Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Nano-Enhanced Diets: Advancing Metabolic Dysfunction-Related Steatotic Liver Disease (MASLD) – A Review
Authors Herdiana Y ![]()
Received 27 August 2025
Accepted for publication 11 December 2025
Published 23 December 2025 Volume 2025:18 Pages 4715—4731
DOI https://doi.org/10.2147/DMSO.S562536
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Jae Woong Sull
Yedi Herdiana
Department of Pharmaceutics and Pharmaceutical Technology, Faculty of Pharmacy, Universitas Padjadjaran, Sumedang, West Java, 45363, Indonesia
Correspondence: Yedi Herdiana, Department of Pharmaceutics and Pharmaceutical Technology, Faculty of Pharmacy, Universitas Padjadjaran, Sumedang, West Java, 45363, Indonesia, Email [email protected]
Abstract: Metabolic Dysfunction-Related Steatotic Liver Disease (MASLD) is a global health challenge requiring effective interventions. Although nutraceuticals possess strong hepatoprotective potential in vitro, their clinical efficacy is often hampered by fundamental formulation issues, such as poor solubility and oral bioavailability. To address these challenges, this review evaluates the translational potential of nano-based nutrient delivery systems, specifically platforms such as nanoemulsions, liposomes, and polymeric nanoparticles. Through synthesis of in vivo evidence, we analyze how these platforms modify pharmacokinetic parameters to enhance therapeutic efficacy. Preclinical evidence indicates that nanoplatforms significantly improve solubility and stability, which directly correlate with superior therapeutic outcomes in animal models (including reduced steatosis and fibrosis) compared to conventional compounds. However, the transition to clinical applications remains hampered by a lack of long-term safety data (nanotoxicity) and scalability issues. The future of this field is predicted to lie in the development of green nanotechnology utilizing sustainable and economically viable “food-grade” (GRAS) biopolymers.
Keywords: bioactive delivery systems, oxidative stress, targeted nutrient delivery, nutraceuticals, nanotechnology, bioavailability
Introduction
The liver plays a crucial role in protein synthesis, glucose and lipid metabolism, and detoxification.1 Metabolic-associated fatty liver disease (MAFLD), previously known as non-alcoholic fatty liver disease (NAFLD), was recently proposed by global consensus to have its terminology updated to Steatotic Liver Disease Associated with Metabolic Dysfunction (MASLD). This condition is a common liver disorder characterized by fat accumulation exceeding 5% in the liver in individuals who do not consume large amounts of alcohol (ie, less than 30 g/day for men and less than 20 g/day for women).2 MASLD represents a significant global health burden; it encompasses a broad spectrum of pathologies, ranging from simple hepatic steatosis to steatohepatitis with varying degrees of fibrosis and liver failure.3,4 Statistically, the collective prevalence of MAFLD worldwide has surged, with the most recent data showing a figure of 38.20% between 2016 and 2019. The lowest prevalence was recorded in Southeast Asia (24.25%) and the highest in North Africa and the Middle East (42.62%). In Western Europe, the prevalence reached 32.47%.5,6
The primary cause of this condition is an imbalance between high energy intake and low energy expenditure, which is exacerbated by insulin resistance, obesity, genetic factors, and an unhealthy lifestyle.5 To date, despite its increasing prevalence, there are no officially approved pharmacological therapies for the treatment of MASLD.7 Therefore, current management focuses on symptomatic and supportive measures (including regulation of blood glucose, lipid levels, and body weight), with lifestyle and dietary changes remaining the mainstay of treatment.4,7 Despite being the cornerstone of therapy, conventional nutritional interventions often face significant challenges. Beneficial bioactive compounds and nutraceuticals often have limited oral bioavailability, poor stability during gastrointestinal transit, and a lack of proper targeting to the liver. This rapid degradation and inefficient absorption ultimately reduce therapeutic efficacy and consistency of clinical outcomes, necessitating innovative approaches.8
Recent advances in nanotechnology have opened up promising new opportunities to overcome these limitations, helping to enhance nutrient absorption, maintain the stability of bioactive compounds, and enable targeted delivery to the liver. However, most of the existing literature reviewed in the field of nanomedicine for liver disease predominantly focuses on pharmacological drug delivery. While important, this focus overlooks the fact that nutritional interventions remain the cornerstone of MASLD management. A significant knowledge gap exists regarding how nanotechnology can specifically optimize dietary and nutraceutical interventions, a critical area that is underserved in the review literature. This review specifically aims to fill this gap, establishing its novelty compared to previous nanomedicine reviews.
In contrast to the vast majority of existing nanomedicine reviews, which predominantly focus on pharmacological drug delivery, this review uniquely fills a critical knowledge gap by centering on nutrient delivery systems (nano-nutraceuticals). This distinction is crucial given that lifestyle and nutritional interventions remain the cornerstone of MASLD management, whereas pharmacological therapies often serve a supportive role. Therefore, this review aims to comprehensively analyze several key aspects. First, we evaluate the underlying molecular and physiological mechanisms, specifically how nanotechnology can exploit specific loopholes in MASLD pathogenesis to enable nutrients to act more effectively on cellular targets. Second, the review examines various nanomaterials used in functional foods and their specific impacts on hepatic steatosis, inflammation, and fibrosis. Finally, we critically assess the challenges regarding production scalability, regulatory approval, cost-effectiveness, and potential nanotoxicity, which remain major hurdles for clinical implementation. By synthesizing current evidence, this review aims to accelerate the integration of nanotechnology into next-generation therapeutic nutritional strategies for metabolic health.
Establishing the Role of Nutraceuticals in MASLD Therapy
MASLD is a progressive disease driven by multiple metabolic and lifestyle risk factors. It progresses through a distinct pathological spectrum, ranging from simple fatty liver (steatosis), which is largely reversible, to steatohepatitis (Metabolic-Dysfunction Associated Steatohepatitis (MASH)), fibrosis, cirrhosis, and finally hepatocellular carcinoma (HCC), at which point intervention becomes much more difficult (Figure 1). Understanding this progression is crucial for contextualizing the various therapeutic approaches currently available.
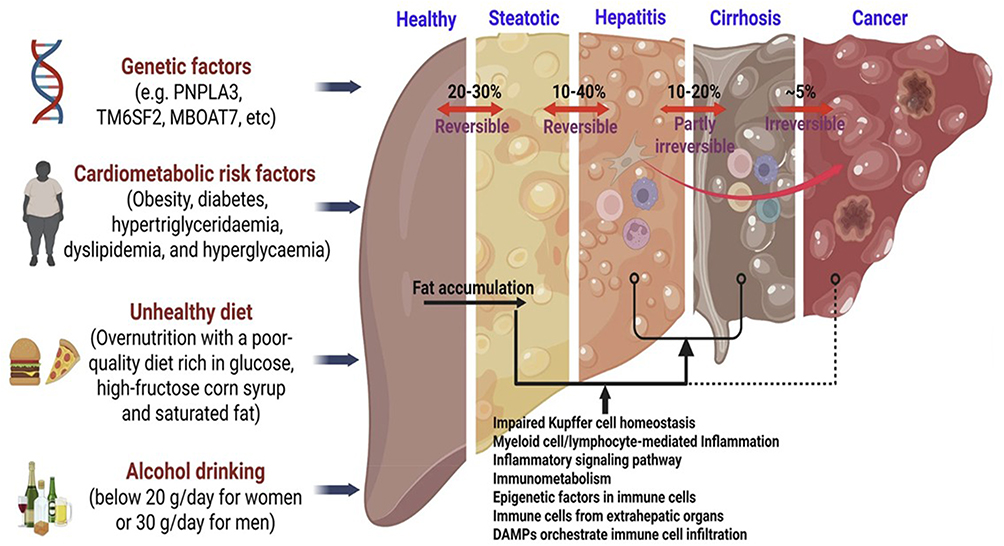 |
Figure 1 A spectrum of MASLD. MASLD represents a spectrum of disorders ranging from simple steatosis to MASH, ultimately resulting in advanced fibrosis, cirrhosis, and cancer. Immunological mechanisms are involved in the development of MASLD, especially simple steatosis-to-MASH conversion.7 |
Overview of Metabolic Dysfunction-Related Fatty Liver Disease (MASLD)
Metabolic Dysfunction-Associated Fatty Liver Disease (MASLD) is a clinicopathological condition closely associated with metabolic syndrome, obesity, and diabetes mellitus.9 This condition encompasses a broad histological spectrum, ranging from simple steatosis (fat accumulation in ≥5% of hepatocytes) to MASH. Progression to MASH is characterized by hepatocyte injury, inflammation, and ultimately, fibrosis.10–12
Pathophysiologically, MASLD is driven by metabolic dysregulation, including increased de novo lipogenesis, insulin resistance, and high fructose intake, that leads to steatosis. The transition from steatosis to MASH is triggered by multiple factors, including oxidative stress, mitochondrial dysfunction, and the release of pro-inflammatory cytokines.13 The key to intervention is reversibility: in the early stages (steatosis or early MASH), the condition is reversible. However, as advanced fibrosis and cirrhosis progress, liver architectural damage becomes irreversible, making early detection and intervention crucial. If current trends persist, MASH could become the leading indication for liver transplantation, surpassing other etiologies such as viral hepatitis and alcohol-related liver disease. HCC represents the terminal stage of MASLD progression, with emerging evidence implicating immune regulation in the transition from MASH to HCC.7
Management of MASLD currently remains a significant clinical challenge. Lifestyle modification (diet and exercise) remains the cornerstone of therapy, but long-term adherence is a major obstacle. Although the recent approval of resmetirom for non-cirrhotic MASLD offers promise, specifically approved pharmacological options remain limited. Various other agents, such as glucagon-like peptide-1 receptor agonists (GLP-1RA) agonists, Sodium-Glucose Transport 2 Inhibitors (SGLT2i), and Thiazolidinediones (TZDs), have shown improvements in liver biomarkers, but often focus on treating comorbidities (such as diabetes) rather than MASLD directly.14
Current Therapeutic Approaches and Their Limitations
Current management of MASLD focuses on non-pharmacological interventions, with lifestyle modifications (diet and exercise) as the mainstay.15–17 This approach has proven effective in reducing liver fat and improving insulin sensitivity. However, the biggest challenge is patient adherence. These therapeutic benefits can only be maintained through long-term commitment, which is often difficult to achieve in the real world, creating a need for more accessible supportive interventions.
In recent years, the pharmacological landscape has evolved rapidly, particularly with the advent of GLP-1 agonists (such as Semaglutide) and the approval of Resmetirome for MASH with fibrosis.12,17 These therapies are very promising, but very targeted: they are intended for patients with more severe disease (confirmed MASH, F2/F3 fibrosis). This leaves the vast majority of patients with early-stage MASLD (simple steatosis) without approved pharmacological options.
For cases of morbid obesity associated with severe MASLD, bariatric surgery (such as RYGB) remains the most effective option for achieving histological resolution.12,18 However, this is an invasive procedure with significant risks, is only intended for a small proportion of the patient population, and is not a scalable public health strategy for the millions of people with early or intermediate-stage disease.
The combination of these three approaches, such as: lifestyle (difficult to maintain), pharmacology (for advanced disease), and surgery (invasive), creates a significant treatment gap. A significant population suffers from simple steatosis or mild inflammation that does not require drastic interventions such as surgery but cannot rely solely on dietary adherence. This is where formulators and nutrition scientists face the greatest clinical opportunity. Table 1 provides an overview that MASLD treatment is continuously being attempted with various approaches.
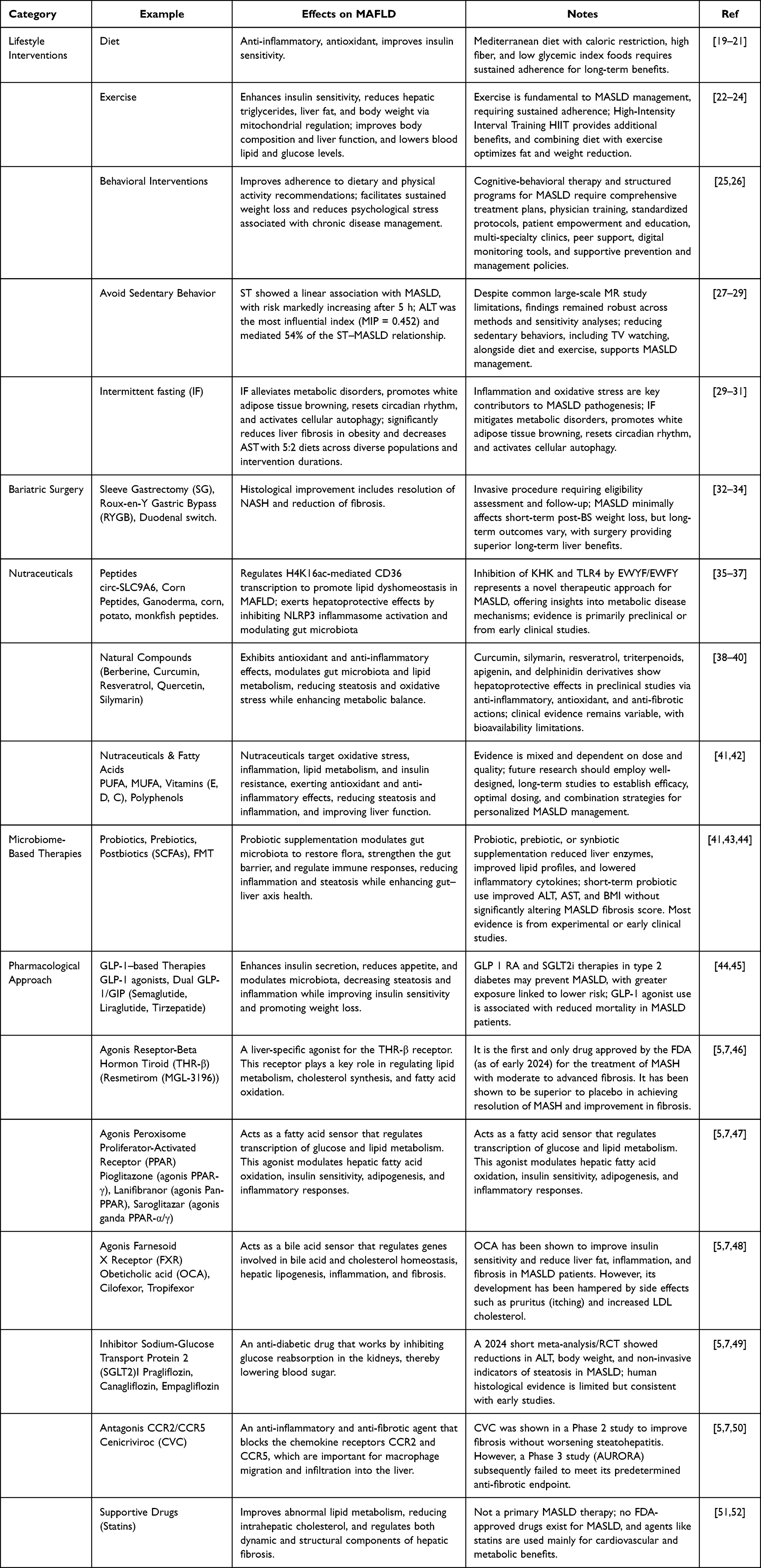 |
Table 1 Developments in MASLD Treatment |
This gap opens the door to safe, effective, and long-term nutraceutical interventions. Compounds such as polyphenols, antioxidants, and probiotics offer significant potential for prevention and early-stage management. However, as we will soon discuss, conventional nutraceuticals have their own limitations that hinder their clinical potential.
Pathological Pathways as Targets for Nano-Nutrients
Dysregulation of Lipid Metabolism
A key target in the pathogenesis of MASLD is dysregulation of lipid metabolism. Molecularly, hyperinsulinemia and excess glucose induce the transcription factor Sterol regulatory element-binding transcription factor 1 (SREBP-1c). SREBP-1c then activates the entire de novo lipogenesis (DNL) program, including the key enzymes Fatty Acid Synthase (FASN) and Acetyl-CoA Carboxylase (ACC), which promote new fatty acid synthesis and triglyceride accumulation (steatosis).53 Many nutraceuticals, particularly polyphenols such as curcumin, resveratrol, and Epigallocatechin gallate (EGCG), have demonstrated strong preclinical potential in modulating this SREBP-1c pathway. However, this therapeutic potential is fundamentally hampered in clinical application. These compounds face a critical gap in the form of very poor aqueous solubility and extensive first-pass metabolism, resulting in very low oral bioavailability, often below 1% for curcumin.54,55 Therefore, the success of nutritional interventions targeting lipogenesis relies heavily on sophisticated delivery systems, creating an urgent need for nanoformulations (such as nanoemulsions or lipid nanoparticles) to enhance solubility, protect compounds, and deliver effective therapeutic doses to the liver.
Oxidative Stress
Excess lipid accumulation in hepatocytes (lipotoxicity) overwhelms the mitochondria, causing electron leakage from the Electron Transport Chain (ETC) and the overproduction of Reactive Oxygen Species (ROS). These ROS then trigger damaging lipid peroxidation, producing highly reactive aldehyde byproducts such as 4-hydroxynonenal (4-HNE).56 Vitamin imbalance plays a crucial role in the pathogenesis of MASLD, particularly in exacerbating oxidative stress. There are two main mechanisms:
Direct Antioxidant Deficiency
Vitamins with potent antioxidant activity, such as vitamins C and E, are directly associated with mitigating hepatocyte injury.
Metabolic Cofactor Deficiency
There is a strong correlation between increasing MASLD severity and decreasing serum levels of other key vitamins. In particular, deficiencies of vitamins D, B12, and folate (B9) are frequently reported.
These imbalances (along with other B-complex vitamins such as B6) contribute to the pathological cycle by exacerbating lipotoxicity, systemic oxidative stress, inflammation, and gut microbiota dysbiosis.57
Therefore, vitamin supplementation should be viewed not only as nutritional replacement but also as a targeted therapeutic intervention to break this cycle of oxidative stress and inflammation. Interventions with potent antioxidants such as Quercetin, Silymarin, and Vitamin E represent a logical therapeutic strategy to neutralize these ROS. However, their clinical efficacy is hampered by significant critical pharmaceutical gaps: Quercetin and Silymarin are practically insoluble in water, while Vitamin E is a lipophilic compound that requires efficient emulsification for absorption. Therefore, nano-encapsulation platforms are crucial for converting these potent but insoluble antioxidants into stable, biodispersible forms, thereby enhancing their intestinal absorption and protective efficacy.
Inflammatory Pathway Activation
The transition from steatosis to MASH is characterized by chronic inflammation. This process is often described as a “two-step signaling pathway”: Signal 1 (priming) occurs when lipopolysaccharide (LPS) or saturated fatty acids activate Nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB). Signal 2 (activation) occurs when ROS or cholesterol crystals activate the nucleotide-binding oligomerization domain, leucine-rich repeat or pyrin domain-containing 3 (NLRP3) inflammasome.58 Nutritional compounds with potent anti-inflammatory properties, such as omega-3 fatty acids (Eicosapentaenoic Acid (EPA)/Docosahexaenoic Acid (DHA)) and some alkaloids (such as berberine), have been shown to modulate the NF-κB and NLRP3 pathways. The critical gap here is twofold: omega-3 fatty acids are highly susceptible to oxidation, which not only reduces their efficacy but also leads to palatability issues (rancid taste/odor). Meanwhile, berberine is known to have very poor oral bioavailability. The nanoscale implications of this are clear: nanoemulsion platforms are crucial for protecting Omega-3s from oxidative degradation and masking their flavor for food fortification, while polymeric nanocarriers are needed to enhance the retention time and absorption of berberine. Emerging therapies such as cytokine inhibitors, antifibrotic agents, metabolic modulators (such as Peroxisome Proliferator-Activated Receptor (PPAR) agonists, Farnesoid X Receptor (FXR) agonists, or GLP-1 receptor agonists), and nutraceuticals show promise in slowing MASLD progression and reducing extrahepatic complications.59
Fibrogenesis
Unmanaged chronic inflammation leads to fibrogenesis. Pro-fibrotic cytokines, particularly Transforming Growth Factor-beta (TGF-β) released by stressed Kupffer cells, trigger the activation of Hepatic Stellate Cells (HSCs). These quiescent HSCs transition into active myofibroblasts, which then produce and deposit large amounts of extracellular matrix (primarily type I collagen).60 Certain nutraceuticals, particularly silymarin (and its active component, silibinin), have demonstrated promising direct antifibrotic effects by inhibiting HSC activation. However, silymarin is perhaps the most classic example of formulation failure in nutraceuticals. Its main critical gap is its near-zero water solubility, which leads to very poor bioavailability and inconsistent clinical trial results, despite its clear in vitro efficacy. Therefore, advances in silymarin delivery rely almost entirely on nanotechnologies, such as phytosomes or solid lipid nanoparticles (SLNs), which directly overcome this fundamental solubility barrier.
Gut-Liver Axis Dysbiosis
Finally, the pathogenesis of MASLD is closely linked to the gut-liver axis. Gut microbiota dysbiosis contributes to increased intestinal permeability, which allows endotoxin (LPS) translocation to the liver and triggers inflammation through TLR4 activation.61 Dietary factors greatly influence the microbiota profile; a high-fat and high-fructose diet exacerbates dysbiosis, while a high-fiber and polyphenol diet shows protective effects through restoration of the microbiota and its metabolites (such as short-chain fatty acids (SCFAs), secondary bile acids, and trimethylamine N-oxide (TMAO)).62–64 A logical intervention strategy is to directly modulate the microbiota through the administration of probiotics and prebiotics. The critical gap for probiotics is unique and absolute: they are fragile living organisms. Most conventional probiotic doses cannot survive the highly acidic pH environment of the stomach. This is where encapsulation (nano- or micro-) becomes crucial.65 The use of food-grade polymers such as alginate or chitosan to encapsulate probiotics is crucial to protect them from gastric transit and ensure their proper release at the target site in the intestine.
Microbial enzymes are also essential factors in the development of MASLD and MASH, primarily through their role in the metabolism of steroids (bile acids), choline, and fatty acids. Specifically, these microbial enzymes are key mediators contributing to the metabolism or biosynthesis of these compounds. Dysfunction in these enzymes due to dysbiosis can compromise the intestinal barrier. This increases permeability to bacterial metabolites and liver exposure to microbial-associated molecular patterns (MAMPs), ultimately worsening liver inflammation and fibrosis. A deeper understanding of the role of these microbial enzymes and metabolites may open up opportunities for more precision therapies in the future.66
Pharmaceutical Gap as Root of Conventional Nutraceutical Failure
The above analyses consistently demonstrate a significant gap between the in vitro mechanistic potential of many nutraceuticals and their in vivo clinical efficacy. This gap is largely not biological in nature, but rather deeply rooted in pharmaceutical and pharmacokinetic barriers.67
The inherent physicochemical properties of these compounds, such as poor aqueous solubility (such as curcumin, silymarin), low gastrointestinal stability (such as probiotics, Omega-3), and inadequate membrane permeability, collectively contribute to their extremely low oral bioavailability.68
Management of MASLD often relies on bioactive compounds, although poor solubility and rapid metabolism limit their therapeutic potential. Turmeric and curcumin have been shown to lower key biomarkers, including liver enzymes (such as Alanine Transaminase (ALT), Aspartate Transaminase (AST)), inflammatory cytokines (such as TNF-α, Interleukin-6 (IL-6)), and serum lipid levels (such as triglycerides, Low-Density Lipoprotein Cholesterol (LDL-C)). Furthermore, both have improved insulin resistance and histological scores (such as NAFLD Activity Score - NAS).69–71 Recent studies resveratrol have identified multiple potential health benefits of RES, including antioxidant, anti-inflammatory, anti-obesity, anticancer, anti-diabetic, cardiovascular, and neuroprotective properties.72 Silymarin does consistently show potential in reducing liver enzymes (ALT, AST) and lipid levels, but this is often linked to its ability to modulate inflammation and oxidative stress.73 Supplementation with hesperidin, naringenin, or green tea extract also improves liver enzymes, lipid profiles, and inflammatory cytokines, while genistein has shown no impact on lipid levels.54
Therefore, the therapeutic potential of these valid molecular targets remains unrealized. Nanotechnology has emerged as a rationally targeted strategy specifically designed to overcome these fundamental pharmaceutical barriers. Table 2 below presents a critical comparison of these challenges and the proposed nano solutions.
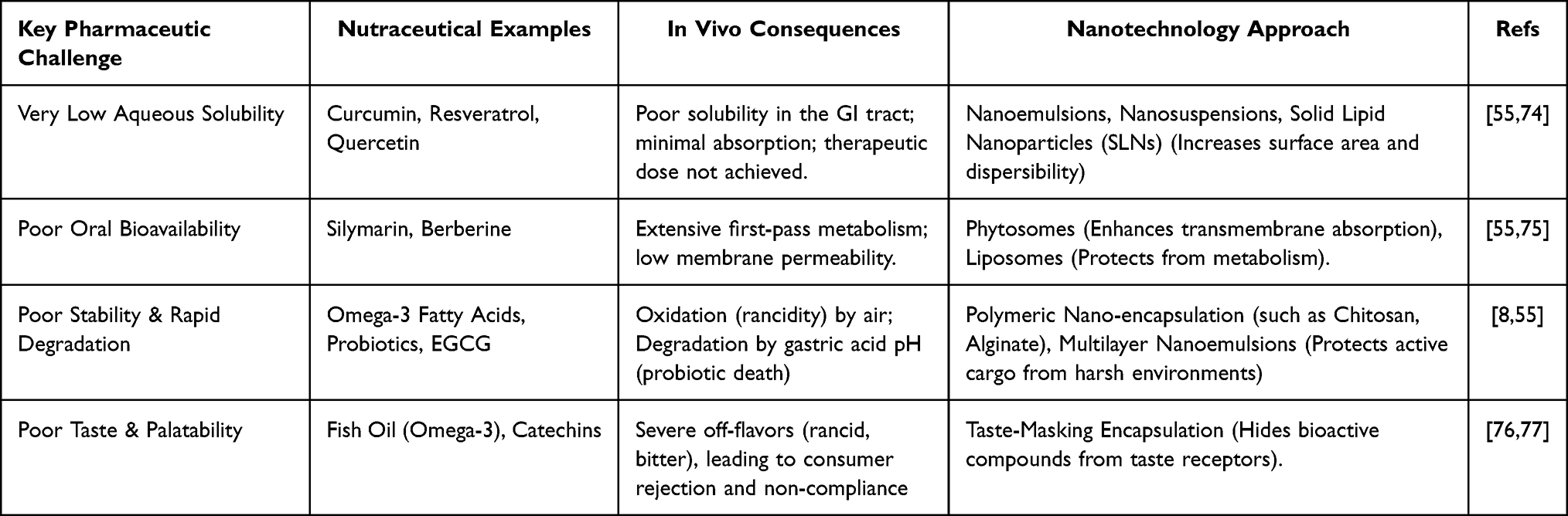 |
Table 2 Critical Comparison of Pharmaceutical Challenges and the Proposed Nanotechnology Approach |
In vivo Evidence for Nano-Nutritional Platforms in MASLD
The clinical potential of conventional nutraceutical interventions for MASLD is fundamentally limited by significant pharmaceutical challenges, primarily poor oral bioavailability and poor gastrointestinal stability. The development of nanotechnology-based delivery systems (NDS) aims to directly address these critical gaps.
Therefore, this chapter specifically presents and analyzes in vivo evidence from preclinical studies. The focus will shift from theoretical discussions of nanoplatforms to specific data demonstrating how nanonutrient formulations quantitatively improve pharmacokinetic parameters and, importantly, produce superior therapeutic efficacy in MASLD models.
Lipid-Based Systems
Lipid-based platforms are the most common and commercially available to address the solubility and bioavailability challenges inherent in lipophilic nutraceutical compounds. Nanoemulsions (NEs), for example, effectively dissolve lipophilic compounds such as curcumin or vitamins in nano-sized oil droplets (<200 nm). This drastically increases the surface area, water dispersibility, and ultimately, intestinal absorption.78 A detailed in vivo example can be seen in dihydromyricetin (DMY), a potent hepatoprotective flavonoid whose in vivo efficacy is limited by poor oral bioavailability.79 In a high-fat diet-induced MAFLD mouse model, this DMY-hNE formulation not only demonstrated significantly higher intestinal absorption, plasma concentration, and liver distribution compared to free DMY, but also clear therapeutic evidence: mice fed DMY-hNE showed significant reductions in hepatic fat accumulation (steatosis), lobular inflammation, and serum ALT/AST levels. The free DMY group, in contrast, showed virtually no effect.79 Similarly, nanoemulsions have been shown to be essential for Omega-3 Fatty Acids. In vivo studies in animal models of MASLD consistently demonstrated that omega-3 nanoemulsions suppress liver inflammatory markers (TNF-α, IL-6) and reduce steatosis more effectively than equivalent doses of conventional fish oil, while addressing oxidation and palatability issues.80
In addition to liquid nanoemulsions, liposomes and phytosomes offer another lipid-based platform. These phospholipid vesicles mimic biological cell membranes, enhancing membrane fusion and compound uptake. Silymarin is a classic example of a potent antifibrotic compound that failed clinically due to very poor bioavailability. When formulated as a phytosome (where silibinin is molecularly bound to a phospholipid), its bioavailability is dramatically improved. In an in vivo study in a mouse model of liver fibrosis, administration of silibinin phytosomes resulted in many-fold higher liver concentrations and a significantly stronger antifibrotic effect, as evidenced by reduced collagen deposition and HSCs activation, compared to standard silymarin.81
Polymer-Based Systems
Moving away from lipid systems, polymer-based platforms, often using food-grade biopolymers such as chitosan, alginate, or starch, excel in protecting fragile compounds from harsh environments and enabling controlled release.8,82
Curcumin, for example, can be formulated not only in nanoemulsions but also encapsulated in polymer nanoparticles (such as chitosan-based) to increase residence time in the intestinal mucosa. In vivo studies in mice treated with curcumin-chitosan nanoparticles demonstrated a more than 20-fold increase in plasma bioavailability compared to free curcumin.80 This pharmacokinetic improvement was directly correlated with greater reductions in hepatic oxidative stress (MDA) markers and improved liver histology in a MASLD model.
The argument for polymer encapsulation becomes even more compelling for highly fragile compounds such as probiotics. Although in vivo MASLD studies directly comparing nano- versus non-nano-based probiotics are still scarce, fundamental gastrointestinal transit studies have proven the principle. In animal models, probiotics nano-encapsulated in alginate/chitosan demonstrated thousands-fold higher survival rates after passage through simulated gastric fluid compared to free probiotics.74,81 This is crucial prerequisite evidence, indicating that encapsulation is a crucial step to ensure that a viable therapeutic dose reaches the gut.
Nutritional Inorganic Nanoparticles
Finally, there is a distinct category where the nanomaterial itself is the active nutrient, not simply a carrier. Selenium (Se) is a prime example. Selenium is an essential cofactor for endogenous antioxidant enzymes (such as glutathione peroxidase).83 In vivo studies in MASLD mouse models have shown that selenium nanoparticles (SeNPs), often synthesized greenly using plant extracts, are more effective than conventional selenium (such as sodium selenite). SeNP administration demonstrated better restoration of hepatic glutathione peroxidase activity, more significant reductions in oxidative stress (MDA), and greater reductions in ALT/AST levels, often with less toxicity at equivalent doses. A key advantage of SeNPs is their lower systemic toxicity compared to other selenium compounds, even at effective doses, making them a promising candidate for safer therapeutic use in liver-targeted therapies.84
Advances in nanotechnology have enabled the optimization of nanoparticle fabrication, composition, morphology, and function for theranostic applications (therapeutic and diagnostic). Many synthetic nanoparticles, natural biomaterials, and bionic nanoparticles have shown particular potential in the diagnosis and treatment of MASH due to their unique properties and superior performance.85 As key mediators of liver fibrogenesis, HSCs are a key target for antifibrotic therapy. However, many drugs with potent in vitro activity show limited in vivo efficacy due to low target cell accumulation. Nanotechnology offers a solution to overcome these limitations. Inorganic NPs, such as selenium and zinc oxide, not only function as therapeutic agents and antioxidants but also improve insulin sensitivity.86
Mechanism Review: Nanoparticles as Metabolic Modulators in MASLD
Diagnosis of MASH remains a challenge, particularly in differentiating it from simple steatosis before it progresses to irreversible cirrhosis or HCC. The limitations of liver biopsy and conventional imaging have driven the development of nanoformulations for theranostic treatment of MASH. Examples include extracellular vesicle (EV)-based omics analysis and functional Fe3O4-based magnetic nanoparticles as magnetic resonance imaging (MRI) contrast agents.85
In the early stages of MASLD (steatosis), therapeutic strategies should focus on suppressing de novo lipogenesis and enhancing β-oxidation. Nanoparticle systems targeting SREBP-1c and PPAR-α have shown promising results: siRNA in chitosan nanoparticles reduced SREBP-1c expression by up to 70%, while omega-3 nanoemulsions increased PPAR-α and CPT1 oxidation by up to threefold. Other formulations, such as rosehip oil (REO) and flaxseed oil nanoemulsions, have also been used to enhance the stability and bioavailability of omega-3 fatty acids87,88 These approaches are effective in restoring lipid homeostasis, although further clinical verification is needed.
In addition to lipid metabolism, mitigating oxidative stress through nanoparticle-enhanced activation of the Nuclear factor erythroid-2 related factor 2 (Nrf2) pathway (such as using gold nanoparticles) is crucial for hepatocellular protection.
As MASLD progresses to MASH, inflammation and fibrogenesis become dominant features. Therapeutic strategies shift toward suppressing the NLRP3 inflammasome (to downregulate IL-1β) and targeting TGF-β signaling (to inhibit HSC activation). Mesoporous silica nanoparticles (MSNs) containing curcumin have demonstrated improved bioavailability and potent NLRP3 inhibition. Synergistic approaches, such as combining MSNs with curcumin with siRNA-TGFβ nanoparticles, offer a promising strategy for simultaneously targeting two key pathways in MASH pathogenesis.89
Theranostic approaches are crucial in this dynamic therapeutic transition, enabling the same system to be used for both diagnosis (such as biomarker monitoring) and therapy delivery. A detailed summary of various nanoplatforms targeting core mechanisms of MASLD is presented in Table 3.
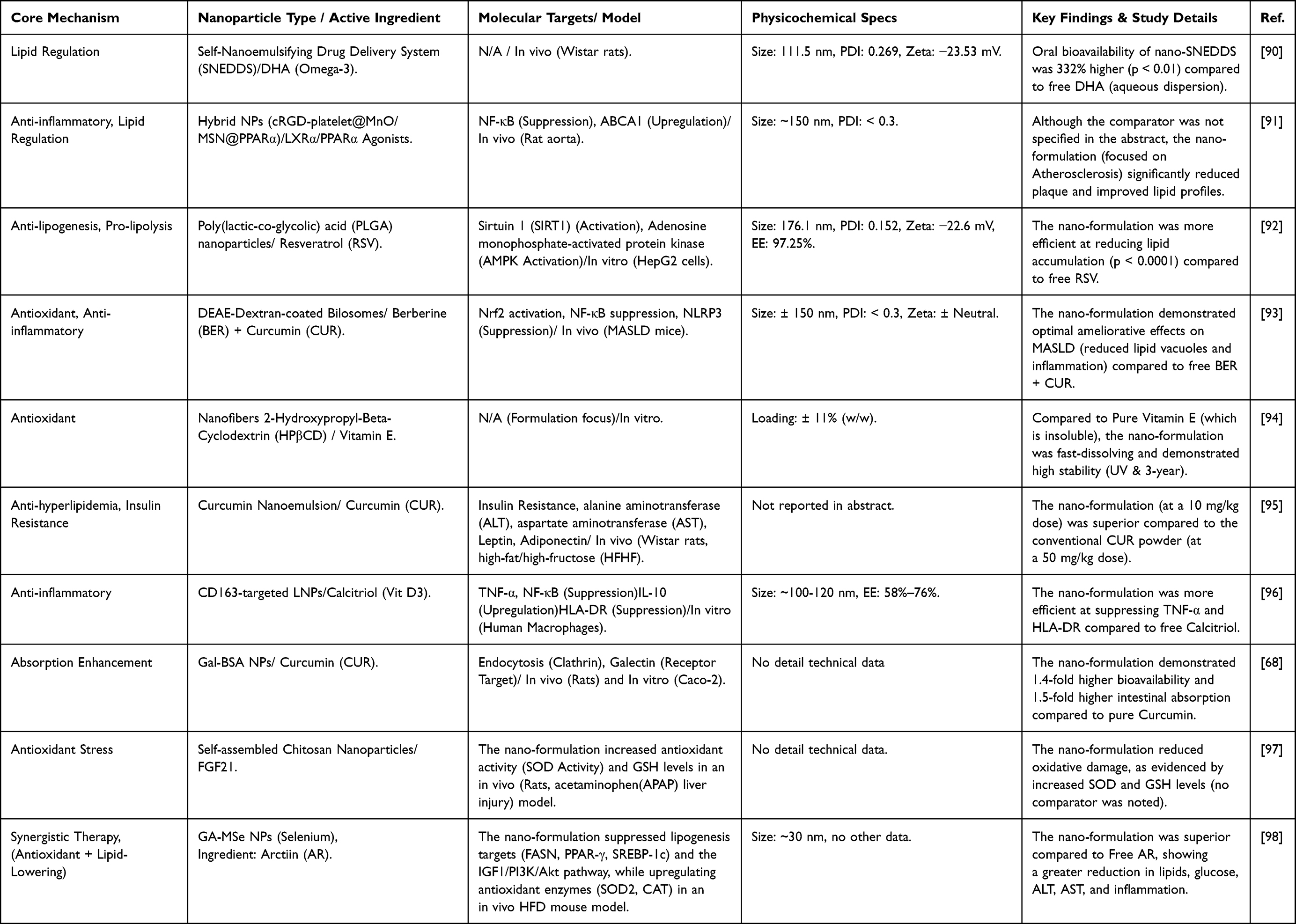 |
Table 3 Summary of the Reported Effects of Nanoparticles in MASLD Management |
A synthesis of this Table 3 confirms the main argument: the historical failure of nutraceuticals for MASLD was not a biological failure, but rather a formulation failure. These preclinical data consistently demonstrate how nanotechnology mechanistically overcomes fundamental pharmacokinetic and pharmaceutical barriers.
Formulations such as SNEDDS and albumin particles directly increase oral bioavailability (up to 332% for DHA), resulting in superior efficacy at much lower doses. Meanwhile, platforms such as nanofibers and PLGA solve fundamental solubility and stability issues, protecting active compounds from degradation (such as UV exposure and long-term storage).
More importantly, the field is moving beyond passive enhancement. We are seeing the emergence of “dual therapy” platforms, where the carrier itself is synergistic (such as selenium), and the use of active liver targeting via ligands such as galactose to target the Asialoglycoprotein Receptor (ASGPR) receptor. Collectively, these strategies directly address the multi-hit pathogenesis of MASLD, with data demonstrating simultaneous suppression of lipogenesis (SREBP-1c), inflammation (NF-κB), and oxidative stress (Nrf2).
However, these data also highlight two critical gaps. First, this remarkable preclinical success has not yet translated into clinical applications; the only identified human study is a protocol with no reported results.99 Second, nanotoxicity is a real risk, with evidence that some carriers (such as PAA-coated IONs) can induce oxidative stress and inflammation in the liver.100 This gap between robust preclinical data and scant clinical data, coupled with safety concerns, represents a major translational challenge the field must overcome.
Challenge Future Perspectives for Nutrition Delivery Systems
Despite the enormous potential of nanonutrient platforms demonstrated in in vivo studies, translation from the laboratory to the patient and to the marketplace faces significant challenges. This chapter will not only address the internal challenges facing NDS but also analyze how the evolving landscape of MASLD therapies will shape the future and role of NDS.
Internal Challenges in NDS Translation
The main challenges stem from within the NDS field itself, including clinical evidence, safety, and scalability.
The Clinical Translation Gap From Preclinical to Human
A major current challenge is the limited number of reliable randomized controlled clinical trials (RCTs) in humans.101 Although preclinical data demonstrate promising results, the success of future clinical applications depends heavily on validating that this increased in vivo bioavailability translates into significant clinical outcomes (eg, reduced fibrosis or improved validated NASH scores) in MASLD patients.
Safety & Nanotoxicity Challenges
Concerns about the long-term safety of nanomaterials (nanotoxicity) remain a major obstacle.102 It is important to distinguish between these types of materials:
- Most of the platforms discussed in this review (such as liposomes, nanoemulsions, phytosomes, chitosan, alginate) are made from materials that are inherently digestible, metabolizable, and GRAS (Generally Recognized as Safe). Food-Grade nanoparticles pose a lower risk.103
- Other materials sometimes studied (such as silver, titanium dioxide, or gold nanoparticles) raise concerns about potential bioaccumulation in organs such as the liver or spleen, as they are not readily metabolized by the body. Inorganic/metallic nanoparticles pose a higher risk.104
A unique challenge for nanonutrients (as opposed to nanomedicines) is that they are intended to be consumed daily over very long periods of time as part of the diet. Data on the toxicological effects of chronic, low-dose consumption of these nanomaterials is still lacking and is a crucial area of research for regulatory and public acceptance.
Production Scalability, Cost, and Stability of Food Matrices
Translating NDS formulations from laboratory batches (mg-scale) to industrial food production (ton-scale) presents significant technical and economic hurdles. Nanoformulations are significantly more expensive to produce than simple powdered extracts. Industry and consumers must be convinced that the increased cost is commensurate with the clinically proven increase in efficacy.105 Furthermore, the stability of NDS in complex food matrices (such as ensuring nanoemulsions do not separate or precipitate in yogurt or juice during shelf life) remains a significant food engineering challenge.
Shaping the Future of NDS in the MASLD Era
The internal challenges previously outlined are not merely theoretical; rather, they are a direct consequence of the substantial public and commercial demand for precision nutrition.106 The global market for nanotechnology-based nutraceuticals, for example, is projected to grow rapidly at a CAGR of over 9%, reflecting a clear societal trend toward preventative health solutions.15 This market push creates a crucial context for the future of NDS: it provides commercial incentives to address scalability and safety challenges, while also increasing the urgency to integrate NDS into the emerging of new MASLD therapies. The future of NDS will not occur in a vacuum. It will be directly shaped and driven by other breakthroughs in the MASLD field, creating both new challenges and opportunities.
New Nomenclature (MASLD/MetALD) as an NDS Opportunity
The shift in terminology from NAFLD to MASLD has significant implications. In particular, the introduction of the category MetALD (Steatotic Liver Disease Associated with Metabolic Dysfunction and Alcohol Consumption) is crucial. This category formally recognizes a very large patient population previously excluded from NASLD diagnosis and clinical trials: those with metabolic dysfunction (obesity, T2DM) but also moderate alcohol consumption (such as 20–50g/day for women, 30–60g/day for men). This MetALD group suffers from a “double-hit” of metabolic stress and alcohol toxicity.7,107 This creates a new niche and clinical need where potent hepatoprotective nutraceutical interventions, such as nano-silymarin or nano-antioxidants, are highly relevant as safe, supportive therapies for this underserved population.
Impact of New Pharmacotherapies on the Role of NDS
The approval of the first pharmacotherapies targeting MASH (such as Resmetirom) does not obsolete NDS; rather, it creates and clarifies a new niche for NDS. These drugs are often expensive, intended for MASH patients with significant fibrosis (stage F2/F3), and have potential side effects.108 This new landscape opens up at least two strategic roles for NDS:
- For the much larger population of patients with early-stage MASLD (simple steatosis) who are ineligible for aggressive pharmacotherapy, NDS serves as a lower-cost preventive intervention.109
- As adjunct therapy, anti-inflammatory or anti-oxidative NDS (nutrient delivery systems) can be used in conjunction with pharmaceutical drugs to manage liver stress, potentially improving outcomes or even reducing side effects.110
Convergence of NDS with Non-Invasive Diagnostics & AI
Currently, one of the biggest barriers to proving NDS efficacy is the need for invasive, expensive, and risky liver biopsies. Therefore, rapid developments in non-invasive biomarkers (from blood) and AI-based diagnostics (imaging, elastography) are crucial for the future of NDS.111 These diagnostic tools will enable NDS clinical trials to be cheaper, faster, larger, and more ethical. AI will not only diagnose MASLD but will also be an essential validation tool that can objectively monitor and prove that, for example, your nano-curcumin actually reduces steatosis or liver stiffness over time, providing the necessary evidence for regulatory approval.
Green Nanotechnology as a Path to Implementation
Given the challenges, such as cost, safety, and scalability, the most realistic future for NDS for mass nutritional applications likely lies not in exotic synthetic materials, but in green nanotechnology.112 This means focusing on the development of sustainable, low-cost, and GRAS-approved platforms derived from natural sources. These include biopolymers such as chitosan (from shrimp waste), alginate (from seaweed), zein (corn protein), and modified starch. These “food-grade” platforms represent the most likely bridge to bring nanonutrients from the laboratory to the supermarket shelf and ultimately to the patient.
Conclusion
Nutritional intervention remains the cornerstone of MASLD management, yet the clinical efficacy of key nutraceuticals (such as curcumin and silymarin) has historically been hampered by poor oral bioavailability. This critical review concludes that nanotechnology-based delivery systems (NDS), specifically nanoemulsions and phytosomes, offer a potent mechanistic solution to overcome this pharmacokinetic gap, translating into superior therapeutic efficacy in preclinical models. However, clinical translation faces significant hurdles regarding long-term safety data (nanotoxicity) and production scalability. Consequently, the future research agenda must prioritize: (1) the advancement of “green nanotechnology” utilizing safe, cost-effective “food-grade” (GRAS) materials, and (2) the integration of personalized therapeutic strategies that account for patient stratification to maximize clinical outcomes in this heterogeneous disease.
Data Sharing Statement
Data sharing not applicable – no new data generated, or the article describes entirely theoretical research.
Author Contributions
Yedi Herdiana: conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, resources, supervision, validation, visualization, writing – original draft, writing – review & editing. The author gave final approval of the version to be published; has agreed on the journal to which the article has been submitted; and agrees to be accountable for all aspects of the work.
Acknowledgements
The author would like to thank the Padjadjaran University for Article Processing Charges (APC) funding.
Funding
No funding was received for the conduct of this study.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Padmanaban S, Baek J-W, Chamarthy SS, et al. Nanoparticle-based therapeutic strategies for chronic liver diseases: advances and insights. Liver Res. 2025;9:104–117. doi:10.1016/j.livres.2025.04.002
2. Chen L, Liu E, Zhao X, et al. Scutellaria baicalensis Georgi in metabolic-associated fatty liver disease treatment: research progress. Front Pharmacol. 2025;16:1–19.
3. Cheng WT, Pei S-Y, Wu J, et al. Cannabinoid-2 receptor depletion promotes non-alcoholic fatty liver disease in mice via disturbing gut microbiota and tryptophan metabolism. Acta Pharmacol Sin. 2025;46:1676–1691. doi:10.1038/s41401-025-01495-w
4. Thomas A, Thomas A. Managing nonalcoholic fatty liver disease through structured lifestyle modification interventions. Am J Lifestyle Med. 2025;15598276251346716. doi:10.1177/15598276251346717
5. Amorim R, Soares P, Chavarria D, et al. Decreasing the burden of non-alcoholic fatty liver disease: from therapeutic targets to drug discovery opportunities. Eur J Med Chem. 2024;277:116723. doi:10.1016/j.ejmech.2024.116723
6. Cebi M, Yilmaz Y. Immune system dysregulation in the pathogenesis of non-alcoholic steatohepatitis: unveiling the critical role of T and B lymphocytes. Front Immunol. 2024;15:1–15. doi:10.3389/fimmu.2024.1445634
7. He Y, Chen Y, Qian S, et al. Immunopathogenic mechanisms and immunoregulatory therapies in MASLD. Cell Mol Immunol. 2025;22:1159–1177. doi:10.1038/s41423-025-01307-5
8. Miah MS, Chy MWR, Ahmed T, et al. Emerging trends in nanotechnologies for vitamin delivery: innovation and future prospects. Nano Trends. 2025;10:100126. doi:10.1016/j.nwnano.2025.100126
9. Tiniakos DG, Anstee QM, Burt AD. 5 - Fatty Liver Disease. In: Burt AD, Ferrell LD, Hübscher SG, editors. Macsween’s Pathology of the Liver.
10. Jang HJ, Jang JK, Heo S, et al. A prospective comparison of two ultrasound attenuation imaging modes using different frequencies for assessing hepatic steatosis. Ultrason. 2025;44:202–211. doi:10.14366/usg.24223
11. Chopinet S, Lopez O, Brustlein S, et al. Comparing different methods for the diagnosis of liver steatosis: what are the best diagnostic tools? Diagnostics. 2024;14(20):2292. doi:10.3390/diagnostics14202292
12. Sun J, Jin X, Li Y. Current strategies for nonalcoholic fatty liver disease treatment. Int J Mol Med. 2024;54. doi:10.3892/ijmm.2024.5412
13. Nie Z, Xiao C, Wang Y, Li R, Zhao F. Heat shock proteins (HSPs) in non-alcoholic fatty liver disease (NAFLD): from molecular mechanisms to therapeutic avenues. Biomark Res. 2024;12:1–28. doi:10.1186/s40364-024-00664-z
14. Chang KC, Kuo F-C, Yang C-Y, et al. Non-alcoholic fatty liver disease risk with GLP-1 receptor agonists and SGLT-2 inhibitors in type 2 diabetes: a nationwide nested case-control study. Cardiovasc Diabetol. 2024;23:367. doi:10.1186/s12933-024-02461-2
15. Clemente-suárez VJ, Bustamante-sanchez A, Rubio-zarapuz A. Biomimetic strategies for nutraceutical delivery: advances in bionanomedicine for enhanced nutritional health. Biomimetics. 2025;10:1–43. doi:10.3390/biomimetics10070426
16. Vachher M, Kaur K, Marothia M, et al. Deciphering the role of dietary modifications and gut dysbiosis in non-alcoholic fatty liver disease. Hum Nutr Metab. 2025;40:200305. doi:10.1016/j.hnm.2025.200305
17. Mabuda TI, Sibuyi NRS, Fadaka AO, et al. Targeted therapeutic strategies as alternative and sustainable treatment options for obesity-induced steatohepatitis. Rev Endocr Metab Disord. 2025;26:955–971. doi:10.1007/s11154-025-09980-7
18. Chen L, Guillot A, Tacke F. Reviewing the function of macrophages in liver disease. Expert Rev Gastroenterol Hepatol. 2025;19:621–637. doi:10.1080/17474124.2025.2508963
19. Nurkolis F, Harbuwono DS, Taslim NA, et al. New insight on dietary strategies to increase insulin sensitivity and reduce diabetes prevalence: an expert perspective and recommendation. Discov Food. 2025;5:136.
20. Monserrat-Mesquida M, Bouzas C, García S, et al. Two-year mediterranean diet intervention improves hepatic health in MASLD patients. Foods. 2025;14:1–16. doi:10.3390/foods14101736
21. Zeng J, Beck M, Barouti AA, et al. Effects of different dietary patterns on glucose management in type 1 diabetes: a systematic review and meta-analysis of randomized controlled trials. eClinicalMedicine. 2025;83:103222. doi:10.1016/j.eclinm.2025.103222
22. Alabdul Razzak I, Fares A, Stine JG, Trivedi HD. The role of exercise in steatotic liver diseases: an updated perspective. Liver Int. 2025;45:1–11. doi:10.1111/liv.16220
23. Qi F, Li T, Deng Q, Fan A. The impact of aerobic and anaerobic exercise interventions on the management and outcomes of non-alcoholic fatty liver disease. Physiol Res. 2024;73:671–686. doi:10.33549/physiolres.935244
24. Shi J, Cui J, Zheng T, et al. Comparative effects of aerobic and resistance exercise on bile acid profiles and liver function in patients with non-alcoholic fatty liver disease. BMC Gastroenterol. 2025;25. doi:10.1186/s12876-025-03826-x
25. Kumar R, Rani M, Kumar V, et al. Effectiveness of mobile health intervention for non alcoholic fatty liver disease- A meta analysis of randomized controlled trials. Clin Res Hepatol Gastroenterol. 2024;48:102433. doi:10.1016/j.clinre.2024.102433
26. Salmanizadeh F, Sabzevari S, Shafieipour S, Zahedi MJ, Sarafinejad A. Challenges and needs in the management of non-alcoholic fatty liver disease from the perspective of gastroenterology and hepatology specialists: a qualitative study. BMC Gastroenterol. 2025;25. doi:10.1186/s12876-025-03921-z
27. Romero-Gómez M, Zelber-Sagi S, Trenell M. Treatment of NAFLD with diet, physical activity and exercise. J Hepatol. 2017;67:829. doi:10.1016/j.jhep.2017.05.016
28. Iahtisham-Ul-Haq, Nadeem M, Sharma A, et al. Beyond medication: unveiling the role of diet and lifestyle in fatty liver disease management. Hum Nutr Metab. 2025;40:200317. doi:10.1016/j.hnm.2025.200317
29. Pu L, Pu C, Zhang X. Association of behavioral factors, liver function and NAFLD: bayesian Mendelian randomization. Nutr Metab. 2025;22:63. doi:10.1186/s12986-025-00961-w
30. Deng Q, Lv R, Zou H, Zou T. Beneficial effects of intermittent fasting on nonalcoholic fatty liver disease: a narrative review. Egypt Liver J. 2024;14. doi:10.1186/s43066-024-00368-x
31. Khalafi M, Rosenkranz SK, Ghasemi F, et al. Efficacy of intermittent fasting on improving liver function in individuals with metabolic disorders: a systematic review and meta-analysis. Nutr Metab. 2025;22:1–15. doi:10.1186/s12986-024-00885-x
32. Sabench F, Rusu EC, Clavero-Mestres H, et al. Metabolic-associated fatty liver disease and weight loss after bariatric surgery: a systematic review and meta-analysis. Obes Surg. 2024;34:4459–4471. doi:10.1007/s11695-024-07585-8
33. Seyedi A, Rabizadeh S, Reyhan SK, et al. Impact of bariatric surgery on liver fibrosis indices among type 2 diabetes patients in a national cohort. Sci Rep. 2025;15:1–10. doi:10.1038/s41598-025-85427-y
34. Tasabehji D, Saleh S, Mokadem M. Impact of bariatric surgery and endoscopic therapies on liver health in metabolic dysfunction-associated steatotic liver disease: a review. J Clin Med. 2025;14:1–25. doi:10.3390/jcm14124012
35. Wayal V, Wang S-D, Hsieh -C-C. Novel bioactive peptides alleviate Western diet-induced MAFLD in C57BL/6J mice by inhibiting NLRP3 inflammasome activation and pyroptosis via TLR4/NF-κB and Keap1/Nrf2/HO-1 signaling pathways. Int Immunopharmacol. 2025;148:114177. doi:10.1016/j.intimp.2025.114177
36. Dang J, Cai T, Tuo Y, et al. Corn peptides alleviate nonalcoholic fatty liver fibrosis in mice by inhibiting NLRP3 inflammasome activation and regulating gut microbiota. J Agric Food Chem. 2024;72:19378–19394. doi:10.1021/acs.jafc.4c04232
37. Wang Y, Tian X, Wang Z, et al. A novel peptide encoded by circ-SLC9A6 promotes lipid dyshomeostasis through the regulation of H4K16ac-mediated CD36 transcription in NAFLD. Clin Transl Med. 2024;14:e1801. doi:10.1002/ctm2.1801
38. Służały P, Paśko P, Galanty A. Natural products as hepatoprotective Agents-A comprehensive review of clinical trials. Plants. 2024;13:1985. doi:10.3390/plants13141985
39. Pezzino S, Sofia M, Mazzone C, et al. Innovative treatments for obesity and NAFLD: a bibliometric study on antioxidants, herbs, phytochemicals, and natural compounds. Heliyon. 2024;10:e35498. doi:10.1016/j.heliyon.2024.e35498
40. Chaudhary N, Arif M, Shafi S, Kushwaha SP, Soni P. Emerging role of natural bioactive compounds in navigating the future of liver disease. iLIVER. 2025;4:100140. doi:10.1016/j.iliver.2024.100140
41. Eid AH, Khachab M, Kobeissy F, Sahebkar A. Pharmacotherapeutic perspectives on nutraceuticals in the treatment of MASLD and MASH. Therapeut Adv Chronic Dis. 2025;16:20406223251339388at. doi:10.1177/20406223251339388
42. Vrentzos E, Pavlidis G, Korakas E, et al. Nutraceutical strategies for metabolic dysfunction-associated steatotic liver disease (MASLD): A path to liver health. Nutrients. 2025;17:1657. doi:10.3390/nu17101657
43. Pan Y, Yang Y, Wu J, Zhou H, Yang C. Efficacy of probiotics, prebiotics, and synbiotics on liver enzymes, lipid profiles, and inflammation in patients with non-alcoholic fatty liver disease: a systematic review and meta-analysis of randomized controlled trials. BMC Gastroenterol. 2024;24. doi:10.1186/s12876-024-03356-y
44. Abd El Hamid AA, Mohamed AE, Mohamed MS, et al. The effect of probiotic supplementation on non-alcoholic fatty liver disease (NAFLD) fibrosis score in patients attending a tertiary hospital clinic in Cairo. Egypt BMC Gastroenterol. 2024;24:354.
45. Havranek B, Loh R, Torre B, Redfield R, Halegoua-DeMarzio D. Glucagon-like peptide-1 receptor agonists improve metabolic dysfunction-associated steatotic liver disease outcomes. Sci Rep. 2025;15:1–11. doi:10.1038/s41598-025-89408-z
46. Harrison SA, Bedossa P, Guy CD, et al. A phase 3, randomized, controlled trial of resmetirom in NASH with liver fibrosis. N Engl J Med. 2024;390:497–509. doi:10.1056/NEJMoa2309000
47. Wang Z, Du H, Zhao Y, et al. Response to pioglitazone in non-alcoholic fatty liver disease patients with vs. without type 2 diabetes: a meta-analysis of randomized controlled trials. Front Endocrinol. 2023:1–11. doi:10.3389/fendo.2023.1111430
48. Zhao JM, Li BM, Zhang KM, Zhu ZM. The effect and safety of obeticholic acid for patients with nonalcoholic steatohepatitis: a systematic review and meta-analysis of randomized controlled trials. Medicine. 2024;7:1–7.
49. Macaire A, Lopez CO, Pajimna JAT, Mendhe D, Zeeshan S, Ahmed Z. Efficacy of sodium glucose cotransporter 2 inhibitors on hepatic fibrosis and steatosis in non ‑ alcoholic fatty liver disease: an updated systematic review and meta ‑ analysis. Sci Rep. 2024;14:1–18. doi:10.1038/s41598-024-52603-5
50. Anstee QM, Neuschwander-Tetri BA, Wai-Sun Wong V, et al. Cenicriviroc lacked efficacy to treat liver fibrosis in nonalcoholic steatohepatitis: Aurora Phase III randomized study. Clin Gastroenterol Hepatol. 2024;22:124–134.e1. doi:10.1016/j.cgh.2023.04.003
51. Boutari C, Pappas PD, Anastasilakis D, Mantzoros CS. Statins’ efficacy in non-alcoholic fatty liver disease: a systematic review and meta-analysis. Clin Nutr. 2022;41:2195–2206. doi:10.1016/j.clnu.2022.08.001
52. Tessier CM, Polyzos SA, Athyros VG, Mantzoros CS. Long-term statin treatment for hepatic fibrosis in patients with nonalcoholic fatty liver disease: is it time to give the emperor a statin robe? Metabolism. 2021;121:154796. doi:10.1016/j.metabol.2021.154796
53. Ferré P, Phan F, Foufelle F. SREBP-1c and lipogenesis in the liver: an update. Biochem J. 2021;478:3723–3739. doi:10.1042/BCJ20210071
54. Ranneh Y, Bedir AS, Abu-Elsaoud AM, Al Raish S. Polyphenol intervention ameliorates non-alcoholic fatty liver disease: an updated comprehensive systematic review. Nutr. 2024;16:1–17.
55. Zhuo Y, Zhao YG, Zhang Y. Enhancing drug solubility, bioavailability, and targeted therapeutic applications through magnetic nanoparticles. Molecules. 2024;29:1–35. doi:10.3390/molecules29204854
56. Mejía-Guzmán JE, Belmont-Hernández RA, Chávez-Tapia NC, Uribe M, Nuño-Lámbarri N. Metabolic-dysfunction-associated steatotic liver disease: molecular mechanisms, clinical implications, and emerging therapeutic strategies. Int J Mol Sci. 2025;26:1–42. doi:10.3390/ijms26072959
57. Hegazi OE, Alalalmeh SO, Alnuaimi GRH, et al. NAFLD and nutraceuticals: a review of completed phase III and IV clinical trials. Front Med. 2023;10. doi:10.3389/fmed.2023.1227046
58. Taru V, Szabo G, Mehal W, Reiberger T. Inflammasomes in chronic liver disease: hepatic injury, fibrosis progression and systemic inflammation. J Hepatol. 2024;81:895–910. doi:10.1016/j.jhep.2024.06.016
59. Jee Y-M, Lee J-Y, Ryu T. Chronic inflammation and immune dysregulation in metabolic-dysfunction-associated steatotic liver disease progression: from steatosis to hepatocellular carcinoma. Biomedicines. 2025;13:1260. doi:10.3390/biomedicines13051260
60. Zeng X, Huang D, Zhu Z, et al. Mechanism-guided drug development and treatment for liver fibrosis: a clinical perspective. Front Pharmacol. 2025;16. doi:10.3389/fphar.2025.1574385
61. Singh S, Kriti M, Catanzaro R, et al. Deciphering the gut–liver axis: a comprehensive scientific review of non-alcoholic fatty liver disease. Livers. 2024;4:435–454. doi:10.3390/livers4030032
62. Agyapong G, Dashti F, Banini BA. Nonalcoholic liver disease: epidemiology, risk factors, natural history, and management strategies. Ann N Y Acad Sci. 2023;1526:16–29. doi:10.1111/nyas.15012
63. Shen Y, Fan N, Ma S-X, et al. Gut microbiota dysbiosis: pathogenesis, diseases, prevention, and therapy. MedComm. 2025;6:e70168. doi:10.1002/mco2.70168
64. Han D, Wang W, Gong J, Ma Y, Li Y. Microbiota metabolites in bone: shaping health and Confronting disease. Heliyon. 2024;10:1–23.
65. Han S, Lu Y, Xie J, et al. Probiotic gastrointestinal transit and colonization after oral administration: a long journey. Front Cell Infect Microbiol. 2021;11:609722. doi:10.3389/fcimb.2021.609722
66. Luo X, Wang K, Jiang C. Gut microbial enzymes and metabolic dysfunction-associated steatohepatitis: function, mechanism, and therapeutic prospects. Cell Host Microbe. 2025;33:836–853. doi:10.1016/j.chom.2025.04.020
67. Herdiana Y. Nanoparticles of natural product-derived medicines: beyond the pandemic. Heliyon. 2025;11:e42739. doi:10.1016/j.heliyon.2025.e42739
68. Huang Y, Deng S, Luo X, et al. Evaluation of intestinal absorption mechanism and pharmacokinetics of curcumin-loaded galactosylated albumin nanoparticles. Int J Nanomed. 2019;14:9721–9730.
69. Roney M, Huq AKMM, Rullah K, Zamri NB, Mohd Aluwi MFF. Curcumin, a bioactive compound of Turmeric (Curcuma longa) and its derivatives as α-amylase and α-glucosidase inhibitors. Cell Biochem Biophys. 2025;83:53–71. doi:10.1007/s12013-024-01477-5
70. Baghcheghi Y, Razazpour F, Mirzaee F, et al. Exploring the molecular mechanisms of curcumin in modulating memory impairment in neurodegenerative disorders. Mol Biol Rep. 2024;52:45. doi:10.1007/s11033-024-10115-5
71. Den Hartogh DJ, Gabriel A, Tsiani E. Antidiabetic properties of Curcumin II: evidence from in vivo studies. Nutrients. 2019;12:58. doi:10.3390/nu12010058
72. Yu X, Jia Y, Ren F. Multidimensional biological activities of resveratrol and its prospects and challenges in the health field. Front Nutr. 2024;11:1–15. doi:10.3389/fnut.2024.1408651
73. Surai PF, Surai A, Earle-Payne K. Silymarin and inflammation: food for thoughts. Antioxidants. 2024;13:98. doi:10.3390/antiox13010098
74. Kamble MG, Singh A, Singh SV, et al. Nanotechnology for encapsulation of bioactive components: a review. Discov Food. 2025;5. doi:10.1007/s44187-025-00386-7
75. Yang Y, Wang X. Nano-drug delivery systems (NDDS) in metabolic dysfunction-associated steatotic liver disease (MASLD): current status, prospects and challenges. Front Pharmacol. 2024;15:1419384. doi:10.3389/fphar.2024.1419384
76. Siddiqui SA, Singh P, Utama DT, et al. Encapsulation of bioactive compounds in foods for diabetics - sources, encapsulation technologies, market trends and future perspectives – a systematic review. Food Bioprod Process. 2024;147:277–303. doi:10.1016/j.fbp.2024.07.007
77. Xu Y, Yan X, Zheng H, et al. The application of encapsulation technology in the food Industry: classifications, recent Advances, and perspectives. Food Chem. 2024;21:101240.
78. Rehman M, Tahir N, Sohail MF, et al. Lipid-based nanoformulations for drug delivery: an ongoing perspective. Pharmaceutics. 2024;16:1–34. doi:10.3390/pharmaceutics16111376
79. Li J, Yin M, Tian M, Fang J, Xu H. Stiff-soft hybrid biomimetic nano-emulsion for targeted liver delivery and treatment of early nonalcoholic fatty liver disease. Pharmaceutics. 2024;16:1303. doi:10.3390/pharmaceutics16101303
80. Shahrebabak MG, Shahabi Haghighi SP, Ravankhah M, et al. A systematic review and meta-analysis of randomised controlled trials on curcumin-piperine supplementation: a promising strategy for managing lipid profiles and liver health in non-alcoholic fatty liver disease. J Herbs Med. 2025;51:101006. doi:10.1016/j.hermed.2025.101006
81. Rezagholizade-shirvan A, Soltani M, Shokri S, et al. Bioactive compound encapsulation: characteristics, applications in food systems, and implications for human health. Food Chem. 2024;24:101953.
82. Gao F, Feng X, Li X. Recent advances in polymeric nanoparticles for the treatment of hepatic diseases. Front Pharmacol. 2025;16:1–17.
83. Karunakar KK, Cheriyan BV, Babu D, et al. Selenium, silver, and gold nanoparticles: emerging strategies for hepatic oxidative stress and inflammation reduction. Nano TransMed. 2025;4:100085. doi:10.1016/j.ntm.2025.100085
84. Zou S, Gong Y, Li X, et al. Functionalized selenium nanoparticles ameliorated Acetaminophen-induced hepatotoxicity through synergistically triggering PKCδ/Nrf2 signaling pathway and inhibiting CYP 2E1. Food Sci Hum Wellness. 2024;13:932–945. doi:10.26599/FSHW.2022.9250080
85. Qin X, Liu J. Nanoformulations for the diagnosis and treatment of metabolic dysfunction-associated steatohepatitis. Acta Biomater. 2024;184:37–53. doi:10.1016/j.actbio.2024.06.014
86. Yu W, Zhang Y, Lu Y, et al. Recent research on the bioactivity of polyphenols derived from edible fungi and their potential in chronic disease prevention. J Funct Foods. 2025;124:106627. doi:10.1016/j.jff.2024.106627
87. Rao S, Radhakrishnan P, Valiathan S, M S. Rosehip oil nanoemulsion as a stable delivery system for omega-3 fatty acids to enhance the nutritional value of yogurt. Food Chem Adv. 2023;3:100545. doi:10.1016/j.focha.2023.100545
88. Almasi K, Esnaashari SS, Khosravani M, Adabi M. Yogurt fortified with omega-3 using nanoemulsion containing flaxseed oil: investigation of physicochemical properties. Food Sci Nutr. 2021;9:6186–6193. doi:10.1002/fsn3.2571
89. Fischer T, Winter I, Drumm R, Schneider M. Cylindrical microparticles composed of mesoporous silica nanoparticles for the targeted delivery of a small molecule and a macromolecular drug to the lungs: exemplified with curcumin and siRNA. Pharmaceutics. 2021;13:844. doi:10.3390/pharmaceutics13060844
90. Alhakamy NA, Aldawsari HM, Hosny KM, et al. Formulation design and pharmacokinetic evaluation of docosahexaenoic acid containing self-nanoemulsifying drug delivery system for oral administration. Nanomater Nanotechnol. 2020;10:184798042095098. doi:10.1177/1847980420950988
91. Lv Z, Zhang Y, Lu M, et al. cRGD-platelet@MnO/MSN@PPARα/LXRα nanoparticles improve atherosclerosis in rats by inhibiting inflammation and reducing blood lipid. Curr Pharm Biotechnol. 2025;26:740–753. doi:10.2174/0113892010314993240819065655
92. Wan S, Zhang L, Quan Y, Wei K. Resveratrol-loaded PLGA nanoparticles: enhanced stability, solubility and bioactivity of resveratrol for non-alcoholic fatty liver disease therapy. R Soc Open Sci. 2018;5:181457. doi:10.1098/rsos.181457
93. Chen Y, Jiang Z, Xu J, et al. Improving the ameliorative effects of berberine and curcumin combination via dextran-coated bilosomes on non-alcohol fatty liver disease in mice. J Nanobiotechnol. 2021;19:230. doi:10.1186/s12951-021-00979-1
94. Celebioglu A, Uyar T. Antioxidant Vitamin E/Cyclodextrin inclusion complex electrospun nanofibers: enhanced water solubility, prolonged shelf life, and photostability of Vitamin E. J Agric Food Chem. 2017;65:5404–5412. doi:10.1021/acs.jafc.7b01562
95. Elbaset MA, Nasr M, Ibrahim BMM, et al. Curcumin nanoemulsion counteracts hepatic and cardiac complications associated with high-fat/high-fructose diet in rats. J Food Biochem. 2022;46:e14442. doi:10.1111/jfbc.14442
96. Rafique A, Etzerodt A, Graversen JH, et al. Targeted lipid nanoparticle delivery of calcitriol to human monocyte-derived macrophages in vitro and in vivo: investigation of the anti-inflammatory effects of calcitriol. Int J Nanomed. 2019;14:2829–2846. doi:10.2147/IJN.S192113
97. Cui X, Sun Q, Wang H. Targeting fibroblast growth factor (FGF)-21: a promising strategy for metabolic dysfunction-associated steatotic liver disease treatment. Front Pharmacol. 2025;16:1510322. doi:10.3389/fphar.2025.1510322
98. Lei S, Wu Q, Zhang B, et al. Liver-targeting nanoparticles GA-MSe@AR treat NAFLD through dual lipid-lowering and antioxidant efficacy. Int J Nanomed. 2025;20:5017–5037. doi:10.2147/IJN.S510577
99. Jazayeri-Tehrani SA, Rezayat SM, Mansouri S, et al. Efficacy of nanocurcumin supplementation on insulin resistance, lipids, inflammatory factors and nesfatin among obese patients with non-alcoholic fatty liver disease (NAFLD): a trial protocol. BMJ Open. 2017;7:e016914. doi:10.1136/bmjopen-2017-016914
100. Couto D, Freitas M, Costa VM, et al. Biodistribution of polyacrylic acid-coated iron oxide nanoparticles is associated with proinflammatory activation and liver toxicity. J Appl Toxicol. 2016;36:1321–1331. doi:10.1002/jat.3323
101. Teja PK, Mithiya J, Kate AS, Bairwa K, Chauthe SK. Herbal nanomedicines: recent advancements, challenges, opportunities and regulatory overview. Phytomedicine. 2022;96:153890. doi:10.1016/j.phymed.2021.153890
102. Herdiana Y, Wathoni N, Shamsuddin S, Muchtaridi M. Scale-up polymeric-based nanoparticles drug delivery systems: development and challenges. OpenNano. 2022;7:100048. doi:10.1016/j.onano.2022.100048
103. Wathoni N, Herdiana Y, Suhandi C, Mohammed A, El-Rayyes A, Narsa A. Chitosan / alginate-based nanoparticles for antibacterial agents delivery. Int J Nanomed. 2024;Volume 19:5021–5044. doi:10.2147/IJN.S469572
104. Shang J, Yan J, Lou H, et al. Oral exposure to food-grade nanoparticles poses a risk of alzheimer’s disease-like symptoms by triggering autophagy defects in neurons. Adv Sci. 2025;08096:1–17.
105. Hua S, Wu SY. Editorial: advances and challenges in nanomedicine. Front Pharmacol. 2018;9:1–3. doi:10.3389/fphar.2018.01397
106. Donovan SM, Abrahams M, Anthony JC, et al. Perspective: challenges for personalized nutrition in the current united states regulatory framework and future opportunities. Adv Nutr. 2025;16:100382. doi:10.1016/j.advnut.2025.100382
107. Dunn N, Al-Khouri N, Abdellatif I, Singal AK. Metabolic dysfunction and alcohol-associated liver disease: a narrative review. Clin Transl Gastroenterol. 2025;16:1–8. doi:10.14309/ctg.0000000000000828
108. Le P, Dasarathy S, Herman WH, et al. Value-based pricing of resmetirom for metabolic dysfunction-associated steatotic liver disease. JAMA Network Open. 2025;8:1–13. doi:10.1001/jamanetworkopen.2025.17122
109. Tacke F, Weiskirchen R. Non-alcoholic fatty liver disease (NAFLD)/non-alcoholic steatohepatitis (NASH)-related liver fibrosis: mechanisms, treatment and prevention. Ann Transl Med. 2021;9:729. doi:10.21037/atm-20-4354
110. Charlton M. Insights into combination therapy for metabolic dysfunction-associated steatohepatitis. Gastroenterol Hepatol. 2024;20:611–613.
111. Zou H, Pan W, Sun X. Assessment of the diagnostic efficacy of five non-invasive tests for MASLD: external validation utilizing data from two cohorts. Front Nutr. 2025;12:1–11. doi:10.3389/fnut.2025.1571487
112. El-Saadony MT, Saad AM, Sitohy M, et al. Chitosan nanoparticles: green synthesis, biological activities, and sustainable frontiers in targeted drug delivery and cancer nanomedicine – a comprehensive review. Mater Today Bio. 2025;35:102358. doi:10.1016/j.mtbio.2025.102358
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.