Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Multidisciplinary Clinicians and the Relational Autonomy of Persons with Neurodegenerative Disorders and an Advance Care Plan: A Thematic Analysis
Authors Craig DP ![]() , Ray R
, Ray R ![]() , Harvey D
, Harvey D ![]() , Shircore M
, Shircore M ![]()
Received 22 October 2021
Accepted for publication 19 November 2021
Published 9 December 2021 Volume 2021:14 Pages 3385—3398
DOI https://doi.org/10.2147/JMDH.S345792
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Denise Patricia Craig,1 Robin Ray,2 Desley Harvey,3,4 Mandy Shircore5
1College of Medicine and Dentistry, James Cook University, Cairns, Queensland, Australia; 2College of Medicine and Dentistry, James Cook University, Townsville, Queensland, Australia; 3Health Practitioner Research Capacity Building, Cairns and Hinterland Hospital and Health Service, Cairns, Queensland, Australia; 4College of Healthcare Sciences, James Cook University, Cairns, Queensland, Australia; 5College of Business, Law and Governance, James Cook University, Cairns, Queensland, Australia
Correspondence: Denise Patricia Craig
College of Medicine and Dentistry, James Cook University, PO Box 4703, Cairns, QLD, 4870, Australia
Email [email protected]
Introduction: People diagnosed with neurodegenerative disorders often grapple with threats to their agency, prompting some to engage in advance care planning. Advance care plans are intended to protect autonomy by helping patients receive goal-consistent healthcare. Accordingly, there is a need to better understand factors associated with hospital doctors’ application of advance care plans to treatment decisions of this patient cohort.
Purpose: The purpose of this study was to explain the recommendations of multidisciplinary hospital-based clinicians about the benefits of advance care plans for people diagnosed with neurodegenerative disorders, and the elements that influence how doctors apply such plans.
Materials and Methods: Using a constructivist grounded theory informed thematic analysis, semi-structured interviews were conducted with purposively and theoretical sampled hospital-based clinicians: 16 doctors, six registered nurses and 10 allied health clinicians who self-reported having experience delivering healthcare to people with neurodegenerative disorders and an advance care plan. Allied health and nurse data helped to inform questions posed to doctors. Data were inductively analysed using open and focused coding.
Results: Analysis revealed two main themes: recommending agency through advance care plans; and limiting agency through advance care plans. These themes formed the basis of the core category: patient agency. All clinicians held positive attitudes towards advance care plans as a means to preserve patient voices and alleviate family of responsibility. However, the extent to which doctors shared decisions with family revealed a tension between individualistic agency associated with advance care plans and relational autonomy perceived by doctors as appropriate.
Conclusion: Although doctors expressed positive attitudes towards advance care plans, they typically practiced relational autonomy wherein they partner with family in contemporaneous healthcare decision on patients’ behalf. Accordingly, the healthcare preferences of hospitalised, incompetent people with neurodegenerative disorders are balanced against judgements of both doctors and family.
Keywords: advance directive, allied health, end-of-life, hospital doctors, patient agency, registered nurses, relational autonomy
Background
People with illnesses such as dementia, Parkinson’s Disease, Huntington’s Disease and Motor Neuron Disease (MND) live with the tangible prospects of disabling and progressive cognitive decline.1 In an ageing population, many people fear loss of autonomy and agency as a consequence of neurodegenerative disorder.2,3 Internationally recognised dementia advocate Christine Bryden4 described her experience of dementia as a “journey of so many losses from diagnosis to death”. Consequently, people diagnosed with neurodegenerative disorders (PWND) often grapple with a threat to agency, loss of self-identity, independence, and control.5
Alongside accumulating losses, PWND are at high risk of hospitalisation in the last months of life, where end-of-life care, and death, can become impersonal and medicalised.6,7 Accordingly, PWND may choose to document their later life care preferences within an Advance Care Plan (ACP) to preserve agency.8 Agency is defined as an individual’s capacity to act independently and exercise free choice,9 albeit in the context of social influences that affect human behaviour.10 Grounded in a principle-based perspective (or “principlism”), ACPs offer a Western-styled, self-determination conception of autonomy11,12 intended to protect patients from paternalism.13 Advance care planning represents a call to action, facilitated by structures within society, and it stands as a powerful, tangible act of agency for individuals who engage in the process.
The primary purpose of an ACP is to protect an individual’s autonomy and dignity by helping to ensure they receive healthcare which is consistent with their values, goals and preferences.2,14,15 Autonomy refers to a person’s capacity to act freely in accordance with a self-chosen plan.16 An individual’s right to autonomy and maximal ownership of healthcare decisions is often reflected in modern codes of ethics17 and global policy.18 Further, the Medical Board of Australia has linked respecting a person’s rights to make their own decisions, including via ACP, with good medical practice.19 When working effectively, ACP support a person’s autonomy by representing the person who exercised agency whilst competent, in order to guide decisions whilst incompetent.14,20
Advance care planning has attracted much discourse surrounding the practical and moral shortcomings of future-focused healthcare decisions.21–23 Contentions include inadequate instructions;24 conflicted or incapable surrogate decision-makers;25,26 the potential of the person to have changed their mind, and limited capacity of the person to have anticipated the presenting circumstances.27 Further, once deemed incompetent, a person is unable to override their earlier decisions, thus binding the person to their earlier “self”. Such a situation raises ethical concerns because of the threat to current autonomy.21 Additionally, individualistic interpretations of autonomy have been criticised for their failure to consider social contexts, with some ethicists instead proposing a “relational autonomy” approach that includes socially embedded insights.13 Not surprisingly then, a recent scoping review found hospital doctors globally have identified numerous apprehensions about the application of ACP in practice.28 Nevertheless, the novel coronavirus disease 2019 (COVID-19) pandemic has been associated with healthcare systems’ renewed interest in ACP in an effort to better meet the needs of both patients and doctors.29,30
The first author (DC) of this study is a psychologist specialised in major neurocognitive disorder (often referred to as dementia). As a result, DC has held a clinical role assisting people living with dementia to better understand their legislated rights. However, both clinical and personal experience has shown that ACP application during hospitalisation has been inconsistent, and the factors associated with application were unclear. Consequently, attempted agency expressed through an ACP may be associated with ethical dilemmas impacting persons involved with caring at end-of-life. Collectively, arguments suggest that ACP may not reliably meet the needs of end-users: PWND, family or friends, and healthcare professionals.
In Queensland (Australia), legislation provides competent adults with the right to complete a statutory ACP, namely an Advance Health Directive (AHD). For an AHD to take effect, the person (known within the AHD as the principal) must be without capacity to make the current healthcare decision. Doctors are not obliged to apply directions which they have reasonable grounds to consider are inconsistent with good medical practice or uncertain, or the doctor reasonably believes that circumstances have changed, and application would be inappropriate. If an AHD refuses life sustaining treatment, certain illness criteria must be met. (Please see Supplementary Figure 1). Alternatively, competent adults may utilise a non-legally binding form (known as a Statement of Choices) to guide decision-makers about their healthcare wishes, values and beliefs.
For this research, an ACP was defined as a written statement articulating future healthcare preferences or directions, owned by the person and applicable only during incapacity to consent. It is important to note that in this manuscript, we refer to the overarching concept of ACP to indicate written documentation of a person’s healthcare preferences. Where relevant to distinguish legislated applicability or to report specific findings arising from the data, ACP type (AHD or Statement of Choices) are differentiated. The Queensland AHD in effect during data collection was Version 4 and the Statement of Choices was Version 5.1. (Please see Supplementary Figures 2 and 3 respectively).
Materials and Methods
Aims
This study constitutes part of a broader constructivist grounded theory [CGT] research study exploring the factors which influence hospital doctors’ application of the ACP of incapacitated PWND. Some aspects of the study, such as the potentially conflicting interests of bedside agents, are considered in more detail elsewhere (please see31) With the purpose and representation of ACP being to keep a person’s autonomy central to medical decision-making, we set out to better understand: the attitudes of multidisciplinary healthcare professionals (referred to as “clinicians”) towards the usefulness of ACP; and the elements that influence how doctors apply ACP to treatment decisions for this group. This research represents an important step in understanding the factors associated with application of ACP to treatment decisions of hospitalised PWND, and ultimately, will help to inform a grounded theory. This paper offers a thematic analysis explaining what clinicians perceived as benefits of ACP, and the factors which have been associated with ACP application for this cohort across two regional health service areas in Queensland.
Study Design
An inductive thematic analysis approach, informed by the CGT principles of Kathy Charmaz32 was used to explore and describe the perspectives hospital-based doctors, allied health and nurses in relation to the intended or actual role of ACP in healthcare decision-making. Grounded theory has become valued for its suitability to the explanation of complex and poorly understood medical-context phenomena.33 We used theoretical sampling and CGT analytic tools to probe participants’ implicit meanings and actions to better understand the processes associated with making recommendations about completing an ACP, or treating a PWND during illness when an ACP might reasonably be expected to take effect. CGT provided a trustworthy, inductive means through which to construct a theory “grounded” in rich data.
Ethical Approvals
The National Statement on Ethical Conduct in Human Research34 underpinned all aspects of the study. Multisite approvals were granted by Townsville Hospital and Health Service Human Research Ethics Committee (54125) and James Cook University (H7930). Verbal and written informed consent from participants was approved by both ethics committees, and participants consented to publication of anonymised responses. Participant access to professional support if distress occurred was incorporated into approvals. This paper was informed by the Consolidated Criteria for Reporting Qualitative Research (COREQ) and data were maintained in accordance with the Declaration of Helsinki.
Participants and Recruitment
Two participant groups were identified using purposive and snowball sampling methods: 1) hospital doctors with experience in decision making with/for this cohort, and 2) allied health and nurse clinicians with experience delivering healthcare to the target cohort in situations where the person lacked decision-making capacity. Snowball sampling was defined as sampling that utilised existing or potential participants to identity other potential participants.35 Whilst doctors were the primary focus of this study, allied health and nurses were included because of their insights into the practices of doctors in the study context. Participants were recruited from two major regional hospitals and three small hospitals. All participants received written and oral information about the study and consented to interviews being digitally recorded and anonymised responses published. Due to geographical distance from the interviewer and several participants’ stated preference to provide only verbal consent, four participants gave verbal consent which was obtained twice: once before and once after digital recording commenced. All other participants provided written consent. Anonymity was assured, and participants were assigned a pseudonym code. Participants were advised that under exceptional circumstances, disclosure of their data could be required by law. Participants were advised of the availability of referral to professional counselling if appropriate, however no onward referral was requested or deemed necessary.
All clinicians were recruited via health service newsletters, snowball referral and bulk emails disseminated by heads of departments. Purposive sampling from units most associated with care at the end-of-life included palliative care, emergency, geriatrics, intensive care, medical oncology, neurology and general medicine. In line with theoretical sampling techniques, some specialities (such as respiratory/renal medicine) and disciplines (such as social workers) were identified and invited to participate. Doctors from the respiratory/renal subspecialty declined participation.
In this manuscript, allied health, nurses and doctors are referred to inclusively as “clinicians”, with disciplines separated only where relevant to distinguish data sources or subject matter.
Data Collection and Analysis
Based on professional experience and research, the authors developed a semi-structured interview guide which was used flexibly to explore factors such the attitudes of clinicians towards the potential benefits of ACP, and the experiences of clinicians in relation to applying the ACP of PWND (see Figure 1). The interview guide was piloted across all groups, then changed iteratively in response to emerging theoretical concepts. Questions were adapted to reflect participant type. Clinicians were asked about their attitudes towards ACP and their utilisation of the ACP process. Interviews were conducted by the first author [DC] and primary advisor [RR], face-to-face or via telephone or “MS TEAMS” online software and ranged from 20 to 70 minutes (mean of 51.9 minutes).
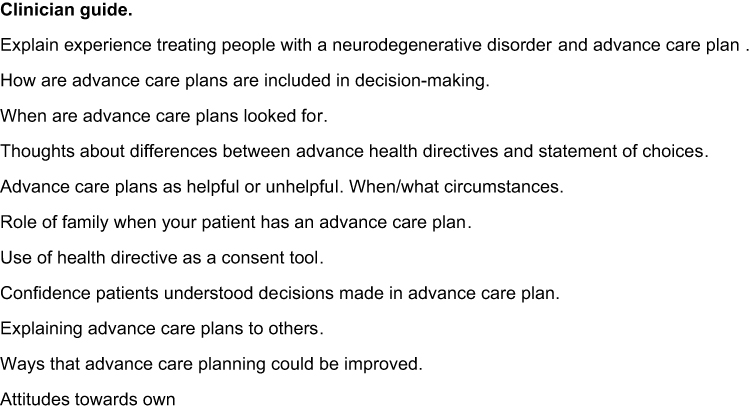 |
Figure 1 Example interview topics. |
All interviews were transcribed verbatim by DC or a professional transcription service. To ensure credibility, each transcript was checked against the recorded interview and further observations and impressions were recorded in memos. DC coded all transcripts whilst another researcher (RR) coded a sample of transcripts, with coding then compared and discussed to enhance confirmability of the data. Coding was conducted line by line using a combination of open and in vivo coding and code books were developed. QSR NVivo 12 software was utilised for data management including organisation and retrieval of transcriptions, storing memos, coding and comparing data, and designing concept map iterations. In line with ensuring trustworthiness of grounded theory data, codes and data were constantly compared, discussed and revised as a research team (DC, RR, DH, MS) increasing confirmability of the data and minimising the potential for personal bias.32 As the analysis progressed, codes were collapsed into categories which captured recurring themes. Reflexive memos were used to explore and interpret our understanding of categories, and diagrams were used extensively to document relationships between themes and to develop an overarching conceptual framework. Data collection and analysis continued until the research team agreed that no new ideas were emerging, and data saturation had occurred.
Results
Participants
A total of 32 people participated between November 2019 and November 2020. Participants represented a broad range of specialties and all self-reported experience treating PWND during incapacity in the context of ACP. Doctors were from subspecialties: emergency, general medicine, intensive care, neurology, medical oncology, geriatrics, and psychiatry. Nurses and allied health were senior clinicians from a broad range of hospital units (see Table 1).
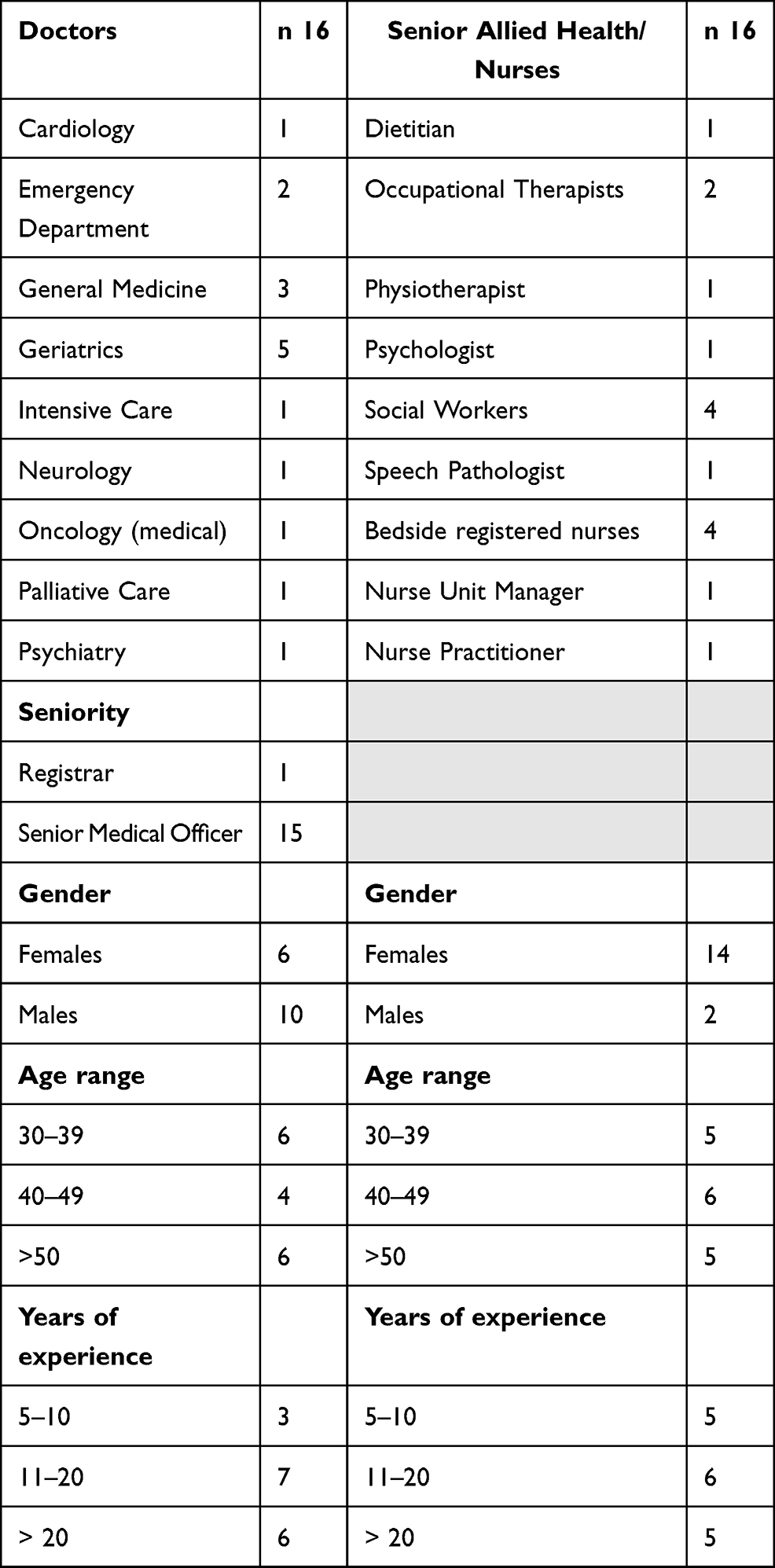 |
Table 1 Participant Characteristics |
Data analysis revealed two main themes: recommending agency through ACP; and limiting agency through ACP. These themes formed the basis of the core category: patient agency (see Table 2). Participants are identified by letters: AH – Allied Health, D – Doctor, RN – Registered Nurse.
 |
Table 2 Example of the Coding Process |
Recommending Agency Through ACP
Clinicians were overwhelmingly supportive of the concept of advance care planning, particularly in the context of neurodegenerative illness or advancing age. Some spoke of ACP being an important means by which thought processes associated with end-of-life preferences of PWND and discussions with family are triggered. Doctors felt more confident discussing treatment limitations with families of PWND who had completed an ACP compared to those who did not have an ACP, suggesting the ACP process extends benefits beyond the PWND to both family and doctors.
When reflecting on their own potential agency as healthcare consumers, only three clinicians (allied health, nurse and doctor) had completed an AHD. Some clinicians stated they might complete an AHD when of advanced age or diagnosed with a chronic illness, whilst others indicated an intention to complete an AHD, but had not. Clinicians overwhelmingly perceived that their family were capable of making decisions and advocating on their behalf. This may reflect the socio-cultural status of highly educated and health literate clinicians with a practice culture favouring contemporaneous, shared decision-making with patient representatives. In relation to their patients, however, clinicians supported PWND’s agency through ACP, with two subthemes arising from the data: having a voice in future healthcare, and relieving family of burden.
Having a Voice in Future Healthcare
Clinicians considered that ACP provide a valuable means by which PWND could represent themselves when they otherwise could not. Clinicians maintained that PWND should be encouraged to engage in advance care planning to make known their healthcare directions so that healthcare could be aligned with their directions.
It’s a way of having a voice when you have no voice. RN2
They may be in a position one day where they won’t be able to make their wishes heard and if they can’t be heard then it can cause a lot of distress for them and their family members. D9
So it’s up to you and what you want, and it’s important that we have these documents … So I tell them that the best thing to do is an Advance Health Directive and I always say, “So you don’t get something done to you that you don’t want” that’s the main thing ….advance care planning is really for when they are not able to tell us what they want … D2
We explain to people that with the health directive, “When you can’t make decisions, it makes decisions for you.” RN3
Although people who generate an ACP are under no legal obligation to share their decisions or decision rationale with a third party (such as family), they are encouraged to do so within Queensland ACP templates and Australian ACP promotional materials.15,36 Interestingly, clinicians appeared to associate much of the benefit of ACP with the likelihood that PWND would discuss their decisions with family. Accordingly, doctors expected that family would have a sound understanding of the PWND’s healthcare priorities and therefore could speak on the PWND’s behalf. Doctors then practiced what we describe as a relational autonomy approach to decision-making by engaging family to represent the voice of the PWND. Relational autonomy refers to complex and intersecting social connectedness and relationships between people37 who are invested in, and affected by, the life or death outcome of the PWND.
It’s actually pretty uncommon that the person who makes one hasn’t discussed to some degree with the family members, close family members anyway, what they’re going to put in there. … it is really hard for family members in a highly emotional situation to think clearly and try to put themselves in the shoes of their loved one because they’re part of the picture in a different way. … D11
If they [family] understand and know your wishes, they’re more likely A). to follow them if you lose capacity and B). to be accepting because it’s very distressing to find yourself having to make choices on someone’s behalf when you don’t know what their preferences are … family who know will often respect much more easily than those who don’t. D1
[When a PWND has an AHD] It means that they’ve thought about it, which is good, particularly if they’ve got a chronic condition which is lethal then that’s very important that we get hold of that directive and to find out what their thoughts and feelings are, particularly if we haven’t got good access to next of kin. Next of kin, of course, is very important indeed and they usually have been involved … and they can usually give us a glimmer as to what’s in that directive but we like to see the directive as well …. None of these decisions are light, they’re very carefully made decisions and they’re always done with the relatives. D5
It works out well if conversations have been had with the patient and with their family and very clear guidelines are written out beforehand. D9
In relation to generating an ACP, doctors typically recommended that people explicitly discuss their choices and preferences with their family. This advice reflected awareness that end-of-life is a relational process,12,13 impacting others (such as family and healthcare staff) who might also exercise agency in decision-making, potentially conflicting that of the patient.31
I think one of the most useful things for the family or the closest enduring relative or friend or whoever is in that substitute decision making role is, I think it’s very important that they personally understand the wishes and preferably not just see the document, but be part of the conversation to frame it. D4
In the end there’s always the bad bit, and so if you accept that it’s a finite life, you need to prepare for that and that means thinking about what’s important to you, writing them down, communicating it to your family in case you lose capacity … and it’s really important to share those things with your doctors and your family so you’re more likely to get the outcomes you decide. D1
I do explain it’s quite convoluted. It’d be good to chat to their family before or whilst doing it, so they’re aware and everyone’s happy and there’s no conflict when the time comes to put that into place. D2
Just try to let them know that, look, this is something serious, they need to think about and need to let your family members know [about preferences for treatment]. D7
Despite asserting that ACP extend the patient’s voice, most doctors conceded they do not reliably refer to ACP. Additionally, some doctors expressed scepticism that PWND’s agency via ACP would be valued by future treating doctors, with implications for advising people to complete an ACP. Therefore, variation in practice culture leaves patients vulnerable to individual preferences of treating doctors.
[Interviewer: How confident are you that your doctor colleagues will follow an ACP?] Not super confident and I think that that’s just based on predetermined thought processes and depending on if their value systems really changes things. D8
I am not confident at all that the effort that people put into trying to make sure that their wishes are known and adhered to, actually, that it is rewarded. I don’t believe that they’re always searched for and thought about … the ARP [Acute Resuscitation Plan] is often done by a statutory health attorney, and this person [PWND], themselves, did an AHD, and that’s not what’s been used to inform the ARP. D2
So working in [UNIT], for instance, where everyone coming in will likely need surgery which has a lot of attendant risks, usually what they will do is they will have an informal chat with a statutory attorney for health matters, or the patient. They don’t usually refer to an advance health directive. D3
Relieving Family of Burden
Despite patient healthcare being the central purpose of medical decision-making, results revealed that doctors extend considerable empathy towards families, indicating a tendency to take a relational autonomy view when caring for patients. Accordingly, clinicians perceived ACP as helpful because they alleviate family member’s burden when making difficult decisions.
I’ve witnessed that they have the comfort of knowing that their decisions are backed up by their relative [PWND]. It’s never easy to say stop providing active management but at least they can say well that’s what he wanted. D9
It takes that responsibility away and it relieves the burden a little because your family knows this is your choice. AH8
Doctors recognised the emotional tole and long-term consequences felt by families involved in end-of-life decision partnerships. Therefore, ACP to lessen burden was endorsed. Although well intended, it was evident that doctors at times coerce individuals to engage in ACP, a process which ethically and legally must be voluntary. In so doing, the burden of decision-making is imposed on patients as a means of protecting family.
I would usually use this phrase that “It is not fair for your daughter or your son to make these decisions …. So to be fair to everyone I think while you can, you probably should make it very clear what you want done” D7
Mostly to point out that it’s going to protect their family members from having to make really difficult decisions in really difficult moments. D11
Collectively, results revealed that doctors recognised the potential benefits of ACP, not only for establishing a person’s healthcare priorities, but also as a mechanism for guiding and relieving family. Doctors also recognised and valued the importance of relationships that surround a dying person, thus involving these relationships in the decision process.
Limiting Agency Through ACP
Perhaps not surprisingly, the critical limitation to agency through ACP was the necessity for doctors to agree with the directions expressed in the ACP. Most doctors explicitly prioritised family consent to healthcare, rather than defer to the statutory AHD. Doctors stated they may rely on an AHD if no family were present. ACP application data revealed three subthemes: recognising the PWND was dying; good medical practice; and “the dance” with family.
Recognising the PWND Was Dying
Recognising that the PWND was dying was broadly endorsed as the primary trigger for doctors to read and consider applying the person’s ACP. Clinicians commonly asserted that doctors are treatment focused and only apply an ACP when illness is irreversible and end stage.38,39 Despite the availability of tools designed to assist doctors to recognise dying in people with diseases such as Parkinson’s Disease38 and dementia,39 prognosticating end-stage neurodegenerative illness (in the absence of cancer) was considered to be particularly challenging because of unpredictable illness trajectory. Accordingly, doctors asserted they see fewer “flags” to review ACP. Therefore, although the purpose of ACP is to give voice during periods of voicelessness, the inclusion of the person’s voice may only occur after (potentially unwanted) medical intervention consistent with hospital doctors’ treatment culture and their inability to recognise palliative phases of neurodegenerative illness until death is imminent.
I wouldn’t be doing it [reading ACP] the first time I see a patient because I’m supposed to be there to help them. I look more at the advance care planning when I start seeing that things are deteriorating, or when I see that …. it’s pretty much at the end … Only when it’s pretty clear that things are not going the right way, that’s when they would apply it, only last resort. Health wants to have them [AHD] just for the very, very last minute, not for in between, not for beforehand, because we are here to help people. D10
I think, again, the more unwell a patient is, the earlier we will look for that plan. D12
The way I look at ACD [Advance Care Directive] implementation is different for cancer patients compared to all the other end stage diseases, which are equally bad, but for some reason, we are cancer focussed when it comes to death. So, cancer patients, they end up at an acute end emergency department, there are enough flags raised, “oh, this patient has cancer, has a prognosis of three months, there’s an ACD, should we just comply with it”, very easily. For non-cancer patients, so to some extent, because of the studies that cancer – the research that has gone on in cancer, we have life expectancy slightly more clearly delineated compared to advanced renal disease, or advanced cancer, dementia, where you don’t really say “well, you are at this stage, your life expectancy is five years, two years, one year”. Even people with a life expectancy of six months, we don’t know if they have severe dementia. So there is no flag raised at the front end. D6
You know, things like MS [Multiple Sclerosis] and motor neurone and all that, they can be going up and down and you don’t know if this is it or if it’s not … these neuro ones can be hard because you just don’t know … Whereas cancer, you just look at the blood results and you can pretty well prognosticate pretty accurately. RN2
There’s a lot of grey in terms of the medical team may not know the prognosis or they may not know whether this is a curable or recoverable illness that the person has … I’ll often feel troubled because I’ll think they keep giving the patient all of this stuff and I’m pretty sure they’re going to die in a month, a week or a couple of weeks but the medical team aren’t saying that. They’re saying, “No, no, no, we’re aiming for curative intent … ” So the dialogue is very much that the patient’s not dying … but I kind of, like in my gut I’m kind of like … they’re not going to survive, and then it’s resulted in their last few weeks have been full of potentially unnecessary medical treatments and interventions. AH9
Good Medical Practice
Pursuant to the Guardianship and Administration Act 2000 (Qld), doctors in Queensland are excused from applying AHD directions which they deem inconsistent with good medical practice. Not surprisingly then, most doctors stated they would only apply directions which they judged to be consistent with good medical practice and in the person’s best interests. In evaluating good medical practice, doctors considered healthcare principles such as beneficence and nonmaleficence.
I would definitely discuss it with the family and say “the advance document said this, we need to think about what’s in their interest” … medicine has great capacity to prolong life, but doesn’t always bring benefit or there comes a time when the benefits are outweighed by the harm … the issue words were good medical practice and I think that’s a subjective thing. D1
It’s Advance Care Planning for your wishes but it has to be … consistent with accepted good medical practice … Now if it’s a different matter like it’s a neurodegenerative thing, someone’s got a motor neurone disease and they come in with aspiration pneumonia and there’s no possibility of them getting better and the health directive says “don’t do anything”, well we wouldn’t do anything, that’s fine because that’s consistent with good medical practice and it’s consistent with what they thought and it fits the scenario that they were likely talking to their GP about … The problem is, is when you’ve got an Advance Health Directive and no relative. And you’ve got somebody who’s unconscious … in neurodegenerative disorders, you know, we would be very loath to, but in that particular situation where they were otherwise well … we’d probably intervene and just fix them overnight and say it was a simple problem and you’re better now. D5
It becomes very challenging when it goes against good medical practice - I use that as a specific legal term - and when family have a dissenting opinion … I think that there also needs to be, in some cases, discussion about good medical care and philosophical changes in care, particularly towards end-of-life. I’ve seen many people say that they want very invasive treatments when you know if they become critically unwell their likelihood of survival is very, very low. And it would be, to use an ethical term, it would probably be a futile medical treatment. And whether or not we actually should give them that option is a real – there’s some nuance there that you need with some clinical experience I think. D8
The treatments that are not really likely to be a great help and they’re actually very burdensome, they cause pain or else they cause a high degree of monitoring or interaction with health staff that is just overall not going to provide a great benefit. And I make that judgement and then use whatever resources I have to try and go towards that direction. D11
As a doctor in this country we are not obliged to provide medical treatment that is futile. D12
In practice, partnering with patients and families and traversing the boundaries between patient autonomy, best interests and good medical practice appears fraught. One doctor described dissonance resulting from the application of an AHD which contravened good medical practice. This case highlights the potential impact of individually autonomous directions that induce discomfort and perhaps unintended consequences for others, such as family and clinicians.
I can tell you specifically about a particular religious group. [PWND’s relative] had very bizarre healthcare ideas or theories or however you’d like to – and [PWND] ascribed to that particular healthcare belief system as well. And it was completely polar opposite to good medical practice. And we had an Advanced Health Directive which, unfortunately, was very non-specific and from a different jurisdiction which made it quite complicated. But, in the end, we managed to navigate a pathway which was consistent with the patient’s healthcare beliefs which was completely opposite of good medical practice. It wasn’t particularly in the family’s best interests either but, I feel, it was in – and everyone in the end came together and was accepting of that decision, I suppose, using the healthcare directive and what is known of her healthcare beliefs … Very challenging, very time consuming. We spent days and days on this case and even when you reflect back on it, I’m still not sure if I did the right thing either. And it’s hard for a medical practitioner or even Allied Health who were involved in that decision-making as well, and family. So it’s quite challenging. D8
“The Dance” with Family
Not surprisingly, both participant groups overwhelmingly considered family to be patient experts and therefore valuable PWND representatives. Interestingly and in contrast to individualistic agency associated with ACP, data showed a strong tendency of doctors to favour a consensus model of decision-making which reflected a relational autonomy reality. Although AHD are intended to provide patient consent, most doctors asserted that it would be rare to apply an AHD without obtaining consent from family.
We try a softly softly … approach, you know, go in and gauge their feelings on things … and then maybe the next day going back in and saying “how do you think they’re doing? I notice that you’re still wanting them to have fluids … you know, it’s clear that his wishes were this and how can we help you get there?” … it’s not black and white … We’ll give them antibiotics for a week or we’ll give them fluids for a few days … as long as it comes under the banner of do no harm to the patient. When to play that, well, it’s not a game but to do the dance I suppose. D9
I fully understand that I probably don’t know that person particularly well either so I probably don’t know what is best for that particular patient either. So, sometimes from a family perspective, they’ve lived with them for 50 years, they’ve been caring for them for 30 and they know what their mum wants when they have lost capacity … I use their judgment because they know them. D8
I don’t think we could say “It’s all there we’re going to follow the health directive, ignore you guys”. We still need to go back to them [family] and say “It’s not working” or “getting worse”, or “we should really stop” … you can’t ignore – you can’t bypass that. D14
That can be quite annoying because, it’s like, well, they’ve got their wishes there, like it’s all written down. But … you still need the family onside and stuff when they’re in hospital. D15
Despite their relational autonomy approach, several doctors referred to tensions between effecting the wishes of the PWND and the practice of partnering with family. Data revealed challenges associated with relational autonomy, in part because family members may not be regularly or proximally involved with the PWND yet become involved at a critical juncture of healthcare. In essence, taking a relational autonomy approach can add complexity to decision-making.
I think that you need to work with the patient, the document and the family member to come up with a plan which is okay. In terms of family, there’s a whole bunch of considerations that need to be taken into account and I use the ‘relative in California’ type syndrome where it can be performed by someone who has no direct involvement in the patient’s care and might not actually be the best person to be making those decisions … So challenging, always challenging. D8
Interestingly, doctors were often aware of a legislated hierarchy of decision-making, yet they frequently referred to relying on a person recorded within medical records as a “next of kin”. In Queensland, a person recorded as next of kin may, or may not, be the lawful decision-maker.
The Health Directive is supposed to be the number one before all else, but in reality, next of kin, for us normally, is like a spouse would be number one. D15
I don’t think that they’re referring to the official hierarchy of consent that we have. I mean, some states have a very explicit hierarchy of consent, Queensland not so much. I think it’s really whoever presents themselves as being somebody who’s in a close and continuing relationship. I think it’s just whoever presents themselves as next of kin. Sometimes it’s formalised, so if you get nursing home patients it will be next-of-kin is listed, sometimes it’s whomever is listed in the existing hospital records. It’s a bit ad hoc. D3
[How is a substitute decision maker ascertained?] Sometimes on their care facility’s pages of information they send they’ve got an EPOA or whatever, or it’s just the next of kin and then you phone the next of kin and ask them. D12
Despite the potential power of life altering healthcare directions contained within an AHD, the written mode by which patients retain “a voice” is controlled by others. Some doctors considered that AHD lacked nuance and therefore applicability to most situations. Several chose to read an AHD only in situations where medical options had been exhausted, or no family were available to provide information or to contest the PWND’s decisions. In the absence of family, ACP provided a useful opportunity to learn about a patient’s preferences. Consequently, absence of family reduced one possible barrier to ACP application, and therefore PWND agency. This factor has been addressed in detail separately.31
Healthcare Directives are quite often “if there’s no quality of life” or “it’s not reversible” or whatever, like it’s quite broad in its terminology and stuff … if there is a Healthcare Directive [and] there is no family to contend it … we can translate that onto an ARP [Acute Resuscitation Form] form like saying that this is the patient’s wishes. D15
Collectively, the extent to which doctors engaged family consent in a shared treatment plan revealed a tension between individualistic agency through ACP as provided for in law, and application requirements as perceived by doctors.
Discussion
This study provides insights into the attitudes of clinicians towards ACP as a mechanism for agency of PWND. Whilst there was considerable support for ACP, the realisation of agency of PWND was limited by family and doctors who asserted their own agency as contemporaneous decision-makers. We found evidence that agency through ACP was usually only actualised when curative options had been exhausted and the person was dying. Broadly, despite the PWND’s attempt to exercise agency through an ACP, doctors’ attitudes reflected a collective, relational autonomy reality. Specifically, the extent to which doctors engaged with their patients’ ACP was associated with doctors’ capacity to recognise approaching death, and further, the importance doctors placed on relational autonomy through shared decision-making with family.
Recommending Agency Through ACP
In line with modern ethical practice principles, a common theme throughout this study was the importance doctors placed on respecting the healthcare priorities of their patients. As with another Queensland-based study40 clinicians overwhelmingly supported the concept of ACP as a means of individuals taking healthcare ownership. Further, ACP represented an important mechanism through which to reduce burden felt by family. Comparable with the findings of Leder et al,41 some clinicians asserted that due to the emotional nature of a loved family member’s death, ACP are often more valuable to family than to doctors. In this study, doctors recognised complex social and cultural underpinnings of their patients’ autonomy, beyond that implied by individualistically oriented ACP.
The consistency with which doctors acknowledged the connection between patient and family revealed a tension between individualised autonomy as provided by Queensland law (through AHD), and the interconnected nature of relationships recognised by clinicians. As a measure of the importance placed on patients’ significant relationships, doctors considered family should share in temporal treatment decisions. Therefore, family were assigned a partnership role, sometimes by interpreting ACP relevance in the given circumstances. Not surprisingly then, doctors generally recommended that the ACP process should include dialogue with family to facilitate decisional agreement. In essence, realisation of agency through ACP of PWND reflected a philosophical dispute between legislated individual-leaning agency and the practices of doctors which favoured a collective (or relational) agency approach.
Limiting Agency Through ACP
Agency through ACP for PWND as inpatients is clearly complex. Despite advising consumers that ACP provide a voice for the voiceless, most doctors constrained this voice by not reading ACP unless treatment options were exhausted and death appeared imminent. Evidently, some doctors do not recognise,39 or acknowledge PWND deterioration, and application of ACP is delayed. In line with other studies,40,42–44 doctors emphasised that ACP are only applicable when consistent with good medical practice and in the person’s best interest. Best interest judgements, however, are often influenced by socially constructed norms10 and potentially unconscious values associated with doctors’ agency.10,45 Despite the legally persuasive AHD being established to apply the patient’s voice to consent or treatment refusal, most doctors did not use them for this purpose. Instead, as stated above and in other research,44 doctors incorporated the voices of family in a medically led, shared decision model on the patient’s behalf.
However well-intended stakeholder actions might be, this study suggests significant limitations to the agency of PWND, at least through ACP, in the hospital context. Doctors consistently presumed that families would have been involved with the person’s ACP and that family are efficient sources of establishing patient preferences. Literature, however, cautions against the reliability of family as informants, with biased and variable capability well documented.46–49 Conversely, others have conceptualised family as ideally placed to enhance patient autonomy, typically through relational knowing associated with their shared history.11 Importantly, cultural variance of both clinician and patient may be associated with end-of-life care preferences50 and attitudes towards the role of family at end of life,51 making cultural sensitivity essential at this time. Doctors in this study adopted a temporal and relational autonomy approach to respecting the healthcare preferences of PWND.
Further important limitations to the individual autonomy model, as represented by ACP, seem relevant to this discussion. For example, Gomez-Virseda, De Maeseneer and Gastmans13 in their review pointed out that certain conditions are required for a decision (such as within ACP) to satisfy ethical autonomy criteria. These criteria include, but are not limited to, that decisions were made without interference (such as coercion) and that the person was sufficiently informed. Current ACP processes in Queensland do not adequately address these requirements. For example, there are minimal protections in place to ensure a person understands the implications of their decisions, and those who do engage in ACP are free to exclude medical advice. Additionally, some doctors in this study admitted pressuring patients to participate in ACP, potentially contravening ethical and legislated prohibition on coercion, and thus inadvertently jeopardising autonomy.
A major contention against individualistic autonomy is the argument that people exist as interconnected beings, as part of a broader social context, and therefore individualised autonomy disregards the social values and autonomy of others.12,13 An alternative interpretation of ethical decision making recognises the different and potentially competing interests to be balanced.12,31 Shared decision-making partnerships between patients, families and clinicians are seen by some bioethicists as more appropriate to end-of-life decisions.12,13 However, people who complete an ACP to restrict involvement of their family, may be disempowered by doctors who presume the supremacy of collective decision-making, or who do not read the patients’ “voice” (expressed through ACP) in a timely manner.
Importantly, legislative and healthcare systems have acknowledged the right of persons to hold views, make choices, and take actions based on their values and beliefs.2,19,36,52–55 However, for good medical practice to be maintained, respect for this right must extend beyond a supportive attitude to supportive actions.16,56 With ACP an institutionally sanctioned offer of choice, it is beholden upon stakeholders to respect an individual’s agency by respecting their ACP. Failure to do so contributes to morally problematic false promises.23 The extent to which an incompetent PWND’s agency is either subjugated behind that of doctors and family, or enriched by relational autonomy, may be open to interpretation by the reader and PWND who are promised a voice through ACP.
Limitations
This study has some limitations. Firstly, we acknowledge that the study may lack cultural relevance to some groups within society who may offer alternative explanations for ACP application. Secondly, the data were collected from a specific region and with a focus on neurodegenerative disorders and relied on self-reported experience of clinicians. Accordingly, results are not intended to be generalised to other populations or all doctors. Thirdly, the first author was known to several of the participants which may have biased their responses. We consider it likely, however, that this factor provided a study strength by supporting participants to reflect about their attitudes and experiences. Fourth, despite efforts to engage doctors from other units and of junior status, the study did not achieve engagement from all sectors or doctor seniority. The study did, however, achieve good representation from senior doctors of varied age, gender, subspecialty, and years practicing. Finally, with data collection occurring during the novel coronavirus disease 2019 (COVID-19) pandemic, positive attitudes towards ACP may have predominated, reflecting a heightened interest in end-of-life care at that time.
Conclusion
In the context of our study, we have examined the attitudes of doctors towards patient agency through ACP and the restricted circumstances within which the ACP is likely be applied to healthcare. We found that doctors prioritised engagement with family for consent to treatment, usually without reviewing the ACP. In essence, doctors practice relational autonomy when they envisage that families understand the person’s likely wishes, and collectively, doctors and family partner in contemporaneous healthcare decision on patients’ behalf. Doctors’ protective concern for family, and their tendency to prioritise active treatment, forms a limitation to realisation of patient agency through ACP. Accordingly, inpatient agency is balanced against judgements of both doctors and family. Further research may herald insights into the system factors which impact ACP application.
Acknowledgments
The authors sincerely thank participants who provided their valuable time and insights. This research was supported by the Australian Government Research Training Program (RTP) and James Cook University Cohort Doctoral Studies Program. The results from this publication are to be included in the doctoral thesis of Denise P Craig which will be uploaded to: James Cook University repository URL: https:// researchonline.jcu.edu.au/.
Disclosure
Ms Craig was financially assisted by the Far North Queensland Hospital Foundation Paul and Dina Kamsler Memorial Award, and the Tropical Australian Academic Health Centre Clinician Researcher Fellowship Scheme. Funders had no further role in the study. The authors have no other conflicts of interest in this work.
References
1. Regan L, Preston NJ, Eccles FJR, Simpson J. The views of adults with neurodegenerative diseases on end-of-life care: a metasynthesis. Aging Ment Health. 2019;23(2):149–157. doi:10.1080/13607863.2017.1396578
2. Australian Health Ministers’ Advisory Council. A National Framework for Advance Care Directives. Australian Government Department of Health and Ageing; 2011. Available from http://www.coaghealthcouncil.gov.au/Portals/0/A%20National%20Framework%20for%20Advance%20Care%20Directives_September%202011.pdf.
3. Awang H, Mansor N, Nai Peng T, Nik Osman NA. Understanding ageing: fear of chronic diseases later in life. J Int Med Res. 2018;46(1):175–184. doi:10.1177/0300060517710857
4. Bryden C, Spiritual Journey A. Into the I-Thou relationship: a personal reflection on living with dementia. J Relig Spiritual Aging. 2016;28(1–2):7–14. doi:10.1080/15528030.2015.1047294
5. Low L-F, Swaffer K, McGrath M, Brodaty H. Do people with early stage dementia experience Prescribed Disengagement®? A systematic review of qualitative studies. Int Psychogeriatr. 2018;30(6):807–831. doi:10.1017/S1041610217001545
6. Watson M, Thomas M. Spiritual and ethical aspects of advance care planning. In: Thomas K, Lobo B, Detering K, editors. Advance Care Planning in End of Life Care.
7. Swerissen H, Duckett S. Dying Well. Report No. 2014-10. Grattan Institute. Available from: https://grattan.edu.au/wp-content/uploads/2014/09/815-dying-well.pdf.
8. Australian Law Reform Commission. Elder Abuse-A National Legal Response: final Report 2017. Available from https://www.alrc.gov.au/publication/elder-abuse-A-national-legal-response-alrc-report-131/.
9. Kabeer N. Resources, agency, achievements: reflections on the measurement of women’s empowerment. Dev Change. 1999;30(3):435–464. doi:10.1111/1467-7660.00125
10. Giddens A, Pierson C. Conversations with Anthony Giddens: Making Sense of Modernity. Stanford University Press; 1998.
11. Robins-Browne K, Hegarty K, Guillmen M, Komesaroff P, Palmer V. The role of relational knowing in advance care planning. J Clin Ethics. 2017;28(2):122–134.
12. Wilson F, Ingleton C, Gott M, Gardiner C. Autonomy and choice in palliative care: time for a new model? J Adv Nurs. 2014;70(5):1020–1029. doi:10.1111/jan.12267
13. Gómez-Vírseda C, de Maeseneer Y, Gastmans C. Relational autonomy: what does it mean and how is it used in end-of-life care? A systematic review of argument-based ethics literature. BMC Med Ethics. 2019;20(1):76. doi:10.1186/s12910-019-0417-3
14. Sudore RL, Lum HD, You JJ, et al. Defining advance care planning for adults: a consensus definition from a multidisciplinary Delphi panel. J Pain Symptom Manage. 2017;53(5):821–832.e821. doi:10.1016/j.jpainsymman.2016.12.331
15. Advance Care Planning Australia. Advance care planning explained; 2020. Available from https://www.advancecareplanning.org.au/understand-advance-care-planning/advance-care-planning-explained.
16. Beauchamp TL, Childress JF. Principles of Biomedical Ethics. Oxford University Press, USA; 2001.
17. World Medical Association. WMA International Code of Medical Ethics; 2018. Available from https://www.wma.net/policies-post/wma-international-code-of-medical-ethics/.
18. Ryan T, McKeown J. Couples affected by dementia and their experiences of advance care planning: a grounded theory study. Ageing Soc. 2020;40(2):439–460. doi:10.1017/S0144686X1800106X
19. Medical Board of Australia. Good medical practice: a code of conduct for doctors in Australia; 2014. Available from https://www.medicalboard.gov.au/Codes-Guidelines-Policies/Code-of-conduct.aspx.
20. Detering KM, Hancock AD, Reade MC, Silvester W. The impact of advance care planning on end of life care in elderly patients: randomised controlled trial. BMJ (Online). 2010;24:340.
21. Davies JK. The concept of precedent autonomy. Bioethics. 2002;16(2):114–133. doi:10.1111/1467-8519.00274
22. Witt K. In defence of advance directives in dementia. Pac Philosophical Quart. 2020;101(1):2–21. doi:10.1111/papq.12292
23. Johnson SB, Butow PN, Kerridge I, Tattersall MHN. Patient autonomy and advance care planning: a qualitative study of oncologist and palliative care physicians’ perspectives. Support Care Cancer. 2018;26(2):565–574. doi:10.1007/s00520-017-3867-5
24. Jimenez G, Tan WS, Virk AK, Low CK, Car J, Ho AHY. Overview of systematic reviews of advance care planning: summary of evidence and global lessons. J Pain Symptom Manage. 2018;56(3):436–459.e425. doi:10.1016/j.jpainsymman.2018.05.016
25. Smith AK, Lo B, Sudore R. When previously expressed wishes conflict with best interests. JAMA Intern Med. 2013;173(13):1241–1245. doi:10.1001/jamainternmed.2013.6053
26. Schenker Y, Crowley-Matoka M, Dohan D, et al. Want to be the one saying ‘we should just let him die’: intrapersonal tensions experienced by surrogate decision makers in the ICU. J Gen Intern Med. 2012;27(12):1657–1665. doi:10.1007/s11606-012-2129-y
27. Mast L. Against autonomy: how proposed solutions to the problems of living wills forgot its underlying principle. Bioethics. 2020;34(3):264–271. doi:10.1111/bioe.12665
28. Craig DP, Ray R, Harvey D, Shircore M. Factors which influence hospital doctors’ advance care plan adherence. J Pain Symptom Manage. 2020;59(5):1109–1126. doi:10.1016/j.jpainsymman.2019.12.008
29. Sinclair C, Nolte L, White BP, Detering K. Advance care planning in Australia during the COVID‐19 outbreak: now more important than ever. Intern Med J. 2020;50(8):918–923. doi:10.1111/imj.14937
30. Funk DC, Moss AH, Speis A. How COVID-19 changed advance care planning: insights from the West Virginia center for end-of-life care. J Pain Symptom Manage. 2020;60(6):e5–e9. doi:10.1016/j.jpainsymman.2020.09.021
31. Craig DP, Ray R, Harvey D, Shircore M. Advance care plans and the potentially conflicting interests of bedside patient agents: a thematic analysis. J Multidiscip Healthc. 2021;14:2087. doi:10.2147/JMDH.S314664
32. Charmaz K. Constructing Grounded Theory.
33. Wong RE, Weiland TJ, Jelinek GA. Emergency clinicians’ attitudes and decisions in patient scenarios involving advance directives. Emerg Med J. 2012;29(9):720–724. doi:10.1136/emermed-2011-200287
34. National Health and Medical Research Council. Australian Code for Responsible Conduct of Research; 2018. Available from https://www.nhmrc.gov.au/about-us/publications/australian-code-responsible-conduct-research-2018.
35. Howie, L. (2010). Narrative enquiry and health research. In: Liamputtong P, editor, Research methods in health foundations for evidence-based practice. South Melbourne: Oxford University Press. 2010:77–90.
36. Queensland Government. My Care My Choices. Advance Care Planning; 2019. Available from https://metrosouth.health.qld.gov.au/acp/explained.
37. Mackenzie C, Stoljar N. Relational Autonomy: Feminist Perspectives on Autonomy, Agency, and the Social Self. Oxford University Press; 2000.
38. Richfield EW, Johnson MJ. Palliative care in Parkinson’s disease: review of needs assessment tools. Ann Palliat Med. 2019;9(Suppl 1):S6–S15. doi:10.21037/apm.2019.09.18
39. Browne B, Kupeli N, Moore KJ, Sampson EL, Davies N. Defining end of life in dementia: a systematic review. Palliat Med. 2021;02692163211025457. doi:10.1177/02692163211025457
40. Willmott L, White B, Tilse C, Wilson J, Purser K. Advance health directives: competing perceptions, intentions and use by patients and doctors in Queensland. QUT Law Rev. 2013;13:30. doi:10.5204/qutlr.v13i1.532
41. Leder N, Schwarzkopf D, Reinhart K, Witte OW, Pfeifer R, Hartog CS. The validity of advance directives in acute situations - A survey of doctors’ and relatives’ perceptions from an intensive care unit. Dtsch Arztebl Int. 2015;112(43):723–729. doi:10.3238/arztebl.2015.0723
42. White B, Willmott L, Cartwright C, Parker M, Williams G, Davis J. Comparing doctors’ legal compliance across three Australian states for decisions whether to withhold or withdraw life-sustaining medical treatment: does different law lead to different decisions? BMC Palliat Care. 2017;16(1):63. doi:10.1186/s12904-017-0249-1
43. White B, Willmott L, Williams G, Cartwright C, Parker M. The role of law in decisions to withhold and withdraw life-sustaining treatment from adults who lack capacity: a cross-sectional study. J Med Ethics. 2017;43(5):327–333. doi:10.1136/medethics-2016-103543
44. Moore N, Detering KM, Low T, Nolte L, Fraser S, Sellars M. Doctors’ perspectives on adhering to advance care directives when making medical decisions for patients: an Australian interview study. BMJ Open. 2019;9(10):e032638. doi:10.1136/bmjopen-2019-032638
45. Billings JA, Krakauer EL. On patient autonomy and physician responsibility in end-of-life care. Arch Intern Med. 2011;171(9):849–853. doi:10.1001/archinternmed.2011.180
46. Shah SGS, Farrow A, Robinson I. The representation of healthcare end users’ perspectives by surrogates in healthcare decisions: a literature review. Scand J Caring Sci. 2009;23(4):809–819. doi:10.1111/j.1471-6712.2008.00674.x
47. Pope TM. Legal fundamentals of surrogate decision making. Chest. 2012;141(4):1074–1081. doi:10.1378/chest.11-2336
48. Kwak J, Wallendal MS, Fritsch T, Leo G, Hyde T. Advance care planning and proxy decision making for patients with advanced Parkinson disease. South Med J. 2014;107(3):178–185. doi:10.1097/SMJ.0000000000000075
49. Fritch J, Petronio S, Helft PR, Torke A. Making decisions for hospitalized older adults: ethical factors considered by family surrogates. J Clin Ethics. 2013;24(2):125.
50. Frost DW, Cook DJ, Heyland DK, Fowler RA. Patient and healthcare professional factors influencing end-of-life decision-making during critical illness: a systematic review. Crit Care Med. 2011;39(5):1174–1189. doi:10.1097/CCM.0b013e31820eacf2
51. Bullock K. The Influence of Culture on End-of-Life Decision Making. J Soc Work End Life Palliat Care. 2011;7(1):83–98. doi:10.1080/15524256.2011.548048
52. Queensland Clinical Senate, Health Consumers Queensland. Charter for care of adult patients at the end of life. Queensland Government. Available from https://clinicalexcellence.qld.gov.au/priority-areas/clinician-engagement/queensland-clinical-senate/publications.
53. Queensland Government. Advance Care Planning Clinical Guidelines; 2018. Available from https://clinicalexcellence.qld.gov.au/priority-areas/service-improvement/improving-care-end-life-queensland/care-plans-clinical-tools.
54. Queensland Government. Advance Care Planning; 2016. Available from https://clinicalexcellence.qld.gov.au/priority-areas/service-improvement/improving-care-end-life-queensland/advance-care-planning.
55. Royal Australian College of General Practitioners. Position Statement: advance care planning should be incorporated into routine general practice; 2012. Available from https://www.racgp.org.au/advocacy/position-statements/view-all-position-statements/clinical-and-practice-management/advance-care-planning.
56. Gutierrez KM. Advance directives in an intensive care unit: experiences and recommendations of critical care nurses and physicians. Crit Care Nurs Q. 2012;35(4):396–409. doi:10.1097/CNQ.0b013e318268fe35
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.