Back to Journals » Nanotechnology, Science and Applications » Volume 19
Nanofiber Matrix Dressing for Split-Thickness Skin Graft Donor Sites: A Randomized Comparative Clinical Study
Authors Biskupski M ![]() , Antonov S, Górecka ZM, Wójcik R, Żuchowska K, Majewski M, Torres K
, Antonov S, Górecka ZM, Wójcik R, Żuchowska K, Majewski M, Torres K
Received 14 April 2026
Accepted for publication 9 June 2026
Published 8 July 2026 Volume 2026:19 616791
DOI https://doi.org/10.2147/NSA.S616791
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Kattesh Katti
Maciej Biskupski, Sergey Antonov, Zofia Małgorzata Górecka, Rafał Wójcik, Katarzyna Żuchowska, Marek Majewski, Kamil Torres
Department of Plastic, Reconstructive Surgery and Microsurgery, Medical University of Lublin, Lublin, Poland
Correspondence: Maciej Biskupski, Department of Plastic, Reconstructive Surgery and Microsurgery, Medical University of Lublin, Jaczewskiego 8, Lublin, 20-090, Poland, Tel +48 501 321 954, Email [email protected]
Background: Donor-site morbidity after split-thickness skin graft (STSG) harvest remains a significant clinical concern, with pain representing one of the most burdensome early postoperative symptoms. Electrospun nanofiber matrices have emerged as a promising wound management strategy, yet clinical evidence supporting their use in STSG donor sites remains limited. We evaluated the clinical performance of a nanofiber matrix for donor-site management after STSG harvest.
Methods: This single-center randomized comparative study enrolled 40 adult patients undergoing STSG harvest into either the nanofiber matrix group (n=20) or the conventional dressing group with chlorhexidine paraffin gauze and povidone-iodine gauze (n=20). Pain intensity was measured on a 0– 10 scale on postoperative days 1, 2, 5, and 14. Secondary outcomes included donor-site healing time, pruritus during healing, late scar hyperpigmentation, scar elevation, late pruritus, and local or systemic signs of infection.
Results: Compared with conventional management, the nanofiber matrix significantly reduced donor-site pain on postoperative day 1 (p< 0.001), day 2 (p< 0.001), and day 5 (p=0.015), but not on day 14 (p=0.36). The nanofiber group also healed faster than the control group (15.05± 2.34 vs 18.15± 4.38 days; p=0.045). Pruritus during healing did not differ significantly between groups (p=0.97). At late follow-up, we found no significant between-group differences in hyperpigmentation (p=0.11), scar elevation (p=0.051), or late pruritus (p=1.0). Mild exudate occurred in 3 patients in the nanofiber group, without a significant between-group difference (p=0.12), and we identified no other infection-related complications.
Conclusion: Nanofiber matrix dressing reduced early postoperative pain and shortened healing time at STSG donor sites compared with conventional dressing, while late scar outcomes and short-term safety remained comparable between groups. These findings support the potential of nanofiber-based donor-site management as a clinically relevant translational application of electrospinning technology.
Keywords: nanofiber matrix, electrospinning, split-thickness skin graft, donor site, wound healing, postoperative pain
Introduction
Skin grafting is a cornerstone of reconstructive surgery used to restore durable epithelial coverage when wounds cannot heal satisfactorily by secondary intention or when rapid wound closure is required. Among the available graft types, split-thickness skin grafts (STSGs) remain especially important because they include the epidermis and part of the dermis, thereby permitting the donor site to heal by re-epithelialization from residual dermal adnexal structures. Although skin grafting has ancient origins extending back more than 3500 years, modern STSG practice was established during the nineteenth century, particularly through the work of Ollier and Thiersch, and was later refined by the development of dermatomes and modern burn surgery principles.1–3
The clinical relevance of STSGs remains substantial. Burn injury alone continues to represent a major global health burden; the World Health Organization estimates approximately 11 million burn injuries annually worldwide, including about 180,000 deaths, and around 90% of burns occur in low- and middle-income settings.4 In a large U.S. all-payer inpatient analysis, skin grafting was recorded in 15,625 of 53,220 burn-related hospital stays in 2013, corresponding to 29.4% of such admissions, which further illustrates the procedural importance of graft-based wound coverage in burn care.5 In this context, autologous skin grafting remains the gold standard for definitive coverage of many burn wounds, and STSGs are also widely used in other acute and chronic defects requiring stable epithelial resurfacing, including traumatic wounds, ulcers, surgical wounds, and defects following oncologic resection.1–3,6
Despite their value, STSGs create a second wound at the donor site, and donor-site morbidity remains a persistent clinical problem. The ideal donor-site dressing should support rapid and uneventful re-epithelialization while minimizing pain, discomfort, exudation, infection risk, and long-term scarring. Importantly, patients often report the donor site as being more painful than the graft recipient site, and donor-site pain has been described as one of the most distressing symptoms in the early postoperative period. A systematic review of donor-site morbidity demonstrated wide variability in outcomes across the literature, with mean epithelialization times ranging from 4.7 to 35.0 days, mean postoperative day 3 pain scores from 1.24 to 6.38 on 0–10 scales, and infection rates from 0% to 56%; scar-related sequelae were also inconsistently reported, with one study documenting hypertrophic donor-site scarring in 28% of patients at 8 years. These data underscore that donor-site management is not a trivial perioperative detail, but a clinically meaningful determinant of patient recovery and experience.7–10
A broad range of donor-site dressings has been investigated, including paraffin- or tulle-based dressings, semi-occlusive films, hydrocolloids, alginates, hydrogels, silicone dressings, hydrofibers, acrylic dressings, and biologically derived materials. Nevertheless, after decades of study, no single universally accepted donor-site dressing has emerged. Systematic reviews and meta-analyses have generally suggested that dressings maintaining a moist wound-healing environment are associated with less pain and faster healing than non-moist approaches, but the literature remains heterogeneous, with inconsistent outcome definitions, variable assessment methods, and many studies of limited methodological strength. Accordingly, donor-site care remains an area in which innovation is still justified.3,7–9
Electrospinning has emerged as a particularly attractive strategy in advanced wound care because it enables the fabrication of nonwoven fibrous matrices with fiber diameters spanning the nano- to microscale range. Electrospun nanofiber membranes are of interest for wound management owing to their high specific surface area, interconnected porosity, tunable architecture, and close structural resemblance to the native extracellular matrix. These characteristics may support a favorable wound microenvironment by facilitating cell adhesion, migration, and proliferation, preserving moisture balance, permitting gas exchange, and providing partial barrier protection against external contamination. In addition, electrospun matrices offer the possibility of incorporating bioactive agents, including antimicrobial compounds, nanoparticles, vitamins, growth factors, drugs, and even living cells. For these reasons, they have been widely investigated as advanced wound dressings and regenerative scaffolds.11–13
The translation of electrospinning into clinical practice has led to the development of portable and handheld systems capable of depositing a temporary nanofibrous matrix directly onto the wound surface. Preclinical work demonstrated the feasibility of such handheld electrospinning devices for superficial partial-thickness wounds, supporting their biocompatibility and practical applicability. Subsequent clinical studies have extended this concept to STSG donor sites and selected burn wounds. In a prospective randomized multicenter donor-site study, Haik et al reported that an electrospun nanofibrous polymeric matrix showed safety and overall efficacy comparable to standard donor-site care, while reducing day 1 dermal irritation. Additional clinical reports have described the use of this platform in superficial-to-partial thickness wounds, partial-thickness facial burns, and superficial-to-intermediate partial-thickness burns, suggesting good tolerability and encouraging healing outcomes. However, the clinical evidence base remains relatively limited, and additional focused comparative studies are needed, particularly for donor-site wounds where pain, healing time, and scar quality are all clinically relevant endpoints.14–18
Therefore, the aim of the present study was to evaluate the clinical performance of a nanofiber matrix used for the management of split-thickness skin graft donor sites, with particular emphasis on postoperative pain, healing time, scar characteristics, pruritus, and donor-site safety outcomes. The novelty of the study lies in its randomized clinical comparison of handheld electrospun nanofiber matrix coverage with conventional donor-site management in routine reconstructive practice, together with the simultaneous assessment of early patient-centered outcomes and later scar-related endpoints.
Methods
Study Design and Ethical Approval
We conducted a single-center randomized comparative study at the Department of Plastic, Reconstructive and Microsurgery, University Clinical Hospital No. 4 in Lublin, Poland, to evaluate whether nanofiber-based donor-site dressing could accelerate healing, reduce pain, improve scar quality, and decrease the risk of infection compared with conventional donor-site management after split-thickness skin graft harvest. The Bioethics Committee of the Medical University of Lublin approved the study protocol (reference No. KE-0024/42/03/2025), and all procedures were conducted in accordance with the Declaration of Helsinki. All participants provided written informed consent for study participation and for publication of anonymized clinical data, including photographs. Patient recruitment and follow-up extended from April 24, 2025, to March 28, 2026.
Participants
A total of 40 patients were enrolled. Eligibility criteria were: age ≥18 years, harvest of a split-thickness skin graft, donor-site area of at least 10 cm2, and provision of informed consent. Exclusion criteria were refusal to participate and treatment with anticoagulant agents, except for prophylactic low-molecular-weight heparin and acetylsalicylic acid at a dose not exceeding 150 mg/day.
Randomization
After participants had provided informed consent, they were randomized in a 1:1 ratio to the study group or the control group using sealed envelopes prepared in advance. Each envelope contained the allocation to either nanofiber matrix treatment or conventional donor-site dressing.
Donor-Site Management
In the study group, nanofiber matrices were generated using the commercially available Spincare® system (Nanomedic Technologies Ltd). After application of the nanofiber matrix, a non-adherent silicone dressing was placed solely to prevent adhesion of the overlying sterile gauze layers. In the control group, the donor site was managed conventionally with a chlorhexidine-containing paraffin dressing and povidone-iodine gauze. Representative stages of donor-site management with the nanofiber system, as well as the appearance of the healed donor site, are shown in Figure 1.
 |
Figure 1 Donor-site management after split-thickness skin graft harvest using the electrospinning system. (A) Fresh donor site immediately after graft harvest, with the electrode attached as required for connection to the device. (B) Application of the nanofiber matrix to the donor site. (C) Donor site after coverage with the nanofiber matrix and a non-adherent silicone dressing. (D) Healed donor site approximately 6 weeks after graft harvest. |
Surgical Technique and Outcome Assessment
All skin grafts were harvested using an electric dermatome. Graft thickness was standardized at 0.2 mm, corresponding to a thin split-thickness skin graft. Before harvesting, the donor area was coated with a thin layer of paraffin to facilitate smooth passage of the dermatome.
Pain intensity at the donor site was self-reported on a 0–10 scale on postoperative days 1, 2, 5, and 14. Information on comorbidities and smoking status was also collected. Donor-site healing time was defined as the interval until separation of the last crusts within the donor area. Scar quality was assessed by a single investigator using separate 0–10 scales for hyperpigmentation and scar elevation, where 0 indicated appearance comparable to adjacent non-donor skin and 10 indicated maximal deviation from the surrounding skin. Pruritus was assessed by patients on a 0–10 scale both during healing and after scar maturation. Patients were additionally monitored for local and systemic signs suggestive of infection, including exudate, erythema around the donor site, fever, and other concerning symptoms. Data were collected during hospitalization, at post-discharge outpatient visits, and by telephone or e-mail.
Statistical Analysis
Statistical analysis was performed using Statistica version 13.3. Quantitative variables were summarized using descriptive statistics appropriate to their distribution, including mean, standard deviation, minimum, maximum, and, where applicable, median and quartiles. Categorical variables were summarized as counts and percentages. Distribution normality was assessed using the Shapiro–Wilk test. Between-group comparisons for normally distributed continuous variables were performed using Student’s t-test, whereas non-normally distributed or ordinal variables were compared using the Mann–Whitney U-test. Categorical variables were compared using Pearson’s chi-square test or Fisher’s exact test, as appropriate. The association between age and donor-site healing time was assessed using Spearman’s rank correlation. All tests were two-sided, and p values <0.05 were considered statistically significant.
Results
A total of 40 patients were included, with 20 patients in each group. Age distribution was consistent with normality in both groups (p=0.54 for the control group and p=0.13 for the study group). Mean age was 58.4±14.9 years in the control group and 59.6±17.3 years in the study group, with no significant between-group difference (p=0.82). Across the entire cohort, 15 patients had diabetes and 8 were smokers; the distribution of diabetes (p=0.74) and smoking status (p=0.12) did not differ significantly between the groups (Table 1).
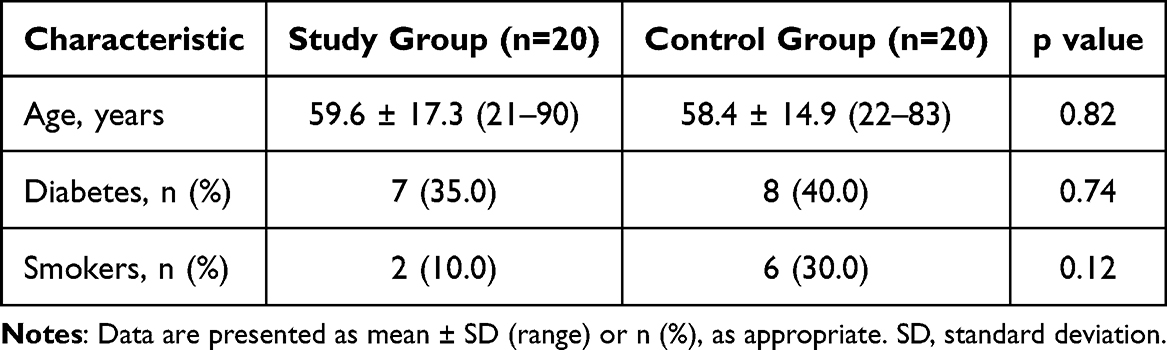 |
Table 1 Baseline Demographic and Clinical Characteristics of the Study Population |
Pain intensity at the donor site was significantly lower in the study group during the early postoperative period (Table 2). On postoperative day 1, mean pain scores were 0.85±0.99 in the study group and 3.16±1.26 in the control group (p<0.001). On day 2, corresponding values were 0.30±0.57 and 2.16±0.90 (p<0.001), and on day 5 they were 0.35±0.67 and 1.21±1.18, respectively (p=0.015). By postoperative day 14, pain was minimal in both groups and the between-group difference was not statistically significant (0.10±0.45 vs. 0.00±0.00; p=0.36).
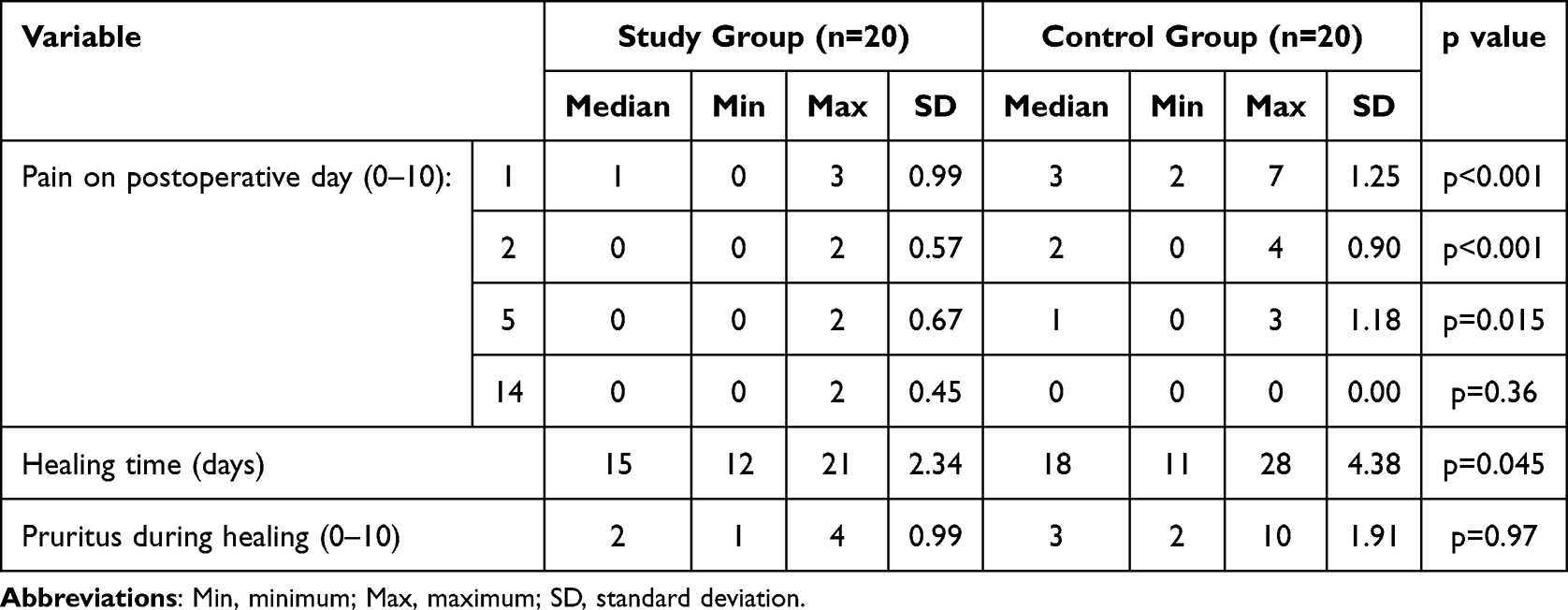 |
Table 2 Early Postoperative Donor-Site Outcomes in the Study and Control Groups |
Donor-site healing time was shorter in the study group than in the control group (Table 2). Mean healing time was 15.05±2.34 days in the study group and 18.15±4.38 days in the control group (p=0.045).
Pruritus during healing did not differ between groups. Mean pruritus scores were 2.5 in the study group and 3.18 in the control group (p=0.97). At late donor-site assessment, hyperpigmentation scores were also comparable between the groups (mean 6.11 in the study group vs. 6.47 in the control group; p=0.11). Scar elevation remained low in both groups; the between-group difference did not reach statistical significance (mean 0.37 in the study group vs. 0.00 in the control group; p=0.051). Late donor-site pruritus was absent in both groups (p=1.0) (Table 3).
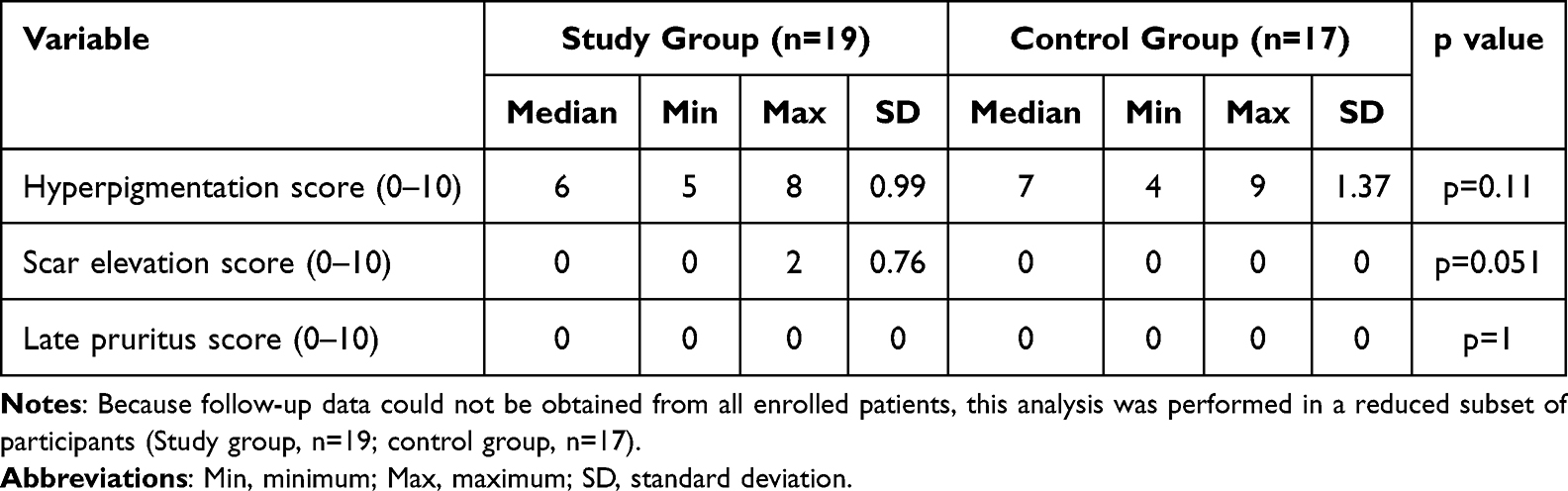 |
Table 3 Late Donor-Site Scar Outcomes in the Study and Control Groups |
Neither diabetes (p=0.27) nor smoking status (p=0.25) was associated with donor-site healing time. Mild exudate during healing was observed in 3 patients in the study group. This difference was not statistically significant between groups (p=0.12). However, the presence of exudate was associated with longer healing time (p=0.048). No other local or systemic signs of infection related to donor-site healing were observed. Older age correlated positively with longer healing time (Spearman R=0.38; p=0.015).
Discussion
The present randomized comparative study suggests that nanofiber matrix dressing may provide clinically meaningful benefits in the management of split-thickness skin graft donor sites. Compared with conventional donor-site care, the nanofiber matrix was associated with markedly lower pain intensity during the early postoperative period and a shorter time to healing, whereas later scar-related outcomes and short-term safety remained broadly comparable between groups. The main value of the present study lies in its translational positioning: rather than revisiting the theoretical advantages of electrospinning alone, it tests whether a handheld electrospun nanofiber matrix can deliver measurable clinical benefit in routine donor-site care. In that sense, the study addresses a specific gap between material-level promise and practical bedside performance by evaluating early pain, healing time, pruritus, later scar-related outcomes, and donor-site safety within a single randomized clinical framework.3,7,15,19
The reduction in early postoperative pain is one of the most clinically relevant findings of the study. Donor-site pain remains a major contributor to morbidity after split-thickness skin graft harvest and, in some patients, may be more troublesome than the recipient site itself.3,7–10 This result is directionally consistent with the broader donor-site dressing literature, which has repeatedly shown that moist and nonadherent dressings may improve patient comfort when compared with more traditional gauze-based strategies.3,8–10,19–22 Our findings also support the clinical rationale for electrospun wound coverage, because nanofiber matrices are designed to form a conformable temporary protective layer that can preserve a favorable wound microenvironment while reducing mechanical irritation.11–13 The most directly comparable study is the prospective randomized multicenter donor-site trial by Haik et al, which found similar overall efficacy and safety between electrospun matrix coverage and standard care, with improved day 1 dermal irritation in the nanofiber group.15 Compared with that study, our data add a more pronounced signal in favor of nanofiber treatment for early pain and healing time. This difference should be interpreted cautiously, because comparator dressings, study setting, sample structure, and assessed outcomes were not identical; however, it also suggests that the practical clinical effect of electrospun donor-site coverage may depend on the specific conventional regimen against which it is tested.15,19,23–25
The shorter healing time observed in the nanofiber group also appears clinically relevant. In the recent meta-analysis by Ho et al, moist dressings showed faster healing than non-moist strategies and were also associated with lower pain, reinforcing the broader concept that donor-site healing may improve when the wound environment is kept more physiologic and less traumatic.22 In this context, the approximately 3-day reduction in healing time in our cohort is not trivial; it may translate into faster recovery, less wound burden, and a shorter period of vulnerability to exudation and dressing-related discomfort. At the same time, our findings should be interpreted in the wider context of advanced donor-site dressings. Randomized studies comparing modern dressings head-to-head have often shown smaller differences than older comparisons against conventional paraffin-based care.23–25 This may explain why our study, which compared nanofiber matrix coverage with a conventional chlorhexidine-paraffin and povidone-iodine gauze approach, demonstrated a clearer early advantage than some studies comparing only contemporary advanced dressings.23–25
In contrast to the early postoperative endpoints, later scar-related outcomes did not differ significantly between groups. Hyperpigmentation remained common, scar elevation was generally low, and late pruritus was negligible in both groups. These findings are not necessarily unexpected. Donor-site scar maturation is multifactorial and may depend not only on the dressing itself, but also on age, skin phenotype, donor-site depth, inflammatory burden, and duration of remodeling.26–28 Moreover, studies of donor-site scarring frequently report heterogeneous and sometimes subtle long-term differences. Hecker et al found broadly similar performance across several modern donor-site dressings, while long-term randomized follow-up by Karlsson et al did not confirm robust subjective differences in scar outcome between dressing groups.24,27 Therefore, the absence of a clear late scar advantage in our study is compatible with the broader literature and should not negate the importance of the early benefits observed in pain and healing.24–27
The safety findings were also reassuring. Although mild exudate occurred in 3 patients in the nanofiber group, the between-group difference was not statistically significant, and no participant developed other local or systemic signs of infection attributable to donor-site healing. This is broadly consistent with the currently available clinical evidence on handheld electrospinning systems in donor sites and selected burn wounds, where the technology has generally shown acceptable tolerability and short-term safety.14–18 The observed association between exudate and longer healing time should be interpreted with caution because the number of affected patients was small. It is more plausible to interpret exudate here as a marker of a slower-healing wound course rather than as evidence of a specific nanofiber-related complication.29 We also found that older age correlated positively with longer donor-site healing time, which is biologically plausible and consistent with the broader wound-healing literature. By contrast, we did not detect a significant association between healing time and diabetes or smoking status; however, given the limited cohort size, this should not be interpreted as evidence that these factors are clinically irrelevant.28,30
Beyond the direct interpretation of outcomes, the present study also has a specific translational relevance. Electrospun wound dressings are often described in terms of their structural or biological advantages, but real-world adoption depends on more than efficacy alone. Wider clinical implementation will likely require not only reproducible clinical benefit, but also robust manufacturing standardization, control of fiber morphology and batch-to-batch consistency, sterilization compatibility, device usability in routine practice, and a regulatory pathway that is sufficiently clear for nanotechnology-based medical devices.31–33 Current translational literature emphasizes that moving advanced wound technologies from laboratory development to clinical routine remains a complex process, shaped by manufacturing, regulatory, and implementation challenges as much as by biological performance.31–33 In this broader context, the unique angle of our study is that it contributes pragmatic clinical data to a field that is still too often dominated by preclinical promise rather than bedside evidence.31–33
Our study also highlights several actionable research gaps. First, larger multicenter randomized trials are needed to determine whether the benefits observed here remain consistent across different institutions, donor-site locations, and dressing routines. Second, future studies should compare electrospun nanofiber matrices not only with conventional paraffin-based care but also with optimized modern moist donor-site dressings, because that is the most clinically relevant comparative standard today.19,22,24,34 Third, later scar assessment should be strengthened by longer follow-up, validated scar scales, and objective tools for pigmentation, pliability, and surface characterization. Fourth, translational studies should move beyond classical healing endpoints and incorporate analgesic consumption, number of dressing changes, patient satisfaction, workflow burden, and cost-effectiveness, because these factors are likely to influence real-world adoption as much as statistical superiority in a single endpoint.31–33 Finally, once the baseline clinical value of the platform is established more firmly, future work may explore whether electrospun donor-site matrices can be rationally upgraded through controlled incorporation of antimicrobial or other bioactive agents while maintaining manufacturing simplicity and regulatory feasibility.11–13,31–33
Several limitations must be acknowledged. This was a single-center study with a relatively small sample size, which limits external validity and reduces power for less frequent outcomes, particularly infection-related events and late scar differences. Not all patients were available for later follow-up, which weakened the scar analysis and introduced the possibility of attrition bias. In addition, scar quality was assessed using a simple investigator-based 0–10 rating system rather than a validated multidomain scar instrument. Nevertheless, the randomized design, clinically meaningful endpoints, and clear signal in early postoperative pain and healing time support the relevance of the findings and justify further investigation.
Conclusions
In this randomized comparative study, nanofiber matrix dressing reduced donor-site pain during the early postoperative period and shortened healing time after split-thickness skin graft harvest when compared with conventional donor-site dressing. By contrast, pruritus during healing, later scar-related outcomes, and short-term safety remained broadly comparable between groups. Mild exudate occurred in a small number of patients treated with the nanofiber matrix, but no other local or systemic infection-related complications were observed. Taken together, these findings suggest that nanofiber-based donor-site management may improve the early postoperative course without compromising short-term safety. In the broader context of donor-site care, the present study supports handheld electrospun nanofiber coverage as a clinically relevant translational application of electrospinning technology in reconstructive surgery.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work the authors used ChatGPT (GPT-5.4 Thinking, OpenAI) to improve the readability and language of the manuscript.
Data Sharing Statement
The data supporting the findings of this study are not publicly available because they contain clinical information collected from human participants and are subject to privacy and ethical restrictions. De-identified data supporting the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
Ethical approval was obtained from the Bioethics Committee of the Medical University of Lublin (reference No. KE-0024/42/03/2025), and all procedures were carried out in accordance with the Declaration of Helsinki. All participants provided informed consent for study participation.
Consent for Publication
Written informed consent for publication was obtained from all participants whose anonymized clinical information and images are presented in this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The following work was conducted as a part of a project “Ocena zastosowania matryc nanowłóknistych w gojeniu pól dawczych po pobraniu przeszczepu skóry pośredniej grubości” carried out from April 2025 to March 2026 within the financial support provided by the Medical University of Lublin.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jeschke MG, Van Baar ME, Choudhry MA, Chung KK, Gibran NS, Logsetty S. Burn injury. Nat Rev Dis Primers. 2020;6(1):11. doi:10.1038/s41572-020-0145-5
2. Kohlhauser M, Luze H, Nischwitz SP, Kamolz LP. Historical evolution of skin Grafting-A journey through time. Medicina. 2021;57(4):348. doi:10.3390/medicina57040348
3. Brown JE, Holloway SL. An evidence-based review of split-thickness skin graft donor site dressings. Int Wound J. 2018;15(6):1000–10. doi:10.1111/iwj.12967
4. Burns. World Health Organization. Available from: https://www.who.int/news-room/fact-sheets/detail/burns.
5. Burn-Related Hospital Inpatient Stays and Emergency Department Visits, 2013. HCUP statistical brief No. 217. Agency for healthcare research and quality. Available from: https://hcup-us.ahrq.gov/reports/statbriefs/sb217-Burn-Hospital-Stays-ED-Visits-2013.jsp.
6. Braza ME, Marietta M, Fahrenkopf MP. Split-Thickness Skin Grafts. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025.
7. Asuku M, Yu TC, Yan Q, et al. Split-thickness skin graft donor-site morbidity: a systematic literature review. Burns. 2021;47(7):1525–1546. doi:10.1016/j.burns.2021.02.014
8. Voineskos SH, Ayeni OA, McKnight L, Thoma A. Systematic review of skin graft donor-site dressings. Plast Reconstr Surg. 2009;124(1):298–306. doi:10.1097/PRS.0b013e3181a8072f
9. Serebrakian AT, Pickrell BB, Varon DE, et al. Meta-analysis and systematic review of skin graft donor-site dressings with future guidelines. Plast Reconstr Surg Glob Open. 2018;6(9):e1928. doi:10.1097/GOX.0000000000001928
10. Sinha S, Schreiner AJ, Biernaskie J, Nickerson D, Gabriel VA. Treating pain on skin graft donor sites: review and clinical recommendations. J Trauma Acute Care Surg. 2017;83(5):954–964. doi:10.1097/TA.0000000000001615
11. Liu X, Xu H, Zhang M, Yu DG. Electrospun medicated nanofibers for wound healing: review. Membranes. 2021;11(10):770. doi:10.3390/membranes11100770
12. Chen S, Liu B, Carlson MA, Gombart AF, Reilly DA, Xie J. Recent advances in electrospun nanofibers for wound healing. Nanomedicine. 2017;12(11):1335–1352. doi:10.2217/nnm-2017-0017
13. Li K, Zhu Z, Zhai Y, Chen S. Recent advances in electrospun nanofiber-based strategies for diabetic wound healing application. Pharmaceutics. 2023;15(9):2285. doi:10.3390/pharmaceutics15092285
14. Haik J, Kornhaber R, Blal B, Harats M. The feasibility of a handheld electrospinning device for the application of nanofibrous wound dressings. Adv Wound Care. 2017;6(5):166–174. doi:10.1089/wound.2016.0722
15. Haik J, Ullman Y, Gur E, et al. Advances in the use of electrospun nanofibrous polymeric matrix for dermal healing at the donor site after the split-thickness skin graft excision: a prospective, randomized, controlled, open-label, multicenter study. J Burn Care Res. 2022;43(4):889–898. doi:10.1093/jbcr/irab216
16. Schulz A, Fuchs PC, Heitzmann W, Kanho CH, Schiefer JL. Our initial experience in the customized treatment of donor site and burn wounds with a new nanofibrous temporary epidermal layer. Ann Burns Fire Disasters. 2021;34(1):58–66.
17. Vasella M, Cirebea J, Gousopoulos E, et al. Outcome of facial burn injuries treated by a nanofibrous temporary epidermal layer. J Clin Med. 2023;12(16):5273. doi:10.3390/jcm12165273
18. Haik J, Ullmann Y, Gur E, et al. Spincare system demonstrates safety and efficacy in treating partial-thickness burns. J Burn Care Res. 2024;45(4):969–977. doi:10.1093/jbcr/irae024
19. Markel JE, Franke JD, Woodberry KM, Fahrenkopf MP. Recent updates on the management of split-thickness skin graft donor sites. Plast Reconstr Surg Glob Open. 2024;12(9):e6174. doi:10.1097/GOX.0000000000006174
20. Weber RS, Hankins P, Limitone E, et al. Split-thickness skin graft donor site management. A randomized prospective trial comparing a hydrophilic polyurethane absorbent foam dressing with a petrolatum gauze dressing. Arch Otolaryngol Head Neck Surg. 1995;121(10):1145–1149. doi:10.1001/archotol.1995.01890100055009
21. Akhoondinasab MR, Karimi H, Sheikhizadeh S, Saberi M. Reducing pain at split thickness donor sites with silicone dressing compared to petrolatum gauze dressing. Ann Burns Fire Disasters. 2019;32(3):210–215.
22. Ho CY, Chou HY, Wang SH, et al. A comprehensive analysis of moist versus non-moist dressings for split-thickness skin graft donor sites: a systematic review and meta-analysis. Health Sci Rep. 2025;8(1):e70315. doi:10.1002/hsr2.70315
23. Karlsson M, Lindgren M, Jarnhed-Andersson I, Tarpila E. Dressing the split-thickness skin graft donor site: a randomized clinical trial. Adv Skin Wound Care. 2014;27(1):20–25. doi:10.1097/01.ASW.0000437786.92529.22
24. Hecker A, Lumenta DB, Brinskelle P, et al. A randomized controlled trial of three advanced wound dressings in split-thickness skin grafting donor sites-a personalized approach? J Pers Med. 2022;12(9):1395. doi:10.3390/jpm12091395
25. Ismail S, Ali Khan FA, Gulzar S, et al. A single centre, randomized control trial of donor site wound dressings after split-thickness skin grafting. J Ayub Med Coll Abbottabad. 2023;35(4):645–649. doi:10.55519/JAMC-04-12318
26. Legemate CM, Ooms PJ, Trommel N, et al. Patient-reported scar quality of donor-sites following split-skin grafting in burn patients: long-term results of a prospective cohort study. Burns. 2021;47(2):315–321. doi:10.1016/j.burns.2020.12.005
27. Karlsson M, Elmasry M, Steinvall I, Sjöberg F, Olofsson P. Scarring at donor sites after split-thickness skin graft: a prospective, longitudinal, randomized trial. Adv Skin Wound Care. 2020;33(12):1–5. doi:10.1097/01.ASW.0000720256.45983.28
28. Khalid KA, Nawi AFM, Zulkifli N, Barkat MA, Hadi H. Aging and wound healing of the skin: a review of clinical and pathophysiological hallmarks. Life. 2022;12(12):2142. doi:10.3390/life12122142
29. Mervis JS. The impact of chronic wound exudate on the patient, clinician and payer: addressing the challenges with foam dressings. Int Wound J. 2025;22(Suppl 1):e70369. doi:10.1111/iwj.70369
30. Beyene RT, Derryberry SL, Barbul A. The effect of comorbidities on wound healing. Surg Clin North Am. 2020;100(4):695–705. doi:10.1016/j.suc.2020.05.002
31. Uhljar LÉ, Ambrus R. Electrospinning of potential medical devices (Wound dressings, tissue engineering scaffolds, face masks) and their regulatory approach. Pharmaceutics. 2023;15(2):417. doi:10.3390/pharmaceutics15020417
32. Lu X, Zhou L, Song W. Recent progress of electrospun nanofiber dressing in the promotion of wound healing. Polymers. 2024;16(18):2596. doi:10.3390/polym16182596
33. Wang C, Shirzaei Sani E, Shih CD, et al. Wound management materials and technologies from bench to bedside and beyond. Nat Rev Mater. 2024;9(8):550–566. doi:10.1038/s41578-024-00693-y
34. Rahman S, Langridge B, Al-Hadad A, Khan RA, Junejo MH, Mosahebi A. Biological versus non-biological dressings in the management of split-thickness skin-graft donor sites: a systematic review and meta-analysis. J Wound Care. 2020;29(10):604–610. doi:10.12968/jowc.2020.29.10.604
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Sustained-Release Nanosystem with MRSA Biofilm-Dispersing and -Eradicating Abilities Accelerates Diabetic Ulcer Healing

He S, Wen H, Yao N, Wang L, Huang J, Li Z
International Journal of Nanomedicine 2023, 18:3951-3972
Published Date: 19 July 2023
Electrospun Nanofibers from Plant Natural Products: A New Approach Toward Efficient Wound Healing
Liu Q, Luo S, Peng J, Chang R
International Journal of Nanomedicine 2024, 19:13973-13990
Published Date: 27 December 2024
Fusidic Acid and Lidocaine-Loaded Electrospun Nanofibers as a Dressing for Accelerated Healing of Infected Wounds
Alsulami KA, Bakr AA, Sirwi A, Elfaky MA, Shaik RA, Alshehri BY, Aodah AH, Al Fayez N, Alshehri AA, Almughem FA, Halwani AA, Tawfik EA
International Journal of Nanomedicine 2025, 20:849-869
Published Date: 20 January 2025
Nano-Biomimetic Fibronectin/Lysostaphin-Co-Loaded Silk Fibroin Dressing Accelerates Full-Thickness Wound Healing via ECM-Mimicking Microarchitecture and Dual-Function Modulation

Liu CT, Huang LD, Liu K, Pang KF, Tang H, Li T, Huang YP, Zhang WQ, Wang JJ, Yin GL, Hua KZ
International Journal of Nanomedicine 2025, 20:7469-7487
Published Date: 12 June 2025