Back to Journals » Cancer Management and Research » Volume 17

Multimodal Psychobehavioral Interventions for Lung Cancer–Related Pain: A Protocol Development and Validation Study Examining the Mediating Role of Self-Efficacy in the Relationship Between Pain Perception and Adaptive Coping Strategies
Authors Liu B, Ding Y, Xu J, Wu X, Yang X, Liu Y, Deng H ![]()
Received 6 June 2025
Accepted for publication 27 August 2025
Published 2 September 2025 Volume 2025:17 Pages 1871—1880
DOI https://doi.org/10.2147/CMAR.S537477
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sanjeev K. Srivastava
Bing Liu,* Yongyong Ding,* Junfei Xu, Xuehai Wu, Xiaofeng Yang, Yi Liu, Hong Deng
Department of Pain, The First People’s Hospital of Zunyi City, Zunyi, Guizhou, 563000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hong Deng, Department of Pain, The First People’s Hospital of Zunyi City, No. 98, North Phoenix Road, Huichuan District, Zunyi, Guizhou, People’s Republic of China, Email [email protected]
Objective: To evaluate the effects of a comprehensive intervention program on cancer pain and self-efficacy in patients with lung cancer.
Methods: A total of 120 lung cancer patients with cancer pain who received treatment from January 2021 to December 2023 at The First People’s Hospital of Zunyi were enrolled in this study. A within-subject design was used, comparing patients’ pain and self-efficacy scores before and after a comprehensive intervention. The intervention included pharmacologic therapy, psychological counseling, health education, mindfulness training, social support, and personalized rehabilitation. Pain was assessed using the Numerical Rating Scale (NRS), and self-efficacy was measured with the Chronic Disease Self-Efficacy Scale (CDSE). Subgroup and regression analyses were performed to explore related factors.
Results: After intervention, the average NRS pain score decreased significantly from 7.2 ± 1.5 to 3.8 ± 1.2 (↓ 47.22%, t=15.6, p< 0.001). Patients participating in mindfulness training reported a greater reduction in pain than non-participants (p=0.013). The total CDSE score increased from 52.3 ± 8.7 to 72.4 ± 9.5 (t=12.4, p< 0.001), with significant improvements across all subscales (self-management, general efficacy, goal achievement, and problem-solving; all p< 0.001). Subgroup analyses revealed that the improvements were consistent across gender, age groups, and education levels (p> 0.05). Logistic regression identified pain relief (NRS score) as a significant predictor of enhanced self-efficacy (OR=1.403, 95% CI: 1.125– 1.885, p=0.002), whereas age and education were not significant.
Conclusion: A comprehensive, multimodal intervention significantly improved both pain control and self-efficacy in patients with lung cancer–related pain. The effects were robust across demographic subgroups, with pain relief being a key factor influencing self-efficacy. These findings support the integration of psychological and behavioral strategies in pain management for cancer patients.
Keywords: lung cancer, cancer pain, pain perception, self-efficacy, relationship, improvement methods
Introduction
Lung cancer is one of the most common malignancies worldwide and a leading cause of cancer-related deaths. According to statistics from the World Health Organization (WHO) and the International Agency for Research on Cancer (IARC), lung cancer ranks high in both incidence and mortality globally.1,2 The incidence of lung cancer is significantly higher in men than in women, particularly among smoking men. Smoking is the most significant risk factor for lung cancer, with approximately 85% of lung cancer cases attributed to smoking. Smokers have a 10 to 20 times higher risk of developing lung cancer compared to non-smokers. Even passive smoking significantly increases the risk of lung cancer.3,4 Despite advances in medical technology improving the survival rates of lung cancer patients, cancer pain remains a common and severe symptom that significantly affects patients’ quality of life and self-efficacy. According to statistics, lung cancer patients generally experience cancer pain during the course of the disease, especially in the advanced stages. Due to factors such as tumor invasion, surgical trauma, and side effects of radiotherapy and chemotherapy, patients experience more obvious pain. Cancer pain not only affects the patient’s quality of life, but may also trigger a series of negative physiological and psychological reactions, such as anxiety, depression, and sleep disorders, further reducing the patient’s self-management ability and treatment compliance. Therefore, how to effectively relieve cancer pain in lung cancer patients and improve their self-efficacy is an urgent problem to be solved in clinical nursing and rehabilitation management.
Cancer pain not only causes physical suffering but also impairs psychological and social functions.5,6 Therefore, we believe that inadequate pain management can lead to a decrease in patients’ self-efficacy, further affecting their treatment adherence and overall rehabilitation outcomes. Self-efficacy refers to an individual’s belief in their ability to complete specific tasks or cope with challenges, playing a crucial role in the psychological adjustment of cancer patients. Patients with high levels of self-efficacy are generally better able to cope with the challenges of the disease, enhancing treatment adherence and quality of life. Pain is a complex subjective experience, which is not only affected by physiological factors, but also closely related to psychological and social factors. The self-efficacy theory was proposed by psychologist Bandura, which refers to an individual’s confidence and ability to complete a certain behavior or task. In the cancer patient population, self-efficacy is closely related to pain management, psychological adaptation and quality of life. Studies have shown that patients with higher self-efficacy tend to be more proactive in coping with the disease and adopt effective pain management strategies, thereby reducing the negative impact of pain on the body and mind. However, many lung cancer patients are prone to helplessness due to the persistent pain caused by the disease, the discomfort suffered during treatment, and concerns about the prognosis of the disease, which leads to a decrease in self-efficacy and thus falls into a vicious cycle of pain-anxiety-low efficiency. Therefore, exploring the relationship between pain and self-efficacy in patients with cancer pain from lung cancer, analyzing the influencing factors, and exploring effective ways to improve it are of great clinical value for optimizing cancer pain management and improving patients’ self-efficacy levels.
At present, the management methods of cancer pain mainly include drug therapy, physical therapy, psychological intervention and comprehensive care. The “three-step analgesia program” proposed by the World Health Organization (WHO) provides basic principles for the treatment of cancer pain, but relying solely on drugs to control pain may increase drug resistance and significant side effects. Therefore, non-drug interventions have gradually received attention in recent years, such as psychological intervention, mindfulness therapy, cognitive behavioral therapy, exercise therapy, etc., which have shown certain effects. Among them, pain management models based on self-efficacy theory, such as health education, pain cognitive reconstruction, relaxation training, etc., can help patients enhance their sense of control over pain and improve their self-management ability, thereby alleviating the adverse effects of cancer pain. However, research on self-efficacy improvement strategies for patients with lung cancer pain is still relatively limited. How to formulate personalized and multi-dimensional intervention plans based on the actual situation of patients is still the focus of current research.
This study aims to evaluate the changes in pain levels and self-efficacy in lung cancer patients with cancer pain through comprehensive interventions and explore the relationship between these two factors. We hypothesize that comprehensive interventions, including medication therapy, psychological counseling, and self-management education, can effectively alleviate patients’ pain, enhance self-efficacy, and improve their quality of life.
The specific objectives of this study include: 1) evaluating the pain levels and self-efficacy of lung cancer patients with cancer pain; 2) exploring the relationship between pain levels and self-efficacy; and 3) analyzing the effectiveness of comprehensive interventions, including medication therapy, psychological counseling, and self-management education, in alleviating pain and enhancing self-efficacy. We hope that the results of this study will provide scientific evidence for clinical practice, helping healthcare professionals better manage lung cancer patients with cancer pain and improve their quality of life.
Subjects and Methods
Study Subjects
This study included lung cancer patients with cancer pain who received treatment at our hospital from January 2021 to December 2023. After excluding subjects who did not meet the complete inclusion criteria, a total of 120 patients were enrolled. All patients were registered and their clinical data were collected. Comprehensive interventions (including medication therapy, psychological counseling, and self-management education) were administered, with the pre-intervention period serving as the control group and the post-intervention period as the study group. This study was approved by the Ethics Committee of The First People’s Hospital of Zunyi (Approval No. ZY2020-015). All patients provided informed consent before participation, and the study was conducted in accordance with the Declaration of Helsinki.
Inclusion and Exclusion Criteria
Inclusion Criteria
Clinically and pathologically confirmed diagnosis of lung cancer.7,8
Pain duration ≥30 days, with a pain score greater than 3.
Age 18 years or older, with complete clinical data.
No consciousness or communication disorders.
Ability to communicate and understand normally.
Expected survival of more than one year.
Exclusion Criteria
Severe heart, liver, or kidney insufficiency.
Presence of other malignant tumors.
Concurrent immune system diseases.
Unconsciousness or accompanied by mental disorders, non-cooperative patients.
Methods
Comprehensive intervention included drug therapy, psychological counseling, and self-management education, aiming to help lung cancer patients with cancer pain relieve pain, improve self-efficacy, and enhance overall quality of life. Specific intervention measures were as follows:
Analysis and Improvement of Nursing Work: A systematic review of prior nursing practices was conducted to identify deficiencies in pain management, patient compliance, and psychological care. Based on the findings, the nursing workflow was optimized, and a targeted nursing plan was developed.
Systematic Pain Assessment: Detailed pain assessments were conducted through face-to-face interviews and the Numerical Rating Scale (NRS). Evaluated parameters included pain perception, type (eg, persistent, breakthrough), frequency, duration, impact on daily activities, subjective pain cognition, psychological coping styles, and expectations regarding pain control.
Drug Treatment and Management: In accordance with the World Health Organization’s three-step analgesic ladder, patients received appropriate pharmacological treatment, including non-steroidal anti-inflammatory drugs (NSAIDs), weak opioids, or strong opioids based on their pain levels. Strict medication management protocols ensured correct drug use. Nurses continuously monitored treatment response, adjusted dosages as needed, and provided patient education on pharmacologic mechanisms, administration, potential side effects, and precautions to enhance treatment adherence and self-management.
Health Education and Pain Cognition Improvement: Individualized health education sessions were delivered at least once weekly (30–45 minutes per session) during the first month, followed by biweekly sessions. Nurses explained the progression of lung cancer, pain mechanisms, treatment options, and potential discomforts. Emphasis was placed on correcting pain-related misconceptions and reducing fear. Supplementary materials, including printed graphics, educational videos, and online lectures, were provided to reinforce knowledge and promote patient engagement.
Psychological Support and Emotional Counseling: Structured psychological support was offered through weekly sessions lasting 45–60 minutes, providing a safe environment for emotional expression via empathetic communication and active listening. Participation in cancer support groups was encouraged. Cognitive Behavioral Therapy (CBT) was implemented to address anxiety and depression. Mindfulness training was conducted twice weekly (20–30 minutes per session), including guided meditation and body scan techniques. Mindfulness was incorporated for its reported role in promoting β-endorphin release and contributing to analgesia.
Pain Management Skills Training: Patients received twice-weekly sessions (45–60 minutes each) focused on non-pharmacological pain management techniques. These included deep breathing exercises to alleviate muscular tension and anxiety, progressive muscle relaxation (PMR) to facilitate sequential physical relaxation, and attention diversion strategies such as listening to music, reading, or painting. Nursing staff provided individualized instruction and closely monitored patient engagement, encouraging consistent daily practice to reinforce coping skills and improve overall pain management efficacy.
Construction of Social Support System: Family members and close contacts were actively engaged in the care process through structured family meetings and accompanying training sessions. These efforts aimed to enhance emotional and practical support for patients, thereby strengthening their social support network and psychological resilience.
Personalized Exercise Rehabilitation Plan: Exercise plans were tailored to each patient’s condition and treatment phase. Patients were prescribed low-to-moderate intensity activities such as walking, stretching, Tai Chi, or yoga, conducted three to five times per week for 20–40 minutes per session. Intensity was progressively increased based on tolerance. Progress was regularly assessed, and the plan adjusted accordingly. Fatigue and sleep quality were monitored, and individualized lifestyle recommendations were provided to optimize rest and recovery.
Regular Follow-Up and Adjustment: A systematic follow-up protocol was implemented. Patients underwent regular outpatient reviews and structured nurse-led interviews using questionnaires—monthly for the first three months, then quarterly. Evaluations focused on pain perception, emotional state, and functional capacity. Intervention plans were dynamically adjusted to maintain treatment effectiveness and long-term benefits.
This multimodal intervention emphasized the integration of pharmacologic management, psychological support, health education, social involvement, and individualized rehabilitation strategies to enhance pain control, improve self-efficacy, and elevate the overall quality of life in patients with lung cancer–related pain.
Observation Indicators
Cancer Pain: Assessed using the Numerical Rating Scale (NRS), ranging from 0 (no pain) to 10 (worst imaginable pain), categorized as mild (1–3), moderate (4–6), or severe (7–10). The NRS is a widely validated, reliable, and responsive tool for pain intensity measurement in cancer populations.9 To minimize bias, assessments were conducted by trained nurses using standardized scripts in a quiet environment before other interventions or assessments.
Self-Efficacy: Assessed using the Chronic Disease Self-Efficacy Scale (CDSE). This validated scale10 measures self-efficacy in managing chronic disease across four 10-point subscales: symptom management, general self-efficacy, achieving results, and problem-solving. Higher scores indicate greater self-efficacy. The CDSE demonstrates good reliability (eg, Cronbach’s α typically >0.80) and validity. To reduce potential bias, the CDSE was administered by research assistants not involved in the direct delivery of the intervention, using standardized instructions.
Statistical Analysis
GraphPad Prism 8 was used for image processing, and SPSS 26.0 software was used for data organization and statistical analysis. Logistic regression was used to analyze the relationship between pain and self-efficacy in lung cancer patients with cancer pain. Measurement data were expressed as mean ± standard deviation (±s) and analyzed using t-tests for statistical differences. Count data were expressed as percentages (%) and analyzed using chi-square tests (χ2) to compare statistical differences. A P-value of less than 0.05 was considered statistically significant.
Results
General Data
This study included 120 patients with lung cancer pain, including 83 males (69.17%) and 37 females (30.83%). The age of the patients ranged from 28 to 70 years old, with an average of 55.88±9.33 years old. The pathological type was mainly adenocarcinoma (69 cases, 57.50%), followed by squamous cell carcinoma (51 cases, 42.50%). The distribution of residence: 52 cases (43.33%) in urban areas and 68 cases (56.67%) in rural areas. In terms of education level, 13 cases (10.83%) were primary school or below, 28 cases (23.33%) were junior high school, 42 cases (35.00%) were high school/technical secondary school, and 37 cases (30.83%) were undergraduates or above. The baseline characteristics of all patients were balanced and comparable (Table 1).
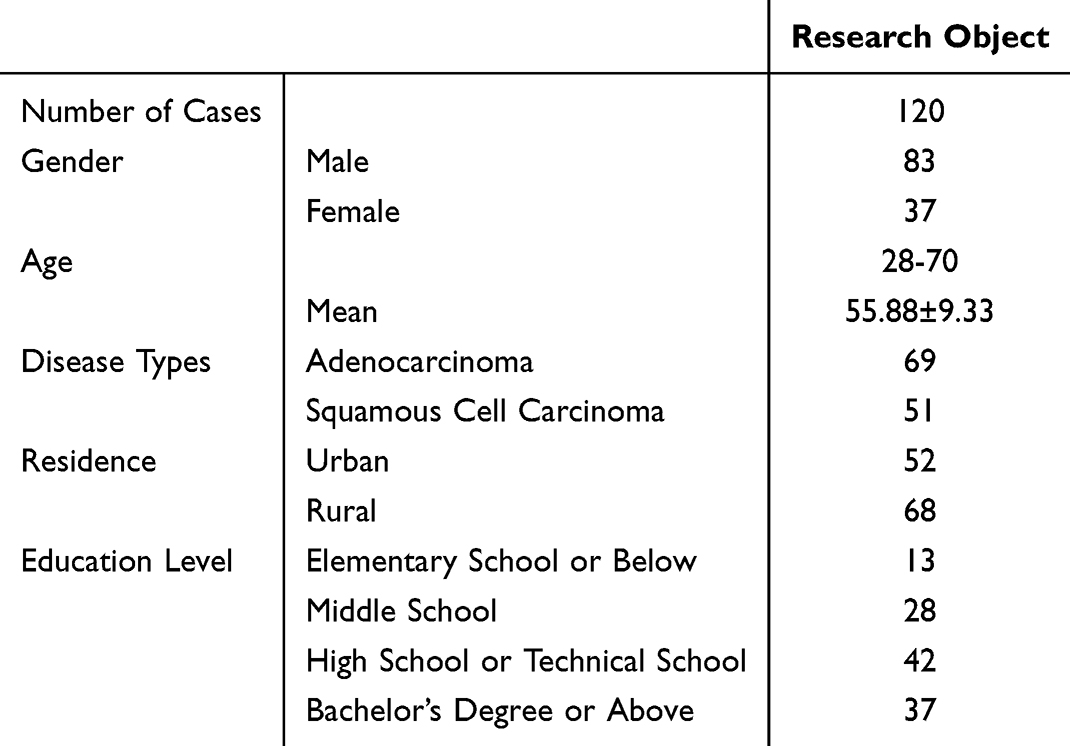 |
Table 1 General Data of All Included Patients |
To assess whether demographic variables affected the intervention effect, subgroup analysis was performed. Stratified t-tests showed that improvement in pain scores and self-efficacy after intervention was consistent across gender, age group (≤60 vs >60), and education level (≤high school vs ≥undergraduate), with no significant interaction effects observed (P>0.05). This suggests that the intervention was broadly effective regardless of patient background (See Table 2).
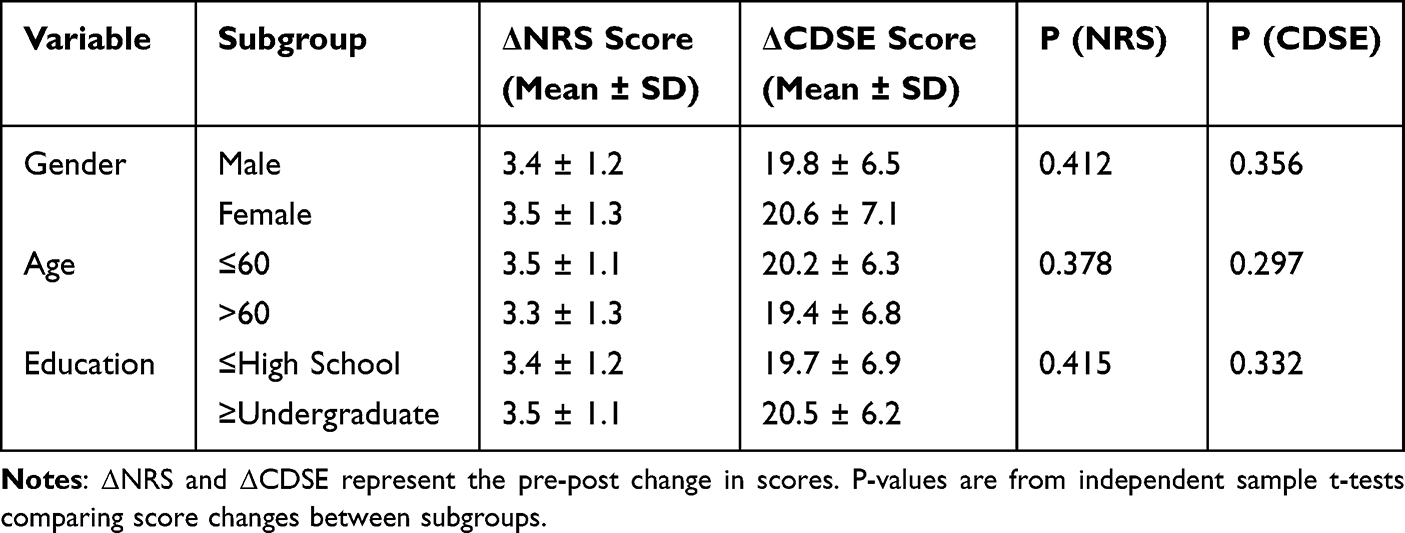 |
Table 2 Subgroup Analysis of Pain and Self-Efficacy Score Improvements by Demographic Variables |
Cancer Pain
After comprehensive intervention, the patients’ pain was significantly relieved. The average NRS score before intervention was 7.2±1.5 points (moderate to severe pain), and after intervention it dropped to 3.8±1.2 points (mild pain), a decrease of 47.22% (t=15.6, P<0.001). Specifically, before intervention, 68 patients (56.67%) had a pain score of 7–10 points (severe pain), and after intervention, only 12 patients (10.00%) had moderate pain (4–6 points), and there were no cases of severe pain (Figure 1). Notably, patients receiving mindfulness-based interventions (n=98, 81.7%) showed greater NRS reduction (ΔNRS=−3.8±1.1) compared to non-participants (ΔNRS=−2.9±0.9, P=0.013), suggesting its specific contribution to pain modulation.
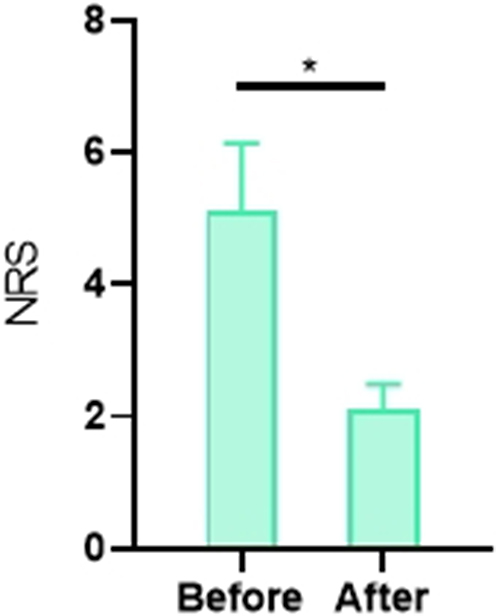 |
Figure 1 Comparison of NRS Scores Before and After Intervention. Note: *indicates a significant difference between the two groups, P<0.05. |
Self-Efficacy
The total score of patient self-efficacy (CDSES) increased from 52.3±8.7 points before intervention to 72.4±9.5 points (t=12.4, P<0.001). Each dimension improved significantly: Self-management: increased from 12.1±2.3 points to 18.5±2.6 points (t=14.2, P<0.001); General self-efficacy: increased from 14.8±3.1 points to 21.7±3.4 points (t=11.9, P<0.001); Goal achievement: increased from 13.5±2.8 points to 19.2±2.9 points (t=10.8, P<0.001); Problem solving: increased from 12.9±2.5 points to 17.0±2.7 points (t=9.6, P<0.001). After the intervention, 89 patients (74.17%) had a CDSES total score ≥ 65 (high self-efficacy), compared with only 22 patients (18.33%) before the intervention (Figure 2).
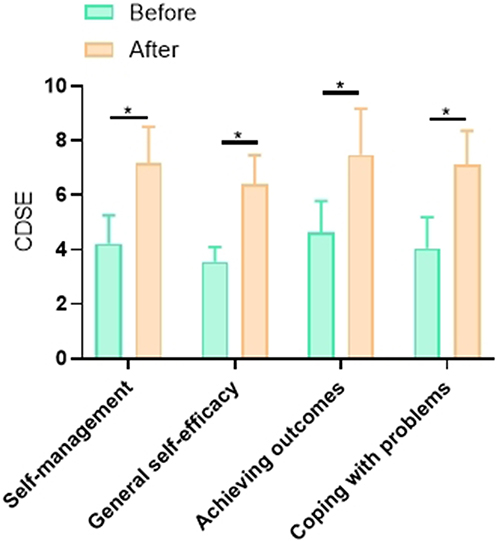 |
Figure 2 Comparison of CDSE Scores Before and After Intervention. Note: *indicates a significant difference between the two groups, P<0.05. |
Patient-reported feedback indicated high intervention acceptability: 92% reported “improved coping skills” and 87% rated mindfulness techniques as “highly useful” for pain crises. Formal satisfaction surveys revealed 94% approval for the multimodal approach.
Relationship Analysis
Multiple linear regression analysis showed that pain level (NRS) was the main independent predictor of self-efficacy (B=0.365, SE=0.174, OR=1.403, 95% CI=1.125–1.885, P=0.002). For every 1 point decrease in pain, the probability of improving self-efficacy increased by 40.3%. In addition, age (P=0.153) and education level (P=0.082) had no significant effect on self-efficacy (Table 3).
 |
Table 3 Logistic Regression Analysis of Pain and Self-Efficacy in Lung Cancer Patients with Cancer Pain |
Discussion
According to statistics from the World Health Organization (WHO), about 40% to 50% of advanced cancer patients experience moderate to severe pain, which not only causes great physical discomfort to patients, but also has a serious impact on their psychological emotions and quality of life. Cancer pain, as a complex bio-psychological-social phenomenon, has been considered one of the key factors affecting the treatment effect and long-term prognosis of tumor patients. Effective pain management can not only relieve patients’ pain, but also improve their treatment compliance, thereby consolidating and optimizing the efficacy of chemotherapy and other anti-cancer treatments.
In recent years, modern medical research has further revealed the multidimensional nature of cancer pain, that is, it is not only a physiological phenomenon, but also involves psychological and social factors of patients. The occurrence and perception of pain are affected by many factors, including physiological and pathological mechanisms, psychological state, social support level, and patients’ cognitive and emotional regulation abilities. Our intervention specifically incorporated mindfulness training, which contributed significantly to the observed 47.22% reduction in NRS scores (from 7.2±1.5 to 3.8±1.2). Mindfulness likely mediates pain through dual pathways: 1) Neuroendocrine regulation by enhancing β-endorphin release during meditative states, activating natural analgesic systems;11 2) Cognitive restructuring through improved attentional control that reduces pain catastrophizing and alters neural processing of nociceptive signals in anterior cingulate and prefrontal cortices.12 Cancer pain can trigger or aggravate negative emotions such as anxiety and depression, which in turn increase patients’ sensitivity to pain, forming a vicious cycle of “pain-anxiety-pain enhancement”. Studies have shown that cancer patients who are in a state of anxiety and depression for a long time often have a low tolerance for pain and are more likely to have catastrophic thinking, which leads to further aggravation of the pain experience. In addition, the psychological expectations and cognitive patterns of cancer patients also have an important impact on pain perception. For example, if patients have extremely negative cognition about pain and believe that increased pain means worsening of the disease or treatment failure, they may amplify the pain through psychological suggestion, further reducing their quality of life.13,14 In cancer pain management, self-efficacy is considered to be an important psychological variable that regulates pain perception and psychological adaptability. The observed improvement in self-efficacy (CDSE increase from 52.3±8.7 to 72.4±9.5) likely enhanced adaptive coping through multiple mechanisms: 1) Neurocognitive modulation where increased perceived control downregulates amygdala hyperactivity and attenuates stress-induced cortisol release;15 2) Behavioral activation through increased adherence to non-pharmacological techniques (eg, 87% reported utilizing mindfulness during pain crises); 3) Attentional redeployment whereby self-efficacy strengthens top-down regulation of pain perception through prefrontal cortex engagement.11 The self-efficacy theory was proposed by psychologist Bandura and refers to the degree of confidence that an individual has in completing a task or goal. For cancer patients, self-efficacy is not only related to their coping style with the disease, but also directly affects the effectiveness of pain management. Patients with high self-efficacy are usually more proactive in adopting effective pain relief strategies, such as taking medication as prescribed by a doctor, using relaxation training, and seeking social support, thereby reducing the negative impact of pain on life. On the contrary, patients with low self-efficacy may reduce active coping behaviors due to lack of confidence, or even passively avoid treatment, further worsening the pain experience. Therefore, improving the self-efficacy of cancer patients has important clinical significance for improving cancer pain management, alleviating patients’ negative emotions, and improving their quality of life.
This study, through comprehensive interventions on 120 lung cancer patients with cancer pain, explored the relationship between pain intensity and self-efficacy and analyzed effective improvement methods. Notably, mindfulness participants demonstrated significantly greater pain reduction than non-participants (ΔNRS=−3.8±1.1 vs −2.9±0.9, P=0.013), suggesting its specific mechanistic role beyond general intervention effects. The results showed that comprehensive intervention measures significantly reduced patients’ pain scores and improved their self-efficacy levels. Therefore, by enhancing pain management and appropriately intervening in cancer-related fatigue for lung cancer patients, it is possible to improve their self-efficacy, thereby strengthening their self-management abilities in coping with symptoms. Studies by foreign scholars have indicated that lung cancer patients with low self-efficacy are more likely to experience pain, fatigue, anxiety, and poor physical and mental functions, all of which can affect the patient’s rehabilitation process.
Pain management is a core component of nursing care for lung cancer patients. Pain not only affects patients’ physical health but also severely impacts their psychological state and quality of life. Through detailed pain assessment and management, pain can be effectively alleviated, thereby enhancing patients’ self-efficacy and quality of life.16,17 Patient feedback substantiated these outcomes: 92% reported improved coping skills and 94% expressed high satisfaction with the multimodal approach, indicating strong intervention acceptability. In this study, patients showed significantly reduced pain scores after comprehensive interventions. Medication is fundamental in relieving pain, psychological counseling helps patients regulate their emotions and reduce psychological stress, and self-management education enhances patients’ understanding and coping abilities regarding their condition. The results indicate that these comprehensive interventions work synergistically to effectively relieve pain, improve self-efficacy, and enhance quality of life.
The study found that most lung cancer patients generally have low self-efficacy, consistent with previous research findings. Self-efficacy reflects patients’ confidence and ability to cope with disease and treatment processes.18,19 The study revealed that self-efficacy levels in lung cancer patients with cancer pain significantly increased after receiving comprehensive interventions. This improvement is likely due to the interventions providing patients with more knowledge and skills, making them more confident and composed when facing pain and disease. Enhancing patients’ self-efficacy aids their active participation in treatment and rehabilitation, thus improving overall prognosis.20,21 Lung cancer patients are typically diagnosed at advanced stages of the disease, with multiple and severe symptoms, often leading to emotional distress. Additionally, economic burdens and lack of social support can undermine patients’ confidence in their treatment and prognosis. Therefore, it is crucial to focus on cultivating self-efficacy in lung cancer patients, helping them build confidence, actively cooperate with medical personnel, and maintain healthy behaviors to enhance coping skills. Providing family and social support is also essential. For patients with severe emotional disorders, professional psychological therapy can help improve their self-efficacy. The study also emphasizes the importance of social support in the patient’s recovery process. Guiding patients’ friends and family to participate in care management and establishing a strong social support network can help patients better cope with pain and disease. Social support not only provides emotional comfort but also offers significant practical assistance in care, boosting patients’ confidence and courage in fighting the disease.22,23
As a protocol validation study, we acknowledge limitations of the single-arm pre-post design. The absence of a concurrent control group prevents direct attribution of effects to the intervention alone. However, this foundational work establishes feasibility and mechanistic hypotheses for our ongoing randomized controlled trial comparing multimodal intervention against conventional care.
Furthermore, aside from the measures adopted in this study, other methods have also been reported to show good effects. For example, within the current Western medical treatment model, traditional Chinese medicine (TCM) can achieve early prevention and pain alleviation through syndrome differentiation and the combination of internal and external treatments. TCM has always emphasized prevention, but not all tumors are accompanied by pain when they occur. For instance, stomach cancer patients may not have stomach pain, or tumor patients may initially have no pain but develop pain after surgery, radiotherapy, or chemotherapy. This type of pain usually lasts longer and is more challenging to control. TCM has advantages in treating cancer pain, including fewer adverse reactions, lower costs, better tolerance, and higher patient acceptance. By tailoring treatment plans to the individual, TCM can prevent diseases before they occur and promptly curb their adverse progression, thereby achieving optimal treatment outcomes. Other methods, such as peripheral nerve stimulation, have also shown good results in treating other cancers clinically.24,25
Although this study has made some progress in exploring the relationship between cancer pain and self-efficacy in lung cancer, there are still some limitations. First, the sample source of this study is limited to patients in a single hospital, and the sample size is relatively small, which may affect the external validity of the research results and limit its application to a wider population. Future studies should expand the sample range and include multi-center data to improve the universality and representativeness of the research results. Second, the follow-up time of this study was short, focusing mainly on the effect of short-term intervention, and failed to fully evaluate the sustained impact of long-term intervention on patients’ pain management, self-efficacy and quality of life. The relief and psychological adaptation of cancer pain is usually a long-term process. Future studies should extend the follow-up period and dynamically track the changes in patients’ pain, the improvement of self-efficacy and long-term treatment compliance, so as to more comprehensively evaluate the long-term effectiveness of the intervention strategy. Additionally, while we collected patient satisfaction metrics (reported in Results), formal qualitative exploration of intervention perceptions was not conducted. Future studies will incorporate semi-structured interviews to capture nuanced patient experiences. In addition, this study mainly relies on questionnaires and subjective assessment tools to measure pain perception and self-efficacy, which may have certain subjective biases. Future studies can combine physiological indicators (such as cortisol levels, heart rate variability, etc.) or objective behavioral measurement methods to provide more objective and comprehensive evaluation results. In addition, the role of individual psychological characteristics, social support systems and other factors in cancer pain management can also be explored to optimize intervention strategies and provide more scientific guidance for clinical practice.
In conclusion, the pain intensity of lung cancer patients with cancer pain is closely related to self-efficacy. Comprehensive interventions have significant effects in alleviating cancer pain in lung cancer patients, improving their self-efficacy, and enhancing their quality of life. Strengthening pain management, enhancing patients’ self-efficacy, and providing good social support can help patients better cope with the disease and improve overall prognosis. Future studies should continue to explore more effective comprehensive intervention strategies to further improve the quality of life for lung cancer patients with cancer pain.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethical Approval Statement
This study was approved by the Ethics Committee of The First People’s Hospital of Zunyi (Approval No. ZY2020-015). Informed consent was obtained from all study participants. All the methods were carried out in accordance with the Declaration of Helsinki.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Bade BC, Cruz CSD. Lung cancer 2020: epidemiology, etiology, and prevention. Clin Chest Med. 2020;41(1):1–24. doi:10.1016/j.ccm.2019.10.001
2. Nasim F, Sabath BF, Eapen GA. Lung cancer. Med Clin North Am. 2019;103(3):463–473. doi:10.1016/j.mcna.2018.12.006
3. Lee E, Kazerooni EA. Lung cancer screening. Semin Respir Crit Care Med. 2022;43(6):839–850. doi:10.1055/s-0042-1757885
4. Mao Y, Yang D, He J, et al. Epidemiology of lung cancer. Surg Oncol Clin N Am. 2016;25(3):439–445. doi:10.1016/j.soc.2016.02.001
5. Magee D, Bachtold S, Brown M, et al. Cancer pain: where are we now? Pain Manag. 2019;9(1):63–79. doi:10.2217/pmt-2018-0031
6. Swarm RA, Paice JA, Anghelescu DL, et al. Adult cancer pain, version 3.2019, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2019;17(8):977–1007. doi:10.6004/jnccn.2019.0038
7. Collins LG, Haines C, Perkel R, et al. Lung cancer: diagnosis and management. Am Fam Physician. 2007;75(1):56–63.
8. Rodriguez-Canales J, Parra-Cuentas E, Wistuba II. Diagnosis and molecular classification of lung cancer. Cancer Treat Res. 2016;170:25–46.
9. Jensen MP. The validity and reliability of pain measures for use in clinical trials in adults: review paper written for the initiative on methods, measurement, and pain assessment in clinical trials (IMMPACT) meeting, April 12–13 2003. 2017.
10. Ownby RL, Simonson M, Caballero J, et al. A mobile app for chronic disease self-management for individuals with low health literacy: a multisite randomized controlled clinical trial. J Ageing Longevity. 2024;4(2):51–71. doi:10.3390/jal4020005
11. Psarianos AE, Philippou A, Papadopetraki A, et al. Cortisol and β-endorphin responses during a two-month exercise training program in patients with an opioid use disorder and on a substitution treatment. Int J Mol Sci. 2025;26(11):5178. doi:10.3390/ijms26115178
12. Shi Y, Wu W. Multimodal non-invasive non-pharmacological therapies for chronic pain: mechanisms and progress. BMC Med. 2023;21(1):372. doi:10.1186/s12916-023-03076-2
13. Fink RM, Gallagher E. Cancer pain assessment and measurement. Semin Oncol Nurs. 2019;35(3):229–234. doi:10.1016/j.soncn.2019.04.003
14. Yoon SY, Oh J. Neuropathic cancer pain: prevalence, pathophysiology, and management. Korean J Intern Med. 2018;33(6):1058–1069. doi:10.3904/kjim.2018.162
15. Zahir FR. Epigenomic impacts of meditative practices. Epigenomics. 2022;14(24):1593–1608. doi:10.2217/epi-2022-0306
16. Maindet C, Burnod A, Minello C, et al. Strategies of complementary and integrative therapies in cancer-related pain-attaining exhaustive cancer pain management. Support Care Cancer. 2019;27(8):3119–3132. doi:10.1007/s00520-019-04829-7
17. Cope DG. Cancer pain management considerations in older adults. Semin Oncol Nurs. 2019;35(3):274–278. doi:10.1016/j.soncn.2019.04.008
18. Langford AT, Ellis KR, Orellana K, et al. Self-efficacy to get cancer-related information or advice. J Cancer Educ. 2023;38(4):1330–1337. doi:10.1007/s13187-023-02266-z
19. Anderson A, Starkweather A, Cong X, et al. Self-efficacy survey study of pain self-management in patients with cancer. Pain Manag Nurs. 2022;23(4):486–493. doi:10.1016/j.pmn.2021.10.002
20. Merluzzi TV, Pustejovsky JE, Philip EJ, et al. Interventions to enhance self-efficacy in cancer patients: a meta-analysis of randomized controlled trials. Psychooncology. 2019;28(9):1781–1790. doi:10.1002/pon.5148
21. Jackson C, Jackson C. Increasing provider self-efficacy to manage chronic cancer pain. Pain Manag Nurs. 2023;24(6):581–586. doi:10.1016/j.pmn.2023.08.002
22. Crombez P, Bron D, Michiels S. Multicultural approaches of cancer pain. Curr Opin Oncol. 2019;31(4):268–274. doi:10.1097/CCO.0000000000000547
23. Paice JA. Pain in cancer survivors: how to manage. Curr Treat Options Oncol. 2019;20(6):48. doi:10.1007/s11864-019-0647-0
24. Deng G. Integrative medicine therapies for pain management in cancer patients. Cancer J. 2019;25(5):343–348. doi:10.1097/PPO.0000000000000399
25. Zhang H. Cancer pain management-new therapies. Curr Oncol Rep. 2022;24(2):223–226. doi:10.1007/s11912-021-01166-z
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.