Back to Journals » International Journal of General Medicine » Volume 13
Myotoxic Mushroom Poisoning in Thailand: Clinical Characteristics and Outcomes
Authors Trakulsrichai S ![]() , Jeeratheepatanont P, Sriapha C
, Jeeratheepatanont P, Sriapha C ![]() , Tongpoo A, Wananukul W
, Tongpoo A, Wananukul W
Received 12 July 2020
Accepted for publication 4 September 2020
Published 17 November 2020 Volume 2020:13 Pages 1139—1146
DOI https://doi.org/10.2147/IJGM.S271914
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Satariya Trakulsrichai,1,2 Peerawich Jeeratheepatanont,1 Charuwan Sriapha,2 Achara Tongpoo,2 Winai Wananukul2,3
1Department of Emergency Medicine, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok 10400, Thailand; 2Ramathibodi Poison Center, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok 10400, Thailand; 3Department of Medicine, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok 10400, Thailand
Correspondence: Satariya Trakulsrichai
Department of Emergency Medicine, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok 10400, Thailand
Tel +66-2-2011484
Fax +66-2-2012404
Email [email protected]
Purpose: To describe the clinical characteristics and outcomes of myotoxic mushroom poisoning in Thailand.
Patients and Methods: We performed a retrospective cohort study of cases of myotoxic mushroom poisoning from the Ramathibodi Poison Center Toxic Exposure Surveillance System during a 5-year period (2012– 2016).
Results: Forty-one cases were included. Most (53.7%) were male with the average age of 49 years. In three cases, the mushrooms were identified as Russula species by an experienced mycologist. Common presenting symptoms were gastrointestinal (GI) symptoms and myalgia. The median onset of GI symptoms and symptoms suggesting rhabdomyolysis after consuming mushrooms was 2 hours (0.17– 24 hours) and 24– 48 hours (2– 120 hours), respectively. Eight patients who ate the mushrooms together with other patients with rhabdomyolysis had GI symptoms but did not develop rhabdomyolysis. For patients with rhabdomyolysis, acute kidney injury (AKI) and hyperkalaemia occurred in 51.5% and 33.3% of cases, respectively. Median initial and maximum creatine phosphokinase (CPK) levels in patients with rhabdomyolysis were 31,145 and 47,861 U/L, respectively. Fifteen of 17 patients who were investigated for troponin levels had elevated troponin. Three patients had a low ejection fraction. Most patients (95.1%) were admitted to hospital, with a median stay of 5 days. The mortality rate was 26.8%. Treatments included intravenous fluid, urine alkalinization, haemodialysis and peritoneal dialysis. Among patients with rhabdomyolysis, AKI, hyperkalaemia during hospitalisation, maximum CPK level, maximum creatinine level and initial and maximum potassium levels were the factors found to be significantly different between patients who died and those who survived.
Conclusion: Myotoxic mushroom poisoning had a high mortality rate. Most patients had early or delayed onset of clinical symptoms after mushroom ingestion. Some patients developed severe cardiovascular effects. Early detection, close monitoring (especially serum potassium, creatinine, CPK and cardiac effect) and good supportive care were the main treatment modalities.
Keywords: mushroom poisoning, rhabdomyolysis, cardiovascular effects, deaths, Russula species
Introduction
Mushroom poisoning is among the common food poisoning and environmental emergencies. It is a health problem in many countries, resulting in morbidity and mortality.1–3 The incidence of mushroom poisoning varies over the world, depending on many factors such as local culture and traditions, climate and the availability of wild mushrooms.1 Foraging for and consuming wild mushrooms has led to an increasing incidence of mushroom poisoning.
Foraging wild mushrooms might be considered as a recreational activity or food resources. Foraging for and eating wild mushrooms are local tradition in some countries. One study shows that the population of different regions in Europe were different in their consumption behaviour of wild mushrooms.4 Mushroom poisoning presents with a wide clinical spectrum, extending from mild to life-threatening severity.2,3 The clinical effects of mushroom poisoning depend on the species and the amount ingested. Toxin-specific manifestations of mushroom poisoning are usually classified into groups based mainly on symptomatology and clinical effects.2,3 Most fatalities are due to amatoxin-containing species, which cause hepatotoxicity and fulminant liver failure.2,3,5–7
Rhabdomyolysis is a syndrome of mushroom poisoning that is described as either rapid or delayed onset myotoxicity.2,3 Mushroom poisoning with delayed onset myotoxicity reported in literature is associated with ingestion of selected Tricholoma species, including T. equestre,2,8–12 and possibly T. terreum.2,13
However, some experts discuss and debate whether T. equestre is a toxic species.14,15 One study in humans did not find evidence of T. equestre toxicity and support that T. equestre is edible if ingested in reasonable amounts by healthy people.15
Mushroom poisoning with rapid onset myotoxicity is associated with ingestion of selected Russula species, including R. subnigricans2,16–18 or Russula subnigricans Hongo. The causative toxin has been reported as a highly strained carboxylic acid, cycloprop-2-ene carboxylic acid.2,19
Rhabdomyolysis is destruction of skeletal muscle resulting in injury to myocytes and their membranes.20 Clinically, myotoxic mushroom-poisoned patients typically present with fatigue, myalgia, muscle weakness and dark urine representing rhabdomyolysis, with or without obvious gastrointestinal (GI) symptoms.8–11,16–18 Some patients with severe illness develop acute renal failure, electrolyte disturbances (hyperkalaemia, hypocalcaemia), respiratory failure, acute myocarditis, cardiac arrhythmias, pulmonary oedema, cardiac failure or cardiovascular collapse.8,11,16–18 Fatalities have been reported from myotoxic mushroom poisoning.8,10–12,17
In some areas of Thailand, foraging for and consuming wild mushrooms are also popular, contributing to the incidence of mushroom poisoning in our country.7 Besides amatoxin poisoning, myotoxic mushroom poisoning has significant or severe clinical effects.21 Clinical data for myotoxic mushroom poisoning are limited. This study was undertaken to ascertain the clinical characteristics, outcome and factors associated with death in myotoxic mushroom poisoning for 5 years (2012–2016).
Patients and Methods
We performed a 5-year retrospective cohort study (January 2012 to December 2016) using data from the Ramathibodi Poison Center (RPC) Toxic Exposure Surveillance System, the database of our poison center. The primary outcomes were the clinical characteristics and outcomes of patients with ingestion of myotoxic mushrooms. The secondary outcome was factors associated with mortality in patients with rhabdomyolysis.
The setting of the study was the poison center of a tertiary teaching hospital. Ramathibodi Poison Center (RPC) responds to the consultations via telephones and provides toxicological information for both healthcare professionals and the general public 24 hours a day, every day of the year. Most telephone calls to the RPC are from medical personnel from every region in Thailand. There are typically 15,000–25,000 calls per year. Follow-up calls by RPC information scientists are periodically made to collect and monitor case progress, to provide ongoing treatment recommendations, and to determine the medical outcomes of cases. All data of cases are recorded in the RPC Toxic Surveillance System database (the database of RPC) and are verified by a team of information scientists and medical toxicologists.
For the inclusion criteria, we included all patients with rhabdomyolysis associated with ingestion of mushrooms who were referred and consulted to the RPC. Other patients who had ingested mushrooms together with the patients who developed rhabdomyolysis, and visited hospitals due to abnormal symptoms, were also included in our study; these patients were also defined as a poisoning group. The diagnosis of myotoxic mushroom poisoning was based on clinical data, including a history of mushroom ingestion and development of rhabdomyolysis after ingestion of mushrooms without other explainable causes. Patients who had coingested mushrooms together with pesticides, illicit drugs, known drugs that can cause or induce rhabdomyolysis (such as statins) or overdose of medications at the presentation, were excluded from the study.
We collected data from patients who met the inclusion criteria on demography, medical history, clinical features, laboratory results, treatment modalities, follow-up details, final diagnosis and outcome. Rhabdomyolysis was defined as creatine phosphokinase (CPK) >1000 U/L.20 Hyperkalaemia was defined as serum potassium >5 mmol/L.22 Acute kidney injury (AKI) was diagnosed based on clinical history and laboratory data using the Kidney Disease: Improving Global Outcomes (KDIGO) clinical practice guideline.23 We assumed that all patients without known underlying disease were healthy and previously had normal kidney function. Elevated levels of aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase, total bilirubin and cardiac enzyme were accepted if the patient’s laboratory results were more than the normal range of each hospital’s laboratory levels. Hypotension was defined as systolic blood pressure <90 mmHg.24 The seasons in Thailand are simply divided into three 4-month periods: rainy season (June–September), winter (October–January) and summer (February–May).25 We used PASW Statistics for Windows, Version 22 (SPSS, Chicago, IL, USA) to analyze the data. Means and standard deviations were used for continuous data with normal distribution; otherwise, medians with minimum and maximum were used. Frequencies and percentages were used for analysis of categorical data. Comparisons between groups were analyzed by Student’s t-test if two independent continuous data were normally distributed; otherwise, they were analyzed by the Mann–Whitney U-test. Differences in categorical variables were evaluated by chi-squared analysis and Fisher’s exact test. P-values less than 0.05 were considered to indicate statistical significance.
Results
Demographic Data
Forty-one poisoning cases from 24 consultations via telephone calls were included in the study. The mean age (±SD) of the patients was 49 (±16) years (range 15–79 years old), and twenty-two patients (22/41, 53.7%) were male. All 41 patients were Thai; twenty-two patients (53.7%) were from the north-east region, eighteen patients (43.9%) from the north region and one patient (2.4%) from the south region. All patients reported that they ate the mushrooms because they believed that those mushrooms were edible. Four patients reported that they coingested ethanol with mushrooms. Twenty-nine patients (70.7%) visited the hospital within 24 hours after eating the mushrooms. Twenty-eight patients (68.3%) presented to the hospital together with other family members or friends who had the same symptoms after consuming the mushrooms; these were considered together as poisoning groups. Four patients reported underlying diseases, which were one case each of HIV infection, type 2 diabetes, hypertension and chronic kidney disease with hypertension and atrial fibrillation. Eleven patients reported the mushrooms they ate as “charcoal mushrooms” which commonly refers to Russula species, 3 patients reported other names of mushrooms (in Thai names; Pai, Karbnang and Kalumma mushrooms) and 27 patients did not know the names of the mushrooms. Twenty-four patients (58.5%) had cooked the mushrooms; there were no data about cooking for other patients. The mushrooms that were brought to the hospital by a group of three patients were identified as Russula species by an experienced mycologist. These three patients also reported the name of the mushroom they ate as Russula species. No spore identification in gastric content was done in all patients. Clinical data, including the onset of GI symptoms, myalgia and abnormal dark urine after consuming mushrooms, are shown in Table 1. The time of onset of GI symptoms after consuming mushrooms was <6 hours, >6 hours and unknown in 13, 22 and 6 patients, respectively.
 |
Table 1 Clinical Characteristics of the Patients (41 Patients) |
Clinical Presentations
The presenting symptoms are summarised in Table 2. Thirty-seven patients (90.2%) presented with GI symptoms, including mucous bloody diarrhea in one poisoning group of three patients. One patient also presented with hiccough. At the first presentation, 11 patients (26.8%) had hypotension, 9 patients (22%) had tachycardia and 7 patients (17%) had a high temperature (≥37.8 C). Almost all patients (95.1%) were admitted to hospital, and the others were treated at outpatient clinics. Eight patients (range of age; 15–54 years old) who ate mushrooms together with other patients with rhabdomyolysis, all had GI symptoms after mushroom ingestion, but did not have rhabdomyolysis. Six from 8 patients were admitted in hospitals. One of these 8 patients had normal CPK level and the other 7 patients did not have results of CPK level noted in our data; however, they did not have symptoms of dark urine or myalgia during hospitalization. These 8 patients were concluded that they had only GI symptoms, but no rhabdomyolysis. Therefore, 80.5% of all patients developed rhabdomyolysis after mushroom ingestion. The clinical features of the patients with rhabdomyolysis during hospital stay are shown in Table 3, and laboratory results are shown in Table 4. A subset of patients underwent laboratory or imaging studies only once, at the first hospital visit or admission.
 |
Table 2 Presenting Symptoms of the Patients (41 Patients) |
 |
Table 3 Clinical Features of Patients with Rhabdomyolysis (33 Patients) During Hospitalisation |
 |
Table 4 Laboratory Findings for Patients with Rhabdomyolysis (33 Patients) |
One 23-year-old patient with underlying heart disease, who had the highest maximum levels of AST (6195 IU/L) and ALT (1926 IU/L) during hospitalisation, presented with dyspnoea and productive cough after eating wild mushrooms 3 days prior to visiting the hospital. At presentation, he had fever and developed shock. His AST, ALT, alkaline phosphatase (ALP), CPK and total bilirubin were 8066 IU/L, 4080 IU/L, 234 IU/L, 11,000 IU/L and 5.09 mg/dL, respectively. His liver function test suggested a hepatocellular pattern of liver injury. A coagulogram was not performed. He had AKI (creatinine 1.9 mg/dL) and cardiomegaly. He was diagnosed with wild mushroom poisoning, community acquired pneumonia and cardiogenic shock. After supportive care and treatment with N-acetylcysteine and antibiotics, he recovered with AST 592, ALT 1597 and CPK 956 IU/L and was discharged 4 days after admission.
The patient who had the second highest maximum AST and ALT during hospitalisation presented to the hospital along with two other patients; all three had rhabdomyolysis. The patient had initial AST, ALT and CPK levels of 124, 52 and 4510 U/L, respectively, and maximum AST, ALT and CPK levels of 6195, 1926 and 229,836 IU/L, respectively. His international normalised ratio (INR) was normal for the entire clinical course.
Among patients with rhabdomyolysis, almost all (32 patients) had both elevated maximum AST (range, 538–8066 IU/L) and ALT (range, 81–4080 IU/L). Two patients had a prothrombin time with INR > 1.5, one patient was taking warfarin and the other was diagnosed with disseminated intravascular coagulation (DIC). An abnormal chest X-ray was recorded in 13 patients, including findings of pulmonary infiltration, pulmonary oedema and pleural effusion in both unilateral or bilateral lungs. The electrocardiogram showed abnormalities in 13 of 21 patients. These included sinus tachycardia, ST segment elevation, ST segment depression, atrial fibrillation, ventricular tachycardia, ventricular fibrillation and junctional rhythm. Three of four patients who received an echocardiogram had a low ejection fraction (EF) (25%, 27% and 30–40%). The patient who had an EF of 25% died.
Management and Medical Outcomes
Thirty-four patients (82.9%) received intravenous fluid therapy. Other treatment regimens were multiple-dose-activated charcoal (MDAC) (27 cases, 65.9%), intravenous (IV) N-acetylcysteine (NAC) (22 cases, 53.7%), urine alkalinization (20 cases, 48.9%), oral high-dose silymarin (8 cases, 19.5%), IV penicillin G (7 cases, 17.1%) and IV antibiotic (11 cases, 26.8%). Haemodialysis and peritoneal dialysis were performed in five (12.2%) and two (4.9%) patients, respectively. Twenty-five patients (61%) were intubated with ventilator support. Fourteen patients (34.1%) received inotropic drugs. The median length of hospital stay was 5 days (range, 1–36 days). Sixteen patients were admitted for more than 1 week. Eleven patients (26.8%) died and all of them had rhabdomyolysis. Eight patients died within 3 days after admission, and the other three died at 4, 16 and 24 days after admission. One patient who died had the complication of ventilator-associated pneumonia and pneumothorax.
To analyze factors associated with death, we compared the clinical characteristics and laboratory findings between patients with rhabdomyolysis who died and those who survived (Table 5). We performed the analysis for only those patients who had rhabdomyolysis. In patients with rhabdomyolysis, differences between dead and surviving patients in the following parameters were found to be statistically significant: AKI, hyperkalaemia during hospitalisation, maximum CPK level, maximum creatinine level and initial and maximum potassium levels.
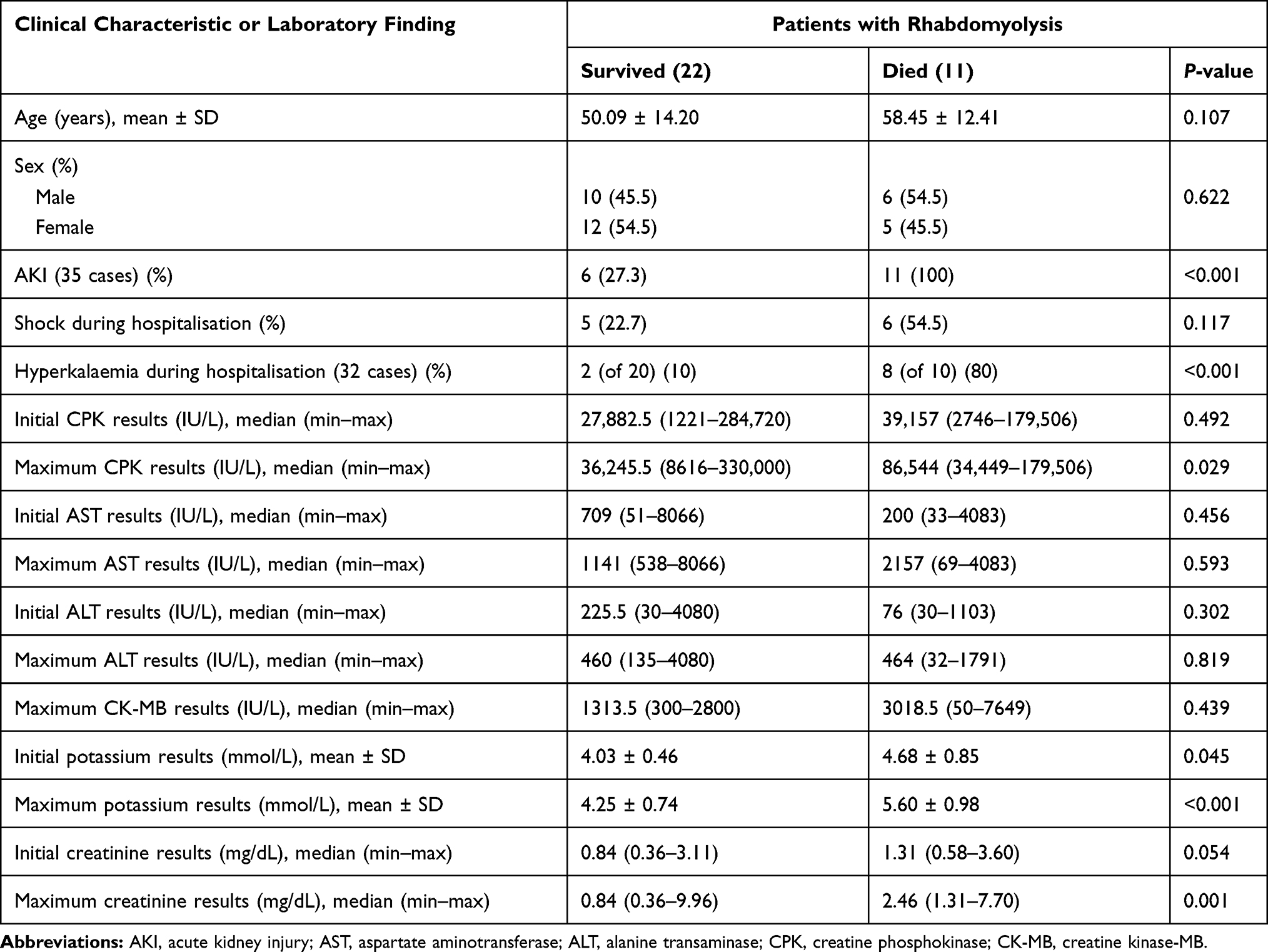 |
Table 5 Differences in Clinical Characteristics and Laboratory Findings Between Patients Who Survived and Patients Who Died for Patients with Rhabdomyolysis (33 Patients) |
Discussion
With 41 cases studied over a 5-year period, this study is one of the largest series of suspected myotoxic mushroom poisoning reported to date. Myotoxic mushroom poisoning was mainly diagnosed based on a history of mushroom ingestion together with symptoms, clinical signs and the finding of rhabdomyolysis. However, most of our patients exhibited rhabdomyolysis after ingestion of mushrooms and exposure as a poisoning group. This might help confirm the diagnosis of mushroom poisoning, even though no definite investigation could be performed. This might represent clinical practice in the real world, in which evaluation by an expert mycologist is not commonly available and the specific toxin either is never analyzed or is reported late after mushroom ingestion.
Nearly all the patients (97.6%) were from the north-east and north regions, where foraging for wild mushrooms is a common cultural practice.7 Mushroom poisoning occurred mainly during the rainy season, which is the growing season for mushrooms. All patients reported that they felt that the mushrooms were edible. Some of them identified the mushrooms as “charcoal mushrooms”, which commonly refers to edible mushrooms including Russula nigricans (large charcoal mushrooms) and Russula densifolia (small charcoal mushrooms) in Thailand.26 Russula subnigricans Hongo is reported to have been discovered in Thailand.21,27 The mushrooms brought by one group of patients were identified by the mycologist as Russula species. Based on previous reports of R. subnigricans poisoning in Asia.16–18 we postulated that the mushroom that caused rhabdomyolysis in our patients might have been R. subnigricans. Performing morphological and molecular identification of mushrooms and/or spores analysis in gastric content or feces, might help confirm the causative mushroom for myotoxic mushroom poisoning in the future study.
Previous studies of R. subnigricans poisoning reported both early and delayed onset of GI symptoms as “within 2 hours”,16 “6 hours”18 and “20 hours”.17 The onset of GI symptoms after mushroom ingestion in our study was reported as either early (<6 hours) or delayed (>6 hours), but still within 24 hours. However, some of our patients did not present with GI symptoms. The median onset of symptoms suggesting rhabdomyolysis was approximately 1–2 days (2–3 hours to 4–5 days) after ingestion of mushrooms. The onset of symptoms (GI symptoms or myalgia or dark urine) of myotoxic mushroom poisoning in our study could be either early or delayed. These were different from other reports of myotoxic mushroom poisoning from R. subnigricans, in which the patients in those reports had GI symptoms and developed myalgia or weakness within 24 hours after consuming mushrooms.16–18 Due to more patients were included in our study, this might explain these findings. Altogether, patients presenting with GI symptoms or other symptoms suggesting rhabdomyolysis after ingestion of mushrooms, either early or delayed, should be investigated for early diagnosis and prompt treatment of the poisoning.
Some patients who ate the mushrooms together and presented with other patients with rhabdomyolysis (classified as a poisoning group), had GI symptoms but did not develop rhabdomyolysis. Therefore, in patients who eat the mushrooms together, there could be only some patients manifested the overt characteristic of toxicity as rhabdomyolysis, not all of them. The explanation for this finding might be contributed from the different amount/dose that patients ingested or the individual susceptibility for rhabdomyolysis, further investigation and studies are required to elucidate and clarify this finding.
Almost all patients with rhabdomyolysis had elevated AST and ALT. However, the patient with the highest AST (8066 IU/L) and ALT (4080 IU/L) in our study had shock at presentation, so the very high AST and ALT might have been partially due to hypotension. The 2nd highest ALT level was 1926 IU/L. ALT can be elevated in patients with rhabdomyolysis in the absence of significant liver injury.28 No patient had coagulopathy except for one patient who was taking warfarin and another patient with DIC. Therefore, elevation of AST and ALT in our patients was resulted from rhabdomyolysis and myotoxic mushroom poisoning itself may not cause significant hepatotoxicity. This is consistent with other studies that did not report hepatotoxicity in their patients.16–18
Most patients in our study who were investigated for cardiac abnormalities had elevated cardiac enzymes, an abnormal electrocardiogram or an abnormal echocardiogram. Some patients developed cardiac dysrhythmia. These findings strengthen previous reports8,11,16–18 that myotoxic mushroom poisoning can cause severe cardiac toxicity, such as acute myocarditis or cardiac arrhythmia in some cases. Therefore, all patients with this mushroom poisoning should be investigated for cardiac abnormalities by electrocardiogram, measurement of cardiac enzymes and echocardiogram in severe cases.
Most patients survived after receiving supportive care. Some patients were treated during hospitalisation with MDAC, intravenous NAC, oral high-dose silymarin or IV penicillin G because of the physician’s suspicion of amatoxin-containing mushroom poisoning. Mortality in our study was about 27% in all patients and 33.3% in patients with rhabdomyolysis, which was higher than that in the report of R. subnigricans mushroom poisoning (14.3%)17 or even some reports of Tricholoma equestre mushroom poisoning.11 Our finding of high mortality may be due to the selection bias resulting from referral of severe cases to our poison centre. Because of the high fatality rate of mushroom poisoning, public education about wild mushroom picking and mushroom poisoning, especially before the beginning of the rainy season, should be implemented and promoted to prevent poisoning. We found that AKI, serum potassium level, serum creatinine level and serum CPK level were associated with death. In addition to cardiac evaluation, patients should be intensively monitored for serum potassium, creatinine and CPK, and abnormalities should be aggressively treated. Early detection, close monitoring and good supportive care are the main management modalities, especially in high-risk patients.
Our study had some limitations which can be listed as follows. First, our study was retrospective in nature together with data obtained from telephone consultations, such that it might have contained some incomplete data (such as the patients’ underlying diseases, the coingestion with other substances or some laboratory results). Medical history was obtained from patients, which they recognized, reported to the medical personnel; therefore, sometimes this might not be clearly or completely accurate. Second, a small number of patients were included in this study. Finally, there was no laboratory test performed to confirm the specific toxin of myotoxic mushrooms.
Conclusions
Myotoxic mushroom poisoning had a high mortality rate in this study. Most patients had either early or delayed onset of clinical symptoms after ingestion of mushrooms. Some patients developed severe cardiovascular effects, including cardiac arrhythmia and myocarditis. AKI, hyperkalaemia during hospitalisation, maximum CPK levels, maximum creatinine level and initial and maximum potassium levels were associated with death. Early detection, close monitoring and good supportive care were the main treatment modalities.
Data Sharing Statement
The data are not available for public access because of patient privacy concerns but are available from the corresponding author upon reasonable request.
Ethical Approval
This study was approved by the Institutional Ethics Committee Board of Ramathibodi Hospital Faculty of Medicine, Mahidol University. The Ethics Approval Reference Number is MURA2017/245 (ID 03-60-73). Because this is a retrospective study that uses the pre-existing confidential database from the poison centre, which was previously recorded, patient consent was not required by our hospital’s ethics committee board. The results of this study have been reported anonymously.
Acknowledgments
The authors express sincere thanks to Mrs. Umaporn Udomsubpayakul, section for Clinical Epidemiology and Biostatistics, Research Center, Faculty of Medicine Ramathibodi Hospital, Mahidol University for her help with statistical analysis.
Funding
We declare no funding for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Diaz JH. Evolving global epidemiology, syndromic classification, general management, and prevention of unknown mushroom poisonings. Crit Care Med. 2005;33(2):419–426. doi:10.1097/01.CCM.0000153530.32162.B7
2. White J, Weinstein SA, De Haro L, et al. Mushroom poisoning: a proposed new clinical classification. Toxicon. 2019;157:53–65. doi:10.1016/j.toxicon.2018.11.007
3. Goldfrank LR. Mushrooms. In: Nelson LS, Howland MA, Lewin NA, Smith SW, Goldfrank LR, Hoffman RS, editors. Goldfrank’s Toxicologic Emergencies.
4. Peintner U, Schwarz S, Mešić A, Moreau PA, Moreno G, Saviuc P. Mycophilic or mycophobic? Legislation and guidelines on wild mushroom commerce reveal different consumption behaviour in European countries. PLoS One. 2013;8(5):e63926. doi:10.1371/journal.pone.0063926
5. Trabulus S, Altiparmak MR. Clinical features and outcome of patients with amatoxin-containing mushroom poisoning. Clin Toxicol (Phila). 2011;49(4):303–310. doi:10.3109/15563650.2011.565772
6. Enjalbert F, Rapior S, Nouguier-Soulé J, Guillon S, Amouroux N, Cabot C. Treatment of amatoxin poisoning: 20-year retrospective analysis. J Toxicol Clin Toxicol. 2002;40(6):715–757. doi:10.1081/CLT-120014646
7. Trakulsrichai S, Sriapha C, Tongpoo A, et al. Clinical characteristics and outcome of toxicity from Amanita mushroom poisoning. Int J Gen Med. 2017;10:395–400. doi:10.2147/IJGM.S141111
8. Bedry R, Baudrimont I, Deffieux G, et al. Wild-mushroom intoxication as a cause of rhabdomyolysis. N Engl J Med. 2001;345(11):798–802. doi:10.1056/NEJMoa010581
9. Chodorowski Z, Waldman W, Sein Anand J. Acute poisoning with Tricholoma equestre. Przegl Lek. 2002;59(4–5):386–387.
10. Anand JS, Chwaluk P, Sut M. Acute poisoning with Tricholoma equestre. Przegl Lek. 2009;66(6):339–340.
11. Sein Anand J, Chwaluk P. Acute intoxication with Tricholoma equestre–clinical course. Przegl Lek. 2010;67(8):617–618.
12. Laubner G, Mikulevičienė G. A series of cases of rhabdomyolysis after ingestion of Tricholoma equestre. Acta Med Litu. 2016;23(3):193–197.
13. Yin X, Feng T, Shang JH, et al. Chemical and toxicological investigations of a previously unknown poisonous European mushroom Tricholoma Terreum. Chemi a Eur J. 2014;20(23):7001–7009. doi:10.1002/chem.201400226
14. Rzymski P, Klimaszyk P. Comment on “Mushroom poisoning: A proposed new clinical classification”. Toxicon. 2019;159:63–64. doi:10.1016/j.toxicon.2019.01.006
15. Klimaszyk P, Rzymski P. The yellow knight fights back: toxicological, epidemiological, and survey studies defend edibility of tricholoma equestre. Toxins (Basel). 2018;10(11):468. doi:10.3390/toxins10110468
16. Lee PT, Wu ML, Tsai WJ, Ger J, Deng JF, Chung HM. Rhabdomyolysis: an unusual feature with mushroom poisoning. Am J Kidney Dis. 2001;38(4):E17. doi:10.1053/ajkd.2001.27725
17. Lin S, Mu M, Yang F, Yang C. Russula subnigricans poisoning: from gastrointestinal symptoms to rhabdomyolysis. Wilderness Environ Med. 2015;26(3):380–383. doi:10.1016/j.wem.2015.03.027
18. Cho JT, Han JH. A case of mushroom poisoning with Russula subnigricans: development of rhabdomyolysis, acute kidney injury, cardiogenic shock, and death. J Korean Med Sci. 2016;31(7):1164–1167. doi:10.3346/jkms.2016.31.7.1164
19. Matsuura M, Saikawa Y, Inui K, et al. Identification of the toxic trigger in mushroom poisoning. Nat Chem Biol. 2009;5(7):465–467. doi:10.1038/nchembio.179
20. Counselman FL. Rhabdomyolysis. In: Tintinalli JE, editor. Tintinalli’s Emergency Medicine, a Comprehensive Study Guide.
21. GNews [homepage on the Internet]. Available from: https://gnews.apps.go.th/news?news=42188.
22. Evans KJ, Greenberg A. Hyperkalemia: a review. J Intensive Care Med. 2005;20(5):272–290. doi:10.1177/0885066605278969
23. Kidney disease: Improving global outcomes (KDIGO). KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl. 2012;2:6. doi:10.1038/kisup.2012.6
24. Nicks BA, Gaillard JP. Approach to nontraumatic shock. In: Tintinalli JE, editor. Tintinalli’s Emergency Medicine, a Comprehensive Study Guide.
25. Thai Meteorological Department [homepage on the Internet]. Available from: https://www.tmd.go.th/info/info.php?FileID=53.
26. Forest Biodiversity Division, Royal Forest Department, Ministry of Natural Resources and Environment [homepage on the Internet]. Available from: http://biodiversity.forest.go.th/index.php?option=com_doffungus&id=661&view=showone&Itemid=37.
27. Species Diversity of Mycorrhizal Fungi in Chiang Dao Wildlife Sanctuary Ecosystem [homepage on the Internet]. Available from: http://www.dnp.go.th/foremic/fmo/data/2CD%20mycorfull%20paperFINAL.pdf.
28. Weibrecht K, Dayno M, Darling C, Bird SB. Liver aminotransferases are elevated with rhabdomyolysis in the absence of significant liver injury. J Med Toxicol. 2010;6(3):294–300. doi:10.1007/s13181-010-0075-9
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.