Back to Journals » International Journal of Nanomedicine » Volume 21
Nanoparticles Navigating the Blood–Brain Barrier for Neurodegenerative Therapy
Authors Zhao X, Sun L, Zhang X, Qi X ![]() , Wu G
, Wu G ![]()
Received 30 April 2026
Accepted for publication 30 June 2026
Published 16 July 2026 Volume 2026:21 620793
DOI https://doi.org/10.2147/IJN.S620793
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Anderson Oliveira Lobo
Xinming Zhao, Liming Sun, Xiaoman Zhang, Xiaochen Qi, Guangzhen Wu
Department of Urology, The First Affiliated Hospital of Dalian Medical University, Dalian, 116011, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaochen Qi, Email [email protected] Guangzhen Wu, Email [email protected]
Abstract: The blood–brain barrier (BBB) blocks most drugs from entering the brain. Over 98% of small-molecule drugs and nearly all biologics fail to cross this barrier. Nanoparticles (NPs) provide multiple ways to bypass the BBB. These include receptor-mediated transcytosis, adsorptive-mediated transport, and intranasal delivery. NPs can also modify disease-related pathways. For example, they promote amyloid-β clearance, reduce tau phosphorylation, and reprogram neuroimmune responses. Many preclinical studies have shown promising results in Alzheimer’s, Parkinson’s, and Huntington’s diseases. However, no NP-based therapy has moved beyond early-stage clinical trials. Several issues remain unresolved. Direct comparisons between different NP platforms are lacking. The long-term toxicity of NPs in the brain is not well understood. Animal models also do not accurately reflect human disease. We suggest that future work should focus on standardized characterization, better predictive models, and clinical trial designs that address NP diversity. Researchers should also compare NP therapies with existing treatments in a rigorous manner.
Keywords: neurodegenerative diseases, nanoparticles, blood-brain barrier, drug delivery, clinical translation
Introduction
Neurodegenerative disorders represent an under-recognized public health problem, associated with progressive deterioration of neurons in the central nervous system. Among them, Alzheimer’s disease (AD) and Parkinson’s disease (PD) are the most common, impacting millions of individuals globally. Their occurrence is steadily increasing worldwide, due to the intricate interplay of various factors, including genetic vulnerability, prenatal characteristics, nutritional status, chronic stress and environmental exposures.1,2 AD is the most frequent type of dementia and now affects 50 million people, a number estimated to climb to 150 million by 2050. This terrible scenario makes the discovery of therapies for AD, and more generally for neurodegenerative illnesses, an essential goal.3,4 Although several medications have been approved for the treatment of neurodegenerative illnesses, their main role is still limited to symptom relief, and the number of such drugs is quite limited. The most challenging problem for the treatment of neurodegenerative diseases nowadays is that the blood-brain barrier (BBB) severely impedes the efficient delivery of drugs to the central nervous system, thus most of the drug molecules cannot reach therapeutic concentrations in the brain.5,6 There are certain medications that can treat the symptoms of diseases such as Alzheimer’s and Parkinson’s, but they are usually only effective for a short time in roughly half of the patients and have considerable adverse effects. More significantly, current available medicines are unable to stop or reverse the neurodegenerative development of the disease. Additionally, the animal models used in conventional drug development are often unable to perfectly simulate the complex pathological characteristics of human diseases. Many drug candidates that were efficacious in preclinical studies fail in clinical trials, further exacerbating the therapeutic bottleneck.7 Therefore, the development of new drug delivery technologies and combination therapies is an urgent research goal.
Nanoparticles (NPs) typically range in diameter from 1 to 100 nanometers and possess excellent stiffness, stability, porosity, and specific surface area, making them the drug of choice for drug delivery systems.8 At the same time, their superior targeted delivery capabilities have also been applied to the delivery of drugs to the brain.9 Recent studies have shown that nanoparticles possess significant advantages over conventional drugs in crossing the blood-brain barrier (BBB).10,11 Nanoparticles can overcome the BBB’s extreme selectivity, thereby enabling the safe and targeted delivery of macromolecular therapeutics—such as proteins and peptides—to the central nervous system.12,13 Among these, nanoplatforms such as metal nanoparticles, nanomicelles, liposomes, and exosomes have attracted widespread attention.14 However, despite their potential as drug delivery carriers, these nanoparticles still face challenges such as instability, uncertain toxicity, and difficulties in clinical translation15,16 (Figure 1).
 |
Figure 1 Administration and Efficacy of Nanoparticles in Neurodegenerative Diseases. Nanoparticles can be administered by many pathways such as intranasal, meningeal lymphatic transportation, oral delivery, and BBB opening by photothermal therapy. Once inside the brain, nanoparticles modify the pathological microenvironment through a number of mechanisms: they reduce neuroinflammation, decrease neuronal injury and provide neuroprotection by stimulating the polarization of microglia from the pro-inflammatory M1 phenotype to the anti-inflammatory M2 phenotype. The balance between degenerative effects (neurotoxicity, inflammation and neuronal damage) and protective effects (anti-inflammation and neuroprotection) indicates the therapeutic potential of nanoparticles to treat central nervous system disorders such as Alzheimer’s disease, Parkinson’s disease and Huntington’s disease. |
Unlike previous reviews, which primarily focused on a single disease or delivery vehicle, this review adopts a different narrative approach. We have constructed an analytical framework comprising two core dimensions: “barrier crossing” and “pathological regulation.” This paper also discusses a special phenomenon, in which some nanoparticles (such as gold nanoparticles and nanoenzymes) are able to affect disease development without drug loading, based solely on their intrinsic physicochemical properties (eg, multi-enzyme activity, ion-binding capacity or photothermal effects) This work aims to explore the possible channels by which nanoparticles influence the inflammatory milieu, discussing mechanisms and focusing on some specific processes such as metabolic reprogramming, ferroptosis pathways and neuroimmune interactions. Furthermore, the paper states that positive results in animal models are not always predictive of therapeutic potential. We discuss issues such as the lack of direct comparisons between different platforms in current research, the lack of understanding of the long-term intracerebral toxicity of nanoparticles and propose a tiered advancement strategy based on existing materials, local administration and physically assisted methods. In summary, from the perspective of the synergy between delivery efficiency and intervention depth, this paper attempts to provide a systematic knowledge framework and direction for research on nanoparticles for neurodegenerative diseases.
The Blood-Brain Barrier in Neurodegenerative Diseases
The blood-brain barrier (BBB) is primarily composed of brain microvascular endothelial cells. These endothelial cells are interconnected via tight junctions (TJ) and adherens junctions (AJ), forming a physical barrier that restricts the free exchange of substances between the bloodstream and brain tissue. Its core function is to maintain the homeostasis of the central nervous system. It not only effectively prevents neurotoxic components, blood cells, and pathogens in plasma from entering the brain parenchyma, but also highly selectively regulates the transport of nutrients (such as glucose and amino acids), energy metabolites, and essential molecules (such as certain hormones and fatty acids) from the blood into the brain, while actively excreting metabolic waste products from the interstitial fluid of brain tissue into the bloodstream.17–19 Disruption of the BBB is a common feature of all neurodegenerative diseases;20 chronic neuroinflammation and dysfunction of the blood-brain barrier have been observed in Alzheimer’s disease, Parkinson’s disease, amyotrophic lateral sclerosis, and Huntington’s disease.21–23
NPs cross the BBB through various strategies, which are primarily categorized into mechanisms such as passive diffusion, carrier-mediated transport, receptor-mediated endocytosis, adsorption-mediated endocytosis, and cell-mediated transport. Among these, Receptor-Mediated transcytosis is one of the most common and efficient strategies. By conjugating a targeted ligand to the surface of a nanoparticle, it can specifically bind to receptors on the surface of BBB endothelial cells (such as the transferrin receptor), triggering endocytosis and transcellular transport, thereby enabling drug delivery to the brain. In addition, adsorption-mediated endocytosis induced by cationic materials or cell-penetrating peptides, cell-mediated transport using immune cells as “Trojan horses,” and the use of surface-modified hydrophilic polymers such as PEG to prolong circulation time and reduce clearance by the reticuloendothelial system are also important strategies for improving the efficiency of nanoparticle BBB crossing.24–26 At the same time, NPs loaded with various “drugs” can also bypass the BBB through intranasal administration, ultrasound-assisted delivery, or delivery via the meningeal lymphatic pathway, enabling direct delivery to the affected areas within the brain27,28 (Figure 2).
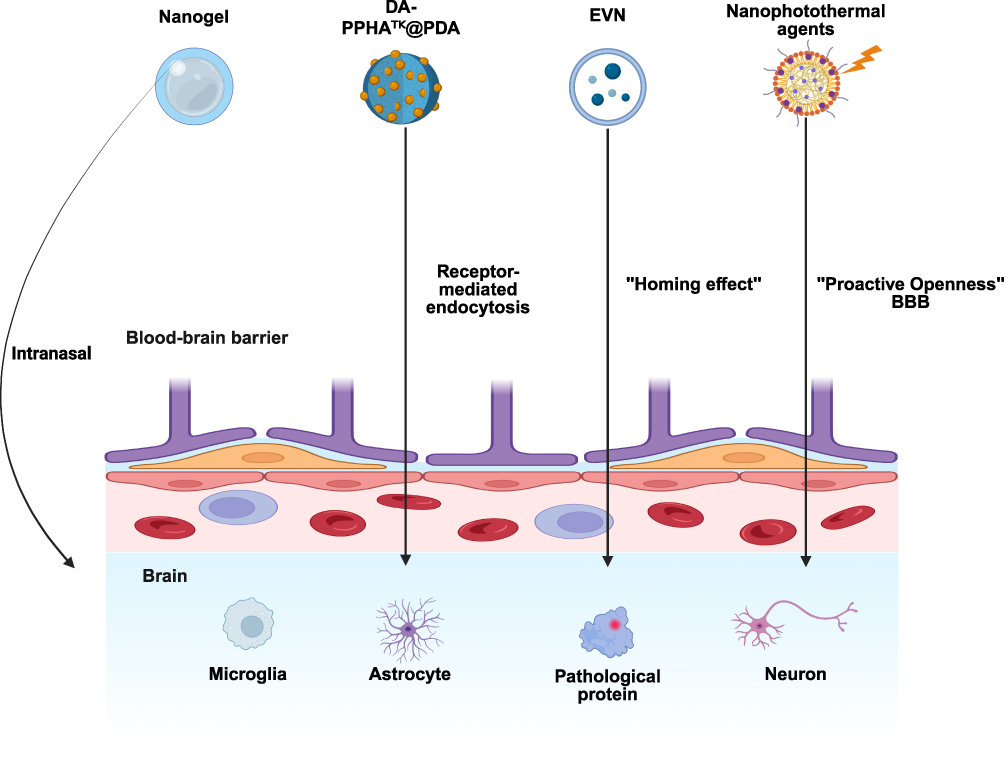 |
Figure 2 Mechanisms by the Nanoparticles Cross the BBB. The primary mechanisms by which nanoparticles cross the BBB include: receptor-mediated endocytosis, active “Homing effect”driven by chemokine gradients, “proactive openness” of the BBB mediated by nitric oxide or photothermal effects, and intranasal administration, which completely bypasses the BBB. Representative nanoplatforms shown in the figure include nanogels, peptide-drug conjugate-based nanoplatforms (eg, DA-PPHATK@PDA), engineered extracellular vesicle (EVN) formulations, and nanophotothermal agents. Once delivered to the brain parenchyma, these nanoparticles act on the major pathological cell types—microglia, astrocytes, and neurons—to clear pathogenic proteins, suppress neuroinflammation, reprogram immunometabolism, or promote neurogenesis, thereby addressing Alzheimer’s disease, Parkinson’s disease, and Huntington’s disease. |
Nanoparticles for the Treatment of Alzheimer’s Disease
Alzheimer’s disease (AD) is the most common neurodegenerative condition and is characterized by extracellular β-amyloid (Aβ) deposits and neurofibrillary tangles of hyperphosphorylated tau protein.3,29,30 Microglia and astrocytes stimulated by Aβ plaques or other stimuli secrete substantial amounts of pro-inflammatory cytokines. These inflammatory factors directly or indirectly promote hyperphosphorylation of tau protein at multiple sites and aggravate abnormal aggregation and post-translational modifications (such as acetylation) of tau by activating key signaling pathways such as p38 MAPK and GSK-3β, thus promoting the formation of pathological tau.31 Memantine, an NMDA receptor antagonist, and the acetylcholinesterase inhibitors donepezil, rivastigmine, and tacrine are among the FDA-approved medications being utilized in the treatment of AD.32 Despite intensive investigation, no medicine has been able to arrest the degenerative course of AD. This has created a very large global health burden and has led to increased study of innovative approaches in pharmacological treatment and combination therapies for AD.
Microglia in AD are resident immune cells of the CNS that serve a dual role as sensors and scavengers of pathogenic stimuli and drivers of neuroinflammation and victims of functional impairment. In the early stages of AD, microglia can quickly transition from oxidative phosphorylation under steady-state conditions to glycolysis by using their highly plastic metabolic system, providing enough energy to enable Aβ phagocytosis and the generation of inflammatory cytokines. As the disease advances, the prolonged exposure to aggregated Aβ and tau proteins triggers metabolic reprogramming in microglia, pushing them into a “immune tolerant” state. It is characterized by downregulation of both glycolysis and oxidative phosphorylation, decreased phagocytic capability and dysregulated inflammatory responses. Thus, microglia targeting and their metabolic modulation have become a novel therapeutic strategy for AD.33–35 A modular nanodelivery system including a peptide-drug conjugate and a polydopamine core was employed for the treatment of late-stage AD (DA-PPHATK@PDA). The nanoplatform utilizes two targeting modules to deliver drugs. On the one hand, it employs an Ab-peptide to target microglia in an immune-tolerant state and delivers hydroxychloroquine (HCQ) to activate their Akt/mTOR/HIF-1α signaling pathway to reprogram the microglia’s metabolic profile from oxidative phosphorylation to glycolysis to restore their energy metabolism and immune activity and thus regain their ability to phagocytose and clear Aβ; However, DAG peptides are employed to target reactive astrocytes and deliver all-trans retinoic acid to activate the PI3K/Akt/NeuroD1 signaling pathway, which induces astrocytes to express the immature neuronal marker DCX and the mature neuronal markers MAP2 and NeuN, leading to the reprogramming of astrocytes into synaptically active neurons.36 Another form of transferrin-targeted self-assembled nanoparticle (SANP-TF-TEMNAP) can penetrate the BBB to transport TEMNAP, a new TSPO ligand, to the hippocampus and cortex of animals with Alzheimer’s disease. It has been shown to exert potent anti-neuroinflammatory and cognitive protective actions at the cellular level by blocking pro-inflammatory signaling pathways activated by lipopolysaccharide (LPS) or Aβ pathology.37 Resveratrol-loaded selenium/chitosan nanoparticles (Res@SeNPs@Res-CS-NPs) can improve brain energy metabolism via regulation of dysregulated glycolipid metabolism. At the same time, they inhibit the JNK/AKT/GSK3β signaling pathway, reduce the phosphorylation of tau protein and β-amyloid (Aβ) aggregation, and enhance the activity of antioxidant enzymes (SOD, GSH-px, CAT) and suppress the release of inflammatory factors (IL-6, IL-1β, TNF-α), thus controlling central nervous system inflammation to improve cognitive function.38 Then, a hybrid cell membrane-coated nanoliposome is developed through hybridizing platelet membranes with HEK293T cell membranes significantly expressing CCR2. The platelet surface membrane is abundant with proteins such as CD47, which can alleviate immune clearance, prolong circulation time, and exploit the impaired BBB characteristics of AD for effective crossing by binding to the injured vascular endothelium. CCR2 can recognize the inflammatory factor CCL2, which is secreted at high levels by activated glial cells in the AD brain, thus achieving active targeting to inflammatory regions. The liposome contains rapamycin and TPPU, a specific inhibitor of soluble epoxide hydrolase (sEH): Rapamycin stimulates autophagy through inhibition of the mTOR pathway and promotes clearance of pathogenic proteins such as Aβ; TPPU inhibits sEH and lowers neuroinflammatory responses; TPPU controls excessive activation of glial cells.39
Also, intranasally delivered nanogel exhibits exceptional targeting efficacy, and uniquely for intranasal administration, where drugs can bypass the BBB and be delivered directly to the brain, this nanogel shows prolonged drug retention time than intravenous administration.40 BP-MB@Gel is a thermosensitive hydrogel intranasal delivery method mostly composed of BP-MB nanocomposites created from loading the methylene blue (MB) on the black phosphorus nanosheets (BP NSs). Upon intranasal administration, it undergoes a sol-gel transition at the temperature of the nasal mucosa (approximately 34°C), forming a highly adhesive gel reservoir that enables prolonged retention and sustained release of the drug in the nasal cavity. As the main part of this nanoplatform, BP-MB can successfully scavenge several reactive oxygen species (ROS) and thereby relieve the oxidative stress damage induced by excessive tau protein phosphorylation. Meanwhile, it greatly inhibits the hyperphosphorylation of tau protein at the location of Ser396 and its aggregation, thus decreasing the formation of neurofibrillary tangles.41 In addition, intranasal delivery of H102 peptide nanoliposomes can pass through the BBB, specifically bind to Aβ monomers, prevent the formation of their β-sheet conformation, thus block the abnormal aggregation and fibrillation of Aβ, and can depolymerize existing Aβ fibrils, decreasing their neurotoxicity. Moreover, the liposomal encapsulation shields H102 from enzymatic breakdown in vivo and allows effective transport to the brain.42
Nanoparticles for delivery of conventional medicines for treatment of Alzheimer’s disease are promising but still cannot overcome the problem that conventional treatments cannot reverse the degenerative course of the illness. The relevance of gene therapy in AD is that it can bypass the constraints of conventional small-molecule medicines, which only relieve symptoms. Gene therapy acts directly on gene expression at the DNA or RNA level, therefore changing the disease process, and offering high specificity and the promise for long term treatment or potentially a cure. However, gene therapy for AD is hampered by three major obstacles, namely pathological heterogeneity among patients, unknown druggable target mechanism and the arduous task of delivering functional therapeutic components (like nucleic acids and gene-editing complexes) precisely through the blood-brain barrier to the site of lesions. Thus, as a new technique for gene therapy of Alzheimer’s disease, the use of nanoparticles to overcome these problems has been developed.43 The biomimetic nanovesicle system is a dual-gene delivery platform based on exosome-liposome hybrid vesicles, designed to deliver siRNA targeting BACE1 (siBACE1) and a TREM2 expression plasmid (pTREM2). siBACE1 inhibits the production of Aβ at its source by knocking down BACE1 gene expression; meanwhile, pTREM2 upregulates the expression of the TREM2 protein in microglia, promoting their transition from the pro-inflammatory M1 phenotype to the anti-inflammatory, repair-promoting M2 phenotype. This enhances their ability to phagocytose and clear Aβ and alleviates neuroinflammatory responses. By surface-modifying the Angiopep-2 peptide and leveraging the natural homing ability of exosomes, this nanoplatform can efficiently cross the BBB, accumulate at AD lesions, and release drugs in a controlled manner in response to ROS. TSEL achieves the treatment of AD through a dual mechanism of “inhibiting Aβ production” and “promoting Aβ clearance”.44
Exosomes are nanosized extracellular vesicles that are released by most cell types and are present in many bodily fluids and tissues including the central nervous system (CNS). Such vesicles are thought to be involved in intercellular communication, clearing of cellular detritus, and intercellular transfer of pathogens.45 The development of exosomes has also offered a new vector for gene therapy.46 In one work, systemic injection of dendritic cell-derived exosomes modified with RVG peptide targeting efficiently transported therapeutic siRNA to the animal brain, resulting in considerable gene silencing and pathological amelioration in an AD model.47 First, the RVG peptide, a particular ligand for neuronal acetylcholine receptors, was fused to the exosomal membrane protein Lamp2b, which endowed the exosomes with the capability of targeting the central nervous system. Next, siRNA targeting beta-secretase 1 was loaded into these RVG-targeted exosomes by electroporation. After tail vein injection into mice, these exosomes could pass the blood-brain barrier and selectively transport the siRNA to neurons, microglia and oligodendrocytes in the brain. The RVG-targeted exosomes showed great delivery efficiency, escaping significantly from nonspecific uptake in other brain regions compared with unmodified exosomes. BACE1 mRNA levels in the cerebral cortex were considerably reduced in animals treated with a co-injection of RVG-targeted exosomes loaded with BACE1 siRNA, as well as BACE1 protein levels. The Aβ levels in the brain of the mice also fell dramatically and no clear adverse effects were found, which confirmed the advantages of RVG-targeted exosomes in the gene treatment of AD.47
Photothermal therapy (PTT) is a multi-functional therapeutic method for AD via the localized thermal action of nanophotothermal agents (NPTAs) under near-infrared irradiation. The local thermal effect can open the BBB reversibly, allowing the delivery of therapeutic drugs into the brain. At the same time, the low thermal stability of Aβ aggregates makes it possible for photothermal treatment to effectively depolymerize Aβ aggregates and tau proteins, inhibit further Aβ aggregation, and thus reduce neurotoxicity and restore cognitive function.48–50 Nb 2 C MXenzyme as a stable neuroprotective platform can modulate metal ion-induced amyloid deposition through its multi-enzyme mimic capabilities and effectively alleviate neuroinflammation in AD. The nanoparticle employs its outstanding photothermal conversion efficiency to slightly raise the local temperature to about 43°C, which reversibly opens the BBB by the downregulation of vascular endothelial calmodulin and the relaxation of tight junctions between brain microvascular endothelial cells, enabling a large amount of intravenously injected nanoparticles to enter the brain parenchyma. Then, Nb2C: on the one hand, specifically chelates pathologically excess Cu2+ through its highly negatively charged surface, thereby breaking the chain of Cu2+-catalyzed Aβ aggregation and ROS generation; on the other hand, it has multi-enzyme activities similar to superoxide dismutase, catalase and peroxidase, and can directly scavenge preformed superoxide anions, hydrogen peroxide and hydroxyl radicals, thereby alleviating oxidative stress and neuroinflammation. In addition, the treatment group mice had significantly less Aβ plaque deposition in the hippocampus. Reduced expression of glial fibrillary acidic protein and calcium-binding protein 1 confirmed the suppression of activation of astrocytes and microglia, and the levels of the pro-inflammatory cytokines interleukin-1β and tumor necrosis factor-α also decreased significantly.51 This indicates the remarkable capacity of NPTAs to cross BBB for drug administration and the promise of nanoparticles in PTT for AD treatment. A nanomedicine, BP-MB, loaded nanoplates of black phosphorus (BP) with methylene blue (MB) was prepared. The 808-nanometer near-infrared light irradiation could induce the photothermal effect of black phosphorus to increase the local temperature to 41–43 degrees Celsius and reversibly downregulate the expression of ZO-1, a tight junction protein in the cerebral microvascular endothelial cells, temporarily impairing the structural integrity of the BBB; Meanwhile, BP-MB is taken up by endothelial cells predominantly via lamellin- and laminin-mediated endocytosis, followed by transport to the endoplasmic reticulum and Golgi apparatus, and finally released into the brain parenchyma through the Golgi/membrane secretory pathway, leading to highly efficient BBB delivery. Both BP and MB synergistically and efficiently scavenge excess ROS caused by neurotoxin OA or LPS to relieve oxidative stress. In addition, BP-MB can significantly limit the excessive phosphorylation of tau protein and reduce its neurotoxicity; BP-MB can successfully reverse neuronal apoptosis by restoring mitochondrial membrane potential and function and downregulating the expression of pro-apoptotic proteins Bax and Cleaved Caspase-3 in terms of neuroprotection. Furthermore, this nanoparticle promotes the polarization of microglia from the pro-inflammatory M1 phenotype to the anti-inflammatory M2 phenotype, thereby reducing damage caused by neuroinflammation and improving the pathological conditions of Alzheimer’s disease from multiple dimensions.52 RPDA@Rb-A is an engineered hybrid exosome nanoparticle constructed using membrane fusion technology; its unique multi-mechanism approach to crossing the BBB represents a novel therapeutic strategy for AD. Exosomal components derived from cerebral microvascular endothelial cells actively guide the nanoparticles across the BBB, while exosomal components from macrophages endow the nanoparticles with a natural tendency to migrate toward areas of inflammation within the brain. Meanwhile, near-infrared light irradiation is used not only for subsequent PTT but also to temporarily open the blood-brain barrier, further enhancing the efficiency of intracerebral delivery of the nanoparticles. This demonstrates the immense potential of these nanoparticles to treat Alzheimer’s disease by utilizing specialized mechanisms to cross the BBB.53
Nanoparticles for the Treatment of Parkinson’s Disease
Parkinson’s disease (PD) is a complex neurological illness marked by progressive loss of voluntary motor control. This is the most common clinical symptom of the disease and its incidence gradually increases with age.54 PD is the second most common neurodegenerative disease. PD is characterized by the conversion of soluble α-synuclein (α-syn) into neuronal aggregates and the degradation of neurons and their processes. Alpha-synuclein is a protein of presynaptic neurons that aggregates and accumulates in the development of Lewy bodies and Lewy neurons in the nervous system.55,56 Levodopa is the most often used medicine in the therapeutic treatment of Parkinson’s disease, and is often used in combination with anticholinergic agents, amantadine, monoamine oxidase inhibitors and dopamine receptor agonists. This pharmaceutical treatment gives good outcomes in the early phases of Parkinson’s disease. However, as the disease develops, certain patients eventually suffer difficulties such as “wearing off”, “on-off” occurrences, and motor abnormalities, which significantly affect their quality of life.57 However, currently there are no dopaminergic neuron-protective medications that can successfully delay disease development. Parkinson’s disease, thus, is a huge burden for the society and families, and the diagnosis and treatment are still hard.55,58,59 Nanoparticles can penetrate the BBB and ameliorate the diseased environment inside the brain by processes such as improving the intracerebral metabolic environment and decreasing neuroinflammation, thus treating PD symptoms (Figure 3).
 |
Figure 3 Nanoparticles Suppress Neuroinflammation. Under pathological situations, microglia switch to a pro-inflammatory M1 phenotype that secretes pro-inflammatory cytokines (eg, TNF-α, IL-1β, IL-6, IL-12, and CCL2), resulting in amplification of neuroinflammation and neuronal death. Nanoparticle treatment caused a phenotypic change of microglia to the anti-inflammatory M2 phenotype as indicated by increased expression of Arg-1, TGF-β and IL-10 and reduced release of inflammatory mediators. This phenotypic switch is achieved by nanoparticle-based processes, including the reduction of reactive oxygen species (ROS) and inhibition of phosphorylation of pathogenic proteins. Switching M1-to-M2 polarization alleviates neuro-inflammation, accelerates tissue regeneration and restores immunological homeostasis, which is an essential therapeutic strategy for the treatment of Alzheimer’s diseases, Parkinson’s diseases and other neurodegenerative diseases with nanoparticles. |
Human serum albumin (HSA)-based selenium nanoparticles (HSA/Se NPs), when administered orally, are able to sequentially cross the intestinal epithelial barrier and the blood-brain barrier (BBB) and accumulate in the dopaminergic neuron region of the compact part of the substantia nigra in the midbrain. HSA/Se NPs inhibit mitochondrial dysfunction and apoptosis via the Bcl-2-cytochrome C-caspase pathway: They restore mitochondrial membrane potential and ATP production, downregulate the expression of the mitochondrial fission protein Drp1, and upregulate the expression of the mitochondrial fusion proteins Mfn1, Mfn2, and Opa1, thereby maintaining normal mitochondrial morphology and function; simultaneously upregulating the anti-apoptotic protein Bcl-2 and downregulating the pro-apoptotic proteins Bax, cytochrome C, activated caspase-9, and activated caspase-3, thereby blocking the mitochondria-related apoptotic pathway. HSA/Se NPs also inhibit ferroptosis by activating the GPX4-SLC7A11-GSH pathway: By upregulating the expression of glutathione peroxidase 4 and the cysteine/glutamate antiporter SLC7A11, they increase GSH levels and the GSH/GSSG ratio, thereby inhibiting cell membrane lipid peroxidation. At the same time, they downregulate the expression of transferrin receptor 1, reducing intracellular iron accumulation and effectively inhibiting the occurrence of ferroptosis. Since apoptosis and ferroptosis are the core pathological mechanisms underlying the progressive loss of dopaminergic neurons in Parkinson’s disease, HSA/Se NPs protect dopaminergic neurons by inhibiting these two forms of cell death, specifically manifested by a significant restoration of the number of tyrosine hydroxylase-positive dopaminergic neurons and the expression levels of the TH protein in the substantia nigra and striatum, as well as an increase in the concentrations of dopamine and its metabolite, o-hydroxyvanillic acid, in substantia nigra tissue. At the same time, these nanoparticles demonstrated significantly low toxicity.60
As an innovative route of administration, the meningeal lymphatic pathway allows nanoparticles injected subcutaneously into the neck of mice to first be drained to the superficial and deep cervical lymph nodes. Subsequently, through the connections between these lymph nodes and the meningeal lymphatic vessels, the nanoparticles are efficiently transported into the brain, thereby completely bypassing the limitations of the BBB.61 Following administration via the meningeal lymphatic pathway, IHM NPs act intracellularly in two ways: first, by inhibiting the expression of the RAGE receptor on the surface of microglia, thereby reducing their excessive phagocytosis of α-syn aggregates; and, on the other hand, by significantly increasing the levels of mature cathepsin D in lysosomes, they enhance the efficient degradation of phagocytosed α-syn aggregates, thereby reducing the generation of α-syn antigenic peptides and decreasing antigen presentation mediated by major histocompatibility complex class II (MHC II) molecules; extracellularly, IRCM in heterozygous cell membranes, due to the high expression of inflammatory factor receptors such as IL1R1, TNFR1, and CCR2, these nanoparticles can bind inflammatory cytokines (such as IL-1β and TNF-α) and chemokines (such as CCL2 and CCL8), thereby blocking the recruitment and infiltration of peripheral CD4⁺ T cells into the brain and suppressing harmful immune crosstalk between microglia and T cells.61
Phytomolecules are essential for PD treatment because they act on the pathophysiological basis and exert neuroprotective effects via various mechanisms: antioxidant, anti-inflammatory, anti-apoptotic actions, inhibition of monoamine oxidase activity, and reduction of α-synuclein aggregation, unlike conventional drugs that offer symptomatic treatment by replacing dopamine. These phytomolecules can modulate several signaling pathways, boost the activity of endogenous antioxidant enzymes, preserve dopaminergic neurons in the substantia nigra and delay or arrest the progression of PD.62,63 As indicated before, nanogels have very good physical characteristics and can be used for PD treatment. What about mixing these nanogels with phytomolecules? Will this result in good therapeutic effects for PD? The simplest hydrolyzable tannin is tannic acid (TA).64 Tannic acid has gained considerable interest because of its broad physiologic effects (and its capacity to interact with many proteins) and the prospective implications of this interaction in materials science and engineering.65,66 BSA/Fe-TA NPs are a nanoenzyme based on tannic acid-iron combination. They exhibit various enzyme-like activities by their iron-catalyzed center including superoxide dismutase-like, catalase-like, glutathione peroxidase-like, ascorbate peroxidase-like and thiol peroxidase-like activities and can transform harmful substances such as superoxide anions and hydrogen peroxide into water and oxygen, and also directly scavenge reactive nitrogen species such as nitric oxide and peroxynitrite. More importantly, this nanoenzyme can also regulate the polarization state of microglia in brain, in oxidative stress condition, to promote the polarization of microglia from the pro-inflammatory M1 phenotype to the anti-inflammatory M2 phenotype, significantly decreasing the secretion of pro-inflammatory cytokines (such as IL-6 and IL-1β) and increasing the production of anti-inflammatory cytokines (such as IL-10), effectively alleviating neuroinflammation.67 The combination of phytomolecules with vesicles can also produce synergistic effects in the treatment of PD. Engineered extracellular vesicle-based nanoformulations (EVN) were prepared by coating nanocarriers (MSeN-DT) loaded with dihydrotanshinone I with CCR2-rich extracellular vesicles derived from mesenchymal stem cells (MSC CCR2 EVs). Following intravenous injection, these formulations respond to the concentration gradient of C-C motif chemokine ligand 2 (CCL2)—released by damaged neurons and capable of crossing the BBB—and, through an active “homing effect,” are effectively enriched from the bloodstream, penetrate the BBB, and enter the lesion sites in the brain parenchyma. Its shell suppresses neuroinflammation and delivers the dihydrotanshinone I loaded in the core to M1-type microglia; subsequently, dihydrotanshinone I is released in response to the high ROS environment at the lesion site. DT deeply activates the Nrf2-GPX4 signaling pathway: on the one hand, it promotes the nuclear translocation of Nrf2 to scavenge upstream-generated ROS; on the other hand, it upregulates GPX4 expression to specifically inhibit ferroptosis in microglia. This converts microglia from the pro-inflammatory M1 phenotype to the anti-inflammatory M2 phenotype, further suppressing neuroinflammation and alleviating the pathological progression of PD.68
Exosomes have also been applied in the treatment of PD. QAE NPs, composed of exosomes derived from mesenchymal stem cells co-loaded with the hydroxyl-terminated phospho-dendrimer AK76 and quercetin, Following intranasal administration, these nanoparticles efficiently penetrate the nasal mucosal barrier by leveraging the intrinsic biological properties of the exosomes and the strong interaction between the hydroxyl groups on the AK76 dendritic molecule and receptors on nasal mucosal epithelial cells, thereby bypassing the BBB to directly enter the brain. Once inside the brain, the exosomes, AK76, and quercetin carried by the QAE NPs jointly exert potent antioxidant and anti-inflammatory activities. They effectively scavenge ROS and, by downregulating the p-p65 and NLRP3 inflammatory signaling pathways, significantly inhibit the secretion of pro-inflammatory factors such as tumor necrosis factor-α, interleukin-1β, and interleukin-6, while promoting the polarization of microglia toward the anti-inflammatory and neuroprotective M2 phenotype, thereby reshaping the brain’s immune microenvironment; On the other hand, QAE NPs can also induce neuronal autophagy (by increasing LC3B staining and decreasing p62 protein levels) and restore mitochondrial membrane potential, thereby alleviating damage and apoptosis in dopaminergic neurons, and have demonstrated good biosafety in animal models.69 The biomimetic nanomodulator L@HT is constructed by fusing neuron-derived exosomes with ionizable liposomes, achieving highly efficient delivery across the BBB through T7 peptide-exosome synergy and ultrasound-assisted delivery. It improves motor dysfunction in Parkinson’s disease by elevating dopamine levels; simultaneously, by inhibiting the phosphorylation of TBK1/IRF3 downstream of the STING pathway and promoting the transition from the pro-inflammatory M1 phenotype to the anti-inflammatory M2 phenotype, it suppresses symptoms of neuroinflammation, thereby achieving a synergistic treatment for PD.70
Many nanoparticles utilize the unique characteristics of drug delivery and adjunctive therapies to overcome or bypass the BBB and deliver “drugs” to pathological regions in the brain; however, some nanoparticles still achieve active targeted transport by triggering receptor-mediated endocytosis. A multifunctional nanoparticle formulation based on nitrogen-doped carbon dots binds to lactoferrin (Lf) receptors overexpressed on BBB endothelial cells via Lf on its surface, triggering receptor-mediated endocytosis to achieve active targeted transport; On the other hand, the carbon dots (CDs) in the nanoparticle core can release NO under oxidative stress, inducing downregulation of tight junction proteins (such as ZO-1 and Claudin-5) and increased activity of matrix metalloproteinase-9, thereby reversibly increasing BBB permeability—effectively “actively” opening the BBB; Subsequently, CD efficiently chelates Fe2⁺ using the lone pair of electrons provided by its pyridine nitrogen site. The resulting complex not only blocks the catalytic cycle of iron in the Fenton reaction, preventing the continued generation of toxic hydroxyl radicals, but also transports the chelated iron ions out of the cell. Meanwhile, lactoferrin efficiently prevents the reabsorption of external iron ions into the cell by inhibiting the expression of divalent metal transportation 1 (DMT1), which in turn reduces the levels of the labile iron pool in the neurons. Furthermore, the nanformulation itself has strong reducing ability, which directly consumes excess intracellular ROS while removing iron ions, thus cutting off the source of oxidative stress damage, reshaping the brain microenvironment, and significantly reducing iron deposition in animal models, restoring the number of TH-positive dopaminergic neurons, suppressing neuroinflammation, and reducing inflammatory factors. More importantly, the BBB opening induced by this nanoparticle is temporary and reversible, and the nanoparticle can be cleared from the brain through the circulation of cerebrospinal fluid after treatment. Therefore, it does not cause significant toxicity to the major organs and shows extremely high biosafety. This gives new promise for treatment of PD.71
Nanoparticles for the Treatment of Huntington’s Disease
Huntington’s disease (HD) is an autosomal dominant, progressive neurodegenerative disorder caused by a cytosine -adenine-guanine (CAG) repeat expansion in the HTT gene, leading to an increase in polyglutamine repeats in the HTT protein and resulting in toxic gain-of-function. It is characterized by a unique phenotype, including chorea and dystonia, coordination deficits, cognitive decline, and behavioral abnormalities.72,73 Currently, there are no approved disease-modifying therapies targeting key pathway proteins in Huntington’s disease; many drugs can only alleviate symptoms (eg, tetrabenazine for relieving Huntington’s disease-related chorea), and previous disease-modifying drug candidates have encountered clinical setbacks due to an unfavorable benefit-risk ratio Therefore, exploring alternative disease-modifying mechanisms and therapeutic approaches is crucial.74 Research progress on nanoparticle-based therapies for Huntington’s disease primarily lies in their ability to achieve efficient crossing of the BBB through surface engineering modifications, enabling the precise delivery of therapeutic agents—such as siRNA, neurotrophic factors, and antioxidants—to affected regions of the brain, including the striatum and cortex. This has led to significant reductions in mutant huntingtin protein aggregation, alleviation of oxidative stress and mitochondrial dysfunction, and improvements in motor and cognitive function across various preclinical models.75,76
The hydrogel system is based on a self-assembling peptide (Fmoc-DDIKVAV) that is employed for the delivery of an adeno-associated virus (AAV-DJ) vector encoding the brain-derived neurotrophic factor (BDNF) gene, hence allowing the therapy of HD. The secret to this approach is the physical entrapment and subsequent controlled release of the AAV-DJ-BDNF viral vector from the nanofiber mesh of the hydrogel. This entrapment and controlled release is possible because of the mesh-like structure of the hydrogel (with pore diameters of roughly 20 nm, smaller than the 24–26 nm diameter of the AAV virus). After injection, the hydrogel constantly releases the viral vector in vivo, infecting local neurons and triggering long-term production and secretion of the BDNF protein. BDNF is a neurotrophic factor that protects neurons from excitotoxic injury and slows down or halts the neurodegenerative process induced by the mutant Huntington protein.77 Nano-EGCG(1) with surface dopamine functionalization preferentially binds to dopamine receptors that are highly expressed on the surface of neurons, thereby efficiently entering the cytoplasm through the membrane via endocytosis. The green tea polyphenol epigallocatechin-3-gallate molecules covalently linked to the NPs firmly attach to the mutant Huntington protein with multivalent interactions after internalization. The strong binding not only inhibits the conversion of soluble mutant protein into insoluble aggregates, but also promotes the disassembly of already produced intracellular aggregates, therefore drastically lowering the quantity of harmful aggregates inside the cell.78
Metal nanoparticles have intrinsic and therapeutic benefits in the treatment of neurodegenerative disorders. For instance they are easy to synthesis, have adjustable size and can be easily surface functionalized. Moreover, metal nanoparticles are also characterized by good biocompatibility and low toxicity, high specific surface area, excellent drug-loading capacity and flexible surface modification, so that they can produce therapeutic effect without additional drug.14,79–83 Prime examples include spherical gold nanoparticles (Au3@PEG1k NP) extensively modified on their surface by polyethylene glycol (PEG). After intravenous administration, these nanoparticles cross the BBB through active transport by endothelial cells, leading to significant enhancement of the oxidative phosphorylation pathway in the brain. The considerable overexpression of numerous proteins (such as Cox4i1, Cox5a, and Ndufb11) in the brains of HD mice reflects this, hence improving ATP generation efficiency and NAD+/NADH ratio, which further reverses the neuronal functional impairment caused by energy metabolism problems in HD. Meanwhile, these nanoparticles can effectively inhibit two pivotal kinases closely associated with HD pathology, p38α mitogen-activated protein kinase (p38α MAPK) and pyruvate dehydrogenase kinase 1, resulting in the suppression of neuroinflammation and restoration of the capacity of oxidative phosphorylation, which improves energy metabolism in the brain and alleviates the deterioration of the microenvironment caused by neuroinflammation.74 On the other hand, citrate-functionalized Mn3O4 nanoparticles (C-Mn3O4 NPs) can efficiently mimic the activity of glutathione peroxidase. With glutathione as a cofactor, they selectively catalyze the reduction of hydrogen peroxide to water and regenerate themselves to continue participating in the reaction, successfully scavenging ROS within and outside cells and avoiding the production of damaging free radicals. In an HD mouse model, these metal nanoparticles significantly reduced lipid peroxidation level in brain tissue and restored the activity of superoxide dismutase, catalase and glutathione peroxidase. They also attenuated mitochondrial swelling, stabilized mitochondrial membrane potential, increased ATP level and restored the activity of respiratory chain complexes II and IV, contributing to a decrease in mitochondrial ROS production and protection of neurons from oxidative damage. Histopathological sections of brain tissue of the treatment group of mice showed preservation of basal ganglia structure and Purkinje cells in the cerebellum with respect to therapeutic efficacy. This demonstrates the therapeutic efficacy of C-Mn3O4 NPs against HD.84
Nanoparticles offer considerable promise for therapeutics and can be used in a range of therapy techniques. Nanoparticles can deliver small-molecule medications and utilize their unique capabilities to traverse the BBB, achieving therapeutic effects that conventional small-molecule pharmaceuticals cannot achieve. Moreover, nanoparticles have the ability to deliver gene therapy vectors like siRNA to allow for precise targeted therapy, enabling novel options for the complete cure of neurodegenerative illnesses. However, the most important therapeutic approach is to improve the pathological environment in the brain. For example, regulating microglia to change from the pro-inflammatory type (M1 type) to the anti-inflammatory type (M2 type) can reduce the damage of neurons caused by neuroinflammation. Meanwhile, nanoparticles can realize the therapeutic effects through targeting the metabolic pathways for metabolic reprogramming, such as blocking the phosphorylation of several critical proteins and scavenging the ROS generated in the brain. What’s more, nanoparticles can degrade certain pathogenic proteins related to neurodegenerative illnesses to block the progress of the disease, delivering truly “targeted, highly effective and low-toxicity” drug delivery.
Challenges in the Clinical Translation of Nanoparticle-Based Drugs
Although NPs have demonstrated tremendous preclinical potential in overcoming the BBB and improving therapeutic outcomes in animal models, very few drugs for the treatment of neurodegenerative diseases have currently advanced to late-stage clinical trials, and there are virtually no clinical trials for NP-based treatments for neurodegenerative diseases (Table 1). The translation of this technology remains limited due to insufficient brain targeting in humans, toxicity issues associated with NPs, the complex pharmacokinetics and clearance processes of different NPs, and the difficulty of achieving large-scale production under Good Manufacturing Practice (GMP) standards.85–88
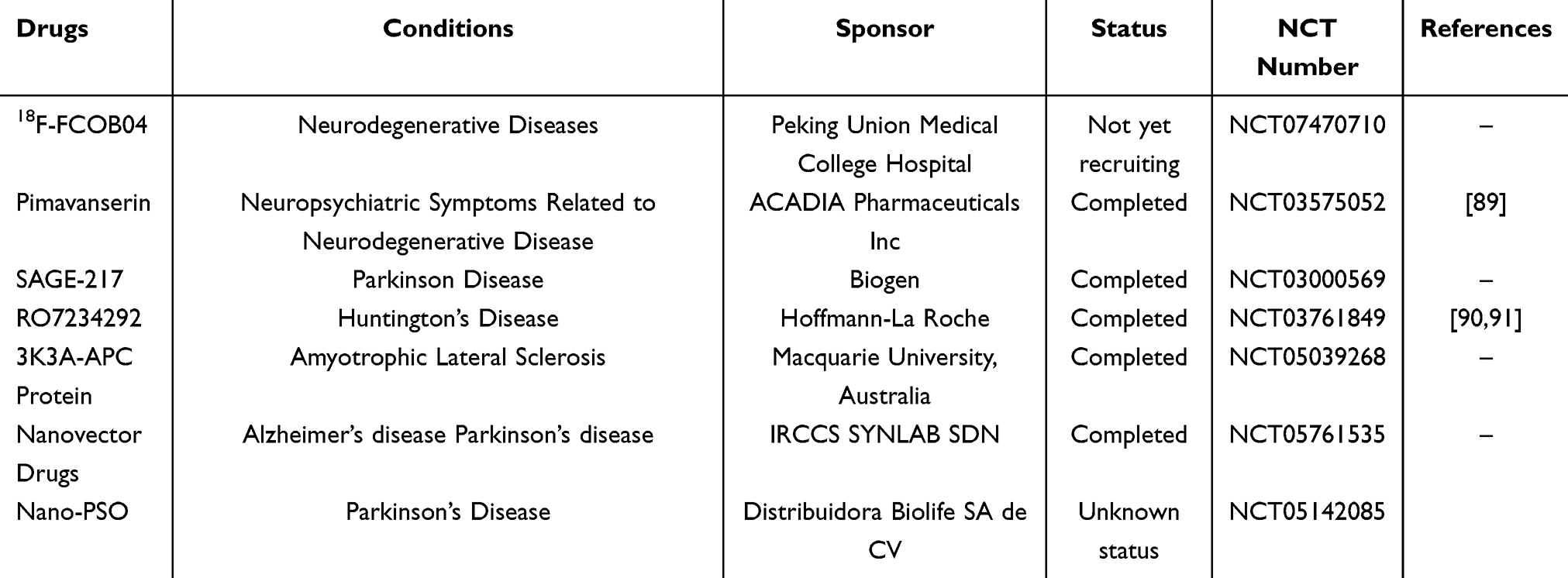 |
Table 1 Clinical Trials of Drugs for Neurodegenerative Diseases |
The toxicity of nanoparticles is a critical factor that must be considered when using them for drug delivery, current research focuses primarily on the ability of nanoparticles to reduce the toxicity of the drugs they carry, with little attention paid to the toxicity of the nanoparticles themselves.92 In particular, local or systemic toxicity resulting from nanoparticle-based therapies—such as that caused by cationic nanoparticles of gold and polystyrene, which have been shown to induce hemolysis and blood clotting—has been documented, and certain concentrations of both anionic and cationic nanoparticles have been found to be toxic to the BBB.93 The increased reactivity resulting from the large specific surface area of NPs not only enhances drug delivery efficiency but also increases the toxicity of the NPs themselves.94,95 The physical properties of nanoparticles, their concentration, and their in vivo biodistribution and clearance characteristics all modulate cellular endocytosis and nanoparticle toxicity.96–98 The solubility of nanoparticles is a key property influencing their acute toxicity; and the free ions released upon intracellular dissolution of certain metal oxide nanoparticles (such as zinc oxide and iron oxide) are associated with their toxicity. At the same time, because the use of nanoparticles for therapeutic purposes is a long-term process, their chronic toxicity should also be a focus of attention,99,100 especially since some nanoparticles can cause severe neurotoxicity (excessive ROS production, release of inflammatory factors, DNA damage, and apoptosis).101
At the same time, the most critical point is the difference in nanoparticle delivery between animal models and the human body. At this stage, research on nanoparticles for the treatment of neurodegenerative diseases is primarily focused on basic research. Although studies have shown that nanoparticles, as drug delivery systems, can treat neurodegenerative diseases through various therapeutic approaches, it remains to be seen whether they can demonstrate the same therapeutic effects in humans. Furthermore, the extent of the difference in nanoparticles’ ability to cross the BBB in vivo versus in vitro remains unclear, as does whether this will have a significant impact on delivery efficacy. Therefore, the most critical step at this stage is to advance nanoparticle research into clinical trials. Translational research is a key step in transforming basic research into clinical applications, and this is particularly important for nanoparticles. However, the process of translational research is lengthy and involves numerous requirements; fewer than 10% of basic research projects are ultimately translated into clinical applications. However, in the specialized field of nanoparticles—where different nanomaterials possess distinct mechanisms of action and target different sites—substantial financial support is required.102 At the same time, human trials require ethical approval; however, early-stage nanoparticle trials are unlikely to provide any benefit to participants, making the implementation of clinical trials extremely difficult.103 Furthermore, to enable the clinical application of nanoparticles, their preparation must adhere to predetermined standards of quality, controls, and good manufacturing practices.104 The cost of manufacturing nanoparticles cannot be overlooked; the probability of successfully translating small-molecule drugs from the preclinical proof-of-concept stage to commercially available products is extremely low.105 Even without considering development risks, the formulation of nanoparticles is complex, the process is lengthy, and the cost of production is high; furthermore, the cost-effectiveness of nanoparticles must be weighed against that of less expensive drug therapies.103,106
Conclusions
Nanoparticles hold significant potential for technology to cross the BBB and treat neurodegenerative diseases. This review systematically summarizes the different applications of nanomaterials in Alzheimer’s disease, Parkinson’s disease, and Huntington’s disease, covering a range of strategies including receptor-mediated endocytosis, intranasal administration, meningeal lymphatic pathway, photothermal-assisted barrier opening, and biomimetic delivery systems based on exosomes and cell membranes. The research had showed significant therapeutic efficacy in animal models, demonstrating the adaptability and promise of nanoparticle platforms for delivery of tiny drugs, nucleic acids, proteins and gene-editing tools.
However, we must clearly recognize that a fundamental gap still exists between animal experiments and clinical application. Currently, no nanomedicines targeting neurodegenerative diseases have entered Phase III clinical trials; this reality suggests that current “successes” remain largely confined to the proof-of-concept stage. Existing studies generally share the following common issues: a lack of head-to-head comparisons between different nanotechnology platforms; extremely limited understanding of the long-term retention, metabolism, and chronic toxicity of nanoparticles in the brain; animal models (especially transgenic mice) that fail to adequately simulate the heterogeneity of human diseases and age-related pathological backgrounds; and the fact that most studies focus on a single target or mechanism as an endpoint, neglecting the multifactorial nature of the disease.
Therefore, we need to gradually address the challenges of clinical translation for nanoparticles. First, we can build upon nanoplatforms based on theoretically well-supported materials (such as exosomes and metal nanoparticles), as their relatively mature toxicological and pharmacokinetic data allow for faster entry into the pathway for modified new drugs; At the same time, we can focus on researching intranasal nanogel or thermosensitive hydrogel systems, as they bypass the BBB and offer controllable risks associated with local administration, demonstrating good feasibility and safety; and we can adopt physical strategies for opening the BBB centered on photothermal therapy or ultrasound-assisted methods, which, through a combination of in vivo and in vitro approaches, use ex vivo interventions to enhance the ability of nanoparticles to cross the BBB and facilitate efficient drug release, which reduces the complexity of nanoparticle design. Subsequently, we must establish uniform standards for nanoparticle production, including mandatory requirements regarding preparation methods, cost, safety, and drug-loading efficiency.
Data Sharing Statement
Data availability is not applicable to this article as no new data were created or analyzed in this study.
Acknowledgments
The authors gratefully acknowledge BioRender (https://www.biorender.com/) for providing the platform used to create the graphical illustrations. All figures are original and were created using BioRender, with appropriate publication rights obtained.
Funding
This research was supported by the Liaoning Provincial Department of Science and Technology, General Program, 2025 Joint Science and Technology Plan Project (No. 5021342), and Youth Medical Expert of Project of Xingliao Gifted Person Program of Liaoning Province (No. XLYC2512073).
Disclosure
The authors declare no competing interests in this work.
References
1. Bianchi VE, Herrera PF, Laura R. Effect of nutrition on neurodegenerative diseases. A systematic review. Nutr Neurosci. 2021;24(10):810–16. doi:10.1080/1028415X.2019.1681088
2. Lamptey RNL, Chaulagain B, Trivedi R, et al. A review of the common neurodegenerative disorders: current therapeutic approaches and the potential role of nanotherapeutics. Int J Mol Sci. 2022;23(3):1851. doi:10.3390/ijms23031851
3. 2024 Alzheimer’s disease facts and figures. Alzheimers Dement. 2024;20(5):3708–3821. doi:10.1002/alz.13809
4. Vogt AS, Jennings GT, Mohsen MO, et al. Alzheimer’s disease: a brief history of immunotherapies targeting amyloid β. Int J Mol Sci. 2023;24(4):3895. doi:10.3390/ijms24043895
5. Ajayi ED, Elazazy M, Abouzid K, et al. Breaking barriers: medicinal chemistry strategies and advanced in-silico approaches for overcoming the BBB and enhancing CNS penetration. Eur J Med Chem. 2025;301:118219. doi:10.1016/j.ejmech.2025.118219
6. Patel NC. Methods to optimize CNS exposure of drug candidates. Bioorg Med Chem Lett. 2020;30(23):127503. doi:10.1016/j.bmcl.2020.127503
7. Akhtar A, Andleeb A, Waris TS, et al. Neurodegenerative diseases and effective drug delivery: a review of challenges and novel therapeutics. J Control Release. 2021;330:1152–1167. doi:10.1016/j.jconrel.2020.11.021
8. Zhao X, Qi X, Liu D, Che X, Wu G. A novel approach for bladder cancer treatment: nanoparticles as a drug delivery system. Int J Nanomed. 2024;19:13461–13483. doi:10.2147/IJN.S498729
9. Wang Y, Ge M, Wang J, Xu Y, Wang N, Xu S. Metabolic reprogramming in ischemic stroke: when glycolytic overdrive meets lipid storm. Cell Death Dis. 2025;16(1):788. doi:10.1038/s41419-025-08114-w
10. Naghib SM, Khorasani MA, Sharifianjazi F, et al. Bifunctional chitosan-based nanocarriers as promising therapeutic approach for brain disease therapy: a critical review focusing on multiple sclerosis over emerging strategies, technologies and applications. Int J Biol Macromol. 2025;330:148003. doi:10.1016/j.ijbiomac.2025.148003
11. Chen T, Duan Y, Wang Y, et al. Size-variable self-feedback nanomotors for glioblastoma therapy via mitochondrial mineralization. Nat Commun. 2025;16(1):8990. doi:10.1038/s41467-025-64020-x
12. Goldsmith M, Abramovitz L, Peer D. Precision nanomedicine in neurodegenerative diseases. ACS Nano. 2014;8(3):1958–1965. doi:10.1021/nn501292z
13. Szunyogh S, Carroll E, Wade-Martins R. Recent developments in gene therapy for Parkinson’s disease. Mol Ther. 2025;33(5):2052–2064. doi:10.1016/j.ymthe.2025.03.030
14. Nayab DE, Din FU, Ali H, et al. Nano biomaterials based strategies for enhanced brain targeting in the treatment of neurodegenerative diseases: an up-to-date perspective. J Nanobiotechnology. 2023;21(1):477. doi:10.1186/s12951-023-02250-1
15. Stanciu GD, Costachescu I, Dascalu C, et al. Smart drug-delivery approaches for enhanced management of comorbid conditions in Alzheimer’s disease. Life. 2026;16(3):510. doi:10.3390/life16030510
16. Hettiarachchi SD, Zhou Y, Seven E, et al. Nanoparticle-mediated approaches for Alzheimer’s disease pathogenesis, diagnosis, and therapeutics. J Control Release. 2019;314:125–140. doi:10.1016/j.jconrel.2019.10.034
17. Obermeier B, Daneman R, Ransohoff RM. Development, maintenance and disruption of the blood-brain barrier. Nat Med. 2013;19(12):1584–1596. doi:10.1038/nm.3407
18. Abbott NJ, Rönnbäck L, Hansson E. Astrocyte-endothelial interactions at the blood-brain barrier. Nat Rev Neurosci. 2006;7(1):41–53. doi:10.1038/nrn1824
19. Zhao Z, Nelson AR, Betsholtz C, et al. Establishment and dysfunction of the blood-brain barrier. Cell. 2015;163(5):1064–1078. doi:10.1016/j.cell.2015.10.067
20. Palmer AM. The role of the blood-CNS barrier in CNS disorders and their treatment. Neurobiol Dis. 2010;37(1):3–12. doi:10.1016/j.nbd.2009.07.029
21. Garbuzova-Davis S, Saporta S, Sanberg PR. Implications of blood-brain barrier disruption in ALS. Amyotroph Lateral Scler. 2008;9(6):375–376. doi:10.1080/17482960802160990
22. Stolp HB, Dziegielewska KM. Review: role of developmental inflammation and blood-brain barrier dysfunction in neurodevelopmental and neurodegenerative diseases. Neuropathol Appl Neurobiol. 2009;35(2):132–146. doi:10.1111/j.1365-2990.2008.01005.x
23. Alkhalifa AE, Al-Ghraiybah NF, Odum J, et al. Blood-brain barrier breakdown in Alzheimer’s disease: mechanisms and targeted strategies. Int J Mol Sci. 2023;24(22):16288. doi:10.3390/ijms242216288
24. Furtado D, Björnmalm M, Ayton S, et al. Overcoming the blood-brain barrier: the role of nanomaterials in treating neurological diseases. Adv Mater. 2018;30(46):e1801362. doi:10.1002/adma.201801362
25. Battaglini M, Marino A, Montorsi M, et al. Nanomaterials as microglia modulators in the treatment of central nervous system disorders. Adv Healthc Mater. 2024;13(12):e2304180. doi:10.1002/adhm.202304180
26. Gonzalez-Carter D, Liu X, Tockary TA, et al. Targeting nanoparticles to the brain by exploiting the blood-brain barrier impermeability to selectively label the brain endothelium. Proc Natl Acad Sci U S A. 2020;117(32):19141–19150. doi:10.1073/pnas.2002016117
27. Nguyen TT, Dung Nguyen TT, Vo TK, et al. Nanotechnology-based drug delivery for central nervous system disorders. Biomed Pharmacother. 2021;143:112117. doi:10.1016/j.biopha.2021.112117
28. Chen L, Cruz E, Oikari LE, et al. Opportunities and challenges in delivering biologics for Alzheimer’s disease by low-intensity ultrasound. Adv Drug Deliv Rev. 2022;189:114517. doi:10.1016/j.addr.2022.114517
29. Hodson R. Alzheimer’s disease. Nature. 2018;559(7715):S1. doi:10.1038/d41586-018-05717-6
30. Zheng Q, Wang X. Alzheimer’s disease: insights into pathology, molecular mechanisms, and therapy. Protein Cell. 2025;16(2):83–120. doi:10.1093/procel/pwae026
31. Chen Y, Yu Y. Tau and neuroinflammation in Alzheimer’s disease: interplay mechanisms and clinical translation. J Neuroinflammation. 2023;20(1):165. doi:10.1186/s12974-023-02853-3
32. Bolognesi ML, Rosini M, Andrisano V, et al. MTDL design strategy in the context of Alzheimer’s disease: from lipocrine to memoquin and beyond. Curr Pharm Des. 2009;15(6):601–613. doi:10.2174/138161209787315585
33. Sarlus H, Heneka MT. Microglia in Alzheimer’s disease. J Clin Invest. 2017;127(9):3240–3249. doi:10.1172/JCI90606
34. Jung ES, Choi H, Mook-Jung I. Decoding microglial immunometabolism: a new frontier in Alzheimer’s disease research. Mol Neurodegener. 2025;20(1):37. doi:10.1186/s13024-025-00825-0
35. Singh D. Astrocytic and microglial cells as the modulators of neuroinflammation in Alzheimer’s disease. J Neuroinflammation. 2022;19(1):206. doi:10.1186/s12974-022-02565-0
36. Liu P, Zhang T, Wu Y, et al. A peptide-drug conjugate-based nanoplatform for immunometabolic activation and in situ nerve regeneration in advanced-stage Alzheimer’s disease. Adv Mater. 2024;36(46):e2408729. doi:10.1002/adma.202408729
37. Casamassa A, Brancaccio P, Campani V, et al. A new nano-encapsulated TSPO ligand reduces neuroinflammation and improves cognitive functions in Alzheimer’s disease model. Theranostics. 2025;15(10):4673–4692. doi:10.7150/thno.106083
38. Yang L, Wang Y, Zheng G, et al. Resveratrol-loaded selenium/chitosan nano-flowers alleviate glucolipid metabolism disorder-associated cognitive impairment in Alzheimer’s disease. Int J Biol Macromol. 2023;239:124316. doi:10.1016/j.ijbiomac.2023.124316
39. Lin RR, Jin -L-L, Xue -Y-Y, et al. Hybrid Membrane-Coated Nanoparticles for Precise Targeting and Synergistic Therapy in Alzheimer’s Disease. Adv Sci. 2024;11(24):e2306675. doi:10.1002/advs.202306675
40. Agrawal M, Saraf S, Saraf S, et al. Nose-to-brain drug delivery: an update on clinical challenges and progress towards approval of anti-Alzheimer drugs. J Control Release. 2018;281:139–177. doi:10.1016/j.jconrel.2018.05.011
41. Liu Y, Tan Y, Cheng G, et al. Customized intranasal hydrogel delivering methylene blue ameliorates cognitive dysfunction against Alzheimer’s disease. Adv Mater. 2024;36(19):e2307081. doi:10.1002/adma.202307081
42. Zheng X, Shao X, Zhang C, et al. Intranasal H102 peptide-loaded liposomes for brain delivery to treat Alzheimer’s disease. Pharm Res. 2015;32(12):3837–3849. doi:10.1007/s11095-015-1744-9
43. Liu Y, Xia X, Zheng M, et al. Bio-nano toolbox for precision Alzheimer’s disease gene therapy. Adv Mater. 2024;36(29):e2314354. doi:10.1002/adma.202314354
44. Jiang S, Cai G, Yang Z, et al. Biomimetic nanovesicles as a dual gene delivery system for the synergistic gene therapy of Alzheimer’s disease. ACS Nano. 2024;18(18):11753–11768. doi:10.1021/acsnano.3c13150
45. Wu X, Zheng T, Zhang B. Exosomes in Parkinson’s disease. Neurosci Bull. 2017;33(3):331–338. doi:10.1007/s12264-016-0092-z
46. Emanueli C, Shearn AIU, Angelini GD, et al. Exosomes and exosomal miRNAs in cardiovascular protection and repair. Vascul Pharmacol. 2015;71:24–30. doi:10.1016/j.vph.2015.02.008
47. Alvarez-Erviti L, Seow Y, Yin H, et al. Delivery of siRNA to the mouse brain by systemic injection of targeted exosomes. Nat Biotechnol. 2011;29(4):341–345. doi:10.1038/nbt.1807
48. Chen J, Zhang X, Sun J, et al. Photothermal nano-agents: an innovative trident weapon for accurate and effective treatment of Alzheimer’s disease. J Nanobiotechnology. 2025;23(1):650. doi:10.1186/s12951-025-03709-z
49. Liang X, Wang Y, Song J, et al. Nontoxic silicene photothermal agents with high near-infrared absorption for disassembly of Alzheimer’s amyloid‑β fibrils. Colloids Surf B Biointerfaces. 2022;216:112575. doi:10.1016/j.colsurfb.2022.112575
50. Zeng F, Peng K, Han L, et al. Photothermal and photodynamic therapies via NIR-activated nanoagents in combating Alzheimer’s disease. ACS Biomater Sci Eng. 2021;7(8):3573–3585. doi:10.1021/acsbiomaterials.1c00605
51. Du C, Feng W, Dai X, et al. Cu(2+)-Chelatable and ROS-Scavenging MXenzyme as NIR-II-Triggered blood-brain barrier-crossing nanocatalyst against Alzheimer’s disease. Small. 2022;18(39):e2203031. doi:10.1002/smll.202203031
52. Xie A, Cheng G, Wu J, et al. Highly BBB-permeable nanomedicine reverses neuroapoptosis and neuroinflammation to treat Alzheimer’s disease. Biomaterials. 2025;312:122749. doi:10.1016/j.biomaterials.2024.122749
53. Du B, Zou Q, Wang X, et al. Multi-targeted engineered hybrid exosomes as Aβ nanoscavengers and inflammatory modulators for multi-pathway intervention in Alzheimer’s disease. Biomaterials. 2025;322:123403. doi:10.1016/j.biomaterials.2025.123403
54. Lotankar S, Prabhavalkar KS, Bhatt LK. Biomarkers for Parkinson’s disease: recent advancement. Neurosci Bull. 2017;33(5):585–597. doi:10.1007/s12264-017-0183-5
55. Dawson VL, Dawson TM. Promising disease-modifying therapies for Parkinson’s disease. Sci Transl Med. 2019;11(520). doi:10.1126/scitranslmed.aba1659
56. Spillantini MG, Crowther RA, Jakes R, et al. alpha-Synuclein in filamentous inclusions of Lewy bodies from Parkinson’s disease and dementia with Lewy bodies. Proc Natl Acad Sci U S A. 1998;95(11):6469–6473. doi:10.1073/pnas.95.11.6469
57. Armstrong MJ, Okun MS. Diagnosis and Treatment of Parkinson Disease: a Review. JAMA. 2020;323(6):548–560. doi:10.1001/jama.2019.22360
58. Costa HN, Esteves AR, Empadinhas N, Cardoso SM. Parkinson’s Disease: a Multisystem Disorder. Neurosci Bull. 2023;39(1):113–124. doi:10.1007/s12264-022-00934-6
59. The Lancet N. Parkinson’s disease needs an urgent public health response. Lancet Neurol. 2022;21(9):759. doi:10.1016/S1474-4422(22)00312-X
60. Xu K, Huang P, Wu Y, et al. Engineered selenium/human serum albumin nanoparticles for efficient targeted treatment of Parkinson’s disease via oral gavage. ACS Nano. 2023;17(20):19961–19980. doi:10.1021/acsnano.3c05011
61. Zheng Q, Gao Y, Han M, et al. Inhibiting immune crosstalk by modulation of the intracellular function and extracellular environment of diseased microglia to boost Parkinson’s disease therapy. ACS Nano. 2025;19(20):19177–19197. doi:10.1021/acsnano.5c01068
62. Pradhan SP, Tejaswani P, Behera A, Sahu PK. Phytomolecules from conventional to nano form: next-generation approach for Parkinson’s disease. Ageing Res Rev. 2024;93:102136.
63. Yavarpour-Bali H, Ghasemi-Kasman M, Pirzadeh M. Curcumin-loaded nanoparticles: a novel therapeutic strategy in treatment of central nervous system disorders. Int J Nanomed. 2019;14:4449–4460. doi:10.2147/IJN.S208332
64. Jing W, Xiaolan C, Yu C, Feng Q, Haifeng Y. Pharmacological effects and mechanisms of tannic acid. Biomed Pharmacother. 2022;154:113561. doi:10.1016/j.biopha.2022.113561
65. Guo Z, Xie W, Lu J, et al. Tannic acid-based metal phenolic networks for bio-applications: a review. J Mater Chem B. 2021;9(20):4098–4110. doi:10.1039/D1TB00383F
66. Fu H, Wang Y, Huang B, et al. Tannic acid‑cerium nanoenzymes serve as broad-spectrum antioxidants to alleviate acute kidney injury by modulating macrophage polarization, mitophagy and endoplasmic reticulum stress. J Control Release. 2025;380:892–909. doi:10.1016/j.jconrel.2025.02.038
67. He W, Liu M, Zhang T, et al. Tannic acid-iron complex-based nanozyme ameliorates Parkinson’s disease via relieving oxidative stress and neuroinflammation. ACS Nano. 2025;19(37):33212–33229. doi:10.1021/acsnano.5c07601
68. Zhang C, Shao W, Yuan H, et al. Engineered extracellular vesicle-based nanoformulations that coordinate neuroinflammation and immune homeostasis, enhancing Parkinson’s disease therapy. ACS Nano. 2024;18(34):23014–23031. doi:10.1021/acsnano.4c04674
69. Zhang L, Zhan M, Sun H, et al. Mesenchymal stem-cell-derived exosomes loaded with phosphorus dendrimers and quercetin treat Parkinson’s disease by modulating inflammatory immune microenvironment. ACS Appl Mater Interfaces. 2025;17(22):32013–32027. doi:10.1021/acsami.5c05809
70. Yang L, Li S, Hou C, et al. Biomimetic nanoregulators mediated tyrosine hydroxylase mRNA and Stimulator of interferon genes antagonist codelivery for synergistic therapy on Parkinson’s disease. ACS Nano. 2025;19(38):33734–33748. doi:10.1021/acsnano.5c00694
71. Guo W, Ji M, Li Y, et al. Iron ions-sequestrable and antioxidative carbon dot-based nano-formulation with nitric oxide release for Parkinson’s disease treatment. Biomaterials. 2024;309:122622. doi:10.1016/j.biomaterials.2024.122622
72. Walker FO. Huntington’s disease. Lancet. 2007;369(9557):218–228.
73. The Huntington’s Disease Collaborative Research Group. A novel gene containing a trinucleotide repeat that is expanded and unstable on Huntington’s disease chromosomes. Cell. 1993;72(6):971–983. doi:10.1016/0092-8674(93)90585-E
74. Lee LKC, Leong LI, Shyngys M, et al. Small gold nanoparticles alleviate Huntington’s disease via modulating p38α mitogen-activated protein kinase and pyruvate dehydrogenase kinase 1. ACS Nano. 2026;20(1):683–699. doi:10.1021/acsnano.5c14751
75. André EM, Passirani C, Seijo B, Sanchez A, c n M-M. Nano and microcarriers to improve stem cell behaviour for neuroregenerative medicine strategies: application to Huntington’s disease. Biomaterials. 2016;83:347–362. doi:10.1016/j.biomaterials.2015.12.008
76. Zhang J, Nie L, Ma J, Wang X. Surface-engineered precision nano-systems for targeted treatment of Huntington’s disease: a review of recent advancements. Int J Nanomed. 2026;21:548892. doi:10.2147/IJN.S548892
77. Dehnavi SS, Mahmoudi N, Wang Y, et al. Renovating neural networks with viral-mediated gene transfer from a tissue contacting matrix mimic. Small. 2026;22(17):e10539. doi:10.1002/smll.202510539
78. Debnath K, Shekhar S, Kumar V, Jana NR, Jana NR. Efficient inhibition of protein aggregation, disintegration of aggregates, and lowering of cytotoxicity by green tea polyphenol-based self-assembled polymer nanoparticles. ACS Appl Mater Interfaces. 2016;8(31):20309–20318. doi:10.1021/acsami.6b06853
79. Sela H, Cohen H, Elia P, et al. Spontaneous penetration of gold nanoparticles through the blood brain barrier (BBB). J Nanobiotechnology. 2015;13:71. doi:10.1186/s12951-015-0133-1
80. Ruff J, Hüwel S, Kogan MJ, et al. The effects of gold nanoparticles functionalized with ß-amyloid specific peptides on an in vitro model of blood-brain barrier. Nanomedicine. 2017;13(5):1645–1652. doi:10.1016/j.nano.2017.02.013
81. Nday CM, Halevas E, Jackson GE, et al. Quercetin encapsulation in modified silica nanoparticles: potential use against Cu(II)-induced oxidative stress in neurodegeneration. J Inorg Biochem. 2015;145:51–64. doi:10.1016/j.jinorgbio.2015.01.001
82. Zheng X, Wu Y, Zuo H, et al. Metal nanoparticles as novel agents for lung cancer diagnosis and therapy. Small. 2023;19(18):e2206624. doi:10.1002/smll.202206624
83. Cong W, Bai R, Li Y-F, et al. Selenium nanoparticles as an efficient nanomedicine for the therapy of Huntington’s disease. ACS Appl Mater Interfaces. 2019;11(38):34725–34735. doi:10.1021/acsami.9b12319
84. Adhikari A, Mondal S, Das M, et al. Incorporation of a biocompatible nanozyme in cellular antioxidant enzyme cascade reverses Huntington’s like disorder in preclinical model. Adv Healthc Mater. 2021;10(7):e2001736. doi:10.1002/adhm.202001736
85. Souto EB, Silva GF, Dias-Ferreira J, et al. Nanopharmaceutics: Part I-Clinical Trials Legislation and Good Manufacturing Practices (GMP) of Nanotherapeutics in the EU. Pharmaceutics. 2020;12(2):146. doi:10.3390/pharmaceutics12020146
86. Abd El-Fattah MA. Challenges and opportunities of drug delivery for treatment of Alzheimer’s disease. AAPS Pharm Sci Tech. 2026;27(1):78. doi:10.1208/s12249-025-03316-z
87. Scott K, Klaus SP. Focused ultrasound therapy for Alzheimer’s disease: exploring the potential for targeted amyloid disaggregation. Front Neurol. 2024;15:1426075.
88. Singh B, Day CM, Abdella S, Garg S. Alzheimer’s disease current therapies, novel drug delivery systems and future directions for better disease management. J Control Release. 2024;367:402–424. doi:10.1016/j.jconrel.2024.01.047
89. Alva G, Cubała WJ, Berrio A, et al. Safety profile of pimavanserin therapy in elderly patients with neurodegenerative disease-related neuropsychiatric symptoms: a Phase 3B Study. J Alzheimers Dis. 2024;98(1):265–274. doi:10.3233/JAD-231167
90. Rodrigues FB, Ferreira JJ, Wild EJ. Huntington’s disease clinical trials corner: June 2019. J Huntingtons Dis. 2019;8(3):363–371. doi:10.3233/JHD-199003
91. Lugrin C, Alecci L, Simillion C, et al. Longitudinal assessment of chorea in Huntington’s disease using digital passive monitoring. NPJ Digit Med. 2026;9. doi:10.1038/s41746-026-02661-y
92. Zhang J, Wang F, Yalamarty SSK, Filipczak N, Jin Y, Li X. Nano silver-induced toxicity and associated mechanisms. Int J Nanomed. 2022;17:1851–1864. doi:10.2147/IJN.S355131
93. De Jong WH, Borm PJ. Drug delivery and nanoparticles: applications and hazards. Int J Nanomed. 2008;3(2):133–149.
94. Arora S, Rajwade JM, Paknikar KM. Nanotoxicology and in vitro studies: the need of the hour. Toxicol Appl Pharmacol. 2012;258(2):151–165.
95. Karlsson HL, Gustafsson J, Cronholm P, et al. Size-dependent toxicity of metal oxide particles--a comparison between nano- and micrometer size. Toxicol Lett. 2009;188(2):112–118. doi:10.1016/j.toxlet.2009.03.014
96. Najahi-Missaoui W, Arnold RD, Cummings BS. Safe nanoparticles: are we there yet? Int J Mol Sci. 2020;22(1):385. doi:10.3390/ijms22010385
97. Ali M. What function of nanoparticles is the primary factor for their hyper-toxicity? Adv Colloid Interface Sci. 2023;314:102881.
98. Midander K, Cronholm P, Karlsson HL, et al. Surface characteristics, copper release, and toxicity of nano- and micrometer-sized copper and copper(II) oxide particles: a cross-disciplinary study. Small. 2009;5(3):389–399. doi:10.1002/smll.200801220
99. Neetika, Sharma M, Thakur P, et al. Cancer treatment and toxicity outlook of nanoparticles. Environ Res. 2023;237(Pt 1):116870.
100. Shi J, Han S, Zhang J, et al. Advances in genotoxicity of titanium dioxide nanoparticles in vivo and in vitro. NanoImpact. 2022;25:100377. doi:10.1016/j.impact.2021.100377
101. Hussain Z, Thu HE, Elsayed I, et al. Nano-scaled materials may induce severe neurotoxicity upon chronic exposure to brain tissues: a critical appraisal and recent updates on predisposing factors, underlying mechanism, and future prospects. J Control Release. 2020;328:873–894.
102. Liang G, Cao W, Tang D, et al. Nanomedomics. ACS Nano. 2024;18(17):10979–11024. doi:10.1021/acsnano.3c11154
103. Satalkar P, Elger BS, Hunziker P, et al. Challenges of clinical translation in nanomedicine: a qualitative study. Nanomedicine. 2016;12(4):893–900. doi:10.1016/j.nano.2015.12.376
104. Gonzalez-Valdivieso J, Girotti A, Schneider J, et al. Advanced nanomedicine and cancer: challenges and opportunities in clinical translation. Int J Pharm. 2021;599:120438. doi:10.1016/j.ijpharm.2021.120438
105. Cook D, Brown D, Alexander R, et al. Lessons learned from the fate of AstraZeneca’s drug pipeline: a five-dimensional framework. Nat Rev Drug Discov. 2014;13(6):419–431. doi:10.1038/nrd4309
106. Metselaar JM, Lammers T. Challenges in nanomedicine clinical translation. Drug Deliv Transl Res. 2020;10(3):721–725. doi:10.1007/s13346-020-00740-5
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
pH/Redox Dual-Responsive Drug Delivery System with on-Demand RGD Exposure for Photochemotherapy of Tumors

Li Y, Nie J, Dai J, Yin J, Huang B, Liu J, Chen G, Ren L
International Journal of Nanomedicine 2022, 17:5621-5639
Published Date: 23 November 2022
Applications of Carbon Dots for the Treatment of Alzheimer’s Disease

Guo F, Li Q, Zhang X, Liu Y, Jiang J, Cheng S, Yu S, Zhang X, Liu F, Li Y, Rose G, Zhang H
International Journal of Nanomedicine 2022, 17:6621-6638
Published Date: 23 December 2022
Multifunctional Nanoparticles Codelivering Doxorubicin and Amorphous Calcium Carbonate Preloaded with Indocyanine Green for Enhanced Chemo-Photothermal Cancer Therapy

Yu J, Wang L, Xie X, Zhu W, Lei Z, Lv L, Yu H, Xu J, Ren J
International Journal of Nanomedicine 2023, 18:323-337
Published Date: 18 January 2023
Mucoadhesive-to-Mucopenetrating Nanoparticles for Mucosal Drug Delivery: A Mini Review
Zheng B, Liu D, Qin X, Zhang D, Zhang P
International Journal of Nanomedicine 2025, 20:2241-2252
Published Date: 20 February 2025
Progress in the Application of Novel Nanomaterials in Targeted Therapy for Liver Cancer

Wei X, Cao W, Wang S, Zhang Y, Gao Z, Wang S, Yao L, Zhang Z, Li X, Deng W, Xie Y, Li M
International Journal of Nanomedicine 2025, 20:2623-2643
Published Date: 3 March 2025