Back to Journals » Risk Management and Healthcare Policy » Volume 16
Multimodality Endoscopic Approach for Benign Central Airway Stenosis in Pediatric Tuberculosis: A Case Report
Authors Li J ![]() , Zhou Y, Liu Z
, Zhou Y, Liu Z ![]() , Ye T
, Ye T
Received 28 September 2022
Accepted for publication 1 February 2023
Published 11 February 2023 Volume 2023:16 Pages 225—229
DOI https://doi.org/10.2147/RMHP.S390214
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mecit Can Emre Simsekler
Jinpei Li,1 Yu Zhou,2 Zhichao Liu,3 Taosheng Ye1
1Department of Respiratory Endoscopy, The Third People’s Hospital of Shenzhen, Shenzhen, Guangdong, 518000, People’s Republic of China; 2Department of Tuberculosis, Public Health Clinical Center of Chengdu, Chengdu, Sichuan, 610011, People’s Republic of China; 3Department of Pulmonary Medicine & Tuberculosis, The Third People’s Hospital of Shenzhen, Shenzhen, Guangdong, 518000, People’s Republic of China
Correspondence: Taosheng Ye, Email [email protected]
Abstract: More children are benefitting from the wide application of bronchoscopy as interventional therapy to complications with airway involvement. We present the case of an 11-year-old boy with tracheobronchial tuberculosis complicated by severe obstruction in the left main bronchus. Early interventional endoscopic balloon dilation and cryoablation were adopted as adjunct therapy to his anti-tuberculosis treatment and had shown satisfying treatment outcomes.
Keywords: pediatric, tuberculosis, balloon dilation procedure, bronchoscopy, interventional therapy
Introduction
Tuberculosis (TB) in children has long been recognized as an important global public health challenge. Children younger than 15 years represent 11% of the global TB caseload and 14% of the overall TB fatality.1 The high case mortality ratio is associated with a low case detection rate in bacteriologically confirmed pediatric tuberculosis. Difficulty in obtaining a quality sputum specimen, low detectable bacilli level, and the lack of specific clinical symptoms in children infected with TB are predominant risk factors leading to delayed diagnosis and treatment.2 The clinical manifestation of pulmonary TB (PTB) in children is non-specific and is frequently misinterpreted as mediastinal lymphadenopathy.
The incidence of airway suppression caused by TB in children under 15 years of age is reported to range from 8% to 38% from different literature.3 Lymphadenopathy can cause extrinsic airway compression and obstruction. Caseation in lymph nodes can herniate into the airway, leading to bronchogenic hematogenous spread. In addition, an obstructed airway can lead to poor bronchial secretion drainage, parenchymal consolidation, and atelectasis, and in the extreme case can result in structural damage to the lungs.4 However, there is limited evidence on the incidence of irreversible lung parenchymal injury caused by tuberculosis-associated airway distress in children.
With advancements in the development and application of bronchoscopy as an interventional diagnostic assay, an increasing number of pediatric bronchial tuberculosis diagnosed with these procedures has been reported in recent years. Children are also benefitting from the generalization and increasing therapeutic use of bronchoscopy in the management of airway stenosis associated with TB.5,6 The optimal time and modality of intervention in pediatrics with airway complications is still controversial. Research reported the institution of interventional treatments such as balloon dilatation, thermal ablation, cryoablation, clamping, and stent placement, after half a month to one month of anti-tuberculosis treatment, can reduce airway stenosis and pulmonary function damage in children.7–9
Here we report a pediatric tuberculosis case complicated with benign stenosis of the central airway successfully managed with bronchoscopy balloon dilation with cryotherapy at an early anti-TB treatment phase.
Case Presentation
An 11-year-old boy suspected of tuberculosis was transferred to our department from a local hospital on November 22, 2021. The patient was 47kg, 140cm tall with a BMI of 23.98. He was HIV-negative and had no previous history or exposure to tuberculosis infection. Parents reported no associated family medical history. He was born full-term and healthy and was BCG inoculated under the National Immunization Program after birth. He presented to a neighborhood hospital on November 12, 2021, for sudden onset of unexplained fever with cough. Chest computed tomography (CT) scan showed left lung consolidation with segmental atelectasis, scattered calcifications in the left upper lobe, and multiple calcifications and enlargement of lymph nodes in the mediastinum and left hilar region (Figure 1A and B). The length of stenosis of the left main bronchus was about 8mm, with about 90% obstruction of the lumen. From these clinical presentations, the patient was highly suspected of pulmonary and left bronchial tuberculosis and was referred to our tuberculosis care center.
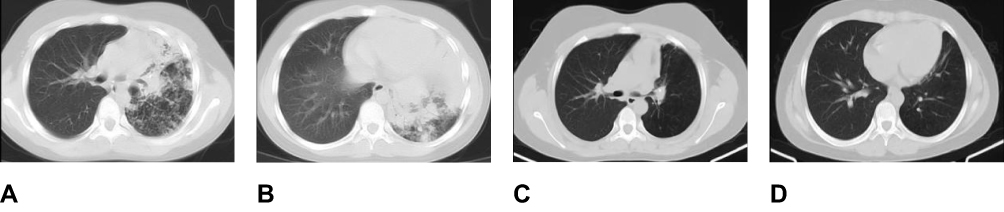 |
Figure 1 Chest computed tomography (CT) scan before and after anti-tuberculosis treatment and interventional treatment. (A and B) Segmental infiltration and consolidation in the left lung and apparent stenosis of the left main bronchus before treatment, (C and D) Improvement of left bronchus stenosis and infiltration absorption observed after therapy. |
On admission, clinical investigation revealed the onset of symptoms started ten days prior and was sudden with uncertain cause. The patient started with fever accompanied by chills, to the highest of 40°C, shivering, intermittent cough, thick white mucus production, no chest tightness, shortness of breath, or breathing difficulties, and no dizziness, headache, nausea, or vomiting. Physical respiratory system assessment showed reduced thoracic expansion on the left lung. Chest auscultation revealed reduced vocal resonance, and distinct lowered breathing sound without crackling or wheezing, all on the left lung. Sputum GeneXpert MTB/RIF for mycobacterium tuberculosis was positive, detected on a very low bacterial load, and mutation in the rpoB gene conferring resistance to rifampicin was not detected. The T-SPOT test was positive. The patient’s anti-TB therapy was initiated with isoniazid, rifampicin, and pyrazinamide on November 24, 2021. Bronchoscopy examination on the following day revealed severe scarring stenosis (grade III) on the left main bronchus, with swollen and inflammatory bronchi. The stenosis was too narrow for a catheter in a 3.8 mm diameter to pass through (Figure 2A).
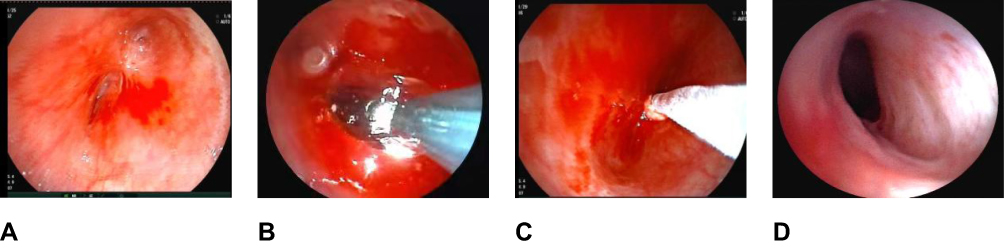 |
Figure 2 Bronchoscopy images of the left main bronchus stenosis before and after treatment. (A) Scarring stenosis of the left mainstem bronchus, (B) Balloon dilation procedure, (C) Cryoablation post dilation to reduce restenosis, (D) Obvious improvement in the patency of the left mainstem bronchus as shown in post-treatment follow-up examinations. |
Considering the severity of the airway obstruction, we performed a balloon dilation procedure on our patient on November 25, 2021, after getting consent from his parents. A balloon catheter sized 8 mm in diameter, 4 cm in length, and 2.5 atmospheres was placed to pass through the scarring stenosis. The stenosed bronchial segment was stretched open with the high-pressure balloon dilation for 60 seconds (Figure 2B). This was followed by cryotherapy for 60 seconds three times to reduce restenosis. (Figure 2C) The patient was administered the following post-procedure treatment: dexamethasone 5 mg on aerosol nebulization, once per day for a week, isoniazid 0.1 g on topical nebulization, twice per day for two months. A bronchoscopy follow-up examination on November 29 showed the patency of the treated site was good for a catheter of 3.8 mm diameter to pass through smoothly. A build-up of excessive mucus in the bronchi was observed. After clearing up, the catheter can pass to reach the distal bronchi.
Cryoablation was performed on another two occasions on November 29 and December 7, 2021, at the previously treated stenosis site.
A follow-up chest CT scan after six months of systematic anti-tuberculosis treatment showed lumen of the left main bronchus was narrow but unobstructed and patent. The rest of the bronchial tree in the left lung showed good patency. We also observed effective absorption of infiltration previously seen on the left lung (Figure 1C and D).
The patient had a follow-up bronchoscopy examination on May 12, 2022. The procedure showed the previously dilated scarring stenosed segment on the left main bronchus was still relatively narrow but with good patency and lumen diameter allowing the smooth passage of a 3.8mm diameter catheter (Figure 2D).
The patient was closely monitored over the course of his anti-TB treatment with clinical follow-up every month, chest imaging examination every three months, and bronchoscopy therapy when deemed necessary. The last follow-up assessment was in August 2022. He had a good treatment response and is now leading a normal life.
Discussion
Current literature reported an over 40% diagnostic accuracy of pediatric pulmonary tuberculosis using bronchoscopy.7 In China, benign central airway stenosis is predominantly caused by tracheobronchial tuberculosis leading to one of the following clinical challenges: 1/ oppression and occlusion against the airway 2/ inflammatory infiltration in the trachea and main bronchus, 3/ caseous lymph nodes herniating into the airways 4/ granulomatous hyperplasia, 5/ lymphatic fistula 6/ late-stage scar contracture. The most widely adopted international classification of stenosis severity is the Cotton-Myer quartile grading system quantifying severity according to the percentage of obstruction, with Grade I denoting 0–50% obstruction, grade II 51%-70%, grade III 71%-99%, and Grade IV complete obstruction. Stenosis with less than 50% airway obstruction usually does not require intervention therapy, unless presented with one of the below scenarios: 1/ severe, life-threatening, acute airway obstruction, 2/ observation of >90% obstruction in a main bronchus on first bronchoscopy examination, 3/ persistent obstruction even after four weeks of anti-TB treatment with oral Prednisone therapy, 4/ collapsing lobes due to airway suppression. All these scenarios should be actively managed with the appropriate endoscopic intervention for relieve the obstruction. Some patients even undergo surgical resection of the stenosis for long-lasting results.
The pediatric patient in our report was identified on his first bronchoscopy assessment to have stenosis with >90% obstruction in the left main bronchus. The left lung was seen to have reduced in size, showing a compromised lung volume, and obstructed with excessive mucus accumulation. To prevent our patient from further left lobar collapse due to continued or worsened airway stenosis, we performed a balloon dilation procedure to expand the narrow airway to resume smooth breathing and sputum clearing capability.
Since Cohen et al first reported the institution of balloon dilation for treating tracheal and bronchial stenosis in 1984,10 the procedure has been widely applied over the years and well established as a highly useful and essential modality in the treatment of stenosis and airway obstruction in pediatrics nowadays.
Balloon dilation is an atraumatic procedure to expand a stenosis-compromised airway with a balloon-shaped catheter. A deflated balloon is inserted to pass through the constricted airway. Water or air is used to inflate the balloon and exert pressure to stretch the stenosis causing numerous superficial longitudinal lacerations around the site, which would be healed through the repair and regeneration process. The result is the stenosis enlarged to the desired lumen diameter to restore patency.
The balloon catheter is available in a variety of sizes, the choice of which depends on the lumen diameter of the airway leading up to the stenosis site. The balloon must be long enough to widen the entire stenosis segment. Adverse events associated with balloon dilation include mild to moderate mucosal hemorrhage, rupture of the airways, pneumothorax, and pneumomediastinum.11 Mild to moderate bleeding can be managed easily with the administration of topical epinephrine at the local site. A bronchial rupture, however, is a severe complication and can result in pneumothorax and pneumomediastinum.12 In-depth assessment based on clinical symptoms, CT images and 3-Dimension construction of the stenosis before the procedure can greatly help prevent adverse events.6 There are no clear guidelines or literature references regarding the optimal balloon expansion time in the procedure. Studies have suggested an inflation time between 30 and 60 seconds in clinical practice, depending on individual circumstances.13
Cryotherapy is the use of extreme cold to freeze, destruct and remove abnormal tissue, damaging intracellular organelles, and the cell wall, and in the process trigger the body’s repair and regeneration process.14 Cryotherapy is applicable to bronchial stenosis caused by granuloma formation in the proliferative phase of tracheobronchial TB.6 The mechanism of cryoablation makes it suitable for the removal of larger granuloma by freezing the diseased tissues off. It is also proven to be highly effective in the treatment of scarring central airway stenosis caused by bronchial tuberculosis.5,9 The choice of thermal therapy for children is usually argon plasma coagulation (APC) which relies on argon gas to conduct an electrical current to perform non-contact coagulation to achieve a superficial necrosis effect on the target tissues. In the comparison of inflammatory and scar tissue formation responses to the use of cryoablation, APC, and radiofrequency, cryotherapy is reported to result in a significantly lower response of inflammation and scar tissue formation at the targeted sites in a mice experiment.14 Patients who suffer from recurrent severe scarring stenosis after receiving multiple balloon dilation and ablation reintervention procedures, or those who suffer from a collapsing lumen can consider stent placement for a long-lasting effect.15
The clinical manifestation of our patient in this study was severe airway stenosis due to necrotic adhesion of diseased tissue accompanied by inflammation, both tuberculosis associated. Given the critical condition, endoscopic balloon dilation was instituted to expand the airway, followed by cryotherapy to reduce the formation of scar tissue. A follow-up examination showed an improved airway; there was no need for further stent placement or surgical intervention.
Regarding the appropriate timing for bronchoscopy intervention therapy, there have been varying opinions documented in different studies. Goussard et al reported that bronchoscopy plays an important diagnostic role in deciding when surgery is needed or whether a condition can be treated by medication alone. As intervention therapy is associated with the risk of airway spread of TB and suggested oral prednisone therapy for a month before airway obstruction reassessment in non-life-threatening <50% airway obstruction cases. Both Liu et al and Jiao et al reported that interventional bronchoscopy should not be instituted for patients with active bronchial tuberculosis until after at least two weeks of systematic anti-TB treatment.7,16 Upon admission, our patient presented with an emergency that required immediate intervention to relieve clinical symptoms. As a primary treatment of airway stenosis, we performed an endoscopic balloon dilation procedure only a day after the initiation of his anti-TB regimen and achieved good clinical outcome. This reminds us in circumstances involving pediatric TB patients with severely obstructed airways, timely intervention is essential in preserving lumen patency and a clear airway from excessive sputum accumulation. Concurrent cryoablation therapy also aids in reducing scar tissue formation and restenosis. Our patient responded well to all the procedures. No spreading of TB had been observed during the process.
As for the management of tuberculosis, our patient was HIV-negative. His sputum Xpert MTB/RIF showed no rifampicin resistance. According to the WHO Guidance for national tuberculosis programs on the management of tuberculosis in children and adolescents 2014 edition, our patient was prescribed a 2HRZ/4HR regimen, comprising two months of intensive treatment with isoniazid, rifampicin and pyrazinamide, followed by four months of isoniazid, and rifampicin. His symptoms were relieved and chest CT image six months after the initiation of anti-TB treatment showed significant clinical improvement.
All in all, thorough preoperative assessment and appraisal should be given to children involving airway obstruction considering the severity of symptoms and all prognostic factors, especially in patients complicated with tuberculosis infection. Timely and accurate interventional therapy can be instituted at an early stage of the anti-tuberculosis treatment to deliver effective results.
Ethics Statement
Written informed consent for publication of all details included clinical data and pictures in this report was obtained from the patient’s parents. This publication of this case report was approved by the The Third People’s Hospital of Shenzhen, China.
Acknowledgments
The authors thank Doctor Peize Zhang, Ms. Jiaohong Zhang and Miss Xuan Zeng for their help in taking care of our little patient and preparing the manuscript. We greatly appreciate the patient and his family for their kind cooperation.
Funding
This study was funded by Shenzhen Science and technology innovation Commission (JCYJ20180228162336873, JCYJ20210324131603008) which is a government fund for the research of tuberculosis treatment and control. This study was also supported by Shenzhen Fund for Guangdong Provincial High-level Clinical Key Specialties (No.SZGSP010).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Jenkins HE, Yuen CM, Rodriguez CA, et al. Mortality in children diagnosed with tuberculosis: a systematic review and meta-analysis. Lancet Infect Dis. 2017;17(3):285–295. doi:10.1016/S1473-3099(16)30474-1
2. Turkova A, Wills GH, Wobudeya E, et al. Shorter treatment for nonsevere tuberculosis in African and Indian Children. N Engl J Med. 2022;386(10):911–922. doi:10.1056/NEJMoa2104535
3. Goussard P, Retief F, Burke J, Malherbe A, Janson J. The role of bronchoscopy in the diagnosis and management of pediatric pulmonary tuberculosis. Ther Adv Infect Dis. 2021;8:1998271984.
4. Andronikou S, Lucas S, Zouvani A, Goussard P. A proposed CT classification of progressive lung parenchymal injury complicating pediatric lymphobronchial tuberculosis: from reversible to irreversible lung injury. Pediatr Pulmonol. 2021;56(12):3657–3663. doi:10.1002/ppul.25640
5. Kose M, Hangul M, Erkan GN, Narin N. Fiberoptic bronchoscopic balloon dilatation of bronchial stenosis in children. J Bronchology Interv Pulmonol. 2019;26(4):260–264. doi:10.1097/LBR.0000000000000581
6. Qin L, Ding WM, Zhang JY, Wang WJ, Fu WX, Guo Y. 冷冻联合球囊扩张术治疗瘢痕狭窄型支气管结核气道闭塞的有效性及安全性 [Efficacy and safety of cryotherapy combined with balloon dilatation through electronic bronchoscope in the management of airway occlusion caused by scar stenosis type of tracheobronchial tuberculosis]. Zhonghua Jie He He Hu Xi Za Zhi. 2018;41(11):857–862. Chinese. doi:10.3760/cma.j.issn.1001-0939.2018.11.006
7. Jiao AX, Sun L, Liu F, et al. Characteristics and clinical role of bronchoscopy in diagnosis of childhood endobronchial tuberculosis. World J Pediatr. 2017;13(6):599–603. doi:10.1007/s12519-017-0046-1
8. Zhang HS, Chen XP, Ye LP, et al. 经支气管镜冷冻介入在儿童气管支气管结核诊疗中的临床应用 [Clinical application of transbronchial cryotherapy in the diagnosis and treatment of tracheobronchial tuberculosis in children]. Zhonghua Er Ke Za Zhi. 2021;59(11):963–967. Chinese. doi:10.3760/cma.j.cn112140-20210504-00378
9. Garcia-Martinez L, Lain FA, Iglesias-Serrano I, Gine PC, Soriano-Arandes A, Lopez M. Endobronchial tuberculosis in children: defining the role of interventional bronchoscopy. Pediatr Pulmonol. 2022;57(11):2688–2695. doi:10.1002/ppul.26084
10. Cohen MD, Weber TR, Rao CC. Balloon dilatation of tracheal and bronchial stenosis. AJR Am J Roentgenol. 1984;142(3):477–478. doi:10.2214/ajr.142.3.477
11. Maturo SC, Hartnick CJ. Pediatric airway balloon dilation. Adv Otorhinolaryngol. 2012;73:112–115. doi:10.1159/000334461
12. McLaren CA, Elliott MJ, Roebuck DJ. Tracheobronchial intervention in children. Eur J Radiol. 2005;53(1):22–34. doi:10.1016/j.ejrad.2004.07.022
13. Goussard P, Andronikou S, Fourie B, Janson JT, Schubert PT. Tuberculous bronchial stenosis: diagnosis and role of interventional bronchoscopy. Pediatr Pulmonol. 2022;57(10):2445–2454. doi:10.1002/ppul.26057
14. Chen Lisong CXZY. The different effects of cryoablation and thermal ablation on inflammation and scar hyperplasia in rat skin. Chin J Tubere Respir Dis. 2015;38(06):451–455.
15. Eber E, Anton-Pacheco JL, de Blic J, et al. ERS statement: interventional bronchoscopy in children. Eur Respir J. 2017;50(6):1700901. doi:10.1183/13993003.00901-2017
16. Liu Fang JA. Diagnosis and treatment of tracheobronchial tuberculosis in children. Chin J Appl Clin Pediatr. 2020;35(10):743–748.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Outcomes and Risk Factor Analysis of Plastic Bronchitis Among 321 Children with Influenza Pneumonia After Bronchoscopy Examination
Hu Q, Wu J, Wang C, Liang W, Wang Y, Zheng Y, Wen F, Wang W, Yu U
Infection and Drug Resistance 2023, 16:4001-4011
Published Date: 21 June 2023
Clinical Characteristics of Tracheobronchopathia Osteochondroplastica: A Retrospective Study of 33 Patients
Liu Q, Hu Y, Lei M, Mei C, Yang C
International Journal of General Medicine 2023, 16:3447-3455
Published Date: 14 August 2023
Factors Affecting the Integration of Pediatric TB Screening in Kabale District of Uganda: A Cross Sectional Study

Mandera I, Ayebazibwe G, Tumusiime A, Byamukama T, Mfitumukiza V, Tamu Munezero JB, Nduhukire T, Maniple EB
Pediatric Health, Medicine and Therapeutics 2024, 15:325-331
Published Date: 23 October 2024