinology strategies are driving and expanding the field of nanovaccinology.12,23 For the viral respiratory infections, these nanotechnology-based vaccines present the ability for the targeted delivery to the lung and the mucosa, and the potential to co-deliver multiple antigens or adjuvants with improved stability.1,11,23 The decades of innovative research from the discovery of liposomes to the FDA-approved LNP-based mRNA vaccines highlight a new era of nanotechnology-enhanced vaccinology.24,25 Despite many reviews focused on nanoscale vaccines have been published, there is still a knowledge gap on particularly nano enabled respiratory vaccines, and their challenges and opportunities related to clinic translation. This review is an effort to examine how these novel nanovaccine strategies develop immunity against the respiratory pathogens, offering highlights of the new opportunities and challenges in this field.
Respiratory Vaccination
Respiratory vaccination is totally different from the conventional systemic vaccination approach as the respiratory pathogens cause infection on the mucosal surfaces, such as nasal cavity and the conducting airways, before spreading deeper into the respiratory tract.26,27 At these sites, the immune system can eliminate the microbes, avoiding unnecessary action against the harmless particles that are inhaled throughout the life. This intricate balance not only makes it appealing to develop strong and sustainable mucosal immunity but also makes it challenging to achieve.28
Respiratory Mucosal Immune System
The respiratory mucosa is an active immune organ comprised the epithelial cells, mucus layers, the innate antimicrobial factors, and the lymphoid tissues organized to support adaptive immunity.29 A central structure in the upper-airway immunity is the nasal-associated lymphoid tissue (NALT), functioning to generate IgA-committed B cells and helper T cell response after the exposure of antigen in the intranasal cavity.30 A successful vaccination through the nasal route depends on the access of the antigen to the lymphoid microenvironments and the antigen-presenting cells. It is, however, a complex process, involving deposition patterns, retention time, and interaction with the immune sampling areas that specifically determine whether an antigen is ignored, tolerated, or used to trigger a protective memory response.31 An important component of the mucosal protection is the antibody secretory IgA (sIgA) that functions in external secretions and blocks microbial attachment, traps particles in mucus, and supports their physical clearing through the mucociliary mechanisms.32 Another important factor is the distinction between IgA and IgG. Conventional approach of intramuscular vaccination can trigger high serum IgG but various cases of SARS-CoV-2 revealed that systemic vaccination alone cannot effectively induce mucosal IgA.33 Additionally, experimental evidence also supports the movement of IgG across the respiratory mucosa, highlighting that it can play a role in protecting the mucosal surfaces. Nonetheless, it cannot be considered as a substitute for the strong secretory IgA layer.33 Apart from the antibodies, the tissue-resident memory T cells (T-RM) are also found in tissues to trigger local antiviral response upon re-exposure, like the production of cytokines.34 Longitudinal profiling of the human nasal lymphoid tissues during the infection by SARS-CoV-2 highlights early adaptive responses by NALT.35 Age is a factor that strongly influences respiratory mucosal immunity. The young children have immature and tolerance biased immunity, with their innate cells producing less inflammatory cytokines.36 The older individuals exhibit declines in the production of naive T and B cell, accumulation of memory cells, and low grade chronic inflammation. For example, the efficacy of influenza vaccine drops from about 70–90% in the young adults to only 30–50% in the individuals over 65.37 Figure 1 displays the intricate organization display of the human respiratory airway at the cellular level.38
 |
Figure 1 Representation of the intricate organization of the human respiratory airway at the cellular level.39 |
Challenges in Mucosal Immunity
The first and the greatest challenge in inducing mucosal immunity is the physical clearance of the mucus layer and mucociliary escalator. Mucus is continuously moved from the upper airways toward pharynx to remove the inhaled particles, which is problematic for vaccination because it can reduce the antigen residence time as well as the uptake probability by the epithelial sampling sites and the antigen-presenting cells.29 Secondly, the enzymatic degradation and dilution is another major challenge. The intranasal formulations have to survive the variable mucus viscosity, the surface liquid in the airways, and the enzymatic activity. The vaccine material can face enzymatic degradation, diminishing the effective antigen dose.38 Additionally, the respiratory mucosa poses another challenge towards the tolerance and controlled inflammation, otherwise exposure to the innocuous antigens would trigger chronic immunopathology. Hence, the mucosal tissues continuously have to balance the immune defense with tolerance to the harmless environmental antigens.40 If the intranasal antigen is not delivered with enough innate activation, it could be tolerated and develop only weak immunity. Thus, the real implication in the design of respiratory vaccine is its formulation and delivery need to be tuned in such a way that it generates strong enough immunity to protect but not too inflammatory that can damage the airway tissues.41
Immunity Mechanisms
The protective respiratory immunity starts with the capturing and presentation of the antigen by the dendritic cells and related antigen-presenting cells in epithelia in the airways. The framework of the mucosal dendritic cells defines the role of these cells in interpreting local cues, and decides whether to induce tolerance or cause protective immunity.42 Another major parameter is the activation of the innate immunity, which provides molecular signals to shape the quality of the adaptive immunity. The microbial recognition systems not only the toll-like receptors (TLRs) but also the non-TLR sensors promote the maturation of the dendritic cells, release of cytokine, and the capacity to present antigens. Therefore, the adjuvants and the delivery systems for stimulating the innate pathways can turn a vaccine from antigenic-exposure to pathogen-like and develop stronger responses of the antibodies and the T cells.43 Additionally, the innate responses need to support the tissue health because the respiratory immunity continuously shifts between clearance of pathogens, the immune modulation, and tissue repair, which exist in eliminating the infection while preserving the functioning of lungs. Thereby, the mucosal vaccines are evaluated by the serum neutralizing antibodies the local parameters, such as sIgA.29 The balance between Th1, Th2, and Th17 form an immune fingerprint to determine the efficacy and safety. Th1 along with its associated cytokines are helpful in the antiviral defense mechanism and the clearance of the infected cells, Th2 and its linked cytokines support the antibody response and drive the hypersecretion of mucus, and Th17 with its associated cytokines play role in the mucosal defense and the recruitment of neutrophil.44 On a broader picture, the respiratory vaccines involve mucosal antibodies (eg, sIgA), local cellular immunity (eg, T-RM), and carefully designed cytokine tuning, making it a challenging task.45 Nanotechnology based vaccines may influence the Th1/Th2/Th17 balance by controlling the delivery of antigens and adjuvants to the antigen presenting cells in respiratory mucosa. The nanoparticles can be engineered to favour Th1 biased responses linked with the production of IFN-γ and the cellular antiviral immunity. The selected mucosal formulations may also support the Th17 associated IL-17 responses that contribute to the recruitment of neutrophils. Avoiding the excessive Th2 skewing is also important as the poorly balanced Th2 responses may increase allergic type inflammation.44
Diversity of Nanotechnology Platforms for Respiratory Vaccines
Historically, the liposomes were first characterized as the prototype delivery vesicles in the 1960s and over decades they had been evolved into various types, eg, cationic liposomes, PEGylated liposomes, and pH-responsive nano formulations, etc, with improved immunogenicity.24 The VLPs emerged as another nanoplatform, which can self-assemble into viral protein shells with exceptional antibody-inducing potentials, laying the basis for the advanced LNP-based vaccines.25 Building on these bases, the recent breakthrough came with the emergence of the COVID-19 vaccines, where two LNP-formulated mRNA vaccines, namely mRNA-1273 by Moderna and BNT162b2 by Pfizer/BioNTech, achieved about 95% efficacy in the clinical trials.23,25,46–48 Other nanomaterials used for applications in vaccinology include polymeric nanoparticles, inorganic nanoparticles, and emulsions as novel constructs, eg, nucleic acid nanostructures and exosomes.23,49 Each nanotechnology-driven platform offers its own unique advantages, for instance the VLPs present viral proteins in their natural conformation, while the nanogels and the mucoadhesive nanoparticles have the characteristics to enhance the delivery at the mucosal surfaces.50,51
Various nanoparticle platforms are being used to overcome the challenges in respiratory vaccination. These novel platforms deliver the antigens across airways into the antigen-presenting cells by driving the mucosal antibodies and the tissue-resident memory into respiratory tract.52 Various nanotechnology-driven vaccination platforms are represented in Figure 2 and discussed in detail in the following.53
 |
Figure 2 A representation of various nanoparticle-based delivery systems in vaccination approaches. (A) VLP, (B) liposome, (C) the immune stimulating complexes, (D) the polymeric nanoparticle, (E) inorganic nanoparticle, (F) emulsion, and (G) the exosome.53 |
Lipid Nanoparticles (LNPs)
The LNPs are composed of an ionizable lipid, helper phospholipid, cholesterol, and a PEG-lipid.54,55 The LNPs are loaded with nucleic acids by mixing lipids with RNA in acidic aqueous buffer medium to form liposomes (Figure 2B), which is a pH-dependent process that forms tightly packed LNP-RNA complexes at low pH and the morphology of these nanoparticles evolves with increase in pH.56 After their uptake, the productive delivery is done through the endosomal escape, where pH-driven protonation of the ionizable lipids strengthens the interactions with anionic endosomal lipids to facilitate the release of RNA in cytosol.57 The intranasal mRNA-LNP vaccination approach has shown protective effects in animal models, for example, the induction of spike-specific IgG/IgA neutralizing response, lower respiratory viral loads, and decreased pathology of lungs was seen in SARS-CoV-2 hamster model.58,59 However, the stability and steady requirements of cold-chain supply due to their temperature sensitive nature limit the applicability of these vaccines.60 While their manufacturing and scalability are the key advantages. For example, the size control, the high-throughput optimization, and the continuous processing enhance their scale-up.61
Polymeric Nanoparticles
The polymeric carriers include natural polymers, synthetic bioresorbable agents and nucleic-acid complexing systems. Their structure is less standardized than the LNPs because the polymer nanoparticles can be solid matrices, nanogels, micelles or electrostatic complexes.1 The payload loading of these nanoparticles is done through encapsulation, surface adsorption, or polyplex formation.62 Additionally, they offer controlled release through polymer erosion, swelling and endosomal pH responsiveness.52 A study conducted in 2021 by Jearanaiwitayakul et al on intranasal SARS-CoV-2 RBD-loaded trimethyl chitosan nanoparticles enhanced mucosal immunity in mice by elevating IgA and IgG response.63 Suberi et al conducted a study on the delivery of mRNA with poly(amine-co-ester) (PACE) polyplex that resulted in protective mucosal vaccination against SARS-CoV-2 in mice by intranasal administration.62 A notable approach to the polymer nanoparticles is to convert them into inhalable dry powders, which is advantageous due to their stability and ease of handling, and can manage deposition and clearance in lungs.64 Interestingly, the inhalable vaccines designed for handling and storage at the room-temperature are advantageous as dry powders, which enhance their stability and shelf life.65
Inorganic Nanoparticles
The inorganic nanomaterials include carbon-based systems, the metallic nanoparticles, metal oxides, and porous silica carriers. Their key advantage is physicochemical stability and high surface area for the loading of antigens, which is usually done by adsorption, covalent conjugation, or pore entrapment.66 For example, Dong et al used electrostatic adsorption on graphene oxide in a mucosal influenza model to incorporate hemagglutinin, which maintained the antigenicity produced nanoparticles enhanced antigen internalization to promote the inflammatory cytokine production and dendritic cell maturation in vitro.66 Wang et al employed gold nanoparticle vaccine to use the material surface as a scaffold, which oriented repetitive presentation of hemagglutinin on the surface of the gold nanoparticles and coupled flagellin TLR5 agonist to enhance immunogenicity.67 The advantages of the inorganic nanoparticle platforms for respiratory delivery are robust association of antigens, the APC uptake, and potential self-adjuvanticity when the surfaces engage innate pathways.66 The mesoporous silica systems are used for sustained release and as mucosal adjuvants, with evidence that particle size can influence cellular uptake and immunological outcomes.68,69 They offer high stability and cold-chain relief as compared to the LNP-RNA systems, but their application in respiratory vaccines still faces low stability.64
Biomimetic and Self-Assembling Nanoplatforms
The biomimetic nanovaccines depend on mimicking the nanoscale patterns of the pathogens and include VLPs, the outer membrane vesicles (OMVs), the exosome-like extracellular vesicles, and the self-assembling protein nanoparticles.70 The VLPs develop immunity based on mimicry explained by geometry. The repetitive epitopes spaced at the nanoscale can cross-link with the B-cell receptors to engage natural IgM or the complement pathways and promote the deposition of antigens on follicular dendritic cells.70 The VLPs can also be loaded with the innate ligands, eg, RNA to stimulate the endosomal TLR pathways.70 On the other hand, the OMVs are a particularly exosome-like system for the respiratory vaccines. They are natural nanoscale vesicles enriched with bacterial membrane components to function as the innate stimulators. A study conducted by van der Ley et al in 2021 on the intranasal OMV-based SARS-CoV-2 vaccine revealed the induction of local as well as the systemic IgA responses through intranasal vaccination in mice.71 Another platform is exosomes, which are the extracellular vesicles derived from the host and are emerging as vaccine delivery and antigen presentation platforms.72 In contrast to the OMVs, the exosome systems face more challenges in their scalable manufacturing and product characterization, which limit their translation despite their appealing biological aspects.72 A study evaluated an unadjuvanted influenza hemagglutinin stem ferritin nanoparticle vaccine and reported safety and increased stem-directed antibody responses that lasted for an extended time.73 While this is an example of the injectable rather than intranasal vaccine, it demonstrates the feasibility and the immune potency of the self-assembling nanoscaffolds for their possible future application in the respiratory mucosal formulations.73 Table 1 summarizes the above-discussed nanotechnology platforms for respiratory vaccines.
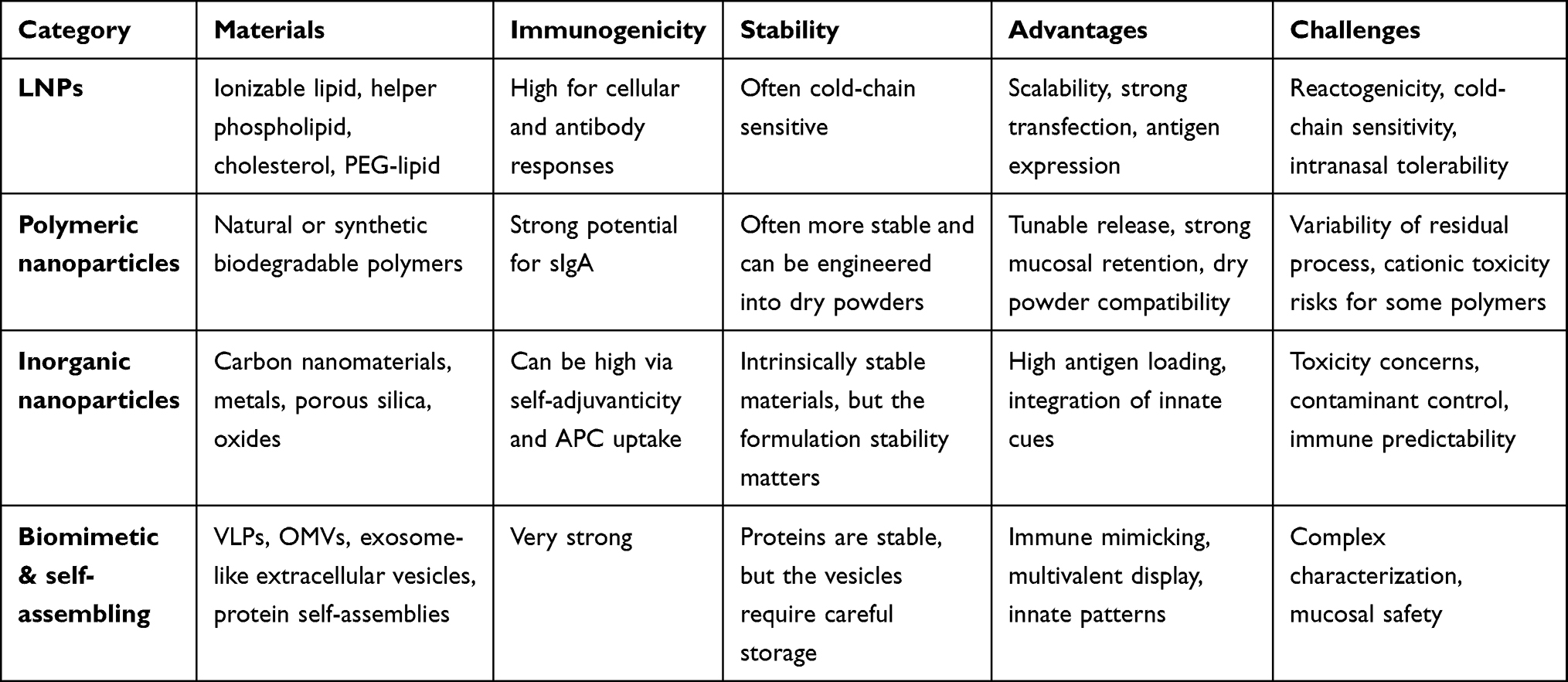 |
Table 1 A Brief Summary of Various Nanotechnology Platforms for Respiratory Vaccines |
Opportunities in Nanotechnology-Driven Respiratory Vaccination
Nanotechnology-enhanced vaccines offer effective vaccination for respiratory infections by targeted delivery of antigens, determining how long they persist, and which immune circuits they engage. In this area, nanotechnology presents many advantages, including dose sparing through multivalent display and improved delivery, needle-free mucosal vaccination with enhanced local immunity at the portal of entry, improved stability and thermotolerance, and cross-protective immunity.74 However, most of the evidence is from animal studies, and their translational challenges have been discussed in the next section. These opportunities are discussed in detail below.
Dose Sparing
Dose sparing originates when the nanoparticles increase the exposure of the effective antigen or adjuvant to the targeted cells while protecting the antigen from wasted by decreasing its clearance, degradation, or failing to reach inductive sites. The nanoparticle vaccines have ability to enhance the deposition of antigen in the lymph nodes and APC processing as compared to the soluble antigen. These vaccines can also enhance the features such as antigen presentation, which can intensify the crosslinking of B cell receptor.74 For example, Song et al reported in their study conducted in 2025 that the antigen bound with liposome achieved over 50 times adjuvant dose sparing and about 20 times antigen dose sparing in comparison with the soluble antigen in a mouse model, attributing the sparing effect to the nanoparticle driven presentation of the antigen.75 The oil in water and liposomal nano adjuvant approaches have been explicitly used to enhance the limited supply of antigen against the influenza formulations. The clinical trial designs of these approaches reduced the antigen content regimens. For instance, a Phase II study of an MF59-adjuvanted cell culture-derived H5N1 vaccine revealed that MF59 reduced the antigen required per dose.76 However, the dose sparing is not guaranteed by nanotechnology alone. Strong innate activation can increase the reactogenicity and adjuvants can produce rare cues that may require large pharmacovigilance datasets to resolve.77
Route of Administration
Against the respiratory infections, nanotechnology enables needle-free respiratory vaccination, which is immensely valuable as the respiratory pathogens enter through the mucosa. Therefore, the intranasal or inhaled delivery of respiratory vaccines can promote the immune effectors in the nose and the lung that conventional intramuscular vaccination can often weakly induce.78 This strategy has the potential to trigger the mucosal secretory IgA and the tissue-resident memory T cells at the sites of viral entry. It presents an immune geography advantage that the nanocarriers can enhance by improving the epithelial and APC delivery despite the presence of challenges posed by the mucus and clearance.78 Nanotechnology can facilitate this even for the vaccines that are traditionally delivered by injection. Vaca et al reported that the intranasal mRNA-LNP vaccination induced spike-specific IgG/IgA and neutralizing antibodies in hamsters, which reduced the respiratory viral loads and the pathology after. This produced dose-dependent effects and decrease in the viral load in both lungs and the nasal turbinates.59 Beyond the LNPs, the polymeric nanoparticles also offer alternative route to the needle-free delivery of RNA. As already discussed, Suberi et al delivered mRNA with poly(amine-co-ester) (PACE) polyplex that produces protective mucosal effects towards SARS-CoV-2 in mice by intranasal administration.62 Furthermore, another study highlighted the potential of needle-free approach using NanoSTING-SN, that is a multi-antigen intranasal vaccine adjuvanted with a nanoparticle agonist which supports serum IgG, cross-reactive IgG/IgA, and the elimination of the infectious virus in the lungs and the nasal tissue in challenged hamsters.79
Enhanced Stability
Nanotechnology offers stability of the respiratory vaccine in two ways. First, the nanoparticle formulation protects the fragile vaccine ingredients like mRNA proteins, etc, from degradation, and secondly, the nanoformulation can also be engineered in such a way that it possesses high stability and can bear higher temperatures during storage and distribution.80 Sarode et al developed a dry powder mRNA-LNPs vaccine by spray drying with mannitol and leucine excipients. Its intratracheal administration caused expression in trachea and the lungs, which demonstrates that the delivery of the functional mRNA can survive the harsh stages of manufacturing the powder.81 Similarly, another pulmonary vaccine study conducted on mRNA-LNP by Lu et al for targeting the lyophilization has reported that the physicochemical properties were maintained after storage of 2 months at 4°C.82 Applying the protein nanoparticle moieties having inherent stable profiles can also contribute to the overall stability of the formulation. For example, the SARS-CoV-2 pike ferritin nanoparticles formulation presented stability for a month at room temperature.83
Cross-Protective Immunity
For respiratory pathogens evolving rapidly, the nanoparticles can be used to bias the immunity against the conserved epitopes and the immune effectors. One such approach is using the multivalent display of antigens, where multiple antigens are co-displayed on a single nanoparticle. In this way, the B cells can be preferentially made to engage with the identified conserved regions.84 For example, a heterologous RBD arrangement was selected to promote the B cell receptors to crosslink with the adjacent RBDs and identify the conserved epitopes in a study on cross reactivity of mosaic‑8 antisera versus homotypic nanoparticles.85 Similarly, SARS‑CoV‑2 ferritin nanoparticle developed neutralizing mechanism against the SARS‑CoV‑2 and also helped in blocking ACE2 and neutralization against the SARS‑CoV‑1.86 The nanoparticle adjuvants can also shape the phenotypes of the T cell and tissue localization in heterologous protection. For example, SpFN formulated with ALFQ induced memory response against CD8 and also identified the lung antigen specific CD8 T cells several weeks after vaccination.87
Challenges and Limitations in Nanotechnology-Based Vaccination Strategies
Although, nanotechnology offers powerful methods in respiratory vaccines, as discussed above, introducing these features poses certain risk factors and challenges as well. The nanotechnology based vaccines have entered the human use, eg, the mRNA-lipid nanoparticle COVID-19 vaccines, and various others are in trials with most of them in early clinical stages.88 Other LNP mRNA vaccines, eg, influenza and RSV mRNA candidates are in mid to late stages of clinical trials. However, most of the evidence is from animal studies and their translational challenges include the safety and toxicity, the unpredictable immune response, the limitations of the intranasal route of administration, manufacturing and the regulatory challenges, as discussed below in detail. Additionally, the nanoparticle vaccines may sometimes provoke rare allergic reactions. For example, some patients have IgE sensitization to excipients like PEG or polysorbate which may cause true type I allergy.89 More commonly, the pre-existing anti PEG IgG/IgM can trigger complement activation related pseudoallergy, which can lead to mast cell degranulation and symptoms mimicking the anaphylaxis.90
Safety and Toxicity
Despite playing role as carriers, the nanoparticle based vaccines can alter the biodistribution and innate immune activation.91 One of the severe concerns is that the nanoparticles can spread beyond the targeted sites. For the LNPs, a commonly observed off-target site is liver due to the ApoE-mediated interactions with hepatic receptors.92 Additionally, the composition and the interfacial chemistry of the LNPs can also change their biodistribution.93 The off-target concerns of the respiratory vaccination also include the systemic translocation from the airways, as the ultrafine particles can reach the systemic circulation and affect the pulmonary organs.94 The size of nanoparticles is another parameter that influences the cellular uptake, clearance routes and the inflammatory signaling. A study conducted by Ernst et al illustrates that the size distribution is directly related to the risk of accumulation.95 The toxicity differences due to variation in size have been experimentally demonstrated in animal and cell models. For example, Zhang et al investigate nano and micro scaled particles and reported higher acute toxicity and potential to induce fibrosis for the nanoparticle fractions.96 Similarly, another study shows that the ultrafine particles may clear more slowly and translocate more rapidly than the larger counterparts in certain ways.94
Unpredictability of the Immune Response
The nanoparticles have the ability to enhance the immune responses, but these responses may sometimes vary from case to case. Same antigen may result different innate and adaptive outcomes depending on the size, charge, and surface composition of the nanocarriers.97 Several consider nanoparticles as foreign materials to the body and the immune system and can trigger innate sensing to enhance and sometimes distort the downstream adaptive immunity. In the LNP systems, the innate activation is a key factor to influence the efficacy and adverse effects, thereby posing a small differentiation between under-stimulation and the excessive reactogenicity.97 The immune responses can also be shifted by the size of the particles, the zeta potential, and the surface modification, which underscores a basic challenge that the tuning of the nanoparticle can either lead to immunity or tolerance. Hence, predicting this intricate balance in the individuals and across various routes remains a highly challenging task.98 Another major issue to be highlighted is that strong innate signals combined with the high local concentration in the nasal or the lung tissues could cause overinflammation. The nanoparticles can not only pose a challenge of the lung inflammation but can also worsen the existing inflammatory states, eg, when the vaccines are deployed in conditions like asthma or the concurrent respiratory infections.99 Furthermore, the composition of the nanoparticles and the innate adjuvant signaling can sometimes shift the cytokine profiles, making them challenging to forecast. This highlights both the advantages as well as the drawbacks of the nanoparticle systems, which can be highly immunogenic but can also pose side effects specific to the nanotechnology platform and the response profiles that need to be optimized very carefully.100
Challenges to the Route of Administration
The respiratory delivery offers stronger local immunity, but it also poses anatomical and physiological challenges related to its route of administration.101 A key challenge is the rapid mucociliary clearance, which reduces the residence time of the antigens. A study shows that a major portion of a solution in the turbinate region can be cleared in about 20–30 minutes. In this way, it reduces the dissolution, diffusion, and interaction with the epithelia of the vaccine.102 For the intranasal formulations, there are also the enzymatic issues, such as the proteins and other sensitive biological ingredients can be subjected to degradation.102 Anatomical differences eg, heterogeneity in the thickness of the mucosa, surface area, and patterns of airflow can cause unequal distribution and inconsistent contact with mucosa, ultimately causing complications related to reproducibility in dosing.103 Additionally, the intranasal delivery has distinct sensitivity for safety due to the proximity to neural structures. Therefore, the novel nasal vaccines need to be tested in large cohorts and the follow up in the trials has to be extended to around three months due to delayed-onset signals. Also, the deposition site depends on the aerodynamic size of the aerosol of the vaccines and respiratory mechanics,101 which leads to another challenge of reproducibility. The effective deposition requires a mass median aerodynamic diameter of 1–5 µm, and the performance also depends on the choice of device.101
Manufacturing and Regulatory Concerns
The synthesis of nano-scale vaccines has shown effective results in the laboratory settings, but their large-scale production is harder as the properties of the nanoparticle are sensitive to conditions in processing.104 For example, a study on the LNP formulation shows that the methods of mixing and the microfluidic mixing parameters can affect the efficacy in the delivery of the mRNA.105 Changes in the composition and the physicochemical parameters can cause substantial changes in pharmacology and toxicity. In addition, a major analytical challenge in the nanomedicine is size and stability that must be measured not only in simple buffers but also in the physiologically relevant media.106 Although the regulatory frameworks for nanotechnological products are evolving, there are still gaps to be filled. The nanovaccines are expected to meet the same standards of safety, efficacy, and quality as the conventional vaccines and also address uncertainties arising from the nanoscale aspects. Some nanomedicines lack particular legal bases and are assessed on the basis of case specific results, which can increase uncertainty in the planning and development stages.107 The nanovaccines are complex combinations of various components, which sometimes make the active ingredient harder to identify. For such cases eg, for mRNA-LNP vaccines, the WHO emphasizes the evaluation of tolerable total mRNA and LNP doses while considering that the interactions between mRNA and LNPs may change depending on multiple factors.108 Nanotechnology can surely enhance the performance of vaccines, but it also increases the factors to be controlled and justified, particularly for the mucosal routes of administration.97
Conclusion
The health threatening burden of the respiratory infections on a global scale has revealed limitations in the conventional strategies of vaccination, which often cannot induce strong mucosal immunity. The nanotechnology-based vaccination approaches have emerged with innovative solutions towards the immunological challenges in the respiratory vaccinology. The nanotechnology platforms not only enhance the presentation of antigens but can also promote the interaction between vaccine components and immune system components at different tissues. The nano-formulated respiratory vaccines present many advantages, including dose sparing through multivalent display, needle-free mucosal vaccination with enhanced local immunity at the portal of entry, and improved thermotolerance stability. However, these nanotechnological advancements come with certain risk factors and challenges as well, including the safety and toxicity, the unpredictable immune response, the limitations of the intranasal route of administration, manufacturing and the regulatory challenges. With the continued research efforts to overcome these challenges and innovation in the regulatory measures, the nanotechnology-based respiratory vaccines offer novel advancements for strengthening the global healthcare towards the existing and future respiratory infections. Future research should prioritize the well designed clinical trials, long term safety assessments, scalable manufacturing, and regulatory standardization. A balanced translational approach will essentially determine if these platforms can move from the experimental promise to widely deployable practical respiratory vaccines.
Data Sharing Statement
No data were used for the research described in the article.
Funding
This work was supported by the Science and Technology Program of Traditional Chinese Medicine in Zhejiang Province (No. 2026ZL0717).
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Li J, Wu G, Huang Z, et al. Advances and prospects of respiratory mucosal vaccines: mechanisms, technologies, and clinical applications. Npj Vaccines. 2025;10(1):230. doi:10.1038/s41541-025-01280-0
2. Troeger C, Blacker B, Khalil IA. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990-2016: a systematic analysis for the global burden of disease study 2016. Lancet Infect Dis. 2018;18(11):1191–14. doi:10.1016/s1473-3099(18)30310-4
3. Sirota SB, Bender RG, Dominguez RM, et al. Global burden of lower respiratory infections and aetiologies, 1990-2023: a systematic analysis for the global burden of disease study 2023. Lancet Infect Dis. 2026;26:343–61. doi:10.1016/s1473-3099(25)00689-9
4. Safiri S, Mahmoodpoor A, Kolahi -A-A, et al. Global burden of lower respiratory infections during the last three decades. Front Public Health. 2023;10:1028525. doi:10.3389/fpubh.2022.1028525
5. Sirota SB, Bender RG, Dominguez R-MV, et al. Global burden of lower respiratory infections and aetiologies, 1990–2023: a systematic analysis for the global burden of disease study 2023. Lancet Infect Dis. 2025. doi:10.1016/S1473-3099(25)00689-9
6. Scheltema NM, Gentile A, Lucion F, et al. Global respiratory syncytial virus-associated mortality in young children (RSV GOLD): a retrospective case series. Lancet Glob Health. 2017;5(10):e984–e991. doi:10.1016/s2214-109x(17)30344-3
7. Keilman LJ. Seasonal influenza (flu). Nursing Clinics. 2019;54(2):227–243. doi:10.1016/j.cnur.2019.02.009
8. Shuaibu BI, Momodu A, Muhibi MA, Dutsinma UA, Yelwa IS. A comparative review on the epidemiology of influenza, COVID-19 and respiratory syncytial viruses. Discov Med. 2025;2(1):274. doi:10.1007/s44337-025-00518-z
9. Li C, Freedman M. Seasonal influenza: an overview. J School Nurs. 2009;25:4S–12S. doi:10.1177/1059840508330066
10. Krammer F. Pandemic vaccines: how are we going to be better prepared next time? Med. 2020;1(1):28–32. doi:10.1016/j.medj.2020.11.004
11. Ramón SS, Manzanares M, Candelas G. MUCOSAL anti-infections vaccines: beyond conventional vaccines. Reumatología Clínica. 2020;16(1):49–55. doi:10.1016/j.reumae.2018.10.020
12. Andey T, Soni S, Modi S. Conventional vaccination methods: inactivated and live attenuated vaccines. In: Advanced Vaccination Technologies for Infectious and Chronic Diseases. 2024: 37–50.
13. Winklmeier S, Rübsamen H, Özdemir C, et al. Intramuscular vaccination against SARS-CoV-2 transiently induces neutralizing IgG rather than IgA in the saliva. Front Immunol. 2024;15:1330864. doi:10.3389/fimmu.2024.1330864
14. Guedes-da-Silva FH, Roncaglia-Pereira VA, Torres S, et al. Antiviral inactivated vaccines: looking to the past to face the future—a narrative review. Vaccines. 2025;13(11):1140. doi:10.3390/vaccines13111140
15. Ayowole DJ, Adebajo GO, Lasisi TO, Bakai JG. Effects of climate change on vaccine storage and cold chain logistics: a qualitative study in Ogun State, Nigeria. BMJ Glob Health. 2025;10(7):e018990. doi:10.1136/bmjgh-2025-018990
16. Rogers B, Dennison K, Adepoju N, Dowd S, Uedoi K. Vaccine cold chain: part 1. proper handling and storage of vaccine. Aaohn J. 2010;58(8):
17. Talbot A, de Koning-Ward TF, Layton D. Left out in the cold - inequity in infectious disease control due to cold chain disparity. Vaccine. 2025;45:126648. doi:10.1016/j.vaccine.2024.126648
18. Krammer F. SARS-CoV-2 vaccines in development. Nature. 2020;586(7830):516–527. doi:10.1038/s41586-020-2798-3
19. Petrovsky N. Comparative safety of vaccine adjuvants: a summary of current evidence and future needs. Drug Saf. 2015;38(11):1059–1074. doi:10.1007/s40264-015-0350-4
20. Poolman JT. Shortcomings of pertussis vaccines: why we need a third generation vaccine. Expert Rev Vaccin. 2014;13(10):1159–1162. doi:10.1586/14760584.2014.944902
21. Jiang Y, Lei L, Zhao M, Tian Y, Huang Y, Yang M. Nanocarrier vaccines for respiratory infections. Trends Mol Med. 2025;31(7):652–668. doi:10.1016/j.molmed.2024.12.002
22. Abusalah MAH, Chopra H. Nanovaccines: a game changing approach in the fight against infectious diseases. Biomed Pharmacother. 2023;167:115597. doi:10.1016/j.biopha.2023.115597
23. Khurana A, Allawadhi P, Khurana I, et al. Role of nanotechnology behind the success of mRNA vaccines for COVID-19. Nano Today. 2021;38:101142. doi:10.1016/j.nantod.2021.101142
24. García AH, De Sanctis JB. Vaccine adjuvants and delivery systems: a comprehensive review. preprints: preprints. 2025.
25. Cullis PR, Felgner PL. The 60-year evolution of lipid nanoparticles for nucleic acid delivery. Nat Rev Drug Discov. 2024;23(9):709–722. doi:10.1038/s41573-024-00977-6
26. Hellfritzsch M, Scherließ R. Mucosal vaccination via the respiratory tract. Pharmaceutics. 2019;11(8):375. doi:10.3390/pharmaceutics11080375
27. Kiyono H, Ernst PB. Nasal vaccines for respiratory infections. Nature. 2025;641(8062):321–330. doi:10.1038/s41586-025-08910-6
28. Zhou X, Wu Y, Zhu Z, et al. Mucosal immune response in biology, disease prevention and treatment. Signal Transduct Targeted Ther. 2025;10(1):7. doi:10.1038/s41392-024-02043-4
29. Mettelman RC, Allen EK, Thomas PG. Mucosal immune responses to infection and vaccination in the respiratory tract. Immunity. 2022;55(5):749–780. doi:10.1016/j.immuni.2022.04.013
30. Kiyono H, Fukuyama S. NALT- versus Peyer’s-patch-mediated mucosal immunity. Nat Rev Immunol. 2004;4(9):699–710. doi:10.1038/nri1439
31. Laube BL, Kesavan J, Farias G, Karavas N, Blondel M, Suman J. Targeting aerosol delivery to regions of nasal-associated lymphoid tissue (NALT) in three dimensional models of human intranasal airways using the BiVax intranasal atomizer. Front Drug Deliv. 2024;4:1456538. doi:10.3389/fddev.2024.1456538
32. Mantis NJ, Rol N, Corthésy B. Secretory IgA’s complex roles in immunity and mucosal homeostasis in the gut. Mucosal Immunol. 2011;4(6):603–611. doi:10.1038/mi.2011.41
33. Marking U, Bladh O, Aguilera K, et al. Impact of systemic SARS-CoV-2 vaccination on mucosal IgA responses to subsequent breakthrough infection. EBioMedicine. 2025;120:105912. doi:10.1016/j.ebiom.2025.105912
34. Carbone FR. Unique properties of tissue-resident memory T cells in the lungs: implications for COVID-19 and other respiratory diseases. Nat Rev Immunol. 2023;23(5):329–335. doi:10.1038/s41577-022-00815-z
35. Coates ML, Richoz N, Tuong ZK, et al. Temporal profiling of human lymphoid tissues reveals coordinated defense against viral challenge. Nat Immunol. 2025;26(2):215–229. doi:10.1038/s41590-024-02064-9
36. Eddens T, Parks OB, Williams JV. Neonatal immune responses to respiratory viruses. Review. Front Immunol. 2022;13. doi:10.3389/fimmu.2022.863149
37. Hou Y, Chen M, Bian Y, et al. Insights into vaccines for elderly individuals: from the impacts of immunosenescence to delivery strategies. Npj Vaccines. 2024;9(1):77. doi:10.1038/s41541-024-00874-4
38. Xu Y, Yuen P-W, Lam JK-W. Intranasal DNA vaccine for protection against respiratory infectious diseases: the delivery perspectives. Pharmaceutics. 2014;6(3):378–415. doi:10.3390/pharmaceutics6030378
39. Park S-C, Wiest MJ, Yan V, Wong PT, Schotsaert M. Induction of protective immune responses at respiratory mucosal sites. Hum Vaccin Immunother. 2024;20(1):2368288. doi:10.1080/21645515.2024.2368288
40. Traxinger BR, Richert-Spuhler LE, Lund JM. Mucosal tissue regulatory T cells are integral in balancing immunity and tolerance at portals of antigen entry. Mucosal Immunol. 2022;15(3):398–407. doi:10.1038/s41385-021-00471-x
41. Jutel M, Akdis M, Budak F, et al. IL-10 and TGF-beta cooperate in the regulatory T cell response to mucosal allergens in normal immunity and specific immunotherapy. Eur J Immunol. 2003;33(5):1205–1214. doi:10.1002/eji.200322919
42. Iwasaki A. Mucosal dendritic cells. Annu Rev Immunol. 2007;25:381–418. doi:10.1146/annurev.immunol.25.022106.141634
43. Iwasaki A, Medzhitov R. Toll-like receptor control of the adaptive immune responses. Nat Immunol. 2004;5(10):987–995. doi:10.1038/ni1112
44. Khader SA, Gaffen SL, Kolls JK. Th17 cells at the crossroads of innate and adaptive immunity against infectious diseases at the mucosa. Mucosal Immunol. 2009;2(5):403–411. doi:10.1038/mi.2009.100
45. Kumar P, Chen K, Kolls JK. Th17 cell based vaccines in mucosal immunity. Curr Opin Immunol. 2013;25(3):373–380. doi:10.1016/j.coi.2013.03.011
46. Du G, Qin M, Sun X. Recent progress in application of nanovaccines for enhancing mucosal immune responses. Acta Pharm Sin B. 2023;13(6):2334–2345. doi:10.1016/j.apsb.2022.08.010
47. Polack FP, Thomas SJ, Kitchin N, et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N Engl J Med. 2020;383(27):2603–2615. doi:10.1056/NEJMoa2034577
48. Meo SA, Bukhari IA, Akram J, Meo AS, Klonoff DC. COVID-19 vaccines: comparison of biological, pharmacological characteristics and adverse effects of Pfizer/BioNTech and Moderna vaccines. Eur Rev Med Pharmacol Sci. 2021;25(3):1663–1669. doi:10.26355/eurrev_202102_24877
49. Fries CN, Curvino EJ, Chen J-L, Permar SR, Fouda GG, Collier JH. Advances in nanomaterial vaccine strategies to address infectious diseases impacting global health. Nat Nanotechnol. 2021;16(4):1–14. doi:10.1038/s41565-020-0739-9
50. Radiom M. Potentiating virus-like particles for mucosal vaccination using material science approaches. Colloids Interfaces. 2024;8(6):68. doi:10.3390/colloids8060068
51. Zhao K, Xie Y, Lin X, Xu W. The mucoadhesive nanoparticle-based delivery system in the development of mucosal vaccines. Int J Nanomed. 2022;Volume 17:4579–4598. doi:10.2147/IJN.S359118
52. Huang M, Zhang M, Zhu H, Du X, Wang J. Mucosal vaccine delivery: a focus on the breakthrough of specific barriers. Acta Pharm Sin B. 2022;12(9):3456–3474. doi:10.1016/j.apsb.2022.07.002
53. Bezbaruah R, Chavda VP, Nongrang L, et al. Nanoparticle-Based Delivery Systems for Vaccines. Vaccines. 2022;10(11):1946.
54. Ly HH, Daniel S, Soriano SKV, Kis Z, Blakney AK. Optimization of lipid nanoparticles for saRNA expression and cellular activation using a design-of-experiment approach. Mol Pharm. 2022;19(6):1892–1905. doi:10.1021/acs.molpharmaceut.2c00032
55. Khairnar SV, Pagare P, Thakre A, et al. Review on the scale-up methods for the preparation of solid lipid nanoparticles. Pharmaceutics. 2022;14(9):1886. doi:10.3390/pharmaceutics14091886
56. Kulkarni JA, Darjuan MM, Mercer JE, et al. On the formation and morphology of lipid nanoparticles containing ionizable cationic lipids and siRNA. ACS Nano. 2018;12(5):4787–4795. doi:10.1021/acsnano.8b01516
57. Wang J, Chen R, Xie Y, Qin X, Zhou Y, Xu C. Endo/Lysosomal-escapable lipid nanoparticle platforms for enhancing mRNA delivery in cancer therapy. Pharmaceutics. 2025;17(7):803. doi:10.3390/pharmaceutics17070803
58. Zhang Z, Yang Y, Huang L, et al. Nanotechnology-driven advances in intranasal vaccine delivery systems against infectious diseases. Front Immunol. 2025;16:1573037. doi:10.3389/fimmu.2025.1573037
59. Baldeon Vaca G, Meyer M, Cadete A, et al. Intranasal mRNA-LNP vaccination protects hamsters from SARS-CoV-2 infection. Sci Adv. 2023;9(38):eadh1655. doi:10.1126/sciadv.adh1655
60. Wu L, Xu W, Jiang H, Yang M, Cun D. Respiratory delivered vaccines: current status and perspectives in rational formulation design. Acta Pharmaceutica Sinica B. 2024;14(12):5132–5160. doi:10.1016/j.apsb.2024.08.026
61. Maeki M, Uno S, Niwa A, Okada Y, Tokeshi M. Microfluidic technologies and devices for lipid nanoparticle-based RNA delivery. J Control Release. 2022;344:80–96. doi:10.1016/j.jconrel.2022.02.017
62. Suberi A, Grun MK, Mao T, et al. Polymer nanoparticles deliver mRNA to the lung for mucosal vaccination. Sci Transl Med. 2023;15(709):eabq0603. doi:10.1126/scitranslmed.abq0603
63. Jearanaiwitayakul T, Seesen M, Chawengkirttikul R, et al. Intranasal administration of RBD nanoparticles confers induction of mucosal and systemic immunity against SARS-CoV-2. Vaccines. 2021;9(7):768. doi:10.3390/vaccines9070768
64. Pasero L, Susa F, Limongi T, Pisano R. A review on micro and nanoengineering in powder-based pulmonary drug delivery. Int J Pharm. 2024;659:124248. doi:10.1016/j.ijpharm.2024.124248
65. Noriega-Fernandes B, Ibrahim M, Cruz R, Kuehl PJ, Shepard KB. Navigating the development of dry powder for inhalation: a CDMO perspective. Pharmaceuticals. 2025;18(3):434. doi:10.3390/ph18030434
66. Dong C, Wang Y, Gonzalez GX, et al. Intranasal vaccination with influenza HA/GO-PEI nanoparticles provides immune protection against homo- and heterologous strains. Proc Natl Acad Sci U S A. 2021;118(19). doi:10.1073/pnas.2024998118
67. Wang C, Zhu W, Luo Y, Wang BZ. Gold nanoparticles conjugating recombinant influenza hemagglutinin trimers and flagellin enhanced mucosal cellular immunity. Nanomedicine. 2018;14(4):1349–1360. doi:10.1016/j.nano.2018.03.007
68. Liu Z, Lu H, Li S, et al. Size effect of mesoporous silica nanoparticles on regulating the immune effect of oral influenza split vaccine. Colloids Surfaces B. 2024;238:113920. doi:10.1016/j.colsurfb.2024.113920
69. Permana Z, Xeliem JN, Zefrina NF, et al. Enhanced delivery of anti-inflammatory therapeutics using pH-responsive histidine-modified poly-L-lysine on mesoporous silica nanoparticles. Narra J. 2025;5(1):e1815. doi:10.52225/narra.v5i1.1815
70. Mohsen MO, Bachmann MF. Virus-like particle vaccinology, from bench to bedside. Cell Mol Immunol. 2022;19(9):993–1011. doi:10.1038/s41423-022-00897-8
71. van der Ley PA, Zariri A, van Riet E, Oosterhoff D, Kruiswijk CP. An intranasal OMV-based vaccine induces high mucosal and systemic protecting immunity against a SARS-CoV-2 infection. original research. Front Immunol. 2021. doi:10.3389/fimmu.2021.781280
72. Tan D, Li G, Fu W, Lei C. Exosomes: the next frontier in vaccine development and delivery. Front Immunol. 2024;15:1435426. doi:10.3389/fimmu.2024.1435426
73. Casazza JP, Hofstetter AR, Costner PJM, et al. Phase 1 dose-escalation trial evaluating a group 2 influenza hemagglutinin stabilized stem nanoparticle vaccine. Npj Vaccines. 2024;9(1):171. doi:10.1038/s41541-024-00959-0
74. Vu MN, Kelly HG, Kent SJ, Wheatley AK. Current and future nanoparticle vaccines for COVID-19. EBioMedicine. 2021;74:103699. doi:10.1016/j.ebiom.2021.103699
75. Song Y, Huang WC, Ivanochko D, et al. 50-fold adjuvant and 20-fold antigen vaccine dose sparing from nanoliposome display of a stabilized malarial protein antigen. ACS Nano. 2025;19(10):10103–10112. doi:10.1021/acsnano.4c16865
76. Frey SE, Shakib S, Chanthavanich P, et al. Safety and immunogenicity of MF59-adjuvanted cell culture–derived A/H5N1 subunit influenza virus vaccine: dose-finding clinical trials in adults and the elderly. Open Forum Infect Dis. 2019;6(4). doi:10.1093/ofid/ofz107
77. Cohet C, van der Most R, Bauchau V, et al. Safety of AS03-adjuvanted influenza vaccines: a review of the evidence. Vaccine. 2019;37(23):3006–3021. doi:10.1016/j.vaccine.2019.04.048
78. Bai Z, Wan D, Lan T, et al. Nanoplatform based intranasal vaccines: current progress and clinical challenges. ACS Nano. 2024;18(36):24650–24681. doi:10.1021/acsnano.3c10797
79. Leekha A, Saeedi A, Sefat KMSR, et al. Multi-antigen intranasal vaccine protects against challenge with sarbecoviruses and prevents transmission in hamsters. Nat Commun. 2024;15(1):6193. doi:10.1038/s41467-024-50133-2
80. Gomez M, McCollum J, Wang H, et al. Evaluation of the stability of a spray-dried tuberculosis vaccine candidate designed for dry powder respiratory delivery. Vaccine. 2021;39(35):5025–5036. doi:10.1016/j.vaccine.2021.07.002
81. Sarode A, Patel P, Vargas-Montoya N, et al. Inhalable dry powder product (DPP) of mRNA lipid nanoparticles (LNPs) for pulmonary delivery. Drug Deliv Transl Res. 2024;14(2):360–372. doi:10.1007/s13346-023-01402-y
82. Lu Y, Yang Y, Yi J, et al. Design, optimization, and evaluation of lyophilized lipid nanoparticles for mRNA-based pulmonary mucosal vaccination. Mater Today Bio. 2025;32:101813. doi:10.1016/j.mtbio.2025.101813
83. Hajduczki A, Chang WC, De La Barrera R, et al. Production of clinical-grade SARS-CoV-2 spike ferritin nanoparticle protein immunogen by transient transfection. Vaccines. 2025;13(10):1041. doi:10.3390/vaccines13101041
84. Zhao Y, Liu J, Peng C, et al. Cross-protection against homo and heterologous influenza viruses via intranasal administration of an HA chimeric multiepitope nanoparticle vaccine. J Nanobiotech. 2025;23(1):77. doi:10.1186/s12951-025-03122-6
85. Cohen AA, van Doremalen N, Greaney AJ, et al. Mosaic RBD nanoparticles protect against multiple sarbecovirus challenges in animal models. bioRxiv. 2022. doi:10.1101/2022.03.25.485875
86. Joyce MG, Chen WH, Sankhala RS, et al. SARS-CoV-2 ferritin nanoparticle vaccines elicit broad SARS coronavirus immunogenicity. bioRxiv. 2021. doi:10.1101/2021.05.09.443331
87. Carmen JM, Shrivastava S, Lu Z, et al. SARS-CoV-2 ferritin nanoparticle vaccine induces robust innate immune activity driving polyfunctional spike-specific T cell responses. Npj Vaccines. 2021;6(1):151. doi:10.1038/s41541-021-00414-4
88. Saleh M, El-Moghazy A, Elgohary AH, Saber WIA, Helmy YA. Revolutionizing nanovaccines: a new era of immunization. Vaccines. 2025;13(2):126. doi:10.3390/vaccines13020126
89. Zhou Z-H, Cortese MM, Fang J-L, et al. Evaluation of association of anti-PEG antibodies with anaphylaxis after mRNA COVID-19 vaccination. Vaccine. 2023;41(28):4183–4189. doi:10.1016/j.vaccine.2023.05.029
90. Dézsi L, Mészáros T, Kozma G, et al. A naturally hypersensitive porcine model may help understand the mechanism of COVID-19 mRNA vaccine-induced rare (pseudo) allergic reactions: complement activation as a possible contributing factor. Geroscience. 2022;44(2):597–618. doi:10.1007/s11357-021-00495-y
91. de Vlieger JS, Crommelin DJ, Tyner K, et al. Report of the AAPS guidance forum on the FDA draft guidance for industry: “drug products, including biological products, that contain nanomaterials”. AAPS J. 2019;21(4):56. doi:10.1208/s12248-019-0329-7
92. Hosseini-Kharat M, Bremmell KE, Prestidge CA. Why do lipid nanoparticles target the liver? Understanding of biodistribution and liver-specific tropism. Mol Ther Methods Clin Dev. 2025;33(1):101436. doi:10.1016/j.omtm.2025.101436
93. Vasileva O, Zaborova O, Shmykov B, Ivanov R, Reshetnikov V. Composition of lipid nanoparticles for targeted delivery: application to mRNA therapeutics. Review. Front Pharmacol. 2024;15. doi:10.3389/fphar.2024.1466337
94. Praphawatvet T, Peters JI, Williams RO. Inhaled nanoparticles–An updated review. Int J Pharm. 2020;587:119671. doi:10.1016/j.ijpharm.2020.119671
95. Ernst LM, Mondragón L, Ramis J, et al. Exploring the long-term tissue accumulation and excretion of 3 nm cerium oxide nanoparticles after single dose administration. Antioxidants. 2023;12(3):765. doi:10.3390/antiox12030765
96. Zhang Y, Li A, Gao J, et al. Differences in the characteristics and pulmonary toxicity of nano- and micron-sized respirable coal dust. Respir Res. 2022;23(1):197. doi:10.1186/s12931-022-02120-8
97. Lee Y, Jeong M, Park J, Jung H, Lee H. Immunogenicity of lipid nanoparticles and its impact on the efficacy of mRNA vaccines and therapeutics. Exp Mol Med. 2023;55(10):2085–2096. doi:10.1038/s12276-023-01086-x
98. Lin G, Wang J, Yang Y-G, Zhang Y, Sun T. Advances in dendritic cell targeting nano-delivery systems for induction of immune tolerance. Review. Front Bioeng Biotechnol. 2023;11. doi:10.3389/fbioe.2023.1242126
99. Zhou X, Jin W, Ma J. Lung inflammation perturbation by engineered nanoparticles. Front Bioeng Biotechnol. 2023;11:1199230. doi:10.3389/fbioe.2023.1199230
100. Filipić B, Pantelić I, Nikolić I, et al. Nanoparticle-based adjuvants and delivery systems for modern vaccines. Vaccines. 2023;11(7):1172. doi:10.3390/vaccines11071172
101. Fan Y, Zhou Y, Zhao J, Zhao Y. Advances in inhaled nanoparticle drug delivery for pulmonary disease management. FASEB J. 2025;39(21):e71191. doi:10.1096/fj.202502624R
102. Forbes B, Goodacre L, Lansley AB, et al. Advances in nasal biopharmaceutics to support product development and therapeutic needs. Pharmaceutics. 2025;17(10):1321. doi:10.3390/pharmaceutics17101321
103. Gandhi S, Shastri DH, Shah J, Nair AB, Jacob S. Nasal delivery to the brain: harnessing nanoparticles for effective drug transport. Pharmaceutics. 2024;16(4):481. doi:10.3390/pharmaceutics16040481
104. Osouli-Bostanabad K, Puliga S, Serrano DR, Bucchi A, Halbert G, Lalatsa A. Microfluidic Manufacture of Lipid-Based Nanomedicines. Pharmaceutics. 2022;14(9):1940. doi:10.3390/pharmaceutics14091940
105. Strelkova petersen DM, Chaudhary N, Arral ML, Weiss RM, Whitehead KA. The mixing method used to formulate lipid nanoparticles affects mRNA delivery efficacy and organ tropism. Eur J Pharm Biopharm. 2023;192:126–135. doi:10.1016/j.ejpb.2023.10.006
106. Clogston JD, Hackley VA, Prina-Mello A, Puri S, Sonzini S, Soo PL. Sizing up the next generation of nanomedicines. Pharm Res. 2019;37(1):6. doi:10.1007/s11095-019-2736-y
107. Rodríguez-Gómez FD, Monferrer D, Penon O, Rivera-Gil P. Regulatory pathways and guidelines for nanotechnology-enabled health products: a comparative review of EU and US frameworks. Front Med. 2025;12:1544393. doi:10.3389/fmed.2025.1544393
108. World Health Organization. Evaluation of the quality, safety and efficacy of messenger RNA vaccines for the prevention of infectious diseases: regulatory considerations. World Health Organization sl; 2021.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.