Back to Journals » Journal of Pain Research » Volume 19
Multimodal Perioperative Management of Elderly Hip Fracture Patients: Integrating Western and Traditional Chinese Medicine Approaches for Sleep, Pain, and PONV Control: A Narrative Review
Authors Hu R, Ding Y, Zhang J, Li C, Huang W, He J, Yue J
Received 28 January 2026
Accepted for publication 10 May 2026
Published 10 June 2026 Volume 2026:19 599583
DOI https://doi.org/10.2147/JPR.S599583
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Jinlei Li
Rui Hu,1,* Yueli Ding,1,* Jiali Zhang,1 Chi Li,1 Wujian Huang,1 Jianbo He,2 Junlin Yue1
1Department of Anesthesiology, Kunming Municipal Hospital of Traditional Chinese Medicine (The Third Affiliated Hospital of Yunnan University of Chinese Medicine), Kunming, Yunnan, People’s Republic of China; 2Yunnan University of Chinese Medicine, Kunming, Yunnan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Junlin Yue, Email [email protected]
Abstract: Hip fractures represent a significant global health burden in the elderly population, with perioperative complications substantially affecting morbidity and mortality. The triumvirate of postoperative pain, sleep disturbance, and postoperative nausea and vomiting (PONV) constitutes interconnected challenges that profoundly influence recovery trajectories in this vulnerable demographic. While Western medicine has established evidence-based protocols through Enhanced Recovery After Surgery (ERAS) frameworks and multimodal analgesia, Traditional Chinese Medicine (TCM) offers complementary therapeutic modalities with emerging evidence supporting their integration into perioperative care pathways. This narrative review synthesizes current evidence on Western and TCM approaches for managing sleep, pain, and PONV in elderly hip fracture patients, exploring mechanistic synergies and proposing an integrative framework for clinical implementation. We examine the neurobiological crosstalk between these three domains, evaluate contemporary Western interventions including peripheral nerve blocks and pharmacological prophylaxis, and critically appraise TCM modalities such as electroacupuncture, transcutaneous electrical acupoint stimulation (TEAS), and auricular therapy. The convergence of these therapeutic traditions offers promising avenues for optimizing perioperative outcomes while minimizing polypharmacy risks inherent to geriatric care. The proposed integrative protocol combines preoperative TCM conditioning, intraoperative peripheral nerve block with concurrent acupoint stimulation, and postoperative multimodal analgesia alongside acupuncture-based therapies, representing a phased clinical framework that targets multiple nodes of the pain-sleep-PONV neurobiological axis through complementary Western and TCM mechanisms. Future research directions emphasizing rigorous methodology and mechanistic investigations are proposed to advance this integrative paradigm.
Keywords: hip fractures, aged, perioperative care, traditional Chinese medicine, acupuncture therapy, postoperative nausea and vomiting, sleep wake disorders, pain management
Introduction
The global demographic transition toward an aging population has precipitated an unprecedented increase in hip fracture incidence, with projections estimating 6.3 million annual cases worldwide by 2050.1,2 Elderly patients sustaining hip fractures represent a uniquely vulnerable cohort characterized by multimorbidity, frailty, and diminished physiological reserve, rendering them exquisitely susceptible to perioperative complications. One-year mortality rates approach 30% in this population, with survivors frequently experiencing protracted functional decline and diminished quality of life.3,4 The economic burden is equally substantial, with hip fracture-related healthcare expenditures exceeding $12 billion annually in the United States alone, underscoring the imperative for optimized perioperative management strategies.5
The perioperative period presents a critical window wherein therapeutic interventions can substantially modify clinical trajectories. Three interrelated domains—postoperative pain, sleep disturbance, and postoperative nausea and vomiting (PONV)—emerge as particularly consequential determinants of recovery. These phenomena do not exist in isolation but rather engage in bidirectional neurobiological crosstalk, creating a self-perpetuating cycle that amplifies each component.6,7 Inadequately managed pain disrupts sleep architecture, while sleep deprivation augments pain perception through descending modulatory pathway dysfunction. Both pain and sleep disturbance activate central stress responses that exacerbate PONV, while antiemetic-induced sedation further compounds sleep disruption.8
Western medicine has responded to these challenges through the development of Enhanced Recovery After Surgery (ERAS) protocols and multimodal analgesia strategies that emphasize opioid-sparing approaches and regional anesthesia techniques.9,10 Despite these advances, substantial proportions of elderly hip fracture patients continue to experience suboptimal outcomes, partly attributable to the limitations of pharmacological interventions in a population susceptible to polypharmacy and drug-related adverse events. The vulnerability of elderly patients to opioid-induced cognitive dysfunction, respiratory depression, and delirium necessitates exploration of complementary therapeutic modalities.11,12
Traditional Chinese Medicine (TCM) offers a philosophical and therapeutic framework that has addressed perioperative symptoms for millennia. Contemporary research has begun to elucidate the mechanisms underlying TCM modalities, revealing effects on neuroinflammation, autonomic regulation, and endogenous opioid systems that complement Western therapeutic targets.13,14 The integration of these traditions holds promise for enhancing therapeutic efficacy while mitigating the risks associated with purely pharmacological approaches. Acupuncture and related techniques have demonstrated efficacy in reducing postoperative pain, preventing PONV, and improving sleep quality across diverse surgical populations.15,16
This review aims to synthesize current evidence on Western and TCM approaches for perioperative management of sleep, pain, and PONV in elderly hip fracture patients, proposing an integrative framework that leverages the complementary strengths of both therapeutic traditions. We examine the pathophysiological interconnections among these three domains, evaluate the contemporary evidence base for both Western and TCM interventions, and propose practical implementation strategies for clinical practice.
Literature Search Strategy
A narrative review methodology was employed to synthesize evidence on perioperative management of elderly hip fracture patients using Western and Traditional Chinese Medicine approaches. Systematic literature searches were conducted in PubMed/MEDLINE, EMBASE, the Cochrane Library, and Web of Science, covering publications from January 2000 to December 2024. The following Medical Subject Headings (MeSH) terms and free-text keywords were used in combination: “hip fracture”, “hip fractures”, “femoral fracture”, “elderly”, “geriatric”, “aged”, “perioperative”, “perioperative care”, “Traditional Chinese Medicine”, “acupuncture”, “electroacupuncture”, “transcutaneous electrical acupoint stimulation”, “TEAS”, “auricular acupuncture”, “PONV”, “postoperative nausea and vomiting”, “sleep disturbance”, “sleep disorders”, “postoperative cognitive dysfunction”, “delirium”, “multimodal analgesia”, “regional anesthesia”, “peripheral nerve block”, “ERAS”, and “integrative medicine”. Study inclusion criteria were: (1) original research articles, systematic reviews, meta-analyses, or consensus guidelines; (2) publications in English; (3) studies involving adult surgical patients or specifically addressing elderly hip fracture populations; and (4) studies evaluating interventions targeting perioperative pain, sleep, PONV, cognitive outcomes, or functionally related perioperative endpoints. Studies were excluded if they focused exclusively on non-surgical conditions, pediatric populations, or interventions with no perioperative relevance. The selection of representative studies for tabular summaries was guided by methodological rigor (preference for RCTs, systematic reviews, and meta-analyses), sample size, recency of publication, and direct relevance to the proposed integrative protocol and target patient population.
The Triad of Perioperative Challenges: Pathophysiological Interconnections
Pain-Sleep-PONV Axis: Neurobiological Crosstalk
The conceptualization of postoperative pain, sleep disturbance, and PONV as discrete entities requiring independent management represents an oversimplification that fails to capture their intricate neurobiological interdependence. These phenomena share common neural substrates and engage in reciprocal modulation that amplifies each component when left unaddressed.17 Understanding these interconnections is essential for designing effective multimodal interventions that address the root causes rather than merely treating symptoms in isolation.
Postoperative pain activates ascending nociceptive pathways that converge upon brainstem nuclei integral to both sleep regulation and emetic reflexes. The periaqueductal gray matter, which orchestrates descending pain modulation, receives dense projections from hypothalamic sleep-wake regulatory centers.18 Surgical tissue injury initiates inflammatory cascades that elevate circulating cytokines—interleukin-1β (IL-1β), interleukin-6 (IL-6), and tumor necrosis factor-α (TNF-α)—which cross the blood-brain barrier to directly modulate both pain processing and sleep architecture.19,20 This neuroinflammatory milieu simultaneously sensitizes chemoreceptor trigger zone neurons, lowering the threshold for emetic responses. The area postrema, lacking a complete blood-brain barrier, is particularly susceptible to circulating inflammatory mediators and emetogenic substances.21
Sleep disturbance in surgical patients extends beyond simple insomnia to encompass profound alterations in sleep architecture. Studies utilizing polysomnography have documented near-complete suppression of rapid eye movement (REM) sleep and substantial reductions in slow-wave sleep during the early postoperative period.22 These architectural changes carry functional consequences: slow-wave sleep deprivation impairs growth hormone secretion critical for tissue healing, while REM suppression disrupts memory consolidation and emotional processing. The systemic inflammatory response to surgery, mediated partly through disrupted sleep, creates a feed-forward loop wherein inflammation begets sleep disturbance, and sleep disturbance amplifies inflammation.23
A comprehensive systematic review examining perioperative sleep disturbances reported a pooled preoperative prevalence of 60% among surgical patients, with postoperative rates substantially higher.24 Key risk factors identified include high preoperative Pittsburgh Sleep Quality Index (PSQI) scores, anxiety, and advanced age. Critically, patients experiencing postoperative delirium—a devastating complication in elderly hip fracture patients with incidence rates of 35–65%—demonstrate significantly elevated prevalence of perioperative sleep disturbances, suggesting sleep optimization as a potentially modifiable delirium risk factor.25,26
Elderly Hip Fracture Patients: Unique Vulnerabilities
Geriatric hip fracture patients present heightened susceptibility to the pain-sleep-PONV triad through multiple converging mechanisms. Age-related neurodegeneration affects the very systems responsible for pain modulation, sleep regulation, and autonomic control. Reductions in endogenous opioid receptor density diminish the efficacy of descending inhibitory pathways, while cholinergic deficits impair both sleep maintenance and cognitive resilience against delirium.27 The aged brain demonstrates reduced neuroplasticity and diminished capacity to compensate for perioperative insults, rendering elderly patients particularly vulnerable to lasting cognitive sequelae.28
Frailty, present in up to 50% of hip fracture patients, emerges as a powerful predictor of adverse perioperative outcomes. A comprehensive meta-analysis incorporating 21 studies and 49,196 patients demonstrated that frail individuals experienced significantly elevated risks of inpatient mortality (relative risk [RR], 1.93; 95% confidence interval [CI], 1.57–2.37), 30-day mortality (RR, 2.13; 95% CI, 1.68–2.71), one-year mortality (RR, 2.44; 95% CI, 2.08–2.86), and complications including delirium (RR, 3.34; 95% CI, 2.12–5.25), pneumonia (RR, 2.31), cardiac complications (RR, 1.95), and urinary tract infection (RR, 3.25).29 This frailty-associated vulnerability reflects diminished physiological reserve across multiple organ systems, rendering standard therapeutic interventions both more necessary and more perilous.
Polypharmacy compounds these challenges, as elderly patients frequently present with medication regimens that interact with perioperative prescriptions. Anticholinergic burden from baseline medications increases delirium susceptibility, while beta-blocker and calcium channel antagonist use may complicate hemodynamic management.30 The imperative to minimize additional pharmacological interventions while maintaining therapeutic efficacy creates a clinical conundrum that motivates exploration of non-pharmacological modalities. Studies have demonstrated that each additional medication in elderly patients increases adverse event risk by approximately 10%, highlighting the importance of opioid-sparing and drug-minimizing strategies.31
The relationship between preoperative sleep disturbance and postoperative delirium has been increasingly recognized. A retrospective cohort study of 489 elderly surgical patients demonstrated that preoperative sleep disturbance significantly increased postoperative delirium incidence (17.0% vs 6.2%, P=0.023), with multivariate regression identifying preoperative sleep disturbance as an independent risk factor (odds ratio [OR], 3.03; 95% CI, 1.09–9.52).25 Similarly, a large prospective cohort study of 3075 elderly patients found that 25.72% experienced operative night sleep disturbances, with significantly higher postoperative delirium risk (adjusted OR, 1.43; 95% CI, 1.11–1.82; P=0.005).26
Understanding the neurobiological crosstalk between postoperative pain, sleep disturbance, and PONV—and appreciating the unique vulnerabilities of elderly hip fracture patients to this interconnected triad—directly informs the therapeutic targets prioritized by contemporary perioperative medicine. Western medicine has systematically developed interventional strategies targeting specific nodes of this axis, while TCM offers complementary approaches acting through distinct but overlapping mechanisms. The following sections evaluate the evidence base for current Western and TCM perioperative interventions in turn, before examining the rationale and framework for their integration.
Western Approaches to Perioperative Management
Regional Anesthesia and Peripheral Nerve Blocks
The evolution of regional anesthesia techniques has fundamentally transformed perioperative pain management in hip fracture surgery. Peripheral nerve blocks targeting the femoral nerve, fascia iliaca compartment, and more recently the pericapsular nerve group (PENG) provide profound analgesia while minimizing systemic opioid exposure. These techniques have become cornerstones of ERAS protocols for hip fracture management.9,32
The landmark Cochrane review by Guay and Kopp, encompassing 49 randomized controlled trials (RCTs) and 3061 patients, established high-certainty evidence that peripheral nerve blocks reduce pain on movement by an amount equivalent to 2.5 points on a 10-point scale (mean difference [MD], −2.5; 95% CI, −2.9 to −2.1).32 More consequentially for elderly patients, nerve blocks significantly reduced acute confusional state risk (RR, 0.67; 95% CI, 0.50–0.88; number needed to treat [NNT], 12) and probably reduced chest infection incidence (RR, 0.41; 95% CI, 0.19–0.89). Time to first mobilization decreased by approximately 11 hours (MD, −11.4 hours; 95% CI, −14.5 to −8.2), a clinically meaningful acceleration of functional recovery that may reduce overall complication rates.
Fascia iliaca compartment block (FICB) has gained widespread clinical adoption for hip fracture management given its technical simplicity and suitability for emergency department administration. A meta-analysis with trial sequential analysis of 11 trials comprising 895 patients demonstrated significant pain relief at rest at 2–4 hours (MD, 1.59; 95% CI, 1.12–2.06), reduced parenteral opioid consumption, decreased nausea and vomiting, and shortened hospital stay.33 The ability to perform FICB with minimal specialized training using landmark or ultrasound guidance expands its applicability across healthcare settings, including resource-limited environments.
The PENG block represents a more recent addition to the regional anesthesia armamentarium, specifically targeting the articular branches of the femoral, obturator, and accessory obturator nerves supplying the anterior hip capsule while preserving motor function.33 A randomized controlled trial published in the British Journal of Anaesthesia demonstrated that PENG block combined with spinal anesthesia significantly improved quality of recovery scores (QoR-15) and reduced 24-hour opioid requirements compared to spinal anesthesia alone. The motor-sparing properties facilitate early mobilization—a cornerstone of ERAS protocols—without compromising patient safety or increasing fall risk.
Multimodal Analgesia Strategies
The PROSPECT (Procedure-Specific Postoperative Pain Management) working group recently published comprehensive recommendations for hip fracture surgery following systematic review of 60 studies.34 The guidelines recommend paracetamol (acetaminophen) and non-steroidal anti-inflammatory drugs (NSAIDs) or cyclooxygenase-2 (COX-2) selective inhibitors as foundational multimodal analgesia components, with single-shot femoral nerve block or FICB for patients without contraindications. Continuous catheter techniques receive recommendation only in specific circumstances such as anticipated prolonged severe pain or multiple procedures, while opioids are reserved as rescue analgesia to minimize cognitive and respiratory adverse effects.
Implementation studies have validated these multimodal approaches in clinical practice. A geriatric pain protocol combining early regional nerve blocks with non-opioid medications significantly reduced morphine milligram equivalents on postoperative days 1 and 2 (P=0.007 and P=0.043, respectively) while maintaining equivalent pain control and facilitating earlier mobilization.35 Such opioid-sparing strategies carry particular relevance for elderly patients susceptible to opioid-induced delirium, respiratory depression, constipation, and falls. The synergistic effects of combining regional anesthesia with systemic multimodal analgesia permit substantial reductions in opioid requirements without compromising pain control.
ERAS implementation for hip fracture management has demonstrated substantial benefits across multiple outcome domains. A systematic review and meta-analysis of 7 cohort studies encompassing 9869 patients demonstrated that ERAS protocols significantly decreased time to surgery, length of hospital stay, and overall complication rates including delirium, without increasing readmission rates or mortality.9 Core ERAS elements include preoperative nutritional optimization, minimization of fasting duration, multimodal analgesia with regional techniques, goal-directed fluid management, and early mobilization protocols initiated within 24 hours of surgery.
PONV Prophylaxis: Current Consensus
The Fourth Consensus Guidelines for the Management of Postoperative Nausea and Vomiting, endorsed by 23 professional societies, codified contemporary approaches to PONV prevention and represent the current standard of care.36 Key updates from previous iterations included lowered thresholds for antiemetic prophylaxis and recommendations for multimodal prophylaxis in patients with one or more risk factors. The guidelines emphasize that PONV prophylaxis is inexpensive, safe, and highly effective, supporting a liberal approach to antiemetic administration. Critically for elderly patients, the guidelines explicitly cautioned against scopolamine use given increased susceptibility to cognitive adverse effects including confusion, agitation, and hallucinations in this demographic.
The therapeutic paradigm has shifted toward general multimodal PONV prophylaxis rather than risk-stratified approaches, reflecting recognition that the benefits of prophylaxis outweigh risks across most patient populations.37 Ondansetron (4 mg intravenously) combined with dexamethasone (4–8 mg intravenously) represents a common first-line combination with complementary mechanisms of action—5-HT3 receptor antagonism and glucocorticoid anti-inflammatory effects, respectively. Neurokinin-1 (NK-1) receptor antagonists (aprepitant, fosaprepitant) are reserved for high-risk patients given their superior efficacy against delayed PONV. A meta-analysis of 17 RCTs examining aprepitant demonstrated significant PONV incidence reduction (OR, 0.34; 95% CI, 0.26–0.44; P<0.001) and improved complete response rates.38
Importantly, opioid-sparing analgesic strategies emerge as foundational PONV prevention, given the strong dose-dependent association between perioperative opioid consumption and emetic complications. Regional anesthesia techniques thus serve dual purposes in reducing both pain and PONV, with studies demonstrating that each 10 mg morphine equivalent reduction decreases PONV risk by approximately 15%.39 Total intravenous anesthesia (TIVA) with propofol, when appropriate, offers additional PONV risk reduction compared to volatile anesthetic-based techniques.
Sleep Optimization Interventions
Pharmacological sleep interventions in elderly surgical patients require careful selection given heightened susceptibility to sedative adverse effects including next-day cognitive impairment, falls, and paradoxical agitation. Melatonin has emerged as a particularly attractive option given its favorable safety profile and physiological role in circadian rhythm regulation.40 Unlike benzodiazepines and Z-drugs, melatonin does not produce tolerance, dependence, or significant morning sedation, making it well-suited for perioperative use in elderly populations.
A meta-analysis of 16 randomized controlled trials encompassing 1981 patients evaluated perioperative melatonin for postoperative delirium prevention, demonstrating significantly lower delirium incidence in treatment groups (RR, 0.57; 95% CI, 0.41–0.79).22 High-dose melatonin (≥5 mg) showed particular efficacy (RR, 0.41; 95% CI, 0.25–0.68), with benefits most pronounced during the early postoperative period (days 1–3, RR, 0.35). The proposed mechanisms include circadian rhythm stabilization, antioxidant effects, and anti-inflammatory properties that may attenuate neuroinflammation underlying delirium pathophysiology.
Dexmedetomidine, an α2-adrenergic agonist with sedative, analgesic, and sympatholytic properties, offers perioperative sleep benefits through mechanisms distinct from traditional sedative-hypnotics.41 A meta-analysis of 5 polysomnographic studies involving 381 patients demonstrated that dexmedetomidine significantly improved postoperative sleep quality by increasing sleep efficiency (MD, 8.2%; 95% CI, 4.1–12.3), reducing arousal index (MD, −5.3/hour; 95% CI, −7.8 to −2.8), decreasing N1 (light) sleep duration, and increasing N2 sleep proportion. Unlike benzodiazepines and opioids, dexmedetomidine preserves physiological sleep architecture without REM suppression.23
Non-pharmacological sleep hygiene interventions—noise reduction, light management, clustering of nursing activities to minimize nocturnal interruptions, and maintenance of day-night orientation—constitute essential but often neglected components of perioperative sleep optimization. The hospital environment itself poses substantial barriers to sleep quality, with noise levels frequently exceeding World Health Organization recommendations of 35 dB during nighttime hours. Studies of hip fracture patients have documented significant sleep quality deterioration persisting three months post-surgery, with PSQI scores increasing from 5.2±2.8 preoperatively to 8.2±4.2 postoperatively (P=0.007) and the proportion of patients meeting diagnostic criteria for sleep disorders increasing from 40% to 60%.42
Traditional Chinese Medicine Approaches
Theoretical Framework: TCM Perspectives on Perioperative Symptoms
Traditional Chinese Medicine conceptualizes health as a dynamic equilibrium of Qi (vital energy), blood, and the interplay of Yin and Yang. Surgical intervention disrupts this equilibrium through tissue trauma, blood loss, and emotional stress, creating patterns of Qi stagnation and blood stasis that manifest as pain, while depletion of Qi and Yin leads to sleep disturbance and internal disharmony manifesting as nausea and vomiting.13 The concept of “surgical shock” in TCM encompasses both the physical trauma and the psychological stress of surgery, both of which contribute to postoperative symptom burden.
This theoretical framework, while employing terminology distinct from Western biomedical discourse, describes phenomena with demonstrable physiological correlates that have been increasingly validated through modern research methodologies. “Qi stagnation” corresponds to inflammatory processes, sympathetic hyperactivity, and microcirculatory dysfunction; “blood stasis” aligns with microcirculatory dysfunction, platelet activation, and coagulation cascade activation.14 TCM therapeutic interventions targeting these patterns engage mechanisms increasingly elucidated through neuroimaging, biochemical analyses, and clinical outcome studies. The meridian system, while not corresponding to anatomically distinct structures, maps onto neuroanatomical pathways and autonomic nerve distributions that explain the remote effects of acupoint stimulation.
Electroacupuncture and Manual Acupuncture
Electroacupuncture (EA) combines traditional acupoint needling with electrical stimulation, enabling standardized treatment parameters and enhanced reproducibility compared to manual acupuncture. The mechanisms underlying EA analgesia involve multiple levels of the neuraxis: peripheral nerve fiber activation (both Aδ and C fibers), spinal cord dorsal horn modulation through segmental inhibition and endogenous opioid release (enkephalins, endorphins, dynorphins), and supraspinal effects on the periaqueductal gray, rostral ventromedial medulla, and descending inhibitory pathways.15 Different stimulation frequencies activate distinct endogenous opioid systems: low-frequency (2–4 Hz) stimulation primarily releases enkephalins and β-endorphins, while high-frequency (100 Hz) stimulation predominantly releases dynorphins.
A network meta-analysis encompassing 41 randomized controlled trials and 3003 patients compared four acupuncture modalities—manual acupuncture (MA), electroacupuncture (EA), transcutaneous electrical acupoint stimulation (TEAS), and auricular therapy (AT)—combined with multimodal analgesia for postoperative pain management following total knee arthroplasty.16 All acupuncture combinations significantly reduced PONV incidence compared to multimodal analgesia alone (OR range, 0.20–0.44; all P<0.05). The surface under the cumulative ranking curve (SUCRA) analysis ranked EA + MA as most effective for PONV prevention, followed by TEAS + MA. The safety profile proved excellent across all modalities, with fewer adverse events reported than multimodal analgesia alone.
Of particular relevance to elderly hip fracture patients, a recent randomized controlled trial evaluated electroacupuncture intervention before and after surgery for perioperative neurocognitive disorders (PND) in 60 patients aged 65 years and older undergoing hip fracture surgery.43 Pre- and postoperative EA at Baihui (DU20), Sishencong (EX-HN1), Neiguan (PC6), and Zusanli (ST36) significantly reduced PND incidence compared to sham acupuncture (15% vs 38%, P<0.05), modulated inflammatory responses (IL-1β, IL-6, S-100β; all P<0.05), stabilized intraoperative hemodynamics, alleviated postoperative pain (visual analog scale scores at 24h: 2.1±0.8 vs 3.4±1.2, P<0.01), and decreased PONV incidence (10% vs 28%, P<0.05). These multimodal benefits align with the integrated nature of perioperative challenges and support EA as a promising intervention for this vulnerable population.
Transcutaneous Electrical Acupoint Stimulation
Transcutaneous electrical acupoint stimulation (TEAS) delivers electrical stimulation to acupoints via surface electrodes, eliminating needle insertion and associated risks including bleeding, infection, and pneumothorax. This non-invasive modality holds particular appeal for elderly or anticoagulated patients in whom needling may be contraindicated, and can be administered by nursing staff following standardized protocols without specialized acupuncture training.44
The largest TEAS meta-analysis to date, incorporating 76 randomized controlled trials and 9665 patients across diverse surgical populations, demonstrated that TEAS reduced cumulative morphine equivalent consumption by 14.60 mg within 24 hours (95% CI, −18.32 to −10.88; P<0.001)—a clinically significant opioid-sparing effect representing approximately 30% reduction from typical postoperative opioid requirements.44 Secondary outcomes revealed meaningful improvements in quality of recovery scores (+10.64 points on QoR-40; 95% CI, 6.82–14.46), accelerated gastrointestinal function recovery (time to first flatus: MD, −8.2 hours; time to first defecation: MD, −12.4 hours), and reduced opioid-related side effects including PONV (RR, 0.67; 95% CI, 0.54–0.83) and dizziness (RR, 0.56; 95% CI, 0.38–0.82). The non-invasive nature and ease of application strongly support TEAS integration into perioperative protocols.
TEAS has demonstrated specific efficacy for postoperative cognitive dysfunction (POCD) prevention—a critical concern in elderly hip fracture patients with reported incidence rates of 10–54% depending on assessment timing and diagnostic criteria. A meta-analysis of 20 trials comprising 1549 patients found that intraoperative TEAS combined with anesthesia significantly reduced POCD incidence (OR, 0.29; 95% CI, 0.22–0.38; P<0.001).45 Subgroup analysis confirmed efficacy in orthopedic surgery populations (OR, 0.31; 95% CI, 0.19–0.51) and elderly patients (OR, 0.27; 95% CI, 0.18–0.40). The combination of Hegu (LI4) and Neiguan (PC6) showed the most consistent benefits across studies, suggesting these acupoints as priority targets for cognitive protection protocols. Proposed mechanisms include modulation of neuroinflammation, preservation of blood-brain barrier integrity, and enhancement of cerebral perfusion during surgery.
Auricular Acupuncture and Auriculotherapy
Auricular acupuncture targets the external ear, which TCM theory and modern neuroanatomical mapping identify as a microsystem reflecting the entire body through somatotopic organization. The vagal auricular branch (Arnold’s nerve) provides a unique pathway through which auricular stimulation can modulate parasympathetic tone, with downstream effects on inflammation (via the cholinergic anti-inflammatory pathway), pain processing, gastrointestinal motility, and cardiovascular function.46 This vagal mechanism has been validated through heart rate variability analyses demonstrating increased parasympathetic activity following auricular stimulation.
A systematic review and meta-analysis of 21 randomized controlled trials encompassing 1527 patients evaluated auricular acupuncture specifically for perioperative pain management across various surgical procedures.47 Auricular acupuncture significantly reduced pain intensity (MD, −0.44 on 0–10 scale; 95% CI, −0.72 to −0.17; P=0.002) and analgesic requirements (standardized mean difference [SMD], −0.38; 95% CI, −0.62 to −0.14). The non-invasive nature of auricular acupressure using vaccaria seeds, magnetic pellets, or ear beads renders it particularly suitable for elderly or frail patients who may not tolerate needle insertion, and allows for patient self-administration of continued stimulation between practitioner sessions.
A recent randomized controlled trial specifically evaluated buccal acupuncture therapy (a related microsystem approach) for postoperative delirium prevention in 120 elderly patients (≥65 years) undergoing orthopedic lower limb surgery.48 The intervention group demonstrated significantly reduced POD incidence (12% vs 27%, P=0.03), decreased intraoperative opioid consumption (fentanyl: 142±38 μg vs 186±45 μg, P<0.01), lower postoperative pain scores, and reduced PONV incidence. Importantly, no serious adverse events were attributed to the acupuncture intervention, supporting its safety in this vulnerable population.
Acupoint Selection: Evidence-Based Protocols
The selection of acupoints for perioperative application follows both traditional TCM theory and contemporary evidence synthesis. Neiguan (PC6), located on the anterior forearm two cun proximal to the wrist crease between the tendons of palmaris longus and flexor carpi radialis, represents the most extensively studied acupoint for PONV prevention with the highest quality evidence base.49 The landmark Cochrane review by Lee et al, incorporating over 40 RCTs and 4858 patients, established that PC6 stimulation through various modalities (acupuncture, electroacupuncture, TEAS, acupressure) significantly reduces postoperative nausea (RR, 0.68; 95% CI, 0.60–0.77) and vomiting (RR, 0.60; 95% CI, 0.51–0.71) with efficacy comparable to commonly used antiemetic drugs. The proposed mechanism involves vagal afferent stimulation that modulates the vomiting center in the medulla oblongata.
Hegu (LI4), located on the dorsum of the hand between the first and second metacarpal bones, and Zusanli (ST36), located on the anterior leg three cun below the knee joint lateral to the tibial tuberosity, constitute commonly employed acupoints for pain management with effects mediated through both segmental spinal mechanisms and supraspinal descending modulation.15 Sanyinjiao (SP6), located on the medial leg three cun above the medial malleolus, provides additional analgesic effects and promotes circulation according to TCM theory. Baihui (DU20) and associated scalp acupoints (Sishencong, EX-HN1) target cognitive function and sleep, with protocols specifically designed for perioperative neurocognitive disorder prevention employing these points in combination with body acupoints.
An integrative systematic review examining acupoint stimulation within ERAS protocols identified Zusanli (ST36) and Neiguan (PC6) as the most frequently employed acupoints across 11 included RCTs, with significant effects on pain intensity (SMD, −0.94; 95% CI, −1.32 to −0.56), analgesic drug consumption (SMD, −1.87; 95% CI, −2.45 to −1.29), and PONV (RR, 0.29; 95% CI, 0.16–0.53).50 Importantly, only one adverse event (minor bruising at insertion site) was reported across all included studies, supporting the excellent safety profile of these interventions in surgical populations.
Critical Appraisal of TCM Evidence Quality
While the evidence supporting TCM modalities in perioperative care is promising, several methodological limitations warrant critical acknowledgment. First, many included RCTs are characterized by small sample sizes (frequently n<100 per group), limiting statistical power and the precision of effect estimates. Second, acupuncture trials face inherent blinding challenges: although sham acupuncture controls have been employed in high-quality studies, the adequacy of patient blinding and the extent to which sham procedures are truly inert remain subjects of ongoing methodological debate. Third, substantial heterogeneity exists in stimulation parameters—including acupoint selection, electrical frequency and intensity, treatment duration, and timing relative to surgery—complicating cross-study comparisons and meta-analytical pooling. Risk of bias assessments in systematic reviews frequently identify unclear or high risk in domains of allocation concealment and performance bias. Fourth, many studies rely on short-term surrogate outcomes and follow-up periods that may not capture clinically meaningful long-term effects, and few studies specifically target elderly hip fracture populations as opposed to general surgical cohorts. Despite these constraints, the consistency of effect direction across independent studies, the biological plausibility of proposed neuromodulatory mechanisms, and the favorable safety profile across all modalities collectively support their cautious incorporation into perioperative protocols as adjunctive therapies, pending higher-quality hip fracture-specific evidence.
Integrative Framework: Combining Western and TCM Approaches
Rationale for Integration
The integration of Western and TCM approaches for perioperative management rests upon recognition of complementary mechanisms and potential synergistic therapeutic effects. Western interventions excel in acute symptom control through targeted pharmacological agents and regional anesthesia techniques with well-characterized dose-response relationships and predictable onset-offset kinetics.9,10 TCM modalities engage broader regulatory systems—autonomic balance through vagal stimulation, endogenous opioid release through acupoint activation, inflammatory modulation through the cholinergic anti-inflammatory pathway, and circadian rhythm support—that address underlying pathophysiology rather than merely suppressing symptoms.13–16
The multimodal nature of acupoint stimulation aligns philosophically with the multimodal analgesia paradigm central to modern perioperative care. Just as combining analgesics with different mechanisms of action (opioid, NSAID, local anesthetic) enhances efficacy while reducing individual drug doses and associated adverse effects, the addition of TCM modalities to Western protocols may permit further reductions in pharmacological interventions while maintaining or improving outcomes.34,44 This is particularly relevant for elderly patients in whom polypharmacy poses substantial risks. The opioid-sparing effects of acupoint stimulation (14.60 mg morphine equivalent reduction) combined with regional anesthesia can substantially reduce or eliminate the need for systemic opioids in many patients.
Multicomponent interventions for delirium prevention have demonstrated significant efficacy in hospitalized elderly patients, with a meta-analysis of 10 RCTs (n=2850) showing reduced delirium incidence (RR, 0.62; 95% CI, 0.54–0.72), duration, and severity.51 A systematic review specifically examining multicomponent interventions in elderly hip fracture patients confirmed these benefits (OR, 0.64; 95% CI, 0.46–0.87).52 The integration of TCM modalities targeting sleep, pain, and cognitive function adds additional non-pharmacological tools to these multicomponent approaches, potentially enhancing their effectiveness while maintaining the drug-free intervention philosophy that reduces polypharmacy-related risks.
Direct comparative evidence between fully integrated Western–TCM protocols and Western-only care in hip fracture populations remains limited; however, indirect evidence supports additive benefits. The network meta-analysis by Liu et al found that combined acupuncture-multimodal analgesia approaches reduced postoperative pain scores more effectively than either modality alone across arthroplasty populations.16 For PONV, PC6 acupoint stimulation combined with ondansetron demonstrated superior prophylactic efficacy compared to ondansetron monotherapy in multiple RCTs.50 For sleep outcomes, combined melatonin supplementation with TEAS has been associated with improvements in sleep architecture beyond pharmacological intervention alone.44 The integrated protocol proposed herein is positioned not as a replacement for established Western ERAS protocols, but as a complementary enhancement that addresses residual gaps in current standard-of-care—particularly the persistent challenges of sleep disturbance and delirium risk that pharmacological approaches alone have failed to fully resolve in this population.
Clinical decision-making regarding the application of Western medicine alone, TCM alone, or an integrated approach should be guided by patient-specific factors, institutional capacity, and symptom burden. Western regional anesthesia and pharmacological prophylaxis remain the foundational interventions for all patients, given their strong evidence base and immediate onset of effect. TCM modalities are most appropriately employed as adjuncts when: (1) opioid-sparing strategies are prioritized due to elevated delirium or respiratory risk; (2) patients show inadequate response to standard pharmacological prophylaxis for PONV or pain; (3) sleep disturbance is severe and pharmacological options are constrained by polypharmacy concerns; or (4) patients express informed preference for complementary approaches. Conversely, conditions that preclude specific TCM modalities—severe coagulopathy contraindicating needling, active cutaneous infections at acupoint sites, or implanted electrical devices that preclude TEAS—should direct clinicians toward Western-only approaches. The integrated framework is most effectively implemented in institutions with trained TCM practitioners and standardized protocols that facilitate systematic incorporation into existing ERAS pathways.
Proposed Integrative Protocol
Based upon synthesis of current evidence from both Western and TCM literature, we propose an integrative multimodal protocol for elderly hip fracture patients addressing sleep, pain, and PONV across the perioperative continuum (Table 1). This protocol stratifies interventions by perioperative phase—preoperative, intraoperative, postoperative, and rehabilitation—and incorporates both Western and TCM modalities targeting each symptom domain with appropriate timing and dosing based on available evidence.
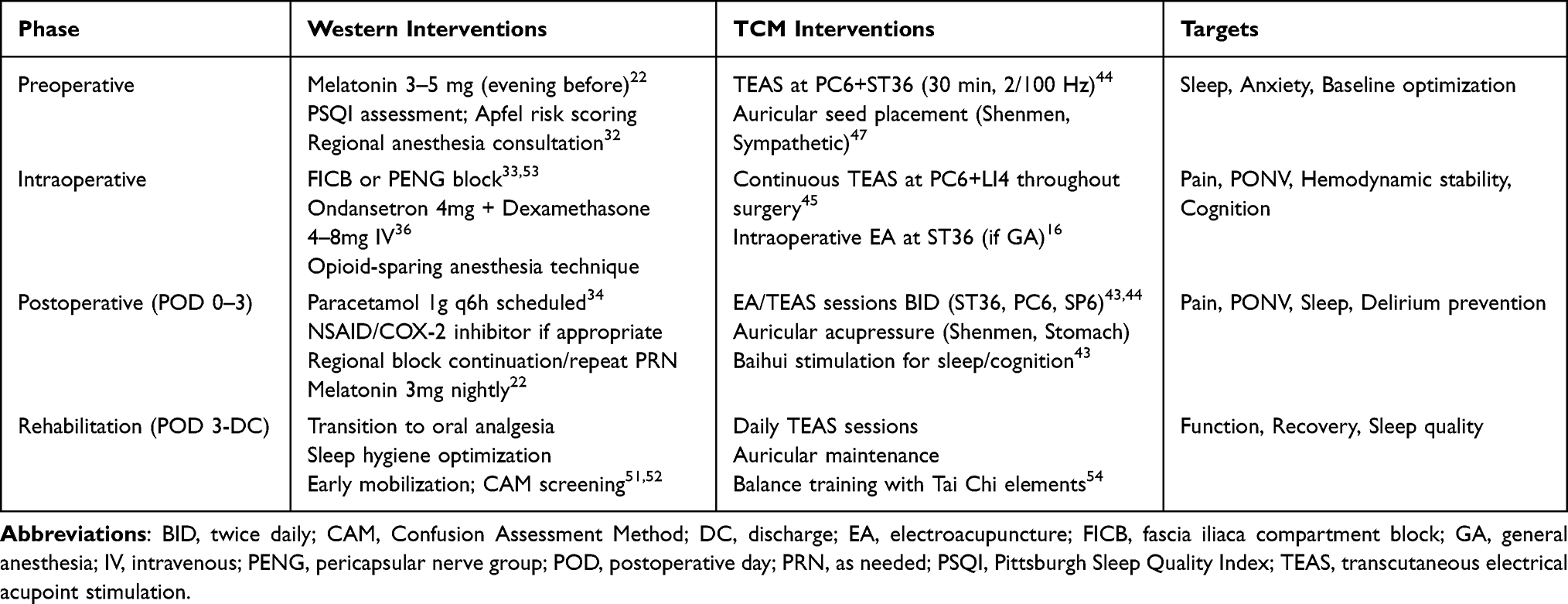 |
Table 1 Proposed Integrative Multimodal Protocol for Elderly Hip Fracture Patients |
During the preoperative phase, comprehensive assessment should include baseline sleep quality evaluation using validated instruments (PSQI), frailty screening (Clinical Frailty Scale or FRAIL scale), cognitive baseline (Mini-Mental State Examination or Montreal Cognitive Assessment), and PONV risk stratification (Apfel simplified score). Melatonin supplementation (3–5 mg) commences the evening before surgery to support circadian rhythm and provide anxiolytic effects.22 TEAS at PC6 and ST36 may begin preoperatively (30-minute session with alternating 2/100 Hz frequency) to establish therapeutic effects and reduce preoperative anxiety.44
The intraoperative phase incorporates peripheral nerve block administration (FICB, femoral nerve block, or PENG block) prior to or following anesthesia induction, providing preemptive analgesia that reduces central sensitization. Multimodal PONV prophylaxis with ondansetron (4 mg IV) and dexamethasone (4–8 mg IV) addresses baseline emetic risk. Intraoperative TEAS at PC6 and LI4 provides supplementary analgesia, PONV prevention, and cognitive protection through mechanisms complementary to pharmacological interventions.45
During the postoperative phase, scheduled multimodal analgesia with paracetamol (1g every 6 hours) and NSAIDs or COX-2 inhibitors (if not contraindicated by renal function, cardiovascular risk, or concurrent anticoagulation) forms the analgesic foundation. Regional anesthesia catheter continuation or repeated single-shot blocks are administered as indicated by pain severity. Electroacupuncture or TEAS sessions targeting ST36, PC6, and SP6 commence on postoperative day 0–1, continuing twice daily through discharge. Auricular acupressure at Shenmen and sympathetic points supports sleep quality and anxiety management with patient self-administered stimulation between sessions. Melatonin continuation (3 mg nightly) maintains circadian support throughout hospitalization.
Evidence Summary for TCM Modalities
Table 2 summarizes the current evidence base for TCM modalities targeting perioperative pain, sleep/cognitive outcomes, and PONV, including effect sizes, sample sizes, and safety profiles from systematic reviews and meta-analyses. This evidence synthesis supports the proposed integrative protocol and identifies areas requiring further investigation.
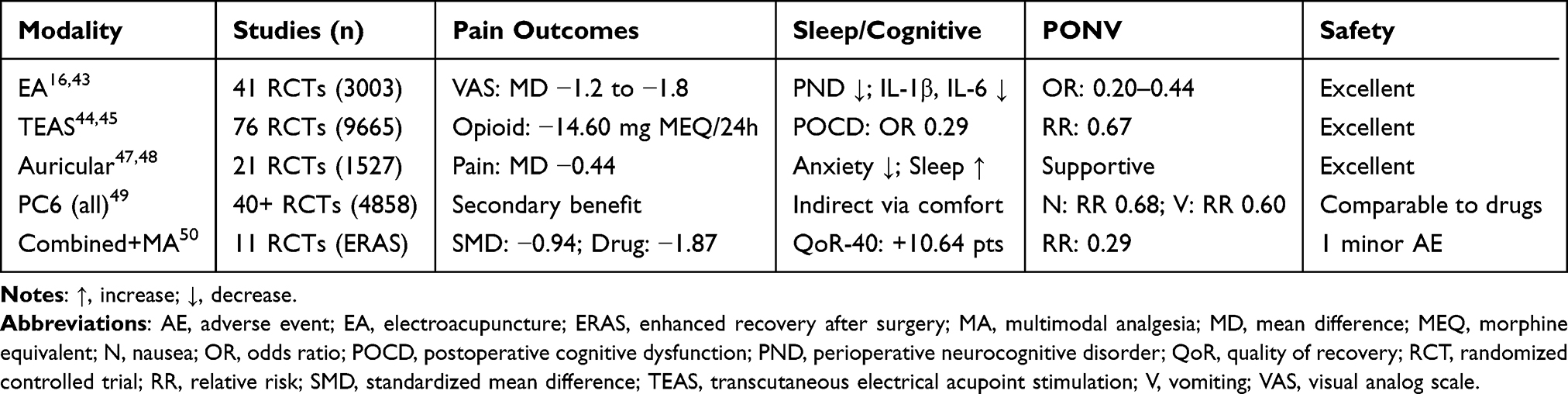 |
Table 2 Summary of Evidence: TCM Modalities for Perioperative Pain, Sleep, and PONV Management |
Synthesis and Critical Appraisal
This review identifies a coherent body of evidence supporting both Western and TCM approaches to the perioperative triumvirate of pain, sleep disturbance, and PONV in elderly hip fracture patients. Western interventions—particularly peripheral nerve blocks and multimodal pharmacological prophylaxis—demonstrate the highest-quality evidence, derived from large, well-designed randomized controlled trials and endorsed by international consensus guidelines. These interventions provide consistent, predictable, and rapid-onset effects appropriate for the acute perioperative context, and should constitute the foundational tier of any integrated management strategy. TCM modalities occupy a complementary evidence tier: acupoint stimulation techniques demonstrate clinically meaningful effect sizes for pain reduction, PONV prevention, and cognitive protection, supported by multiple systematic reviews and meta-analyses, but constrained by methodological limitations that temper confidence in precise effect magnitude estimates. Critically, the theoretical framework of neurobiological crosstalk across the pain-sleep-PONV axis provides biological plausibility for the integrated approach: Western interventions predominantly address peripheral and acute nociceptive pathways and emetic trigger zones, while TCM modalities appear to exert broader modulatory effects through autonomic, neuroendocrine, and neuroinflammatory mechanisms. Comparative evaluation across studies reveals a consistent pattern—interventions targeting multiple nodes of the pain-sleep-PONV axis outperform single-target strategies—whether comparing multimodal Western analgesia to opioid monotherapy, or combined acupoint-pharmacological prophylaxis to pharmacological prophylaxis alone. This convergent finding across therapeutic traditions supports the integrative framework proposed herein and highlights the limitations of single-modality approaches in this complex patient population.
Evidence Gaps and Future Directions
Despite the promising evidence supporting integrative perioperative management, significant gaps remain that warrant systematic investigation. No large-scale randomized controlled trials have specifically examined comprehensive Western-TCM integration in hip fracture populations; existing studies typically evaluate single TCM modalities in isolation, precluding assessment of additive or synergistic effects from combining multiple approaches.13–16 The heterogeneity of acupoint selection, stimulation parameters (frequency, intensity, duration), and treatment timing across studies limits the ability to identify optimal protocols.
Mechanistic studies employing advanced neuroimaging (functional MRI, PET) and comprehensive biomarker panels could elucidate the neurobiological substrates underlying TCM effects, facilitating optimization of treatment parameters and identification of patient subpopulations most likely to benefit.15 The pain-sleep-PONV axis itself requires investigation as an integrated system rather than three independent outcomes; studies examining the interconnections among these domains and the effects of interventions targeting one domain on the others would advance understanding of optimal multimodal approaches.
Standardization of TCM intervention protocols—including acupoint selection based on TCM diagnosis, stimulation parameters, treatment timing relative to surgery, and session frequency/duration—would enhance reproducibility and comparability across studies. Development of core outcome sets incorporating patient-reported outcomes (quality of recovery, patient satisfaction, functional status) alongside traditional clinical endpoints (pain scores, opioid consumption, length of stay) would better capture the holistic benefits of integrative approaches.
Cost-effectiveness analyses comparing integrative protocols to Western-only care would inform healthcare system adoption decisions and resource allocation. Given the substantial costs associated with hip fracture complications—particularly delirium (estimated $16,000–64,000 additional costs per episode) and prolonged hospitalization—interventions preventing these complications may prove cost-saving despite additional TCM-related resource utilization.27,29 Implementation research examining barriers and facilitators to integrative protocol adoption in diverse healthcare settings would guide knowledge translation efforts.
Practical implementation of the proposed integrative protocol requires systematic attention to implementation science. Key operational questions include: (1) Personnel: who administers TCM therapies—licensed acupuncturists, certified anesthesiology nurses, or trained physical therapists? Regulatory frameworks governing acupuncture practice vary substantially across healthcare systems, necessitating site-specific adaptation of the proposed protocol. (2) Training requirements: brief standardized training programs (8–16 hours) for perioperative nurses in TEAS and auricular acupressure have been successfully implemented in Chinese tertiary hospitals and may represent a scalable model for international adoption. (3) Cost implications: while the upfront cost of TCM equipment (TEAS devices, acupressure pellets) is modest (estimated USD 5–50 per patient), staffing costs and training investment require institutional commitment; favorable analyses suggest that reductions in opioid consumption, rescue antiemetic use, and delirium episodes may offset initial costs. (4) Standardization within ERAS: protocol-driven checklists specifying acupoint selection, stimulation parameters, and treatment timing relative to anesthesia induction facilitate integration into existing fast-paced surgical pathways without disrupting workflow.
Digital health technologies offer emerging opportunities for perioperative optimization and post-discharge monitoring. A systematic review of home-based digital health interventions for elderly hip fracture patients demonstrated significant functional improvements including decreased Timed Up and Go test times (−7.89 seconds, P<0.001) and improved Short Physical Performance Battery scores.55 Integration of wearable devices for sleep monitoring, mobile applications for TEAS delivery guidance, and telehealth follow-up could extend the benefits of integrative approaches beyond the hospital stay and into the critical rehabilitation phase.
Future research should prioritize the following study designs: (1) a pragmatic, multicenter randomized controlled trial comparing the full proposed integrative perioperative protocol versus standard Enhanced Recovery After Surgery (ERAS) care in elderly hip fracture patients, powered to detect clinically meaningful differences in a composite endpoint incorporating pain scores, sleep quality (polysomnographic assessment), PONV incidence, and delirium rates; (2) mechanistic studies employing inflammatory biomarkers (IL-6, TNF-α, IL-1β), cortisol, melatonin, heart rate variability, and functional neuroimaging to objectively characterize the physiological effects of combined Western–TCM interventions; (3) cost-effectiveness analyses incorporating quality-adjusted life years (QALYs), complication rates, and length of hospital stay; and (4) implementation science studies using mixed-methods designs to evaluate barriers and facilitators to protocol adoption across diverse healthcare systems with differing regulatory frameworks for TCM practice.
Limitations
This review has several inherent limitations. As a narrative review, the synthesis is subject to potential selection bias, as the literature search was not exhaustive and no formal meta-analytical pooling was performed. The absence of large-scale, hip fracture-specific randomized controlled trials evaluating fully integrated Western–TCM perioperative protocols represents a critical evidence gap that tempers the clinical certainty of the proposed integrative framework. Most TCM evidence is derived from heterogeneous surgical populations, and direct extrapolation to elderly hip fracture patients—who present unique physiological vulnerabilities—requires caution. Institutional and cultural heterogeneity in TCM practice standards further complicates generalizability across international healthcare settings. Additionally, the evidence base for some TCM modalities, particularly auricular acupuncture and less-studied acupoint combinations, is derived from studies with high or unclear risk of bias, necessitating conservative interpretation. These limitations underscore the preliminary nature of the proposed integrative protocol and the importance of rigorous prospective investigation before widespread clinical adoption.
Conclusion
Elderly hip fracture patients face a triumvirate of perioperative challenges—pain, sleep disturbance, and PONV—that engage in bidirectional neurobiological crosstalk amplifying each component and contributing to adverse outcomes including delirium, prolonged hospitalization, functional decline, and mortality. Western medicine has developed evidence-based approaches including peripheral nerve blocks, multimodal analgesia, pharmacological PONV prophylaxis, and sleep optimization strategies that form the foundation of contemporary perioperative care. Traditional Chinese Medicine offers complementary therapeutic modalities—electroacupuncture, transcutaneous electrical acupoint stimulation, and auricular therapy—with mounting evidence supporting efficacy in each symptom domain through mechanisms distinct from yet complementary to pharmacological interventions.
The integration of Western and TCM approaches leverages complementary mechanisms—targeted symptom control from pharmacological agents and regional anesthesia combined with systemic regulatory effects from acupoint stimulation—to potentially enhance therapeutic efficacy while reducing polypharmacy burden in this vulnerable population. The opioid-sparing effects of TCM modalities (14.60 mg morphine equivalent reduction with TEAS) are particularly valuable given the heightened susceptibility of elderly patients to opioid-related adverse effects. While robust evidence from large-scale integrative trials specifically in hip fracture populations remains limited, the consistent safety profile and encouraging efficacy signals from existing studies across surgical populations support thoughtful clinical implementation within appropriately designed protocols.
Future research should prioritize rigorous methodology including adequately powered RCTs with sham controls, mechanistic investigation through neuroimaging and biomarker studies, standardized intervention protocols, and comprehensive outcome assessment incorporating patient-reported measures. The demographic imperative posed by global population aging—with hip fracture incidence projected to reach 6.3 million annually by 2050—demands innovative approaches to optimize perioperative outcomes in this growing patient population. The synthesis of Western and Traditional Chinese Medicine therapeutic traditions offers a promising path forward, combining the precision of evidence-based Western medicine with the holistic, regulatory approach of TCM to address the complex, interconnected challenges of perioperative care in elderly hip fracture patients.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by 2023 Yunnan University of Chinese Medicine Nursing Special Fund (Grant No. YZHZ202304).
Disclosure
Rui Hu and Yueli Ding are co-first authors for this study. The authors have no conflicts of interest to declare for this work.
References
1. Veronese N, Maggi S. Epidemiology and social costs of Hip fracture. Injury. 2018;49(8):1458–15. doi:10.1016/j.injury.2018.04.015
2. Kanis JA, Norton N, Harvey NC, et al. SCOPE 2021: a new scorecard for osteoporosis in Europe. Arch Osteoporos. 2021;16(1):82. doi:10.1007/s11657-020-00871-9
3. Haentjens P, Magaziner J, Colón-Emeric CS, et al. Meta-analysis: excess mortality after Hip fracture among older women and men. Ann Intern Med. 2010;152(6):380–390. doi:10.7326/0003-4819-152-6-201003160-00008
4. Dyer SM, Crotty M, Fairhall N, et al. A critical review of the long-term disability outcomes following Hip fracture. BMC Geriatr. 2016;16:158. doi:10.1186/s12877-016-0332-0
5. Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A. Incidence and economic burden of osteoporosis-related fractures in the United States, 2005–2025. J Bone Miner Res. 2007;22(3):465–475. doi:10.1359/jbmr.061113
6. Schenning KJ, Deiner SG. Postoperative delirium in the geriatric patient. Anesthesiol Clin. 2015;33(3):505–516. doi:10.1016/j.anclin.2015.05.007
7. Krenk L, Rasmussen LS. Postoperative delirium and postoperative cognitive dysfunction in the elderly - what are the differences? Minerva Anestesiol. 2011;77(7):742–749.
8. Chung F, Liao P, Yegneswaran B, Shapiro CM, Kang W. Postoperative changes in sleep-disordered breathing and sleep architecture in patients with obstructive sleep apnea. Anesthesiology. 2014;120(2):287–298. doi:10.1097/ALN.0000000000000040
9. Duan Y, Chen X, Chen S, et al. Enhanced recovery after surgery for Hip fractures: a systematic review and meta-analysis. Perioper Med. 2021;10:31. doi:10.1186/s13741-021-00201-8
10. Melnyk M, Casey RG, Black P, Koupparis AJ. Enhanced recovery after surgery (ERAS) protocols: time to change practice? Can Urol Assoc J. 2011;5(5):342–348. doi:10.5489/cuaj.11002
11. Clegg A, Young JB. Which medications to avoid in people at risk of delirium: a systematic review. Age Ageing. 2011;40(1):23–29. doi:10.1093/ageing/afq140
12. Oresanya LB, Lyons WL, Finlayson E. Preoperative assessment of the older patient: a narrative review. JAMA. 2014;311(20):2110–2120. doi:10.1001/jama.2014.4573
13. Lu L, Liao M, Zeng J, He J. Acupuncture for postoperative pain management: a review of evidence-based research. J Acupunct Meridian Stud. 2021;14(6):203–210. doi:10.51507/j.jams.2021.14.6.203
14. Zhang R, Lao L, Ren K, Berman BM. Mechanisms of acupuncture-electroacupuncture on persistent pain. Anesthesiology. 2014;120(2):482–503. doi:10.1097/ALN.0000000000000101
15. Vickers AJ, Vertosick EA, Lewith G, et al. Acupuncture for chronic pain: update of an individual patient data meta-analysis. J Pain. 2018;19(5):455–474. doi:10.1016/j.jpain.2017.11.005
16. Liu N, Liu G, Chang X, et al. Combining various acupuncture therapies with multimodal analgesia to enhance postoperative pain management following total knee arthroplasty: a network meta-analysis of randomized controlled trials. Front Neurol. 2024;15:1361037. doi:10.3389/fneur.2024.1361037
17. Finan PH, Goodin BR, Smith MT. The association of sleep and pain: an update and a path forward. J Pain. 2013;14(12):1539–1552. doi:10.1016/j.jpain.2013.08.007
18. Tracey I, Mantyh PW. The cerebral signature for pain perception and its modulation. Neuron. 2007;55(3):377–391. doi:10.1016/j.neuron.2007.07.012
19. Mullington JM, Simpson NS, Meier-Ewert HK, Haack M. Sleep loss and inflammation. Best Pract Res Clin Endocrinol Metab. 2010;24(5):775–784. doi:10.1016/j.beem.2010.08.014
20. Besedovsky L, Lange T, Haack M. The sleep-immune crosstalk in health and disease. Physiol Rev. 2019;99(3):1325–1380. doi:10.1152/physrev.00010.2018
21. Horn CC. Why is the neurobiology of nausea and vomiting so important? Appetite. 2008;50(2–3):430–434. doi:10.1016/j.appet.2007.09.015
22. Shin HW, Kwak JS, Choi YJ, et al. Efficacy and safety of perioperative melatonin for postoperative delirium in patients undergoing surgery: a systematic review and meta-analysis. J Int Med Res. 2024;52(5):03000605241239854. doi:10.1177/03000605241239854
23. Zhang M, Wang B, Li D, et al. Effects of dexmedetomidine on postoperative sleep quality: a systematic review and meta-analysis of randomized controlled trials. BMC Anesthesiol. 2023;23:118. doi:10.1186/s12871-023-02048-6
24. Butris N, Tang E, Engelman DT, et al. The prevalence and risk factors of sleep disturbances in surgical patients: a systematic review and meta-analysis. Sleep Med Rev. 2023;69:101786. doi:10.1016/j.smrv.2023.101786
25. Guo H, Li LH, Lv XH, et al. Association between preoperative sleep disturbance and postoperative delirium in elderly: a retrospective cohort study. Nat Sci Sleep. 2024;16:389–400. doi:10.2147/NSS.S452517
26. Ou-Yang CL, Ma LB, Wu XD, et al. Association of sleep quality on the night of operative day with postoperative delirium in elderly patients: a prospective cohort study. Eur J Anaesthesiol. 2024;41(3):212–221. doi:10.1097/EJA.0000000000001937
27. Inouye SK, Westendorp RG, Saczynski JS. Delirium in elderly people. Lancet. 2014;383(9920):911–922. doi:10.1016/S0140-6736(13)60688-1
28. Alam A, Hana Z, Jin Z, Suen KC, Ma D. Surgery, neuroinflammation and cognitive impairment. EBioMedicine. 2018;37:547–556. doi:10.1016/j.ebiom.2018.10.021
29. Dong X, Zhang X, Hu F, Yang S, Hong Z, Geng Q. Association of frailty with adverse outcomes in surgically treated geriatric patients with Hip fracture: a meta-analysis and trial sequential analysis. PLoS One. 2024;19(6):e0305706. doi:10.1371/journal.pone.0305706
30. Morin L, Johnell K, Laroche ML, Fastbom J, Wastesson JW. The epidemiology of polypharmacy in older adults: register-based prospective cohort study. Clin Epidemiol. 2018;10:289–298. doi:10.2147/CLEP.S153458
31. Maher RL, Hanlon J, Hajjar ER. Clinical consequences of polypharmacy in elderly. Expert Opin Drug Saf. 2014;13(1):57–65. doi:10.1517/14740338.2013.827660
32. Guay J, Kopp S. Peripheral nerve blocks for Hip fractures in adults. Cochrane Database Syst Rev. 2020;(11):CD001159. doi:10.1002/14651858.CD001159.pub3
33. Mysore K, Sancheti SA, Howells SR, et al. Quality of recovery after pericapsular nerve group (PENG) block for primary total Hip arthroplasty under spinal anaesthesia: a randomised controlled observer-blinded trial. Br J Anaesth. 2023;130(6):773–779. doi:10.1016/j.bja.2023.02.017
34. Pissens S, Cavens L, Joshi GP, et al. Pain management after Hip fracture repair surgery: a systematic review and procedure-specific postoperative pain management (PROSPECT) recommendations. Acta Anaesthesiol Belg. 2024;75:15–31.
35. Garlich J, Pendo E, Engelsgjerd J, et al. Geriatric pain protocol: impact of multimodal pain care for elderly orthopaedic trauma patients. Orthop Nurs. 2023;42(4):202–210. doi:10.1097/NOR.0000000000000954
36. Gan TJ, Belani KG, Bergese S, et al. Fourth consensus guidelines for the management of postoperative nausea and vomiting. Anesth Analg. 2020;131(2):411–448. doi:10.1213/ANE.0000000000004833
37. Jin Z, Gan TJ, Bergese SD. Prevention and treatment of postoperative nausea and vomiting (PONV): a review of current recommendations and emerging therapies. Ther Clin Risk Manag. 2020;16:1305–1317. doi:10.2147/TCRM.S256234
38. Liu Y, Li W, Wei X, et al. The efficacy of aprepitant for the prevention of postoperative nausea and vomiting: a meta-analysis. Medicine. 2023;102(29):e34385. doi:10.1097/MD.0000000000034385
39. Roberts GW, Bekker TB, Carlsen HH, Moffatt CH, Slattery PJ, McClure AF. Postoperative nausea and vomiting are strongly influenced by postoperative opioid use in a dose-related manner. Anesth Analg. 2005;101(5):1343–1348. doi:10.1213/01.ANE.0000180204.64588.EC
40. Seely D, Wu P, Fritz H, et al. Melatonin as adjuvant cancer care with and without chemotherapy: a systematic review and meta-analysis of randomized trials. Integr Cancer Ther. 2012;11(4):293–303. doi:10.1177/1534735411425484
41. Weerink MAS, Struys MMRF, Hannivoort LN, Barber CB, Absalom AR, Colin P. Clinical pharmacokinetics and pharmacodynamics of dexmedetomidine. Clin Pharmacokinet. 2017;56(8):893–913. doi:10.1007/s40262-017-0507-7
42. Cha Y, Kim JT, Kim JW, et al. Analysis of changes in sleep quality and patterns after Hip fracture using real evidence of artificial intelligence linked (REAL) hip cohort data. Medicina. 2023;59(12):2125. doi:10.3390/medicina59122125
43. Long J, Zhang X, Zhang J, Zhou T, Chen W. Effect of electroacupuncture intervention before and after operation on perioperative neurocognitive disorders in elderly patients with Hip fractures: a randomized controlled trial. Injury. 2025;56(2):112052. doi:10.1016/j.injury.2025.112052
44. Tan SY, Jiang H, Ma Q, et al. Effects of transcutaneous electrical acupoint stimulation on early postoperative pain and recovery: a comprehensive systematic review and meta-analysis of randomized controlled trials. Front Med. 2024;11:1302057. doi:10.3389/fmed.2024.1302057
45. Gan L, Qian K, Yang J, et al. Intraoperative transcutaneous electrical acupoint stimulation combined with anesthesia to prevent postoperative cognitive dysfunction: a systematic review and meta-analysis. PLoS One. 2025;20(1):e0313622. doi:10.1371/journal.pone.0313622
46. Badran BW, Dowdle LT, Mithoefer OJ, et al. Neurophysiologic effects of transcutaneous auricular vagus nerve stimulation (taVNS) via electrical stimulation of the tragus: a concurrent taVNS/fMRI study and review. Brain Stimul. 2018;11(3):492–500. doi:10.1016/j.brs.2017.12.009
47. Zhou Y, Bao Q, Yang C, et al. Auricular acupuncture for perioperative pain management: a systematic review and meta-analysis of randomized controlled trials. J Pain Res. 2024;17:2827–2841. doi:10.2147/JPR.S488525
48. Wang P, Zhang J, Liao Q, et al. Effect of buccal acupuncture therapy on the incidence of postoperative delirium in older adults undergoing orthopedic lower limb surgery: a randomized controlled trial. J Psychosom Res. 2025;189:112025. doi:10.1016/j.jpsychores.2025.112025
49. Lee A, Chan SK, Fan LT. Stimulation of the wrist acupuncture point PC6 for preventing postoperative nausea and vomiting. Cochrane Database Syst Rev. 2015;(11):CD003281. doi:10.1002/14651858.CD003281.pub4
50. Chen J, Xu Y, Li L, Yang G, Zhou X. Acupoint stimulation for pain control in enhanced recovery after surgery: systematic review and meta-analysis. J Integr Complement Med. 2024;30(1):85–96. doi:10.1089/jicm.2023.0272
51. Avendaño-Céspedes A, Cortés-Borra A, Ortega-Belmonte MC, García-Cantos N, Abizanda P. Multicomponent interventions for the prevention of delirium in hospitalized older people: a meta-analysis. J Am Geriatr Soc. 2020;68(11):2602–2610. doi:10.1111/jgs.16704
52. Oberai T, Laver K, Crotty M, Killington M, Jaarsma R. Effectiveness of multicomponent interventions on incidence of delirium in hospitalized older patients with Hip fracture: a systematic review. Int Psychogeriatr. 2018;30(4):481–492. doi:10.1017/S1041610217002782
53. Makkar JK, Singh NP, Bhatia N, Samra T, Singh PM. Fascia iliaca block for Hip fractures in the emergency department: meta-analysis with trial sequential analysis. Am J Emerg Med. 2021;50:654–660. doi:10.1016/j.ajem.2021.09.038
54. Chang H, Luan C, Li C. Effect of comprehensive rehabilitation training based on balance function on postoperative recovery and function of Hip fracture in the elderly: a systematic review and meta-analysis. Geriatr Orthop Surg Rehabil. 2024;15:21514593241261506. doi:10.1177/21514593241261506
55. Pliannuom S, Pinyopornpanish K, Buawangpong N, et al. Characteristics and effects of home-based digital health interventions on functional outcomes in older patients with Hip fractures after surgery: systematic review and meta-analysis. J Med Internet Res. 2024;26:e49482. doi:10.2196/49482
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.