Back to Journals » Cancer Management and Research » Volume 10
Musculoskeletal complication in kaposiform hemangioendothelioma without Kasabach–Merritt phenomenon: clinical characteristics and management
Authors Ji Y ![]() , Yang K, Chen S, Peng S, Lu G, Liu X
, Yang K, Chen S, Peng S, Lu G, Liu X
Received 15 April 2018
Accepted for publication 25 June 2018
Published 7 September 2018 Volume 2018:10 Pages 3325—3331
DOI https://doi.org/10.2147/CMAR.S171223
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Kenan Onel
Yi Ji,1 Kaiying Yang,1 Siyuan Chen,2 Suhua Peng,1 Guoyan Lu,3 Xingtao Liu4
1Division of Oncology, Department of Pediatric Surgery, West China Hospital of Sichuan University, Chengdu, China; 2Pediatric Intensive Care Unit, Department of Critical Care Medicine, West China Hospital of Sichuan University, Chengdu, China; 3Department of Pediatrics, Pediatric Intensive Care Unit, West China Second University Hospital, Sichuan University, Chengdu, China; 4Department of Vascular and Interventional Radiology, Chengdu Women and Children’s Central Hospital, Chengdu, China
Purpose: Musculoskeletal complications have been associated with kaposiform hemangioendothelioma (KHE) and can lead to disability and reduced quality of life. We aimed to determine the clinical characteristics of musculoskeletal complication in patients with KHE without Kasabach–Merritt phenomenon (KMP) in order to identify features that may aid clinicians in KHE treatment.
Patients and methods: We conducted a cohort study of KHE without KMP associated with musculoskeletal complication between January 2006 and February 2017 at three tertiary medical centers in China. The study included 29 nonthrombocytopenic patients with KHE and musculoskeletal complication.
Results: The mean age at diagnosis of KHE was 4.5 years (range, 0.3–50.0 years). The mean follow-up was 4.1 years (range, 0.5–9.0 years). In most cases (72.4%), decreased range of motion (ROM) appeared within 2 years of KHE onset. Associated chronic pain was reported in 12 patients. Bone–joint changes were common in patients with decreased ROM (75.9%). All the patients received at least one medical therapy including corticosteroids, vincristine, propranolol, and sirolimus. Sirolimus demonstrated the highest efficacy rate, with 94.7% of patients showing improvements in ROM and chronic pain.
Conclusion: Musculoskeletal complication can occur early in the disease course of KHE without KMP. Although no uniformly effective treatment modality was found, sirolimus demonstrated the best response in patients with KHE with decreased ROM and chronic pain.
Keywords: kaposiform hemangioendothelioma, musculoskeletal disorders, clinical characteristics, complication, sirolimus
Introduction
Kaposiform hemangioendothelioma (KHE) is a rare, locally aggressive, and nonmetastatic vascular tumor of intermediate malignancy. The annual incidence of KHE has been estimated at 0.071 per 100,000 children.1 In contrast to infantile hemangiomas, which have a tendency to spontaneously regress, KHE shows a highly invasive behavior with a very low tendency to resolve spontaneously. Clinically, KHE has high mortality and morbidity rates, primarily due to local invasion characteristics, compressive effects, or the life-threatening complication known as Kasabach–Merritt phenomenon (KMP). KMP is profound thrombocytopenia with hypofibrinogenemia resulting from intralesional platelet activation, trapping, and consumption.2–4
The outcome of KHE is strongly influenced by tumor characteristics, timing of diagnosis, and initiation of appropriate treatment.5,6 The infiltrative nature of the tumor, risk of bleeding, and anatomic site of the lesion can make complete surgical removal difficult or impossible. Clinically, the management of high-risk patients is very challenging. Several different approaches, including various medical therapy regimens, have been described, but they have shown variable degrees of success.7,8 The destructive growth patterns of the tumor and the development of muscular and periarticular fibrosis can cause pain and functional limitations, all of which may affect patients’ abilities to perform routine daily activities,9 potentially leading to a substantial decrease in quality of life.
Musculoskeletal complications in KHE without KMP have received less attention in clinical research than the life-threatening complications associated with KMP (eg, thrombocytopenia, acquired hypofibrinogenemia, and severe anemia), and the decreased range of motion (ROM) is likely underappreciated in clinical practice. Currently, there is a paucity of literature specifically addressing musculoskeletal complications in patients with KHE. Therefore, the purpose of this study was to investigate the features of musculoskeletal complication in KHE without KMP to improve our understanding of this rare disease.
Patients and methods
From January 2006 to February 2017, a descriptive study was conducted across three tertiary medical centers in China. The study was approved by the Ethics Committee of the West China Hospital of Sichuan University, the study site of the principal investigator, and by the local institutional review boards at each participating site. Patients were included if they 1) had verified KHE by pathological examination; 2) showed decreased ROM; 3) had no history of KMP; 4) had given written informed consent or patients’ parents had given the consent for their clinical records to be used in this study; and 5) had a minimum of 6 months of follow-up.
Clinical data including demographics, clinical presentation, anatomic location, laboratory results, imaging results, pathology reports, follow-up examinations, and outcome were obtained. Diagnosis of KHE was based on clinical presentation, imaging, and histopathologic examination. All patients underwent incisional biopsy or punch biopsy during diagnostic workup. Thrombocytopenia is the most definitive and distinguishing factor associated with KMP symptoms. We defined KMP as a platelet count of <100×109/L.1 In addition to the ultrasound results, the available radiology database was queried for magnetic resonance imaging data. Based on our previous studies, KHE was typed according to the depth of infiltration as determined by radiographic findings and designated as superficial, mixed, or deep.10,11
Decreased ROM was defined as ≥10° of extension loss, flexion <120°, or both. Associated chronic pain was defined as daily pain for at least 3 months. ROM measurements were performed using standard goniometers. To determine intrarater reliability, goniometer measurements were performed twice for each joint. A targeted history was obtained by trained study coordinators, with questions addressing signs and symptoms related to musculoskeletal complication. Based on previous studies, the severity of musculoskeletal complication was scored by using a 4-point scale: 1, asymptomatic or mild symptoms, clinical or diagnostic observations only; 2, moderate symptoms, limiting age-appropriate instrumental activities of daily living; 3, severe or medically significant symptoms, disabling or limiting self-care activities of daily living; and 4, life-threatening consequences, with urgent intervention indicated. Higher values represent more profound functional disability or symptoms.10
Treatment responses were evaluated at the initiation of each treatment regimen, at 1, 2, 3, and 6 months after treatment, at each scheduled visit, and at the last available visit. Successful treatment responses were defined as an improvement in the patient’s signs and/or symptoms. According to previous studies, improvement in signs and/or symptoms was defined as a decrease in the severity score of ≥1.10
Results
Twenty-nine patients were considered to have decreased ROM related to KHE. None of these patients had a history of KMP. Nearly all were referred because of KHE complexity and/or musculoskeletal complication. The demographic and clinical characteristics of these patients are presented in Table 1. The sex distribution was 16 males and 13 females. The age at diagnosis of KHE ranged from 3.5 months to 50 years, with a mean age at diagnosis of 4.5 years.
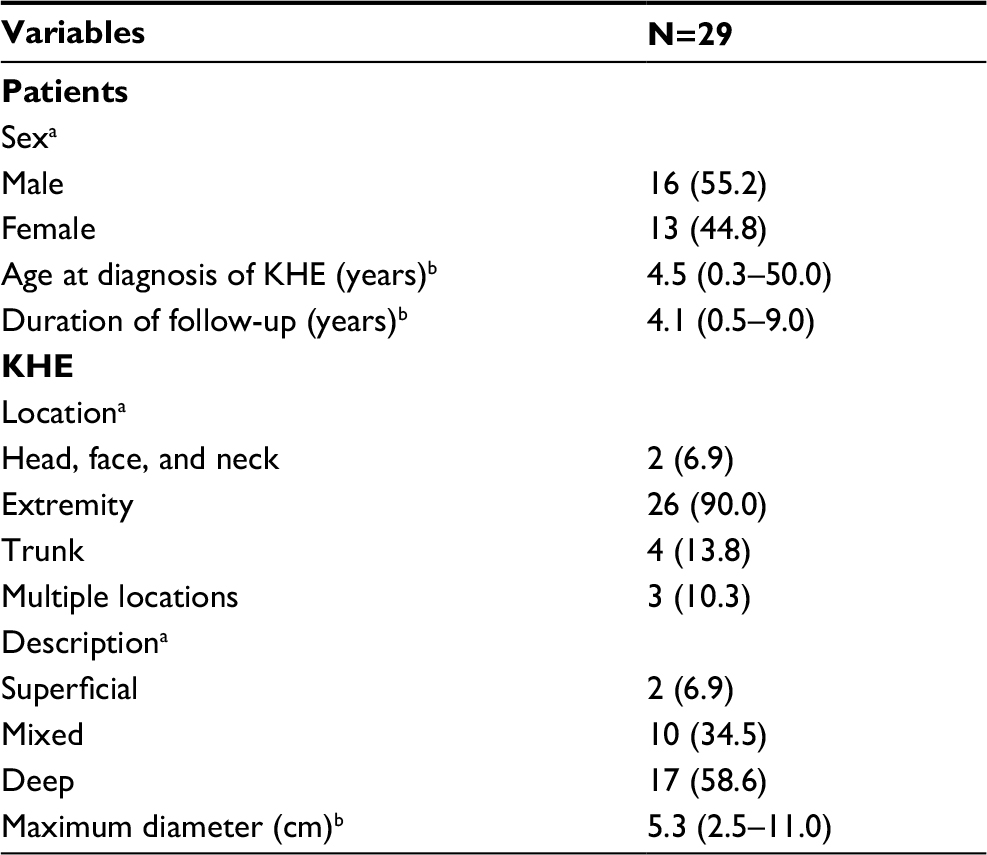 | Table 1 Demographics and clinical characteristics of KHE with decreased ROM without KMP Notes: aValues are presented as the number (%). bValues are presented as the mean (range). Abbreviations: KHE, kaposiform hemangioendothelioma; KMP, Kasabach–Merritt phenomenon; ROM, range of motion. |
Twenty-six lesions (90.0%) involved the extremities. Three patients had multiple locations where the KHE lesions extended into more than one anatomic region: one patient had lesion involving both neck and trunk and two patients had lesions involving both trunk and extremity. The maximum diameter of the lesions ranged from 2.5 to 11.0 cm (mean, 5.3 cm). Ten patients (34.5%) had mixed-type KHE. These cutaneous lesions infiltrated deeply into muscles, bones, and joints. Two patients had superficial lesions on the knee involving the dermis, subcutaneous tissue, and deep fascia. The remaining 17 patients had lesions confined to the involved muscle–bone–joint regions. The most commonly involved joints were the knees, followed in order of decreasing frequency by the shoulders and hip joints. Bone–joint changes, including bone–joint erosion or destruction, were noted in 22 cases (75.9%; Figure 1).
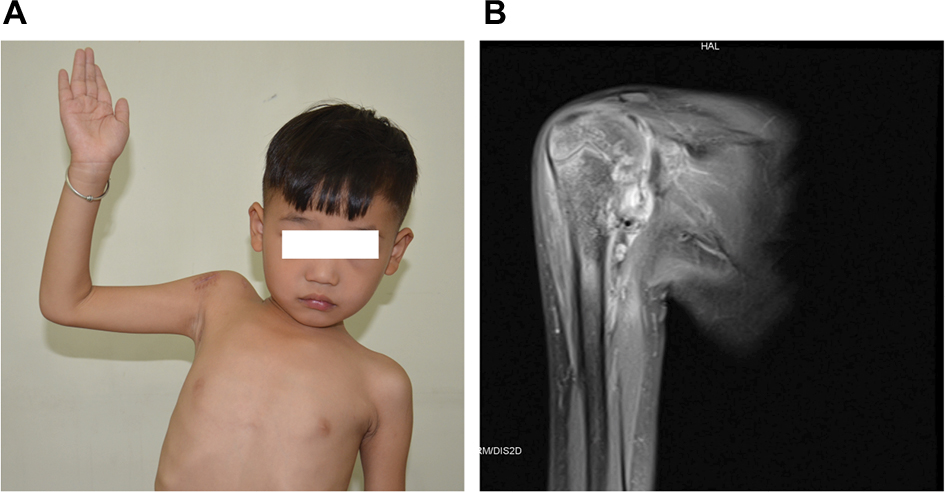 | Figure 1 Deep KHE with bone–joint erosion. Notes: (A) A 6-year-old boy with decreased right shoulder ROM for 3 years. (B) Coronal T2-weighted MRI shows a deep lesion with marked abnormal enhancement at the proximal humerus, glenoid cavity, scapula, and the surrounding soft tissue. Abbreviations: KHE, kaposiform hemangioendothelioma; MRI, magnetic resonance imaging; ROM, range of motion. |
Eight patients (27.6%) did not have decreased ROM at the initial evaluation, but developed ROM decreases thereafter. In the remaining patients (72.4%), decreased ROM was identified within 2 years of KHE onset. Only 2 (2/29, 6.9%) patients reported decreased ROM before the age of 12 months. Associated chronic pain was reported in 12 patients, including 4 of 5 patients with lesions involving the spine. Over the study period’s mean follow-up time of 4.1 years (range 0.5–9.0 years), the highest severity scores in each patient ranged from 1 to 4, with a mean highest score of 2.8.
All patients received at least one medical therapy. In eight cases, multiple agents were given in sequence: these patients received at least two different medical therapies. Corticosteroids were used in eight patients, six of whom did not show an improvement in associated musculoskeletal complications, requiring a switch to partial resection and orthopedic physical therapy (three) or sirolimus (three). Vincristine monotherapy was used in seven patients, with three showing definite improvement of ROM. The four patients who did not respond to vincristine underwent treatment including surgical excision (two), partial resection and orthopedic physical therapy (one), and sirolimus (one). Propranolol was used in three patients, all of whom suffered from progressive enlargement of their tumors and ongoing decreased ROM (Table 2).
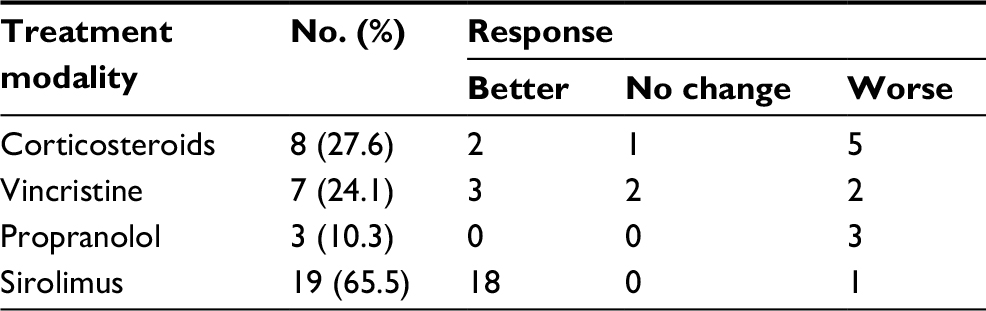 | Table 2 Management of KHE with decreased ROM without KMP Note: Eight patients received at least two different medical therapies, which were given in sequence. Abbreviations: KHE, kaposiform hemangioendothelioma; KMP, Kasabach–Merritt phenomenon; ROM, range of motion. |
Oral sirolimus was used in 19 patients, including 7 patients who had been treated with drugs described above: corticosteroids (3), vincristine (1), and propranolol (3). All but one of the patients showed improvement (Figure 2). The size of the lesions was significantly reduced, with rapid improvements in ROM (Figure 3). In eight patients with chronic pain, significant pain relief was obtained within 3 months of sirolimus treatment. At the last follow-up, eleven patients had been successfully tapered off sirolimus treatment. The mean duration of sirolimus therapy in these patients was 26.0 months (range, 17–36 months). One patient who was tapered and discontinued from sirolimus after 18 months of treatment showed newly diagnosed decrease in ROM. Additional courses of sirolimus were administered with subsequent improvement.
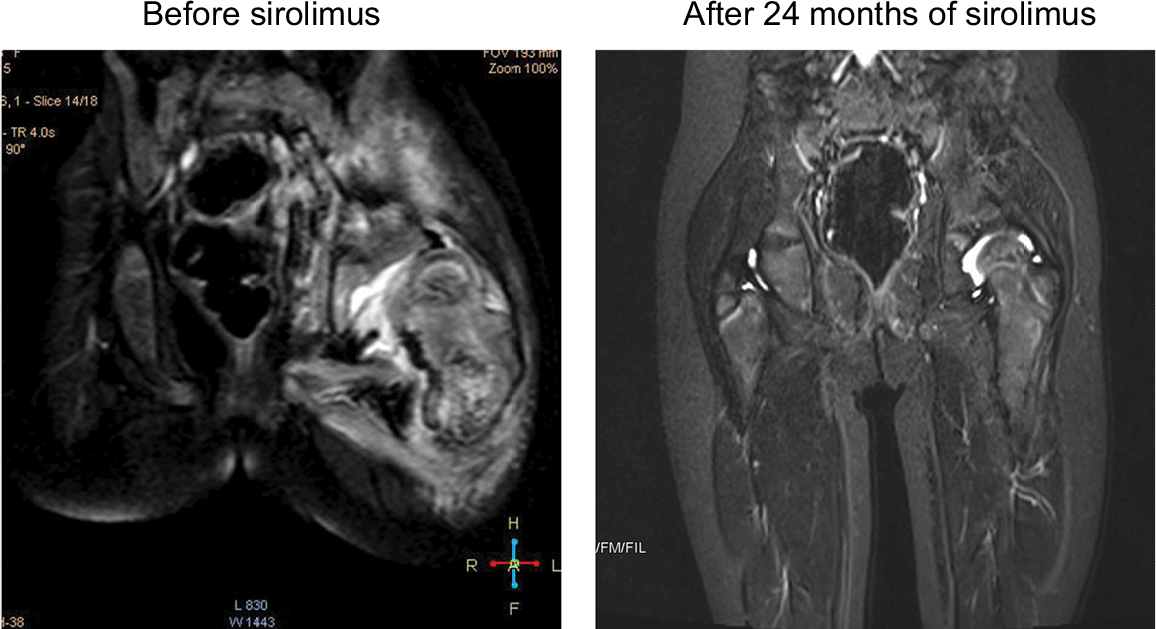 | Figure 2 MRI changes in KHE with decreased hip ROM before and at 24 months after treatment. Notes: A 2.2-year-old girl demonstrated progressively decreased hip ROM for 12 months (left). Coronal T2-weighted MRI revealed a deep lesion infiltrating the proximal femur and ilium. MRI at 24.0 months after sirolimus treatment revealed nearly complete involution of the lesion (right). Abbreviations: KHE, kaposiform hemangioendothelioma; MRI, magnetic resonance imaging; ROM, range of motion. |
 | Figure 3 MRI changes in KHE with decreased knee ROM before and at 12 and 24 months after treatment. Notes: A 1-year-old boy had pathologically confirmed KHE involving the right ankle. The boy demonstrated progressively decreasing knee ROM for 6 months despite treatment with oral propranolol. MRI revealed the superficial lesion infiltrating the subcutaneous tissue and deep fascia (left). The patient received 12.0 months of sirolimus monotherapy (middle). MRI revealed a partial involution of the lesion. At 3-years of age, MRI showed obvious tumor shrinkage (right). Abbreviations: KHE, kaposiform hemangioendothelioma; MRI, magnetic resonance imaging; ROM, range of motion. |
Discussion
Previous studies have demonstrated that decreased ROM is a complication of KHE.12–15 We present the clinical features of decreased ROM in a sample of 29 KHE without KMP, which has rarely, if ever, been previously reported. Using this well-characterized cohort of KHE patients, we show that decreased ROM and associated chronic pain may be common in KHE without KMP. To the best of our knowledge, this is the largest study that assesses the clinical feature and treatment of musculoskeletal complication in KHE. In addition, this is the first study that assesses the efficacy of different treatment regimens in KHE. We hope that the information gained in this study will help improve the diagnosis and treatment of KHE and associated musculoskeletal complications to ultimately improve patients’ quality of life.
The majority of KHEs with decreased ROM but without KMP were mixed and deep lesions, but a significant minority of KHEs consisted of superficial lesions. Decreased ROM was commonly seen in patients with KHE involving the extremities, with a majority of these lesions located on or adjacent to large joints. Patients may become debilitated over time by decreases in ROM at the involved site. We also found that decreased ROM occurred most commonly in older children and adults, with only 6.9% of the patients showing decreased ROM before 12 months of age. Interestingly, the lesions involving spine did seem to result in significant pain and disability. This is important. Perhaps these patients should be treated more aggressively at the outset even in the absence of KMP.
We demonstrated that decreased ROM did occur in several patients who attained partial tumor involution. We suspect that decreased ROM may be an independent complication of therapy, which is consistent with the results of previous studies.6 In addition, decreased ROM can occur early in the disease course. Our study provides novel data showing that decreased ROM typically presented within 2 years of KHE onset. The precise etiology of KHE-associated decreases in ROM remains uncertain. Tumor infiltration of the muscles, connective tissues, and joint structures can alter the structural matrix and mechanical properties of these tissues, leading to diffuse muscle fibrosis and joint contracture.16 Clinically, the stabilization of lesions and/or hematological parameters did not indicate complete and durable remission. In most patients, the lesion was still present even after long-term treatment.6,14 Pathologically, all residual lesions are characterized by progressive fibrosis.17 We suspect that in addition to the location and infiltrative characteristics of the tumor, unknown biological differences likely influence the development of subsequent fibrosis. Experimental evidence has demonstrated that platelet trapping in different tissues and organs is correlated with the development of fibrosis with inflammation.18,19 Interestingly, the microscopic characteristics of KHE without KMP were the same as those observed in patients with KMP. Notably, platelet trapping and hematoma formation were also observed histologically in patients with normal serum platelet levels.6,17 It is possible that platelet trapping in muscle and joint structures during KHE infiltration can activate fibrotic pathways.
Clinically, no individual therapeutic modality has been found to be uniformly effective in treating symptomatic musculoskeletal complications.20 Poor responses to treatment appeared to be associated with long-term complications. Over the past several years, our treatment approach has evolved with the advent of new pharmacologic treatment regimens, which have been reported to be effective. Previously, we and others have revealed that many patients respond well to sirolimus.7,10,21–24 In the present study, sirolimus was found to show the highest efficacy rate in our cohort. A treatment switch from conventional drugs to sirolimus improved therapeutic efficacy. Some of the most impressive improvements were seen in patients with decreased ROM and chronic pain, which is consistent with previous reports.10,16 The mechanisms underlying the therapeutic effect of sirolimus on these symptomatic musculoskeletal complications have not been elucidated. Previous studies have shown that sirolimus reduced profibrotic gene expression in both experimental and clinical settings.25 In addition, reports from various groups have demonstrated that sirolimus reduced fibrosis and attenuated disease progression in multiple animal models.26–29 Therefore, an attractive possibility is that the therapeutic effects of sirolimus in KHE with decreased ROM may prevent both the initiation and progression of established fibrosis and associated alterations in musculoskeletal mechanics.
Currently, there is no definite treatment guideline for the long-term observation of patients with KHE. In the present study, we found that more than one-fourth of patients did not experience musculoskeletal complication at the initial assessment. We advocate for at least annual visits to monitor for musculoskeletal complications. For lesions at high risk of causing mid- or long-term functional complications, patients and their families should be educated about potential symptoms and the need for observation. Further study is needed to evaluate the precise duration of treatment required to avoid long-term complications. For certain cases, maintenance treatment with sirolimus monotherapy should be evaluated. In this regard, various studies have demonstrated that a relatively low dose of sirolimus can markedly ameliorate the development of inflammation and fibrogenesis.30,31
Conclusion
This is the largest study assessing the clinical characteristics and treatment of musculoskeletal complication in KHE patients. We demonstrate that musculoskeletal complications may be common in patients with KHE without KMP. In addition, our data demonstrate that sirolimus therapy can improve outcomes in patients with musculoskeletal complication. Nonetheless, better treatments are needed to improve the life expectancy of KHE and associated musculoskeletal complication. Surveillance for musculoskeletal complications should be added as a recommendation to the routine care and follow-up schedule of patients with KHE. Given the rarity of KHE, an international collaborative effort may be able to shed new insights regarding the demographics, etiology, management, and prognosis of patients with KHE.
Acknowledgments
This work was supported by grants from the National Natural Science Foundation of China (grant numbers: 81401606 and 81400862) and the Science Foundation for Excellent Youth Scholars of Sichuan University (grant number: 2015SU04A15). The authors would like to thank patients’ parents for their cooperation and support and for providing their consent regarding the publication of this manuscript. Written informed consents for publication of this study and accompanying images were obtained from the patients’ parents.
Disclosure
The authors report no conflicts of interest in this work.
References
Croteau SE, Liang MG, Kozakewich HP, et al. Kaposiform hemangioendothelioma: atypical features and risks of Kasabach–Merritt phenomenon in 107 referrals. J Pediatr. 2013;162(1):142–147. | ||
Enjolras O, Wassef M, Mazoyer E, et al. Infants with Kasabach–Merritt syndrome do not have “true” hemangiomas. J Pediatr. 1997;130(4):631–640. | ||
Sarkar M, Mulliken JB, Kozakewich HP, Robertson RL, Burrows PE. Thrombocytopenic coagulopathy (Kasabach–Merritt phenomenon) is associated with kaposiform hemangioendothelioma and not with common infantile hemangioma. Plast Reconstr Surg. 1997;100(6):1377–1386. | ||
O’Rafferty C, O’Regan GM, Irvine AD, Smith OP. Recent advances in the pathobiology and management of Kasabach–Merritt phenomenon. Br J Haematol. 2015;171(1):38–51. | ||
Fernandez-Pineda I, Lopez-Gutierrez JC, Chocarro G, Bernabeu-Wittel J, Ramirez-Villar GL. Long-term outcome of vincristine-aspirin-ticlopidine (VAT) therapy for vascular tumors associated with Kasabach–Merritt phenomenon. Pediatr Blood Cancer. 2013;60(9):1478–1481. | ||
Enjolras O, Mulliken JB, Wassef M, et al. Residual lesions after Kasabach–Merritt phenomenon in 41 patients. J Am Acad Dermatol. 2000;42(2 Pt 1):225–235. | ||
Blatt J, Stavas J, Moats-Staats B, Woosley J, Morrell DS. Treatment of childhood kaposiform hemangioendothelioma with sirolimus. Pediatr Blood Cancer. 2010;55(7):1396–1398. | ||
Liu XH, Li JY, Qu XH, et al. Treatment of kaposiform hemangioendothelioma and tufted angioma. Int J Cancer. 2016;139(7):1658–1666. | ||
Ma J, Shi QL, Jiang SJ, Zhou HB, Zhou XJ. Primary kaposiform hemangioendothelioma of a long bone: two cases in unusual locations with long-term follow up. Pathol Int. 2011;61(6):382–386. | ||
Ji Y, Chen S, Xiang B, et al. Sirolimus for the treatment of progressive kaposiform hemangioendothelioma: a multicenter retrospective study. Int J Cancer. 2017;141(4):848–855. | ||
Ji Y, Yang K, Peng S, et al. Kaposiform haemangioendothelioma: clinical features, complications and risk factors for Kasabach–Merritt phenomenon. Br J Dermatol. Epub 2018 Mar 30. | ||
Fahrtash F, McCahon E, Arbuckle S. Successful treatment of kaposiform hemangioendothelioma and tufted angioma with vincristine. J Pediatr Hematol Oncol. 2010;32(6):506–510. | ||
Uno T, Ito S, Nakazawa A, Miyazaki O, Mori T, Terashima K. Successful treatment of kaposiform hemangioendothelioma with everolimus. Pediatr Blood Cancer. 2015;62(3):536–538. | ||
Schaefer BA, Wang D, Merrow AC, Dickie BH, Adams DM. Long-term outcome for kaposiform hemangioendothelioma: a report of two cases. Pediatr Blood Cancer. 2017;64(2):284–286. | ||
Gruman A, Liang MG, Mulliken JB, et al. Kaposiform hemangioendothelioma without Kasabach–Merritt phenomenon. J Am Acad Dermatol. 2005;52(4):616–622. | ||
Oza VS, Mamlouk MD, Hess CP, Mathes EF, Frieden IJ. Role of sirolimus in advanced kaposiform hemangioendothelioma. Pediatr Dermatol. 2016;33(2):e88–e92. | ||
Lyons LL, North PE, Mac-Moune Lai F, Stoler MH, Folpe AL, Weiss SW. Kaposiform hemangioendothelioma: a study of 33 cases emphasizing its pathologic, immunophenotypic, and biologic uniqueness from juvenile hemangioma. Am J Surg Pathol. 2004;28(5):559–568. | ||
Fujita M, Mason RJ, Cool C, Shannon JM, Hara N, Fagan KA. Pulmonary hypertension in TNF-α-overexpressing mice is associated with decreased VEGF gene expression. J Appl Physiol. 2002;93(6):2162–2170. | ||
O’Sullivan BP, Linden MD, Frelinger AL, et al. Platelet activation in cystic fibrosis. Blood. 2005;105(12):4635–4641. | ||
Drolet BA, Trenor CC, Brandão LR, et al. Consensus-derived practice standards plan for complicated kaposiform hemangioendothelioma. J Pediatr. 2013;163(1):285–291. | ||
Adams DM, Trenor CC, Hammill AM, et al. Efficacy and safety of sirolimus in the treatment of complicated vascular anomalies. Pediatrics. 2016;137(2):e20153257. | ||
Hammill AM, Wentzel M, Gupta A, et al. Sirolimus for the treatment of complicated vascular anomalies in children. Pediatr Blood Cancer. 2011;57(6):1018–1024. | ||
Zhang G, Chen H, Gao Y, Liu Y, Wang J, Liu XY. Sirolimus for treatment of kaposiform haemangioendothelioma with Kasabach–Merritt phenomenon: a retrospective cohort study. Br J Dermatol. 2018;178(5):1213–1214. | ||
Wang C, Li Y, Xiang B, et al. Successful management of pancreatic kaposiform hemangioendothelioma with sirolimus: case report and literature review. Pancreas. 2017;46(5):e39–e41. | ||
Oliveira JG, Xavier P, Sampaio SM, et al. Compared to mycophenolate mofetil, rapamycin induces significant changes on growth factors and growth factor receptors in the early days post-kidney transplantation. Transplantation. 2002;73(6):915–920. | ||
Bonegio RG, Fuhro R, Wang Z, et al. Rapamycin ameliorates proteinuria-associated tubulointerstitial inflammation and fibrosis in experimental membranous nephropathy. J Am Soc Nephrol. 2005;16(7):2063–2072. | ||
Wu MJ, Wen MC, Chiu YT, Chiou YY, Shu KH, Tang MJ. Rapamycin attenuates unilateral ureteral obstruction-induced renal fibrosis. Kidney Int. 2006;69(11):2029–2036. | ||
Korfhagen TR, Le Cras TD, Davidson CR, et al. Rapamycin prevents transforming growth factor-alpha-induced pulmonary fibrosis. Am J Respir Cell Mol Biol. 2009;41(5):562–572. | ||
Zhu J, Wu J, Frizell E, et al. Rapamycin inhibits hepatic stellate cell proliferation in vitro and limits fibrogenesis in an in vivo model of liver fibrosis. Gastroenterology. 1999;117(5):1198–1204. | ||
Neef M, Ledermann M, Saegesser H, Schneider V, Reichen J. Low-dose oral rapamycin treatment reduces fibrogenesis, improves liver function, and prolongs survival in rats with established liver cirrhosis. J Hepatol. 2006;45(6):786–796. | ||
Cruzado JM, Poveda R, Ibernón M, et al. Low-dose sirolimus combined with angiotensin-converting enzyme inhibitor and statin stabilizes renal function and reduces glomerular proliferation in poor prognosis IgA nephropathy. Nephrol Dial Transplant. 2011;26(11):3596–3602. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.