Back to Journals » Journal of Pain Research » Volume 18
Murottal and Classical Music Effect on Pain: Clinical Trial
Authors Prihatno MR ![]() , Perkasa G, Prihartini H, Suryani S, Cahyono ID
, Perkasa G, Prihartini H, Suryani S, Cahyono ID
Received 27 May 2025
Accepted for publication 4 November 2025
Published 7 November 2025 Volume 2025:18 Pages 5941—5946
DOI https://doi.org/10.2147/JPR.S542508
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jinlei Li
MM Rudi Prihatno, Guruh Perkasa, Hermin Prihartini,* Shila Suryani,* Iwan D Cahyono*
Department of Anesthesiology and Intensive Care, Medical Faculty of Jenderal Soedirman University, Purwokerto, Central Java, Indonesia
*These authors contributed equally to this work
Correspondence: MM Rudi Prihatno, Deparment of Anesthesiology and Intensive Care, Medical Faculty of Jenderal Soedirman University, Medica Gumbreg No. 1 Street, Purwokerto, Central Jawa, 53124, Indonesia, Email [email protected]
Background: Indonesia has the highest incidence of fractures in Southeast Asia, reaching 1.3 million cases per year, with a prevalence of 5.5% in 2020, predominantly involving lower extremity fractures. Uncontrolled pain can reduce rehabilitation effectiveness and increase the risk of complications.
Purpose: In some cases, long-term use of analgesics can cause detrimental side effects, necessitating the search for alternatives. Another alternative in this study, adapted to local conditions and culture, is listening to Quranic recitals accompanied by classical music. The objective of this study is to examine the effect of Quranic recitation and classical music on the Numeric Rating Scale (NRS) pain score and interleukin-6 (IL-6) levels in patients undergoing lower extremity orthopedic surgery under intrathecal anesthesia.
Methods: A double-blind, randomized controlled trial (RCT) was conducted at Prof. Dr. Margono Soekarjo Hospital in Purwokerto, Central Java, Indonesia. Patients undergoing elective lower extremity orthopedic surgery who met the inclusion and exclusion criteria were randomly assigned to three groups: Group A (murottal with standard care, n = 11), Group B (classical music with standard care, n = 11), and Group C (control without music therapy with standard care, n = 11). The study compared IL-6 levels 30 minutes before and 30 minutes after surgery, as well as pain levels NRS measured 4 hours postoperatively (pre- and post-intervention) in lower extremity orthopedic surgery patients.
Results: A significant difference was observed, showing that murottal reduced NRS with a p-value of < 0.05 (p = 0.003), and classical music also reduced NRS with a p-value of < 0.05 (p = 0.003), compared to the control group, which had a p-value of > 0.05 (p = 1.000), there was no significant effect of murottal on IL-6 levels (p > 0.05, p = 0.277) or classical music on IL-6 levels (p > 0.05, p = 0.740) in patients undergoing lower extremity orthopedic surgery.
Conclusion: The study results indicate the use of murottal and classical music for pain management provides better effects compared to no music intervention, there was no significant effect of murottal and classical music on IL-6 levels.
Keywords: IL-6, music therapy, orthopedic surgery, postoperative pain, quranic recital
Introduction
According to The International Association for the Study of Pain, pain is defined as: “Sensory and emotional experiences that are unpleasant or resemble real or potential tissue damage”.1 Pain is a personal experience influenced by biological, psychological, and social factors. Through human life experiences, a person learns what pain is. Although pain usually has an adaptive function, it can have a negative impact on social and psychological function and well-being.2
Effective postoperative pain management is essential to reduce postoperative morbidity, if acute pain is not properly managed, it can develop into persistent chronic pain, which will be a great burden for the patient’s rehabilitation. Therefore, a better understanding of acute pain can help minimize the risk of transitioning from acute pain to chronic pain.3
As the global life expectancy increases, experts predict that the number of orthopedic surgeries for knee or hip replacements, as well as procedures to stabilize, align, and repair fractures, will increase significantly. Indonesia is the country with the highest number of fractures in Southeast Asia, reaching 1.3 million per year. The morbidity rate related to fractures is expected to continue to increase every year.4
Hearing quranic recitation or music are known to activate the body’s cells by converting sound waves into waves that the body receives, thereby reducing pain receptor stimulation, and stimulating the brain to secrete endogenous natural opioid analgesics that block pain nociceptors. In acute care, listening to music has been shown to be effective in reducing postoperative patient pain.5,6
Music therapy is a natural intervention that supports various aspects of recovery such as physical, emotional, psychological, spiritual, and social. Music can stimulate waves α the brain, cause relaxation and reduce muscle tension, as well as trigger the limbic system that releases endorphins, neurotransmitters that induce a sense of comfort. Music can slow down the transmission of pain signals through hearing, reduce pain, and reduce the dose of postoperative analgesic medications. Listening to music also stimulates the parasympathetic nervous system, inhibits the activity of the sympathetic nervous system, and is effective in reducing anxiety.6,7
Methods
This study is an experimental study (Randomized Double Blind Control Trial) on the effect of murotal and classical music on IL-6 levels and analgesia levels in lower extremity orthopedic surgery patients. This study compared the effects of group A (Murotal), group B (Classical Music), and group C (Non Murotal and Non Music) on IL-6 levels and analgesia levels in lower extremity orthopedic surgery patients.
All patients who meet the criteria will be included as research subjects. The sampling technique uses consecutive sampling, each one that meets the criteria will be included in the sample until the sample number is met. Experimental design of a numerical randomized controlled trial with multiple treatment groups.
Randomization was carried out using a spin application, which was made into 3 groups with a ratio of 1:1:1, namely, the murotal group, classical music and control. Then the application will do a random round 3 times until one of the selected groups is selected. The main researcher and the study subject did not know the type of intervention given.
Measurement of the level of analgesia using NRS scores. Measurement of the inflammatory level used the IL-6 Human (Enzym-Linked Immunosorbent Assay) (ELISA) Elabscience Kit, with a serum sample of 30 microliters, a measurement range of 0.01–100 pg/mL to measure Interleukin-6 levels. The OD (optical density) results were analyzed using the arigo ELISA gain data calculator.
This research, based on an agreement between the researchers and their members, was submitted for ethical review and has received a certificate of ethical clearance and site permit. The certificate of ethical clearance and site permit were issued by the Research Ethics Commission of the Faculty of Medicine, Jenderal Soedirman University, under number 109/KEPK/PE/XII/2024, in accordance with the Declaration of Helsinki. It was registered in clinicaltrials.gov on November 24, 2024, under registry number NCT06713044. Data was saved in https://data.mendeley.com/drafts/23gpj85wkw. This research uses private funding and is not tied to various parties and interests. First patient was start entered into the national insurance database in September 2024 and research procedure is carried out from Nov 24, 2024 after the release of ethical clearance.
Result
Characteristics in this study included gender, age, education, surgical diagnosis, length of surgery, bleeding, fluids during surgery, and BMI. The distribution of the characteristics of the study subjects, which included age, education, gender, surgical diagnosis, was presented in the form of percentages, while age, duration of surgery, bleeding, and fluid during surgery were in the form of mean and standard deviations. Based on the results of the homogeneity test with the levene test, it was found that all the characteristic variables of the research subjects showed a data distribution (p > 0.05), meaning that the data were homogeneous (details of the results can be seen in Table 1).
 |
Table 1 Characteristics of Research Subjects |
The prerequisite test carried out in this study is the normality test. The normality test aims to test whether the variables used in the study are normally distributed. To detect the normality of the data, it can be done through statistical analysis, one of which can be seen through Shapiro Wilk because the data used is <50 (n = 33). The results of data distribution in group A (Murottal) were for pre and post NRS data (p value 0.000), IL-6 post (p value 0.000) and for IL-6 pre data (p value 0.141). Group B (Classical Music) for NRS pre (p value 0.000), NRS post (p value 0.001), for IL-6 pre data (p value 0.186) and IL-6 post (p value 0.062). Group C (Control) for NRS pre (p 0.000), NRS post (p 0.000) and IL-6 pre (p 0.000) IL-6 post (p 0.000), followed by non-parametric (Wilcoxon test) and parametric (T test Dependent) tests.
NRS murotal and NRS classical music with a p value of 0.003 (p<0.05) H0 were rejected and Ha was accepted which means that there was an influence of murottal and classical music on the NRS score in patients with lower extremity orthopedic surgery who were given intrathecal anesthesia which showed that murotal and classical music reduced the intensity of postoperative pain. The results of murotal IL-6 with a p value of 0.277 (p>0.05) and classical music p value 0.740 (p>0.05) which means that H0 was accepted Ha was rejected which means that there was no influence of murottal and classical music on IL-6 levels in lower extremity orthopedic surgery patients who were given intrathecal anesthesia, while in the control group NRS data were obtained with p value 1.000 (p>0.05) and IL-6 with a p value of 0.293 (p>0.05) so that H0 was accepted and Ha was rejected which means that there was no effect on the control group on IL-6 and NRS levels in lower extremity orthopedic surgery patients who underwent intrathecal anesthesia (Table 2).
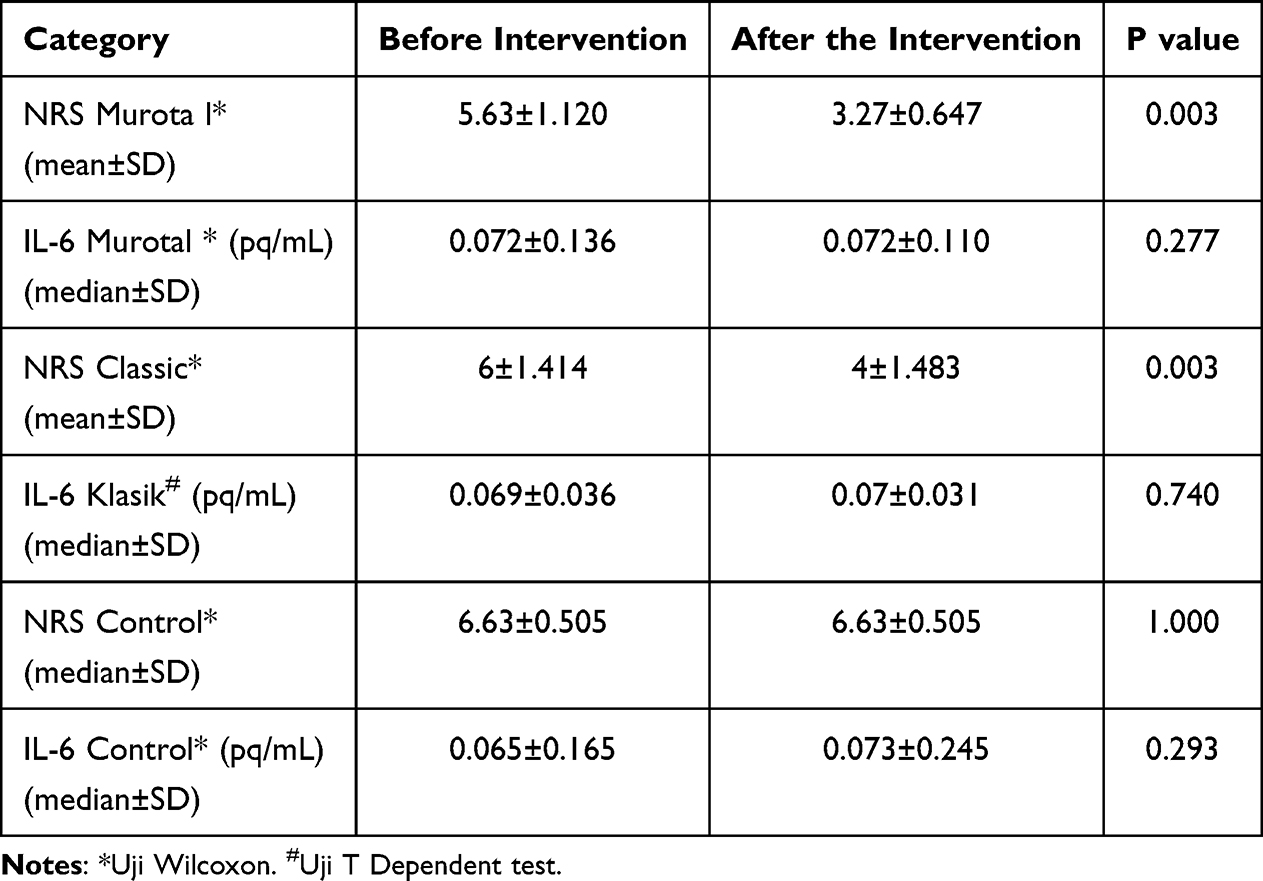 |
Table 2 Comparison of NRS Values and Pre- and Post-Murotal IL-6 Levels, Classical Music and Controls in Lower Extremity Orthopedic Surgery Patients Under Intrathecal Anesthesia |
The results of the analysis in Table 2 show that there are differences in the levels of pre and post NRS in group A (Murotal), group B (Classical Music) which is meaningful (p < 0.05), and group C (Control) which is meaningless (p > 0.05). There was a significant difference and consisted of more than 2 independent variables, then a test was carried out between groups to see the median difference between groups using the Kruskal Wallis test (Table 3).
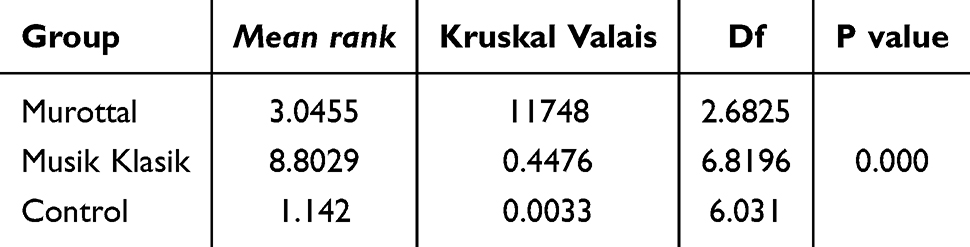 |
Table 3 Effect of Analgesia Levels Between Murotal Groups, Classical Music and Control on NRS Values |
The analysis in Table 3, shows that there is a significant difference in NRS between group A (murotal), group B (classical music), and group C (control) with a p value of 0.000 (p < 0.05), then a comparison test was carried out to determine which group pairs were significantly different. The test used was the non-parametric statistical test of the Dunn Test which was used as a post hoc test to compare differences between more than 2 groups after the Kruskal–Wallis Test.
The analysis in Table 4 shows that NRS scores have significant differences between the murotal and control groups, as well as the classical and control groups, but not between the murotal and classical music groups.
 |
Table 4 Comparison of Pre and Post NRS Between 3 Groups |
Discussion
The decrease in pain intensity measured using the NRS analyzed in this study, both the murottal and classical music groups showed a significant decrease in NRS scores compared to the control group. The results of this study showed that group A NRS (murotal) and group B (classical music) had similar results in lowering NRS levels, but not for group C (control). Statistical tests showed that there was a significant difference between the 3 groups (p < 0.05) and the statistical test also showed that the NRS score was significantly different between the murotal and control groups (p < 0.05), as well as the classical and control groups (p < 0.05), but not between the murotal and classical music groups (p > 0.05), while for IL-6 it showed that group A (murotal), group B (classical music) and group C (control) there was no significant decrease in IL-6 between pre and post IL-6 with p values of all three groups (p > 0.05).
The results of this study are in line with previous research for NRS which found that the administration of music-based interventions may lower NRS scores, but not for IL-6 levels. Several reasons may explain these findings. First, IL-6 is a cytokine that increases after injury and its peak often occurs within a period of a few hours to days after surgery, depending on the severity of the inflammation. Second, the lack of analysis of the research subjects’ personal experiences of murotal and classical music can affect how these interventions affect the psychological and emotional state of the participants.8
Music-based interventions have been shown to lower IL-6 levels in the organism and in advanced adult patients. Recent evidence suggests that music can be used to reduce the negative impact of interventions that affect IL-6, a pro-inflammatory cytokine, especially those resulting from stress, trauma, and psychological effects. Soothing music can reduce stress levels, which often increases the production of IL-6 in the body. Soothing music can make the parasympathetic nervous system responsible for relaxation stimulated, while the activity of the sympathetic nervous system associated with stress responses can be reduced.8
Soothing music can make the parasympathetic nervous system responsible for relaxation stimulated, while the activity of the sympathetic nervous system associated with the stress response can be reduced. Music of 120 decibels or more can increase the inflammatory response including IL-6, the use of music of 60 decibels can block the release of IL-6 by suppressing stress hormones so that they do not release inflammatory mediators.9
The decrease in pain threshold that occurs can be explained by various psychophysiological mechanisms associated with music exposure. Murottal as well as classical can affect the central nervous system, stimulating the production of neurotransmitters such as endorphins and dopamine, which directly play a role in reducing pain perception.8,10
Musical interventions (murottal and classical music) successfully reduce the perception of pain. This pain-reduction mechanism is more likely related to the psychological and neurophysiological effects of music. A number of previous studies have shown that music can induce relaxation effects, as well as affect the activity of brain waves related to pain processing. McCaffrey’s research showed that pain intensity decreased by 33% after 20 minutes of music therapy using Mozart’s classical music in osteoarthritis patients, low sound intensity, between 50 and 60 decibels had a positive impact on the listener.11,12
Research shows that listening to the Qur’anic murottal can provide benefits in the healing process, such as reducing pain and helping patients feel more relaxed. This is related to a decrease in adrenal corticotropin hormone (ACTH), known as the stress hormone. Other studies have also shown that listening to the Qur’an for a few minutes can reduce the intensity of pain and have a positive effect on the listener. The Quran has a human element that can function as an effective healing tool, this sound can lower stress hormones and stimulate the release of natural endorphins, which are beneficial for providing calm, controlling emotions, and improving the quality of thought, so that it can inhibit the release of stress hormones.13,14
Quranic therapy and music are known to activate the body’s cells by converting sound waves into waves that the body receives, thereby reducing the stimulation of pain receptors. In acute care, listening to music-based interventions has been shown to be effective in reducing postoperative patient pain.5,6
Music-based interventions have been shown to reduce NRS levels. Soothing sounds can make the parasympathetic nervous system responsible for relaxation stimulated, while the activity of the sympathetic nervous system associated with the stress response can be reduced. Excessive stress can increase levels of the hormone cortisol, which in turn can trigger an inflammatory response.8,10
Previous research has shown that listening to music helps patients distract from environmental noise and conversations conducted by surgical teams. Anxiety experienced before and during surgery can cause problems during the postoperative recovery period. Therefore, it is important to control anxiety through music therapy and eliminate anxiety to be a consideration in the postoperative healing process.11
The study examined the analgesic and anti-inflammatory effects of the use of murotal and classical music in lower extremity orthopedic surgery patients who performed intratechal anesthesia. The design in this study was random and double-blind, so the risk of bias was kept to a minimum. Murotal and classical music-based interventions are widely available and effective tools in lowering pain levels.
Conclusion
Murottal Al Qur’an and classical music lower NRS scores but do not lower IL-6 levels. The decrease in NRS scores in the murotal and classical music groups was no different in lower extremity orthopedic surgery patients who were given intrathecal anesthesia.
The limitations of this study are that the study subjects’ personal experience of murotal and classical music was not analyzed, the intervention was relatively short and no other inflammatory biomarker examination was conducted.
Data Sharing Statement
All data from this study with DOI: 10.17632/23gpj85wkw.3 can be accessed without any time limit on the website https://data.mendeley.com/datasets/23gpj85wkw/3.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rajaa SN, Carrb DB, Cohenc M, et al. The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises. Pain. 2020;161:1976–1982. doi:10.1097/j.pain.0000000000001939
2. Aydede M. Does the IASP definition of pain need updating? Pain Rep. 2019;4:e777. doi:10.1097/PR9.0000000000000777
3. Delaney LD, Clauw DJ, Waljee JF. The management of acute pain for musculoskeletal conditions: the challenges of opioids and opportunities for the future. J Bone Joint Surg Am. 2020;102(Suppl 1):3–9. doi:10.2106/JBJS.20.00228
4. Platini H, Chaidir R, Rahayu U. Karakteristik Pasien Fraktur Ekstermitas Bawah. Jurnal Keperawatan ‘Aisyiyah. 2020;7(1):49–53. doi:10.33867/jka.v7i1.166
5. Karagoz I, Yigit U, Ilce A. The effect of music therapy on pain, anxiety, and vital signs in patients undergoing spinal anaesthesia: a randomized controlled trial. Ther Adv Psychopharmacol. 2021. doi:10.51972/tfsd.956551
6. Kahna M, Ghariani W. The contribution of music therapy to the operating room: a randomized control study. Med Care Res Rev. 2020;1(01):14.
7. Hsu C, Chen S, Lee P, Lin P. The effect of music listening on pain, heart rate variability, and range of motion in older adults after total knee replacement. Clin Nurs Res. 2019;28:529–547. doi:10.1177/1054773817749108
8. Saifman J, Colverson A, Prem A, Chomiak J, Dorél S. Therapeutic potential of music-based interventions on the stress response and neuroinflammatory biomarkers in COVID-19: a review. Music Sci. 2023;6:1–18. doi:10.1177/20592043231150912
9. Wang H, Chai Y, Xu Y, et al. Long-term music stimulating alleviated the inflammatory responses caused by acute noise stress on the immune organs of broilers by NF-κB signaling pathway. Ecotoxicol Environ Saf. 2024;234:116131. doi:10.1016/j.ecoenv.2024.116131
10. Frickmann FCS, Urman RD, Siercks K, Burgermeister G, Luedi MM, Lersch FE. The effect of perioperative auditory stimulation with music on procedural pain: a narrative review. Curr Pain Headache Rep. 2023;27:217–226. doi:10.1007/s11916-023-01138-x
11. de Araújo Azi LMT, Azi ML, Viana MM, et al. Benefits of intraoperative music on orthopedic surgeries under spinal anesthesia: a randomized clinical trial. Complement Ther Med. 2021;63:102777. doi:10.1016/j.ctim.2021.102777
12. Yu R, Zhuo Y, Feng E, et al. The effect of musical interventions in improving short-term pain outcomes following total knee replacement: a meta-analysis and systematic review. J Orthop Surg Res. 2020;15:465. doi:10.1186/s13018-020-01995-x
13. Kirnawan F, Mustofa A. The effectiveness of murottal Al-Qur’an therapy and virtual reality to reduce pain intensity in post-operating patients. Southeast Asian Nurs Res. 2020;2(2):74–81. doi:10.26714/seanr.2.2.2020.74-81
14. Priyanto AFK, Dahlia D. The effectiveness of psychoreligious intervention: Murottal Al-Quran on pain and stress level of bone cancer patients. Int J Glob Health Public Health. 2020;2(4):375–384. doi:10.37287/ijghr.v2i4.260
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.