Back to Journals » Infection and Drug Resistance » Volume 19
Multiple Intracranial Nocardia brevicatena Abscesses in a Patient with a Previous History of Tuberculosis: A Case Report
Authors Li Z, Zhang Y, Zhang X, Li H, Gong X, Zhang Q, Xu J, Cheng X, Wang J, Wang T, Zhang Q, Yang Q, Zhao C
Received 13 February 2026
Accepted for publication 24 March 2026
Published 15 April 2026 Volume 2026:19 603379
DOI https://doi.org/10.2147/IDR.S603379
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Zhaoyang Li,1,* Yuheng Zhang,1,* Xiaoming Zhang,1,* Hongchun Li,2,* Xue Gong,2,* Qian Zhang,2,* Jing Xu,2,* Xiaofeng Cheng,2,* Jinghuan Wang,2,* Tao Wang,2 Qiuxin Zhang,3 Qingwu Yang,2,4 Chenhao Zhao2
1College of Basic Medicine, Army Medical University, Chongqing, 404100, People’s Republic of China; 2Department of Neurology, Xinqiao Hospital, Army Medical University, Chongqing, 400037, People’s Republic of China; 3Graduate School, North Sichuan Medical College, Nanchong, Sichuan, 637002, People’s Republic of China; 4Chongqing Institute for Brain and Intelligence, Guangyang Bay Laboratory, Chongqing, 400064, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qingwu Yang, Department of Neurology, Xinqiao Hospital, Army Medical University, No. 83, Xinqiao Main Street, Shapingba District, Chongqing, People’s Republic of China, Email [email protected] Chenhao Zhao, Department of Neurology, Xinqiao Hospital, Army Medical University, No. 83, Xinqiao Main Street, Shapingba District, Chongqing, People’s Republic of China, Email [email protected]
Background: Nocardia brevicatena (N. brevicatena) is an uncommon cause of brain infections, frequently mistaken for intracranial tuberculosis, especially in patients with a tuberculosis (TB) history, leading to improper treatment. This case report outlines the symptoms, diagnosis, and treatment of a patient with multiple brain abscesses from N. brevicatena after laryngeal TB, highlighting the importance of next-generation sequencing (NGS) for accurate diagnosis.
Case Presentation: This report details a 55-year-old man with a history of TB. Symptoms included dizziness, headache, and unsteady gait, with MRI revealing brain nodules and edema. He initially received anti-TB treatment, but it was ineffective. NGS identified N. brevicatena, and TB tests were negative. He was treated with anti-Nocardia drugs (compound sulfamethoxazole tablets (0.96 g, orally twice daily), amikacin sulfate injection (0.6 g, once daily), and imipenem-cilastatin sodium (0.5 g, every 6 hours)), leading to symptom improvement and MRI changes. Symptoms worsened when treatment was paused but resolved within a week of resuming therapy, following 45 days of treatment, the patient fulfilled the discharge criteria. After seven months, the patient fully recovered with normal MRI results.
Conclusion: Intracranial N. brevicatena infections are frequently misdiagnosed as TB in patients with a TB history. NGS of blood or cerebrospinal fluid accurately detects pathogens, and TB Xpert helps rule out TB. Both are crucial for targeted treatment and better patient outcomes.
Keywords: case report, Nocardia, intracranial infection
Introduction
Nocardia is a gram-positive opportunistic actinomycete. Nocardial infections of the central nervous system are clinically rare, and the multifocal intracranial subtype is even less frequently encountered, with cases predominantly reported in immunocompromised individuals.1 Insidious onset and atypical clinical manifestations are observed in this disease, and imaging findings are easily misdiagnosed as tuberculosis, fungal abscesses or intracranial tumors, leading to a low early diagnostic rate.2 Rapid disease progression, high mortality, prolonged treatment duration and frequent recurrence are documented, which bring considerable challenges to clinical diagnosis and management. In the present case report, one patient with multifocal intracranial nocardiosis is described. The clinical features, diagnostic procedures and therapeutic regimens are analyzed, so as to provide a reference for the clinical management of similar cases.
Case Presentation
A 55-year-old male patient with a history of pulmonary tuberculosis (TB) presented with persistent dizziness, paroxysmal severe throbbing headaches primarily localized to the vertex, and an unsteady gait. On admission, the patient’s axillary body temperature was 36.5 °C, and the temperature remained below 37 °C throughout the entire initial hospital stay. A chest computed tomography (CT) scan revealed interstitial changes in both lungs, as well as multiple infections and partial consolidation of lung tissue. Pathological examination confirmed laryngeal TB. An enhanced magnetic resonance imaging (MRI) scan of the head showed multiple nodules in the bilateral parieto-occipital lobes, basal ganglia, left temporal lobe, and pons (Figure 1). These nodules were accompanied by significant cerebral edema. Small, spherical, peripheral, enhancing nodules were observed with extensive perilesional edema (Figure 1A–C). No thin meningeal enhancement was detected. No Cryptococcus was detected in the cerebrospinal fluid (CSF) using three staining methods. Aerobic bacterial culture of CSF performed for 10 consecutive days yielded negative results, with no bacterial or fungal growth observed.
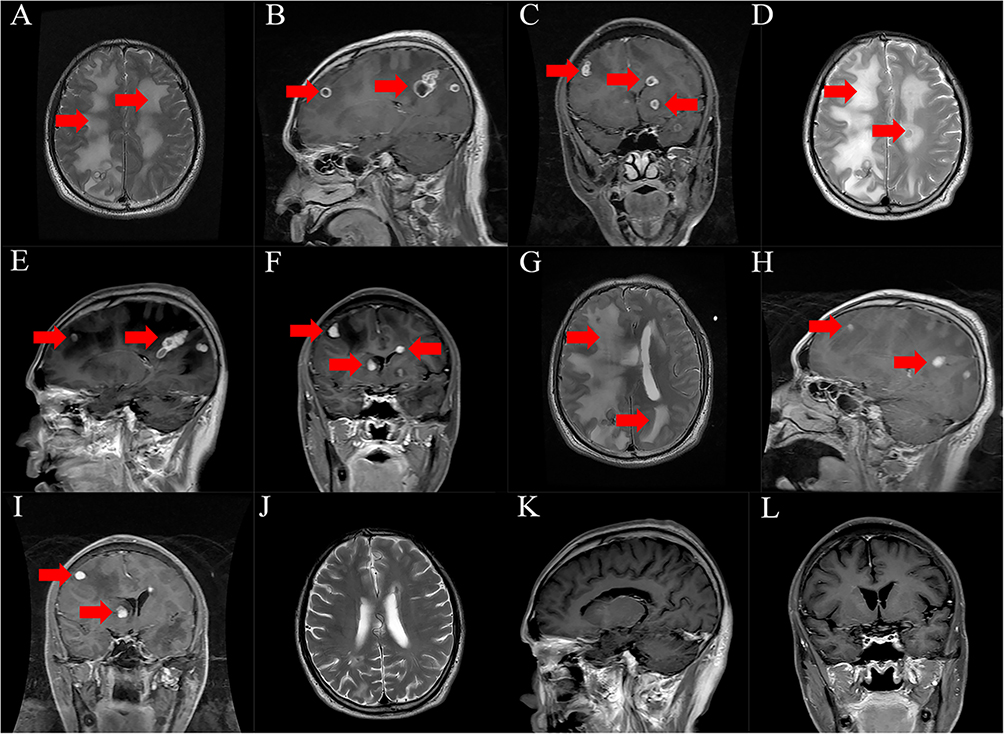 |
Figure 1 T1 FLAIR sequence shows a large edematous lesion (A). Images (B and C) (both T1 FLAIR) show multiple abscess lesions. Imaging findings of recurrence after the patient discontinued medication on his own (Images (D–F)). Following the reinstitution of anti-Nocardia therapy, the patient’s symptoms improved significantly, (G–I). On T2 FLAIR sequence (J), the edema is significantly reduced compared to the previous image (A–I). On T1 FLAIR sequences (K and L), the multiple intracranial abscess lesions have disappeared. |
Initially, the presence of positive laryngeal TB pathology suggested the possibility of multiple intracranial TB infections. However, TB treatment was ineffective. Subsequent tests were conducted for parasites and fungi. Next-generation sequencing (NGS) of blood and cerebrospinal fluid samples identified Nocardia brevicatena (N. brevicatena) (Figure 2A and B), and the TB Xpert results were negative. This confirmed the presence of multiple intracranial N. brevicatena infections. Meanwhile, we implemented a multidisciplinary team (MDT) consultation approach involving departments including Neurology, Respiratory Medicine, and Clinical Pharmacy. Through this MDT collaboration, we administered symptomatic and supportive treatments to the patient, encompassing dehydration therapy for intracranial hypertension reduction, neuroprotective therapy, nutritional support, targeted analgesia, and maintenance of electrolyte balance. Concurrently, the triple antimicrobial therapy regimen was ultimately determined, consisting of compound sulfamethoxazole tablets (0.96 g, orally twice daily), amikacin sulfate injection (0.6 g, once daily), and imipenem-cilastatin sodium (0.5 g, every 6 hours). Following one week of treatment, the patient’s condition was significantly improved. Upon discharge, the patient independently discontinued the prescribed medication and opted to resume anti-TB treatment. Two months later, the patient’s condition critically deteriorated, characterized by drowsiness, necessitating readmission. On readmission, the patient’s body temperature was 37.2 °C. During the second hospital stay, body temperature exhibited a slightly elevated trend compared with the first admission, with a peak temperature of 38.9 °C documented on the night of September 3, 2024. Concurrently, the patient’s mean heart rate was significantly higher than that recorded at the initial admission, manifesting as a clinical pattern of overall elevated heart rate with relatively low body temperature—defined as temperature–heart rate dissociation, which suggests the possibility of occult shock. An enhanced MRI of the brain revealed multiple nodules located in the bilateral parieto-occipital lobes, basal ganglia, left temporal lobe, and brainstem, accompanied by significant cerebral edema. Compared to the previous imaging, the walls of certain ring-enhanced lesions were thicker, and some lesions had grown larger with an expanded area of surrounding edema (Figure 1D–F). After re-initiating anti-Nocardia therapy——, these symptoms began to subside approximately one week later (Figure 1G–I), and after 45 days of treatment, the patient had achieved sufficient clinical recovery to meet the discharge criteria. Over the subsequent seven-month follow-up, the patient’s clinical symptoms resolved completely, and MRI scans of the brain returned to normal (Figure 1J–L).
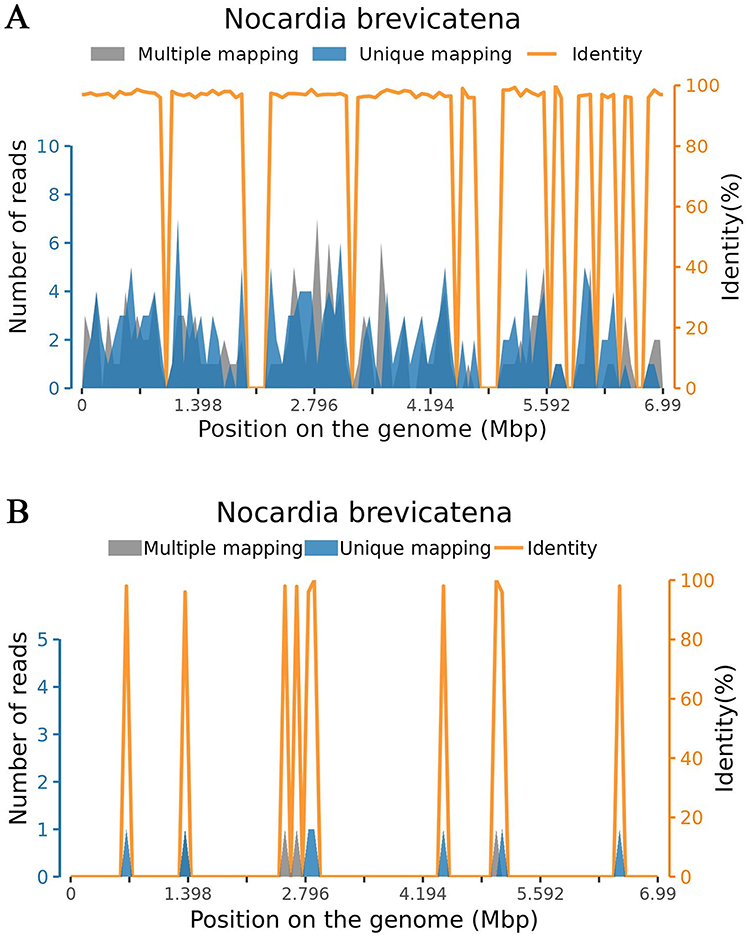 |
Figure 2 Sequence alignment and identity profile of Nocardia brevicatena detected by NGS. Multiple Mapping: reads aligning to ≥2 microbial species, representing conserved genomic regions (not counted as species-specific sequences); Unique Mapping: reads uniquely aligned to N. brevicatena, the core indicator of pathogen presence; Identity: percentage of base-pair matches to the reference genome, approaching 100% in mapped regions, confirming alignment accuracy. (A) Cerebrospinal fluid (CSF) sample. (B) Peripheral blood sample. The markedly higher number of species-specific sequences in CSF suggests a greater likelihood of primary intracranial nocardiosis. |
Discussion and Conclusions
Nocardia spp. are opportunistic pathogens mainly causing lung infections,3 but they can also affect the skin, soft tissues, and CNS, with CNS nocardiosis having a 22.8% mortality rate.4–6 Nocardia farcinica is the most common species, while Nocardia brevicatena is rare,3,5,7 with few cases reported.8 Nocardia brevicatena, part of the N. brevicatena/N. paucivorans complex (including type II drug susceptibility pattern), as one of the six major pathogenic complexes within the genus Nocardia, cannot break down casein, xanthine, tyrosine, or hypoxanthine and only uses trehalose as a carbon source. It is distinguished from N. paucivorans by its ability to utilize isoamyl alcohol and 1,2-propanediol, as confirmed by DNA–DNA hybridization.9–12 The susceptibility pattern R(resistance)S(susceptibility)SR to gentamicin, tobramycin, amikacin, and erythromycin further differentiates N. brevicatena from other Nocardia species.11
This document presents the first case of multiple intracranial N. brevicatena infection alongside Mycobacterium tuberculosis coinfection, offering potential insights for improving diagnosis and treatment of N. brevicatena infections.
A definitive diagnosis was crucial for this case. Considering the patient’s history of laryngeal and pulmonary tuberculosis, cerebral tuberculoma was a key differential diagnosis. Active tuberculosis was ruled out due to negative acid-fast bacilli results in CSF and sputum cultures. Brain abscess was excluded through bacterial cultures of CSF and blood. Cranial MRI and parasitic antibody tests helped rule out parasitic intracranial infections. Intracranial tumors were preliminarily excluded using tumor marker detection.
The presence of interstitial pneumonia and pulmonary infection, shown as patchy and honeycomb-like opacities in both lungs, required linking to the patient’s long-term dust exposure and pulmonary alveolar proteinosis. Given the patient’s history of tuberculosis, a multifactorial cause is possible. No immunodeficiency disorders or immunosuppressive treatments were found, suggesting that impaired immunity from previous lung injury might be a mechanism for the co-infection.
As an emerging sequencing modality, NGS presents irreplaceable value in the diagnosis of infectious diseases, particularly for the identification of rare, novel, or non-culturable pathogens, thereby providing a more comprehensive and innovative perspective on microbial communities than conventional culture methods.13 Compared with conventional culture approaches, NGS exhibits distinct advantages for the diagnosis of nocardiosis in terms of turnaround time, diagnostic accuracy, and the detection of mixed infections.14–18 Despite its rapid, broad, efficient, and robust detection capabilities,19–23 the limitations of NGS warrant considerable attention. These limitations include, but are not limited to, potential nucleic acid contamination, sophisticated data interpretation workflows, and challenges in the identification of antimicrobial resistance genes; furthermore, the longstanding conundrum of distinguishing colonizing agents from pathogenic pathogens remains unresolved.13,24,25
N. brevicatena is an uncommon pathogen that causes brain infections. Early diagnosis is challenging in patients with a history of TB and N. brevicatena brain infection because detecting the pathogen in brain infections is difficult. This can potentially lead to a misdiagnosis of brain TB. NGS of blood and cerebrospinal fluid testing can identify the pathogen, and TB Xpert can help rule out TB infection, aiding in the diagnosis and treatment of N. brevicatena infections.26
Data Sharing Statement
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.
Ethics Approval and Consent to Participate
The participants provided their written informed consent to participate in this study. Meanwhile, this study has been reviewed and approved by the Medical Ethics Committee of the Second Affiliated Hospital of Army Medical University, PLA. The patient provided consent for the publication of the case details. This case report was conducted in accordance with the institutional policy of Xinqiao Hospital, Army Medical University, regarding the publication of anonymized case reports. Formal ethics committee approval was not required as per this policy, given that the report involves no experimental intervention, and all patient data have been fully anonymized.
Consent for Publication
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author Contributions
Zhaoyang Li, Yuheng Zhang, Xiaoming Zhang, Hongchun Li, Xue Gong, Qian Zhang, Jing Xu, Xiaofeng Cheng, and Jinghuan Wang are co-first authors. Tao Wang and Qiuxin Zhang are co-second authors. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Chongqing Center for Prevention and Treatment of Cardiovascular and Cerebrovascular Diseases (No. 2022C060). National Science and Technology Major Project of China: Study on Early Warning and Treatment of Ineffective Reperfusion and Critical Complications of Reperfusion Therapy for Acute Ischemic Stroke, Grant No. 2024ZD0527900. 2022 General Program of Chongqing Science and Technology Bureau, Grant No. CSTB2022NSCQ-MSX0196. 2024 Young Doctor Research Fund Project of the Second Affiliated Hospital of Army Medical University, Grant No. 2024YQB004.
Disclosure
The authors declare that they have no competing interests.
References
1. Machiavello Roman FJ, Grubman A, Yakubu R, Peaper D, Azar MM, Farhadian SF. Nocardiosis in immunocompromised hosts: a retrospective, single-center analysis of clinical and microbiological determinants of central nervous system involvement. Transpl Infect Dis. 2026;e70183. doi:10.1111/tid.70183
2. Li X, Zhou W, Zhao K, Li Y. A case of disseminated nocardia infection with initial symptoms manifesting as cognitive impairment: case report and literature review. Medicine. 2024;103(49):e39535. doi:10.1097/MD.0000000000039535
3. Saubolle MA, Sussland D. Nocardiosis: review of clinical and laboratory experience. J Clin Microbiol. 2003;41(10):4497–6. doi:10.1128/JCM.41.10.4497-4501.2003
4. Lynch JP, Reid G, Clark NM. Nocardia spp.: a rare cause of pneumonia globally. Semin Resp Crit Care Med. 2020;41(4):538–554. doi:10.1055/s-0040-1708816
5. Meena DS, Kumar D, Bohra GK, Midha N, Garg MK. Clinical characteristics and treatment outcome of central nervous system nocardiosis: a systematic review of reported cases. Med Principles Pract. 2022;31(4):333–341. doi:10.1159/000525509
6. Gao S-Q, Huang J-W, Guo Y. Diagnosis and treatment of hydrocephalus caused by intracranial Nocardia infection: a case report and review of the literature. Brain Disord. 2025;19:100251. doi:10.1016/j.dscb.2025.100251
7. Anagnostou T, Arvanitis M, Kourkoumpetis TK, Desalermos A, Carneiro HA, Mylonakis E. Nocardiosis of the central nervous system: experience from a general hospital and review of 84 cases from the literature. Medicine. 2014;93(1):19–32. doi:10.1097/MD.0000000000000012
8. Li X, Zhuang S, He L, Wang S, Zhao M, Lyu X. Brain abscess caused by Nocardia brevicatena in an immunocompetent patient: a case report. Infect Drug Resist. 2022;15:7693–7697. doi:10.2147/IDR.S396085
9. Yassin AF, Rainey FA, Burghardt J, Brzezinka H, Mauch M, Schaal KP. Nocardia paucivorans sp. nov. Int J Systematic Evolutionary Microbiol. 2000;50 Pt 2(2):803–809. doi:10.1099/00207713-50-2-803
10. Brown-Elliott BA, Brown JM, Conville PS, Wallace RJ. Clinical and laboratory features of the Nocardia spp. based on current molecular taxonomy. Clin Microbiol Rev. 2006;19(2):259–282. doi:10.1128/CMR.19.2.259-282.2006
11. Kiska DL, Hicks K, Pettit DJ. Identification of medically relevant nocardia species with an abbreviated battery of tests. J Clin Microbiol. 2002;40(4):1346–1351. doi:10.1128/JCM.40.4.1346-1351.2002
12. Wilson JW. Nocardiosis: updates and clinical overview. Mayo Clin Proc. 2012;87(4):403–407. doi:10.1016/j.mayocp.2011.11.016
13. Zhao Y, Zhang W, Zhang X. Application of metagenomic next-generation sequencing in the diagnosis of infectious diseases. Front Cell Infect Microbiol. 2024;14:1458316. doi:10.3389/fcimb.2024.1458316
14. Fan N, Fang H, Huang F, et al. Metagenome next-generation sequencing plays a key role in the diagnosis and selection of effective antibiotics on the treatment of nocardia pneumonia: a case report. Front Med. 2024;11:1373319. doi:10.3389/fmed.2024.1373319
15. Zheng X, Zou W, Zou S, Ye J, Bao Z, Song Y. Diagnostic significance of metagenomic next-generation sequencing in immunocompromised patients with suspected pulmonary infection. Immunology. 2025;175(1):112–122. doi:10.1111/imm.13911
16. Huang T, Chen Y, Zhang J, et al. Rapid and accurate diagnosis of brain abscess caused by nocardia asiatica with a combination of Ziehl-Neelsen staining and metagenomics next-generation sequencing. Eur J Neurol. 2021;28(1):355–357. doi:10.1111/ene.14533
17. Weng SS, Zhang HY, Ai JW, et al. Rapid detection of nocardia by next-generation sequencing. Front Cell Infect Microbiol. 2020;10:13. doi:10.3389/fcimb.2020.00013
18. Jiao M, Ma X, Li Y, et al. Metagenomic next-generation sequencing provides prognostic warning by identifying mixed infections in nocardiosis. Front Cell Infect Microbiol. 2022;12:894678. doi:10.3389/fcimb.2022.894678
19. Han D, Li Z, Li R, Tan P, Zhang R, Li J. mNGS in clinical microbiology laboratories: on the road to maturity. Crit Rev Microbiol. 2019;45(5–6):668–685. doi:10.1080/1040841X.2019.1681933
20. Rodino KG, Simner PJ. Status check: next-generation sequencing for infectious-disease diagnostics. J Clin Invest. 2024;134(4). doi:10.1172/JCI178003
21. Zhang W, Wu T, Guo M, et al. Characterization of a new bunyavirus and its derived small RNAs in the brown citrus aphid, Aphis citricidus. Virus Genes. 2019;55(4):557–561. doi:10.1007/s11262-019-01667-x
22. Gu W, Deng X, Lee M, et al. Rapid pathogen detection by metagenomic next-generation sequencing of infected body fluids. Nature Med. 2021;27(1):115–124. doi:10.1038/s41591-020-1105-z
23. Mu S, Hu L, Zhang Y, et al. Prospective evaluation of a rapid clinical metagenomics test for bacterial pneumonia. Front Cell Infect Microbiol. 2021;11:684965. doi:10.3389/fcimb.2021.684965
24. Liu BM, Mulkey SB, Campos JM, DeBiasi RL. Laboratory diagnosis of CNS infections in children due to emerging and re-emerging neurotropic viruses. Pediatr Res. 2024;95(2):543–550. doi:10.1038/s41390-023-02930-6
25. Liu BM. Epidemiological and clinical overview of the 2024 Oropouche virus disease outbreaks, an emerging/re-emerging neurotropic arboviral disease and global public health threat. J Med Virol. 2024;96(9):e29897. doi:10.1002/jmv.29897
26. Zhou C, Wang K, Li H, Zhang X. Idiopathic thrombocytopenic purpura with brain abscess caused by Nocardia farcinica diagnosed using metagenomics next-generation sequencing of the cerebrospinal fluid: a case report. BMC Infect Dis. 2021;21(1):380. doi:10.1186/s12879-021-06071-1
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.