Back to Journals » Clinical Ophthalmology » Volume 16
Myopia: An Increasing Problem for Medical Students at the University of Gondar
Authors Berhane MA, Demilew KZ ![]() , Assem AS
, Assem AS ![]()
Received 17 March 2022
Accepted for publication 10 May 2022
Published 19 May 2022 Volume 2022:16 Pages 1529—1539
DOI https://doi.org/10.2147/OPTH.S365618
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Michael Assefa Berhane,1 Ketemaw Zewdu Demilew,2 Abel Sinshaw Assem2
1Department of Ophthalmology, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia; 2Department of Optometry, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Ketemaw Zewdu Demilew, Department of Optometry, College of Medicine and Health Sciences, University of Gondar, PO Box 196, Gondar, Ethiopia, Tel +251-918150629, Email [email protected]
Purpose: The purpose of this study was to assess the prevalence and associated factors of myopia among medical students at the University of Gondar College of Medicine and Health Sciences, Northwest Ethiopia.
Patients and Methods: Institution-based cross-sectional study was conducted at the University of Gondar College of Medicine and Health Sciences from June 20 to August 15, 2021. A simple random sampling technique with proportional allocation was used to select 492 students. Interviewer-administered questionnaire, Snellen acuity chart, pinhole, retinoscope and direct ophthalmoscope were used to collect the data. The data were entered to EpiData version 4.6 and exported to SPSS version 25 for analysis. Descriptive statistics were summarized by measures of central tendency. Variables with p-value ≤ 0.2 in bivariable regression were entered into a multivariable logistic regression model. Adjusted odds ratio with 95% confidence interval was used and variables with p-values < 0.05 were considered as statistically significant.
Results: A total of 492 respondents participated giving a response rate of 98.3%. The prevalence of myopia was found to be 16.7% (95% CI = 12.8– 19.4%). Urban residents (AOR = 1.56; 95% CI: 1.28– 6.21), family history of myopia (AOR = 2.31; 95% CI: 1.33– 4.54), near-work activity of 5– 7 hours (AOR = 2.41; 95% CI: 1.31– 5.76) and ≥ 8 hours (AOR = 4.35; 95% CI: 1.96– 9.66), outdoor activity for < 3 hours (AOR = 1.65 95% CI: (1.14– 4.53), were significantly associated with myopia.
Conclusion: The prevalence of myopia among medical students at the University of Gondar College of Medicine and Health Sciences was high. Urban residency, positive family history, longer time spent on near-work activities and less outdoor activity were positively associated with myopia.
Keywords: myopia, medical students, Gondar, Ethiopia
Introduction
Myopia is a common cause of correctable visual reduction and is the leading cause of visual impairment globally. The main clinical presentations of myopia include reduction of distance and/or near vision, reduction of color vision, diminished contrast sensitivity, constriction of visual field, fear of light and loss of vision.1
The prevalence of myopia has been shown to vary widely with geographic location.2 Globally, the prevalence of myopia was estimated to be 34% by 2020 and it is estimated that 50% of the global population will be myopic by 2050.3 4 A study done in East Asia showed a prevalence of myopia exceeding 70%.5 Age-specific prevalence of myopia from age 20–29 years in Asia and Europe is reported as 45−50% and 20–35%, respectively.6,7 Its prevalence and distribution in Africa is lower than Asian and European countries.8 The prevalence of myopia in East Africa was 4.2% in 2010 and projected to be 8.2%, 12.3% and 22.7% by the years 2020, 2030 and 2050, respectively.9
Myopia has been associated with complications, such as myopic macular degeneration (MMD), retinal detachment (RD), cataract, and open angle glaucoma (OAG).10 These complications can lead to irreversible visual impairment later in life.11
The rapid increase in the prevalence of myopia has huge social, educational and economic consequences to the society.12 Uncorrected myopia was estimated to cause $244 billion potential productivity loss worldwide and macular degeneration due to myopia alone was associated with another $6 billion potential productivity loss annually.13 Myopia has also a great impact on career choices, ocular health, learning capability, educational potential and quality of life.14,15
Evidence suggests that both genetic and environmental factors affect myopia.16 According to available evidence excessive near-work, little outdoor activity, positive family history of myopia, joining higher education, increased use of computers and electronic devices are the major risk factors for myopia development.17–19
A variety of clinical methods are currently utilized for prevention and management of myopia. The possible alternatives to treat myopia are spectacles, contact lenses, medications such as atropine, phenylephrine, increasing time spent outdoors, reducing near-work intensity, proper diet and study breaks.20
Although there are some community and school-based myopia studies on pre-school and school children, there is no published information about prevalence and associated factors of myopia among medical students in Ethiopia specifically in the study area. Therefore, the purpose of this study was to assess the prevalence of myopia and its associated risk factors among medical students at the University of Gondar, College of Medicine and Health Sciences (CMHS).
Methods and Materials
Study Area, Design and Period
An institution-based cross-sectional study was conducted at the University of Gondar, College of Medicine and Health sciences from June 20, 2021 to August 15, 2021.
Source and Study Population
All medical students at the University of Gondar, College of Medicine and Health Sciences were the source population for this study.
Inclusion Criteria
All medical students at University Gondar, College of Medicine and Health Science during the data collection period.
Exclusion Criteria
Students who had active ocular infection, previous intra-ocular surgery and media opacity were excluded from the study.
Sample Size Determination
The required sample size was determined using a single population proportion formula. By taking the prevalence of myopia (11.9%) from a study conducted on high school students in Gondar city,14 margin of error 3%, z statistic at 95% confidence interval 1.96 and 10% non-response rate, the final sample was determined to be 492.
Sampling Technique and Procedure
A simple random sampling technique was used to recruit 492 study participants. The total number of medical students at the University of Gondar, College of Medicine and Health Sciences was 943. The sample was proportionally allocated to the year of study of students and simple random sampling was used to select participating students (Figure 1).
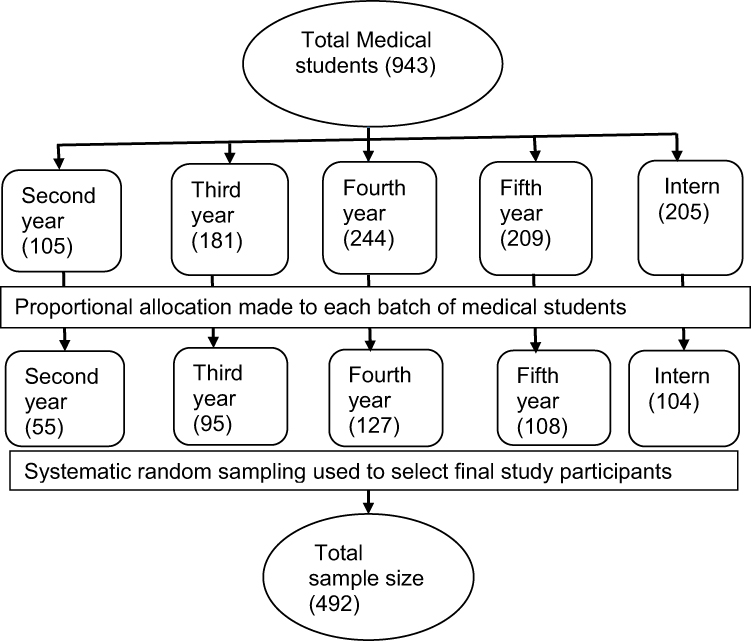 |
Figure 1 Flow chart showing sampling procedures sampling technique and how proportional allocation was made among different batches of University of Gondar Medical students in 2021. |
Variables of the Study
Dependent Variable
Myopia (yes or no).
Independent Variables
Socio-demographic factors (age, sex, year of study, residence).
Environmental and educational factors (time spent on near-work, working distance, illumination during study, reading hours, time spent outdoors, using visual display unit, staying up late, break during study).
Family-related factors (positive family history of myopia, family educational status, family income).
Operational Definition
Myopia was defined as a spherical equivalent refractive error (SER = sphere + 1/2 cylinder) of ≤−0.50 D.
Degree of myopia: Myopia is considered as low myopia when it is −0.50 D to −3.00 D, moderate myopia when it is <−3.00 D to −6.00 D and high myopia when it is <−6.00 D.
Familial myopia: First degree relatives (father, mother, brother and sister) with any degree of myopia previously diagnosed by a professional.
Ocular abnormality: Any ocular disorder such as keratoconus, strabismus, ptosis, corneal opacity, cataract, lens subluxation or dislocation.
Outdoor activity: Activities such as walking, playing football outside, per day.
Working distance: The regular distance in centimeters at which a person adapts to do near tasks. The average working distance for a normal individual is 33 cm.
Visual display unit (VDU): A screen-based device that displays text or pictures that reflect data stored in a computer’s memory.
Data Collection Procedures and Personnel
English version structured questionnaire was prepared by reviewing different studies.14,21–26 Interview and ocular examination were conducted for study participants by five trained optometrists. Three-meter Snellen acuity chart, pinhole, streak retinoscope and direct ophthalmoscope were used for ocular examination of the students. Non-cycloplegic refraction was done for study participants to screen for myopia.
At the end of the examination, study participants were told and advised about their visual status and eye conditions. Participants with conditions were linked to the optometry department for further treatment and follow-up.
Data Quality Assurance
The quality of data was assured through different strategies. Pretest (5%) was conducted on 5% of the total sample size among medical students of Debre-Tabor University, College of Medicine and Health Sciences before the actual data collection time. Based on the pretest some modifications were done on unclear questions, concept and sequences of the question before applying it to the actual study participants. Data collectors and supervisors were trained for a half-day about the data collection. Respondents were oriented about the objective of the study on the data collection day. In addition, 5% of the data was cross checked for completeness at the end of each data collection day. The data were further cleaned and coded after data entry.
Data Processing and Analysis
The collected data were entered into EpiData version 4.6 and exported to SPSS version 25 statistical software for analysis.
The outcome variable was dichotomized and coded as “0” and “1”, representing those who do not have or have myopia, respectively. Statistics were described using frequencies, mean and standard deviation and presented by tables, figures, and text.
Binary logistic regression analysis was carried out to identify factors associated with myopia. Those variables with p ≤0.2 from bivariable analysis was entered to multivariable logistic regression model to control the possible effects of confounder/s, and then variables with a p-value of ≤0.05 in multivariable logistic regression model was considered statistically significant. Before conducting the multivariable logistic regression, model multicollinearity was checked using variable inflation factor (VIF). Hosmer and Lemeshow goodness of fit was computed and the model was adequate with a p value of 0.32. Adjusted odds ratio with 95% confidence interval was computed to see the presence, strength and direction of association between dependent and independent variables.
Ethical Considerations
The study was conducted according to the Declaration and tenets of Helsinki. Ethical clearance was obtained from University of Gondar, College of Medicine and Health Sciences, School of Medicine Ethical Review Committee. Written informed consent was obtained from each study participant after explaining the purpose of the study. Participants were given a full right to participate, refuse or withdraw from the study at any time they wanted. Confidentiality was maintained and assured by excluding their names from the questionnaire, coding and locking the data.
Students with myopic and other ocular conditions were linked to the optometry department for treatment and follow-up. All study participants were advised about the importance of regular ocular screening even in the absence of any visual symptoms or problems.
Result
Socio Demographic and Economic Characteristics of Participants
A total of 484 medical students participated in this study with a response rate of 98.3%. The mean age of the participants was 22.81 ± 2.11 (SD). From all participants, 234 (46.5) were between age group of 21–23 years, 63.1% were previously urban residents, 307 (63.4%) were male and 361 (74.6%) were orthodox followers. Regarding year of study, the largest proportion of participants (126; 26%) were fourth year students. Most of the participants (258; 53.3%) had parents with an educational status of college and above. There were 142 (29.3%) students who had at least one positive family history. The median family monthly income of the respondents was 7000 (IQR = 4000) Ethiopian Birr (ETB) (Table 1).
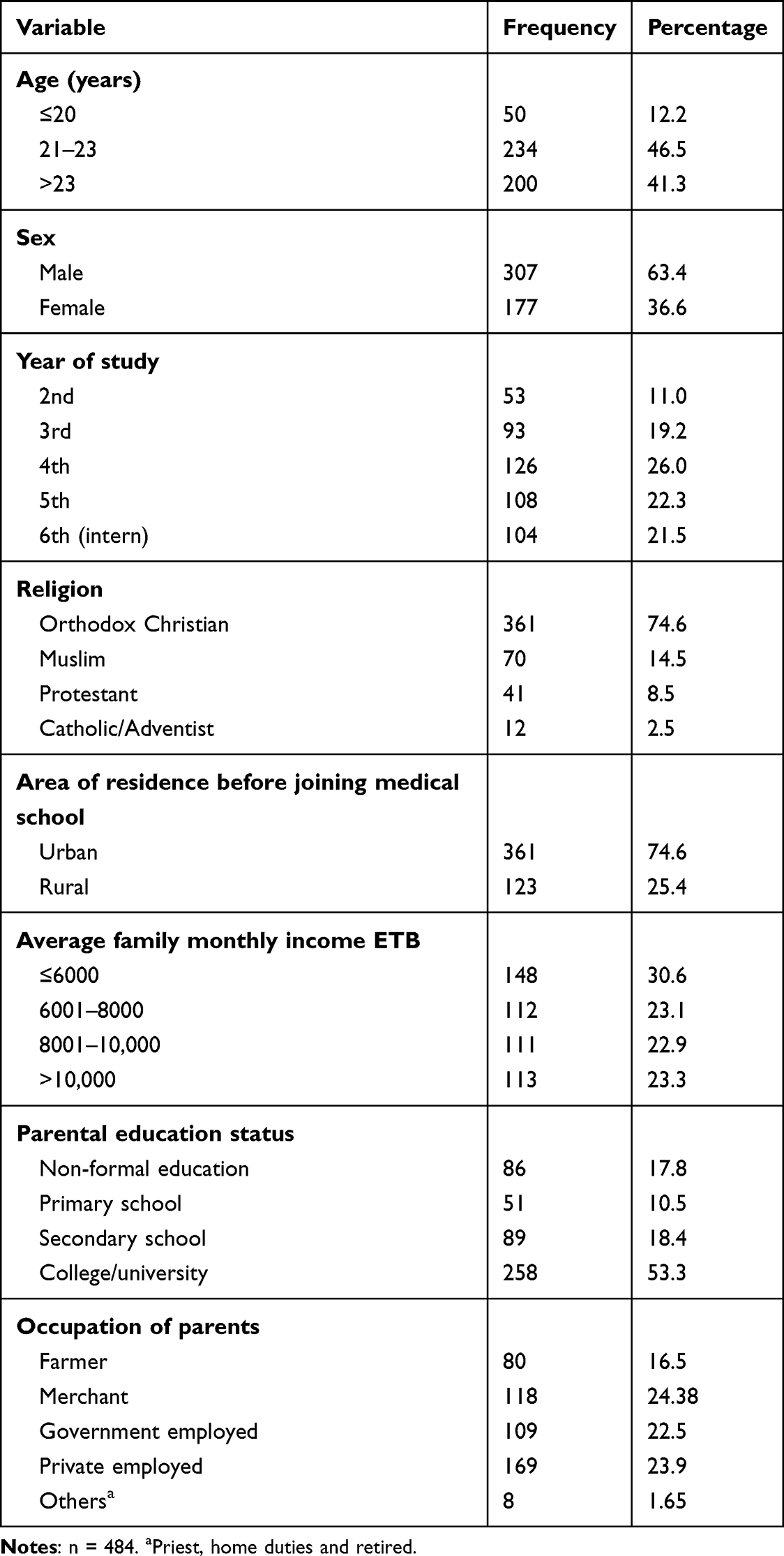 |
Table 1 Socio Demographic and Economic Characteristics of Medical Students at University of Gondar College of Medicine and Health Sciences, Northwest Ethiopia, 2021 |
Environmental Characteristics and Family-Related Myopia
The mean working distance was 45.86 cm ±4.97 (SD). Out of 484 participants, 148 (30.6%) had working distance between 42–46 cm; 246 (50.8%) students were not taking a break after 1 hour reading, and had a habit of staying up late after 12 AM (midnight); and 271 (56.8) of the participants use a fluorescent or lamp while reading.
About 128 (26.4%) of students spent more than 7 hours per day and 171 (35%) students spent more than 5 hours per day on near-work and visual display unit, respectively. In addition, more than two-thirds (86%) of participants were not reading under dim light; 312 (64.5%) students had less than 3 hours per day outdoor activity; and 142 (29.3%) participants had a positive family history of myopia (Table 2).
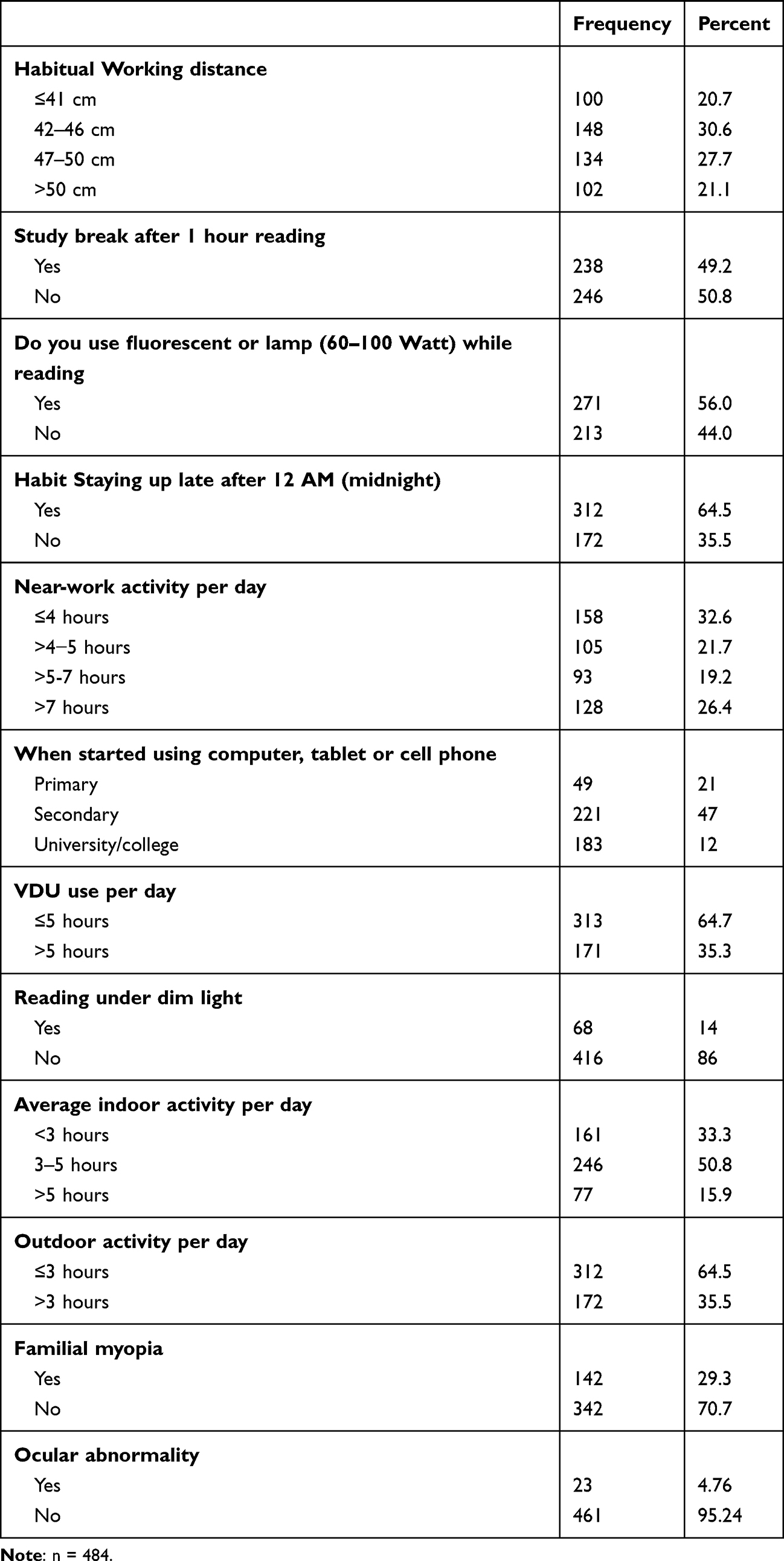 |
Table 2 Environmental Characteristics and Family Related Myopia of Medical Students at the University of Gondar, College of Medicine and Health Sciences, Northwest Ethiopia, 2021 |
Prevalence of Myopia Among Medical Students
The overall prevalence of myopia among medical students at the University of Gondar, College of Medicine and Health Sciences was found to be 16.7% (95% CI: 12.8–19.2%). Considering the degree of myopia, 63 (77.7%) had low myopia, 16 (19.8%) had moderate myopia and 2 (2.5) had high myopia.
Factors Associated with Myopia
Bivariable logistic regression analysis was done with the variables age, sex, year of study, residence before joining university, time spent on near-work, working distance, illumination during study, reading hours, time spent outdoors, using a visual display unit, staying up late, break during reading, positive family history of myopia, family educational status and average family income and variables with p value of <0.2 were selected for multivariable analysis. Age, sex, area of residence before joining university, average family income, positive family history, working distance, study break after 1 hour reading, staying up late, excessive near-work and less outdoor activity were all revealed to be significant in bivariable logistic regression analysis. However, on multivariable logistic regression analysis, area of residence before joining university, family history of myopia, excessive near-work and less outdoor activity remained statistically significant factors for development of myopia.
Accordingly, the odds of being myopic among participants who were previously urban residents were 1.56 times (AOR=1.58; 95% CI: 1.28, 6.21) compared with those who were rural residents. The odds of developing myopia among medical students who had positive family history of myopia were 2.31 times (AOR = 2.31; 95% CI: 1.33–4.14) higher than students who had no positive family history of myopia.
Regarding near-work of participants, the odds of being myopic among participants who had spent >5–7 hours per day and >7 hours per day were 2.41 times (AOR = 2.41; 95% CI: 1.31–5.76) and 4.35 times (AOR = 4.35; 95% CI: 1.96–9.66) high chance of developing myopia respectively compared with those who had spent ≤4 hours on near-work. Students who spent <3 hours on outdoor activity per day were 1.65 times (AOR = 1.65; 95% CI: (1.14–4.60) more likely to develop myopia compared with students who spent ≥3 hours on outdoor activity per day (Table 3).
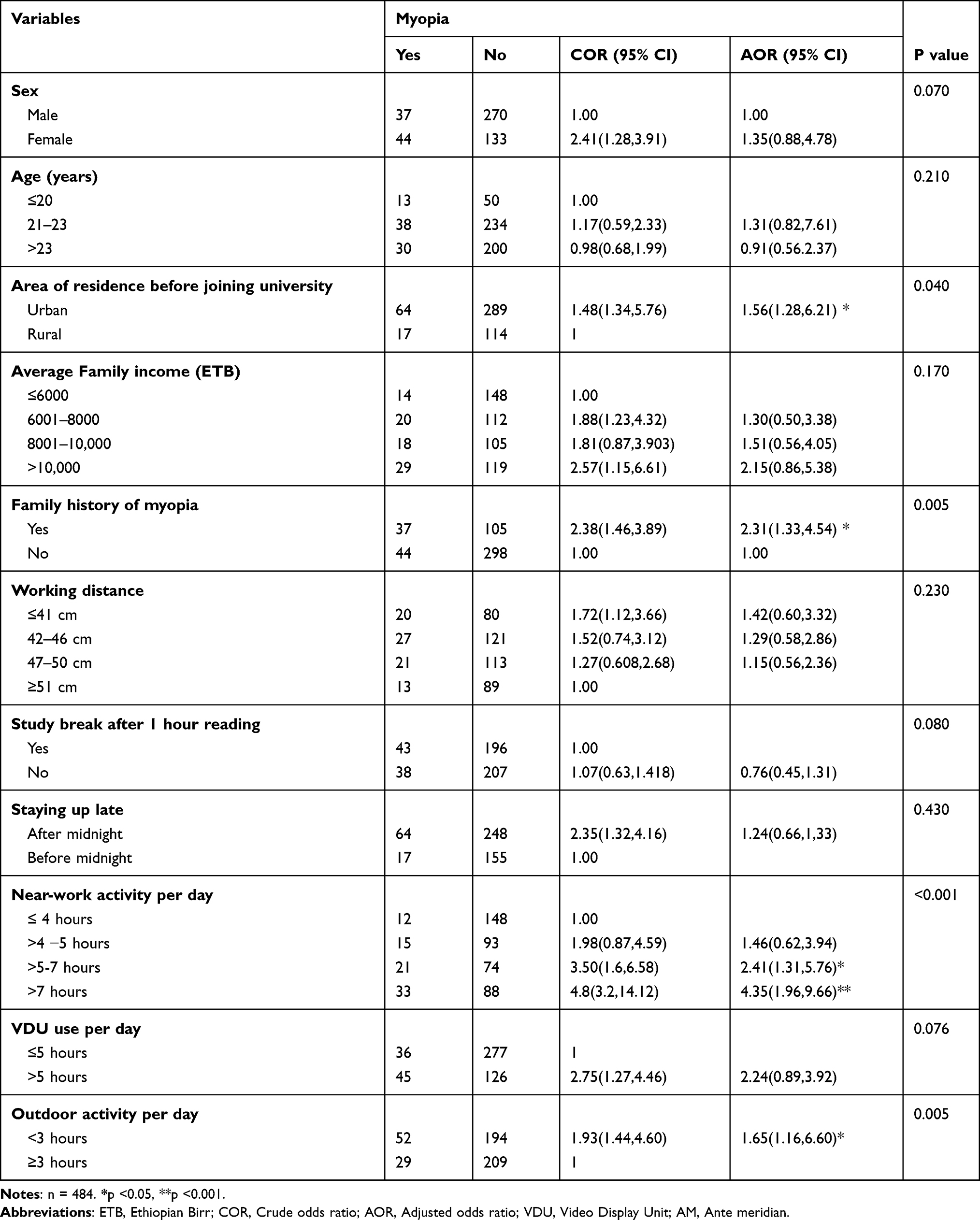 |
Table 3 Bivariable and Multivariable Logistic Regression Analysis for Factors of Myopia Among Medical Students at the University of Gondar, College of Medicine Health Sciences, Northwest Ethiopia, 2021 |
Discussion
The prevalence of myopia among medical students at the University of Gondar College of Medicine and Health Sciences, Northwest Ethiopia was found to be 16.7% (95% CI: 12.8–19.2). The prevalence in the current study was not in line with any previous figures reported among medical students. Nevertheless, it was consistent with studies conducted in Norway among adolescent age groups (13%)27 and Jordan among school-age children (17.6%).28
Compared with other school-based studies previously done in Gondar 11.9%,14 Bahir Dar8.49%,22 Welkite 6.5%,29 Nigeria 7.5%30 and South Africa 5%,31 the reported prevalence in the present study was higher. The variation might be due to the differences in the extent of exposure to risk factors of myopia. Medical students spend most of their time on reading and near-work activities in addition to limited outdoor activity which might have contributed to a higher prevalence of myopia compared with these schoolchildren.
The overall prevalence of myopia in the present study was lower than found in a study done in Nigeria among medical students (68.4%).32 Differences in inclusion criteria might be responsible for the observed difference. The study subjects in the Nigerian study were only spectacle wearers. Patients with refractive errors such as myopia are more likely to wear spectacles which may increase the reported prevalence of myopia. The prevalence was also found to be lower compared with reports from similar studies conducted in Aljouf Saudi Arabia 53.5%,33 Qassim 53.7%,21 Iran 42.71%,34 Mongolia China 69.21%,26 Northern China 78.5%,28 Lahore India 57.6%,35 Singapore 78.5%,36 Maharashtra, India 58.83%,37 Rajasthan, India 52.79%,38 Karachi, Pakistan 57.6523 and Vietnam 20.4%.39 This might be because of the difference in sample size, study setting and socio-demographic characteristics and type of screening tools used.
Studies done in Iran,34 Mongolia China26 and Northern China36 were based on a larger sample size. As these studies are from Asian countries where myopia is highly prevalent even in the general population, the increased prevalence of myopia among medical students in these countries might be due to the effects of complex genetic traits favoring myopia.40 Additionally, high utilization of digital devices which increases near-work involvement might be the reason for higher prevalence of myopia in the above studies.
In the present study it was found that students who were urban residents before joining medical school were 1.56 times more likely to develop myopia compared with those who were rural residents. This finding was supported by studies conducted in Asian countries such as Singapore,7 South Korea,41 Taiwan,42 China43–45 and Israel.46 The reason for this might be because urban residents spend more time indoors and engaged more on near-work activities.
Medical students who had a positive family history of myopia in at least one person in their family were 2.31 times more likely to develop myopia compared with those who had no family history of myopia. This finding was consistent with other cross-sectional studies conducted in Pakistan,47 China26 and India48 and several school-based studies in Gondar, Bahir Dar14,22 and China.49–51 This might be because of the hereditary predisposition of myopia.52
This study also discovered that medical students who spent >5–7 hours per day and >7 hours per day on near-work were 2.41 and 4.35 times more likely to develop myopia, respectively, than those who spent ≤4 hours per day. The result was consistent with studies done in Singapore,35 India,53 Pakistan,54 Turkey55 and Norway.56 This could be because prolonged near-work causes ciliary spasm which causes a defocused peripheral retinal image. The defocused peripheral retinal image is a stimulus for axial length elongation and progression of myopia.14
The odds of being myopic among participants with outdoor activity of ≤3 hours per day were 1.65 times higher compared with those who had >3 hours of outdoor activity per day. In this regard, the finding was similar with other cross-sectional findings previously reported in Norway,56 Beijing,57 Indonesia58 and Turkey.55 Dopamine, which is obtained from sunlight exposure, inhibits axial elongation and the occurrence of myopia. When outdoor activities are limited, the exposure to sunlight is limited so that the amount of dopamine released will be less leading to less inhibition of axial elongation. This increases the risk of myopia development and progression.59
Limitation of the Study
The study was a single center study, the students who participated in this study may not be representative of the overall university medical students with myopia. There may be self-reported bias during completion of the questionnaire on time spent on visual display electronic devices, family history of myopia and family monthly income.
Conclusion
The prevalence of myopia among medical students at the University of Gondar, College of Medicine and Health Sciences was relatively low compared with similar studies done elsewhere in the world. Urban residency, positive family history, longer time spent on near-work activities and less time spent outdoors were the factors significantly associated with myopia among medical students.
Acknowledgments
We would like to acknowledge all participants of the study who kindly volunteered to take part in the interview. Our gratitude also goes to data collectors for their tireless work during data collection.
Funding
There was no funding provided for this research work.
Disclosure
The authors declare that there are no conflicts of interest in this work.
References
1. Wu LJ, You QS, Duan JL, et al. Prevalence and associated factors of myopia in high school students in Beijing. PLoS One. 2015;10(3):e0120764.
2. Vitale S, Sperduto RD, Ferris FL. Increased prevalence of myopia in the United States between 1971-1972 and 1999-2004. Arch Ophthalmol. 2009;127(12):1632–1639. doi:10.1001/archophthalmol.2009.303
3. Sankaridurg P, Tahhan N, Kandel H, et al. IMI Impact of myopia. Invest Ophthalmol Vis Sci. 2021;62(5):2. doi:10.1167/iovs.62.5.2
4. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036–1042. doi:10.1016/j.ophtha.2016.01.006
5. You QS, Wu LJ, Duan JL, et al. Factors associated with myopia in school children in China: the Beijing childhood eye study. PLoS One. 2012;7(12):e52668. doi:10.1371/journal.pone.0052668
6. Pan C-W, Dirani M, Cheng C-Y, et al. The age-specific prevalence of myopia in Asia: a meta-analysis. Optometry Vision Sci. 2015;92(3):258–266. doi:10.1097/OPX.0000000000000516
7. Matsumura S, Ching-Yu C, Saw S-M. Global Epidemiology of Myopia. Singapore: Springer; 2020:27–51.
8. Pan CW, Ramamurthy D, Saw SM. Worldwide prevalence and risk factors for myopia. Ophthalmic Physiological Optics. 2012;32(1):3–16. doi:10.1111/j.1475-1313.2011.00884.x
9. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036–1042.
10. Flitcroft D. The complex interactions of retinal, optical and environmental factors in myopia aetiology. Prog Retin Eye Res. 2012;31(6):622–660. doi:10.1016/j.preteyeres.2012.06.004
11. Tideman JWL, Snabel MCC, Tedja MS, et al. Association of axial length with risk of uncorrectable visual impairment for Europeans with myopia. JAMA Ophthalmol. 2016;134(12):1355–1363. doi:10.1001/jamaophthalmol.2016.4009
12. Morgan IG, Ohno-Matsui K, Saw SM. Myopia. Lancet. 2012;379(9827):1739–1748. doi:10.1016/S0140-6736(12)60272-4
13. Naidoo KS, Fricke TR, Frick KD, et al. Potential lost productivity resulting from the global burden of myopia: systematic review, meta-analysis, and modeling. Ophthalmology. 2019;126(3):338–346. doi:10.1016/j.ophtha.2018.10.029
14. Belete GT, Anbesse DH, Tsegaye AT, Hussen MS. Prevalence and associated factors of myopia among high school students in Gondar town, northwest Ethiopia, 2016. Clinical Optometry. 2017;9:11. doi:10.2147/OPTO.S120485
15. Rose K, Harper R, Tromans C, et al. Quality of life in myopia. Br j Ophthalmol. 2000;84(9):1031–1034. doi:10.1136/bjo.84.9.1031
16. Pokharel GP, Negrel AD, Munoz SR, et al. Refractive error study in children: results from Mechi Zone, Nepal. Am J Ophthalmol. 2000;129(4):436–444. doi:10.1016/S0002-9394(99)00453-5
17. Jacobsen N, Jensen H, Goldschmidt E. Does the level of physical activity in university students influence development and progression of myopia?—a 2-year prospective cohort study. Invest Ophthalmol Vis Sci. 2008;49(4):1322–1327. doi:10.1167/iovs.07-1144
18. Kinge B, Midelfart A. Refractive changes among Norwegian university students‐A three‐year longitudinal study. Acta Ophthalmologica Scandinavica. 1999;77(3):302–305. doi:10.1034/j.1600-0420.1999.770311.x
19. Sun J, Zhou J, Zhao P, et al. High prevalence of myopia and high myopia in 5060 Chinese university students in Shanghai. Invest Ophthalmol Vis Sci. 2012;53(12):7504–7509. doi:10.1167/iovs.11-8343
20. Saw S-M, Matsumura S, Hoang QV. Prevention and management of myopia and myopic pathology. Invest Ophthalmol Vis Sci. 2019;60(2):488–499. doi:10.1167/iovs.18-25221
21. Al–Rashidi SH, Albahouth AA, Althwini WA, et al. Prevalence refractive errors among Medical Students of Qassim University, Saudi Arabia: cross-sectional descriptive study. Open Access Macedonian j Med Sci. 2018;6(5):940. doi:10.3889/oamjms.2018.197
22. Assem AS, Tegegne MM, Fekadu SA. Prevalence and associated factors of myopia among school children in Bahir Dar city, Northwest Ethiopia, 2019. PLoS One. 2021;16(3):e0248936. doi:10.1371/journal.pone.0248936
23. Chaudhry R, Ali H, Sheikh NH. Frequency and underlying factors of myopia among medical students. Biomedica. 2011;27(2):154–160.
24. Patel K. Prevalence of refractive errors and determinants of myopia among students in GMERS Medical College, Patan, Gujarat, India. Nat J Physiol Pharm Pharmacol. 2019;9(7):652–656.
25. Moafa MAM. Quantifying Risk Factors for Myopia: instrument Validation and Establishing Dosage for Light Intensity and Duration. 2018.
26. Wang L, Du M, Yi H, et al. Prevalence of and Factors Associated with Myopia in Inner Mongolia Medical Students in China, a cross-sectional study. BMC Ophthalmol. 2017;17(1):1–7. doi:10.1186/s12886-017-0446-y
27. Hagen LA, Gjelle JV, Arnegard S, et al. Prevalence and possible factors of myopia in Norwegian adolescents. Sci Rep. 2018;8(1):1–10. doi:10.1038/s41598-018-31790-y
28. Khader Y, Batayha W, Abdul Aziz S, Al Shiekh Khalil M. Prevalence and risk indicators of myopia among schoolchildren in Amman, Jordan. EMHJ. 2006;12(3–4):434–439.
29. Gessesse SA, Teshome AW. Prevalence of myopia among secondary school students in Welkite town: south-Western Ethiopia. BMC Ophthalmol. 2020;20(1):1–6. doi:10.1186/s12886-020-01457-2
30. Atowa UC, Wajuihian SO, Munsamy AJ. Prevalence and risk factors for myopia among school children in Aba, Nigeria. African Vision Eye Health. 2017;76(1):1–5. doi:10.4102/aveh.v76i1.369
31. Wajuihian SO, Hansraj R. Refractive error in a sample of black high school children in South Africa. Optometry Vision Sci. 2017;94(12):1145–1152. doi:10.1097/OPX.0000000000001145
32. Megbelayin EO, Asana UE, Nkanga DG, et al. Refractive errors and spectacle use behavior among medical students in a Nigerian medical school. J Adv Med Med Res. 2014;4(13):2581–2589. doi:10.9734/BJMMR/2014/7518
33. Algorinees R, Alqahtani N, Aljarbou A, AlShammari R, Alrashidi A. Prevalence of myopia and its related risk factors among medical students in Saudi Arabia. Adv Ophthalmol Vis Syst. 2017;6(1):00165.
34. Hashemi H, Derakhshan A, Mousavi MN, Mohazzab-Torabi S. The prevalence of refractive errors among Iranian university students. J Curr Ophthalmol. 2014;26(3):129.
35. Woo W, Lim K, Yang H, et al. Refractive errors in medical students in Singapore. Singapore Med J. 2004;45:470–474.
36. Lv L, Zhang Z. Pattern of myopia progression in Chinese medical students: a two-year follow-up study. Graefe’s Arch Clin Exp Ophthalmol. 2013;251(1):163–168. doi:10.1007/s00417-012-2074-9
37. Wakode N, Wakode S, Ksheersagar D. Risk factors for myopia in medical students. Int J Recent Trends Sci Technol. 2013;8(1):09–11.
38. Mehta R, Bedi N, Punjabi S. Prevalence of myopia in medical students. Indian J Clin Exp Ophthalmol. 2019;5(3):322–325. doi:10.18231/j.ijceo.2019.077
39. Paudel P, Ramson P, Naduvilath T, et al. Prevalence of vision impairment and refractive error in school children in B a R ia–V ung T au province, V ietnam. Clin Experiment Ophthalmol. 2014;42(3):217–226. doi:10.1111/ceo.12273
40. Verhoeven VJ, Buitendijk GH, Rivadeneira F, et al. Education influences the role of genetics in myopia. Eur J Epidemiol. 2013;28(12):973–980. doi:10.1007/s10654-013-9856-1
41. Ahn H, Lyu IS, Rim TH. The influence of parental myopia on children’s myopia in different generations of parent-offspring pairs in South Korea.
42. Tsai T-H, Liu Y-L, Ma I-H, et al. Evolution of the prevalence of myopia among Taiwanese schoolchildren: a review of survey data from 1983 through 2017. Ophthalmology. 2021;128(2):290–301. doi:10.1016/j.ophtha.2020.07.017
43. Chen X, Ye G, Zhong Y, et al. Prevalence, incidence and risk factors for myopia among urban and rural children in southern China: protocol for a school-based cohort study. medRxiv. 2021.
44. Jan C, Li L, Keay L, Stafford RS, Congdon N, Morgan I. Prevention of myopia, China. Bull World Health Organ. 2020;98(6):435. doi:10.2471/BLT.19.240903
45. Kung Y-J, Wei -C-C, Chen LA, et al. Kawasaki disease increases the incidence of myopia. Biomed Res Int. 2017;2017:554.
46. Shapira Y, Mimouni M, Machluf Y, et al. The increasing burden of myopia in Israel among young adults over a generation: analysis of predisposing factors. Ophthalmology. 2019;126(12):1617–1626. doi:10.1016/j.ophtha.2019.06.025
47. Parveen N, Hassan SH, Rehman J, Shoukat U. Prevalence of myopia and its associated risk factors in local medical students. Cell. 2015;334:3887822.
48. Vaidya CV, Majmudar DK. A retrospective study of clinical profile of stroke patients from GMERS medical college and hospital, Gandhinagar, Gujarat. Int J Clin Trials. 2014;1(2):62–66. doi:10.5455/2349-3259.ijct20140805
49. Morgan IG, Ohno-Matsui K, Saw S-M. Myopia. Lancet. 2012;379(9827):1739–1748.
50. Wong Y-L, Saw S-M. Epidemiology of pathologic myopia in Asia and worldwide. Asia Pacific J Ophthalmol. 2016;5(6):394–402. doi:10.1097/APO.0000000000000234
51. Zhang X, Qu X, Zhou X. Association between parental myopia and the risk of myopia in a child. Exp Ther Med. 2015;9(6):2420–2428. doi:10.3892/etm.2015.2415
52. Ang M, Wong TY. Updates on Myopia: A Clinical Perspective. Springer Nature; 2020.
53. Chalasani S, Jampala VK, Nayak P. Myopia among medical students-A cross sectional study in a South Indian medical college. Al Ameen J Med Sci. 2012;5(3):233–242.
54. Khan AR, Ali B, Khan B, et al. Refractive Errors among Medical Students–A Cross-sectional Study. Int J Sci Study. 2021;8(10):23–29.
55. Onal S, Toker E, Akingol Z, et al. Refractive errors of medical students in Turkey: one year follow-up of refraction and biometry. Optometry Vision Sci. 2007;84(3):175–180. doi:10.1097/OPX.0b013e3180335c52
56. Midelfart A, Aamo B, Sjøhaug KA, Dysthe BE. Myopia among medical students in Norway. Acta Ophthalmol. 1992;70(3):317–322. doi:10.1111/j.1755-3768.1992.tb08571.x
57. Huang L, Kawasaki H, Liu Y, Wang Z. The prevalence of myopia and the factors associated with it among university students in Nanjing: a cross-sectional study. Medicine. 2019;98:10.
58. Nanis ATA, Fatmawati NK, Yuliana Y, Sawitri E. The Differences Of Myopia Risk Factors On Medicine Student And Pyshical, Health And Recreation Education Students In Unmul Samarinda. Jurnal Ilmu Kesehatan. 2019;7(2):130.
59. Rose KA, Morgan IG, Ip J, et al. Outdoor activity reduces the prevalence of myopia in children. Ophthalmology. 2008;115(8):1279–1285. doi:10.1016/j.ophtha.2007.12.019
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Peripheral Cytopenia and Its Associated Factors in Type 2 Diabetes Mellitus Patients, Northwest Ethiopia
Aynalem M, Getu F, Adane T
Journal of Blood Medicine 2022, 13:373-383
Published Date: 4 July 2022
Self-Medication Prevalence and Factors Associated with Knowledge and Attitude Towards Self-Medication Among Undergraduate Health Science Students at GAMBY Medical and Business College, Bahir Dar, Ethiopia
Siraj EA, Yayehrad AT, Kassaw AT, Kassahun D, Solomon E, Abdela H, Gizachew G, Awoke E
Patient Preference and Adherence 2022, 16:3157-3172
Published Date: 5 December 2022
Evaluation of Seven Different Brands of Metformin Hydrochloride Tablets Available in the Market in Gondar City, Ethiopia
Flatie Alemu A, Tegegne AA, Getaw NS
Drug, Healthcare and Patient Safety 2024, 16:19-28
Published Date: 1 February 2024