Back to Journals » Therapeutics and Clinical Risk Management » Volume 15
Multivariate analysis of poor outcome after anterior surgery in multilevel cervical spondylotic myelopathy patients with heterotopic ossification and preoperative kyphotic alignment
Authors Li S, Zhang B, Shen Y, Wu Z
Received 16 March 2019
Accepted for publication 27 July 2019
Published 27 August 2019 Volume 2019:15 Pages 1053—1060
DOI https://doi.org/10.2147/TCRM.S208991
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
ShaoQing Li,1 BaoYang Zhang,2 Yong Shen,2 ZhanYong Wu1
1Department of Orthopedic Surgery, The Orthopedics Hospital of XingTai City, XingTai 054000, People’s Republic of China; 2Department of Orthopedic Surgery, The Third Hospital of Hebei Medical University, Shijiazhuang 050051, People’s Republic of China
Correspondence: ZhanYong Wu
Department of Orthopedic Surgery, The Orthopedics Hospital of XingTai City, No. 202 Bayi Road, XingTai 054000, People’s Republic of China
Tel +86 1 863 116 4033
Fax +86 0 319 206 9476
Email [email protected]
Objective: The aim of this study was to evaluate the risk factors for poor outcome in patients who underwent multi-segmental anterior surgery, and analyze postoperative complications.
Methods: We retrospectively reviewed 158 patients after anterior surgery due to multilevel cervical spondylotic myelopathy (m-CSM) between June 2008 and June 2016. Adjusted ORs and 95% CIs were determined by multivariate logistic regression analysis. Cutoff values and the area under the curve for continuous risk factors were calculated through receiver operating characteristic curve analysis. The chi-squared test was performed for the comparison of complications among the three surgical groups.
Results: By analyzing 105 patients with good outcome and 53 patients with poor outcome, we established that the risk factors for poor outcome were advanced age (OR =1.12, P=0.003), longer duration of symptoms (OR =1.07, P=0.028), and bigger kyphotic angle at final follow-up (OR =1.29, P< 0.001). The optimal cutoff values for age, duration of symptoms, and kyphotic angle at final follow-up were 63.1 years, 15.5 months, and 5.3 angle. Postoperative complications occurred in 21 patients (13.3%). The incidence of dysphagia and cerebrospinal fluid leakage were higher in multilevel anterior cervical discectomy and fusion (m-ACDF) group than in other groups (P< 0.05).
Conclusion: Advanced age, longer duration of symptoms, and bigger kyphotic angle at final follow-up were the risk factors for poor postoperative outcome in patients with m-CSM. The complications after hybrid approach and m-ACDF approach were less than after anterior cervical corpectomy and fusion approach.
Keywords: multilevel cervical spondylotic myelopathy, kyphotic, heterotopic ossification, hybrid approach, complication
Introduction
Cervical spondylotic myelopathy (CSM) results from anatomic and structural degenerative changes that lead to progressive spinal cord disorders. It is usually accompanied by decreased intervertebral disc space, osteophytes, and ligamentum hypertrophy. Cervical lordosis potentially occurs loss even formation of kyphosis with advancement of degenerative changes. Cervical kyphosis is associated with spinal cord compression, kinematics of the cervical spine, and neurologic recovery.1,2 Decompression of symptomatic spinal cord compression and fusion has become an effective intervention for patients with multilevel cervical spondylotic myelopathy (m-CSM) to obtain quality of life recovery.3,4 However, the selection of surgical procedures applied in patients with m-CSM and cervical kyphotic alignment is controversial. A 2-level corpectomy has been considered effective treatment of m-CSM.5,6 Unfortunately, many complications such as C5 palsy, too much bleeding, titanium mesh displacement or subsidence, and others have been reported.7,8 With the improvement of surgical skill and technology, the complications have gradually decreased in multilevel anterior cervical discectomy and fusion (m-ACDF) and hybrid technique (discectomy combined with corpectomy), which provide good options for spinal reconstruction and decompression of spinal cord.
Some scholars have reported the comparisons of m-ACDF, hybrid approach, and 2-level corpectomy.9,10 Nonetheless, few investigations have focused on the relationship between postoperative outcomes and improvement of preoperative kyphotic alignment. In addition, the complications after anterior removal of heterotopic ossification (including posterior annulus fibrosus ossification, ossification of the posterior longitudinal ligament (OPLL), and osteophytes at the posterior vertebral edge) have rarel been studied. This can provide the surgeon with direction when treating patients with heterotopic ossification and preoperative kyphotic alignment, thereby decreasing the probability of poor postoperative outcome.
Materials and methods
Ethical considerations
This study was approved by the Institutional Ethics Board of the orthopedics hospital of XingTai and the 3rd Hospital of Hebei Medical University, and written informed consent was obtained from all individual participants included. The methods were carried out in accordance with the doctor-patient relationship regulations which strictly adhered to the STROBE statement.
Patient inclusion and exclusion criteria
There were 158 cases with m-CSM along with heterotopic ossification and cervical kyphotic deformity, identified from a retrospective analysis of clinical records of patients who underwent anterior decompression and fusion approach from June 2008 to June 2016 at the Department of Spinal Surgery, the Third Hospital of Hebei Medical University and the orthopedics hospital of XingTai, China.
The criteria for inclusion were the following: 1) diagnosis of m-CSM with mild or moderate cervical kyphosis (Cobb <40°); 2) heterotopic ossification: the circumscribed-type OPLL, posterior annulus fibrosus ossification and osteophytes at the posterior vertebral edge; 3) obvious clinical symptoms; and 4) patients underwent m-ACDF, 2-level anterior cervical corpectomy and fusion (ACCF) or hybrid (1-level ACDF+1-level ACCF) approach (Figure 1).
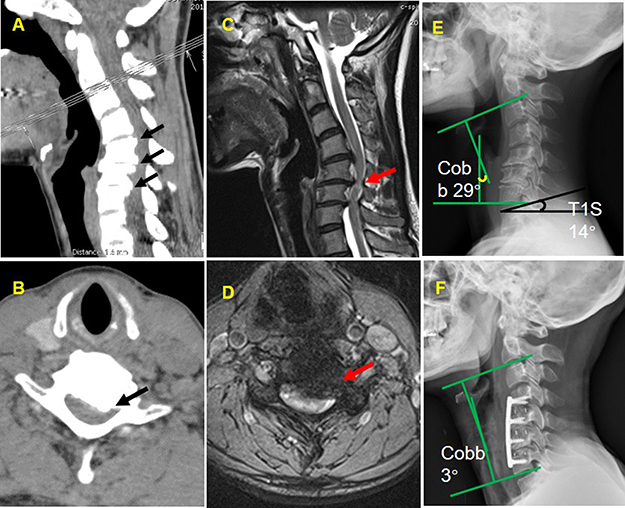 |
Figure 1 The multilevel compression of spinal cord with heterotopic ossification on CT (A, B) and ISI of spinal cord on MRI (C, D). The kyphotic alignment with C2–7 Cobb =29 angle (E) and three-levels ACDF were performed at final follow-up (F). |
Some exclusion criteria included: 1) prior cervical surgery; 2) presence of spinal tumors or other complex concomitant diseases; 3) incomplete imaging data.
Patient follow-up
All the patients were followed-up for an average of 21.4±7.6 months (range, 12–42 months). Clinical data were collected including age, gender, body mass index, diabetes mellitus diagnosis, duration of symptoms, anteroposterior diameter of spinal canal (AODC), preoperative and last follow-up Japanese Orthopedic Association (JOA) score and C2–7 Cobb, preoperative T1 slope angle, last follow-up cervical range of motion (ROM), cerebrospinal fluid (CSF) leakage, surgical approach, and grade of increased signal intensity (ISI). In the present study, 83 males and 75 females were enrolled and their mean age was 60.2 years. The recovery rate of JOA score was used to evaluate surgical outcome at preoperative and final follow-up. The recovery rate = (postoperative JOA score - preoperative JOA score)/(17 - preoperative JOA score)×100%. A score ≥75% was designated as excellent, ≥50% but <75% as good, ≥25% but <50% as fair, and <25% as poor. Therefore, we defined recovery rates <50% as a poor postoperative outcome in this study.
Surgical procedures
Patients had various symptoms such as gait disturbance, sensory abnormality of the trunk or extremities, and urinary dysfunction before surgery. The surgical approach was determined by physical condition, degree of symptoms, the location of spinal cord compression, and ISI of the spinal cord on sagittal T2-weighted magnetic resonance imaging (MRI). When the location of spinal cord compression due to continuous ossification zone had more than 3 segments, posterior approach would be considered.
The patients were placed on a surgical bed under general anesthesia in supine position. We adopted right transverse skin incision after the determination of surgical segment by body surface location. It reached the anterior edge of diseased level at medial side of sternocleidomastoid by blunt separation of the neck muscles. The assistant medially pulled the trachea and esophagus to the left side with a thyroid retractor. We expanded both sides of the intervertebral space and removed part of the end plate, which would remove the lesion for the decompression of spinal cord. The optimal poly-ether-ether-ketone cage or titanium mesh with autologous bone was inserted into the disc space, and the anterior fixation with plate system. It has to be noted that the rupture of venous plexus will increase intraoperative bleeding. All patients were restricted to bed only 1 or 2 days and told to use a cervical collar for 3 weeks after surgery.
Radiological assessment
The cervical curvature was defined as the angle of intersection between lines parallel to the inferior end plates of C2 and C7. Kyphotic: more than +5°; straight: +5° to −5°; lordotic: less than −5° (positive = kyphotic; negative = lordotic) (Figure 1A). We measured the narrowest distance from the posterior vertebral edge to the fundus of spinous process as AODC. The ROM was defined as the change in the maximal flexion and extension on lateral radiographs. The grade of ISI was classified: Grade 0= no ISI on T2-weighted MRI; Grade 1= ISI on T2-weighted MRI limited to one disc level; Grade 2= ISI on T2-weighted MRI beyond one disc level11 (Figure1B–D). The thoracic 1(T1) slope was defined as the angle between the superior endplate of T1 and a horizontal line on standing lateral radiograph (Figure 1E and F). Patients’ imaging data were evaluated on lateral radiographs and T2 MRI by one orthopedic surgeon (S.Q.L.).
Statistical analyses
In the data description, continuous variables were made using means and SDs and categorical variables were described by frequencies and percentages. Univariate analyses were performed to identify correlations between prognostic factors and postoperative effect at last follow-up. Counting data were compared with the chi-squared test, while measurement data were analyzed using the independent t-test or Mann–Whitney U test, as appropriate. In univariate analysis, the factors of P-value <0.05 were brought into the multivariate logistic model. Multivariate logistic regression analysis was applied to control for potential confounding variables with the dependent variable of “poor outcome”, with adjusted ORs within 95% CIs. The receiver operating characteristic (ROC) curves were constructed to evaluate the cutoff values for the continuous variables of risk factors. Finally, the comparative analyses of the three approaches were performed using the chi-squared test, independent t-test or Mann–Whitney U test, as appropriate. A P-value <0.05 was considered statistically significant. All data analyses were performed by SPSS software Version 21.0 (IBM Corporation, Armonk, NY, USA), and the figures were plotted with GraphPad Prism 8.
Results
Univariate and multivariate analyses
All patients were apportioned to two groups according to the recovery rates of JOA score: good group (≥50%, n=105) and poor group (<50%, n=53). Compared with the good group, the poor group had a significantly higher mean age at operation (P=0.001), longer duration of symptoms (P<0.001), kyphotic alignment at last follow-up (P=0.001), underwent 2-levels ACCF (P<0.001), and had higher grade of ISI on T2 MRI (P=0.006). There was no significant difference between the two groups with regard to other variables (Table 1). In the multivariate logistic regression analysis, age (OR =1.12, 95% CI =1.041–1.207, P=0.003), duration of symptoms (OR =1.07, 95% CI =1.007–1.128, P=0.028), and C2–7 Cobb at last follow-up (OR =1.29, 95% CI =1.184–1.408, P<0.001) were identified as the risk factors of poor outcome after surgery (Table 2).
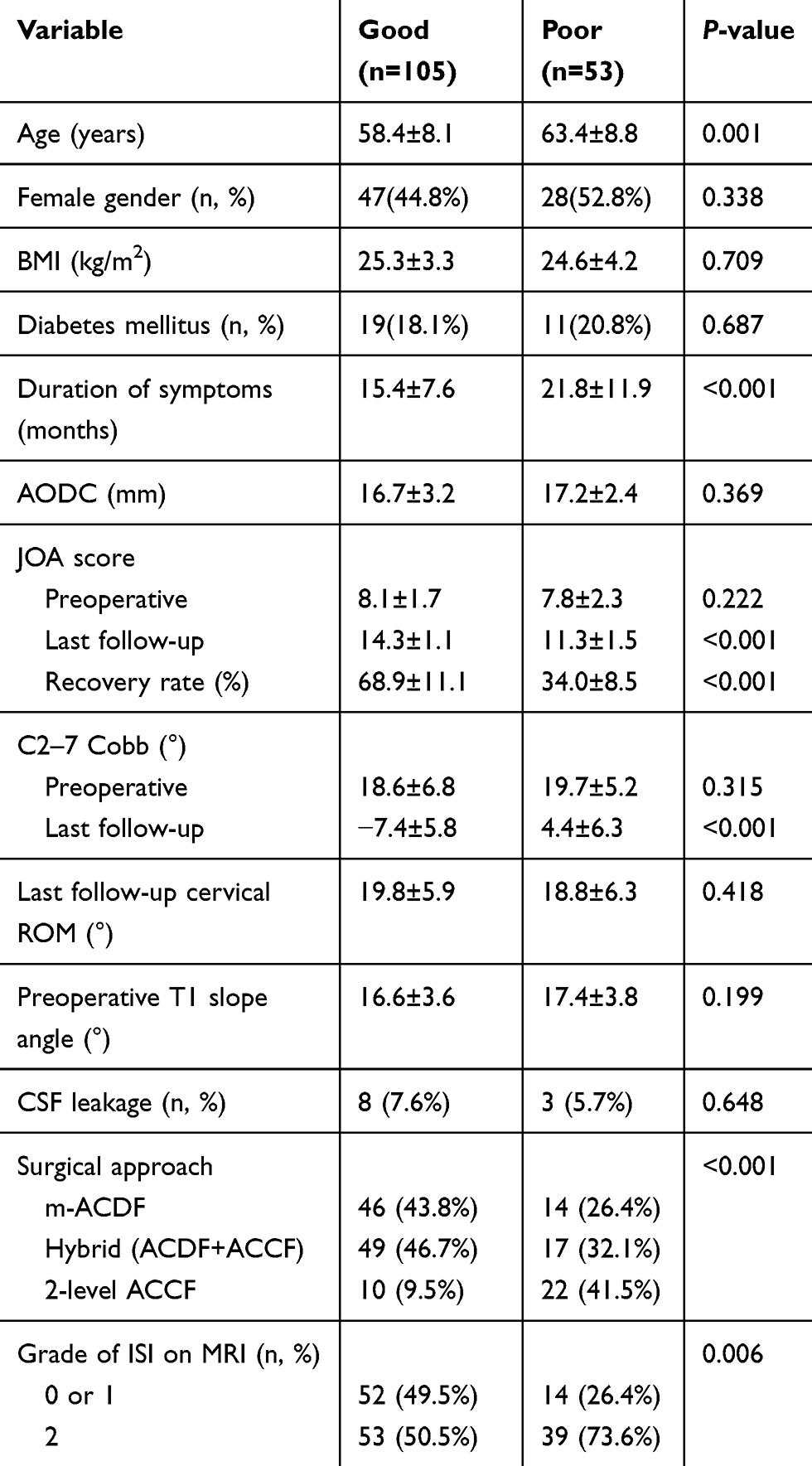 |
Table 1 Demographic characteristics of the good and poor outcome groups |
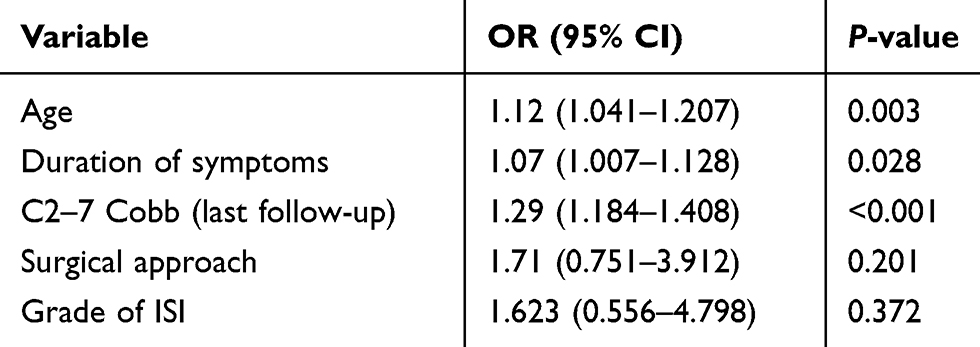 |
Table 2 Multiple logistic regression analysis forecasted risk factors for poor outcome |
ROC curve analysis
The ROC analysis was performed to obtain good accuracy of risk factors, which was illustrated by the area under the curve and cutoff. It mean that had a close relationship between risk factors and poor postoperative outcomes with the larger the area under the curve. Age, duration of symptoms, and C2–7 Cobb at last follow-up were 0.672, 0.675, and 0.889, respectively. The cutoff was defined as the maximum of Youden index, which represented the best compromise between sensitivity and specificity. The cutoff values of age, duration of symptoms, and C2–7 Cobb at last follow-up were 63.1 years, 15.5 months, and 5.3 angle, respectively (Table 3 and Figure 2A–C).
 |
Table 3 Sensitivity, specificity, AUC, and cutoff of risk factors for predicting poor outcome |
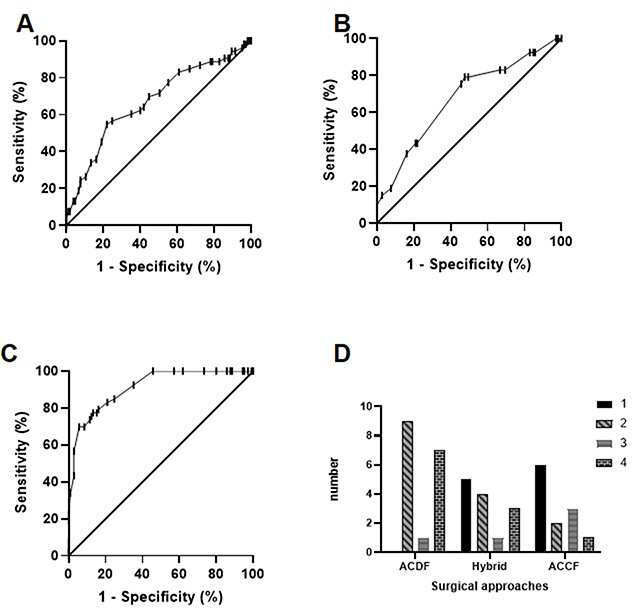 |
Figure 2 Age, duration of symptoms, and C2–7 Cobb at final follow-up were drawn by ROC (A, B and C, respectively). A histogram demonstrates the postoperative complications of the three types of surgery (D). |
Comparative analysis of the three approaches
The operated levels included C3–C6, C4–C7, and C3–7 in three groups, and the involved 4-levels operations were performed in only m-ACDF group (n=4). The fusion rates were 97%, 92%, and 84% at 3 months after surgery in m-ACDF group, hybrid group, and ACCF group, respectively, and fusion occurred in all patients at the last follow-up. Postoperative complications including graft dislodgment or subsidence, dysphagia, C5 palsy, and CSF leakage occurred in 21 patients (13.3%), and the data were reviewed from medical history. The ACDF group had the least amount of bleeding compared with the ACCF group, which had the the most bleeding. The correction degree of C2–7 Cobb in the m-ACDF group, hybrid group, and 2-level ACCF group was 25.2±6.6, 24±6.2, and 14±6.1 angle, respectively. The m-ACDF group had the most correction compared with the ACCF group which had the least correction. Although there was a difference in the three groups for JOA score at the final follow-up (ACDF: 61.3±16.6, hybrid: 62.2±16.5, and ACCF: 51.8±17.2), clinical outcome was improved in all three groups. Dysphagia and CSF leakage had a higher rate of occurrence in the m-ACDF group, while graft dislodgment, subsidence, and C5 palsy had a higher rate of occurrence in the 2-level ACCF group (Table 4 and Figure 2D).
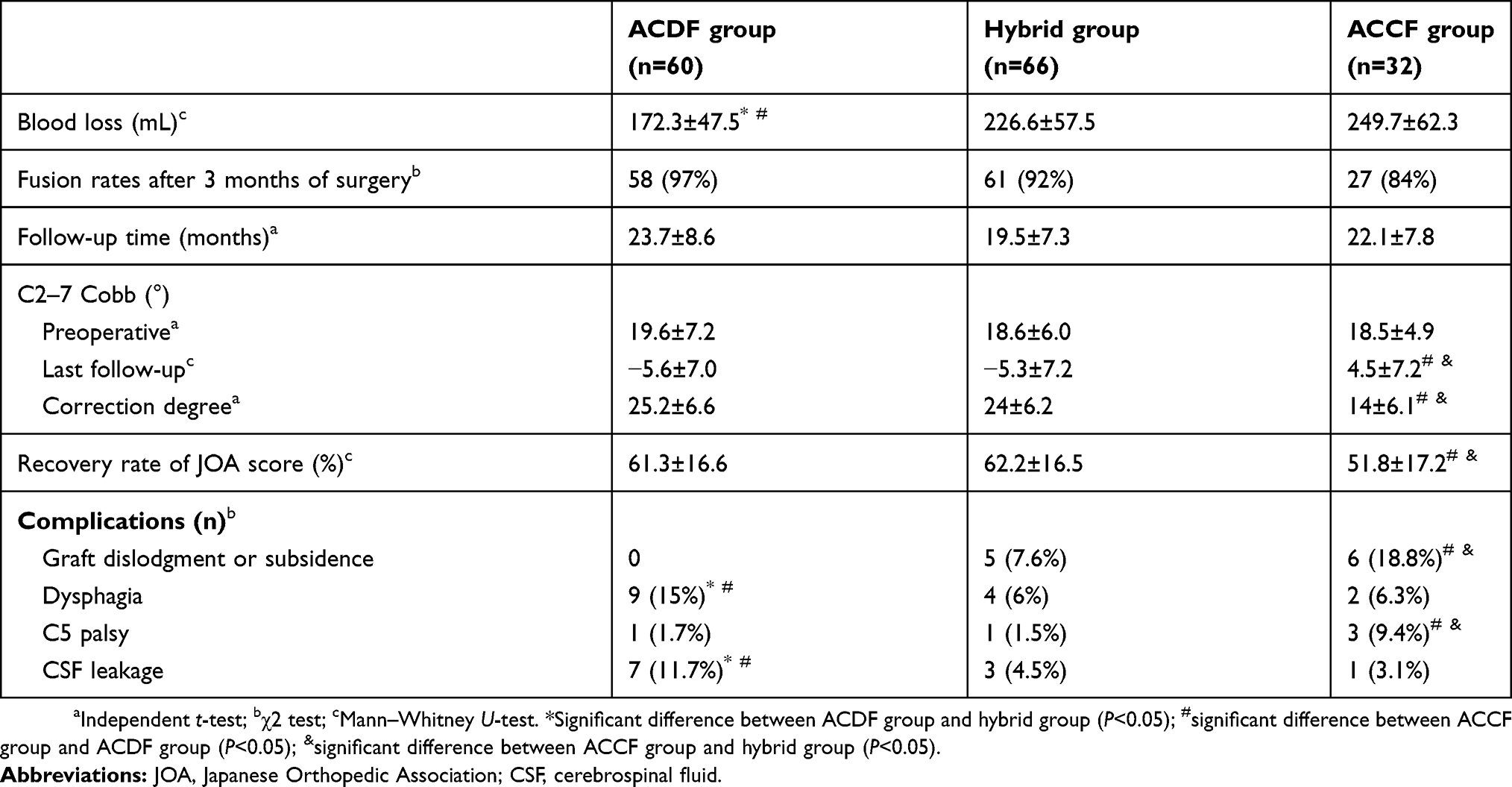 |
Table 4 Summary of characteristics of patients in three groups (ACDF, hybrid, and ACCF) |
Discussion
Operation methods
CSM with degeneration of multi-segmented disc can lead to a mild or moderate kyphosis deformity, which puts the spinal cord in a tensional state. Surgical treatment including anterior, posterior, and combined anteroposterior approaches for patients with m-CSM are becoming more common. However, controversy remains regarding the selection of surgical procedures for treatment of multilevel CSM.8,12,13 Posterior laminoplasty is a successful surgical procedure in properly selected patients with m-CSM or part of type of OPLL.14 Whereas, the spinal cord cannot “drift backward” well after posterior approach in patients with cervical kyphotic deformity, resulting in poor curative effect.15 Anterior decompression and fusion have become popular because it can directly relieve pressure of spinal cord. The anterior m-ACDF, ACCF, and hybrid techniques have been applied in clinics, but potential complications still exist.8 Moreover, the combined procedure has been applied in patients with severe kyphotic alignment to achieve a large correction and high fusion rate.16 In the present study, severe cervical kyphosis caused by congenital, trauma, tumor or other reasons was excluded in order to clearly elaborate the relationship between postoperative outcome and the degree of kyphotic correction after single anterior surgery.
Maintaining lordosis
Cervical lordosis is an important role in the maintenance of postoperative outcome.17 The loss of cervical lordosis causes disordered distribution of cervical sagittal stress which leads to further deterioration of the degeneration. In addition, Chavanne18 found that cervical kyphosis of more than 7.5 degrees resulted in the increase of cervical spinal cord intramedullary pressure. Historically, anterior surgical approaches could correct kyphosis deformity. Previous studies all found greater kyphosis correction after m-ACDF than corpectomy, but it was difference between corpectomy and discectomy-corpectomy hybrid procedures about correction of kyphosis.9,12,19,20 Our results showed that, in terms of kyphotic correction, there was no significant difference between m-ACDF group and hybrid group, but the ACCF group was not as good as the other two groups. We considered that the causes were related to fusion delay, graft subsidence or dislodgment, and straight form of titanium mesh in the ACCF group. Compared with the good group, the poor group had a significant difference in C2–7 Cobb at final follow-up, which confirms the importance of maintaining cervical lordosis for postoperative outcome. It is worth noting that correction of cervical kyphosis is one of the prominent preconditions of maintaining lordosis.
Postoperative outcomes
In previous studies, some scholars reported that surgical treatment of m-CSM by m-ACDF or ACCF had no significant differences in terms of postoperative outcome, but more complications would occur after ACCF.12,21 In this study, postoperative patients with cervical kyphotic deformity obtained a better result and kyphotic change in m-ACDF group and hybrid group than in the ACCF group. So we considered that the reconstruction of cervical sagittal alignment could decompress the spinal cord. Furthermore, some studies showed that advanced age and long-term symptoms were related to poor postoperative outcome in patients with CSM.22,23 Our predictions also supported the previously mentioned view. In our study, the multi-segment ISI of spinal cord on T2 MRI had an obvious association with poor outcome after anterior surgery to treat kyphosis deformity. The forecast analysis showed that we should improve preoperative preparation and early postoperative rehabilitation treatment when encountering a patient with advanced age, long-term symptoms, and multi-segment ISI at the same time.
Complications
The complications after anterior surgery have been reported in some research.7,8,19–21 However, few studies showed a detailed analysis of the technical difficulties of anterior surgery and interoperative and postoperative complications in patients with cervical heterotopic ossification. Removal of heterotopic ossification requires enlargement of the intervertebral space or resection of the vertebral body, but this increases the risks of intraoperative bleeding, nerve root injury, and postoperative graft subsidence, especially removed the circumscribed-type OPLL with a ≥50% canal occupying ratio.11,24 In addition, Lubelski25 found that C5 palsy was association with AODC and diameter intervertebral foramen. In our study, compared with the other two groups, there was a higher incidence of C5 palsy in the ACCF group. We considered that the reconstruction of cervical curvature after vertebral resection was associated with postoperative C5 palsy. Interoperative CSF leakage had an incidence of 11.7% in the m-ACDF group, due to the narrow operating space and heterotopic ossification adhesion to the dura mater. Our study found that patients commonly experienced temporary dysphagia after excessive correction of cervical kyphotic alignment. Release of the Luschka joints, gentle manipulation and proper removal of the endplate are strategies for complication avoidance. Understanding and preventing these complications is an indispensable prerequisite to obtaining good surgical outcomes.
Limitations
As with all studies, there were some weaknesses and limitations in the current study. Firstly, this study was a retrospective non-randomized case control study, and the number of eligible patients were not large. Secondly, the follow-up term of involved patients was over 12 months after surgery, but a relationship between long-term outcome and risk factors could not be clearly established. We only predicted the future condition from the trends observed. Thirdly, it had an undefined relationship among adjacent-segment degeneration, cervical kyphotic alignment, and poor outcome. Finally, the JOA scores were calculated based on patients’ subjective feelings, which inevitably leads to the deviation of outcomes. Although the selection of surgical style, after thoughtful consideration, depended on the symptoms and the degree of compressed spinal cord, we still could not guarantee which was optimal for patients with m-CSM and kyphotic deformity.
Conclusion
Advanced age, longer duration of symptoms, and bigger C2–7 Cobb angle at final follow-up were the risk factors of poor postoperative outcome in patients with m-CSM. The complications after hybrid approach and m-ACDF approach were less than after ACCF approach.
Acknowledgment
The authors thank all patients who took part in this study and the language proofreader.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ruangchainikom M, Daubs MD, Suzuki A, et al. Effect of cervical kyphotic deformity type on the motion characteristics and dynamic spinal cord compression. Spine. 2014;39:932–938. doi:10.1097/BRS.0000000000000330
2. Shamji MF, Mohanty C, Massicotte EM, Fehlings MG. The association of cervical spine alignment with neurologic recovery in a prospective cohort of patients with surgical myelopathy: analysis of a series of 124 cases. World Neurosurg. 2016;86:112–119. doi:10.1016/j.wneu.2015.09.044
3. Fehlings MG, Arvin B. Surgical management of cervical degenerative disease: the evidence related to indications, impact, and outcome. J Neurosurg Spine. 2009;11:97–100. doi:10.3171/2009.5.SPINE09210
4. Grosso MJ, Hwang R, Krishnaney AA, Mroz TE, Benzel EC, Steinmetz MP. Complications and outcomes for surgical approaches to cervical kyphosis. J Spinal Disord Tech. 2015;28:E385–E393. doi:10.1097/BSD.0b013e318299953f
5. Nirala AP, Husain M, Vatsal DK. A retrospective study of multiple interbody grafting and long segment strut grafting following multilevel anterior cervical decompression. Br J Neurosurg. 2004;18:227–232.
6. Hilibrand AS, Yoo JU, Carlson GD, Bohlman HH. The success of anterior cervical arthrodesis adjacent to a previous fusion. Spine. 1997;22:1574–1579. doi:10.1097/00007632-199707150-00009
7. Hee HT, Majd ME, Holt RT, Whitecloud TS, Pienkowski D. Complications of multilevel cervical corpectomies and reconstruction with titanium cages and anterior plating. J Spinal Disord Tech. 2003;16:1–9. doi:10.1097/00024720-200302000-00001
8. Liu Y, Hou Y, Yang L, et al. Comparison of 3 reconstructive techniques in the surgical management of multilevel cervical spondylotic myelopathy. Spine. 2012;37:E1450–E1458. doi:10.1097/BRS.0b013e31826c72b4
9. Li Z, Wang H, Tang J, et al. Comparison of three reconstructive techniques in the surgical management of patients with four-level cervical spondylotic myelopathy. Spine. 2017;42:E575–E583. doi:10.1097/BRS.0000000000001907
10. Zhao CM, Chen Q, Zhang Y, Huang AB, Ding WY, Zhang W. Anterior cervical discectomy and fusion versus hybrid surgery in multilevel cervical spondylotic myelopathy a meta-analysis. Medicine. 2018;97:e11973
11. Kim B, Yoon DH, Shin HC, et al. Surgical outcome and prognostic factors of anterior decompression and fusion for cervical compressive myelopathy due to ossification of the posterior longitudinal ligament. Spine J. 2015;15:875–884. doi:10.1016/j.spinee.2015.01.028
12. Lin Q, Zhou X, Wang X, Cao P, Tsai N, Yuan W. A comparison of anterior cervical discectomy and corpectomy in patients with multilevel cervical spondylotic myelopathy. Eur Spine J. 2012;21:474–481. doi:10.1007/s00586-011-1961-9
13. Manzano GR, Casella G, Wang MY, Vanni S, Levi AD, Prospective A. Randomized trial comparing expansile cervical laminoplasty and cervical laminectomy and fusion for multilevel cervical myelopathy. Neurosurgery. 2012;70:264–276. doi:10.1227/NEU.0b013e3182305669
14. Iwasaki M, Kawaguchi Y, Kimura T, Yonenobu K. Long-term results of expansive laminoplasty for ossification of the posterior longitudinal ligament of the cervical spine: more than 10 years follow up. J Neurosurg. 2002;96:180–189.
15. Suda K, Abumi K, Ito M, Shono Y, Kaneda K, Fujiya M. Local kyphosis reduces surgical outcomes of expansive open-door laminoplasty for cervical spondylotic myelopathy. Spine. 2003;28:1258–1262. doi:10.1097/01.BRS.0000065487.82469.D9
16. Nottmeier EW, Deen HG, Patel N, Birch B. Cervical kyphotic deformity correction using 360-degree reconstruction. J Spinal Disord Tech. 2009;22:385–391. doi:10.1097/BSD.0b013e318180e672
17. Anakwenze OA, Auerbach JD, Milby AH, Lonner BS, Balderston RA. Sagittal cervical alignment after cervical disc arthroplasty and anterior cervical discectomy and fusion results of a prospective, randomized, controlled trial. Spine. 2009;34:2001–2007. doi:10.1097/BRS.0b013e3181b03fe6
18. Chavanne A, Pettigrew DB, Holtz JR, Dollin N, Kuntz C. Spinal cord intramedullary pressure in cervical kyphotic deformity a cadaveric study. Spine. 2011;36:1619–1626. doi:10.1097/BRS.0b013e3181fc17b0
19. Song K-J, Lee K-B, Song J-H. Efficacy of multilevel anterior cervical discectomy and fusion versus corpectomy and fusion for multilevel cervical spondylotic myelopathy: a minimum 5-year follow-up study. Eur Spine J. 2012;21:1551–1557. doi:10.1007/s00586-012-2296-x
20. Guo Q, Bi X, Ni B, et al. Outcomes of three anterior decompression and fusion techniques in the treatment of three-level cervical spondylosis. Eur Spine J. 2011;20:1539–1544. doi:10.1007/s00586-011-1735-4
21. Uribe JS, Sangala JR, Duckworth EA, Vale FL. Comparison between anterior cervical discectomy fusion and cervical corpectomy fusion using titanium cages for reconstruction: analysis of outcome and long-term follow-up. Eur Spine J. 2009;18:654–662. doi:10.1007/s00586-009-0897-9
22. Zhang JT, Wang LF, Wang S, Li J, Shen Y. Risk factors for poor outcome of surgery for cervical spondylotic myelopathy. Spinal Cord. 2016;54:1127–1131. doi:10.1038/sc.2016.64
23. Montgomery DM, Brower RS. Cervical spondylotic myelopathy - clinical syndrome and natural-history. Orthop Clin North Am. 1992;23:487–493.
24. Yoshii T, Sakai K, Hirai T, et al. Anterior decompression with fusion versus posterior decompression with fusion for massive cervical ossification of the posterior longitudinal ligament with a ≥50% canal occupying ratio: a multicenter retrospective study. Spine J. 2016;16:1351–1357. doi:10.1016/j.spinee.2016.07.532
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.