Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Multidisciplinary Collaborative Nursing Management Improves Health Behaviors and Psychological Status in Patients with Diabetes Mellitus and Coronary Heart Disease
Received 15 October 2025
Accepted for publication 8 January 2026
Published 19 January 2026 Volume 2026:19 574565
DOI https://doi.org/10.2147/JMDH.S574565
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Qingwen Liu,1 Zeyin Li2
1Department of Geratology, the First Affiliated Hospital of China Medical University, Shenyang, 110001, People’s Republic of China; 2Department of Cardiac Surgery, the First Affiliated Hospital of China Medical University, Shenyang, 110001, People’s Republic of China
Correspondence: Zeyin Li, Email [email protected]
Objective: To evaluate the effectiveness of a multidisciplinary collaborative nursing management model in patients with diabetes mellitus and coronary heart disease, focusing on blood glucose control, cardiac function, psychological adjustment, and health-promoting behaviors.
Methods: A retrospective controlled study was conducted including 150 patients admitted from April 2022 to April 2025. Patients were divided into a control group (n=75, routine nursing) and an observation group (n=75, multidisciplinary collaborative nursing). Outcomes included blood glucose [fasting plasma glucose (FPG), 2-hour postprandial glucose (2 h PG), HbA1c], cardiac function [LVEF, LVESD, LVEDD], psychological status [SAS, SDS], health behaviors [HPLP-II], and nursing satisfaction [NSNS].
Results: After intervention, both groups showed improvements in all outcomes, with the observation group achieving significantly greater improvements (P< 0.05). Specifically, blood glucose levels decreased, LVEF increased while LVESD and LVEDD decreased, SAS and SDS scores improved, health behavior scores increased, and nursing satisfaction was higher in the observation group (93.3% vs 81.3%, P< 0.05).
Conclusion: Multidisciplinary collaborative nursing management effectively improves clinical and psychological outcomes, enhances health behaviors, and increases nursing satisfaction in patients with diabetes mellitus and coronary heart disease.
Keywords: diabetes mellitus, coronary heart disease, multidisciplinary collaborative nursing, blood glucose control, cardiac function, psychological status, health behavior
Introduction
Diabetes mellitus and coronary heart disease are two of the most prevalent chronic non-communicable diseases threatening human health, often exhibiting a bidirectional relationship of mutual influence and promotion.1 Studies2,3 have shown that the risk of coronary heart disease in patients with diabetes is significantly higher than that in the general population, while patients with coronary heart disease complicated with diabetes present with more complex conditions, including glucose metabolism disorders, vascular endothelial dysfunction, accelerated atherosclerosis, and reduced cardiac function. These factors further increase the risk of cardiovascular events and mortality. Therefore, achieving comprehensive management and effective intervention for such patients during clinical nursing has become a critical and challenging issue in the healthcare field. Traditional nursing models mostly focus on routine care and health education for a single disease, with limitations such as disciplinary fragmentation, insufficient communication, and lack of continuity and individualization of interventions.4 For patients with diabetes mellitus complicated with coronary heart disease, single-disciplinary nursing management often fails to meet their complex and diverse healthcare needs. For example, if only cardiology nurses are responsible for monitoring cardiac function and medication adherence, long-term blood glucose control may be overlooked. Conversely, if only blood glucose monitoring and dietary management are emphasized, potential cardiac dysfunction and psychological burdens may not be promptly addressed. Such fragmented nursing approaches are not conducive to the overall improvement of the patient’s condition and may also lead to confusion and poor adherence to healthy behaviors.5,6
In recent years, the multidisciplinary collaborative nursing management model has attracted increasing attention. This model emphasizes the joint participation of multiple disciplines, including cardiology, endocrinology, nutrition, psychology, and nursing teams, to provide comprehensive and systematic health management through multidimensional collaboration, information sharing, and individualized intervention planning.7 Importantly, this approach aligns with integrated care frameworks and behavior change theories, which suggest that coordinated interventions targeting biological, psychological, and behavioral dimensions can synergistically improve chronic disease outcomes.8 By combining professional expertise across disciplines, multidisciplinary collaborative nursing not only contributes to improved glucose control and cardiac function, but also enhances patients’ self-management capacity and psychological adjustment, ultimately promoting healthier long-term behaviors. Previous studies9–11 have suggested that multidisciplinary collaborative nursing management can improve quality of life and treatment adherence in patients with chronic diseases, but its application in patients with diabetes mellitus complicated with coronary heart disease requires further validation. Moreover, emerging evidence has shown that integrated cardiometabolic care models can effectively reduce cardiovascular risk factors and improve disease control in patients with diabetes and coexisting cardiovascular conditions, supporting the importance of multidisciplinary strategies in this population.12
Therefore, this study addressed the following research question: Does multidisciplinary collaborative nursing management provide superior benefits compared with routine nursing management in patients with diabetes mellitus complicated with coronary heart disease. Based on existing literature, we hypothesized that: (1) multidisciplinary collaborative nursing management would lead to better glycemic control and cardiac function; (2) it would further improve psychological adjustment and health behaviors; (3) it would enhance overall nursing satisfaction. This study aims to provide a more scientific and generalizable nursing management strategy for this complex patient population and support evidence-based clinical decision-making.
Materials and Methods
Study Design and Participants
This study was a single-center retrospective controlled study aimed at comparing the effects of the multidisciplinary collaborative nursing management model with the conventional nursing management model on glycemic control, cardiac function, psychological status, health behaviors, and nursing satisfaction in patients with diabetes mellitus combined with coronary heart disease. The enrollment period was from April 2022 to April 2025.
As a retrospective, hospital-based case enrollment study, the sample size was primarily determined by the number of cases that met the inclusion/exclusion criteria (a total of 150 cases were included in this study). During the study period, the hospital implemented two different routine nursing models in different wards: the conventional nursing model, which had long been established as standard care, and the multidisciplinary collaborative nursing model, which began to be progressively implemented in designated cardiometabolic management wards starting from early 2023. Patients naturally received one of the two nursing models based on the ward to which they were admitted, rather than by researcher allocation, thus avoiding selection bias.
All psychological, behavioral, and satisfaction assessments were part of the hospital’s standard chronic disease nursing evaluation process and were routinely recorded in the medical system. The present study retrospectively extracted these pre-existing clinical records without altering patient management or adding extra assessments.
Based on the nursing model previously received during clinical treatment, eligible patients were divided into the control group (conventional nursing, n=75) and the observation group (multidisciplinary collaborative nursing, n=75).
This study followed the ethical principles of the Declaration of Helsinki. All procedures were approved by the First Affiliated Hospital of China Medical University ethics committee (Approval No.: MXBLCHL2511). All patients and their families provided informed consent to participate in the interventions and data analysis and signed the relevant written documents. Medical records were anonymized to protect personal privacy.
Inclusion/Exclusion Criteria
Inclusion criteria: ① Inpatients or outpatients diagnosed with type 2 diabetes mellitus (meeting relevant clinical diagnostic criteria13) combined with coronary heart disease (diagnosed by coronary angiography, history of myocardial infarction, history of percutaneous coronary intervention, or clear diagnosis of stable/unstable angina pectoris); ② Age 18–85 years; ③ Complete inpatient records or outpatient follow-up records at enrollment, with available baseline and at least one follow-up indicator; ④ No severe communication barriers, able to cooperate with scale completion and follow-up.
Exclusion criteria: ① Type 1 diabetes mellitus or other specific types of diabetes; ② Severe end-stage organ failure (eg, requiring long-term dialysis, Child–Pugh class C hepatic insufficiency); ③ Active malignancy or expected survival <6 months; ④ Severe infection, psychosis, or significant cognitive impairment preventing completion of interventions or scale assessments; ⑤ Pregnant or lactating women; ⑥ Cases with missing key clinical indicators or without follow-up data.
Interventions
Control Group: Conventional Nursing Management Model
The control group received nursing care and health education according to the hospital’s conventional nursing process. The main contents included: Routine monitoring of vital signs and relevant indicators (blood pressure, pulse, blood oxygen, blood glucose, etc).; Execution of physician’s medication orders and medication education (timing, dosage, precautions for adverse reactions); Basic dietary, exercise, and lifestyle guidance (routinely provided by nursing staff or nutritionists); Provision of written health education materials at discharge and recommendations for outpatient follow-up or routine departmental re-examination; Follow-up conducted primarily via outpatient review or telephone (once every 4 weeks); Outpatient re-examination arranged at 8 weeks.
Observation Group: Multidisciplinary Collaborative Nursing Management Model
The observation group received a structured multidisciplinary collaborative nursing management program. To facilitate understanding, the intervention components are summarized in Table 1.
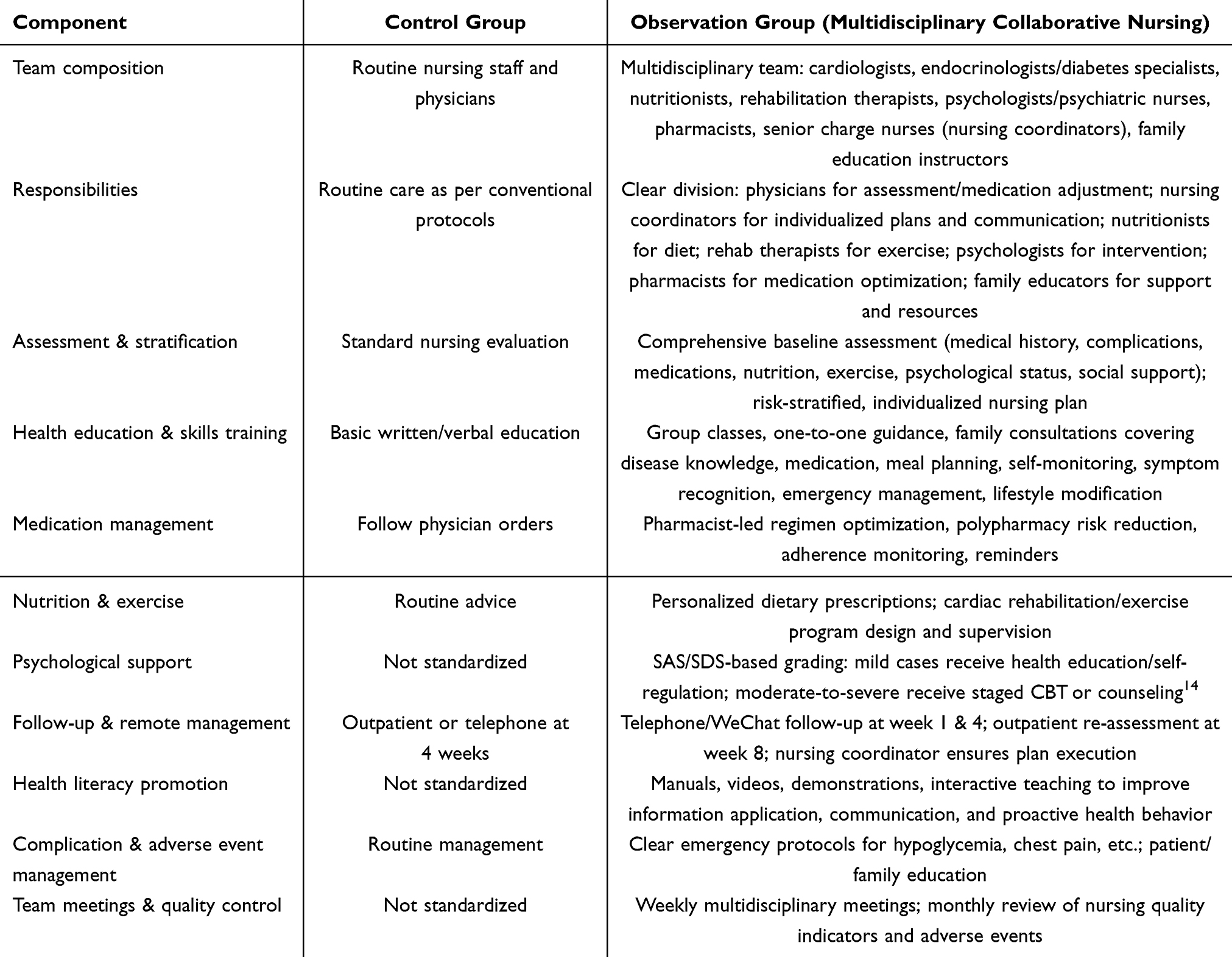 |
Table 1 Comparison of Intervention Components Between Control and Observation Groups |
Observation Indicators and Measurement Methods
Glycemic Control
At pre-intervention and 8 weeks post-intervention (post-intervention), 5 mL of fasting venous blood was collected from patients. A glucometer was used to measure fasting plasma glucose (FPG) and 2-hour postprandial glucose (2 h PG), while an automatic biochemical analyzer was applied to detect glycated hemoglobin (HbA1c).
Cardiac Function Indicators
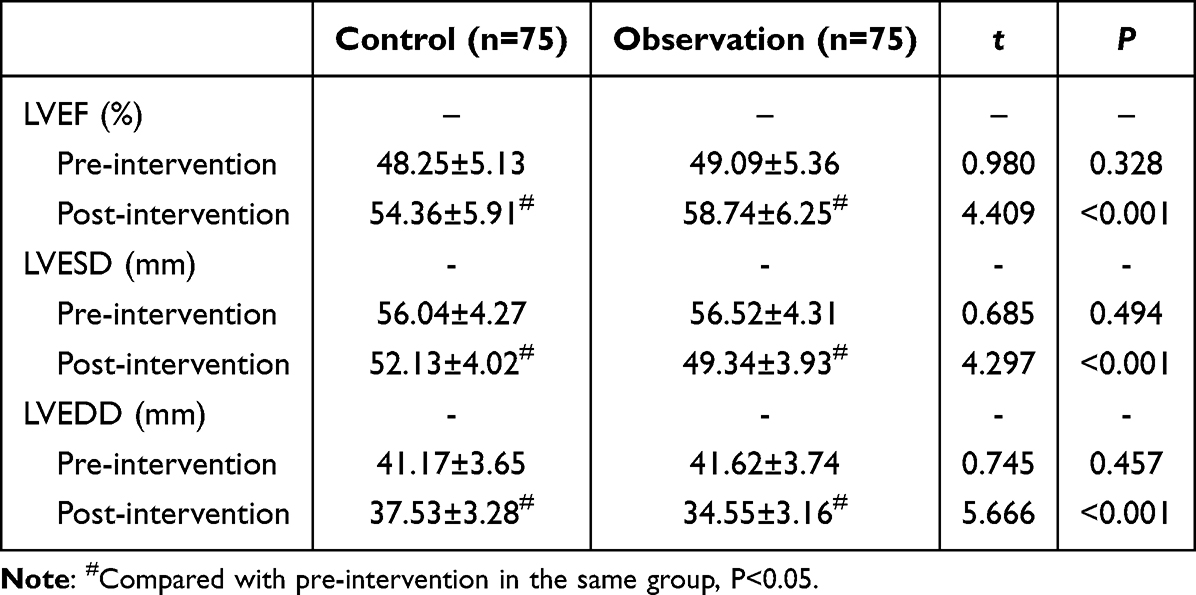
At pre-intervention and post-intervention, echocardiographic data were collected to measure the following parameters: left ventricular ejection fraction (LVEF), left ventricular end-systolic diameter (LVESD), and left ventricular end-diastolic diameter (LVEDD).
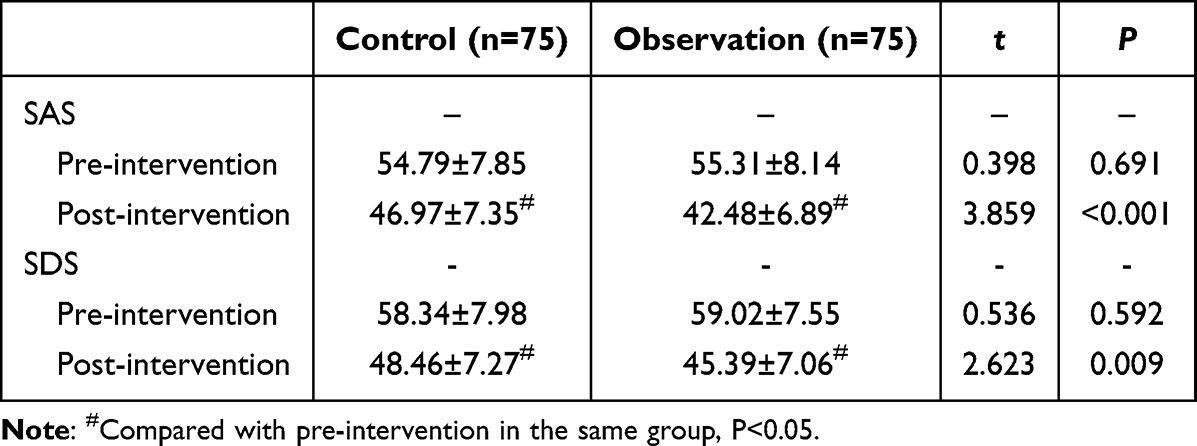
Psychological Status15
At pre-intervention and post-intervention, the Self-Rating Anxiety Scale (SAS, Cronbach’s α=0.784, validity=0.749) was used to evaluate patients’ anxiety level. The scale has a total score of 100, with a cutoff value of 50. Higher scores indicate greater anxiety. The Self-Rating Depression Scale (SDS, Cronbach’s α=0.795, validity=0.762) was used to evaluate depression, with a total score of 100, a cutoff value of 53, and higher scores indicating more severe depression.
Health Behavior Status
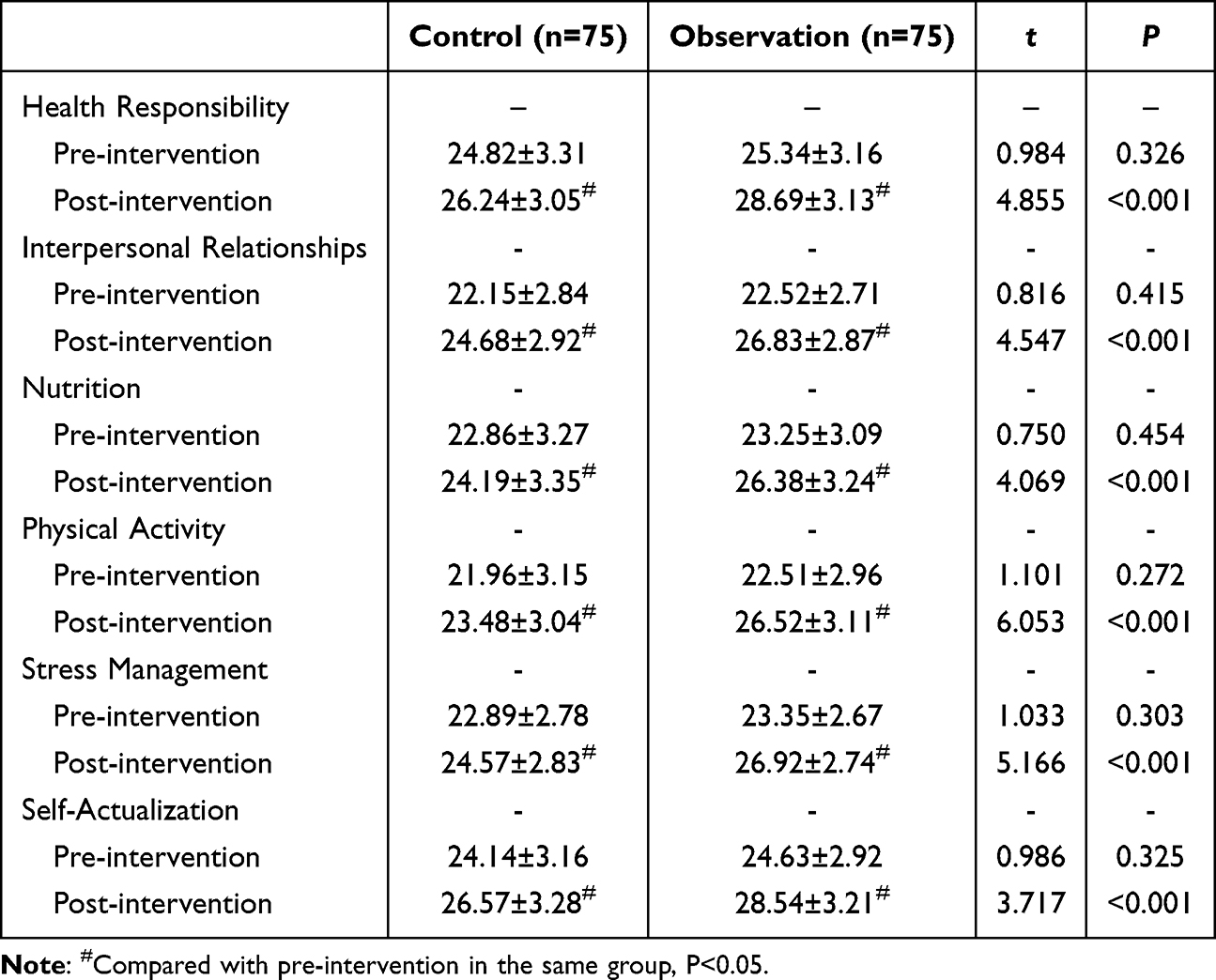
At pre-intervention and post-intervention, the Health-Promoting Lifestyle Profile-II (HPLP-II, Cronbach’s α=0.856, validity=0.822)16 was used to assess health behavior. The scale consists of 52 items across six dimensions (health responsibility, interpersonal relationships, nutrition, exercise, stress management, self-actualization), scored from 1–4 points, with a maximum total score of 208. Higher scores in each dimension indicate better health behaviors.
Nursing Satisfaction
The Newcastle Satisfaction with Nursing Scale (NSNS, Cronbach’s α=0.759, validity=0.784)17 was used to assess nursing satisfaction. The scale contains 19 items scored on a 5-point Likert scale, with higher scores indicating higher satisfaction. According to the scores, satisfaction was categorized as: very satisfied (≥76 points), satisfied (57–75 points), average (38–56 points), or dissatisfied (<38 points). Total satisfaction rate = (number of very satisfied cases + number of satisfied cases)/total cases ×100%.
Data Collection and Quality Control
Two researchers independently extracted research data from electronic and paper medical records and entered them into a database. Double entry was used to reduce input errors. Random checks (≥10% of cases) were performed on key variables to verify consistency. The reasons for missing values were traced, and when necessary, in-hospital laboratory/follow-up records were reviewed to supplement the data. Outcome assessors (eg, imaging physicians, psychological scale evaluators) were blinded to group assignments when possible to reduce assessment bias. Unified standard operating procedures (SOP) were applied for measurement and intervention implementation. All participants underwent standardized training and assessment prior to study initiation.
Statistical Methods
SPSS 26.0 was used for data analysis, and GraphPad Prism software was applied for plotting and advanced analyses. Normality was tested using the Shapiro–Wilk method, showing that continuous variables followed a normal distribution. Data were expressed as mean ± standard deviation ( ). Independent samples t-tests were used for intergroup comparisons, and paired t-tests were applied for intragroup pre- and post-comparisons. Categorical data were expressed as counts or percentages, and intergroup comparisons were conducted using the χ2-test or Fisher’s exact test. Two-tailed tests were applied, with P<0.05 considered statistically significant.
). Independent samples t-tests were used for intergroup comparisons, and paired t-tests were applied for intragroup pre- and post-comparisons. Categorical data were expressed as counts or percentages, and intergroup comparisons were conducted using the χ2-test or Fisher’s exact test. Two-tailed tests were applied, with P<0.05 considered statistically significant.
Results
Comparison of General Characteristics
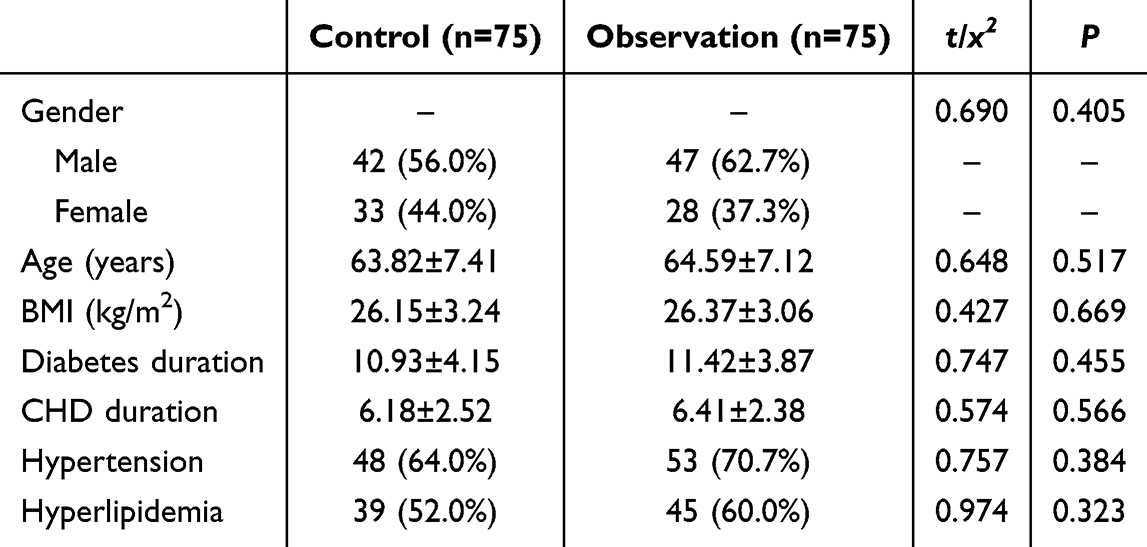
There were no statistically significant differences between the control and observation groups in terms of gender, age, body mass index (BMI), duration of diabetes, duration of coronary heart disease, or comorbidities (P>0.05), indicating comparability (Table 2).
 |

Comparison of Glycemic Control
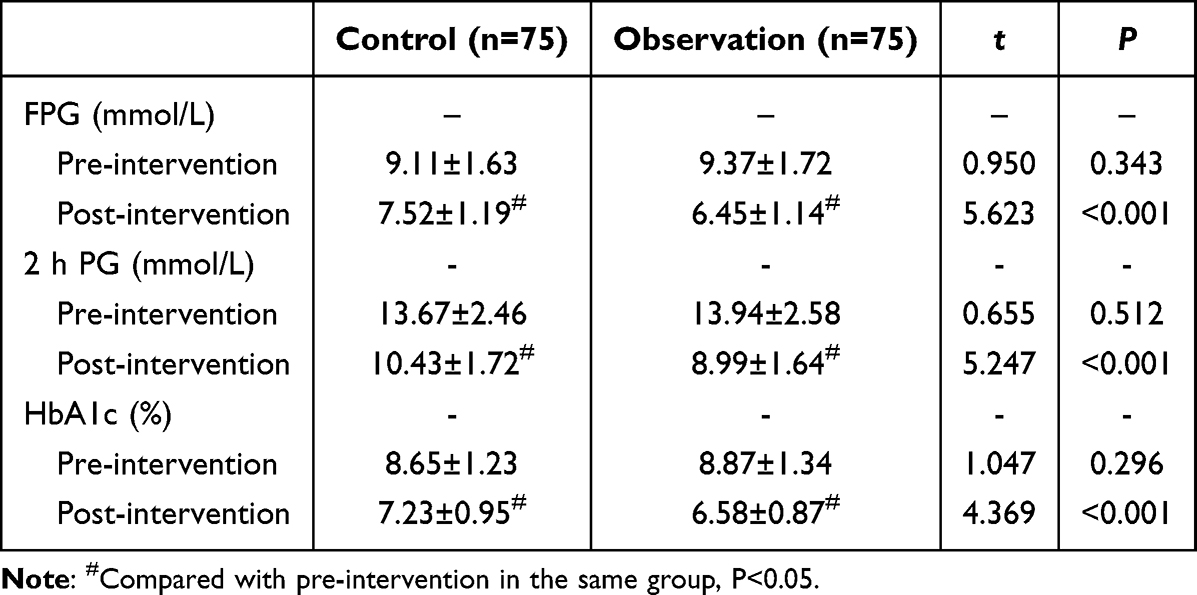
After the intervention, both groups showed reductions in FPG, 2 h PG, and HbA1c compared with pre-intervention levels, with greater improvement in the observation group (P<0.05) (Table 3 and Figure 1).
 |

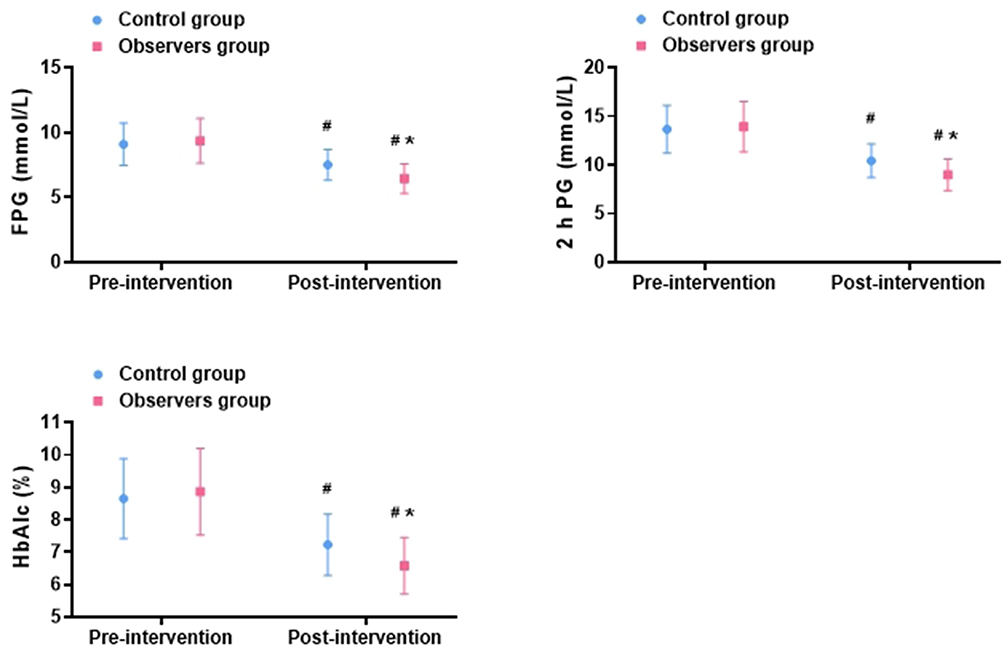 |
Figure 1 Comparison of Glycemic Control ( Notes: #Compared with pre-intervention in the same group, P<0.05; *Between-group comparison, P<0.05. |

Comparison of Cardiac Function
After the intervention, LVEF increased while LVESD and LVEDD decreased in both groups, with greater improvements in the observation group (P<0.05) (Table 4 and Figure 2).
 |

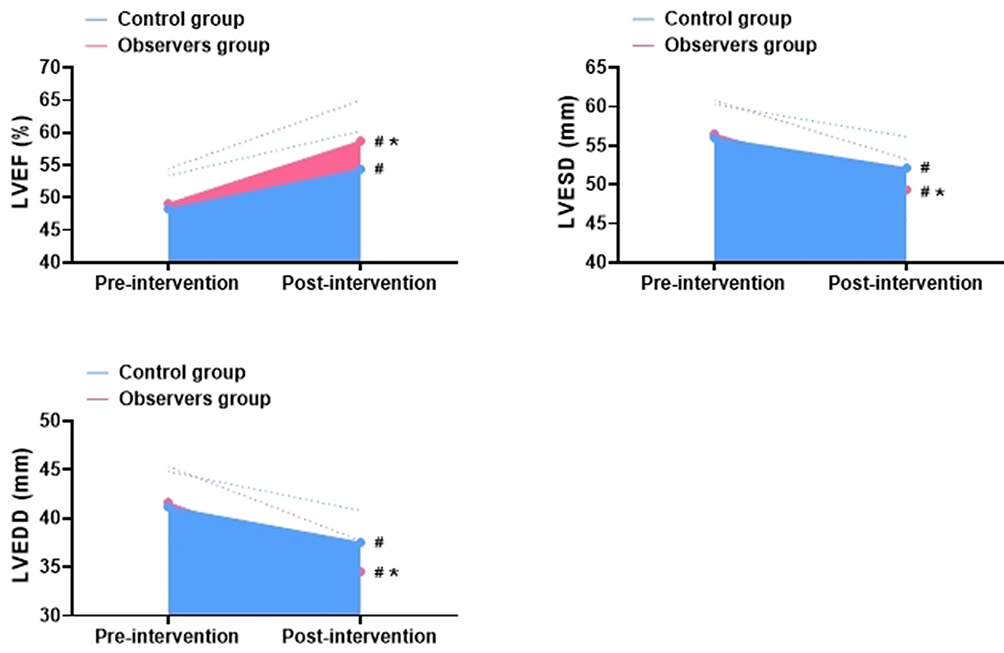 |
Figure 2 Comparison of Cardiac Function Indicators ( Notes: #Compared with pre-intervention in the same group, P<0.05; *Between-group comparison, P<0.05. |

Comparison of Psychological Status
Post-intervention, SAS and SDS scores decreased in both groups, with larger reductions in the observation group (P<0.05) (Table 5 and Figure 3).
 |

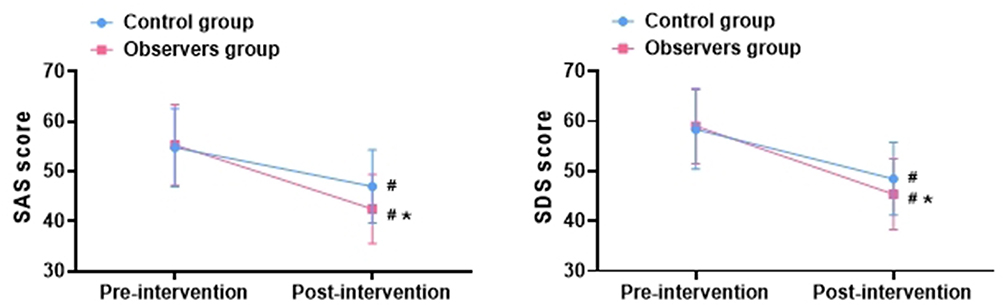 |
Figure 3 Comparison of Psychological Status ( Notes: #Compared with pre-intervention in the same group, P<0.05; *Between-group comparison, P<0.05. |

Comparison of Health Behavior Status
After intervention, both groups improved in health responsibility, interpersonal relationships, nutrition, physical activity, stress management, and self-actualization, with greater improvements in the observation group (P<0.05) (Table 6 and Figure 4).
 |

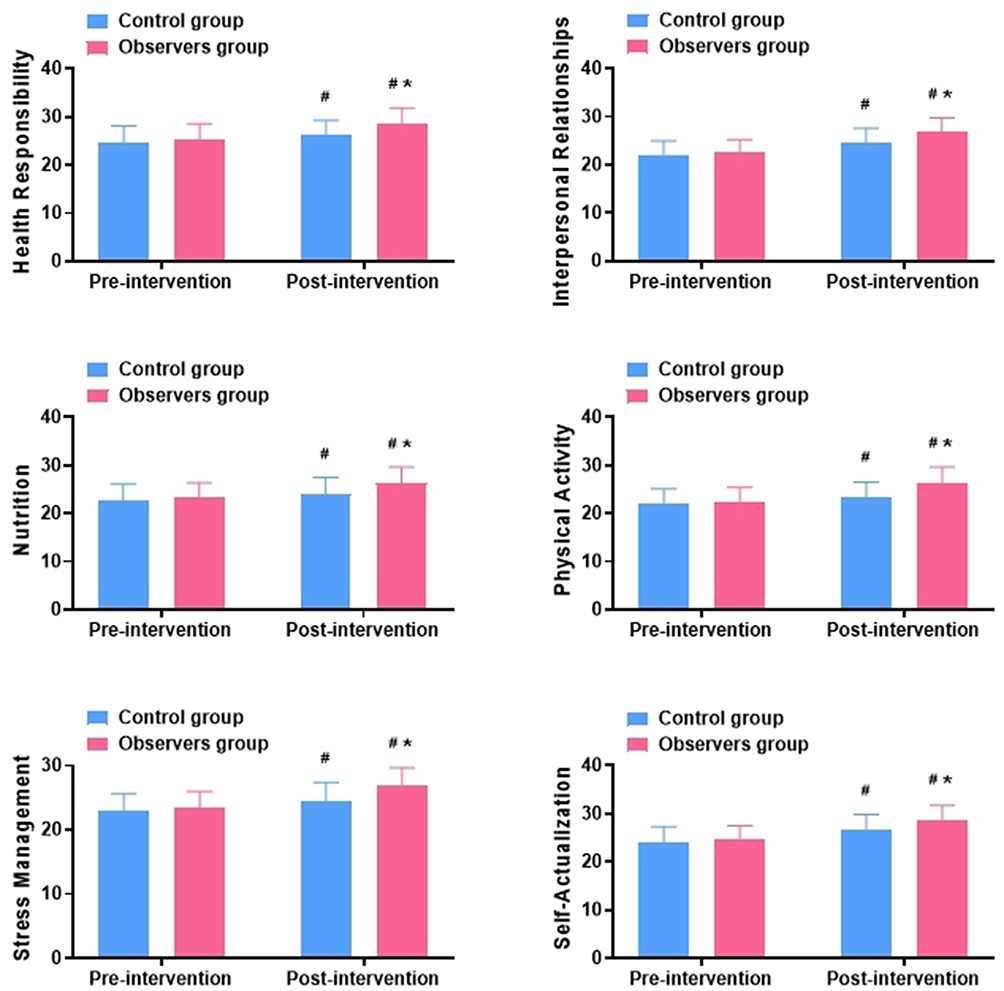 |
Figure 4 Comparison of Health Behavior Status ( Notes: #Compared with pre-intervention in the same group, P<0.05; *Between-group comparison, P<0.05. |

Comparison of Nursing Satisfaction
The total nursing satisfaction was higher in the observation group (93.3%) than in the control group (81.3%) (P<0.05) (Table 7 and Figure 5).
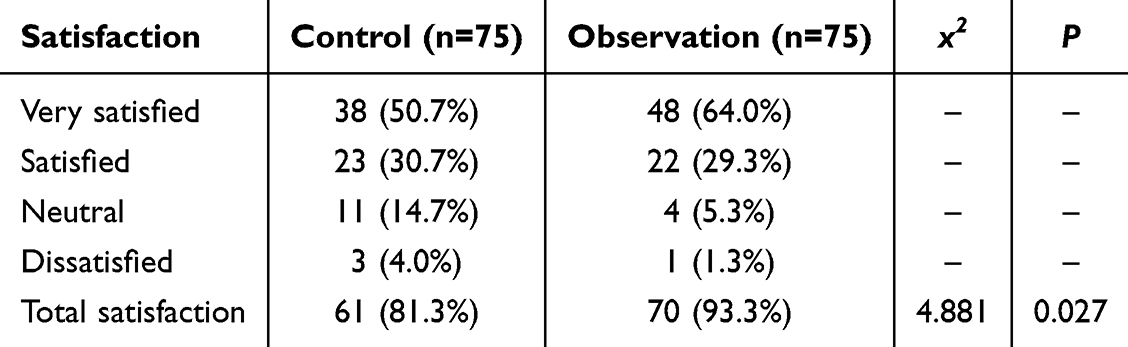 |
Table 7 Comparison of Nursing Satisfaction [n (%)] |
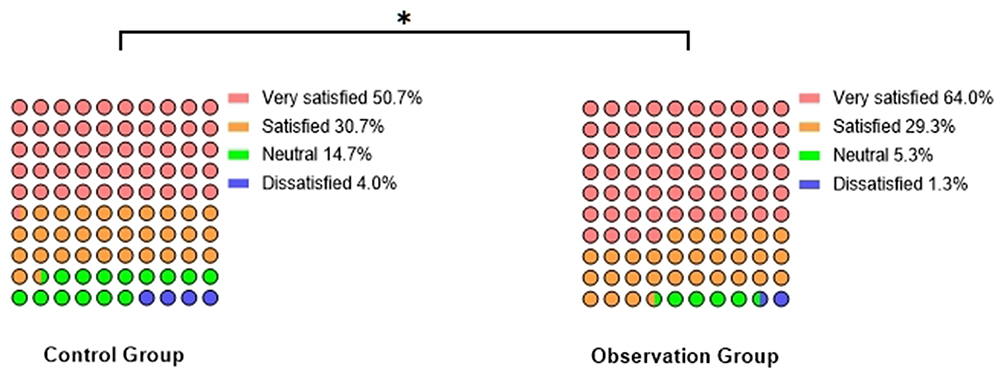 |
Figure 5 Comparison of Nursing Satisfaction [n (%)]. Note: *Between-group comparison, P<0.05. |
Results
Comparison of General Data
No statistically significant differences were observed between the control and observation groups in terms of gender, age, body mass index (BMI), duration of diabetes, duration of coronary heart disease, and comorbidities (P>0.05), indicating comparability (see Table 1).
Comparison of Glycemic Control
At post-intervention, FPG, 2 h PG, and HbA1c levels decreased in both groups compared with pre-intervention, with the observation group showing greater improvements than the control group (P<0.05, see Table 2).
Comparison of Cardiac Function Indicators
At post-intervention, LVEF increased in both groups compared with pre-intervention, while LVESD and LVEDD decreased. The improvements in the observation group were more significant than those in the control group (P<0.05, see Table 3).
Comparison of Psychological Status
At post-intervention, SAS and SDS scores decreased in both groups compared with pre-intervention, with greater reductions observed in the observation group than in the control group (P<0.05, see Figure 1).
Comparison of Health Behavior Status
At post-intervention, scores for health responsibility, interpersonal relationships, nutrition, exercise, stress management, and self-actualization all increased in both groups compared with pre-intervention, with greater improvements in the observation group (P<0.05, see Figure 2).
Comparison of Nursing Satisfaction
In the control group (n=75), there were 38 cases of very satisfied, 23 satisfied, 11 average, and 3 dissatisfied. In the observation group (n=75), there were 48 cases of very satisfied, 22 satisfied, 4 average, and 1 dissatisfied. The overall nursing satisfaction rate was higher in the observation group (93.3%) than in the control group (81.3%) (P<0.05, see Figure 3).
Discussion
This study retrospectively analyzed 150 patients with diabetes mellitus complicated with coronary heart disease to explore the effects of a multidisciplinary collaborative nursing management model on blood glucose control, cardiac function improvement, psychological status regulation, health behavior promotion, and nursing satisfaction. The results demonstrated that this model exhibited significant advantages at multiple levels compared with conventional nursing models, providing more comprehensive and systematic healthcare support to meet the complex health needs of patients with chronic comorbidities.
In terms of blood glucose control, this study showed that after intervention, patients in the observation group had significantly decreased FPG, 2 h PG, and HbA1c levels, with reductions superior to those in the control group. Stable blood glucose control is the core goal of diabetes mellitus treatment, as fluctuations in blood glucose not only directly influence the progression of diabetes mellitus but are also closely related to the onset and progression of coronary heart disease.18,19 The advantage of the multidisciplinary collaborative nursing model in glycemic management lies in the individualized and refined programs developed through the collaboration of endocrinologists, dietitians, nursing staff, and pharmacists. Regarding diet, nutritionists designed reasonable dietary structures tailored to patients’ blood glucose levels, body mass index, and comorbidities; regarding exercise, rehabilitation specialists and nurses guided patients in gradual aerobic and resistance training; regarding medication, pharmacists monitored drug adherence and adverse effects to maximize therapeutic efficacy. In addition, incorporating psychological care reduced sympathetic nerve excitability and endocrine disturbances caused by anxiety and depression,20 thereby stabilizing blood glucose fluctuations. Jones et al21 also found that multidisciplinary integrated management led to greater reductions in blood glucose compared with single nursing interventions, which is consistent with the findings of this study and further confirms the importance of collaborative models in glycemic control for diabetes mellitus patients.
Regarding cardiac function, the results of this study indicated that after intervention, LVEF levels in the observation group significantly increased, while LVESD and LVEDD markedly decreased, showing improvements in both systolic and diastolic cardiac functions. In patients with diabetes mellitus and coronary heart disease, cardiac dysfunction often results from coronary ischemia, abnormal glucose-lipid metabolism, and impaired myocardial energy utilization.22,23 The multidisciplinary collaborative nursing model improved cardiac function through the synergistic effects of precise pharmacological management by cardiologists, exercise prescriptions by rehabilitation specialists, and nutrition and psychological interventions. For example, regular rehabilitation exercise not only enhanced myocardial metabolism and increased cardiac oxygen utilization efficiency but also suppressed left ventricular remodeling, thereby delaying further deterioration of cardiac function.24 Moreover, effective glycemic control reduced the damage of advanced glycation end-products to myocardial cells, indirectly improving cardiac pump function.25 Previous studies26 have shown that patients receiving systematic cardiac rehabilitation experienced significant improvements in LVEF and exercise tolerance, which aligns with the findings of this study. These results suggest that the multidisciplinary collaborative model does not focus solely on disease-specific management but instead integrates resources to optimize both metabolism and cardiac function.
In terms of psychological status, this study revealed that post-intervention SAS and SDS scores were significantly reduced in the observation group, with improvements superior to those in the control group. Anxiety and depression are common in patients with diabetes mellitus and coronary heart disease, and such negative emotions not only decrease treatment adherence but also aggravate disease burden through neuroendocrine pathways.27,28 In the multidisciplinary collaborative nursing model, the involvement of psychiatrists and nurses played a key role. Regular psychological counseling, group communication, and relaxation training helped patients establish positive attitudes toward disease management. Meanwhile, supportive measures from other disciplines indirectly alleviated psychological distress—for instance, effective improvements in glycemic control and cardiac function reduced patients’ fear of disease progression, thereby lowering anxiety levels. Wu et al29 also reported that psychological interventions for patients with diabetes mellitus and cardiovascular disease significantly improved anxiety and depression, which is consistent with our findings. Notably, this study showed greater improvements in psychological status in the observation group, suggesting that comprehensive, multidimensional psychological interventions are more effective than single nursing measures, which has important implications for optimizing clinical nursing models.
In terms of health behavior improvement, this study found that patients in the observation group showed significant increases in scores across six dimensions of health behavior: Health Responsibility, Interpersonal Relationships, Nutrition, Physical Activity, Stress Management, and Self-Actualization, with greater improvements than those in the control group. This indicates that multidisciplinary collaborative nursing helps patients gradually develop positive health behavior habits in long-term disease management. The mechanism may lie in the fact that multidisciplinary collaboration not only delivers health education at the knowledge level but also emphasizes behavior change and execution. For instance, the nursing team improved patients’ adherence through WeChat follow-up and telephone reminders; nutritionists and rehabilitation specialists provided scientific dietary and exercise guidance; the psychological team enhanced patients’ self-efficacy, increasing the stability of behavioral maintenance. Dankoly et al30 similarly demonstrated that multidisciplinary interventions significantly improved healthy lifestyle scores in diabetes mellitus patients and maintained stability during long-term follow-up, consistent with our findings. This suggests that in chronic disease management, single education is often insufficient for sustained behavior change, whereas collaborative nursing models can foster health behavior formation through comprehensive interventions.
Finally, regarding nursing satisfaction, this study found that overall nursing satisfaction in the observation group reached 93.3%, significantly higher than the 81.3% in the control group. This result indicates that the multidisciplinary collaborative nursing management model not only improved physiological and psychological outcomes but also enhanced patients’ overall recognition of and trust in nursing services. The increase in patient satisfaction can be attributed to individualized, holistic, and continuous care services.31,32 Through cross-disciplinary collaboration, patients experienced differentiated and humanized nursing care, which improved their trust in healthcare services. Previous studies33,34 have confirmed that multidisciplinary collaborative nursing models can enhance patient satisfaction and adherence, consistent with the findings of this study. Moreover, improved nursing satisfaction not only reflects higher care quality but also helps improve doctor–patient relationships, fostering positive interaction.
Based on the above results, this study verified the significant advantages of the multidisciplinary collaborative nursing management model from multiple dimensions. Its mechanisms of action include not only direct medical and nursing interventions but also indirect psychological and social support effects. Compared with previous studies, the findings of this study are generally consistent, while expanding in terms of sample size and indicator coverage, thereby further enriching the evidence base in this field. However, several limitations remain: first, as a single-center retrospective study, selection bias may exist; second, the follow-up duration was relatively short, which failed to fully reflect the long-term prognostic effects of this nursing mo third, an in-depth analysis of the cost-effectiveness of the nursing model was not performed, which requires improvement in future studies.
Conclusion
The findings of this study indicate that the multidisciplinary collaborative nursing management model provides significant advantages in the comprehensive management of patients with diabetes mellitus complicated with coronary heart disease. Compared with conventional nursing models, this approach more effectively reduces blood glucose levels, improves cardiac function, alleviates adverse psychological states, and enhances multiple dimensions of health behavior, including Health Responsibility, Interpersonal Relationships, Nutrition, Physical Activity, Stress Management, and Self-Actualization. Nursing satisfaction was also markedly higher under the multidisciplinary model.
Importantly, this study suggests that the effectiveness of this model may stem from its integrated and coordinated approach that combines medical, nursing, nutritional, psychological, and rehabilitative support, thereby offering patients multidimensional benefits in “body–mind–behavior”. In addition, acknowledging the retrospective design and the absence of long-term follow-up, the conclusions should be interpreted with caution. Nevertheless, the overall results support the model’s potential for broader application in chronic disease management. Future multicenter, large-sample prospective studies are needed to further validate long-term efficacy, explore underlying mechanisms, and examine its applicability among patients with other chronic comorbidities.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Xu JJ, Zhu P, Song Y, et al. [Impact of prolonging dual antiplatelet therapy on long-term prognosis of elderly patients with coronary heart disease complicated with diabetes mellitus undergoing drug-eluting stent implantation]. Zhonghua Xin Xue Guan Bing Za Zhi. 2022;50(5):450–13. Polish. doi:10.3760/cma.j.cn112148-20211120-01002
2. Wang J, Xu HB, Zhang HP, et al. [Impact of type 2 diabetes mellitus on the progression and revascularization of coronary non-target lesions in patients with coronary heart disease]. Zhonghua Xin Xue Guan Bing Za Zhi. 2020;48(5):393–400. Polish. doi:10.3760/cma.j.cn112148-20190425-00204
3. Wang M, Fan XK, Su J, et al. [Association of serum gamma-glutamyl transferase levels with cardiovascular disease risk in type 2 diabetes patients: a prospective cohort study]. Zhonghua Liu Xing Bing Xue Za Zhi. 2024;45(10):1339–1347. Danish. doi:10.3760/cma.j.cn112338-20240628-00384
4. Kumar SS, Jenn Ng C, Oka P, et al. Establishing continuity of care through a team-based care approach: implementation challenges. J Prim Care Community Health. 2025;16:21501319251369674. doi:10.1177/21501319251369674
5. Stocker M, Pilgrim S, Burmester M, et al. Interprofessional team management in pediatric critical care: some challenges and possible solutions. J Multidiscip Healthc. 2016;9:47–58. doi:10.2147/JMDH.S76773
6. Fury S, Sparbel K, Tadda B. Interprofessional collaboration with pharmacist-driven education for hypertension control in federally qualified health center patients. J Dr Nurs Pract. 2018;11(1):43–51. doi:10.1891/2380-9418.11.1.43
7. Wu KJ. [Multidisciplinary cooperation strengthens individualized management of breast cancer in pregnancy]. Zhonghua Wai Ke Za Zhi. 2020;58(2):95–98. Hawaiian. doi:10.3760/cma.j.issn.0529-5815.2020.02.004
8. Fakolade A, Walters AJ, Cameron J, Latimer-Cheung AE, Pilutti LA. Healthy together: a systematic review of theory and techniques used in health interventions for persons with chronic neurological conditions and their caregivers. Patient Educ Couns. 2020;103(4):788–803. doi:10.1016/j.pec.2019.10.022
9. Hsu HT, Chiang Y-C, Lai Y-H, et al. Effectiveness of multidisciplinary care for chronic kidney disease: a systematic review. Worldviews Evid Based Nurs. 2021;18(1):33–41. doi:10.1111/wvn.12483
10. Tang YH, Zhang J. Clinical effect of enhanced recovery after surgery based on multidisciplinary collaboration model in postoperative gastric cancer surgery. World J Gastrointest Surg. 2025;17(7):105387. doi:10.4240/wjgs.v17.i7.105387
11. You LF, Zhang P, Zhang QQ. Multidisciplinary collaborative enhanced recovery after surgery nursing in patients with colorectal cancer: a comparative study. World J Gastrointest Oncol. 2025;17(8):104569. doi:10.4251/wjgo.v17.i8.104569
12. Tu Q, Lin S, Hyun K, et al. The effects of multidisciplinary collaborative care on cardiovascular risk factors among patients with diabetes in primary care settings: a systematic review and meta-analysis. Prim Care Diabetes. 2024;18(4):381–392. doi:10.1016/j.pcd.2024.05.003
13. Chinese Diabetes Society. [National handbook for the prevention and control of diabetes in primary care (2022)]. Zhonghua Nei Ke Za Zhi. 2022;61(7):717–748. Polish. doi:10.3760/cma.j.cn112138-20220509-00350
14. Golovacheva VA, Golovacheva AA, Fateeva TG, et al. [Cognitive behavioral therapy in the treatment of patients with chronic migraine and concomitant chronic insomnia: a prospective, randomized trial]. Zh Nevrol Psikhiatr Im S S Korsakova. 2024;124(5. Vyp. 2):110–117. Hungarian. doi:10.17116/jnevro2024124052110
15. Ma CQ, Meng X-J, Zhu M-Y, et al. [Clinical application value of preoperative emotional management combined with family members’ interactive description nursing in plasmakinetic enucleation of the prostate]. Zhonghua Nan Ke Xue. 2022;28(10):909–914. Basque
16. Deniz F, Altunay IK, Ozkur E, et al. Evaluation of Healthy Lifestyle Behaviors in Psoriasis Patients. Sisli Etfal Hastan Tip Bul. 2021;55(2):197–202. doi:10.14744/SEMB.2020.01799
17. Karadaş A, Ergün S, Kaynak S. Relationship between missed nursing care and patients’ trust in nurses and satisfaction with care: a cross-sectional study. Nurs Health Sci. 2024;26(3):e13149. doi:10.1111/nhs.13149
18. Sun PT, Du X-C, Wang R-D, et al. [predictive value of pancreatic steatosis for severity of coronary atherosclerosis in patients with type 2 diabetes mellitus]. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2020;42(2):172–177. Danish. doi:10.3881/j.issn.1000-503X.11524
19. Uysal N, Aşıkoğlu C. The effect of nursing Care satisfaction on illness perception in patients with acute coronary syndrome. J Mod Nurs Pract Res. 2025;5(1):1. doi:10.53964/jmnpr.2025001
20. Kintzoglanakis K, Gkousiou A, Vonta P, et al. Depression, anxiety, and diabetes-related distress in type 2 diabetes in primary care in Greece: different roles for glycemic control and self-care. SAGE Open Med. 2022;10:20503121221096605. doi:10.1177/20503121221096605
21. Jones A, Bardram JE, Bækgaard P, et al. Integrated personalized diabetes management goes Europe: a multi-disciplinary approach to innovating type 2 diabetes care in Europe. Prim Care Diabetes. 2021;15(2):360–364. doi:10.1016/j.pcd.2020.10.008
22. Pan CJ, Wang T, Yin R-H, et al. Coronary imaging characteristics and risk factors in patients with type 2 diabetes mellitus with coronary heart disease complication. World J Diabetes. 2025;16(4):99151. doi:10.4239/wjd.v16.i4.99151
23. Zhao S, Xu H, Liu F, Guo X, Zhang Y. Application of early multi-dimensional cardiac rehabilitation nursing in percutaneous coronary intervention and its effects on adverse events and patients’ adherence to medication. J Mod Nurs Pract Res. 2(4):16. doi:10.53964/jmnpr.2022016
24. Siam NH, Snigdha NN, Tabasumma N, et al. Diabetes mellitus and cardiovascular disease: exploring epidemiology, pathophysiology, and treatment strategies. Rev Cardiovasc Med. 2024;25(12):436. doi:10.31083/j.rcm2512436
25. Hu RY, He QF, Pan J, et al. [Association between body mass index changes and other risk factors for cardiovascular disease in patients with type 2 diabetes mellitus]. Zhonghua Liu Xing Bing Xue Za Zhi. 2021;42(7):1194–1199. Danish. doi:10.3760/cma.j.cn112338-20200615-00841
26. Oldridge N, Taylor RS. Cost-effectiveness of exercise therapy in patients with coronary heart disease, chronic heart failure and associated risk factors: a systematic review of economic evaluations of randomized clinical trials. Eur J Prev Cardiol. 2020;27(10):1045–1055. doi:10.1177/2047487319881839
27. Tusa N, Kautiainen H, Elfving P, et al. Depressive symptoms decrease health-related quality of life of patients with coronary artery disease and diabetes: a 12-month follow up study in primary care. Scand J Prim Health Care. 2023;41(3):276–286. doi:10.1080/02813432.2023.2233995
28. Miao Jonasson J, Hendryx M, Shadyab AH, et al. Social support, social network size, social strain, stressful life events, and coronary heart disease in women with type 2 diabetes: a cohort study based on the women’s health initiative. Diabetes Care. 2020;43(8):1759–1766. doi:10.2337/dc19-2065
29. Wu X, Zu Y, Li D, et al. Psychosocial and behavioral risk patterns and risk of cardiovascular complications in people with type 2 diabetes. Diabet Res Clin Pract. 2025;221:112037. doi:10.1016/j.diabres.2025.112037
30. Dankoly US, Vissers D, El Mostafa SB, et al. Perceived barriers, benefits, facilitators, and attitudes of health professionals towards type 2 diabetes management in Oujda, Morocco: a qualitative focus group study. Int J Equity Health. 2023;22(1):29. doi:10.1186/s12939-023-01826-5
31. Zhang HM, Wang Q-H, Xu S-T, et al. [Psychological care combined with enhanced recovery after surgery management in perioperative nursing care of andrological patients: a randomized controlled study]. Zhonghua Nan Ke Xue. 2020;26(10):917–921. Basque
32. Huang XM, Meng P, Li H, et al. [Psychological status-based early risk warning combined with multidisciplinary team intervention improves satisfaction of the outpatients in the andrology clinic HUANG Xun-mei1, MENG Ping1, LI Hui2, HE Wei-xiang1, MA Xiao-li3, GAO Jing-jing4, XUE Rui-zhi1, CHENG Rui1]. Zhonghua Nan Ke Xue. 2024;30(10):878–883. Basque
33. Gu YH, Wang X, Sun SS. Benefits of multidisciplinary collaborative care team-based nursing services in treating pressure injury wounds in cerebral infarction patients. World J Clin Cases. 2022;10(1):43–50. doi:10.12998/wjcc.v10.i1.43
34. Zou F, Sun D, Chang J, et al. Impact of multidisciplinary collaborative jejunal nutrition care on nutritional status and quality of life in severely burned patients. Medicine. 2025;104(14):e41965. doi:10.1097/MD.0000000000041965
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.