Back to Journals » Infection and Drug Resistance » Volume 13
Mutations in the Antibiotic Target Genes Related to Clarithromycin, Metronidazole and Levofloxacin Resistance in Helicobacter pylori Strains from Children in China
Authors Zhang Y, Wen Y, Xiao Q ![]() , Zheng W
, Zheng W ![]() , Long G
, Long G ![]() , Chen B
, Chen B ![]() , Shu X, Jiang M
, Shu X, Jiang M
Received 22 October 2019
Accepted for publication 17 December 2019
Published 30 January 2020 Volume 2020:13 Pages 311—322
DOI https://doi.org/10.2147/IDR.S235615
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Yanyi Zhang, Yi Wen, Qiulin Xiao, Wei Zheng, Gao Long, Bo Chen, Xiaoli Shu, Mizu Jiang
Department of Gastroenterology, Children’s Hospital, Zhejiang University School of Medicine, National Clinical Research Center for Child Health, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Mizu Jiang
Department of Gastroenterology, Children’s Hospital, Zhejiang University School of Medicine,National Clinical Research Center for Child Health, Hangzhou 310003, Zhejiang, People’s Republic of China
Tel +86-571-86670046
Fax +86-571-86658653
Email [email protected]
Purpose: This study aimed to characterize common mutations of antibiotic-resistant gene of clarithromycin, metronidazole and levofloxacin in Helicobacter pylori (H. pylori) and determine their association with antibiotic resistance of H. pylori for providing a strategy for eradication therapy of H. pylori infection in children.
Patients and Methods: The antibiotic resistance to clarithromycin, metronidazole and levofloxacin for H. pylori strains isolated from children was determined by E-test. The mutation of domain V of 23S rRNA, rdxA and frxA genes, gyrA and gyrB genes was performed by PCR-based sequencing of DNA fragments.
Results: Out of the 79 H. pylori strains examined, 66 (83.5%) were resistant to at least one of the tested antibiotics and 13 (16.5%) were fully sensitive. A total of 29 (36.7%) strains were resistant to clarithromycin. Analysis of the 23S rRNA gene showed that most mutations occurred at the A2143G and T2182C sites, showing a frequency of 82.8% (24/29) and 89.7% (26/29) respectively. In the 11 sensitive strains to clarithromycin, the frequency of A2143G mutation was only 45.5%, which was significantly lower than that in resistant strains (P< 0.05). There were 54 strains (68.4%) resistant to metronidazole, with most mutations occurring at G47A and T184G in the rdxA gene. T184G mutation was recognized in metronidazole-sensitive strains, but no G47A mutation was identified. Twelve strains (15.2%) were resistant to levofloxacin. Position 91 mutation of the gyrA gene occurred only in resistant strains, whereas position 87 mutations were detected in both sensitive and resistant strains to levofloxacin.
Conclusion: In H. pylori resistant strains isolated from children in China, most mutations occurred at A2143G of the 23S rRNA gene for clarithromycin; G47A mutation of rdxA gene for metronidazole; and at 91 mutation of gyrA gene for levofloxacin. It is suggested that susceptibility testing together with screening the mutation of antimicrobial-resistant gene prior to treatment is important for the eradication of H. pylori in children.
Keywords: Helicobacter pylori, Metronidazole, Clarithromycin, Levofloxacin, antibiotic resistant, gene
Introduction
Helicobacter pylori (H. pylori) is a gram-positive, microaerophilic bacterium that was first identified from human gastric mucosa by Australia scientists Barry Marshall and Robin Warren in 1982.1 H. pylori plays a significant role in the pathogenesis of gastrointestinal diseases, including chronic gastritis, peptic ulcer, gastric adenocarcinoma and gastric mucosa-associated lymphoid tissue lymphoma.2 In 1994, the International Association for Cancer Research listed H. pylori as a class I carcinogen. H. pylori is one of the most common human bacterial infections in the world, with a global infection rate as high as 50%.3,4 The prevalence of H. pylori infection in developing countries is higher than in developed countries, and studies showed that the prevalence of H. pylori infection in China is about 58.07%.5 In the past few decades, standard therapy regimen consisting of a proton pump inhibitor (PPI) in combination with two antibiotics such as amoxicillin, clarithromycin, metronidazole, or levofloxacin has been recommended as the first-line treatment regimen for H. pylori infection. However, with the increase of H. pylori resistant strains, this traditional treatment regimen is being replaced by quadruple therapy or sequential therapy.6
The increasing prevalence of antibiotic resistance in H. pylori is a cause for concern as this is one of the most important causes of therapy failure. The resistance rate of H. pylori in developing countries is significantly higher than that in developed countries.7 We also found that the total resistance rates of H. pylori to clarithromycin, metronidazole, and levofloxacin in children were 20.6%, 68.8%, and 9.0%, respectively, and the H. pylori resistance rate increased significantly from 2012 to 2014.8 Generally, H. pylori acquires antibiotic resistance by chromosomal mutations, not by acquiring plasmids.9 Although drug efflux proteins can contribute to the natural insensitivity to antibiotics and emerging antibiotic resistance, the main mechanism that contributes to H. pylori resistance is vertically transmitted point mutations in the DNA.10 Clarithromycin interacts with the peptidyl transferase region of the domain V of 23S rRNA subunit, an interaction that suppresses bacterial ribosome activity and inhibits bacterial protein synthesis.10 Point mutations in the 23S rRNA gene have been shown to lead to a modification in ribosome conformation, which consequently reduces clarithromycin affinity and leads to bacterial resistance to the drug.10 The most common mutations are A2143G, A2142G and A2142C. In addition, mutations A2115G, G2141A, C2147G, T2190C, C2195T, A2223G and C2694A have also been reported, but their role in resistance to clarithromycin is not yet clear.11 Metronidazole, a nitroimidazole, acts as a biocidal agent by its interaction with a nitroreductase homolog, rdxA. Mutations in rdxA were shown to be the cause of H. pylori resistance to metronidazole, while mutations in another gene, frxA, encoding to NADH flavin oxidoreductase was also implicated in H. pylori metronidazole resistance.12,13 Levofloxacin, a fluoroquinolone, generally target chromosome replication and in particular, DNA gyrase, which allows DNA unraveling before replication. This resistance has been associated with point mutations occurring at positions Asn87 and Asp91 of the quinolone resistance determining region (QRDR) within gyrA gene.14 Amino acid substitutions at positions 91 (D91G, N, A, Y or H) and 87 (N87L, I, A or K) of gyrA were most frequently associated with levofloxacin resistance, while gyrB frequently occurred alongside gyrA mutations.15,16 Despite the studies on the resistance-related genes, resistant isolates with other mutations seem to be emerging, and the mutations of resistance genes of H. pylori in children are poorly understood.
H. pylori antimicrobial resistance can be investigated in the laboratory by phenotypic and genotypic methods. Bacterial culture and determination of the minimum inhibitory concentration (MIC) of the antibiotic are characteristics of the phenotypic method. In this study, PCR amplification and DNA sequencing were performed to detect genetic mutations in drug-resistance and sensitive H. pylori strains from children, and we also determined the mutations of H. pylori strains resistant to clarithromycin, metronidazole and fluoroquinolone. We analyzed the correlation between drug resistance and gene mutations by molecular biology software.
Materials and Methods
Isolation and Culture of H. pylori
Gastric mucosa samples were collected from children (aged from 2 to 16 years old) with gastrointestinal diseases such as chronic gastritis or ulcer during endoscopy from 2012 to 2014 in Children’s Hospital, Zhejiang University School of Medicine. Isolation, culture and identification of H. pylori were performed at the laboratory of the Hangzhou Zhiyuan Medical Inspection Institute as described in previous studies.17 The antibiotic susceptibility testing was performed by E-test and agar dilution methods according to the protocols of the Clinical and Laboratory Standards Institute (Wayne, PA, USA).18 Written informed consents were obtained from the parents of the children involved in our study. The study protocol was approved by the Medical Ethics Committee in the Children’s Hospital, Zhejiang University School of Medicine (2018-IRB-003) and was conducted in accordance with the declaration of Helsinki. Exclusion criteria included history of treatment by use of antibiotic, antacid, H2 receptor antagonist, PPI, bismuth-containing compounds, or non-steroidal anti-inflammatory drugs (NSAID) in the last 4 weeks.
Antibiotic Susceptibility Tests
Susceptibility of H. pylori to five antibiotics (clarithromycin, amoxicillin, tetracycline, metronidazole, and levofloxacin) was tested via agar dilution method using reference standards obtained from the National Institutes for Food and Drug Control. Tenmicroliter suspensions (108 CFU/mL) of each isolate from a mixture of colonies in brain-heart infusion broth (Oxoid) were inoculated onto Mueller-Hinton agar plates (Oxoid) that included 5% sheep blood and a single antibiotic and incubated at 37°C for 3 days under microaerophilic conditions. The resistance break points to clarithromycin, amoxicillin, tetracycline, metronidazole, and levofloxacin were set at ≥1 μg/mL, ≥2 μg/mL, ≥2 μg/mL, ≥8 μg/mL, and ≥2 μg/mL, respectively. ATCC43504 (NCTC11637) was used as the control strain.
PCR and DNA Sequencing
H. pylori Strain Culturing and DNA Extraction
H. pylori strains were recovered and cultured under microaerophilic conditions. DNA extraction was performed using the Takara LA Taq Kit according to the manufacturer’s instructions, and the isolated genomic DNA was stored at −20°C.
Detection of DNA Purity and Concentration
DNA purity was examined using UV spectroscopy. DNA extracted from each strain was diluted in 5 μL water, and measured with light absorbance at 260 nm and 280 nm. The concentration and purity of DNA were determined. Purified DNA should have an A260/A280 ratio within 1.7–1.9.
PCR Amplification
PCR was performed for amplification regions, including following genes: 16S rRNA (139bp), 23S rRNA (280bp),19 rdxA (749bp),20 frxA (913bp),20 gyrA (582bp),21 gyrB (465bp).21 Based on the sequence of reference strain 26695 available on the GenBank website, the following primers were designed to detect point mutations (Table 1). Primers were diluted to 10 μM before use. The 50 μL PCR system contained Takara LA Taq (5 U/μL) 0.5 μL, 10×LA PCR Buffer II (Mg2+ Plus) 5 μL, dNTP Mixture (2.5 mM each) 4 μL, template DNA 5 μL, primer F (10 μM) 1 μL, primer R (10 μM) 1 μL, and dH2O 33.5 μL. The reaction condition was set as: 95°C pre-denaturation 5 min, 94°C 30 s, 58°C 30 s, 72°C 30 s, 30 cycles, and 72°C final elongation 10 min, followed by preservation at 4°C. After that, PCR products (9 μL) were added with 10×loading Buffer (1 μL), and electrophoresed through 1% agarose gel with 0.5 mg/L ethidium bromide at 100 mV for 30 min. For validation, electrophoresis strips were observed under a gel imager.
 |
Table 1 Primer Sequences for Molecular Detection of H. pylori |
DNA Sequencing
PCR products were first recognized by electrophoresis, and determined with DNA purity as well as concentration by measuring the A260/A280 ratio. DNA sequencing was accomplished by Qingke Zixi Biotechnology Co., Ltd (Hangzhou, China). Each sequence was compared to the sequences of H. pylori 26695 reference strains, available on the GenBank website. With sequences from NCBI for reference, mutations were identified from each sensitive or resistant strain using the MEGA 5 software.
Results
Clinical Data
A total of 79 H. pylori strains be isolated, identified and preserved from the patients because of abdominal pain, vomiting, and gastrointestinal bleeding. The mean age was 9.7± 2.8 years old. All of them were diagnosed as H. pylori-related gastritis by gastroendoscopy, histopathological examination, and H.pylori culture of gastric mucosa. Among them, 21 cases were diagnosed as duodenal ulcer, 1 case was gastric ulcer, 1 case was concomitant gastric and duodenal ulcer. Out of the 79 H. pylori strains examined, 66 (83.5%) were resistant to at least one of the tested antibiotics and 13 (16.5%) were fully sensitive. Among these strains, 66 were resistant strains, and most of them were resistant to multiple antibiotics. 29 (36.7%) were resistant to clarithromycin, 54 (68.4%) to metronidazole, and 12 (15.2%) to levofloxacin. No resistance of H. pylori strains to amoxicillin and to tetracycline was observed in our study.
rRNA Gene Mutations in Clarithromycin-Resistant Strains
Among 29 H. pylori resistant strains to clarithromycin, 22 were multi-drug resistant. A 280-bp segment on the 23S rRNA gene was successfully amplified by PCR and sequenced from both 11 sensitive strains and 29 resistant strains. We found most mutations in resistant strains occurred at A2143G and T2182C, with a frequency of 82.8% (24/29) and 89.7% (26/29), respectively, but mutations at A2142G and C2131T were detected only in one case, respectively. As for those 11 sensitive strains, the frequency of A2143G mutation was 45.5% (5/11), which was significantly lower than that in resistant strains (X2=6.714, P<0.05); the frequency of T2182C was 90.9% (10/11), which was not significantly different from that in resistant strains (89.7%, 26/29); No mutations were detected at A2142G or C2131T in sensitive strains as shown in Table 2. The figure of sequencing fluorograms of 23S rRNA gene amplification products in resistant and sensitive strains of H. pylori was shown in Supplementary Figure S1.
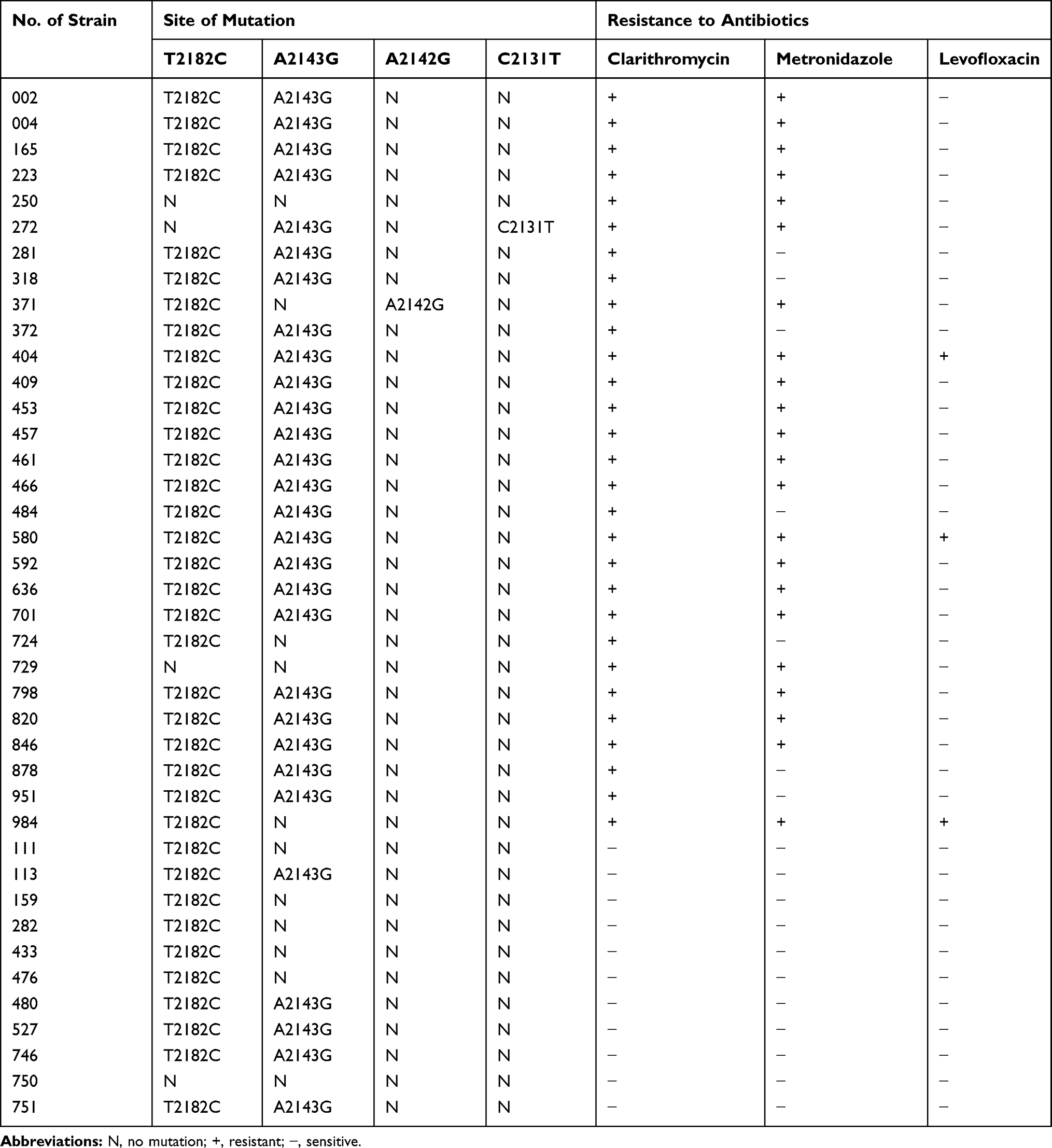 |
Table 2 Mutations Within 23S rRNA Gene for Clarithromycin-Resistant and Sensitive Strains of H. pylori |
rdxA and frxA Mutations in Metronidazole-Resistant Strains
The resistant rate of metronidazole to H. pylori was 68.4% (54/79), and 28 out of them had multiple drug resistance.
rdxA Mutations
A 749-bp segment of rdxA gene was successfully amplified by PCR and sequenced from both 6 sensitive strains and 54 resistant strains. The frequency of G47A mutation in resistant strains was 20.4% (11/54), and T184G mutation 70.4% (38/54), other mutations including G60A mutation in 3 resistant strains, C273T mutation in 2 resistant strains, and C49T mutation in 1 resistant strain. However, a mutation rate of T184G in sensitive strains was 83.3% (5/6), similar to the resistant strains. The above other 4-point mutations were not detected in any sensitive strains. In addition, deletion of A at position 329,330/Frameshift, a stop codon at position 111 and deletion of G at position 570/Frameshift at position 191 of rdxA gene were observed both in resistance strains and in sensitive strains of H. pylori as shown in Table 3. The figure of sequencing fluorograms of rdxA gene amplification products in resistant and sensitive strains of H. pylori was shown in Supplementary Figure S2.
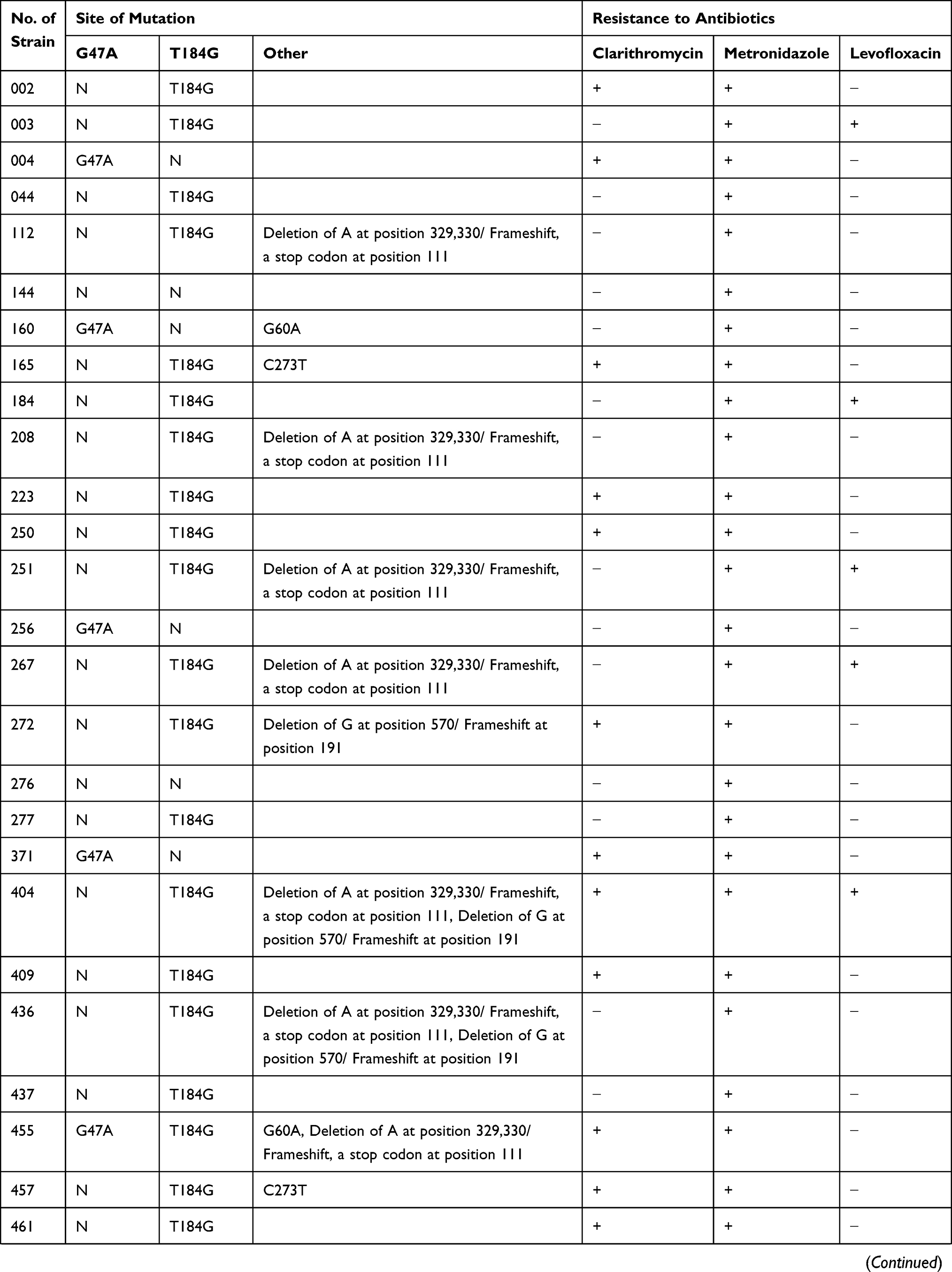 | 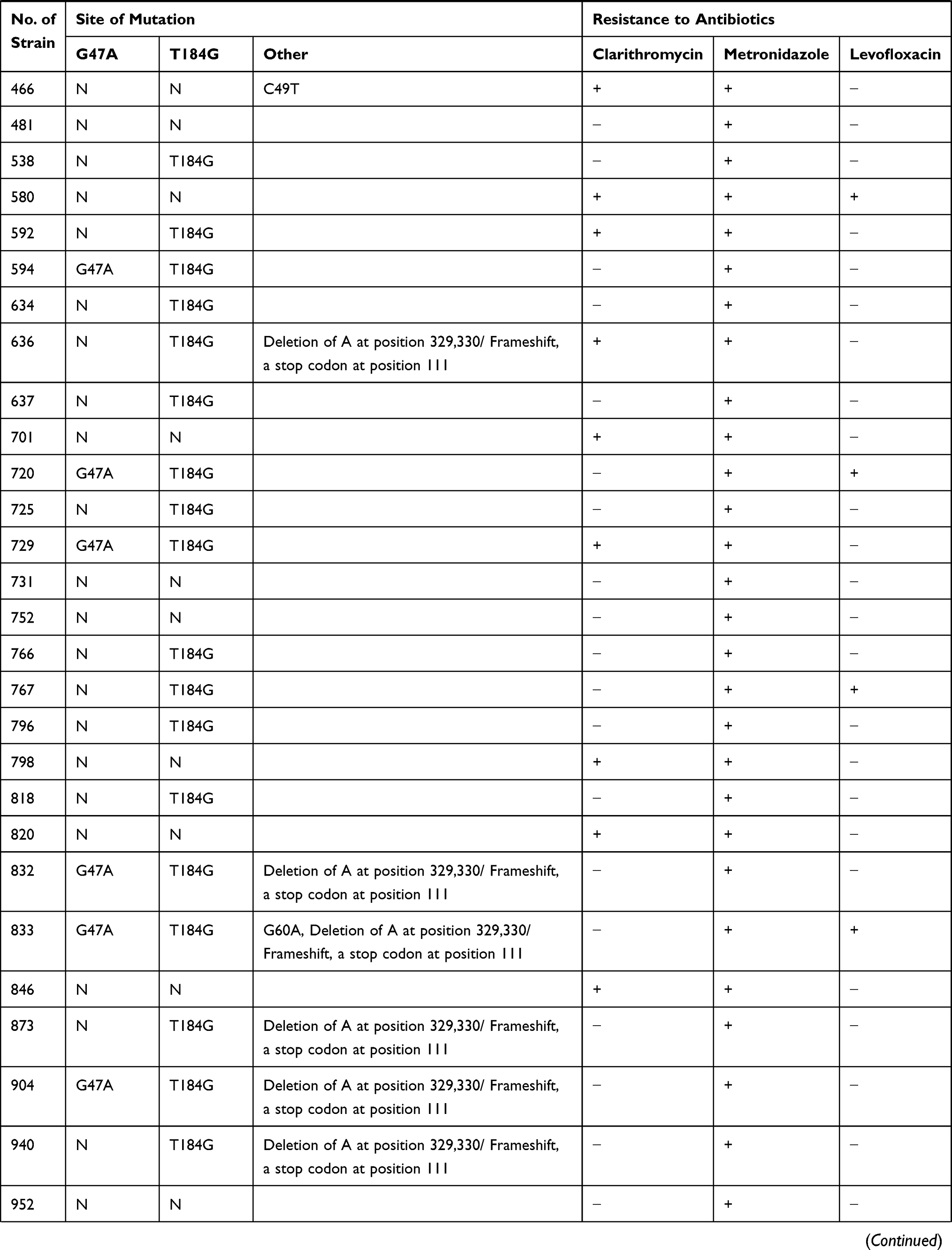 | 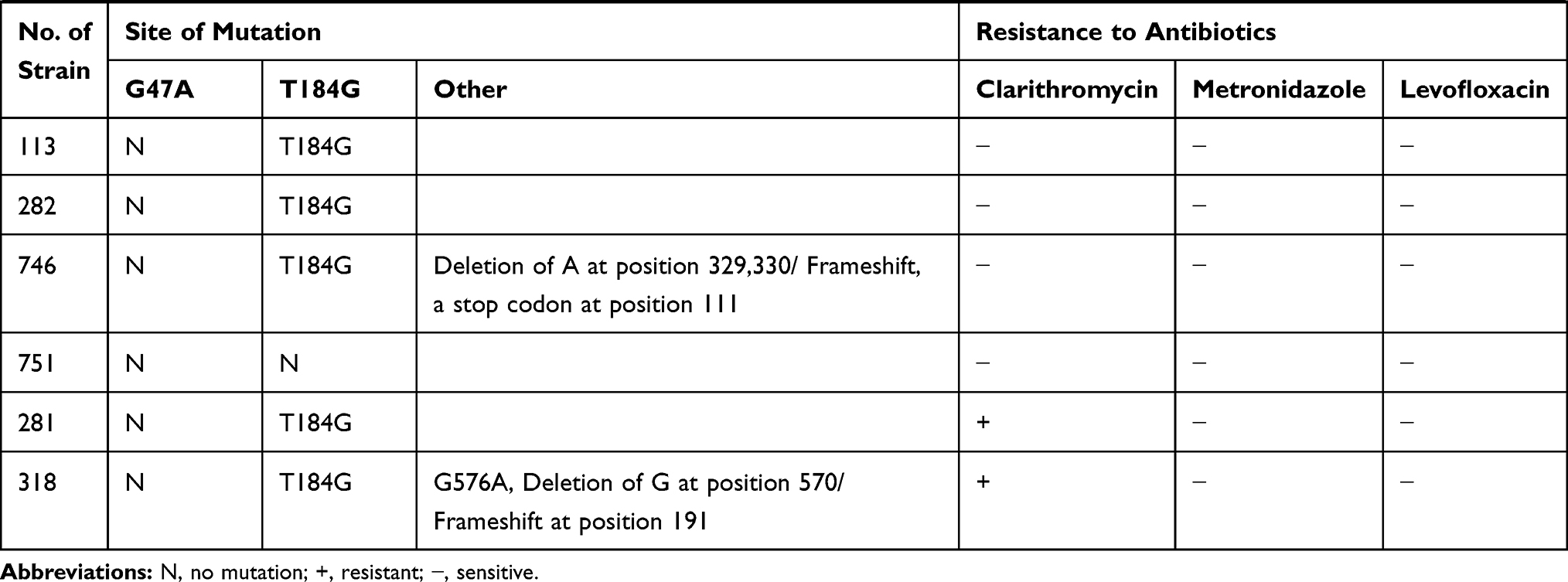 |
Table 3 Mutations Within rdxA for Metronidazole-Resistant and Sensitive Strains of H. pylori |
frxA Mutations
A 913-bp segment of frxA gene was successfully amplified by PCR and sequenced from both 6 sensitive strains and 43 resistant strains. The frequency of A48G mutations in resistant strains was 70% (30/43). Other 13 resistant strains did not have these point mutations. Among 30 resistant strains had the A48G mutations, 1 strain had a G441A mutation, 1 strain had a deletion of G at position 208. Besides, A48G mutation was also identified from all the 6 sensitive strains, and 1 strain had a C13A mutation in sensitive strain as shown in Table 4. The figure of sequencing fluorograms of frxA amplification products in resistant and sensitive strains of H. pylori was shown in Supplementary Figure S3.
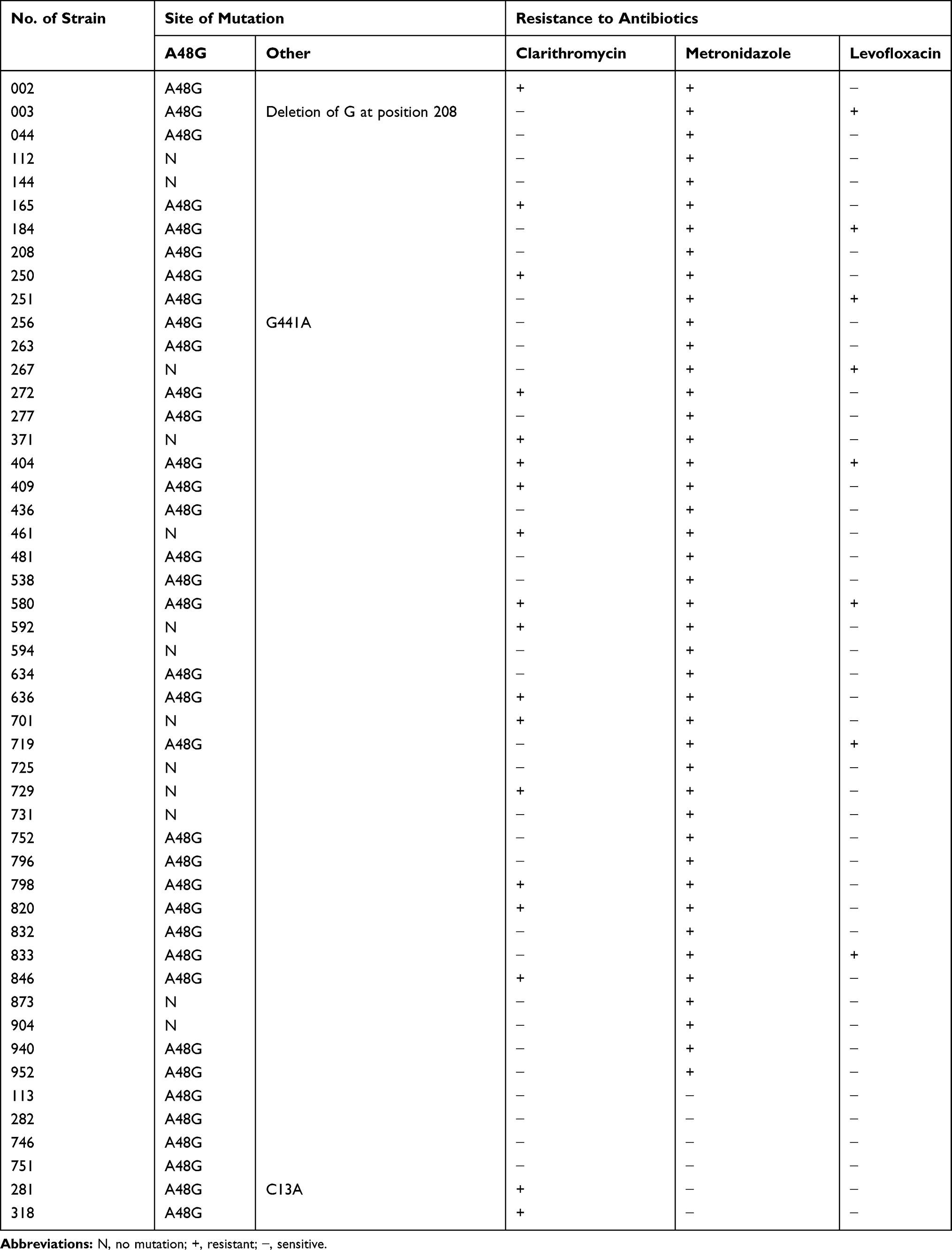 |
Table 4 Mutations Within frxA for Metronidazole-Resistant and Sensitive Strains of H. pylori |
gyrA and gyrB Mutations in Levofloxacin-Resistant Strains
The resistant rate of levofloxacin to H. pylori was 15.2% (12/79), and 11 out of them had multiple drug resistance. A 582-bp segment of gyrA was successfully amplified by PCR and sequenced from both 12 sensitive and 12 resistant strains. Three resistant strains of them had a mutation at ASP 91, and one mutated from Asp to Tyr, and it was resistant to both metronidazole and levofloxacin; the other two resistant strains mutated from Asp to Asn. In addition, there were N87K (Asn87Lys) mutations for both sensitive strains (6/12) and resistant strains (10/12). Other mutation including R140K (Arg140Lys) and V150A (Val 150Ala) were identified in one resistant strain and one sensitive strain, respectively. No D91Y or D91N mutation was found in sensitive strains as shown in Table 5. This study did not identify any mutations for gyrB gene in both resistant strains and sensitive strains. The figure of sequencing fluorograms of gyrA gene amplification products in resistant and sensitive strains of H. pylori was shown in Supplementary Figure S4.
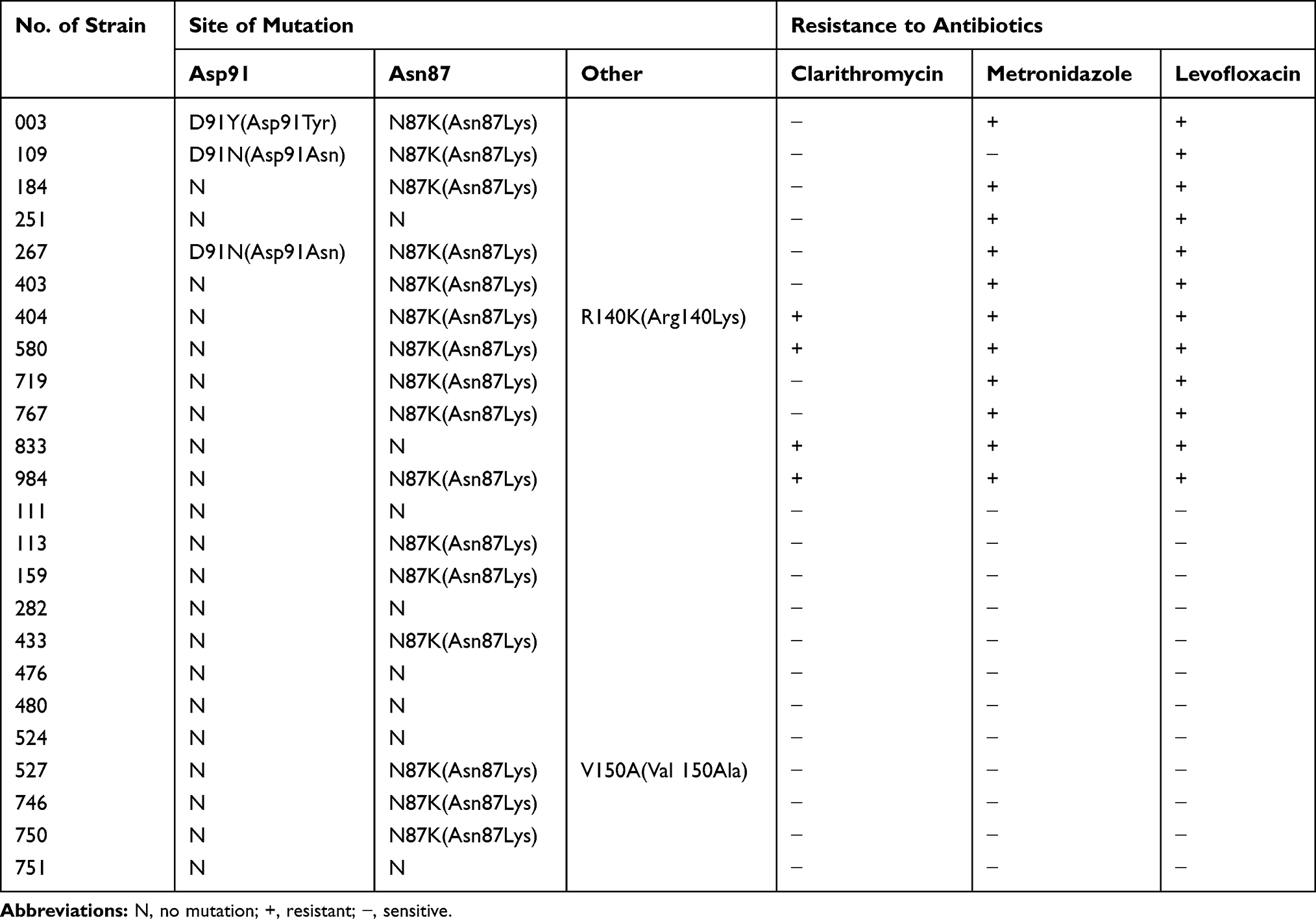 |
Table 5 Mutations Within gyrA for Levofloxacin-Resistant and Sensitive Strains of H. pylori |
Discussion
H. pylori infection has become a global problem. Nearly half of the world population are infected with the pathogen, and the infectious rate among children is estimated to be 10–80% with different age, with more than a half being infected before the age of 10 years old.15,16 In fact, many adult gastric H. pylori infections are suffered from childhood. H. pylori eradication is the key to the treatment of H. pylori related diseases, but it is controversial in children with H. pylori infection. Therapy failure is inherent and can be due to multiple factors (human and bacterial), including improper drug dose, short treatment duration, early treatment discontinuation, drug activity associated with the use of other substances, quick reinfection of successfully treated patients, and the presence of antibiotic-resistant strains.11 Many reports have indicated that antibiotic resistance has become a predominant factor for therapy failure in which containing clarithromycin and metronidazole. No consensus of indications and therapy of H. pylori eradication in children have yet been reached. It is very important to use sensitive antibiotics to treat H. pylori infection. Unfortunately, most of them have not performed any sensitivity tests including the E-test before H.pylori eradication therapy in the clinics. Point mutations detection by PCR or sequencing of the amplified fragment has higher sensitivity and specificity than that of MIC determination, which could be served as a new treatment regimen for antibiotics selection in the H. pylori eradication, especially in children.
In this study, the resistant rate of clarithromycin of H. pylori was 36.7% (29/79). A2143G and T2182C were the major mutations among the 29 strains with clarithromycin resistance. The frequency of A2143G in sensitive strains was significantly lower than that in resistant strains (45.5 vs 82.8%), while the frequency of T2182C had not reached significant difference between in sensitive strains and in resistant strains (90.9 vs 89.7%), indicating that clarithromycin resistance might be associated with A2143G mutation in children. A study in adults from the same district in Zhejiang Province showed that all of phenotype-resistant strains (n=6) presented mutation A to G at position 2143 of the 23S rRNA, while 2 mutant-type of 23S rRNA gene at position 2143 (A>G) was also detected in sic phenotype-susceptible strains.22 Another study in adults from the same area showed that 90.4% gene mutations of the 23S rRNA were the A2143G mutation.23 H. pylori strains were found to carry A2143G, A2142G, A2147G and A2146G mutations that can lead to clarithromycin-resistance in Africa, Asia, South America, Europe and North America.24–30 The T2183C and A2223G transformations have been frequently found to be the cause of observed clarithromycin resistance in Asian countries than those in Europe and North America,31 but not be observed in our study. In addition to these mutations, other mutations in different positions have been found in other parts of the world to confer clarithromycin resistance in H. pylori strains (T2182C, T2190C, C2195T, A2223G, G2141A, C2694A, G2224A, C2245T, T2289C).30 The T2182C was detected in this study both in sensitive strains and in resistant strains, which were identified with low resistance level in other studies, and were detected in most of the strains in China for geographical and genetic factors.22,32,33
The resistant rate of metronidazole to H. pylori was 68.4% (54/79), and 28 out of resistant strains had multiple drug resistance. In recent years, many studies believe that mutations in NADPH rdxA and frxA genes are the main causes of metronidazole resistance. In this study, the mutation frequency of rdxA gene G47A mutation in resistant strains was 20.4% (11/54), and T184G mutation 70.4% (38/54). However, a mutation rate of T184G in sensitive strains was 83.3% (5/6), but no G47A mutation was identified. Luo et al reported that 87.2% of the resistant strains identified in the Guiyang Medical College contained 4 fixed-site mutations in their rdxA gene, and that might be associated with H. pylori resistance to metronidazole.34 Mirzaei et al suggested that the W(209)R mutation within rdxA might be related to metronidazole resistance.35 Tanih et al identified 13 amino acid alterations at 9 sites, and truncations at 14 sites within the rdxA gene of metronidazole-resistant strains.36 The mutation frequency of frxA gene A48G mutations in resistant strains was 70% (30/43), while A48G mutation was also identified from all 6 sensitive strains. With these different mutations, more studies are needed to verify which mutations are related to drug resistance.
Point mutations at Asp-91 and Asn-87 in the quinolone-resistance determining region of gyrase are the key to drug resistance.37–39 In this study, 3 out of the 12 levofloxacin-resistant strains carried mutations at Asp-91, and another 10 had mutations at Asn-87, but 6 out of the 12 sensitive strains also had Asn-87 mutations but not Asp-91 mutations. Thus, we speculate that Asp-91 mutation might be a key point to the resistance of H. pylori. One study in adults from the same district in Zhejiang Province showed that the N87K mutation was the predominant mutation in the 14 levofloxacin-resistant isolates with gyrA mutations, while only 2 of the 29 isolates with gyrA mutations contained the D91G mutation, and these 2 isolates were susceptible to levofloxacin.23 The results were not consistent with our results in levofloxacin-resistant gene mutations. Binkowska et al reported that the most common mutation presented in 40% of H. pylori strains resistant to levofloxacin was a change at position 91 of gyrA in children.25 De Palma et al reported that resistance of levofloxacin was due to substitution at position 87 (K,I) and 91 (G,N,A) of gyrA QRDR in the 92.8% of the resistant isolates.40 Miftahussurur et al reported that mutations at Asn-87 and/or Asp-91 were predominantly in levofloxacin-resistant strains, and the gyrB mutation had a steady relationship with gyrA 87–91 mutations.41 None of the substitutions found in gyrB proved conferring resistance in this study. These findings revealed that the mutations of genes related to H. pylori resistance are diversified, especially in children.
In conclusion, in H. pylori resistant strains isolated from children in China, most mutations occurred at A2143G of the 23S rRNA gene for clarithromycin; G47A mutation of rdxA gene for metronidazole; and at 91 mutation of gyrA gene for levofloxacin. It is suggested that susceptibility testing together with screening the mutation of antimicrobial-resistant gene prior to treatment is important for future clinical practice. Further studies of H. pylori resistant gene mutation and its relationship to H. pylori resistance to antibiotics should be highlighted in the eradication of H. pylori in children.
Acknowledgments
This study was sponsored by the National Natural Science Foundation of China (81270459). We thank Zheng Shen for data analysis.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Marshall BJ, Warren JR. Unidentified curved bacilli in the stomach of patients with gastritis and peptic ulceration. Lancet. 1984;1:1311–1315. doi:10.1016/s0140-6736(84)91816-6
2. McColl KE. Clinical practice. helicobacter pylori infection. N Engl J Med. 2010;362:1597–1604. doi:10.1056/NEJMcp1001110
3. Francois F, Blaser MJ. Improving helicobacter pylori eradication regimens. Ann Intern Med. 2006;144:140–141. doi:10.7326/0003-4819-144-2-200601170-00013
4. Brown LM. Helicobacter pylori: epidemiology and routes of transmission. Epidemiol Rev. 2000;22:283–297. doi:10.1093/oxfordjournals.epirev.a018040
5. Xiang L, Zhu X, Huang D, Meng L, Wang L. Analysis on infection and drug resistance of helicobacter pylori in patients with gastric diseases. Chin J Nosocomiol. 2015;25:1710–1711.
6. Bayerdorffer E, Neubauer A, Rudolph B, et al. Regression of primary gastric lymphoma of mucosa-associated lymphoid tissue type after cure of helicobacter pylori infection. MALT lymphoma study group. Lancet. 1995;345:1591–1594. doi:10.1016/s0140-6736(95)90113-2
7. Zhang YX, Zhou LY, Song ZQ, Zhang JZ, He LH, Ding Y. Primary antibiotic resistance of helicobacter pylori strains isolated from patients with dyspeptic symptoms in Beijing: a prospective serial study. World J Gastroenterol. 2015;21:2786–2792. doi:10.3748/wjg.v21.i9.2786
8. Shu X, Yin G, Liu M, Peng K, Zhao H, Jiang M. Antibiotics resistance of helicobacter pylori in children with upper gastrointestinal symptoms in Hangzhou, China. Helicobacter. 2018;23(3):e12481. doi:10.1111/hel.12481
9. Megraud F, Lehours P. Helicobacter pylori detection and antimicrobial susceptibility testing. Clin Microbiol Rev. 2007;20:280–322. doi:10.1128/cmr.00033-06
10. Megraud F, Benejat L, Ontsira Ngoyi EN, Lehours P. Molecular approaches to identify helicobacter pylori antimicrobial resistance. Gastroenterol Clin North Am. 2015;44:577–596. doi:10.1016/j.gtc.2015.05.002
11. Thung I, Aramin H, Vavinskaya V, et al. Review article: the global emergence of helicobacter pylori antibiotic resistance. Aliment Pharmacol Ther. 2016;43:514–533. doi:10.1111/apt.13625
12. Matteo MJ, Perez CV, Domingo MR, Olmos M, Sanchez C, Catalano M. DNA sequence analysis of rdxA and frxA from paired metronidazole-sensitive and -resistant helicobacter pylori isolates obtained from patients with heteroresistance. Int J Antimicrob Agents. 2006;27:152–158. doi:10.1016/j.ijantimicag.2005.09.019
13. Tu IF, Liao JH, Yang FL, Lin NT, Chan HL, Wu SH. Lon protease affects the RdxA nitroreductase activity and metronidazole susceptibility in helicobacter pylori. Helicobacter. 2014;19:356–366. doi:10.1111/hel.12140
14. Lee JW, Kim N, Nam RH, et al. Mutations of helicobacter pylori associated with fluoroquinolone resistance in Korea. Helicobacter. 2011;16:301–310. doi:10.1111/j.1523-5378.2011.00840.x
15. Garcia M, Raymond J, Garnier M, Cremniter J, Burucoa C. Distribution of spontaneous gyrA mutations in 97 fluoroquinolone-resistant helicobacter pylori isolates collected in France. Antimicrob Agents Chemother. 2012;56:550–551. doi:10.1128/aac.05243-11
16. Rimbara E, Noguchi N, Kawai T, Sasatsu M. Fluoroquinolone resistance in helicobacter pylori: role of mutations at position 87 and 91 of GyrA on the level of resistance and identification of a resistance conferring mutation in Gyr B. Helicobacter. 2012;17:36–42. doi:10.1111/j.1523-5378.2011.00912.x
17. Su P, Li Y, Li H, et al. Antibiotic resistance of helicobacter pylori isolated in the Southeast Coastal Region of China. Helicobacter. 2013;18:274–279. doi:10.1111/hel.12046
18. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing: Seventeenth Informational Supplement M100-S17. Wayne, PA, USA: CLSI; 2007.
19. Ribeiro ML, Vitiello L, Miranda MC, et al. Mutations in the 23S rRNA gene are associated with clarithromycin resistance in helicobacter pylori isolates in Brazil. Ann Clin Microbiol Antimicrob. 2003;2:11. doi:10.1186/1476-0711-2-11
20. Marais A, Bilardi C, Cantet F, Mendz GL, Mégraud F. Characterization of the genes rdxA and frxA involved in metronidazole resistance in helicobacter pylori. Res Microbiol. 2003;154:137–144. doi:10.1016/s0923-2508(03)00030-5
21. Wang LH, Cheng H, Hu FL, Li J. Distribution of gyrA mutations in fluoroquinolone-resistant helicobacter pylori strains. World J Gastroenterol. 2010;16:2272–2277. doi:10.3748/wjg.v16.i18.2272
22. Chen J, Ye L, Jin L, et al. Application of next-generation sequencing to characterize novel mutations in clarithromycin-susceptible helicobacter pylori strains with A2143G of 23S rRNA gene. Ann Clin Microbiol Antimicrob. 2018;17:10. doi:10.1186/s12941-018-0259-8
23. Zhang J, Zhong J, Ding J, et al. Simultaneous detection of human CYP2C19 polymorphisms and antibiotic resistance of helicobacter pylori using a personalized diagnosis kit. J Glob Antimicrob Resist. 2018;13:174–179. doi:10.1016/j.jgar.2017.12.018
24. Mahmoudi S, Mamishi S, Banar M, et al. Antibiotic susceptibility of helicobacter pylori strains isolated from Iranian children: high frequency of A2143G point mutation associated with clarithromycin resistance. J Glob Antimicrob Resist. 2017;10:131–135. doi:10.1016/j.jgar.2017.04.011
25. Binkowska A, Biernat MM, Kaczmariski K, Gosciniak G. Molecular patterns of resistance among helicobacter pylori strains in South-Western Poland. Front Microbiol. 2018. doi:10.3389/fmicb.2018.03154
26. Quek C, Pham ST, Tran KT, et al. Antimicrobial susceptibility and clarithromycin resistance patterns of helicobacter pylori clinical isolates in Vietnam. F1000Research. 2016;5:671. doi:10.12688/f1000research.8239.1
27. Cagan-Appak Y, Gazi H, Ayhan S, Cengiz-Ozyurt B, Kurutepe S, Kasirga E. Clarithromycin resistance and 23S rRNA gene point mutations of helicobacter pylori infection in children. Turk J Pediatr. 2016;58:371–376. doi:10.24953/turkjped.2016.04.004
28. De Francesco V, Margiotta M, Zullo A, et al. Clarithromycin-resistant genotypes and eradication of helicobacter pylori. Ann Intern Med. 2006;144:94–100. doi:10.1016/j.jpeds.2010.02.007
29. Phan TN, Santona A, Tran VH, et al. High rate of levofloxacin resistance in h background of clarithromycin and metronidazole-resistant helicobacter pylori in vietnam. Inter J Antimicrob Agents. 2015;45:244–248. doi:10.1016/j.ijantimicag.2014.10.019
30. Jaka H, Rhee JA, Ostlundh L, et al. The magnitude of antibiotic resistance of helicobacter pylori in Africa and identified mutations which confer resistance to antibiotics: a systematic review and meta-analysis. BMC Infect Dis. 2018;18:193. doi:10.1186/s12879-018-3099-4
31. Ieradi E, Giorgio F, Lousurdo G, Di Leo A, Principi M. How antibiotic resistances could change helicobacter pylori treatment: A matter of geography? World J Gastroenterol. 2013;19:8168–8180. doi:10.3748/wjg.v19.i45.8168
32. Kim KS, Kang JO, Eun CS, Han DS, Choi TY. Mutations in the 23S rRNA gene of helicobacter pylori associated with clarithromycin resistance. J Korean Med Sci. 2002;17:599–603. doi:10.3346/jkms.2002.17.5.599
33. Fock KM, Ang TL. Epidemiology of helicobacter pylori infection and gastric cancer in Asia. J Gastroenterol Hepatol. 2010;25:479–486. doi:10.1111/j.1440-1746.2009.06188.x
34. Luo Z, Zhang S, Sun Z, et al. Study on relationship between drug resistance of helicobacter pylori to metronidazole and rdx A genotype and cagA gene. Chin Hosp Pharm J. 2015;35:689–694. doi:10.1016/j.jms.2008.06.014
35. Mirzaei N, Poursina F, Moghim S, Rahimi E, Safaei HG. The mutation of the rdxA gene in metronidazole-resistant helicobacter pylori clinical isolates. Adv Biomed Res. 2014;3:90. doi:10.4103/2277-9175.128469
36. Tanih NF, Ndip LM, Ndip RN. Characterisation of the genes encoding resistance to metronidazole (rdxA and frxA) and clarithromycin (the 23S-rRNA genes) in South African isolates of helicobacter pylori. Ann Trop Med Parasitol. 2011;105:251–259. doi:10.1179/136485911X12899838683485
37. Miyachi H, Miki I, Aoyama N, et al. Primary levofloxacin resistance and gyrA/B mutations among helicobacter pylori in Japan. Helicobacter. 2006;11:243–249. doi:10.1111/j.1523-5378.2006.00415.x
38. Chisholm SA, Owen RJ. Frequency and molecular characteristics of ciprofloxacin-and rifampicin-resistant helicobacter pylori from gastric infections in the UK. J Med Microbiol. 2009;58:1322–1328. doi:10.1099/jmm.0.011270-0
39. Tankovic J, Lascols C, Sculo Q, Petit JC, Soussy CJ. Single and double mutations in gyrA but not in gyrB are associated with low-and high-level fluoroquinolone resistance in helicobacter pylori. Antimicrob Agents Chemother. 2003;47:3942–3944. doi:10.1128/AAC.47.12.3942-3944.2003
40. De Palma GZ, Mendiondo N, Wonaga A, et al. Occurrence of mutations in the antimicrobial target genes related to levofloxacin, clarithromycin, and amoxicillin resistance in helicobacter pylori isolates from Buenos Aires city. Microb Drug Resist. 2016;23:351–358. doi:10.1089/mdr.2015.0361
41. Miftahussurur M, Shrestha PK, Subsomwong P, Sharma RP, Yamaoka Y. Emerging helicobacter pylori levofloxacin resistance and novel genetic mutation in Nepal. BMC Microbiol. 2016;16:256. doi:10.1186/s12866-016-0873-6
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.