")
Back to Journals » International Journal of Nanomedicine » Volume 19
Nanoparticles for the Treatment of Bone Metastasis in Breast Cancer: Recent Advances and Challenges
Received 26 October 2023
Accepted for publication 15 February 2024
Published 23 February 2024 Volume 2024:19 Pages 1867—1886
DOI https://doi.org/10.2147/IJN.S442768
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor R.D.K. Misra
Xianzhe Yu,1,2 Lingling Zhu1
1Department of Medical Oncology, Cancer Center & Lung Cancer Center/Lung Cancer Institute, West China Hospital, Sichuan University, Chengdu, Sichuan Province, People’s Republic of China; 2Department of Gastrointestinal Surgery, Chengdu Second People’s Hospital, Chengdu, Sichuan Province, People’s Republic of China
Correspondence: Lingling Zhu, Department of Medical Oncology, Cancer Center & Lung Cancer Center/Lung Cancer Institute, West China Hospital, Sichuan University, No. 37, Guo Xue Xiang, Wuhou District, Chengdu, Sichuan Province, 610041, People’s Republic of China, Tel +86 18782934368, Email [email protected]
Abstract: Although the frequency of bone metastases from breast cancer has increased, effective treatment is lacking, prompting the development of nanomedicine, which involves the use of nanotechnology for disease diagnosis and treatment. Nanocarrier drug delivery systems offer several advantages over traditional drug delivery methods, such as higher reliability and biological activity, improved penetration and retention, and precise targeting and delivery. Various nanoparticles that can selectively target tumor cells without causing harm to healthy cells or organs have been synthesized. Recent advances in nanotechnology have enabled the diagnosis and prevention of metastatic diseases as well as the ability to deliver complex molecular “cargo” particles to metastatic regions. Nanoparticles can modulate systemic biodistribution and enable the targeted accumulation of therapeutic agents. Several delivery strategies are used to treat bone metastases, including untargeted delivery, bone-targeted delivery, and cancer cell-targeted delivery. Combining targeted agents with nanoparticles enhances the selective delivery of payloads to breast cancer bone metastatic lesions, providing multiple delivery advantages for treatment. In this review, we describe recent advances in nanoparticle development for treating breast cancer bone metastases.
Keywords: breast cancer, bone metastasis, nanoparticle, drug delivery
Introduction
Breast cancer (BC) is the primary cause of cancer-associated morbidity, disability, and mortality in women globally. According to the World Health Organization, 2.3 million women worldwide were clinically diagnosed with BC in 2020, among which 685,000 women died from the disease.1 Metastasis to vital organs remains the leading cause of death in patients with BC.2 The evolution of solid tumor metastasis is a complex process involving cell invasion from the primary tumor, circulatory system infiltration and extravasation, and distant growth.3 As the tumor progresses, a locally supportive and receptive microenvironment known as the pre-metastatic niche prepares the tumor cells to colonize before these cells reach distant organs, thus facilitating tumor settlement and metastasis.4 Some cells that escape from the primary tumor successfully colonize distant organs, whereas most circulating tumor cells are recognized and eliminated by the immune system. Once circulating tumor cells colonize the bone microenvironment, they are referred to as disseminated tumor cells.5 Different BC subtypes have specific organ preferences for metastasis, with estrogen receptor-positive (ER+) BC showing a propensity for bone metastasis and triple-negative BC typically spreading aggressively to internal organs.6
Because of its rich vascular supply and the chemo-attractiveness provided by stromal cells, osteoblasts, and osteoclasts that produce large amounts of growth factors and prostaglandins, the bone microenvironment is suitable for tumor cell attachment and proliferation. After reaching the skeleton, disseminated tumor cells settle into a suitable environment or ecological niche.7,8 This may be partly because bone sinuses have a discontinuous endothelium that facilitates the passage of hematopoietic and other cells, as well as interactions between the tumor and vascular system, leading to a metastatic preference for bone tissue. Various factors increase the likelihood that breast cancer cells will metastasize to the skeleton.9 Relatively slow blood flow through the bone marrow and the presence of adhesion receptors on endothelial cells in the bone marrow capillaries support the localization of cancer cells in the bone. These features, together with a bone marrow environment rich in growth factors and cytokines, promote the progression of bone metastasis.10 (Figure 1) Bone metastases affect 80% of patients with advanced BC, causing several bone-related complications such as nerve compression, pathologic fracture, and hypocalcemia.11 Bone metastases markedly reduce overall survival and lead to poor quality of life for patients because of pain, fatigue, and skeletal-related events (SREs).12 SREs resulting from bone metastases are associated with painful complications that adversely impact mobility, the ability to perform daily tasks, quality of life, and the psychological well-being of afflicted patients, thus greatly increasing the burden of BC bone metastasis (BCBM).13
 |
Figure 1 Bone metastases from breast cancer. |
Bone metastasis is caused by a feed-forward loop of cancer cells, osteoblasts, and osteoclasts, which promotes tumor development and osteoclast activity.14 Osteoblasts, as the most abundant cells in the skeletal tissues, regulate initial cancer-induced osteogenesis and subsequent osteoclast formation through growth factors, such as receptor activator of nuclear factor-κβ ligand (RANKL), osteoprotegerin, and sclerostin.15 Although the hard bone matrix restricts the growth of tumor cells, bone contains nutrients and growth factors that support tumor development via the osteolytic–metastatic cycle. Simultaneously, the increased osteoclast activity leads to the release of nutrients and growth factors in the bone matrix, facilitating the viability and proliferation of tumor cells.16
The predominant form of BCBM primarily involves osteolytic metastases characterized by increased osteoclast-mediated bone resorption at the tumor–bone interface, leading to abnormal bone breakdown. Currently, two main strategies are used to treat bone metastases: inhibition of cancer cell growth and inhibition of osteoclast activity. Although several recently approved drugs can relieve bone-related complications, the fatality rate remains significantly high because of drug resistance.17 Proper integration of systemic and bone-targeted drugs, as well as precision medicine, is necessary to accurately identify high-response patients and effectively treat BCBM. Through recent advances in nanotechnology, nanomedicines have emerged as a potential treatment strategy for BCBM. In this review, we discuss the challenges of BCBM treatment and recent advances in drug-carrying nanoparticles (NPs), which may help improve the prognosis of patients with BCBM.
Biological Processes of Bone Metastasis
Bone metastasis results from interactions of metastatic cancer cells with bone microenvironments, a phenomenon that is in line with Paget’s “seed and soil” hybrid hypothesis proposed in 1889.18 The development of BCBM is a complex process involving interactions among bone macrophages that phagocytose cancer cells and osteoblasts that disrupt the normal process of bone remodeling.19 The bone tissue matrix is densely calcified; however, its internal cavities are comprised of well-vascularized bone marrow. Diffused metastatic cancer cells first localize near the bone endosteal surface and interact with various types of bone marrow cells to form micrometastatic colonies known as metastatic ecotopes.20
The osteo-microenvironment is a unique and dynamic space containing osteoblasts, osteoclasts and their precursors, hematopoietic and immunological proteins, stromal cells, adipocytes, fibroblasts, endothelial cells, and the extracellular matrix that contains many growth and/or signaling factors. Slow blood flow, mechanical properties, chemokines, and growth factors promote tumor cell development in bones.21 Furthermore, the bone marrow contains abundant sinusoidal blood vessels that facilitate the migration of tumor cells into circulation. Tumor cells migrate to the bone wall niche, where they colonize and form dormant cancer cells that can be reactivated when inhibitory signals are removed. The primary tumor produces cytokines that create a pre-metastatic niche in the bones.22
BC inhibits the secretion of osteoprotegerin from osteoblasts and stromal cells through the production of parathyroid hormone-related protein. Additionally, BC stimulates RANKL expression in osteoblasts, causing excess osteolysis, and promotes bone metastasis via the RANK–RANKL signaling pathway. Elevated RANKL levels hyperactivate osteoclastogenesis and bone resorption, facilitating the invasion of metastatic clones into the bone. Both osteoblasts and osteoclasts produce several trophic elements and cell factors, including transforming growth factor-β, vascular endothelial growth factor, insulin-like growth factor, bone morphogenic proteins, and calcium. These factors promote the external growth of tumors, thereby triggering a malignant chain of events that facilitates skeletal damage and tumor advancement.23,24 In contrast, osteoprotegerin, secreted by osteoblasts, inhibits the RANK/RANKL signaling pathway and negatively regulates osteoclastogenesis.
Elevated Jagged1 expression in BCBM activates the Notch signaling pathway in osteoblasts, inducing the growth of Jagged1-expressing cancer cells by promoting interleukin-6 secretion or transforming growth factor-β secretion during bone destruction.25 Notably, the “vicious cycle” between tumor growth and osteolysis exacerbates the progression of BCBM, leading to life-threatening bone-related events that severely reduce patient survival and quality of life (Figure 2).
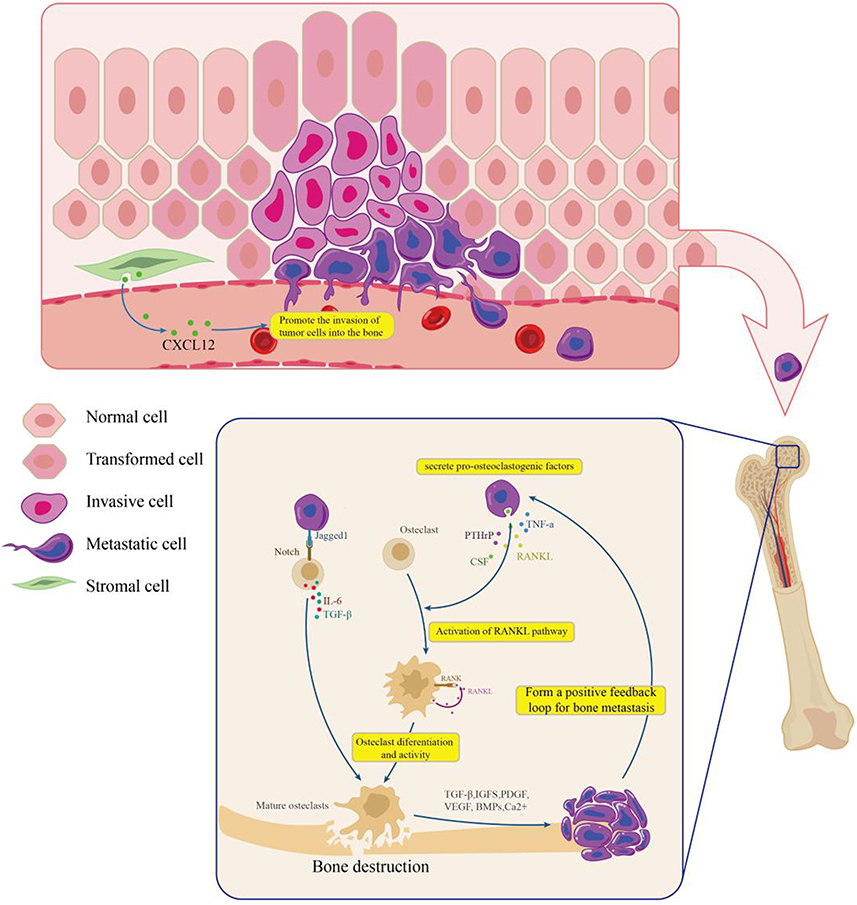 |
Figure 2 Vicious cycle in the bone microenvironment of breast cancer bone metastases. |
Cancer-related fibroblasts in the tumor stroma contribute to the proliferation of tumor cells in bones by producing C-X-C motif chemokine ligand 12 (CXCL12).26 CXCR4 and CXCR7 overexpression in BC cells induces CXCL12 gradient chemotaxis, which facilitates bone colonization.27 Moreover, high CXCR4 expression in BC is related to an increased occurrence of remote and bone metastases.28 The CXCL12–CXCR4 axis induces cancer cells to release osteoclastogenic factors, enhancing bone metastasis.29 Targeted therapies directed against this signaling axis may be clinically important for treating metastatic bone tumors.
Limitations to Therapeutic Drug Design for BCBM
Current treatments for BCBM focus on pain management, addressing or reducing the risk of SREs, and inhibiting tumor progression.30 The main treatment strategies involve surgery, external radiation therapy, biotherapy, chemotherapy, endocrine therapy, bio-targeted therapy, and immunotherapy.24 The goal of surgery is to improve the survival and quality of life of patients with smaller or solitary bone metastases by preventing pathologic fractures or by relieving localized pressure. However, its benefits are limited for patients with larger or multiple bone metastases.31
The structure of the bone sinus and slow local blood flow hinders local drug accumulation following systemic administration of chemotherapy drugs, limiting their therapeutic efficacy against bone metastases.32 This may be attributed to the unique histologic characteristics of bone, which serves as a blood–bone marrow barrier formed by lining cells that prevent the entry of large amounts of exogenous substances from the bone surface.33 Increasing the drug dosage to reach therapeutic levels in bone may result in intolerable toxicity in critically ill patients.34 Additionally, the density of the extracellular matrix associated with osteoblastic bone metastases reduces drug permeation and accumulation in metastatic sites, thereby decreasing drug uptake by cancer cells or alternative target cells.35 Chemotherapeutic agents produce Jagged1 in osteoblast cells via the reactive oxygen pathway, which promotes cancer cell dissemination to the bone and chemotherapy resistance,36 eventually leading to serious clinical problems such as myelosuppression and abnormal bone metabolism.37 Additionally, long-term utilization of antiresorptive medications causes severe complications, such as osteonecrosis of the jaws and renal failure.32
To effectively target bone/mineralized tissue, systemic drug delivery systems (DDSs) must cross the blood–bone marrow barrier, including the sinusoidal capillary fissures of the bone marrow, which are approximately 80–100 nm in diameter.38 Therefore, the development of alternative approaches for treating BCBM, particularly to overcome the challenges of drug delivery, is an important area of study. Nanomaterial-based DDSs have been increasingly recognized as a therapeutic option for various tumor types because of their ability to cross biological barriers to enhance drug delivery.39 Emerging therapeutic approaches involve the use of NPs for direct drug delivery to secondary bone–tumor sites to improve the treatment of bone metastases (Table 1).
 |
Table 1 Nanoparticle-Based Targeted Drug Delivery System for the Treatment of Breast Cancer Bone Metastasis |
NPs in Cancer Bone Metastasis Diagnosis
Early diagnosis of metastases is essential for effective treatment. Current standard imaging methods for detecting bone metastases include X-ray, bone scintigraphy, and computed tomography (CT), all of which assess the stromal response of cancer cells within the bone marrow rather than characterize the cancer lesion. This factor limits the detection of early metastases and assessment of the treatment response.30 NPs have been developed to target and image BCBM at the macro- and micro-scales.61 The use of contrast agents, such as NPs and magnetic NPs, overcomes inherent imaging limitations and enables targeted imaging.62 Available nanotools for early cancer detection and targeted therapy can be categorized as organic and inorganic particles. Organic nanotools include liposomes, polymeric micelles, dendrimers, and nanocantilevers.63 Imaging of bone metastases, in which inorganic NPs with heavy atoms were coated with metastatic-targeting entities, revealed different X-ray attenuation characteristics in damaged bone compared with those in normal bone.64 Prolonged blood circulation and enhanced interaction with tumors are keys to NP accumulation at tumors. NP contrast agents for magnetic resonance imaging offer advantages over conventional contrast agents, such as higher sensitivity and an extended blood circulation time.65 Radionuclide imaging has also been used to image radiolabeled NPs in metastatic breast cancer. Gamma scintillation scans were performed using Technetium-99m as a radionuclide marker for NPs.66
NPs in Cancer Bone Metastasis Therapy
Nanomedicine is a promising strategy for treating bone metastases. This approach is designed to improve the therapeutic index through passively-targeted, actively-targeted, and stimulated drug-releasing strategies to deliver drugs to tumor sites while reducing accumulation in non-targeted tissues.67 NPs are a fundamental component of nanotechnology. The successful delivery and therapeutic efficacy of nanomedicines are strongly affected by the size, shape, and surface properties of the NPs.68 These NPs can be fabricated from metals, metal oxides, carbon, polymers, lipids, proteins, nucleic acids, and other materials via bottom-up or top-down strategies.69 NPs have numerous advantages, such as small particle size, high stability, high solubility of insoluble drugs, and low drug toxicity. Nanocarriers 70–100 nm in size are commonly used for bone targeting. Nanomaterials modulate the cytoskeletal dynamics of cancer cells, and multi-walled carbon nanotubes that can attach to cell membranes alter stiffness and mobility, impacting the biomechanical characteristics of tumors.70 (Figure 3).
 |
Figure 3 Passive targeting of nanoparticles for anti-tumor effects. |
NPs concentrate at tumor locations through the enhanced vascular permeability and retention (EPR) effect. Nanocarriers penetrate cancer cells via endocytosis, constituting a form of passive drug targeting.71 Actively targeted NPs exploit the EPR effect to enter tumor tissue and bind to cancer cells by recognizing tumor biomarkers through specific ligands. Additionally, active targeting can enhance the EPR effect by facilitating the entry of NPs into the tumor mesenchyme, where particles already adhering to cancer cells reduce the concentration of free NPs in the mesenchymal space.72 (Figure 4) Surface molecular modifications of NPs can direct the NPs to their targets, thus enhancing drug accumulation at tumor sites. By incorporating reactive ligands, NPs can liberate therapeutic agents spatially and temporally in response to the local microenvironment or external stimuli.73 In addition, preclinical animal research on pH-responsive NPs loaded with chemotherapeutic drugs demonstrated increased drug activity in acidic tumor environments compared with that after pH-unresponsive NP or free drug administration.74
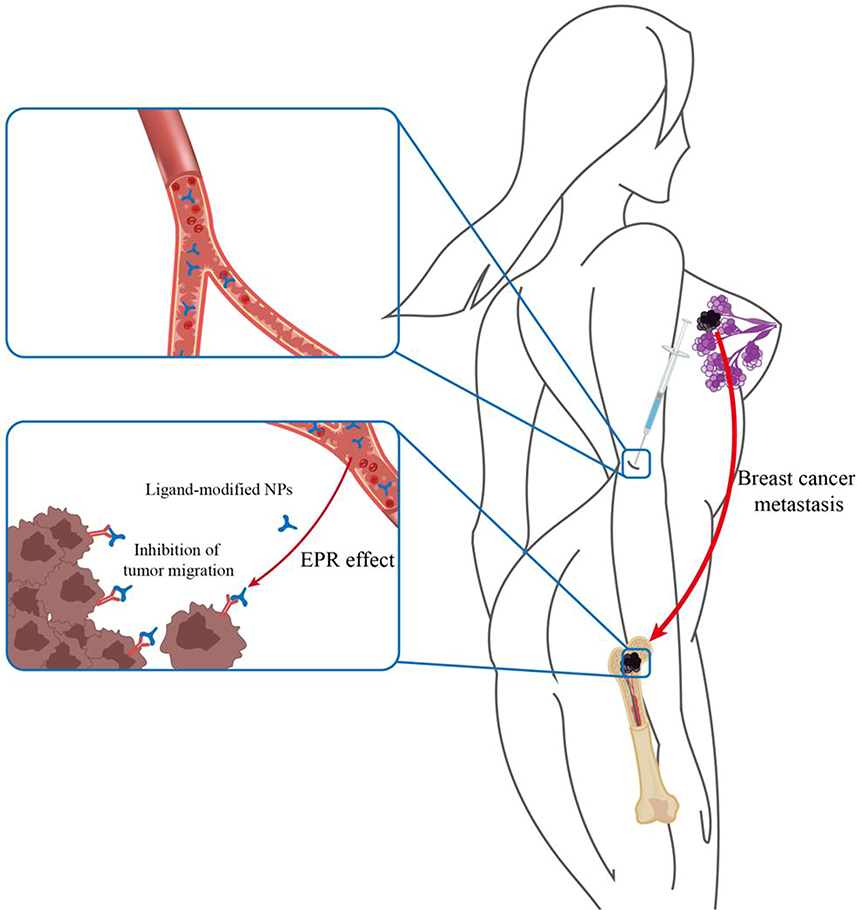 |
Figure 4 Active targeting of nanoparticles for anti-tumor effects. |
Surface-engineered NPs can improve drug targeting, facilitate drug crossing of the blood-bone marrow barrier, reduce clearance, and extend the circulation time.75 NPs smaller than 50 nm can easily enter most cells, whereas NPs smaller than 20 nm can circulate through blood vessels. Thus, NPs deliver drugs to cancer cells while healthy cells are unaffected.76 NPs are surrounded by several organic or inorganic coatings that determine the properties of NPs, thereby increasing the drug concentration within the tumor and decreasing systemic toxicity, drug biodistribution, circulation time, and targeting ability in healthy tissues.77,78 The size, shape, charge, and density of NPs must be controlled to avoid renal clearance and clearance by the mononuclear phagocyte and reticuloendothelial systems to maximize their circulation times.79,80 The functions of NPs can be enhanced through controlled synthesis, functionalization, or modification by polymers to enhance the carrier requirements and greatly extend their blood circulation time, which is a desirable property for NP storage into bone tissue.40
Because of the low permeability of the blood-bone marrow barrier, the size of NPs plays an important role in permeation.81 Various structural factors are incorporated into NP assemblies to manipulate the size, shape, charge, surface functionality, and stimulus responsiveness to improve drug stability during transport and enable selective drug delivery and effective tumor penetration to overcome blood-bone marrow barriers and ultimately enhance therapeutic efficacy.82 The transendothelial pathway is a metabolically active process that requires endothelial cells to re-arrange their structure to present vesicles that can absorb NPs and further deliver them to nearby tumor cells, as well as help NPs pass through the blood-bone marrow barrier.83 In the tumor setting, pro-inflammatory cytokines cause endothelial cells to lose their junctional integrity. The gaps between endothelial cells are enlarged, which allows NPs to extravasate from the vascular system into diseased tissue, thus overcoming the blood-bone marrow barrier.84
NP carriers have shown promising outcomes in patients with cancer and in various clinical trials. Notably, NPs are designed to efficiently deliver therapeutic agents to lesion sites and reduce multidrug resistance, demonstrating their potential for treating metastatic BC (Table 2).85 Targeted NPs can carry various active substances, including antitumor drugs, small interfering RNA (siRNA), proteins, and contrast agents for the diagnosis and treatment of bone metastases.86 Using NPs to treat metastases prolongs the circulation time and prevents the premature clearance or degradation of the active drug, thereby increasing drug accumulation at the metastatic site.87 Bisphosphonates (BPs) have a high affinity for hydroxyapatite and thus attach to NPs.24 In addition to their ability to target tumors and their prolonged circulation time in the body, NPs can improve the immunosuppressed tumor microenvironment and activate tumor-killing T-cells, thus improving the therapeutic effect of tumors while reducing the therapeutic dosage of medications and toxic adverse effects on normal organs.88,89 NPs currently available for drug delivery include polymer conjugates, lipid-based carriers such as liposomes and micelles, dendrimers, carbon nanotubes, and gold NPs.90 The advent of NP-based DDSs has ushered in a novel era for BCBM therapy involving targeted drug delivery.
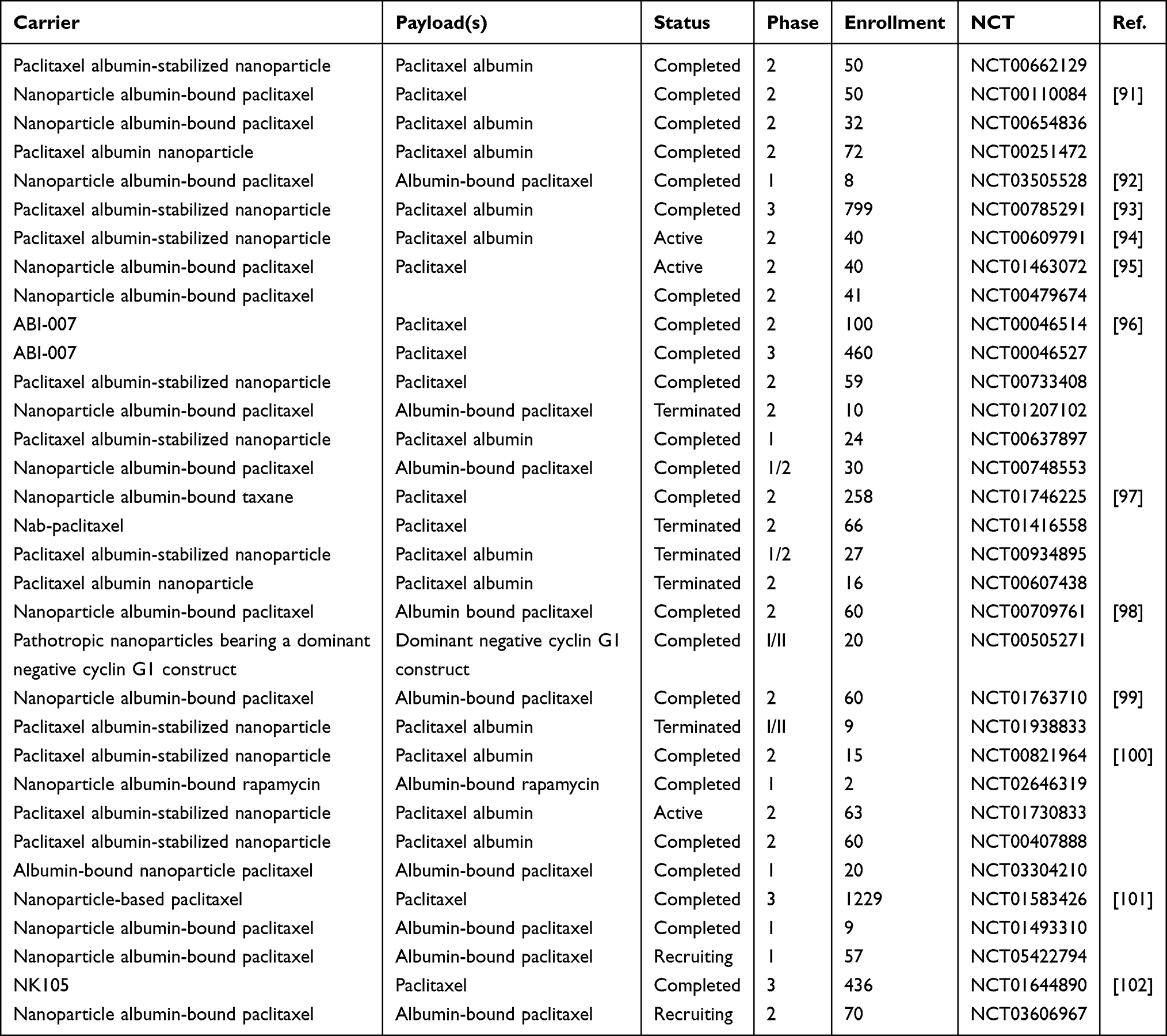 |
Table 2 Nanoparticles for Metastatic Breast Cancer |
NPs Enhance Drug Biodistribution in BCBM
Nanocarriers are widely employed for drug delivery because of their pharmacokinetic properties, which improve drug bioavailability in systemic circulation and enhance drug availability in tumors; nanocarriers show high tissue targeting ability, low adverse effects, and high stability.103 Recent studies of NP-based DDSs led to improvements in the EPR effect in bone metastasis. DDSs for bone metastasis therapy often target hydroxyapatite and ανβ3 integrin, a unique mineral present in bone. CD44 expression is important in the interactions between metastatic BC cells and myeloid epithelial cells, as it enhances cancer cell propagation, invasion, metastasis, and angiogenesis. Its expression also influences the effectiveness of chemotherapeutic agents.104
Polyethylene glycol (PEG)-coated NPs are widely employed to decrease complement activation, enhance plasma stability, and extend their circulation time, which are essential factors for effective tumor targeting.105 (Asp)8-PEG-PCL NPs, which show biocompatibility, cellular permeability, bone specificity, and effectiveness as carriers and hydrophobic drug release systems, exhibit enhanced bone affinity in vivo through (Asp)8 linkage to PEG-PCL NPs. These NPs show high potential for delivering hydrophobic anticancer agents to bone niches and treating patients with BCBM.106 Liposomal NPs accumulate in tumor cells through cell membrane-bound bilayers and surface modification with PEG can extend their half-life and enhance their targeting ability.107
Encapsulation of doxorubicin (DOX) into liposomes alters its tissue profile and pharmacokinetics, improving the therapeutic index compared with that of traditional adriamycin. By avoiding mononuclear phagocytes, DOX-loaded PEG liposomes experience a prolonged half-life and extended circulation time.108 A preclinical study demonstrated that DOX-PEG-alendronate (ALN) self-assembled micelles delayed tumor development, decreased bone loss, and limited cardiotoxicity in mice compared with free DOX. Myocet is a non-PEGylated liposome of DOX citrate used to treat metastatic BC. Myocet has a different pharmacokinetic profile from traditional DOX, with lower cardiotoxicity but similar antitumor activity. Wong and Chiu109 reported that co-encapsulation of vincristine and quercetin in PEG liposomes extended the circulation of drugs in the plasma and ensured controlled release of the drug in vivo. PEG liposomal DOX is DOX hydrochloride encapsulated in liposomes with methoxy PEG bound to their surfaces. PEG liposomal DOX has a mean half-life of 55 h in humans and has demonstrated substantial effectiveness in BCBM monotherapy and combination therapy, with a significantly increased circulation time. Additionally, flexible NPs carry drugs through the blood vessels and bone sinuses, and invisible NPs can circulate in the bloodstream to reach lesions while evading detection by the immune system.110
Precision-designed, targeted NPs can direct anticancer drugs to a specific site of action for precise treatment.111 Bone-targeted ligands, including BPs, tumor-targeted ligands such as CD44, and local drug delivery, have been widely employed in nanotechnology-based therapies for bone metastases.112 One strategy used to achieve this goal is modifying NPs to specifically target BCBM or its microenvironment. Several dosing strategies exist for treating bone metastases, including non-targeted drug delivery, bone-targeted drug delivery, and cancer cell-targeted drug delivery.53 Collectively, preclinical studies indicate the potential of nanomedicines for treating BCBM.
NPs in BC and Skeletal System Drug Therapy
NP Non-Targeting of BCBM
Non-target drug delivery relies on the EPR effect for NP enrichment at the tumor site. Tumor neovascularization, characterized by structural incompleteness and high permeability, enables NPs to penetrate the tumor mesenchyme. Incomplete lymphatic drainage at the tumor site limits the removal of NPs, leading to prolonged NP retention within the tumor.113 Adjei et al found that NPs ~150 nm in size localized in the bone marrow more easily than did larger NPs (~320 nm) and that NPs with a neutral surface charge showed higher bone marrow targeting efficiency than did NPs with a positive or negative surface charge. Notably, the size and surface potentials of NPs strongly affect their efficacy in bone metastasis. These two factors are critical for improving the efficacy of NPs.114 The EPR effect is based on the abnormal pathophysiological properties of the tumor microenvironment. Elevated interstitial fluid pressure in the tumor reduces the pressure difference between the vasculature and tumor interstitium, disrupting the diffusion dynamics of nanomedicine from the vasculature to the tumor, thus weakening the EPR effect.115 An increase in interstitial fluid pressure in the tumor center to match the capillary pressure induces outward convection, rendering the tumor impenetrable to NPs, causing NP extravasation and decreased lymphatic clearance. Given that the EPR effect is related to differences in the vascular gap size between cancerous and normal tissues, NP accumulation in tumors is strongly affected by the NP size.116
Improving exudation of NPs at the tumor site is crucial for prolonging their circulation time in the bloodstream. A widely employed strategy involves surface modification with PEG. PEG modification prolongs circulation, improves stability, enhances half-life, and reduces immune cell uptake of NPs, thereby reducing systemic phagocytosis.117 Specifically, PEGylation induces the formation of a hydrophilic barrier around NPs, which extends their circulatory half-life by several-fold via repulsive spatial forces and reduces clearance through the mononuclear phagocyte system.118 Neutrally charged poly(lactic-hydroxyglycolic acid (PLGA) NPs have a longer half-life in the blood and enhanced accumulation in the bone compared with similarly sized anionic and cationic PLGA NPs.119
Polymeric and liposomal NPs are currently employed to deliver anticancer drugs via passive targeting; PEGylated liposomes are effective carriers for drug delivery.120 PLGA-based NPs passively target tumors through the EPR effect and are transferred directly into the cytoplasm through the permeable cell membrane. To maximize efficacy through passive targeting, NPs must penetrate the tumor and release the drug. MM-DX-929 is a drug-free, non-targeted 100-nm PEG liposome with adequate stability in vitro and in vivo. Positron emission tomography assessment of the stratification of tumor deposition using a single pre-treatment with MM-DX-929 indicated that tumors with high MM-DX-929 deposition had significantly higher antitumor activity after multiple treatment cycles with different liposomal drugs.121 Non-targeted drug delivery may be more effective than active targeting because the expression of cell surface receptors may be persistently decreased by ligand-mediated NP–cell interactions. Non-targeted drug delivery has promising benefits, such as ease of design, strong antitumor effects, and a high potential for clinical translation, making this system a promising approach for treating BCBM.
NP Direct Targeting to Bone
Currently available bone-targeted therapies are designed to inhibit bone resorption, minimize complications, and prolong survival.122 BPs induce apoptosis in osteoclasts, which are responsible for bone erosion. BPs indirectly induce cancer cell apoptosis by inhibiting adenine nucleotide transposase through the accumulation of intracellular isopentenyl pyrophosphate. NPs utilize BPs to target the bone, release anticancer drugs, and inhibit cancer cells. The loaded drug can be secreted through chemical coupling of the nanocarrier or by physical encapsulation or adsorption through diffusion, carrier erosion, or chemical bond breakage.123 Zoledronic acid (ZOL) is a representative third-generation BP that can be rapidly distributed into the bone, particularly in bone lesions with two phosphate groups, and can be absorbed by osteoclasts to slow bone resorption by inhibiting osteoclast activity.124 Combining ZOL with other agents and delivering both drugs simultaneously to the site of bone metastasis inhibits cancer cells and osteoclasts and greatly reduces the necessary doses of less selective chemotherapeutic agents, thereby reducing dose-related adverse effects.125 Several studies have been performed to investigate the delivery of anticancer drugs to the bone via BP-functionalized polymer-carriers. PLGA NPs loaded with ZOL and anchored with DOX showed favorable bone-targeting characteristics. ZOL-labeled NPs increased the bone preservation-capacity and disrupted cancerous tumors.126
ALN is a common BP used to inhibit bone resorption, with a 10–20-fold higher binding affinity to cancer-infiltrated bones than to healthy bone tissues, resulting in effective NP delivery to the bone, prolonged retention, and controlled release of the encapsulated chemotherapeutic agent.127 Otaka et al46 developed a bone-targeting drug by adding an ALN unit to an amphiphilic polymer (2-methacryloyloxyethylphosphorylcholine-co-butyl methacrylate) loaded with DOX. Additionally, ALN-coupled PEG-modified calcium phosphate NPs used in bone metastasis therapy have shown good biocompatibility, biodegradability, and bone-targeting ability.128
Dual-targeted chemotherapy for bone/tumor metastasis can be achieved by immobilizing folic acid on allyl-phosphonic acid-modified paclitaxel (PTX)-loaded PLGA NPs. Another approach involves the encapsulation of agents in PLGA NPs functionalized with ALN acid on the NP surface to promote active targeting of the bone microenvironment, which inhibits the development of metastatic skeletal lesions by regulating osteoclasts. Salerno et al129 revealed that DOX-loaded PLGA and ALN NPs targeted the bone microenvironment and reduced the number of osteoclasts, thereby decreasing bone resorption in an in situ mouse model of BC translocation to the bone. Chaudhari et al125 found that PLGA-PEG-ZOL NPs enhanced targeting via their strong affinity for infected bone, the EPR effect, their prolonged circulating half-life, and enhanced endocytosis. Moreover, ZOL-anchored PLGA NPs can be used to treat bone metastases. Overall, in vitro and in vivo studies demonstrated that PLGA NPs have good biodistribution and can inhibit primary tumors and bone metastasis, and alleviate bone erosion to some extent.
Wu et al41 coupled DOX-liposomes with ALN and low-molecular weight heparin to achieve bone targeting and prolong the liposome circulation time, respectively. Morton et al130 developed a tailorable layer-by-layer nano-system that achieved precise DOX-targeted delivery to bone tissue. They used a layer-by-layer assembly of polyanionic poly(acrylic acid) and poly(cationic) poly(L-lysine) to encapsulate solid NPs, with the outer poly(acrylic acid)layer fitted using ALN as the bone-targeting molecule.
Recently, bone-targeted mesoporous silica NPs (MSNs) have been widely used in DDSs because of their large specific surface area, biocompatibility, and easy surface functionalization. For example, a ZOL-conjugated MSN nano-delivery system with internally enclosed gold nanorods (Au@MSNs) was constructed to deliver gold, which is toxic to cancer cells to bones.131 Compared with normal silica NPs, ZOL-anchored MSNs exhibited a four-fold increase in their binding capacity to bone. Additionally, ZOL-encapsulated MSNs significantly interacted with cancer cells, leading to increased cell death.132 Qiao et al133 found that ZOL anchored to mesoporous silica-coated upconverting NPs can target osteoblasts to attenuate bone metastasis in early BC and that ZOL preferentially localizes to sites of high osteoclast activity and targets sites of bone metastasis.
Similarly, self-assembled pH-sensitive micelles functionalized with PEG and anchored to ALN showed increased accumulation in bones, with the NPs undergoing degradation and subsequently releasing their therapeutic load in the acidic tumor microenvironment for the treatment of BCBM.134 Clementi et al135 designed, characterized, and coupled a non-toxic PTX and ALN using PEG-(β-Glu)-dendrimer macromolecules, which ensured strong bone targeting through high hydroxyapatite binding. DOX-loaded PLGA-PEG-ALN showed higher efficacy in inhibiting BCBM than did free drugs or unloaded NPs. Huang et al55 reported that functionalized coordination polymer NPs (DZ@ALN) co-delivered a cisplatin prodrug (DSP) and the antiresorptive drug, ZOL, for combination therapy. The multifunctional DZ@ALN, with a diameter of approximately 40 nm, can cross the fissures of bone marrow sinus capillaries and has shown excellent bone-seeking ability both in vitro and in vivo. DZ@ALN significantly inhibits tumor cell proliferation, relieves bone pain, and significantly suppresses osteoclast activation without causing significant systemic toxicity. The particle size of DSP-Zn@PEG-ALN NPs can be controlled by adjusting the volume ratio of the aqueous phase to the oil phase in the microemulsion. A particle size of approximately 55 nm allows exudation through the slits of the bone sinus capillaries (80 nm) and localization in transferred bone. In vivo biodistribution studies demonstrated that intravenously injected DSP-Zn@PEG-ALN NPs delivered approximately four-fold more platinum into bone metastases.40 Pang et al45 used surface-modified immune-stimulating cytosine-phosphate-guanosine-loaded metal-organic framework (MOF) NPs with the FDA-approved antiresorptive BP ZOL to enhance bone-targeting. These functionalized bone-targeted immunostimulatory MOF NPs bind tightly to calcium phosphates ex vivo and accumulate in bone tissue in vivo. Moreover, researchers developed PLA NPs loaded with DOX and encapsulating bone-targeting pamidronate for targeting malignant bone tumors. The biodistribution of radiolabeled pamidronate-NPs showed stronger bone–tumor accumulating capacity and longer retention time in vivo than those of non-targeting NPs.
Polyphosphates (polyP) are also utilized in bone-targeting systems. ZOL-anchored Ca-polyP nanomaterials/microparticles can maintain the morphogenetic and mineralization induction activities of polyP and the anti-osteolytic properties of BP.136 Mann et al137 proposed E-selectin-targeted porous silicon-based NPs for targeting bone marrow endothelial cells, demonstrating an eight-fold increase in their bone marrow targeting ability compared to non-targeted drugs in a mouse mammary metastasis model. The strategy for localizing these NPs in the bone marrow utilizes the unique properties of bone marrow capillary endothelial cells that express E-selectin and vascular cell adhesion molecule-1, which facilitate cell homing.138 Zhao et al139 reported that bone-targeted NPs DOX@ALN-(HA-PASP)CL inhibited bone resorption and tumor cell propagation by specifically releasing ALN and DOX at the site of bone metastases. Researchers developed a multifunctional and multi-responsive superparamagnetic iron oxide NP system that specifically targets bone metastasis sites to release furin inhibitory peptides via MMP2/9-triggered cleavage to exert anticancer and anti-osteoclastic effects.58 Xiang et al140 also developed indocyanine green-enhanced PTX prodrug NPs for advanced near-infrared imaging and chemotherapy. The hydrophilicity of indocyanine green confers enhanced assembly and colloidal stability to PTX prodrugs, as well as tumor bio-imaging and precision therapeutic capabilities, demonstrating preferential tumor accumulation and comparable anticancer efficacy while mitigating the systemic toxicity of chemotherapy.
Bone tissue-targeted therapy has overcome the inefficiencies of nanomedicine penetration and bone tissue accumulation, offering promising prospects for drug delivery in BCBM. Extensive research is necessary to improve the delivery and efficacy of nanomedicines for bone metastasis treatment. Studies of bone-targeted NPs are currently in the preclinical trial stage. Moreover, the metabolism of nanodrugs and their effects on healthy bone remains unclear, limiting the clinical translation of bone-targeted NPs. Hence, studies are needed to investigate the metabolism and safety of bone-targeted NPs in bone tissue.
Tumor Cell-Targeted Drug Delivery
Tumor-targeting ability is an essential feature of nanocarrier DDSs to improve the effectiveness of chemotherapeutic agents and protect normal cells from cytotoxicity.141 NPs modified with tumor-specific ligands partially facilitate drug delivery into the tumor, leading to higher local drug concentrations at the malignant tumor sites and lower off-target effects.142 NPs with high affinity selectively bind to targeted molecules, such as sugars, proteins, folic acid, transferrin, haptamers, or lipids, expressed on the cancer cell surface, thereby minimizing damage to non-cancerous cells.143 The advantages of NPs include an improved drug therapeutic index, reversal of the multidrug resistance phenotype in tumor cells, bypassing of drug efflux, and selective targeting of tumor cells in addition to the potential to mediate slow drug release.144 Optimization of the PEG structure can further enhance the tumor targeting and cancer cell internalization abilities of NPs.145 Surface modification of P-NP-DDS is achieved by coupling ligand-like moieties to ensure efficient tumor targeting.146 Chitosan-based nanocarriers exhibit strong tumor-targeting ability, primarily through pH-responsive drug delivery, utilizing the lower pH in the tumor region compared with physiological pH. Aminoplasmic protonation under acidic conditions leads to a prolonged circulation time and increased cellular penetration, facilitating the uptake of chitosan NPs by tumor cells.147
CD44 expression is higher in various tumor cells than in normal tissues and is associated with the tumorigenicity, invasiveness, and lymphatic metastasis of tumor cells.148 NPs targeting CD44 can precisely deliver antibodies to the tumor site, where they exert a therapeutic effect.149 Furthermore, the CD44 receptor selectively binds to the extracellular matrix, particularly hyaluronic acid, and hyaluronic acid modification enhances nanocarrier internalization in tumor cells. The CD44 receptor is highly expressed in BC cells that have migrated to the bone tissue.150 Niu et al151 constructed biomineralized MOF NPs carrying protein toxins with both bone-seeking and CD44 receptor-targeting abilities. Notably, the MOF NPs not only enhanced the attenuating effect of protein toxins in bone metastatic tumor cells but also synergistically intervened in crosstalk between osteoblasts and tumor cells to reduce SREs, such as bone loss. Lu et al152 showed that co-delivery of cyclobenzaprine and adriamycin using albumin NPs targeted primary BC and metastatic lymph nodes and inhibited tumor metastasis in vivo. Shen et al59 developed a bone and tumor dual-targeting nanocarrier using an NF-κB inhibitor in zeolitic imidazolate backbone-8. These dual-targeted NPs aggregate in the bone under the guidance of bone-targeted ligands, and the modified cellular ligands contribute to NP absorption in cancer cells.
Integrin αVβ3 is not expressed or is expressed at low levels in normal tissues and mature vascular endothelial cells. In contrast, this protein is highly expressed on the surface of tumor cells and neovascular endothelial cells and participates in tumor angiogenesis, invasion, and metastasis. Overexpression of integrin β3 subunits by bone metastatic BC cells is an important target for targeted drug delivery in BCBM.153 Ross et al154 developed a carrier system capable of targeting integrin β3 to deliver DOX; the system specifically localizes to mammary carcinoma bone metastases, enhancing the delivery of chemotherapy to BC cells. In addition to facilitating drug delivery to tumor tissues, the NP structure can modulate the function of tumor-associated macrophages, thereby improving the therapeutic efficacy toward BC.155 Zheng et al156 constructed a biomimetic nanoplatform (EMM@DJHAD) using engineered macrophage membranes and drug-carrying NPs, which exerted a strong tumor-suppressive and analgesic effect by inhibiting μ-opioid receptors in a mouse model of bone metastasis. This biocompatible biomimetic nanoplatform can be used to treat BCBM. Thus, using receptors highly expressed by cancer cells, NPs can be finely modified for the specific tumor targeting of bone metastases.
Therapeutic NPs Against ER-Positive BCBM
Temporary and reversible phenotypic shifts in ER+ BC cells in bone microenvironments have the potential to shift the diffusion of ER+ BC cells from bone colonization to invasive secondary metastases.157 In an estradiol-dependent ER+ BCBM mouse model, Erα increased the production of the tumor osteolytic factor parathyroid hormone-related protein, the number of osteoclasts at the bone–tumor interface, and osteolytic bone damage in an estradiol-dependent manner, which explains the propensity of ER+ tumors to develop osteolytic pathologies.158 Considering the risk of bone metastasis in ER-overexpressing BC, augmenting ER-targeted therapy may provide new treatment avenues for this BC subtype and improve survival.
Li et al159 developed a bio-compatible micellar nanomedicine, PPFA-cRGD, for targeted co-administration of drugs to tumors to enhance treatment efficacy, abrogate drug tolerance, and reduce side effects. Modifying peptides targeting the NP surface facilitated site-specific drug release, ensuring tissue-specific toxicity to the tumor tissue without affecting healthy tissues. This nanomedicine eliminated tumor cells in an in vitro organoid model and in vivo ER-positive BC model.159 Chittasupho et al160 demonstrated that encapsulating DOX using a LFC131 peptide-modified polyamidoamine dendrimer led to the targeting and inhibition of CXCR4 on the surface of ER+ BC cells. Paoletti et al161 proposed an innovative nano-delivery system based on hyaluronic acid involving a biologically active endogenous anionic polysaccharide functionalized with estradiol to produce an amphiphilic derivative, which can form soft NPs or nanohydrogels in water. The researchers investigated the adsorption of hydrophobic molecules by these estradiol-nanohydrogels through curcumin and docetaxel loading, and both inhibited the growth of ER+ BC. Zhang et al162 constructed pRNA-HER2apt-siMED1 NPs that selectively targeted HER2-overexpressing ER+ BC cells in vitro and in vivo. The NPs inhibited MED1 development and attenuated ER functions, thereby suppressing cancer cell propagation and tumor development. Tang et al163 developed estrogen-functionalized PEG liposomes encapsulating epirubicin and PTX to improve the antitumor effectiveness of the drugs against BC cells and reduce undesirable off-target effects.
Echogenic NPs are liposomes that are conjugated to naturally derived estrone bioligands to avoid antagonism, prolong the circulation of carriers containing chemotherapeutic agents, and precisely target ER+ BC cells. Xiong et al164 proposed a pharmaceutical-organic-inorganic self-assembling nano-system that combines DOX as a therapeutic agent for ER+ BC treatment, ferric chloride to induce apoptosis, and tannic acid to activate an intracellular cascade of superoxide dismutase-like reactions. NPs have the potential to greatly alter the treatment outlook for ER+ BC by expanding treatment options.
NPs for Gene Therapy Against BCBM
Gene therapy is an emerging area of BCBM treatment with the goal of treating the disease by regulating apoptosis and cell function at the genetic level.165 siRNA is a promising tool for gene silencing because it can specifically inhibit cancer-related genes and help maintain homeostasis between osteoclasts and osteoblasts. Recently, there has been growing interest in using siRNA to target unique genes in cancer cells. However, delivering specific siRNAs to cancer cells in vivo is challenging for several reasons, such as their poor circulatory time and rapid degradation.166 NPs can carry various genes to target cells and protect genes from nuclease damage and degradation.167 NPs are widely used to treat bone metastases and accelerate bone formation during osteogenesis and can serve as vectors for gene targeting and bone loss inhibition when combined with siRNA.
Combining gene expression profile analysis with preclinical BCBM mouse modeling may improve the understanding of the different phases of metastatic progression. Several studies have revealed the molecular complexities of BCBM, demonstrating that tumor metastasis to the bone is not determined by a single gene or pathway.168 Given that siRNA is readily degraded by serum nuclease and cleared by the kidneys, NPs 1–100 nm in size have been designed for siRNA binding and delivery.169 NPs can function as siRNA carriers, enabling increased cellular uptake and integration into components with specific functions.170 Endosomal pH-responsive NPs, designed to carry Rac1 siRNA and cisplatin, delivered Rac1-targeted oligonucleotides and cisplatin to breast tumors and showed promising synergistic antitumor effects.171 Hammond et al172 proposed a multilayered NP for systemic co-delivery of siRNA and adriamycin for metastatic BC therapy. siRNA-loaded NPs exhibit enhanced cellular uptake and targeted gene knockdown. Wang et al173 reported that treatment with siRNA-loaded lipid NPs increased siRNA uptake by MDA-MB-468 triple-negative BC cells in vitro, resulting in the suppression of target genes and inhibition of tumor development, invasion, and propagation in mice. Compared with traditional therapies that target cancer-related genes, gene therapy can potentially treat unresponsive cancer targets, address the problem of low bioavailability, evade immune system recognition, and deliver gene regulators.174 Liposomal NPs are efficient carriers for delivering oligonucleotides, peptides, and siRNA-based BC gene therapeutics. In hormonally manipulated mice, target genes were suppressed, which inhibited tumor growth, invasion, and migration. Xu et al175 developed an acid-sensitive bonded PEG-PLGA copolymer to encapsulate siRNA. Notably, PEG was degraded in an acidic tumor microenvironment, leading to the release of the siRNA into tumor cells. Overall, NPs can serve as delivery systems for gene modification, providing a new therapeutic approach for targeting BCBM.
Conclusion
In the last few years, many advances have been made in the field of nanotechnology, particularly in medical applications. Nanotechnology has gained widespread attention as a developing technology, showing promise in various disciplines that affect daily life. Rapid advances in nanotechnology have provided avenues for developing new anticancer strategies. Nanotechnology-based treatments can potentially overcome the limitations of surgery, radiotherapy, and chemotherapy for treating BCBM. NP-based drug delivery improves the effectiveness of cancer therapy while reducing toxicity to normal cells. More importantly, NPs can be designed to deliver multiple drugs for combination therapy, which is a trend in tumor therapy. Numerous targeted NPs have been developed for the diagnosis and treatment of bone metastases. NPs may revolutionize BCBM therapy by efficiently transporting drugs or genes by increasing the circulation time, improving the bioavailability, decreasing immune detection, and improving the delivery accuracy of chemotherapeutic agents.
However, most nanomedicines are still in the in vitro research stage and facilities for large-scale production are currently unavailable. Tumor heterogeneity in terms of the EPR effect and increased circulation time are key features that must be considered; however, these factors do not guarantee that the nanomedicine will enter the tumor site. Relying on the EPR effect alone is insufficient, particularly for poorly perfused tumors. Additionally, NPs suffer from poor penetration within the tumor and rapid clearance by the reticuloendothelial system. Therefore, further research is necessary to develop NP-based carriers capable of stimulating drug release into the tumor microenvironment. Nano-therapies are thought to be selective and effective for systematically delivering therapeutic drugs to metastatic cancer cells in the body.
Further studies in nanotechnology will improve the understanding of BCBM pathogenesis and lead to the development of effective nanomedicines for BCBM treatment. Designing multifunctional NPs for BCBM is a major trend. Although multiple functionalities may improve the therapeutic efficacy of BCBM, there are some limitations, such as poor reproducibility and complex preparation processes. Researchers should focus on developing simple but multifunctional NPs, which may have better clinical translational potential.
Acknowledgments
We sincerely appreciate Huifang Li from the Core Facility of West China Hospital for her assistance and suggestions. This work was supported by the National Natural Science Foundation of China (No. 82202989); China Postdoctoral Science Foundation (No. 2022M722279, China); Sichuan Science and Technology Program (No. 2023YFS0163, China); Postdoctoral Research Project of West China Hospital, Sichuan University, Chengdu, China (No. 2021HXBH045); Sichuan Province Science and Technology Activities Funding for Returned Overseas Scholars (awarded to Lingling Zhu); Fundamental Research Funds for the Central Universities (awarded to Lingling Zhu); and Sichuan University Postdoctoral Interdisciplinary Innovation Fund (2022SCU12063, awarded to Lingling Zhu).
Disclosure
The authors report no conflicts of interest to declare for this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Ibragimova MK, Tsyganov MM, Kravtsova EA, Tsydenova IA, Litviakov NV. Organ-specificity of breast cancer metastasis. Int J Mol Sci. 2023;24(21):15625. doi:10.3390/ijms242115625
3. Williams ED, Gao D, Redfern A, Thompson EW. Controversies around epithelial-mesenchymal plasticity in cancer metastasis. Nat Rev Cancer. 2019;19(12):716–732. doi:10.1038/s41568-019-0213-x
4. Liu Y, Cao X. Characteristics and significance of the pre-metastatic niche. Cancer Cell. 2016;30(5):668–681. doi:10.1016/j.ccell.2016.09.011
5. Allocca G, Hughes R, Wang N, et al. The bone metastasis niche in breast cancer: potential overlap with the haematopoietic stem cell niche in vivo. J Bone Oncol. 2019;17:100244. doi:10.1016/j.jbo.2019.100244
6. Satcher RL, Zhang XH. Evolving cancer-niche interactions and therapeutic targets during bone metastasis. Nat Rev Cancer. 2022;22(2):85–101. doi:10.1038/s41568-021-00406-5
7. Wu X, Li F, Dang L, Liang C, Lu A, Zhang G. RANKL/RANK system-based mechanism for breast cancer bone metastasis and related therapeutic strategies. Front Cell Dev Biol. 2020;8:76. doi:10.3389/fcell.2020.00076
8. Zhang W, Bado I, Wang H, Lo H-C, Zhang XH-F. Bone metastasis: find your niche and fit in. Trends Cancer. 2019;5(2):95–110. doi:10.1016/j.trecan.2018.12.004
9. Esposito M, Guise T, Kang Y. The biology of bone metastasis. Cold Spring Harbor Perspectives Med. 2018;8(6):a031252. doi:10.1101/cshperspect.a031252
10. Vijayaraghavalu S, Gao Y, Rahman MT, et al. Synergistic combination treatment to break cross talk between cancer cells and bone cells to inhibit progression of bone metastasis. Biomaterials. 2020;227:119558. doi:10.1016/j.biomaterials.2019.119558
11. Yuan X, Qian N, Ling S, et al. Breast cancer exosomes contribute to pre-metastatic niche formation and promote bone metastasis of tumor cells. Theranostics. 2021;11(3):1429–1445. doi:10.7150/thno.45351
12. Qin A, Zhao S, Miah A, et al. Bone metastases, skeletal-related events, and survival in patients with metastatic non-small cell lung cancer treated with immune checkpoint inhibitors. J Natl Compr Canc Netw. 2021;19(8):915–921. doi:10.6004/jnccn.2020.7668
13. Ihle CL, Wright-Hobart SJ, Owens P. Therapeutics targeting the metastatic breast cancer bone microenvironment. Pharmacol Ther. 2022;239:108280. doi:10.1016/j.pharmthera.2022.108280
14. Zhang L, Qu J, Qi Y, et al. EZH2 engages TGFβ signaling to promote breast cancer bone metastasis via integrin β1-FAK activation. Nat Commun. 2022;13(1):2543. doi:10.1038/s41467-022-30105-0
15. Mahmoud NS, Mohamed MR, Ali MAM, Aglan HA, Amr KS, Ahmed HH. Osteoblast-based therapy-a new approach for bone repair in osteoporosis: pre-clinical setting. Tissue Eng Regen Med. 2020;17(3):363–373. doi:10.1007/s13770-020-00249-5
16. Li X, Liang Y, Lian C, et al. CST6 protein and peptides inhibit breast cancer bone metastasis by suppressing CTSB activity and osteoclastogenesis. Theranostics. 2021;11(20):9821–9832. doi:10.7150/thno.62187
17. Loibl S, Poortmans P, Morrow M, Denkert C, Curigliano G. Breast cancer. Lancet. 2021;397(10286):1750–1769. doi:10.1016/S0140-6736(20)32381-3
18. Akhtar M, Haider A, Rashid S, Al-Nabet A. Paget’s ”seed and soil” theory of cancer metastasis: an idea whose time has come. Adv Anatomic Pathol. 2019;26(1):69–74. doi:10.1097/PAP.0000000000000219
19. Zhang Z, Yao Y, Yuan Q, et al. Gold clusters prevent breast cancer bone metastasis by suppressing tumor-induced osteoclastogenesis. Theranostics. 2020;10(9):4042–4055. doi:10.7150/thno.42218
20. Song MK, Park SI, Cho SW. Circulating biomarkers for diagnosis and therapeutic monitoring in bone metastasis. J Bone Miner Metab. 2023;41(3):337–344. doi:10.1007/s00774-022-01396-6
21. Zhu J, Huo Q, Xu M, et al. Bortezomib-catechol conjugated prodrug micelles: combining bone targeting and aryl boronate-based pH-responsive drug release for cancer bone-metastasis therapy. Nanoscale. 2018;10(38):18387–18397. doi:10.1039/C8NR03899F
22. Kan C, Vargas G, Pape FL, Clézardin P. Cancer cell colonisation in the bone microenvironment. Int J Mol Sci. 2016;17(10):1674. doi:10.3390/ijms17101674
23. Jacome-Galarza CE, Percin GI, Muller JT, et al. Developmental origin, functional maintenance and genetic rescue of osteoclasts. Nature. 2019;568(7753):541–545. doi:10.1038/s41586-019-1105-7
24. Clézardin P, Coleman R, Puppo M, et al. Bone metastasis: mechanisms, therapies, and biomarkers. Physiol Rev. 2021;101(3):797–855. doi:10.1152/physrev.00012.2019
25. Wu C, Chen M, Sun Z, et al. Wenshen Zhuanggu formula mitigates breast cancer bone metastasis through the signaling crosstalk among the Jagged1/Notch, TGF-β and IL-6 signaling pathways. J Ethnopharmacol. 2019;232:145–154. doi:10.1016/j.jep.2018.12.023
26. Yu PF, Huang Y, Xu CL, et al. Downregulation of CXCL12 in mesenchymal stromal cells by TGFβ promotes breast cancer metastasis. Oncogene. 2017;36(6):840–849. doi:10.1038/onc.2016.252
27. Łabędź W, Przybyla A, Zimna A, Dąbrowski M, Kubaszewski Ł. The role of cytokines in the metastasis of solid tumors to the spine: systematic review. Int J Mol Sci. 2023;24(4):3785. doi:10.3390/ijms24043785
28. Akonnor A, Makise M, Kuniyasu A. CXCR4-targeted necrosis-inducing peptidomimetic for treating breast cancer. ACS Omega. 2023;8(27):24467–24476. doi:10.1021/acsomega.3c02415
29. Duan L, Lu Y, Xie W, et al. Leptin promotes bone metastasis of breast cancer by activating the SDF-1/CXCR4 axis. Aging (Albany NY). 2020;12(16):16172–16182. doi:10.18632/aging.103599
30. Coleman RE, Croucher PI, Padhani AR, et al. Bone metastases. Nat Rev Dis Primers. 2020;6(1):83. doi:10.1038/s41572-020-00216-3
31. Ban J, Fock V, Aryee DNT, Kovar H. Mechanisms, diagnosis and treatment of bone metastases. Cells. 2021;10(11):2944. doi:10.3390/cells10112944
32. Jiang B, Cao J, Zhao J, et al. Dual-targeting delivery system for bone cancer: synthesis and preliminary biological evaluation. Drug Deliv. 2012;19(7):317–326. doi:10.3109/10717544.2012.714809
33. Katsumi H, Yamashita S, Morishita M, Yamamoto A. Bone-targeted drug delivery systems and strategies for treatment of bone metastasis. Chem Pharm Bull. 2020;68(7):560–566. doi:10.1248/cpb.c20-00017
34. Harris V, Lloyd K, Forsey S, Rogers P, Roche M, Parker C. A population-based study of prostate cancer chemotherapy. Clin Oncol. 2011;23(10):706–708. doi:10.1016/j.clon.2011.04.014
35. D’Antonio C, Passaro A, Gori B, et al. Bone and brain metastasis in lung cancer: recent advances in therapeutic strategies. Ther Adv Med Oncol. 2014;6(3):101–114. doi:10.1177/1758834014521110
36. Zheng H, Bae Y, Kasimir-Bauer S, et al. Therapeutic antibody targeting tumor- and osteoblastic niche-derived jagged1 sensitizes bone metastasis to chemotherapy. Cancer Cell. 2017;32(6):731–747.e736. doi:10.1016/j.ccell.2017.11.002
37. Koizumi M, Motegi K, Umeda T. A novel biomarker, active whole skeletal total lesion glycolysis (WS-TLG), as a quantitative method to measure bone metastatic activity in breast cancer patients. Ann Nucl Med. 2019;33(7):502–511. doi:10.1007/s12149-019-01359-4
38. Sarin H. Physiologic upper limits of pore size of different blood capillary types and another perspective on the dual pore theory of microvascular permeability. J Angiogenes Res. 2010;2(1):14. doi:10.1186/2040-2384-2-14
39. Xu M, Li S. Nano-drug delivery system targeting tumor microenvironment: a prospective strategy for melanoma treatment. Cancer Lett. 2023;574:216397. doi:10.1016/j.canlet.2023.216397
40. He Y, Huang Y, Huang Z, et al. Bisphosphonate-functionalized coordination polymer nanoparticles for the treatment of bone metastatic breast cancer. J Control Release. 2017;264:76–88. doi:10.1016/j.jconrel.2017.08.024
41. Wu H, Luo Y, Xu D, Ke X, Ci T. Low molecular weight heparin modified bone targeting liposomes for orthotopic osteosarcoma and breast cancer bone metastatic tumors. Int J Biol Macromol. 2020;164:2583–2597. doi:10.1016/j.ijbiomac.2020.08.068
42. Bussard KM, Gigliotti CM, Adair BM, et al. Preferential uptake of antibody targeted calcium phosphosilicate nanoparticles by metastatic triple negative breast cancer cells in co-cultures of human metastatic breast cancer cells plus bone osteoblasts. Nanomedicine. 2021;34:102383. doi:10.1016/j.nano.2021.102383
43. Wen W, Guo P, Xue HY, Lun Wong H. Development of local injectable, bone-targeting nanocarriers of triptolide for treatment of bone-only metastasis. Int J Pharm. 2022;625:122092. doi:10.1016/j.ijpharm.2022.122092
44. Li J, Hu H, Jiang Z, et al. Near-infrared-induced IR780-loaded PLGA nanoparticles for photothermal therapy to treat breast cancer metastasis in bones. RSC Adv. 2019;9(62):35976–35983. doi:10.1039/C9RA05813C
45. Pang Y, Fu Y, Li C, et al. Metal-organic framework nanoparticles for ameliorating breast cancer-associated osteolysis. Nano Lett. 2020;20(2):829–840. doi:10.1021/acs.nanolett.9b02916
46. Otaka A, Yamaguchi T, Saisho R, Hiraga T, Iwasaki Y. Bone-targeting phospholipid polymers to solubilize the lipophilic anticancer drug. J Biomed Mater Res Part A. 2020;108(10):2090–2099. doi:10.1002/jbm.a.36968
47. Hatami E, Bhusetty Nagesh PK, Chowdhury P, et al. Development of zoledronic acid-based nanoassemblies for bone-targeted anticancer therapy. ACS Biomater Sci Eng. 2019;5(5):2343–2354. doi:10.1021/acsbiomaterials.9b00362
48. Vanderburgh JP, Kwakwa KA, Werfel TA, et al. Systemic delivery of a Gli inhibitor via polymeric nanocarriers inhibits tumor-induced bone disease. J Controlled Release. 2019;311–312:257–272. doi:10.1016/j.jconrel.2019.08.038
49. Zhang Y, Wang Y, Zhu A, Yu N, Xia J, Li J. Dual-targeting biomimetic semiconducting polymer nanocomposites for amplified theranostics of bone metastasis. Angew Chem. 2024;63(2):1.
50. Vanderburgh J, Hill JL, Gupta MK, et al. Tuning ligand density to optimize pharmacokinetics of targeted nanoparticles for dual protection against tumor-induced bone destruction. ACS Nano. 2020;14(1):311–327. doi:10.1021/acsnano.9b04571
51. Lim CW, Kim D. Bone targeting nano-aggregates prepared from self-assembled polyaspartamide graft copolymers for pH sensitive DOX delivery. Biomater Sci. 2021;9(5):1660–1667. doi:10.1039/D0BM01473G
52. Liu C, Hu A, Chen H, et al. The osteogenic niche-targeted arsenic nanoparticles prevent colonization of disseminated breast tumor cells in the bone. Acta pharmaceutica Sinica B. 2022;12(1):364–377. doi:10.1016/j.apsb.2021.06.012
53. Li Z, Liu P, Chen W, et al. Hypoxia-cleavable and specific targeted nanomedicine delivers epigenetic drugs for enhanced treatment of breast cancer and bone metastasis. J Nanobiotechnol. 2023;21(1):221. doi:10.1186/s12951-023-01939-7
54. Zou B, Xiong Z, He L, Chen T. Reversing breast cancer bone metastasis by metal organic framework-capped nanotherapeutics via suppressing osteoclastogenesis. Biomaterials. 2022;285:121549. doi:10.1016/j.biomaterials.2022.121549
55. Huang Y, Xiao Z, Guan Z, et al. Bone-seeking nanoplatform co-delivering cisplatin and zoledronate for synergistic therapy of breast cancer bone metastasis and bone resorption. Acta pharmaceutica Sinica B. 2020;10(12):2384–2403. doi:10.1016/j.apsb.2020.06.006
56. Jie S, Guo X, Ouyang Z. Tumor ablation using novel photothermal Na(x)WO(3) nanoparticles against breast cancer osteolytic bone metastasis. Int J Nanomed. 2019;14:7353–7362. doi:10.2147/IJN.S217974
57. Jiang Z, Li J, Chen S, et al. Zoledronate and SPIO dual-targeting nanoparticles loaded with ICG for photothermal therapy of breast cancer tibial metastasis. Sci Rep. 2020;10(1):13675. doi:10.1038/s41598-020-70659-x
58. Pang Y, Su L, Fu Y, et al. Inhibition of furin by bone targeting superparamagnetic iron oxide nanoparticles alleviated breast cancer bone metastasis. Bioact Mater. 2021;6(3):712–720. doi:10.1016/j.bioactmat.2020.09.006
59. Shen Y, Lv Y. Dual targeted zeolitic imidazolate framework nanoparticles for treating metastatic breast cancer and inhibiting bone destruction. Colloids Surf B. 2022;219:112826. doi:10.1016/j.colsurfb.2022.112826
60. Chen SH, Liu TI, Chuang CL, Chen HH, Chiang WH, Chiu HC. Alendronate/folic acid-decorated polymeric nanoparticles for hierarchically targetable chemotherapy against bone metastatic breast cancer. J Mat Chem B. 2020;8(17):3789–3800. doi:10.1039/D0TB00046A
61. Kievit FM, Stephen ZR, Veiseh O, et al. Targeting of primary breast cancers and metastases in a transgenic mouse model using rationally designed multifunctional SPIONs. ACS nano. 2012;6(3):2591–2601. doi:10.1021/nn205070h
62. Luengo Morato Y, Ovejero Paredes K, Lozano Chamizo L, Marciello M, Filice M. Recent advances in multimodal molecular imaging of cancer mediated by hybrid magnetic nanoparticles. Polymers. 2021;13(17):2989. doi:10.3390/polym13172989
63. Cheng Z, Li M, Dey R, Chen Y. Nanomaterials for cancer therapy: current progress and perspectives. J Hematol Oncol. 2021;14(1):1–27.
64. Gao X, Li L, Cai X, Huang Q, Xiao J, Cheng Y. Targeting nanoparticles for diagnosis and therapy of bone tumors: opportunities and challenges. Biomaterials. 2021;265:120404. doi:10.1016/j.biomaterials.2020.120404
65. Estelrich J, Sánchez-Martín MJ, Busquets MA. Nanoparticles in magnetic resonance imaging: from simple to dual contrast agents. Int J Nanomed. 2015;10:1727–1741. doi:10.2147/IJN.S76501
66. Doolittle E, Peiris PM, Doron G, et al. Spatiotemporal targeting of a dual-ligand nanoparticle to cancer metastasis. ACS Nano. 2015;9(8):8012–8021. doi:10.1021/acsnano.5b01552
67. Fang J, Islam W, Maeda H. Exploiting the dynamics of the EPR effect and strategies to improve the therapeutic effects of nanomedicines by using EPR effect enhancers. Adv Drug Deliv Rev. 2020;157:142–160. doi:10.1016/j.addr.2020.06.005
68. Aghebati-Maleki A, Dolati S, Ahmadi M, et al. Nanoparticles and cancer therapy: perspectives for application of nanoparticles in the treatment of cancers. J Cell Physiol. 2020;235(3):1962–1972. doi:10.1002/jcp.29126
69. He Q, Guo S, Qian Z, Chen X. Development of individualized anti-metastasis strategies by engineering nanomedicines. Chem Soc Rev. 2015;44(17):6258–6286. doi:10.1039/C4CS00511B
70. Huang Y, Li C, Zhang X, et al. Nanotechnology-integrated ovarian cancer metastasis therapy: insights from the metastatic mechanisms into administration routes and therapy strategies. Int J Pharm. 2023;636:122827. doi:10.1016/j.ijpharm.2023.122827
71. Wei W, Zhang X, Zhang S, Wei G, Su Z. Biomedical and bioactive engineered nanomaterials for targeted tumor photothermal therapy: a review. Mater Sci Eng C Mater Biol Appl. 2019;104:109891. doi:10.1016/j.msec.2019.109891
72. Yang T, Zhai J, Hu D, et al. ”Targeting design” of nanoparticles in tumor therapy. Pharmaceutics. 2022;14(9):1919. doi:10.3390/pharmaceutics14091919
73. Martin JD, Cabral H, Stylianopoulos T, Jain RK. Improving cancer immunotherapy using nanomedicines: progress, opportunities and challenges. Nat Rev Clin Oncol. 2020;17(4):251–266. doi:10.1038/s41571-019-0308-z
74. Kang Y, Ha W, Liu Y-Q, et al. pH-responsive polymer–drug conjugates as multifunctional micelles for cancer-drug delivery. Nanotechnology. 2014;25(33):335101. doi:10.1088/0957-4484/25/33/335101
75. Yoo J, Park C, Yi G, Lee D, Koo H. Active targeting strategies using biological ligands for nanoparticle drug delivery systems. Cancers. 2019;11(5):640. doi:10.3390/cancers11050640
76. Patel DJ, Mistri PA, Prajapati JJ. Treatment of cancer by using nanoparticles as a drug delivery. Int J Drug Dev Res. 2012;4(1):14–27.
77. Xiao K, Liu Q, Suby N, et al. LHRH-targeted redox-responsive crosslinked micelles impart selective drug delivery and effective chemotherapy in triple-negative breast cancer. Adv Healthcare Mater. 2021;10(3):e2001196. doi:10.1002/adhm.202001196
78. Vemuri SK, Halder S, Banala RR, et al. Modulatory effects of biosynthesized gold nanoparticles conjugated with curcumin and paclitaxel on tumorigenesis and metastatic pathways-in vitro and in vivo studies. Int J Mol Sci. 2022;23(4):2150. doi:10.3390/ijms23042150
79. Kong X, Qi Y, Wang X, et al. Nanoparticle drug delivery systems and their applications as targeted therapies for triple negative breast cancer. Pro Mater Sci. 2023;2023:101070.
80. Du J, Zhang Y, Jin Z, et al. Targeted NIRF/MR dual-mode imaging of breast cancer brain metastasis using BRBP1-functionalized ultra-small iron oxide nanoparticles. Mater Sci Eng C. 2020;116:111188. doi:10.1016/j.msec.2020.111188
81. Dhas N, García MC, Kudarha R, et al. Advancements in cell membrane camouflaged nanoparticles: a bioinspired platform for cancer therapy. J Controlled Release. 2022;346:71–97. doi:10.1016/j.jconrel.2022.04.019
82. Hou Y, Bu W, Ai H, Lu ZR, Lammers T. Stimuli‐Responsive Nanotheranostics. Vol. 10. Wiley Online Library; 2021:2100243.
83. Sindhwani S, Syed AM, Ngai J, et al. The entry of nanoparticles into solid tumours. Nature Mater. 2020;19(5):566–575. doi:10.1038/s41563-019-0566-2
84. Galley HF, Webster NR. Physiology of the endothelium. Br J Anaesth. 2004;93(1):105–113. doi:10.1093/bja/aeh163
85. Singh T, Kaur V, Kumar M, Kaur P, Murthy RS, Rawal RK. The critical role of bisphosphonates to target bone cancer metastasis: an overview. J Drug Target. 2015;23(1):1–15. doi:10.3109/1061186X.2014.950668
86. Chen Y, Ye J, Lv G, et al. Hydrogen peroxide and hypochlorite responsive fluorescent nanoprobes for sensitive cancer cell imaging. Biosensors. 2022;12(2):1.
87. Blanco E, Shen H, Ferrari M. Principles of nanoparticle design for overcoming biological barriers to drug delivery. Nat Biotechnol. 2015;33(9):941–951. doi:10.1038/nbt.3330
88. Kang Y, Li S. Nanomaterials: breaking through the bottleneck of tumor immunotherapy. Int J Biol Macromol. 2023;230:123159. doi:10.1016/j.ijbiomac.2023.123159
89. Chen Z, Yue Z, Yang K, Li S. Nanomaterials: small particles show huge possibilities for cancer immunotherapy. J Nanobiotechnol. 2022;20(1):484. doi:10.1186/s12951-022-01692-3
90. Núñez C, Estévez SV, Del Pilar Chantada M. Inorganic nanoparticles in diagnosis and treatment of breast cancer. J Biol Inorg Chem. 2018;23(3):331–345. doi:10.1007/s00775-018-1542-z
91. Roy V, LaPlant BR, Gross GG, Bane CL, Palmieri FM. Phase II trial of weekly nab (nanoparticle albumin-bound)-paclitaxel (nab-paclitaxel) (Abraxane) in combination with gemcitabine in patients with metastatic breast cancer (N0531). Ann Oncol. 2009;20(3):449–453. doi:10.1093/annonc/mdn661
92. Prasanna T, Malik L, McCuaig RD, et al. A phase 1 proof of concept study evaluating the addition of an LSD1 inhibitor to nab-paclitaxel in advanced or metastatic breast cancer (EPI-PRIMED). Front Oncol. 2022;12:862427. doi:10.3389/fonc.2022.862427
93. Rugo HS, Barry WT, Moreno-Aspitia A, et al. Randomized Phase III trial of paclitaxel once per week compared with nanoparticle albumin-bound nab-paclitaxel once per week or ixabepilone with bevacizumab as first-line chemotherapy for locally recurrent or metastatic breast cancer: CALGB 40502/NCCTG N063H (Alliance). J Clin Oncol. 2015;33(21):2361–2369. doi:10.1200/JCO.2014.59.5298
94. Hurria A, Blanchard MS, Synold TW, et al. Age-related changes in nanoparticle albumin-bound paclitaxel pharmacokinetics and pharmacodynamics: influence of chronological versus functional age. Oncologist. 2015;20(1):37–44. doi:10.1634/theoncologist.2014-0202
95. Hurria A, Soto-Perez-de-Celis E, Blanchard S, et al. A phase II trial of older adults with metastatic breast cancer receiving nab-paclitaxel: melding the fields of geriatrics and oncology. Clin Breast Cancer. 2019;19(2):89–96. doi:10.1016/j.clbc.2018.10.002
96. Blum JL, Savin MA, Edelman G, et al. Phase II study of weekly albumin-bound paclitaxel for patients with metastatic breast cancer heavily pretreated with taxanes. Clin Breast Cancer. 2007;7(11):850–856. doi:10.3816/CBC.2007.n.049
97. Gennari A, Sun Z, Hasler-Strub U, et al. A randomized phase II study evaluating different maintenance schedules of nab-paclitaxel in the first-line treatment of metastatic breast cancer: final results of the IBCSG 42-12/BIG 2-12 SNAP trial. Ann Oncol. 2018;29(3):661–668. doi:10.1093/annonc/mdx772
98. Yardley DA, Hart L, Bosserman L, et al. Phase II study evaluating lapatinib in combination with nab-paclitaxel in HER2-overexpressing metastatic breast cancer patients who have received no more than one prior chemotherapeutic regimen. Breast Cancer Res Treat. 2013;137(2):457–464. doi:10.1007/s10549-012-2341-9
99. Ciruelos E, Apellániz-Ruiz M, Cantos B, et al. A pilot, phase II, randomized, open-label clinical trial comparing the neurotoxicity of three dose regimens of nab-paclitaxel to that of solvent-based paclitaxel as the first-line treatment for patients with human epidermal growth factor receptor type 2-negative metastatic breast cancer. Oncologist. 2019;24(11):e1024–e1033. doi:10.1634/theoncologist.2017-0664
100. Salazar LG, Lu H, Reichow JL, et al. Topical imiquimod plus nab-paclitaxel for breast cancer cutaneous metastases: a phase 2 clinical trial. JAMA Oncol. 2017;3(7):969–973. doi:10.1001/jamaoncol.2016.6007
101. Untch M, Jackisch C, Schneeweiss A, et al. Nab-paclitaxel versus solvent-based paclitaxel in neoadjuvant chemotherapy for early breast cancer (GeparSepto-GBG 69): a randomised, Phase 3 trial. Lancet Oncol. 2016;17(3):345–356. doi:10.1016/S1470-2045(15)00542-2
102. Fujiwara Y, Mukai H, Saeki T, et al. A multi-national, randomised, open-label, parallel, phase III non-inferiority study comparing NK105 and paclitaxel in metastatic or recurrent breast cancer patients. Br J Cancer. 2019;120(5):475–480. doi:10.1038/s41416-019-0391-z
103. Fuentes-Chust C, Parolo C, Rosati G, et al. The microbiome meets nanotechnology: opportunities and challenges in developing new diagnostic devices. Adv Mater. 2021;33(18):e2006104. doi:10.1002/adma.202006104
104. El-Haibi CP, Bell GW, Zhang J, et al. Critical role for lysyl oxidase in mesenchymal stem cell-driven breast cancer malignancy. Proc Natl Acad Sci U S A. 2012;109(43):17460–17465. doi:10.1073/pnas.1206653109
105. La-Beck NM, Islam MR, Markiewski MM. Nanoparticle-induced complement activation: implications for cancer nanomedicine. Front Immunol. 2020;11:603039. doi:10.3389/fimmu.2020.603039
106. Liu J, Zeng Y, Shi S, et al. Design of polyaspartic acid peptide-poly (ethylene glycol)-poly (ε-caprolactone) nanoparticles as a carrier of hydrophobic drugs targeting cancer metastasized to bone. Int J Nanomed. 2017;12:3561–3575. doi:10.2147/IJN.S133787
107. Yang T, Cui FD, Choi MK, et al. Enhanced solubility and stability of PEGylated liposomal paclitaxel: in vitro and in vivo evaluation. Int J Pharm. 2007;338(1–2):317–326. doi:10.1016/j.ijpharm.2007.02.011
108. Shafei A, El-Bakly W, Sobhy A, et al. A review on the efficacy and toxicity of different doxorubicin nanoparticles for targeted therapy in metastatic breast cancer. Biomed Pharmacother. 2017;95:1209–1218. doi:10.1016/j.biopha.2017.09.059
109. Wong MY, Chiu GN. Liposome formulation of co-encapsulated vincristine and quercetin enhanced antitumor activity in a trastuzumab-insensitive breast tumor xenograft model. Nanomedicine. 2011;7(6):834–840. doi:10.1016/j.nano.2011.02.001
110. Petros RA, DeSimone JM. Strategies in the design of nanoparticles for therapeutic applications. Nat Rev Drug Discov. 2010;9(8):615–627. doi:10.1038/nrd2591
111. Zheng P, Ding B, Jiang Z, et al. Ultrasound-augmented mitochondrial calcium ion overload by calcium nanomodulator to induce immunogenic cell death. Nano Lett. 2021;21(5):2088–2093. doi:10.1021/acs.nanolett.0c04778
112. Cheng X, Wei J, Ge Q, et al. The optimized drug delivery systems of treating cancer bone metastatic osteolysis with nanomaterials. Drug Deliv. 2021;28(1):37–53. doi:10.1080/10717544.2020.1856225
113. Nichols JW, Bae YH. EPR: evidence and fallacy. J Control Release. 2014;190:451–464. doi:10.1016/j.jconrel.2014.03.057
114. Wang W, Mattoussi H. Engineering the bio-nano interface using a multifunctional coordinating polymer coating. Acc Chem Res. 2020;53(6):1124–1138. doi:10.1021/acs.accounts.9b00641
115. Salavati H, Debbaut C, Pullens P, Ceelen W. Interstitial fluid pressure as an emerging biomarker in solid tumors. Biochim Biophys Acta Rev Cancer. 2022;1877(5):188792. doi:10.1016/j.bbcan.2022.188792
116. Aftab S, Shah A, Nadhman A, et al. Nanomedicine: an effective tool in cancer therapy. Int J Pharm. 2018;540(1–2):132–149. doi:10.1016/j.ijpharm.2018.02.007
117. Suk JS, Xu Q, Kim N, Hanes J, Ensign LM. PEGylation as a strategy for improving nanoparticle-based drug and gene delivery. Adv Drug Deliv Rev. 2016;99(Pt A):28–51. doi:10.1016/j.addr.2015.09.012
118. Shi L, Zhang J, Zhao M, et al. Effects of polyethylene glycol on the surface of nanoparticles for targeted drug delivery. Nanoscale. 2021;13(24):10748–10764. doi:10.1039/D1NR02065J
119. Adjei IM, Sharma B, Peetla C, Labhasetwar V. Inhibition of bone loss with surface-modulated, drug-loaded nanoparticles in an intraosseous model of prostate cancer. J Control Release. 2016;232:83–92. doi:10.1016/j.jconrel.2016.04.019
120. Raj S, Khurana S, Choudhari R, et al. Specific targeting cancer cells with nanoparticles and drug delivery in cancer therapy. Semin Cancer Biol. 2021;69:166–177. doi:10.1016/j.semcancer.2019.11.002
121. Lee H, Gaddy D, Ventura M, et al. Companion diagnostic (64)cu-liposome positron emission tomography enables characterization of drug delivery to tumors and predicts response to cancer nanomedicines. Theranostics. 2018;8(9):2300–2312. doi:10.7150/thno.21670
122. Ramamoorthi G, Kodumudi K, Gallen C, et al. Disseminated cancer cells in breast cancer: mechanism of dissemination and dormancy and emerging insights on therapeutic opportunities. Semin Cancer Biol. 2022;78:78–89. doi:10.1016/j.semcancer.2021.02.004
123. Zeng Y, Hoque J, Varghese S. Biomaterial-assisted local and systemic delivery of bioactive agents for bone repair. Acta Biomater. 2019;93:152–168. doi:10.1016/j.actbio.2019.01.060
124. Raina DB, Qayoom I, Larsson D, et al. Guided tissue engineering for healing of cancellous and cortical bone using a combination of biomaterial based scaffolding and local bone active molecule delivery. Biomaterials. 2019;188:38–49. doi:10.1016/j.biomaterials.2018.10.004
125. Ramanlal Chaudhari K, Kumar A, Megraj Khandelwal VK, et al. Bone metastasis targeting: a novel approach to reach bone using Zoledronate anchored PLGA nanoparticle as carrier system loaded with Docetaxel. J Control Release. 2012;158(3):470–478. doi:10.1016/j.jconrel.2011.11.020
126. Au KM, Satterlee A, Min Y, et al. Folate-targeted pH-responsive calcium zoledronate nanoscale metal-organic frameworks: turning a bone antiresorptive agent into an anticancer therapeutic. Biomaterials. 2016;82:178–193. doi:10.1016/j.biomaterials.2015.12.018
127. Bai SB, Cheng Y, Liu DZ, et al. Bone-targeted PAMAM nanoparticle to treat bone metastases of lung cancer. Nanomedicine. 2020;15(9):833–849. doi:10.2217/nnm-2020-0024
128. Chu W, Huang Y, Yang C, et al. Calcium phosphate nanoparticles functionalized with alendronate-conjugated polyethylene glycol (PEG) for the treatment of bone metastasis. Int J Pharm. 2017;516(1–2):352–363. doi:10.1016/j.ijpharm.2016.11.051
129. Salerno M, Cenni E, Fotia C, et al. Bone-targeted doxorubicin-loaded nanoparticles as a tool for the treatment of skeletal metastases. Curr Cancer Drug Targets. 2010;10(7):649–659. doi:10.2174/156800910793605767
130. Morton SW, Shah NJ, Quadir MA, Deng ZJ, Poon Z, Hammond PT. Osteotropic therapy via targeted layer-by-layer nanoparticles. Adv Healthc Mater. 2014;3(6):867–875. doi:10.1002/adhm.201300465
131. Sun W, Ge K, Jin Y, et al. Bone-targeted nanoplatform combining zoledronate and photothermal therapy to treat breast cancer bone metastasis. ACS Nano. 2019;13(7):7556–7567. doi:10.1021/acsnano.9b00097
132. Sun W, Han Y, Li Z, Ge K, Zhang J. Bone-targeted mesoporous silica nanocarrier anchored by zoledronate for cancer bone metastasis. Langmuir. 2016;32(36):9237–9244. doi:10.1021/acs.langmuir.6b02228
133. Qiao H, Cui Z, Yang S, et al. Targeting osteocytes to attenuate early breast cancer bone metastasis by theranostic upconversion nanoparticles with responsive plumbagin release. ACS Nano. 2017;11(7):7259–7273. doi:10.1021/acsnano.7b03197
134. Ye WL, Zhao YP, Li HQ, et al. Doxorubicin-poly (ethylene glycol)-alendronate self-assembled micelles for targeted therapy of bone metastatic cancer. Sci Rep. 2015;5(1):14614. doi:10.1038/srep14614
135. Clementi C, Miller K, Mero A, Satchi-Fainaro R, Pasut G. Dendritic poly(ethylene glycol) bearing paclitaxel and alendronate for targeting bone neoplasms. Mol Pharmaceut. 2011;8(4):1063–1072. doi:10.1021/mp2001445
136. Müller WEG, Neufurth M, Wang S, et al. Amorphous, smart, and bioinspired polyphosphate nano/microparticles: a biomaterial for regeneration and repair of osteo-articular impairments in-situ. Int J Mol Sci. 2018;19(2):427. doi:10.3390/ijms19020427
137. Mann AP, Tanaka T, Somasunderam A, Liu X, Gorenstein DG, Ferrari M. E-selectin-targeted porous silicon particle for nanoparticle delivery to the bone marrow. Adv Materials. 2011;23(36):H278–H282. doi:10.1002/adma.201101541
138. Murahashi M, Kogami A, Muramoto A, et al. Vascular E-selectin expression detected in formalin-fixed, paraffin-embedded sections with an E-selectin monoclonal antibody correlates with ulcerative colitis activity. J Histochem Cytochem. 2022;70(4):299–310. doi:10.1369/00221554221085336
139. Zhao YP, Ye WL, Liu DZ, et al. Redox and pH dual sensitive bone targeting nanoparticles to treat breast cancer bone metastases and inhibit bone resorption. Nanoscale. 2017;9(19):6264–6277. doi:10.1039/C7NR00962C
140. Xiang X, Feng X, Lu S, et al. Indocyanine green potentiated paclitaxel nanoprodrugs for imaging and chemotherapy. Exploration. 2022;2(4):20220008. doi:10.1002/EXP.20220008
141. Yao Y, Zhou Y, Liu L, et al. Nanoparticle-based drug delivery in cancer therapy and its role in overcoming drug resistance. Front Mol Biosci. 2020;7:193. doi:10.3389/fmolb.2020.00193
142. You X, Kang Y, Hollett G, et al. Polymeric nanoparticles for colon cancer therapy: overview and perspectives. J Mater Chem B. 2016;4(48):7779–7792. doi:10.1039/C6TB01925K
143. Björnmalm M, Thurecht KJ, Michael M, Scott AM, Caruso F. Bridging bio-nano science and cancer nanomedicine. ACS Nano. 2017;11(10):9594–9613. doi:10.1021/acsnano.7b04855
144. Jokerst JV, Lobovkina T, Zare RN, Gambhir SS. Nanoparticle PEGylation for imaging and therapy. Nanomedicine. 2011;6(4):715–728. doi:10.2217/nnm.11.19
145. Stefanick JF, Ashley JD, Bilgicer B. Enhanced cellular uptake of peptide-targeted nanoparticles through increased peptide hydrophilicity and optimized ethylene glycol peptide-linker length. ACS Nano. 2013;7(9):8115–8127. doi:10.1021/nn4033954
146. Li B, Li Q, Mo J, Dai H. Drug-loaded polymeric nanoparticles for cancer stem cell targeting. Front Pharmacol. 2017;8:51.
147. Dubey SK, Bhatt T, Agrawal M, et al. Application of chitosan modified nanocarriers in breast cancer. Int J Biol Macromol. 2022;194:521–538. doi:10.1016/j.ijbiomac.2021.11.095
148. Liu X, Taftaf R, Kawaguchi M, et al. Homophilic CD44 interactions mediate tumor cell aggregation and polyclonal metastasis in patient-derived breast cancer models. Cancer Discov. 2019;9(1):96–113. doi:10.1158/2159-8290.CD-18-0065
149. Guo C, Chen Y, Gao W, et al. Liposomal nanoparticles carrying anti-IL6R antibody to the tumour microenvironment inhibit metastasis in two molecular subtypes of breast cancer mouse models. Theranostics. 2017;7(3):775–788. doi:10.7150/thno.17237
150. Youm I, Agrahari V, Murowchick JB, Youan BB. Uptake and cytotoxicity of docetaxel-loaded hyaluronic acid-grafted oily core nanocapsules in MDA-MB 231 cancer cells. Pharm Res. 2014;31(9):2439–2452. doi:10.1007/s11095-014-1339-x
151. Niu Y, Yang H, Yu Z, et al. Intervention with the bone-associated tumor vicious cycle through dual-protein therapeutics for treatment of skeletal-related events and bone metastases. ACS Nano. 2022;16(2):2209–2223. doi:10.1021/acsnano.1c08269
152. Lu YL, Ma YB, Feng C, et al. Co-delivery of cyclopamine and doxorubicin mediated by bovine serum albumin nanoparticles reverses doxorubicin resistance in breast cancer by down-regulating p-glycoprotein expression. J Cancer. 2019;10(10):2357–2368. doi:10.7150/jca.30323
153. Wang L, Song L, Li J, et al. Bone sialoprotein-αvβ3 integrin axis promotes breast cancer metastasis to the bone. Cancer Sci. 2019;110(10):3157–3172. doi:10.1111/cas.14172
154. Ross MH, Esser AK, Fox GC, et al. Bone-induced expression of integrin β3 enables targeted nanotherapy of breast cancer metastases. Cancer Res. 2017;77(22):6299–6312. doi:10.1158/0008-5472.CAN-17-1225
155. Amreddy N, Babu A, Muralidharan R, et al. Recent advances in nanoparticle-based cancer drug and gene delivery. Adv Cancer Res. 2018;137:115–170.
156. Zheng C, Zhang D, Kong Y, et al. Dynamic regulation of drug biodistribution by turning tumors into decoys for biomimetic nanoplatform to enhance the chemotherapeutic efficacy of breast cancer with bone metastasis. Exploration. 2023;3(4):20220124. doi:10.1002/EXP.20220124
157. Bado IL, Zhang W, Hu J, et al. The bone microenvironment increases phenotypic plasticity of ER(+) breast cancer cells. Dev Cell. 2021;56(8):1100–1117.e1109. doi:10.1016/j.devcel.2021.03.008
158. Cheng JN, Frye JB, Whitman SA, Kunihiro AG, Pandey R, Funk JL. A role for TGFβ signaling in preclinical osteolytic estrogen receptor-positive breast cancer bone metastases progression. Int J Mol Sci. 2021;22(9). doi:10.3390/ijms22094463
159. Li B, Qi F, Zhu F, et al. Nanoparticle-based combination therapy enhances fulvestrant efficacy and overcomes tumor resistance in ER-positive breast cancer. Cancer Res. 2023;83(17):2924–2937. doi:10.1158/0008-5472.CAN-22-3559
160. Chittasupho C, Anuchapreeda S, Sarisuta N. CXCR4 targeted dendrimer for anti-cancer drug delivery and breast cancer cell migration inhibition. Eur J Pharm Biopharm. 2017;119:310–321. doi:10.1016/j.ejpb.2017.07.003
161. Paoletti L, Zoratto N, Benvenuto M, et al. Hyaluronan-estradiol nanogels as potential drug carriers to target ER+ breast cancer cell line. Carbohydr Polym. 2023;314:120900. doi:10.1016/j.carbpol.2023.120900
162. Zhang Y, Leonard M, Shu Y, et al. Overcoming tamoxifen resistance of human breast cancer by targeted gene silencing using multifunctional pRNA nanoparticles. ACS Nano. 2017;11(1):335–346. doi:10.1021/acsnano.6b05910
163. Tang H, Chen J, Wang L, et al. Co-delivery of epirubicin and paclitaxel using an estrone-targeted PEGylated liposomal nanoparticle for breast cancer. Int J Pharm. 2020;573:118806. doi:10.1016/j.ijpharm.2019.118806
164. Xiong H, Wang C, Wang Z, Jiang Z, Zhou J, Yao J. Intracellular cascade activated nanosystem for improving ER+ breast cancer therapy through attacking GSH-mediated metabolic vulnerability. J Controlled Release. 2019;309:145–157. doi:10.1016/j.jconrel.2019.07.029
165. Charlesworth CT, Hsu I, Wilkinson AC, Nakauchi H. Immunological barriers to haematopoietic stem cell gene therapy. Nat Rev Immunol. 2022;22(12):719–733. doi:10.1038/s41577-022-00698-0
166. Wang T, Shigdar S, Shamaileh HA, et al. Challenges and opportunities for siRNA-based cancer treatment. Cancer Lett. 2017;387:77–83. doi:10.1016/j.canlet.2016.03.045
167. Guo Y, Wang J, Zhang L, et al. Theranostical nanosystem-mediated identification of an oncogene and highly effective therapy in hepatocellular carcinoma. Hepatology. 2016;63(4):1240–1255. doi:10.1002/hep.28409
168. Liang Y, Zhang H, Song X, Yang Q. Metastatic heterogeneity of breast cancer: molecular mechanism and potential therapeutic targets. Semin Cancer Biol. 2020;60:14–27. doi:10.1016/j.semcancer.2019.08.012
169. Kamaruzman NI, Aziz NA, Poh CL, Chowdhury EH. Oncogenic signaling in tumorigenesis and applications of siRNA nanotherapeutics in breast cancer. Cancers (Basel). 2019;11(5):632. doi:10.3390/cancers11050632
170. Ngamcherdtrakul W, Yantasee W. siRNA therapeutics for breast cancer: recent efforts in targeting metastasis, drug resistance, and immune evasion. Transl Res. 2019;214:105–120. doi:10.1016/j.trsl.2019.08.005
171. Zuckerman JE, Davis ME. Clinical experiences with systemically administered siRNA-based therapeutics in cancer. Nat Rev Drug Discov. 2015;14(12):843–856. doi:10.1038/nrd4685
172. Deng ZJ, Morton SW, Ben-Akiva E, Dreaden EC, Shopsowitz KE, Hammond PT. Layer-by-layer nanoparticles for systemic codelivery of an anticancer drug and siRNA for potential triple-negative breast cancer treatment. ACS Nano. 2013;7(11):9571–9584. doi:10.1021/nn4047925
173. Wang X, Yu B, Wu Y, Lee RJ, Lee LJ. Efficient down-regulation of CDK4 by novel lipid nanoparticle-mediated siRNA delivery. Anticancer Res. 2011;31(5):1619–1626.
174. Mirza Z, Karim S. Nanoparticles-based drug delivery and gene therapy for breast cancer: recent advancements and future challenges. Semin Cancer Biol. 2021;69:226–237. doi:10.1016/j.semcancer.2019.10.020
175. Xu CF, Zhang HB, Sun CY, et al. Tumor acidity-sensitive linkage-bridged block copolymer for therapeutic siRNA delivery. Biomaterials. 2016;88:48–59. doi:10.1016/j.biomaterials.2016.02.031
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.