Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Multidisciplinary Formulation of a Walking Rehabilitation Nursing Protocol for Patients with Lower Extremity Arteriosclerosis Obliterans: A Delphi Study
Authors Niu Q ![]() , Zhang Q, Yu Y, Jia Y
, Zhang Q, Yu Y, Jia Y ![]() , Li X, Zhang Y
, Li X, Zhang Y ![]()
Received 23 November 2025
Accepted for publication 15 February 2026
Published 3 March 2026 Volume 2026:19 583880
DOI https://doi.org/10.2147/JMDH.S583880
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Qingmei Niu,1 Qian Zhang,1 Ying Yu,1 Yatian Jia,2 Xinru Li,2 Yihua Zhang2
1Department of Nursing, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Third Hospital of Shanxi Medical University, Tongji Shanxi Hospital, Taiyuan, Shanxi, People’s Republic of China; 2Department of Nursing, School of Nursing, Shanxi University of Traditional Chinese Medicine, Jinzhong, Shanxi, People’s Republic of China
Correspondence: Qian Zhang, Department of Nursing, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Third Hospital of Shanxi Medical University, Tongji Shanxi Hospital, Taiyuan, Shanxi, People’s Republic of China, Tel +86 13835176091, Email [email protected]
Objective: To develop a contextually tailored walking rehabilitation protocol for Chinese patients with lower extremity arteriosclerosis obliterans (ASO), providing evidence-based theoretical and practical guidance for clinical nursing.
Background: Lower extremity ASO is a prevalent chronic vascular disease with rising incidence, high morbidity, and mortality. Exercise interventions effectively improve patients’ walking ability, and supervised walking programs are promising, yet standardized clinical guidelines remain lacking.
Methods: An evidence-based protocol was developed via systematic review of domestic and international literature. A preliminary draft was refined through two rounds of Delphi consultations with 20 multidisciplinary experts (vascular surgery, nursing, rehabilitation). Statistical analysis of expert agreement finalized the standardized protocol.
Results: Both rounds achieved a 100% response rate. Expert authority coefficients were 0.918 (Round 1) and 0.945 (Round 2). Coefficients of variation ranged 0.00– 0.21 (Round 1) and 0.00– 0.10 (Round 2). Kendall’s concordance coefficients were 0.131 and 0.339 (p< 0.05), indicating significant consensus. The final protocol includes 5 primary, 13 secondary, and 40 tertiary indicators.
Conclusion: This Delphi-derived standardized walking rehabilitation protocol addresses gaps in current guidelines and provides an evidence-based foundation for standardized Lower extremity ASO interventions.
Keywords: lower extremity ASO, walking exercise, nursing, Delphi
Introduction
Lower extremity arteriosclerosis obliterans (ASO) is an ischemic vascular disease caused by atherosclerosis. Its core pathological mechanism is that atherosclerotic plaques gradually form, accumulate and continuously enlarge in the intima of lower extremity arteries, leading to progressive stenosis of the vascular lumen. In severe cases, complete occlusion can occur, thereby blocking blood flow to the lower extremities and causing ischemia and hypoxia in the lower extremity tissues.1 According to global epidemiological data estimates, the number of people affected by this disease worldwide has reached 236.6 million,2 with approximately 45.3 million cases in China alone.3,4 The annual prevalence rate is 10.7%, and this rate is expected to continue to rise with the acceleration of the global aging process.5,6 This disease is characterized by a high incidence rate, high amputation rate and high mortality rate.7 Intermittent claudication is a typical clinical symptom, and about one-third of patients will present with this manifestation.8,9 The limb pain and weakness caused by ischemia and hypoxia will further lead to the decline of lower extremity motor function and a significant decrease in the quality of life of patients.10
If not properly managed, lower extremity arteriosclerosis obliterans (ASO) can advance to total arterial blockage, resulting in critical limb ischemia and eventual tissue death. These advanced cases often necessitate costly surgical procedures, placing substantial pressure on healthcare resources.11 Exercise-based interventions have demonstrated efficacy in preserving ambulatory function and alleviating functional limitations in individuals with lower extremity ASO.12,13 The therapeutic benefits of exercise are attributed to several physiological adaptations: promoting capillary proliferation and enhancing peripheral circulation; restoring endothelial function and redistributing blood flow more efficiently; boosting mitochondrial efficiency and skeletal muscle oxidative capacity; modulating muscle fiber characteristics to counteract atrophy from inactivity; and suppressing systemic inflammation, potentially slowing or reversing disease progression.14 Supervised exercise programs have been shown to significantly enhance walking performance and overall well-being in these patients,15,16 yet their widespread adoption is hindered by barriers including financial constraints, limited insurance reimbursement, and logistical challenges such as travel difficulties.17 Home-based walking exercise (HB-WE) presents a practical and cost-effective solution, enabling patients to engage in structured, monitored physical activity within their own environment.18 With the national “14th Five-Year Plan” highlighting the need for improved health literacy and chronic illness management, greater emphasis has been placed on optimizing care strategies for lower extremity ASO.19 Recently, there has been a growing shift toward delivering exercise rehabilitation in community or home settings, supported by digital tools that facilitate real-time monitoring and guidance throughout the training process.20
Although the clinical benefits of walking exercise rehabilitation have been well established in current research, a standardized and universally accepted intervention protocol remains lacking. Significant variations exist across studies regarding key parameters such as exercise intensity, duration, monitoring metrics, and safety limits, which complicates direct comparison of findings and restricts widespread clinical implementation. Moreover, patients with lower extremity arteriosclerosis obliterans exhibit considerable heterogeneity. Variables including age, disease progression, coexisting conditions, and overall physical status can greatly influence the suitability and effectiveness of specific exercise regimens. Traditional literature reviews are often insufficient to capture the complexity and individualized requirements inherent in real-world clinical settings. To address these challenges, the Delphi method—an approach grounded in multidisciplinary expert consensus—offers a structured, iterative process characterized by anonymity, controlled feedback, and statistical aggregation of opinions.21 This method enables the integration of practical insights and evidence from specialists in fields such as vascular surgery, rehabilitation medicine, and nursing, thereby reducing individual bias and enhancing the reliability of the resulting recommendations. By leveraging this approach, the study aims to synthesize existing evidence and clinical expertise to develop a robust, evidence-based framework for walking exercise rehabilitation tailored to patients with lower extremity arteriosclerosis obliterans. The ultimate goal is to support functional preservation and promote standardized, effective disease management.
Methods
Design
The Delphi method typically involves conducting multiple rounds of questionnaires with a group of recognized experts. This study was divided into two key phases: (1) the preliminary research phase, in which an evidence-based nursing framework was utilized to develop a draft version of the walking exercise rehabilitation program for patients with lower extremity arteriosclerosis obliterans, while referencing the “Expert Consensus on Chinese Exercise Prescription (2023)”;22 (2) the Delphi expert consultation phase, during which a Delphi questionnaire was designed based on the initial draft and underwent two rounds of surveys to achieve consensus among experts. The study followed the recommendations outlined in the Consensus on Reporting of Delphi Studies (CREDES)23 (see Supplementary Table 1), Figure 1 presents the flowchart of the Delphi process.
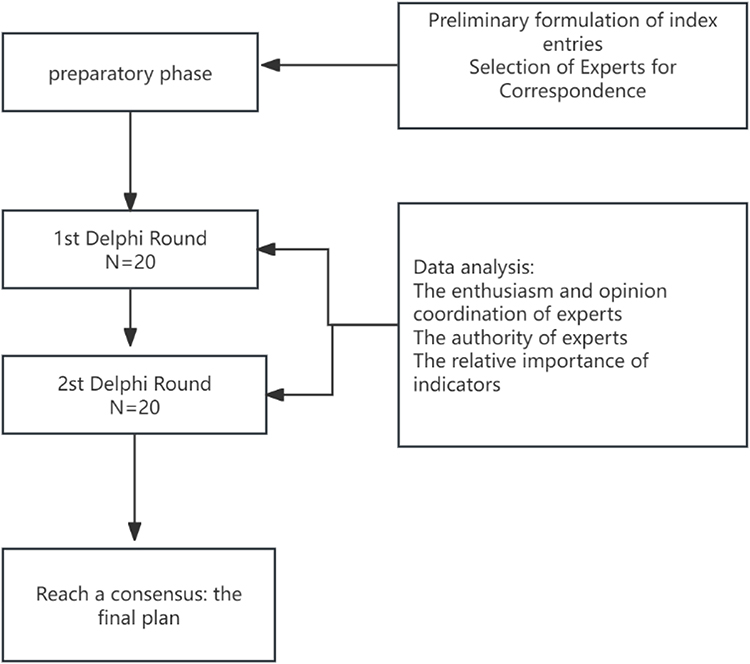 |
Figure 1 Flow chart of Delphi process to reach consensus. |
The Formulation of the Initial Draft of the Walking Training Program for Patients with ASO of the Lower Extremities
This Delphi study was undertaken to develop a standardized nursing care protocol for walking-based rehabilitation in patients with lower extremity ASO. The initial pool of candidate items was derived from a comprehensive evidence synthesis on the topic (see Supplementary Table 2), which systematically evaluated one clinical guideline, one expert consensus document, one randomized controlled trial, and twelve systematic reviews, resulting in the identification of 35 core evidence-based statements. The methodological quality of the synthesis was appraised using the JBI Levels of Evidence and Grades of Recommendation (2014) framework,24 yielding an overall assessment of “moderate” quality. A detailed account of the methodology and findings will be published in the forthcoming manuscript. These 35 evidence-derived statements were subsequently integrated with the “Chinese Expert Consensus on Exercise Prescription (2023)” to formulate a final set of 38 candidate items for inclusion in the Delphi questionnaire.22 To enhance content validity and clarity, a pre-round consultation was conducted with five domain experts, including specialists in vascular surgery and sports rehabilitation. Feedback focused on clarifying ambiguous terminology, merging overlapping items, and refining the scoring framework. Following iterative revisions based on expert input, all 38 items were retained, as they demonstrated strong conceptual alignment with the core objectives of walking rehabilitation in lower extremity ASO patients, thereby supporting advancement to the formal Delphi consensus rounds (see Supplementary Figure 1).
Delphi Process
Establish a Research Group
The research team comprises 10 members, including a doctoral-level nursing specialist, the head of the vascular surgery department, five senior nurses holding associate senior professional titles with expertise in vascular surgery, and three graduate students majoring in nursing. The team is responsible for the selection of consulting experts, development of the questionnaire, data collection and analysis, as well as the synthesis and feedback of expert opinions and recommendations.
Expert Selection Procedure
This study utilized purposive sampling to systematically identify and recruit experts, ensuring the expert panel exhibited strong professional expertise, broad representativeness, and multidisciplinary diversity. The selection process was conducted in four sequential phases, as described below.
Phase 1: Establishment of Selection Criteria
Prior to candidate identification, a comprehensive and multi-dimensional expert selection framework was developed based on the research focus—“Exercise Interventions for Lower Extremity Arteriosclerosis Obliterans”. Inclusion criteria were established as follows: (1) Professional qualifications: possession of an associate senior title or higher, or a doctoral degree with at least five years of research experience in vascular surgery or exercise rehabilitation; (2) Academic and practical background: publication of no fewer than three SCI/SSCI-indexed articles as first or corresponding author in the relevant field within the past five years, or participation in provincial- or national-level research projects related to exercise-based rehabilitation for lower extremity arteriosclerosis obliterans; (3) Clinical or professional engagement: documented involvement in the development of clinical guidelines, industry standards, or academic consensus documents relevant to the topic; (4) Commitment to participation: demonstrated willingness and capacity to complete all rounds of the Delphi consultation process and provide timely, constructive feedback. Exclusion criteria included potential conflicts of interest with the research team or inability to commit to full participation throughout the consultation period.
Phase 2: Development of the Preliminary Candidate Pool
To ensure heterogeneity and reduce selection bias, the initial candidate pool was constructed through three complementary strategies. First, corresponding authors of the top 20% most-cited publications in the target area over the past five years were identified through systematic searches in PubMed, Web of Science, and CNKI. Second, experienced clinicians were nominated by the Vascular Surgery Committee of the Provincial Medical Association based on their clinical leadership and expertise. Third, researchers with prior collaboration in related studies were included to leverage existing academic networks. This approach resulted in a preliminary pool of 51 eligible candidates.
Phase 3: Two-Stage Screening and Validation
The screening process comprised two stages. The first stage—eligibility review—included independent assessment by members of the research team, who evaluated each candidate’s academic credentials, professional titles, publication history, and research project involvement using verified institutional records and authoritative academic databases. Candidates who did not meet the inclusion criteria were excluded, yielding a refined list of 38 qualified individuals. The second stage—representativeness optimization—included categorization of the remaining candidates by primary professional domain (clinical practice, academic research, or health policy/industry management) and geographic region. Proportions were adjusted to achieve balanced representation: 50% clinical practitioners, 30% academic researchers, and 20% professionals in policy or industry roles, thereby ensuring diverse stakeholder perspectives. Inter-rater reliability was assessed using the Kappa statistic, which yielded a value of 0.81, indicating substantial agreement among evaluators.
Phase 4: Formal Invitation and Final Confirmation
Formal invitations were distributed via Email to the 38 shortlisted candidates. Each invitation package included the research protocol, detailed consultation procedures, and an informed consent form, clearly outlining the study objectives, participant rights and responsibilities, and confidentiality measures to safeguard the anonymity of responses. Following a one-week response period, 20 experts provided written confirmation of participation, constituting the final expert panel. All members remained actively engaged throughout the consultation process with no attrition, ensuring methodological consistency, data integrity, and robustness of the expert consensus outcomes.
Formulate a Letter of Inquiry and Questionnaire
Building upon the preliminary draft, the research team developed a structured questionnaire to evaluate the walking exercise program for patients with lower extremity ASO. The instrument consists of five principal sections: an introductory overview, expert demographic and professional background information, assessment of the importance of each indicator, evaluation of experts’ familiarity with the subject matter, and a rationale section for justifying individual ratings. The significance of each indicator was assessed using a 5-point Likert scale, ranging from 1 (“very unimportant”) to 5 (“very important”).25 Additionally, an open-ended feedback section was incorporated to enable specialists to provide suggestions for refinement and improvement.
Conducting Delphi Surveys
This study implemented a two-round Delphi method to systematically gather and refine expert opinions through the use of anonymous questionnaires. To preserve the independence and objectivity of individual responses, experts remained unidentified to one another, and direct interaction among participants was prohibited; all communication was facilitated exclusively through the research team. Following the acquisition of formal informed consent from each expert, the questionnaires were distributed electronically via email. After dissemination, the principal investigator conducted personalized follow-up communications with each participant to clarify the study objectives, provide comprehensive instructions for questionnaire completion, and resolve any uncertainties regarding specific items. Experts were requested to return their completed evaluations by Email within a two-week period. The retention of candidate indicators in both rounds was determined according to predefined consensus criteria: a mean importance rating of at least 4.0 on a 5-point Likert scale,25 a coefficient of variation below 0.25, and agreement from no less than 75% of the expert panel.26,27 To prevent the premature or unjustified removal of potentially significant indicators, any item meeting the statistical criteria for exclusion underwent a rigorous internal evaluation by the research team. Final exclusion was permitted only upon collective judgment confirming that the indicator had no substantive relevance to the core objectives of walking exercise programs for patients with lower extremity arteriosclerosis obliterans.
Data Analysis
Data analysis was carried out using Excel 2013 and SPSS version 26.0. Continuous variables are presented as mean ± standard deviation, whereas categorical variables are summarized as frequencies and percentages. Expert participation was assessed based on the questionnaire response rate, and expert authority was quantified using the authority coefficient (Cr), calculated as Cr = (Cs + Ca) / 2, where Cs denotes the degree of familiarity with the subject matter and Ca represents the rationale underlying expert judgment.28 A Cr value of ≥0.70 was considered to reflect adequate reliability, thereby ensuring the trustworthiness and consistency of the expert consultation results and establishing a solid foundation for the development of the evaluation framework.28 The level of agreement among experts was examined through Kendall’s coefficient of concordance (W), which ranges from 0 to 1, with values approaching 1 indicating higher levels of consensus. Statistical significance was defined as p < 0.05. This statistical result confirms substantial agreement within the expert panel regarding the selected indicators, thus strengthening the construct validity of the indicator system. In this study, only indicators that achieved a mean score of at least 4 from a minimum of 75% of the participating experts were included in the final framework.
Result
Results of Expert Consultation Letters
Basic Information of the Expert
A panel of twenty experts was recruited from ten provinces and municipalities directly under the jurisdiction of China’s Central Government, including Shanxi, Beijing, Chongqing, Henan, Fujian, Heilongjiang, Inner Mongolia, Hebei, Shandong, and Hubei. The experts’ ages ranged from 35 to 57 years, with a mean age of 45.15 ± 6.24 years. Their professional experience in vascular surgery or sports rehabilitation varied between 15 and 37 years, with a mean of 23.75 ± 8.61 years. The expert panel comprised 3 medical specialists, 5 sports rehabilitation specialists, and 12 nursing specialists. With regard to professional titles, 18 held associate senior or full senior titles, while 2 held intermediate-level titles. Detailed demographic characteristics of the participants are presented in Table 1.
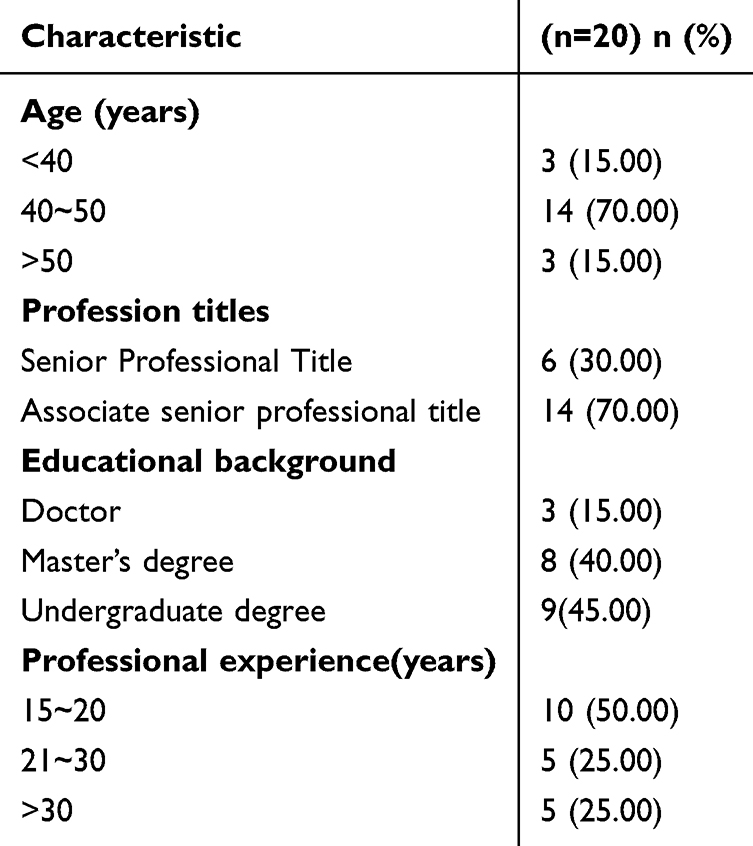 |
Table 1 General Information of Experts in Two Rounds of Consultation |
Degree of Expert Activism and Expert Authority
Two rounds of questionnaire surveys were administered, with 20 questionnaires distributed and fully retrieved in each round, resulting in a 100% effective recovery rate for both rounds. In the first round, 10 experts (50% of the total) offered six suggestions, demonstrating a high level of expert participation and engagement. The authority coefficients for the first round were Cs = 0.92, Ca = 0.915, and Cr = 0.918, whereas in the second round, these values improved to Cs = 0.94, Ca = 0.95, and Cr = 0.945, confirming the consistently strong credibility of the expert panel.
Degree of Harmonization of Expert Advice
In the first round of expert consultation, the coefficient of variation ranged from 0.00 to 0.21, and in the second round, it further narrowed to between 0.00 and 0.10. The Kendall’s coefficient of concordance in the first round was 0.131 (χ2 = 143.628, P < 0.001), and it significantly increased to 0.339 (χ2 = 386.38, P < 0.001) in the second round. These results indicate that the expert opinions were consistent.
Establishment of a Walking Exercise Rehabilitation Program for Patients with ASO of the Lower Extremities
In the initial phase of the Delphi survey, expert panels systematically reviewed the preliminary version of the walking exercise program designed for patients with lower extremity arteriosclerosis obliterans. This assessment covered 5 primary indicators, 13 secondary indicators, and 38 tertiary indicators. A total of 11 expert suggestions were collected during this initial phase. The research team subsequently reviewed and refined these recommendations, as detailed in Table 2. Following these refinements, the questionnaire for the second round of expert consultation was developed. In the subsequent Delphi phase, all project indicators reached consensus under the guidance of predefined criteria. Ultimately, the finalized framework consisted of 5 primary indicators, 13 secondary indicators, and 40 tertiary indicators, as presented in Table 3.
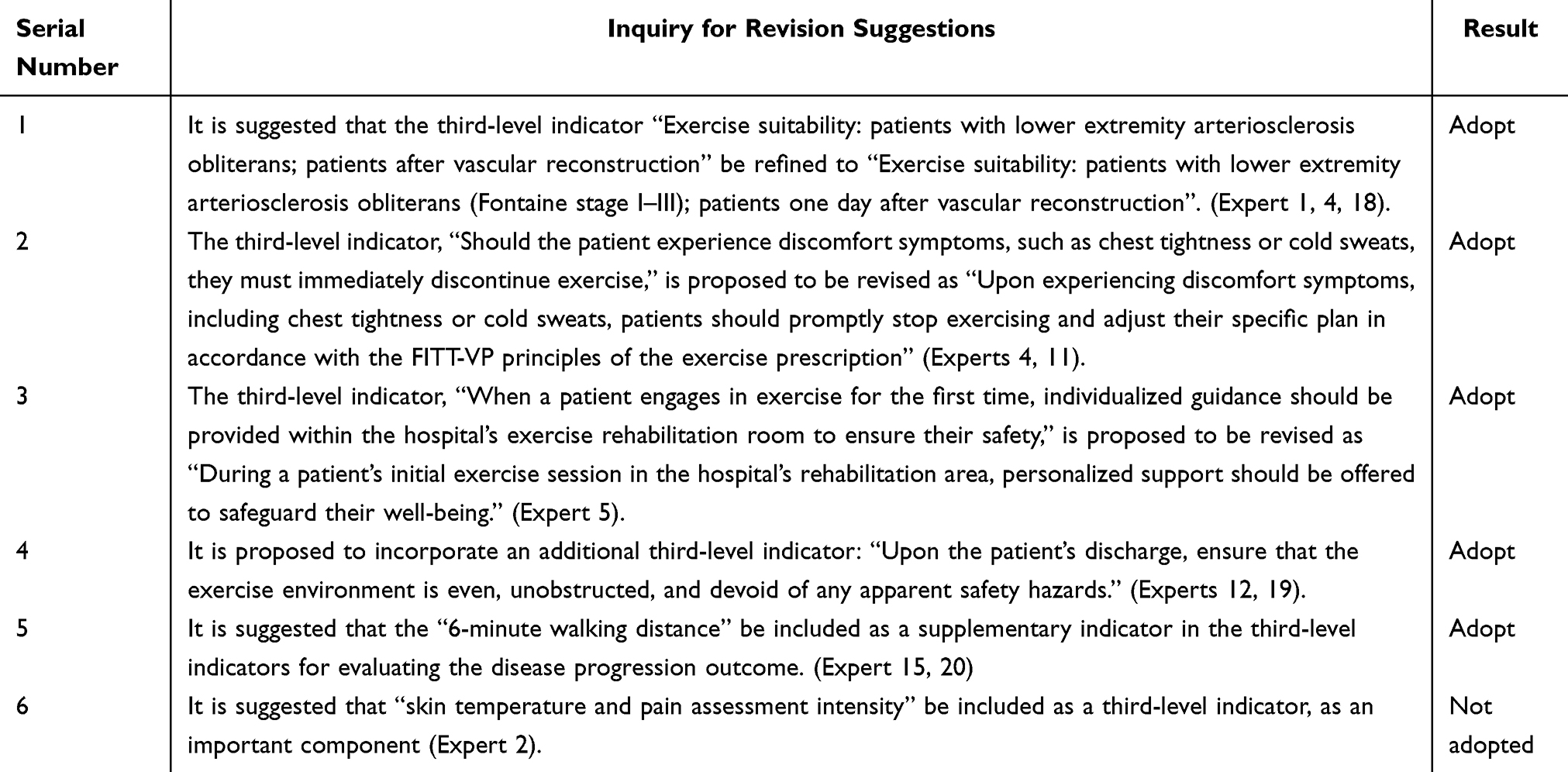 |
Table 2 Modification Suggestions and Discussion Results of the First Round of Expert Consultation |
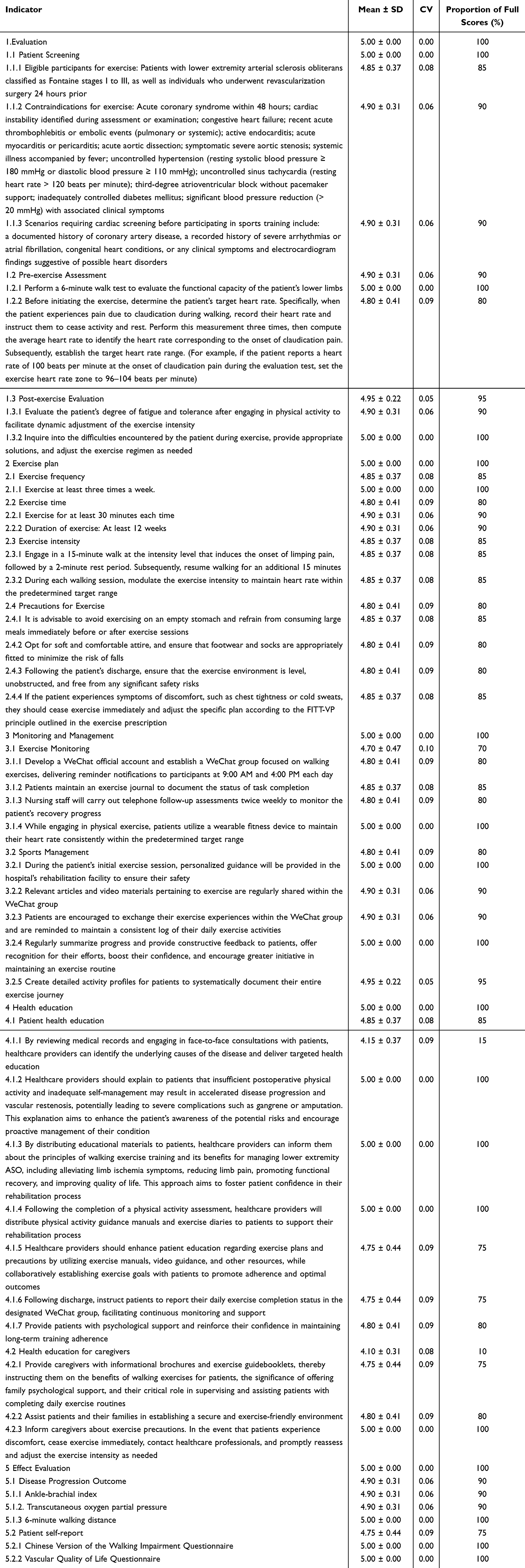 |
Table 3 Walking Exercise Program for Patients with ASO of the Lower Limbs |
Discussion
The Necessity of Constructing a Walking Exercise Rehabilitation Program for Patients with ASO of the Lower Extremities
At present, a substantial number of randomized controlled trials and systematic reviews conducted both domestically and internationally have focused on walking exercise rehabilitation for lower extremity ASO. This underscores the ongoing global interest among medical professionals in this area. However, there remains a lack of consensus regarding the optimal duration, intensity, and frequency of such rehabilitation exercises. A notable trend in exercise therapy for patients with lower extremity ASO is the implementation of community- or home-based exercise training programs, complemented by the use of information technology to monitor the entire exercise process.29 Although significant progress has been made in recent years regarding exercise training recommendations, additional robust scientific evidence is still needed to further optimize and standardize clinical practices.30 Therefore, the development of a well-designed and scientifically grounded walking exercise rehabilitation program is critical for effectively addressing limb dysfunction in patients with lower extremity ASO.
The Walking Exercise Rehabilitation Program for Patients with ASO in the Lower Extremities Is Scientifically Sound and Reliable
From the perspective of expert selection, this study engaged a multidisciplinary panel of professionals representing 10 provinces and municipalities across China, including specialists in vascular surgery, nursing, healthcare management, and scholars in sports rehabilitation. This diverse disciplinary composition effectively minimizes potential biases arising from domain-specific viewpoints and ensures a balanced integration of clinical applicability and rehabilitation expertise within the proposed framework. All participating experts held associate senior or higher professional titles and had an average of over 15 years of practical experience in their respective fields. Their contributions therefore reflect not only extensive frontline clinical experience but also a comprehensive understanding of established diagnostic guidelines and rehabilitation requirements, thereby providing a strong authoritative foundation for the validity of the core components of the protocol. With regard to the consultation process, the 100% response rate achieved in both rounds of the Delphi survey reflects a high level of expert engagement and strong recognition of the research focus—standardizing walking exercise rehabilitation for patients with lower extremity arteriosclerosis obliterans—a critical issue given the current absence of uniform training protocols in clinical practice. The continuous increase in the authority coefficient and the progressive reduction in the coefficient of variation across rounds indicate a trend toward increasing consensus among experts. Initial variations in opinion were systematically addressed through iterative feedback and anonymous revision cycles. Importantly, the significant improvement in Kendall’s coefficient of concordance demonstrates substantial agreement on the importance ratings assigned to each protocol item. This convergence of opinions is not indicative of mere consensus for consensus’ sake, but rather represents a rigorous, evidence-informed judgment derived from careful consideration of key factors such as clinical feasibility, patient safety, and practical implementation. In sum, the resulting walking-based rehabilitation protocol is methodologically robust and offers a reliable basis for future standardization, clinical application, and broader dissemination.
Content Analysis of the Walking Exercise-Based Rehabilitation Program for Patients with Lower Extremity ASO
For patients with lower extremity ASO, systematic assessment before and after walking training is critical to ensuring patient safety and maximizing rehabilitation outcomes. This approach not only adheres to established clinical practice principles but also aligns with the evolving emphasis on precision-based rehabilitation strategies within the lower extremity ASO management domain. Current clinical guidelines recommend that individuals intending to engage in high-intensity physical activity or those identified as having elevated cardiovascular risk should undergo comprehensive cardiovascular risk evaluation prior to initiating any structured exercise program.29 Pre-exercise health and risk assessment entails the integration of multiple clinical and behavioral factors—including habitual physical activity levels, symptom presentation, history of cardiovascular and metabolic comorbidities, and anticipated exercise intensity—enabling a shift away from generalized recommendations toward individualized, evidence-informed care planning.31 This study places particular emphasis on evaluating exercise endurance and determining personalized target heart rate thresholds prior to the initiation of walking therapy, reflecting a commitment to tailored intervention design. Given the variable extent of peripheral vascular involvement among lower extremity ASO patients, inter-individual differences in exercise tolerance are substantial. The use of non-individualized or empirically derived training protocols may lead to adverse events such as intensified claudication symptoms or cardiac rhythm disturbances. By quantitatively assessing aerobic capacity and establishing patient-specific heart rate targets, this method facilitates proactive risk stratification based on objective physiological parameters, thereby reducing the incidence of exercise-related complications. Moreover, in light of ongoing scholarly debate regarding optimal exercise intensity for individuals with lower extremity ASO,32–38 this protocol directly addresses a pivotal clinical challenge: achieving an appropriate balance between therapeutic benefit and patient safety. The primary objective is to improve peripheral perfusion and functional capacity while avoiding undue cardiovascular strain. Existing research indicates that maintaining exercise heart rate within the range corresponding to the onset of claudication pain may enhance walking performance and aerobic endurance.39 To operationalize this principle, the present study implements a standardized procedure in which the target heart rate zone is determined by calculating the mean heart rate recorded at the onset of claudication during three repeated treadmill trials.40 This iterative measurement approach improves data reliability, while constraining the target zone near the claudication threshold ensures adequate training stimulus without exceeding safe physiological limits through controlled intensity regulation. The strong consensus among expert reviewers regarding this component highlights its clinical relevance and practical applicability. It successfully addresses the fundamental challenge of standardizing and quantifying exercise intensity in a manner that is both individualized and reproducible, while reinforcing patient safety through systematic risk assessment. Consequently, this framework provides a robust, scientifically grounded model for the standardized and safe delivery of walking-based rehabilitation programs for patients with lower limb ASO.
This rehabilitation program is founded on the development of tailored guidelines for the timing, frequency, and intensity of walking exercises specifically designed for individuals with lower extremity ASO. The framework adheres to the FITT-VP principle—a well-established model in exercise prescription that encompasses six core components: frequency (F), intensity (I), time (T), type (T), volume (V), and progression (P).29 Based on expert consensus derived from Delphi method consultations, the recommended regimen consists of walking sessions conducted at least three times per week, each lasting a minimum of 30 minutes, with the overall intervention maintained for no less than 12 weeks.41 Walking is designated as the primary mode of physical activity, and exercise intensity is operationally defined by maintaining the patient’s heart rate within a pre-established target range throughout each session.40 Continuous monitoring and quantitative assessment of physiological responses during exercise are essential for optimizing the balance between oxygen supply and metabolic demand in ischemic lower limbs. This approach not only reduces the incidence of intermittent claudication but also supports individualized adjustments through data-informed feedback mechanisms, thereby enhancing patient confidence and adherence. Such a strategy improves clinical feasibility and facilitates the attainment of functional rehabilitation goals. With respect to volume (V) and progression (P), the protocol incorporates an interval-based training structure: patients perform two 15-minute walking bouts at an intensity sufficient to elicit claudication symptoms, separated by a 2-minute rest period.42 Each 15-minute walking segment ensures adequate “moderate ischemic stimulus” within the target heart rate zone while avoiding excessive ischemia accumulation associated with prolonged continuous exertion. The 2-minute recovery interval allows for partial hemodynamic restoration—rebalancing perfusion and tissue oxygen requirements—thereby mitigating pain exacerbation due to sustained ischemia and enabling transient heart rate reduction, which supports the maintenance of target intensity in subsequent exercise phases. From a systematic perspective aligned with the FITT-VP framework, the integration of heart rate–guided intensity control and structured intermittent scheduling addresses two critical dimensions: precision in exercise dosing and controllability of session duration, with both elements reinforcing one another. From a pathophysiological standpoint specific to lower extremity ASO, this dual-component design effectively overcomes the limitations inherent in unidimensional approaches—either relying solely on fixed-intensity continuous exercise or employing non-standardized intermittent patterns without objective metrics. Given the impaired peripheral arterial perfusion characteristic of lower extremity ASO, prolonged exercise without rest may result in intolerable claudication and early termination of training. Conversely, intermittent protocols lacking quantifiable intensity benchmarks risk under- or over-exertion due to variability in subjective perception of symptom onset. In this protocol, the target heart rate serves as a “safe upper threshold” for exercise intensity. For example, if a patient consistently develops claudication at a heart rate of 100 beats per minute during preliminary testing, the prescribed target range is set at 96–104 bpm. During each 15-minute walking phase, real-time heart rate monitoring ensures that exercise intensity remains within this individualized window, achieving the therapeutic aim of controlled ischemic conditioning. The intervening rest period permits partial cardiovascular recovery, alleviating ischemic discomfort and minimizing symptom accumulation. This “dynamic regulation with periodic recovery” paradigm closely mirrors the physiological cycle of “ischemia-reperfusion” observed in lower extremity ASO, effectively reducing claudication-related risks while promoting adaptive vascular and muscular responses. From a clinical implementation perspective, the combination of quantifiable intensity parameters and standardized temporal structure enhances both the objectivity and reproducibility of the intervention, thereby improving patient compliance and scalability across diverse care settings. For healthcare professionals, the target heart rate provides a clear, evidence-based metric for supervision, while the fixed interval format offers a consistent and easily communicable training rhythm. Particularly in community or home-based rehabilitation contexts, clinicians can rapidly train patients using a straightforward protocol: “target heart rate range + fixed work-rest cycle.” For patients, user-friendly wearable devices such as wrist-worn monitors or chest strap heart rate sensors enable real-time self-monitoring,29,39 while the predictable structure of the interval schedule supports autonomous regulation of exercise pace, reducing anxiety related to uncertainty about appropriate effort levels or fear of pain. Collectively, these features address the persistent challenge of “subjective intensity estimation” in lower extremity ASO rehabilitation and reduce implementation barriers, providing robust support for the standardized, scalable delivery of supervised exercise therapy.
The monitoring of walking activities in patients with lower limb arterial stenosis or occlusion constitutes a critical component of their rehabilitation management. A growing body of evidence from recent clinical studies demonstrates that wearable device–based activity monitoring significantly improves ambulatory function in individuals diagnosed with lower extremity ASO.43–47 With regard to monitoring instrumentation, the research team recommends the use of wearable fitness trackers during walking exercises to ensure that heart rate remains within a clinically defined target range. This approach has been rigorously evaluated through expert consultation and has received strong consensus regarding its clinical feasibility and therapeutic relevance. In addition, structured health education delivered throughout the intervention period plays a pivotal role in fostering patient adherence. To enhance compliance, the program integrates a multifaceted support system, including visually enhanced educational materials, video-based instructional modules, and facilitated peer experience sharing. Patients receive regular, individualized feedback on their progress, supplemented by motivational reinforcement. Educational content also addresses the potential adverse consequences of physical inactivity, while caregivers are provided with evidence-based strategies to assist patients in maintaining consistent exercise adherence.48 The program synergistically combines digital health technologies—such as WeChat group communication and real-time smart wristband monitoring—with established traditional modalities, including printed educational handouts and telephone follow-ups. This integrated, multimodal framework ensures both methodological rigor and practical accessibility, rendering it highly appropriate for long-term outpatient and home-based rehabilitation. Future refinements may involve the incorporation of automated exercise data logging and multilingual educational resources to further improve scalability and inclusivity.
The findings of the walking exercise rehabilitation program developed for patients with lower extremity atherosclerotic occlusive disease reveal that expert agreement on two health education-related indicators (4.1.1 and 4.2) is notably lower compared to other evaluation criteria. This outcome reflects experts’ cautious assessment of the practicality of these specific interventions and highlights a critical area for refining clinical strategies in walking rehabilitation education. Specifically, regarding indicator 4.1.1—face-to-face health education—the low level of consensus stems largely from challenges tied to the real-world context in which walking exercises are performed. As walking serves as the central intervention in this program and requires long-term adherence for optimal results, its effectiveness hinges on consistent implementation. However, most patients carry out their walking routines at home, creating logistical barriers for traditional face-to-face education models. Healthcare providers would need substantial time and personnel to conduct regular in-person follow-ups, yet limited medical resources and patients’ geographically dispersed locations make sustained personal contact impractical. In contrast, digital tools such as instant messaging via WeChat groups or feedback from wearable fitness trackers offer greater immediacy and convenience, making them more adaptable to daily life. Consequently, experts question the sustainability and efficiency of relying solely on direct consultations. Similarly, the low rating for indicator 4.2—family-based health education—arises from inherent limitations in family members’ capacity to engage effectively. Caregivers often juggle multiple roles involving employment, household responsibilities, and patient care, leaving little room for consistent involvement in structured rehabilitation activities. This constraint undermines the reliability of family-led support in home-based walking programs. Additionally, some relatives may lack sufficient awareness or hold misconceptions about the importance and methods of walking rehabilitation, further diminishing confidence among experts in the feasibility of this approach. It is important to emphasize that the reduced expert endorsement of these two indicators does not imply a rejection of their potential clinical benefits; rather, it underscores a misalignment between conventional educational approaches and the actual conditions under which patients perform rehabilitation. To address this gap, the current study enhances the traditional model by incorporating digital innovations into a comprehensive, multi-channel health education framework: “smart monitoring + online guidance + telephone follow-up + printed materials.” This hybrid system leverages WeChat platforms to enable continuous interaction between healthcare professionals and patients, allowing timely responses to exercise-related inquiries and partially substituting in-person visits. Data from wearable devices, particularly heart rate monitoring, inform tailored guidance based on individual performance. Meanwhile, telephone check-ins and physical handouts are retained to ensure inclusivity for older adults and individuals with limited digital proficiency. By combining these modalities, the proposed strategy overcomes the shortcomings of isolated face-to-face or family-centered education while accommodating diverse patient needs, thereby enhancing both the reach and impact of health education in clinical practice.
This study developed a walking rehabilitation program for patients with lower extremity arteriosclerosis obliterans by incorporating WeChat-based platforms and wearable fitness trackers, thereby improving the timeliness and precision of intervention delivery. Despite these advancements, several challenges are associated with the use of digital technologies. Most individuals suffering from this condition are older adults, many of whom possess limited familiarity with digital tools, making it difficult to operate wearable devices, interpret collected data, or navigate WeChat features. Additionally, the financial cost of acquiring such devices may create economic strain for certain patients, potentially limiting broad access and practical implementation across diverse populations. To address these barriers, the study deliberately avoided overreliance on technology alone. Instead, it implemented a comprehensive, multi-modal intervention framework combining “smart monitoring, online support, telephone follow-ups, and printed instructional materials.” For elderly participants or those less comfortable with digital interfaces, personalized phone calls were conducted to assist with device usage and clarify exercise procedures in a timely manner. A visually oriented, illustrated paper manual was also provided, detailing key aspects such as exercise duration, intensity levels, and safety guidelines, enabling patients to easily reference instructions independently. By integrating digital innovation with conventional approaches, this hybrid model capitalizes on the efficiency of modern tools while ensuring inclusivity through low-tech alternatives, thus enhancing overall accessibility and ensuring equitable benefits across varied patient demographics.
The evaluation phase incorporates a combination of objective measures, including the ankle-brachial index (ABI), the 6-minute walk test (6MWT), and transcutaneous oxygen partial pressure (TcPO2), as well as subjective assessment tools such as the Walking Impairment Questionnaire (WIQ) and the VascuQoL. Following expert consultation, all these metrics received relatively high importance scores. The ABI quantitatively assesses lower extremity blood flow restriction by comparing the systolic pressures of the ankle and brachial arteries. It is notable for its non-invasive nature, repeatability, and strong correlation with angiography results.49,50 TcPO2 reflects tissue oxygen metabolism and can sensitively detect minor changes in blood flow, making it especially valuable for evaluating ischemic compensation and predicting outcomes.51 The 6MWT directly quantifies a patient’s functional walking capacity over six minutes, with results demonstrating a significant inverse relationship to the Fontaine clinical staging.46 For subjective assessments, the Chinese-adapted WIQ and the VascuQoL were selected due to their cross-cultural validation.52,53 These tools systematically evaluate multidimensional health aspects, such as pain, walking ability, and social functioning, thereby addressing the limitations of purely biomedical indicators and aligning with international standards for vascular disease evaluation.
Limitations and Future Directions
The rehabilitation monitoring program developed for patients with lower limb arterial stenosis or occlusion, although systematically structured through clearly defined modules and validated by expert consensus, is subject to several notable limitations. First, it has not yet undergone rigorous clinical validation; the current rationale is largely based on theoretical foundations and expert opinion, with limited evidence regarding its applicability to high-risk or complex patient populations, including older adults, individuals with advanced claudication, and those with multiple comorbidities. Second, critical components related to implementation—such as the technical reliability of wearable monitoring devices and the procedural fidelity of intervention elements like health education delivery—have not been empirically tested in real-world settings. To address these gaps, the next phase of research will focus on evaluating the program’s effectiveness through a randomized controlled trial (RCT). This study will adopt a multicenter design, enrolling a diverse cohort of patients representing varying disease severities and comorbidity burdens, and will compare outcomes between the intervention group and those receiving standard care. Primary outcome measures will include changes in walking capacity, exercise-related safety, and treatment adherence, with the aim of generating robust clinical evidence to support the program’s broader adoption and integration into routine vascular rehabilitation practice.
Conclusion
This study designed a structured walking exercise rehabilitation program for patients with lower extremity arteriosclerosis obliterans by integrating evidence-based methodologies and the Delphi technique. The program encompasses five core components: patient screening, pre- and post-exercise evaluation, exercise monitoring, exercise management, health education, as well as disease progression outcomes and patient self-reporting. These elements collectively address 13 critical dimensions and provide 40 detailed recommendations. It comprehensively covers the entire process of walking exercise rehabilitation for ASO patients in the lower extremities. The program is meticulously developed, highly practical, and operationally feasible, serving as a robust and scientifically grounded framework for vascular surgery nurses to implement exercise interventions for lower extremity ASO patients. Future efforts will concentrate on applying this program in clinical practice to assess its efficacy and validity.
Abbreviations
ASO, arteriosclerosis obliterans; HB-WE, home-based walking exercise training; JBI, Joanna Briggs Institute; CNKI, China National Knowledge Infrastructure; FITT-VP, frequency, intensity, duration, type, volume, and progression.; RCT, Randomized Controlled Trial; ABI, Ankle-Brachial Index; WIQ, Walking Impairment Questionnaire; 6MWT, 6-Minute Walk Test; TcPO2, transcutaneous oxygen partial pressure; VascuQoL, the Vascular Quality of Life Questionnaire.
Data Sharing Statement
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Ethical Approval and Consent
This study was approved by the Medical Ethics Committee of Shanxi Bethune Hospital (Ethics Approval Code: YXLL-2025-030) and adheres to the ethical principles set forth in the Declaration of Helsinki. Furthermore, all experts who participated in this study signed written informed consent forms.
Acknowledgments
The authors would like to extend their sincere gratitude to all consulting experts for their valuable contributions, active involvement, and steadfast support throughout this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the 2024 Annual Nursing Research Fund Project of Shanxi Bethune Hospital (Grant Number: 2024YH10). The funder had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dake MD, Fanelli F, Lottes AE, et al. Prediction model for freedom from TLR from a multi-study analysis of long-term results with the Zilver PTX drug-eluting peripheral stent. Cardiovasc Intervent Radiol. 2021;44.
2. Mazzolai L, Belch J, Venermo M, et al. Exercise therapy for chronic symptomatic peripheral artery disease. Eur Heart J. 2024;45:1303–16. doi:10.1093/eurheartj/ehad734
3. Bonaca MP, Nault P, Giugliano RP, et al. Low-density lipoprotein cholesterol lowering with evolocumab and outcomes in patients with peripheral artery disease: insights from the fourier trial (Further cardiovascular outcomes research with PCSK9 inhibition in subjects with elevated risk). Circulation. 2018;137:338–350. doi:10.1161/CIRCULATIONAHA.117.032235
4. Chinese Cardiovascular Health and Disease Report Writing Group. Summary of the Chinese Cardiovascular Health and Disease Report 2020. Chinese J Cardiol. 2021;36:521–545.
5. Poorthuis MH, Sherliker P, Morris DR, et al. Development and internal validation of a risk score to detect asymptomatic carotid stenosis. Eur J Vasc Endovasc Surg. 2021;61.
6. Megaly M, Abraham B, Saad M, et al. Outcomes with cilostazol after endovascular therapy of peripheral artery disease. Vasc Med. 2019;24:313–323. doi:10.1177/1358863X19838327
7. Campia U, Gerhard-Herman M, Piazza G, Goldhaber SZ. Peripheral artery disease: past, present, and future. Am J Med. 2019;132:132. doi:10.1016/j.amjmed.2018.07.031
8. Polonsky TS, McDermott MM. Lower extremity peripheral artery disease without chronic limb-threatening ischemia: a review. JAMA. 2021;325:2188–2198. doi:10.1001/jama.2021.2126
9. Ingwersen M, Kunstmann I, Oswald C, Best N, Weisser B, Teichgräber U. Exercise training for patients with peripheral arterial occlusive disease. Dtsch Arztebl Int. 2023;120:879–885. doi:10.3238/arztebl.m2023.0231
10. Abaraogu UO, Abaraogu OD, Dall PM, et al. Exercise therapy in routine management of peripheral arterial disease and intermittent claudication: a scoping review. Ther Adv Cardiovasc Dis. 2020;14:1753944720924270. doi:10.1177/1753944720924270
11. Cornelis N, Buys R, Dewit T, et al. Satisfaction and acceptability of telemonitored home-based exercise in patients with intermittent claudication: pragmatic observational pilot study. JMIR Rehabil Assist Technol. 2021;8:e18739. doi:10.2196/18739
12. Mazzolai L, Bäck M, Belch J, Venermo M. The benefits of exercise in patients with peripheral arterial disease are far too great to be ignored! Vasa. 2023;52:212–213. doi:10.1024/0301-1526/a001077
13. Fassora M, Calanca L, Jaques C, Mazzolai L, Kayser B, Lanzi S. Intensity-dependent effects of exercise therapy on walking performance and aerobic fitness in symptomatic patients with lower-extremity peripheral artery disease: a systematic review and meta-analysis. Vasc Med. 2022;27:158–170. doi:10.1177/1358863X211034577
14. Osinbowale OO, Milani RV. Benefits of exercise therapy in peripheral arterial disease. Prog Cardiovasc Dis. 2011;53:447–453. doi:10.1016/j.pcad.2011.03.005
15. Treat-Jacobson D, McDermott MM, Bronas UG, et al. Optimal exercise programs for patients with peripheral artery disease: a scientific statement from the American Heart Association. Circulation. 2019;139:e10–33. doi:10.1161/CIR.0000000000000623
16. Harwood AE, Pymer S, Ingle L, et al. Exercise training for intermittent claudication: a narrative review and summary of guidelines for practitioners. BMJ Open Sport Exerc Med. 2020;6e000897.
17. Quan X, Song P, Wang D, Xiong H, Zhang M, Shi M. Meta-analysis of the effects of home-based walking exercise on walking ability and quality of life in patients with lower extremity arteriosclerosis obliterans. Geriatric Med Res. 2023;4:14–23.
18. Sandberg A, Bäck M, Cider Å, et al. Effectiveness of supervised exercise, home-based exercise, or walk advice strategies on walking performance and muscle endurance in patients with intermittent claudication (SUNFIT trial): a randomized clinical trial. Eur J Cardiovasc Nurs. 2023;22:400–411. doi:10.1093/eurjcn/zvac070
19. Zhu L, Xu Y, Wang X, et al. New developmental ideas for the “four-in-one” prevention, treatment, and management of venous thromboembolism: the value of caregivers. Chin J Modern Nurs. 2021;27:421–424.
20. Zhang T, Tang W, Guo J. Research progress on the application of exercise training under professional guidance and its modification in patients with peripheral artery disease. J Intervent Radiol. 2022;31:927–931.
21. Nasa P, Jain R, Juneja D. Delphi methodology in healthcare research: how to decide its appropriateness. World J Methodol. 2021;11(4):116–129. PMID: 34322364; PMCID: PMC8299905. doi:10.5662/wjm.v11.i4.116
22. Expert Group of “Chinese Expert Consensus on Exercise Prescription (2023)”. Chinese Expert Consensus on Exercise Prescription (2023). Chin J Sports Med. 2023;42:3–13.
23. Jünger S, Payne SA, Brine J, Radbruch L, Brearley SG. Guidance on conducting and REporting DElphi Studies (CREDES) in palliative care: recommendations based on a methodological systematic review. Palliat Med. 2017;31:684–706. doi:10.1177/0269216317690685
24. Wang C, Hu Y. JBI evidence pre-grading and evidence recommendation level system (2014 Edition). J Nurs. 2015;964–967.
25. Yang L, Wang Y. Application of a peer learning and assessment model in an undergraduate pharmacy course. BMC Med Educ. 2023;23:362. doi:10.1186/s12909-023-04352-8
26. Ge H, Wang Q, Liu S, Tian Y, Ma J. Development and validation of an indicator system for evaluating clinical nursing process quality using mobile nursing information systems. J Multidiscip Healthc. 2025;18:2225–2236. doi:10.2147/JMDH.S512781
27. Rico V, Zelinsky M, Ford PJ, et al. Recommended approaches to sharing individual research results in Alzheimer’s disease research: a multidisciplinary expert Delphi consensus. J Alzheimers Dis. 2025;108:703–718. doi:10.1177/13872877251379076
28. Liu J, Qiu H, Zhang X, Zhang C, He F, Yan P. Development of billing post competency evaluation index system for nurses in China: a Delphi study. BMC Nurs. 2023;22:136. doi:10.1186/s12912-023-01301-0
29. Thangada ND, Zhang D, Zhao L, Tian L, McDermott MM. Safety and efficacy of home-based walking exercise for peripheral artery disease. J Vasc Surg. 2025;81:441–449.e1. doi:10.1016/j.jvs.2024.10.013
30. Aaij AGL, Wermelink B, Haalboom M, Vahl AC, Meerwaldt R, Geelkerken RH. Real world practice deviation from nationwide guidelines in patients with intermittent claudication. Eur J Vasc Endovasc Surg. 2021;62:432–438. doi:10.1016/j.ejvs.2021.05.001
31. Ravindhran B, Prosser J, Lim A, et al. Tailored risk assessment and forecasting in intermittent claudication. BJS Open. 2024;8:zrad166. doi:10.1093/bjsopen/zrad166
32. Lanzi S. From bed rest to never-ending walk: highlighting the importance of exercise training in patients with peripheral artery disease. Eur J Prev Cardiol. 2024;31:378–379. doi:10.1093/eurjpc/zwad303
33. Seed SA, Harwood AE, Sinclair J, et al. A systematic review of exercise prescription in patients with intermittent claudication: does pain matter? Ann Vasc Surg. 2021;77:315–323. doi:10.1016/j.avsg.2021.06.025
34. Manfredini F, Lamberti N, Traina L, et al. Effectiveness of home-based pain-free exercise versus walking advice in patients with peripheral artery disease: a randomized controlled trial. Methods Protoc. 2021;4:29. doi:10.3390/mps4020029
35. McDermott MM, Spring B, Tian L, et al. Effect of low-intensity vs high-intensity home-based walking exercise on walk distance in patients with peripheral artery disease: the LITE randomized clinical trial. JAMA. 2021;325:1266–1276.
36. Sieland J, Niederer D, Engeroff T, et al. Changes in miRNA expression in patients with peripheral arterial vascular disease during moderate- and vigorous-intensity physical activity. Eur J Appl Physiol. 2023;123:645–654.
37. Yang Q, Zhao Y, Huang Y, et al. Best evidence summary of exercise training for patients with peripheral artery disease. Chin J Nurs. 2022;57:2661–2668.
38. Li C, Du L, Xue X, et al. Associations of daily steps and step intensity with peripheral arterial disease in Chinese community-dwelling older women. Exp Gerontol. 2025;201:112706. doi:10.1016/j.exger.2025.112706
39. Thanigaimani S, Jin H, Silva MT, Golledge J. Network meta-analysis of trials testing if home exercise programs informed by wearables measuring activity improve peripheral artery disease related walking impairment. Sensors. 2022;22:8070. doi:10.3390/s22208070
40. Cucato GG, Chehuen MR, Costa LAR, et al. Exercise prescription using the heart of claudication pain onset in patients with intermittent claudication. Clinics. 2013;68:974–978. doi:10.6061/clinics/2013(07)14
41. Mazzolai L, Belch J, Venermo M, et al. Exercise therapy for chronic symptomatic peripheral artery disease: a clinical consensus document of the European Society of Cardiology Working Group on Aorta and Peripheral Vascular Diseases in Collaboration With the European Society of Vascular Medicine and the European Society for Vascular Surgery. Eur J Vasc Endovasc Surg. 2024;16:
42. Yasu T. Comprehensive cardiac rehabilitation program for peripheral arterial diseases. J Cardiol. 2022;80:303–305. doi:10.1016/j.jjcc.2021.11.011
43. de Müllenheim P-Y, Abraham P, Noury-Desvaux B. Use of a wearable activity monitor in a home-based exercise intervention for peripheral artery disease. JAMA. 2018;320:1285–1286. doi:10.1001/jama.2018.10771
44. Chan C, Sounderajah V, Normahani P, et al. Wearable activity monitors in home based exercise therapy for patients with intermittent claudication: a systematic review. Eur J Vasc Endovascular Surg. 2021;61:676–687. doi:10.1016/j.ejvs.2020.11.044
45. Veiga C, Pedras S, Oliveira R, Paredes H, Silva I. A systematic review on smartphone use for activity monitoring during exercise therapy in intermittent claudication. J Vasc Surg. 2022;76(1734):1734–1741. doi:10.1016/j.jvs.2022.04.045
46. Wiesmüller F, Prenner A, Ziegl A, et al. Support of home-based structured walking training and prediction of the 6-minute walk test distance in patients with peripheral arterial disease Based on telehealth data: prospective cohort study. JMIR Form Res. 2025;9e65721.
47. Herrero-Alonso C, López-Lifante V-M, Costa-Garrido A, et al. Adherence to supervised and unsupervised exercise programmes in ageing population with intermittent claudication: a randomized controlled trial. J Clin Med. 2024;13:3690. doi:10.3390/jcm13133690
48. Cleary CM, Adajian A, Gifford ED, et al. Incentives and individualized coaching improve completion rates of supervised exercise therapy for claudication. J Vasc Surg. 2024;80:821–830.e3. doi:10.1016/j.jvs.2024.04.055
49. Huang H-L, Chang C-H, Lo M-T, Lin C. Diagnostic potential of combined photoplethysmography and ankle-brachial index in peripheral arterial disease: a duplex ultrasonography-based comparative study. J Am Heart Assoc. 2024;13:e034625. doi:10.1161/JAHA.124.034625
50. Memarian E, Hamrefors V, Kharraziha I, et al. Associations between physical activity and ankle-brachial index: the Swedish CArdioPulmonary bioImage Study (SCAPIS). BMC Cardiovasc Disord. 2024;24:459. doi:10.1186/s12872-024-04137-x
51. Braet DJ, Pourak K, Delbono L, et al. Comparative evaluation of transcutaneous oxygen tension and ankle-brachial index as predictors of reoperation following below-knee amputation. J Vasc Surg. 2024;80:223–231.e2. doi:10.1016/j.jvs.2024.02.031
52. Inácio MCG, Karsten M, Santos LCA, Oliveira RDB, Pereira DAG. Diagnostic test accuracy of the walking impairment questionnaire in individuals with intermittent claudication. Vasa. 2025;54:253–258. doi:10.1024/0301-1526/a001190
53. Oliveira R, Pedras S, Pimenta R, Silva I. Contributions for the validation of the european portuguese version of the vascular quality of Life-6 questionnaire for peripheral artery disease. Acta Med Port. 2024;37:436–444. doi:10.20344/amp.20760
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.