Back to Journals » Vascular Health and Risk Management » Volume 18
Multiple Venous and Pulmonary Artery Thrombosis as a Presenting Complaint of Nephrotic Syndrome-Case Report and Challenges in Management
Authors Mohamed HN, Bashir AM ![]() , Mohamed YG
, Mohamed YG ![]()
Received 20 April 2022
Accepted for publication 21 July 2022
Published 28 July 2022 Volume 2022:18 Pages 589—593
DOI https://doi.org/10.2147/VHRM.S371373
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Daniel Duprez
Hawa Nuradin Mohamed,1 Ahmed Muhammad Bashir,1 Yahye Garad Mohamed2
1Department of Internal Medicine, Mogadishu Somali Turkey, Training and Research Hospital, Mogadishu, Somalia; 2Department of Radiology, Mogadishu Somali Turkey, Training and Research Hospital, Mogadishu, Somalia
Correspondence: Ahmed Muhammad Bashir, Department of Internal Medicine, Mogadishu Somali Turkey, Training and Research Hospital, Mogadishu, Somalia, Email [email protected]
Abstract: Nephrotic Syndrome (NS) patients are prone to develop deep venous thrombosis as a complication. But it is unusual to present initially with multiple venous thrombosis and pulmonary artery thrombosis before the diagnosis of NS. Here, we present 60 years old female patient with a known history of diabetes mellitus who presented with shortness of breath and lower limb edema for 2 weeks. CT angiography showed thromboembolism at the right main pulmonary artery and its bronchus intermedius, lower and segmental with right lower lobe small pulmonary infarction and inferior vena cava (IVC) thrombosis extending in both renal veins, right common and left common iliac vein, moderate ascites. Her 24-hour urinary protein was 6.7g. a diagnosis of NS was reached and she was admitted to the ward. Anticoagulation with heparin and warfarin, methyl prednisone, and furosemide was initiated. After she become clinically stable, she was discharged with oral medications. Awareness of the complication of nephrotic syndrome is important not only to nephrologists but to all physicians. Using contrast-enhanced computed tomography to diagnose multiple venous and pulmonary arterial thrombosis is critical. Additionally, it is known that steroid-resistant NS, like membranous glomerulonephritis, are more susceptible to the complication of thromboembolism than steroid-sensitive NS. Contrast venography is used to diagnose DVT. CTPA is the gold standard test for pulmonary embolism.
Keywords: pulmonary artery thrombosis, nephrotic syndrome, multiple venous thromboembolism
Introduction
Proteinuria of ≥3.5 g/24 hours, albuminemia <of 3.0 g, peripheral edema, hyperlipidemia, lipiduria, and increased thrombotic risk are all characteristics of nephrotic syndrome (NS).1 NS is classified into two types based on its etiology: primary NS and secondary NS. Additionally, secondary causes of NS can be classified as NS-associated systemic disorders and NS-associated pharmaceutical usage. After removing identified causes like malignancy, systemic illnesses, and drugs, the most common main causes of NS are focal segmental glomerulosclerosis (FSGS), membranous nephropathy (MN), and minimal change disease (MCD).2 Diabetes mellitus, systemic lupus erythematosus, multiple myeloma, amyloidosis, malignancy, and infections are all common causes of NS secondary to systemic diseases.2 Pamidronate, nonsteroidal anti-inflammatory medicines, penicillamine, and gold compounds are only a few of the medications that have been linked to the development of NS.2 The incidence of NS is two to seven per 100,000 children,3 while its three per 100,000 adults.2
There are two types of NS complications: disease-related and drug-related issues. Infections (eg, peritonitis, sepsis, cellulitis, and chicken pox), thromboembolism (eg, venous thromboembolism and pulmonary embolism), hypovolemic crisis (eg, abdominal pain, tachycardia, and hypotension), cardiovascular problems (eg, hyperlipidemia), acute renal failure, anemia, and others (eg, hypothyroidism, hypocalcemia, bone disease, and intussusception) are among the disease-related complications. Corticosteroids, alkylating agents, cyclosporin A, and mycophenolate mofetil have treatment-related complications.4
Nephrotic Syndrome (NS) patients tend to develop venous thrombosis, particularly deep vein thrombosis (DVT) and renal vein thrombosis (RVT).5 The overall risk of venous thrombosis is 1.0% per year, which is eight times greater than the Worcester DVT study’s age- and sex-matched annual incidence.6 It is also known that steroid-resistant NS have a greater risk of thromboembolism as a complication than steroid-sensitive NS.4 Immobility, oedema, a concomitant prothrombotic tendency, and a history of thromboembolic events must all be considered, although no “threshold” of proteinuria or hypoalbuminemia has been established as a trigger for anticoagulation. In NS, the risk of venous thrombosis is higher when serum albumin is <20–25 g/l.2
Contrast venography has been the gold standard for determining the diagnosis of deep vein thrombosis.7 Computed tomography pulmonary angiography (CTPA) is the gold standard test for the diagnosis of pulmonary embolism.8
The lack of large-scale studies of NS in Africa that address crucial questions about incidence and outcomes reflects the limited resources available, which include medical records, diagnostics, medications, and clinical and research staff.9,10
Here, we present an adult case of an unusual combination of multiple venous and pulmonary artery thrombosis as the presentation of nephrotic syndrome.
Case Report
A 60-year-old woman presented to the emergency room with a complaint of lower limb edema and shortness of breath with exertion on movement over the past 2 weeks. She had a history of diabetes mellitus for 15 years, for which she took glibenclamide and metformin 5/500 mg twice a day.
She was conscious and oriented to time, place, and person during the examination. She looked ill, anxious, in respiratory distress and edematous. She had decreased breath sounds in both lungs and her heart sounds were normal. Bilateral 3+ pitting edema was positive for the lower extremity. The other physical examinations were unremarkable. On room air, the heart rate was 81 beats per minute, the blood pressure was 120/60 mmHg, the temperature was 36.2 degrees Celsius, the respiratory rate was 26 breaths per minute, and the oxygen saturation was 95%.
On laboratory investigation: White blood count (WBC) 6.34xx1000/mm3, Hemoglobin 8.9g/dl, Platelets 346x1000/mm3, Creatinine 1.87mg/dL, alanine transaminase 8U/L, total protein 4g/dl, albumin 1.4g/dl, corrected calcium 8.9mg/dl. Total cholesterol 156mg/dl, triglyceride 159 mg/dl, HDL 48mg/dl, LDL 83 mg/dl, sodium 144, potassium 2.38, CRP 60mg/dl and 24 hour’s urinary protein was 6.7g. Hepatitis B, C and HIV were negative.
Chest x-ray showed bilateral pleural effusion, EKG and echocardiography were normal. CT angiography was requested to exclude pulmonary embolism and showed thromboembolism at the right main pulmonary artery and its bronchus intermedius, lower and segmental with right lower lobe small pulmonary infraction (Figure 1) and inferior vena cava (IVC) thrombosis extending in both renal veins, right common and left common iliac vein, moderate ascites (Figures 2 and 3).
 |
Figure 1 A CT pulmonary angiography (CTPA) revealed a filling defect in the pulmonary arterial phase in the right main pulmonary artery cava. and right pleural effusion. |
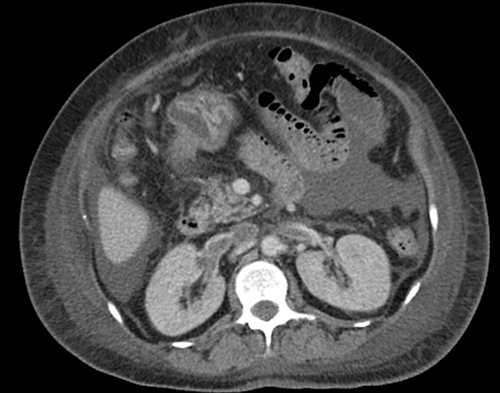 |
Figure 2 Contrast-enhanced CT image shows linear hypodense thrombus in IVC and bilateral renal veins. |
 |
Figure 3 Contrast-enhanced CT image at the level of the diaphragm shows a filling defect (thrombus) in the inferior vena cava. and perihepatic free fluid. |
We reached a diagnosis of Nephrotic syndrome complicated by multiple venous and pulmonary artery thrombosis. We started with on low molecular weight heparin, warfarin 5mg, methylprednisolone 60mg, ramipril 5mg, furosemide 80mg and potassium replacement.
After 1 week of admission, patient clinically improved, and she was discharged with medications and follow up with internal medicine outpatient was recommended.
Discussion
Patients with NS have an increased risk of thrombosis, both arterial and venous. The severity of proteinuria and hypoalbuminemia is related to venous thromboembolism, including pulmonary artery thrombosis, whereas a glomerular filtration rate and many classic atherosclerotic risk factors are related to less frequency of arterial thromboembolism.11 Patients who have had pulmonary artery thrombosis with NS are very rare, especially in adults. Pulmonary artery thrombosis has mostly been reported in children with nephrotic syndrome. Most of these cases occur during the treatment of massive generalized edema with steroids and aggressive diuretic therapy.12
As per our patient with a known case of diabetes mellitus, who presented with shortness of breath and lower limb edema at the first presentation, the diagnosis was missed due to the inappropriate CT imaging of the chest and less clinical suspicion due to her age, as nephrotic syndrome is commonly seen in children. The other scenario in this case that makes the diagnosis very challenging is the lack of kidney biopsy, which is required to determine what type of nephrotic syndrome is the diagnosis so that the patient can be managed accordingly.
A study by Uezono et al found that diabetic adult patients with nephrotic syndrome are often diagnosed with focal glomerulosclerosis (23%), minimal change disease (19%), and membranous nephropathy (15%) based on biopsy specimens.13 The nephrotic syndrome patients are more likely to have primary glomerular disease than secondary glomerular disease as the underlying cause. This is true except in one report,14 which found that benign nephrosclerosis was very common, especially in the elderly (80 years and above) with nephrotic syndrome. This clearly shows that we should not always assume nephrotic syndrome in our adult patients as secondary, and renal biopsy may be needed if there is no contraindication. In most of developing countries, kidney biopsy is not always available, which further complicates treatment decisions. Due to the small number of nephrologists, it can also be difficult to treat nephrotic syndrome.
In nephrotic syndrome, preventing thromboembolic events with oral anticoagulants necessitates a thorough case-by-case assessment of the risks of thromboembolic events balanced by the risks of anticoagulant-induced bleeding.15
Despite the lack of evidence, corticosteroids are often used in the treatment of NS. Corticosteroids and other immunosuppressive therapies have been studied for use in NS in recent years.16 If NS is steroid-resistant or does not improve, other immunosuppressive treatments should be considered in cooperation with a nephrologist. This will be difficult in Somalia, a war-torn country, where there is a very limited number of nephrologists.
Conclusion
This case illustrates the subtle appearance that multiple venous and pulmonary artery thrombosis might have in the nephrotic syndrome and we recommend our physicians should show high clinical suspicion to reach diagnosis earlier and treat effectively. Using contrast-enhanced computed tomography to diagnose multiple venous and pulmonary arterial thrombosis is critical.
Ethical Approval and Patient Consent
Ethical approval is waived from case reports in our hospital. Written and informed consent was taken from the patient for the publication of the case.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Stewart Cameron JH, Hicks J. The origins and development of the concept of a “nephrotic syndrome”. Am J Nephrol. 2002;22(2–3):240–247. doi:10.1159/000063768
2. Hull RP, Goldsmith DJA. Nephrotic syndrome in adults. BMJ. 2008;336(7654):1185–1189. doi:10.1136/bmj.39576.709711.80
3. Hilmanto D, Mawardi F, Lestari AS, Widiasta A. Disease-associated systemic complications in childhood nephrotic syndrome: a systematic review. Int J Nephrol Renovasc Dis. 2022;15:53–62. doi:10.2147/IJNRD.S351053
4. Se Jin Park JIS, Shin JI. Complications of the nephrotic syndrome. Korean J Pediatr. 2011;54(8):322–328. doi:10.3345/kjp.2011.54.8.322
5. Radhakrishnan J. Hypercoagulability in nephrotic syndrome – uptodate; 2020:1–18. Available from: https://www.uptodate.com/contents/hypercoagulability-in-nephrotic-syndrome.
6. Anderson FA, Wheeler HB, Goldberg RJ, et al. A population-based perspective of the hospital incidence and case-fatality rates of deep vein thrombosis and pulmonary embolism: the Worcester DVT study. Arch Intern Med. 1991;151(5):933–938. doi:10.1001/archinte.1991.00400050081016
7. Tovey C, Wyatt S, Charles P. Clinical review thrombosis treatment. Br Med J. 2003;326:1180–1184. doi:10.1136/bmj.326.7400.1180
8. Estrada-Y-Martin RM, Oldham SA. CTPA as the gold standard for the diagnosis of pulmonary embolism. Int J Comput Assist Radiol Surg. 2011;6(4):557–563. doi:10.1007/s11548-010-0526-4
9. Bhimma R, Adhikari M, Asharam K. Steroid-resistant nephrotic syndrome: the influence of race on cyclophosphamide sensitivity. Pediatr Nephrol. 2006;21(12):1847–1853. doi:10.1007/s00467-006-0276-2
10. Yao Doe J, Funk M, Mengel M, Doehring E, Ehrich JHH. Nephrotic syndrome in African children: lack of evidence for “tropical nephrotic syndrome”? Nephrol Dial Transplant. 2006;21(3):672–676. doi:10.1093/ndt/gfi297
11. Mahmoodi BK, Ten Kate MK, Waanders F, et al. High absolute risks and predictors of venous and arterial thromboembolic events in patients with nephrotic syndrome: results from a large retrospective cohort study. Circulation. 2008;117(2):224–230. doi:10.1161/CIRCULATIONAHA.107.716951
12. Robert L, Zimmerman SN, James TT, Chen VR. Pulmonary thrombosis in a 10-year-old child with minimal change disease and nephrotic syndrome. Anat Pathol. 1993;101(2):230–236.
13. Uezono S, Hara S, Sato Y, et al. Renal biopsy in elderly patients: a clinicopathological analysis. Ren Fail. 2006;28(7):549–555. doi:10.1080/08860220600840165
14. Nair R, Bell JM, Walker PD. Renal biopsy in patients aged 80 years and older. Am J Kidney Dis. 2004;44(4):618–626. doi:10.1016/S0272-6386(04)00944-8
15. Glassock RJ. Prophylactic anticoagulation in nephrotic syndrome: a clinical conundrum. J Am Soc Nephrol. 2007;18(8):2221–2225. doi:10.1681/ASN.2006111300
16. Chen Y, Schieppati A, Chen X, et al. Immunosuppressive treatment for idiopathic membranous nephropathy in adults with nephrotic syndrome (Review). Cochrane Database Syst Rev. 2014;(10). doi:10.1002/14651858.CD004293.pub3
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.