Back to Journals » Patient Preference and Adherence » Volume 19
Multi-Stakeholders’ Perspective on Enhancing Health Literacy for Effective Management of Tuberculosis-Multimorbidity in Odisha, India
Authors Panigrahi S, Sahoo KC, Pradhan R, Parida D ![]() , Sinha A, Chauhan A, Rehman T, Bhattacharya D, Pati S
, Sinha A, Chauhan A, Rehman T, Bhattacharya D, Pati S ![]()
Received 5 June 2025
Accepted for publication 13 September 2025
Published 15 November 2025 Volume 2025:19 Pages 3633—3646
DOI https://doi.org/10.2147/PPA.S544825
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Sucharita Panigrahi,1,* Krushna Chandra Sahoo,1,2,* Rachita Pradhan,1 Debasini Parida,1 Abhinav Sinha,1,3 Arohi Chauhan,3 Tanveer Rehman,1 Debdutta Bhattacharya,1,4 Sanghamitra Pati1,3,5
1Department of Microbiology and One Health, ICMR-Regional Medical Research Centre, Bhubaneswar, OD, India; 2Health Technology Assessment India, Department of Health Research, New Delhi, India; 3South Asian Institute of Health Promotion, Bhubaneswar, OD, India; 4Academy of Scientific and Innovative Research, New Delhi, India; 5Indian Council of Medical Research, New Delhi, India
*These authors contributed equally to this work
Correspondence: Sanghamitra Pati, ICMR-Regional Medical Research Centre, Chandrasekharpur, Bhubaneswar, OD, India, Email [email protected] Debdutta Bhattacharya, ICMR-Regional Medical Research Centre, Chandrasekharpur, Bhubaneswar, OD, India, Email [email protected]
Purpose: Effective management of tuberculosis-multimorbidity is crucial to reducing disease burden and preventing complications. While studies have explored the role of health literacy in improving TB-treatment adherence and self-management, few have addressed how a collective, multi-faceted approach can optimize the management of TB-multimorbidity. This study aims to bridge these gaps by exploring how various stakeholders perceive health literacy and its role in managing TB-multimorbidity, ultimately providing a more holistic understanding that could guide policy interventions and healthcare strategies in India.
Methods: A qualitative study was carried out among multiple stakeholders engaged in the management of TB-multimorbidity in Odisha, India. A total of 27 in-depth interviews and 13 key informant interviews were conducted. The data were digitally recorded, transcribed, and translated into English. A thematic framework analysis of stakeholder perceptions, guided by the Health Literacy Instrument for Adults (HELIA), was performed. HELIA informed our interpretation by structuring coding around its literacy dimensions, including access, understand, appraise, and apply, which allows to map interview insights onto literacy-related barriers and facilitators to ground the interpretation of the theme in a validated health-literacy framework.
Results: The findings explored the significance of health literacy in the management of TB multimorbidity. Information gaps exist in TB materials concerning comorbidities. Furthermore, low-literacy patients often faced cultural and semantic challenges, and they relied on community networks; however, the high-literacy patients trusted digital information. The literacy levels many times shape the care plan and patient navigation pathways. The navigation difficulties indicate the possible use of community health workers as trusted guides. The participants suggested including visual tools, improved provider training, and integrated IEC materials addressing multimorbidity, with clear implications for policy and practical healthcare interventions in India to enhance accessibility, trust, and patient-centred care in India.
Conclusion: The study indicates the need for concrete and actionable steps to improve TB-multimorbidity management in India, including the development of accessible multilingual materials, enhancing provider training in health literacy and communication, and strengthening trust and navigation through community and system-level supports. We recommend piloting and evaluating these targeted interventions to generate practical guidance for policymakers and practitioners.
Plain Language Summary: This study focuses on improving health literacy to better manage tuberculosis patients having other chronic illnesses in India. This study documented the experiences and opinions of patients, family care-givers, community health workers, and primary healthcare providers. This study highlights health literacy’s role in treating patients with tuberculosis and other conditions like diabetes, hypertension or mental illness. While healthcare providers recognize the need for clear communication, many resources only address tuberculosis, leaving out other co-occurring morbidities. Patients with low literacy often struggle with managing their medications and rely on family for help. The study highlights the need for better communication, training for providers, and tailored approaches to empower patients and improve health outcomes. To improve patient care, we need to make health information easier to access, provide better training for healthcare workers, and build trust and teamwork in the healthcare system. It’s important to use personalized and culturally aware methods to help patients understand and manage their health better.
Keywords: health literacy, tuberculosis, multimorbidity, stakeholders, odisha
Introduction
Despite continuous efforts at the global, regional, and national levels, Tuberculosis (TB) continues to be the major infectious cause of death worldwide.1 It often co-exists with many non-communicable diseases (NCDs) and certain communicable diseases (CDs), which adversely affect each other.2 However, TB multimorbidity – TB with one or more other chronic conditions is largely overlooked in current health programs.3–6 In the wake of managing and intervention strategies to alleviate system burden, it entails patients’ active involvement in their disease management.7 The “health literacy” (HL) is a multifaceted construct that encompasses the knowledge, competencies, and critical abilities necessary to effectively access, appraise, comprehend, and apply health-related information to influence behaviour patterns to improve population-level health outcomes.8–10 In the case of TB-multimorbidity, adequate health knowledge or information plays a vital role in control and management.11–13 Limited health literacy constitutes a barrier to effective healthcare delivery and TB patient care. Along with that, other co-occurring morbidities worsen its symptoms and progression, exhibiting low medication adherence, experiencing high emergency care visits, and depicting an increased risk of hospitalisation.14–18 Therefore, it is important to explore the role of HL in managing TB-multimorbidity.
Tuberculosis is one of the leading infectious killers in India, with a considerable share of patients experiencing multimorbidity, especially diabetes, hypertension, and HIV. The Indian healthcare systems continue to fight with fragmented TB care with variable health literacy across various population characteristics. While global priority for integrated TB care focuses on multimorbidity management, in India, the National TB Elimination Program (NTEP) has limited protocols to enhance multimorbidity management among TB patients.19–22 Addressing the HL has largely emphasised individual behaviours rather than systemic barriers. Furthermore, across the high-burden TB regions in India, the frontline providers – primary health centre physicians, community workers, and family caregivers – often faced practical challenges relating to training gaps. The gaps are mainly misalignment between standardised TB protocols and multimorbidity, trust gaps in formal healthcare, and problems in coordinating care across multiple conditions. The current literature on TB multimorbidity in India has predominantly focused on individual patient behaviours—particularly medication adherence and self-management practices, while largely neglecting the perspectives of healthcare providers, community workers, and carers who shape the care ecosystem. For instance, primary health centre physicians often lack training to manage TB alongside other chronic conditions; community health workers struggle to reconcile standardised TB protocols with the realities of multimorbidity; and family members frequently become de facto care coordinators due to trust gaps in formal health systems.3–8 The above contextual factors in India indicate that research beyond individual-level HL is essential to capture multi-stakeholder perspectives that can illuminate how health literacy, communication, and system navigation improve the TB-multimorbidity management.
This study followed a multi-stakeholder lens to explore how patients, family caregivers, community health workers and healthcare providers perceive health literacy and its role in navigating TB-multimorbidity management. By documenting these perspectives, we aim to identify actionable insights that can inform policy and practice, such as multilingual and pictorial information tools, provider training in health literacy, patient-centred communication, and strengthened linkages between communities and health systems to support integrated, patient-centred care and contribute to India’s TB elimination goals.
Methods
Study Design and Approach
We chose a qualitative study design using a phenomenological approach to snap multi-stakeholders’ perspectives by describing, interpreting, and developing theories about social interactions and personal experiences as they unfold in natural rather than controlled settings. Furthermore, the phenomenological approach, which involves systematic steps of identifying and describing the phenomenon, minimises researcher bias through bracketing. We employed a phenomenological qualitative approach to capture multi-stakeholder perspectives on TB-comorbidity management. This method prioritises participants’ lived experiences and their ascribed meanings in natural contexts, aligning with our goal to understand stakeholder roles and challenges without imposing preconceived theories and assumptions, emphasising detailed accounts of real-world experiences.
Overview of Tuberculosis Management, Study Settings and Participants
The Government of India has implemented the Revised National Tuberculosis Control Program (RNTCP), part of the National Tuberculosis Elimination Program (NTEP) (18). The identification of cases through symptom screening by community health workers (CHWs) and diagnostic testing and reported in the Nikshay portal. Treatment for DS-TB involves a six-month regimen with a four-drug combination, while DR-TB requires longer treatment with second-line drugs. Adherence is monitored through Directly Observed Treatment (DOT) and regular follow-ups. Patients are declared cured based on clinical and microbiological criteria, followed by post-treatment monitoring for relapses.23 The program also promotes community awareness, private sector involvement, and financial support for vulnerable populations.24
This study was carried out in Khurdha district of Odisha, India. In Khordha district, 13 Tuberculosis Units (TUs) are there; among them, six high-TB-burden TUly selected for this study. This study focuses on areas struggling to acquire HL by TB multimorbidity, highlighting the complexities of accessible and understandable information for the patients in Odisha. From our previous quantitative survey on TB-multimorbidity health literacy, we identified patients with only TB and patients with TB-multimorbidity, along with their high literacy and low literacy levels. The most frequent diseases reported were diabetes, hypertension, severe gastritis, asthma, thyroid, chronic back pain, and depression.
A total of 27 patients participated in the study, among whom 12 had only TB, and the remaining had TB with other chronic conditions. The median age of the 27 patients was 42 for males and 33 for females. In terms of educational qualification, three had no formal education, nine had completed their primary level education, even had completed their upper primary education, eight had secondary, and graduate level education. Four males worked in private organisations, and one female worked in a private school. Three fishermen and four males sold vegetables and fruits. Five males and three females worked as skilled labourers, and seven were homemakers. A total of 13 healthcare providers – four CHWs (ASHA: Accredited Social Health Activists), three TB Health Visitors, four Senior Treatment Supervisors, and two physicians from Primary Health Centres (PHCs) – have participated in this study. Patients and healthcare providers were recruited through purposive sampling. Initially, participants and healthcare providers were contacted, followed by an in-person.
Data Collection Methods
We conducted 27 in-depth interviews and 13 key informant interviews using an open-ended interview guide and probes (Supplementary File 1). Data was collected from September to December 2024. All interviews were conducted in the local language (Odia). Standardised prompts and probes were used to elicit more details or seek clarification to identify factors that facilitate or impede patients’ health literacy and use of services. The interviews lasted for an average of 30 (range 20–50) minutes. Patient interviews were conducted in their Semi-structured space, and healthcare provider interviews were conducted at health centres by trained staff familiar with the local language and qualitative interview techniques.
Data Management and Analysis
The digitally recorded interviews were transcribed verbatim and translated into English. In the preliminary phase, the team reviewed a set of transcripts multiple times for data familiarisation, then began coding and identifying themes. We used the thematic framework analysis method to identify and interpret patterns or themes within textual data. In the first step, we familiarised ourselves with the content by immersing ourselves in the data, reading transcripts, and noting key ideas. In the next step, we identify initial codes based on research questions and emerging insights. We had systematically applied the thematic framework based on the Health Literacy Instrument for Adults (HELIA)25 for mapping and interpretation of the entire dataset by coding segments of the text. Rearranged the data according to themes into charts or matrices for comparison by using the MAXQDA software. After the primary check of the results by the third author, consensus was reached through discussions with the other researchers. In order to avoid any misinterpretation during data coding, both Odia and English versions of the transcripts were used. We have reported the results of this study following the consolidated criteria for reporting qualitative studies (COREQ) (Supplementary File 2).26
Data Saturation
Data saturation was achieved when no new themes emerged after conducting 27 in-depth interviews and 13 key informant interviews. The repetition in participant responses confirmed the comprehensiveness of our thematic framework. Although most participants described significant communication barriers, one community worker recounted instances of patients successfully using pictorial medication guides, suggesting that certain innovative approaches may help overcome literacy challenges. These outlier perspectives highlight that while communication barriers are widespread, tailored visual strategies may mitigate some of the challenges faced by low-literate patients.
Trustworthiness
Diverse perspectives from both patients and providers supported the collection of comprehensive and detailed information. The research group covered several disciplinary backgrounds, including public health researchers (SP, RP, DP, AS), domain experts (SP2, KCS, AC), and medical microbiologists (DB). All members of the research team had experience in conducting qualitative research in the tuberculosis and multimorbidity domain. We used the voices of participants and accurately reported their perspectives to ensure the credibility of the findings. Transcripts were verified for accuracy by the research team to ensure the authenticity of participants’ perspectives. Multiple readings and listening of transcripts and audio recordings took place to align with the methodology of thematic analysis for descriptive validity. Furthermore, participants’ voices were relied on as much as possible for interpretation of meaning, alongside the meaning attributed by the researcher. The findings were corroborated with relevant theory in the field of health literacy. Different perspectives and previous work in this domain allowed the researchers to reflect on their personal assumptions about health literacy and the social contexts that influence their reflexivity. We checked multiple sources of information, such as interview transcripts, memos, and relevant theory, during analysis.
We implemented reflexivity and bracketing to enhance transparency and trustworthiness. Researchers maintained reflexivity throughout data collection and analysis to note personal biases and assumptions. Before data collection, team members underwent training on bracketing and bias awareness, and interview guides were piloted to minimise leading questions. We conducted routine peer debriefing and coding meetings to challenge interpretations, and maintained an audit trail of decisions, including memoing and versioning of thematic frameworks. Where possible, we used investigator triangulation and member checking to confirm interpretations with participants, strengthening the study’s credibility.
Results
The findings were presented under five themes: 1) Accessibility of information and communication gaps in the management of TB-multimorbidity; 2) Patients’ understanding of TB-multimorbidity care information, focusing on clear communication and cultural appropriateness, 3) Appraisal of information on TB-Multimorbidity management; 4) Application of information on decision-making for TB-Multimorbidity management; and 5) Navigating the healthcare system for care of TB-multimorbidity.
Theme 1. Accessibility of Information and Communication Gaps in the Management of TB-Multimorbidity
Category 1.1. Information Accessibility in TB-Multimorbidity Management
Healthcare providers were perceived as recognising the importance of effective information and communication in managing TB-multimorbidity. They contend that this information enables the improvement of the care-seeking pathway, coordinated treatment, and accurate diagnosis. They stated that the risk of medication interactions and complications is reduced by the proper counselling and the patient’s literacy on self-management of disease conditions, as all aspects of a patient’s condition are considered and managed appropriately. Furthermore, patient-friendly information facilitates comprehension of the treatment plan, enhances adherence, and addresses any apprehensions or obstacles that patients may encounter. To enhance health outcomes and provide integrated, patient-centred care in the management of TB-multimorbidity, it is imperative to implement effective communication, education, and information practices. According to them, the current IEC materials primarily focus on tuberculosis, neglecting comorbidities like diabetes, hypertension, and mental health disorders.
When we deliver clear, patient-friendly information and maintain open communication, patients understand the treatment plan, seek care promptly, and adhere to medications. Proper counselling and health literacy empower patients to manage all aspects of their conditions, not just TB, and improve the overall care pathway. (Healthcare provider)
The recommendations include creating user-friendly, multilingual, and condition-specific materials, along with visual aids for low-literacy populations. Patients often rely on peers or family for information due to perceived trust issues with healthcare providers and the complexity of managing multiple conditions. Nevertheless, the majority of healthcare providers recognised that current information, education, and communication (IEC) materials primarily address tuberculosis and make little to no reference to the coexistence of TB with conditions such as diabetes, hypertension, or mental health disorders.
When I started working as an ASHA, they provided these materials. I have been using this material since then. I told my patient, if you know, check yourself. I will ask to our sir if you have any doubts. (Community Health Worker)
Participants recommended the design of user-friendly, multilingual, and condition-specific materials that address tuberculosis and its comorbidities, including explanations of symptoms, dietary advice, treatment interactions, and self-care strategies. All health workers interviewed recommended the inclusion of self-explanatory visual aids and audio formats for low-literacy populations. The well-being status of patients with TB multimorbidity was assessed to determine whether integrated care was impeded or supported.
How many times you will ask to someone or got to someone, hard to keep on needing different information for different medications in different times. (TB patient)
Additionally, the lack of perceived trustworthiness among both patients and community health workers may serve as a further obstacle to obtaining health information. Affordability encompasses the nature and quality of the information needed. Patients with tuberculosis multimorbidity, especially older adults, indicated that they sought advice from peers or family members to reduce unnecessary medical facility visits. Patients reported that healthcare providers communicated more effectively in private settings compared to government health facilities.
It is difficult to keep track of many information for multiple medications at various times; how often will you need to ask someone or get someone to help you? (TB Multimorbidity Patient)
Category 1.2. Patient Experiences and Needs
Patients with TB-multimorbidity express challenges in tracking information for multiple medications and often feel overwhelmed by their conditions. Educational attainment influences patients’ ability to seek and understand information; literate patients desire more tailored information, while low-literate patients may avoid seeking information due to anxiety. There is a demand for specialist consultations to address comprehensive health issues, as many patients feel they lack concrete guidance on managing their conditions.
Tracking multiple medications and managing my conditions overwhelms me, and I often avoid seeking information because I feel anxious; I need tailored, clear guidance and specialist consultations to address all my health issues effectively. (TB Multimorbidity Patients)
Certain patients reported that access to information about service availability affected their utilisation of services. Participants indicated that healthcare providers primarily concentrated on tuberculosis, with minimal attention given to extrapulmonary tuberculosis or related comorbidities. Many patients with low literacy reported being inadvertently diagnosed with tuberculosis while seeking care for other health issues. The lack of awareness regarding free and accessible services during periods of multiple health issues often compels individuals to seek more comprehensive information.
Educational attainment influences how patients seek information about tuberculosis. Higher-educated patients are aware of information sources but find relevant details lacking. Conversely, low-literate patients often avoid seeking information due to anxiety and fear, relying on healthcare professionals for guidance. Some literate patients expressed a desire for more tailored information regarding TB and related conditions, beyond general knowledge. They also requested connections with specialists to obtain accurate information and care suited to their specific needs. Overall, there is a clear need for improved communication and resources tailored to patients’ educational backgrounds.
I would like to see someone, who is specialist in these conditions. So that I could talk about all health issues I have been through, what I have had. But, no, I didn’t receive any guidance. Staff, you can go here and there, but not concrete information. (Patient with TB, Diabetes and Hypertension)
The findings of this theme demonstrate that TB-focused IEC materials leave patients with multimorbidity lacking essential information about other conditions. To improve care, providers should offer integrated counselling and use clear visual and audio resources. Policy-wise, the NTEP should broaden its IEC approach to include multilingual materials on diabetes, hypertension, and mental health, supporting better self-management and reducing misinformation.
Theme 2: Patients’ Understanding of TB-Multimorbidity Care Information, Focusing on Clear Communication and Cultural Appropriateness
Category 2.1. Communication Challenges in TB-Multimorbidity Care
Healthcare providers encounter significant challenges in communicating with TB patients who have multiple health issues, especially those with low literacy. This communication gap arises from providers’ feelings of inadequacy and helplessness, stemming from limited resources and high patient loads, resulting in brief interactions. Consequently, healthcare professionals struggle to understand complex medical information, leading to semantic barriers that confuse patients regarding medical terminology, lab results, and prescriptions. These misunderstandings can result in medication errors, missed appointments, and delays in seeking care.
We have a heavy patient load, and giving time to individual patients is difficult. We just observed whether the patient’s condition is improving or not. (Healthcare Provider)
Patients have noted disparities in access to TB-related information based on age, education, and literacy levels. To address these issues, some participants suggested utilising mixed media approaches, such as posters, SMS, videos, street plays, and social media to reach diverse patient demographics. While adult patients expressed a preference for digital interventions, elderly patients favoured verbal, community-based communication. Furthermore, patients reported positive experiences when they received consistent advice from the same healthcare provider, fostering a low threshold for understanding their health conditions. Using informal language facilitated better communication, allowing patients to express their health concerns more easily. Low-literate patients particularly benefited from visual aids, such as pictures and wall paintings, which effectively conveyed information about managing their conditions and understanding treatment processes. Overall, tailored communication strategies are essential for improving patient comprehension and engagement in their healthcare.
I can easily understand information about TB painted on the hospital wall, but nothing is given about diabetes or hypertension. If these conditions are also given in the same way, then I can understand something. (TB-Multimorbidity Patient)
Category 2.2. Training and Resource Gaps for Healthcare Providers
Healthcare providers face significant training and resource gaps in managing TB-multimorbidity conditions. According to them, there is a lack of structured training modules, which hinders effective communication and patient-centered counselling. Providers emphasise the need for regular training sessions that focus on multimorbidity care, communication techniques, and culturally sensitive approaches to cater to diverse patient populations. Many healthcare providers, including ASHAs, have highlighted that the absence of balanced information regarding the risks and benefits of multiple medications leads patients to prioritise TB treatment over other health issues.
Additionally, patients and their caregivers encounter semantic barriers, struggling with complex medical terminology and a limited understanding of laboratory results and prescriptions. This lack of comprehension can hinder effective health communication. One carer expressed frustration over their inability to understand medical reports despite their educational background, indicating a broader issue of accessibility to health information. Many participants suggested that for the smooth management of TB-multimorbidity patients, it is crucial to implement regular training for healthcare providers on identifying overlapping symptoms and managing referral systems effectively. Enhancing communication strategies and providing clearer health-related messages can empower patients and carers, ultimately improving health outcomes for those managing TB with comorbidities.
Regular training for providers to identify overlapping symptoms and explain lab results and prescriptions in plain language would empower me and other caregivers to manage TB with comorbidities more effectively. (Healthcare Provider)
Category 2.3. Patient-Centric Approaches and Cultural Sensitivity
Positive experiences were reported when patients received consistent advice from the same healthcare providers, fostering trust and enhancing comprehension of health conditions. However, cultural factors and perceived power imbalances often hinder open communication, making some patients hesitant to ask questions about their treatment. Low-literate patients frequently felt that healthcare providers did not listen or communicate information in an understandable manner, often due to language barriers.
Doctor said it; it must be ok, or I didn’t know. I couldn’t understand these conditions, but I didn’t want to ask again. (TB-Multimorbidity Patient)
Additionally, cultural perceptions sometimes place healthcare providers on a pedestal, discouraging patients from questioning them. Healthcare providers, on the other hand, expressed challenges related to the lack of specialised care in facilities, complicating their ability to translate complex information and communicate effectively with patients. High-literate patients noted that available resources, whether online or from community healthcare providers, often lacked balanced information regarding the benefits and risks of taking multiple medications for conditions related to TB-multimorbidity. This imbalance led some patients to prioritise TB treatments while neglecting other health issues, highlighting the need for improved communication and resource availability in healthcare settings.
Information available on the internet mainly focuses on single conditions; diabetes and hypertension won’t get cured, so I focused on taking TB medicines. (TB-Multimorbidity Patient)
This theme underlines how provider workload, lack of training, and cultural hierarchies reduce effective patient–provider communication. Regular training on communication skills, use of culturally sensitive language, and incorporation of visual aids can help providers engage with patients more effectively. These findings call for institutionalizing communication training modules in TB and NCD programs and mandating refresher courses for frontline workers like ASHAs and Senior Treatment Supervisors. Such policy reforms can institutionalise patient-centered, culturally appropriate communication across the health system.
Theme 3. Appraisal of Information on TB-Multimorbidity Management
Category 3.1. Patient Information Sources
Patients often struggle to find health information in their native language, leading to confusion, especially among low-literate individuals. They tend to rely on community healthcare workers, treating doctors, family, and peers with similar health experiences for trustworthy information. This preference stems from a belief that shared experiences are more genuine and relatable due to cultural sensitivities, which can delay proper treatment.
Category 3.2. Trust Dynamics
Trust in information sources varies significantly between high- and low-literate patients. High-literate patients critically assess information from multiple websites, often encountering contradictory advice regarding managing multiple health conditions. They seek consistency across sources to validate the information they receive. Rapport with HCPs is crucial for both groups; a strong relationship fosters trust, whereas poor rapport can lead to scepticism and negative evaluations of the information provided. Experiences of discrimination and a lack of systemic knowledge further exacerbate distrust in healthcare professionals, which points to improved communication and culturally sensitive approaches in patient care.
I had thyroid before. Now I have TB and hypertension. According to information I found on the internet, consuming salt is beneficial for thyroid conditions but not advisable for hypertension. What should I do in this situation? (TB-Multimorbidity Patient)
This theme elaborates that patients with higher health literacy often encounter conflicting health information, while those with lower literacy depend primarily on providers or peers for guidance. To address this, healthcare providers should routinely verify patients’ information sources and direct them to credible resources. At the policy level, there is an urgent need to develop standardized, evidence-based health information repositories in regional languages, ideally integrated with existing platforms like Ni-kshay. This dual approach would ensure consistent messaging about TB and its comorbidities, reduce misinformation, and ultimately strengthen patient trust in healthcare systems.
Theme 4. Application of Information on Decision-Making for TB-Multimorbidity Management
Category 4.1. Patient Empowerment and Decision-Making
In the context of TB-multimorbidity management, patients exhibit varying levels of empowerment in decision-making based on their literacy. Low-literate patients often defer entirely to healthcare providers, viewing them as the ultimate experts. This reliance stems from difficulties in understanding treatment necessity and fear of questioning healthcare providers, leading to feelings of overwhelm and lack of agency in their treatment decisions. Conversely, high-literate patients tend to engage more actively, expressing preferences and negotiating treatment options based on past experiences. They appreciate when healthcare providers provide explanations about how their conditions affect daily life, which promotes a sense of autonomy.
I have gone to the facilities. They had given me the medicines for TB and told me to go to a higher hospital. They said my condition is worse; it can’t be treated here. I was scared then. (TB Multimorbidity Patient)
Category 4.2. Barriers to Effective Communication
Despite the potential for shared decision-making, significant barriers hinder effective communication between patients and healthcare providers. A common issue is the lack of clarity regarding which provider is responsible for specific aspects of care, particularly in cases of multiple conditions. Time constraints during consultations further exacerbate communication challenges, limiting opportunities for thorough discussions.
Additionally, patients often report insufficient information about their treatment plans, which contributes to their feelings of helplessness. While some patients express a desire for visual aids to facilitate understanding. High-literate patients specifically advocate for multidisciplinary discussions involving various healthcare providers to enhance treatment management and decision-making.
When I started TB medicine, my head was reeling, I had severe gastritis, and I had black patches on my skin all over. I was also taking medicines for pain. So I told the doctor on my next visit, and he changed my medicines. (TB Multimorbidity Patient)
This theme reveals unequal participation in decision-making, with low-literate patients deferring to providers and high-literate patients negotiating treatment choices. This suggests the need to introduce simple decision aids (visual care pathways, pictorial leaflets) and structured shared decision-making during consultations.
Theme 5. Navigating the Healthcare System for Care of TB-Multimorbidity
Category 5.1. Healthcare Provider Perspectives
Healthcare providers noted a lack of intersectoral collaboration in managing TB multimorbidity, particularly among professionals outside tertiary care settings. While healthcare providers in tertiary facilities reported no issues with comprehensive care due to available resources on-site, those in community settings discussed the potential roles of community health workers like ASHA and community health officers in facilitating patient appointments and follow-ups. This data suggests a need for better integration of services across different levels of care.
If we could train ASHA and other workers present on the field to communicate properly between healthcare providers and patients, guiding them where to go exactly for TB and multiple other conditions, it could reduce our burden. (Healthcare Provider)
Category 5.2. Patient Experiences
Patients reported significant challenges navigating a fragmented healthcare system, particularly when dealing with multiple health conditions. Many felt overwhelmed by the lack of clear communication regarding which specialists to consult for specific health issues, leading to confusion and insecurity. Low literacy patients struggled even more, as they were not adequately informed about the various healthcare organisations and services available to them. They expressed a strong need for health navigators or help helpdesks at healthcare facilities to assist them in understanding and accessing the necessary services, emphasising the importance of improved information and support systems in enhancing patient care.
In a large hospital, there are many rooms and departments. You keep asking staff where to go for TB treatment or for asthma/diabetes care, but they just tell you to go right or left without listening properly. They don’t even listen properly. (Patient Family Care-giver)
This theme highlights that patients often face confusion in navigating fragmented health services. Practically, introducing patient navigators or trained ASHAs to guide referrals can help. Policy should strengthen coordination between NTEP and NCD programs and embed navigation support in TB guidelines to ease provider burden, streamline care, and improve continuity across health levels.
Discussion
This qualitative study explores a range of health literacy barriers and facilitators faced by TB-multimorbidity patients in India. Healthcare providers acknowledge the necessity for effective communication and personalised information regarding TB-multimorbidity; however, existing resources predominantly address tuberculosis, overlooking comorbidities such as diabetes and hypertension. Patients with low literacy often struggle to manage multiple medications and depend on peers or family for support, reflecting trust issues with providers. Communication barriers exacerbate misunderstandings and hinder health outcomes. Trust in information sources varies by literacy level, affecting patient engagement and decision-making, while navigating a fragmented healthcare system poses additional challenges. Key gaps and recommendations are provided in Table 1.
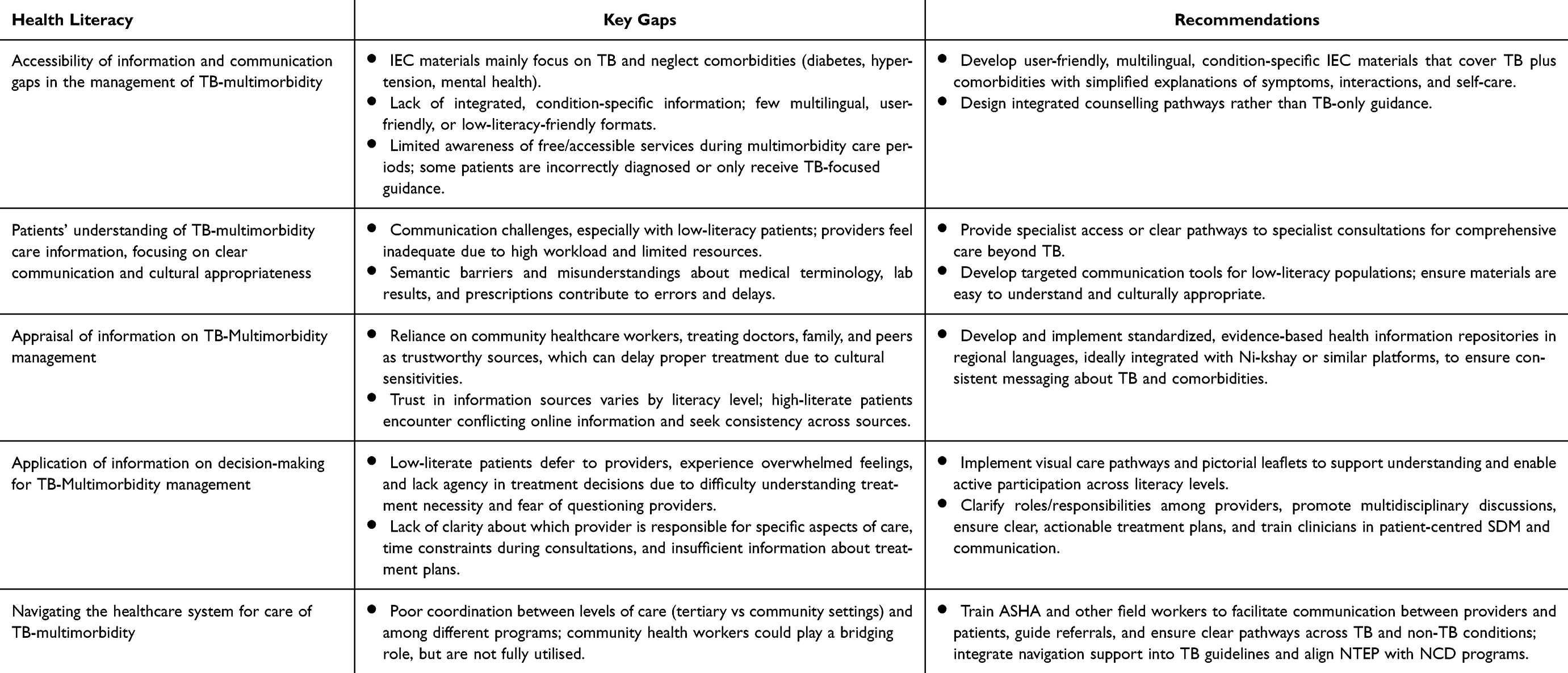 |
Table 1 Key Gaps and Recommendations |
Our findings highlight that access to information, understanding health information, decision-making processes, and navigating the healthcare system are critical, as outlined by the Health Literacy Index Assessment (HELIA) framework.25 According to the previous studies, patients with TB multimorbidity, particularly those with low literacy levels, encounter significant barriers that hinder their ability to manage their health effectively. These barriers include affordability issues, strained relationships with healthcare providers, the use of technical language, poor patient-provider communication, time constraints, and a lack of awareness about available services.11–13 The previous studies also showed that patients often face contradictory information from various sources, leading to confusion and fragmented healthcare experiences. Such challenges are detrimental to treatment adherence and overall health outcomes, especially for those managing multiple chronic conditions simultaneously.26–29 The study shows that patients with low literacy find it hard to judge if health information is trustworthy, so they depend on family or healthcare providers they know, unlike patients with higher literacy who might look for information online or in government documents. To address these issues, patient education materials must be simplified to a sixth-grade reading level, making them accessible to patients and carers with limited literacy. Participants in the study expressed difficulty in understanding existing materials, which were often too technical or overwhelming. Other research supports this observation, indicating that available resources often fail to meet the necessary criteria for effective patient education.30–32 Given India’s diverse population, educational resources must be provided in multiple languages to cater to varying demographics.
Healthcare providers also face obstacles in identifying patient needs and assessing health literacy levels. The study indicates that time constraints, heavy workloads, and a lack of condition-specific materials hinder healthcare providers’ ability to provide adequate support.30–32 The absence of collaborative meetings among specialists and the lack of updated educational materials further exacerbate these challenges. This aligns with findings from Greaney et al,29 who emphasise the need for improved training and resources for healthcare providers. Training and capacity building for healthcare providers on TB multimorbidity management are vital. The study highlights that many healthcare providers lack current knowledge on this topic, which affects their competency in assessing health literacy and managing multimorbidity. Previous studies have shown that training in health literacy can significantly improve treatment adherence.13,31–33 Most healthcare providers involved in TB programs have traditionally focused solely on TB, often neglecting the co-existence of other chronic conditions.34 The complexity of accessing healthcare services, which often requires coordination among multiple specialists, poses additional challenges for patients. Evidence supports the role of patient navigators in improving appointment adherence and health outcomes.28,29 For TB multimorbidity patients, navigation support can be crucial in understanding treatment plans, scheduling appointments, and advocating for patients within fragmented healthcare systems.35–37 Moreover, patients’ preferences for information channels vary based on their literacy levels and cultural contexts.38 To ensure accessibility and comprehension, communication strategies should incorporate diverse media types, including interactive mobile content, animated videos, pictorial pamphlets, and peer educator sessions.
Despite advancements in the National TB Elimination Program, the integration of TB care with chronic disease management remains underdeveloped. Addressing the TB burden necessitates a multifaceted approach that encompasses not only medical treatment but also improvements in health literacy, healthcare infrastructure, stakeholder coordination, and the social determinants of health that contribute to TB’s prevalence. The study underscores the urgent need for healthcare policies that prioritise health literacy development among TB patients with multimorbidity. Strategies should focus on creating culturally appropriate educational materials, enhancing communication training for community health workers, and fostering strong patient-provider relationships to improve shared decision-making. Integrating health literacy initiatives into TB care programs is essential for TB elimination in India.
Conclusions
This study highlights a health-literacy-driven framework for TB-multimorbidity management in India, linking information accessibility, patient understanding, decision-making, and system navigation to improve uptake, adherence, and coordinated care. This study suggests creating user-friendly condition-specific IEC materials for TB and comorbidities like diabetes, hypertension, and mental health and combining NTEP with NCD programs to improve referrals and treatment continuity. Making materials and interventions culturally responsive and regionally relevant may reduce misinformation, distrust, and care access inequities. To prevent fragmentation, hospitals need patient navigators or help desks to guide patients through complex services.
Data Statement
The data that support the findings of this study are available on reasonable request from the corresponding author. The transcripts are not publicly available due to privacy or ethical considerations.
Ethical Considerations and Informed Consent
The study complied with the Declaration of Helsinki ethical guidelines. The study was approved by the Indian Council of Medical Research, New Delhi review board. Ethical approval was given by the ICMR-RMRC institutional Ethics committee and the State Research and Ethics committee (20314/MS-2-IV-01/2024). Before the involvement of participants, all were provided with the participants’ information sheet and consent form. Participants were informed that they could withdraw from the study anytime without penalty. Everyone had given written informed consent and claimed to have fully understood the objectives and procedures of the study. Throughout the study, measures were taken to ensure the confidentiality and anonymity of the participants. All the personal identifiers were removed from the collected data, and digital audio recordings were deleted securely. The participants’ informed consent included publication of anonymized responses/direct quotes.
Acknowledgments
The author acknowledges all the participants for their valuable time and suggestions. The authors are grateful to the Indian Council of Medical Research (ICMR), New Delhi, for the institutional support and guidance throughout this study. “We also thank our field staff for facilitating the participant recruitment and interview.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Indian Council of Medical Research (ICMR) Intramural grant under the Communicable Diseases program.
Disclosure
The authors have no conflicts of interest to disclose in this work.
References
1. Siddiqi K, Stubbs B, Lin Y, Elsey H, Siddiqi N. TB multimorbidity: a global health challenge demanding urgent attention. int j tuberc lung dis. Intl J Tubercul Lung Dis. 2021;25(2):87–90. doi:10.5588/ijtld.20.0751
2. Muscat DM, Song W, Cvejic E, Ting JHC, Medlin J, Nutbeam D. The impact of the chronic disease self-management program on health literacy: a pre-post study using a multi-dimensional health literacy instrument. IJERPH. 2019;17(1):58. doi:10.3390/ijerph17010058
3. Chauhan A, Parmar M, Rajesham JD, et al. Landscaping tuberculosis multimorbidity: findings from a cross-sectional study in India. BMC Public Health. 2024;24(1):453. doi:10.1186/s12889-024-17828-z
4. Dutta A, Pattanaik S, Choudhury R, et al. Impact of involvement of non-formal health providers on TB case notification among migrant slum-dwelling populations in Odisha, India. PLoS One. 2018;13(5):e0196067. doi:10.1371/journal.pone.0196067
5. Dubey S, Sahoo KC, Dash GC, et al. Housing-related challenges during COVID-19 pandemic among urban poor in low-and middle-income countries: a systematic review and gap analysis. Front Public Health. 2022;10:1029394. doi:10.3389/fpubh.2022.1029394
6. Sahoo KC, Dubey S, Dash GC, et al. A systematic review of water, sanitation, and hygiene for urban poor in low-and middle-income countries during the COVID-19 pandemic through a gendered lens. Int J Environ Res Public Health. 2022;19(19):11845. doi:10.3390/ijerph191911845
7. Brabers AEM, Rademakers JJDJM, Groenewegen PP, Van Dijk L, De Jong JD. What role does health literacy play in patients’ involvement in medical decision-making? Renzaho AMN, editor. PLoS One. 2017;12(3):e0173316. doi:10.1371/journal.pone.0173316
8. Shnaigat M, Downie S, Hosseinzadeh H. Effectiveness of health literacy interventions on COPD self-management outcomes in outpatient settings: a systematic review. COPD. 2021;18(3):367–373. doi:10.1080/15412555.2021.1872061
9. Sørensen K, Van Den Broucke S, Fullam J, et al. Health literacy and public health: a systematic review and integration of definitions and models. BMC Public Health. 2012;12(1):80. doi:10.1186/1471-2458-12-80
10. Spencer M, Cruickshank V, Kemp N, Nash R. Exploring health literacy development through co-design: understanding the expectations for health literacy mediators. Health Promotion Int. 2025;40(1):daaf003. doi:10.1093/heapro/daaf003
11. Muniyandi M, Rao VG, Bhat J, Yadav R, Sharma RK, Bhondeley MK. Health literacy on tuberculosis amongst vulnerable segment of population: special reference to Saharia tribe in central India. Indian Journal of Medical Research. 2015;141(5):640–647. doi:10.4103/0971-5916.159566
12. Chauhan A, Parmar M, Dash GC, et al. Health literacy and tuberculosis control: systematic review and meta-analysis. Bulletin World Health Organization. 2024;102(6):421. doi:10.2471/BLT.23.290396
13. Pati S, Pati S, van den Akker M, Schellevis FG, Sahoo KC, Burgers JS. Managing diabetes mellitus with comorbidities in primary healthcare facilities in urban settings: a qualitative study among physicians in Odisha, India. BMC Family Pract. 2021;22(1):99. doi:10.1186/s12875-021-01454-4
14. Muscat DM, Shepherd HL, Nutbeam D, Trevena L, McCaffery KJ. Health literacy and shared decision-making: exploring the relationship to enable meaningful patient engagement in healthcare. J Gen Intern Med. 2021;36(2):521–524. doi:10.1007/s11606-020-05912-0
15. McKenna VB, Sixsmith J, Barry M. Facilitators and barriers to the development of health literacy capacities over time for self-management. HLRP. 2020;4(2). doi:10.3928/24748307-20200221-01
16. Tomita S, Aoki T, Ohde S, Takahashi O, Kimura T, Matsushima M. Association between health literacy and multimorbidity: a nationwide, cross-sectional study of a Japanese population. BMJ Open. 2022;12(1):e052731. doi:10.1136/bmjopen-2021-052731
17. Shahid R, Shoker M, Chu LM, Frehlick R, Ward H, Pahwa P. Impact of low health literacy on patients’ health outcomes: a multicenter cohort study. BMC Health Serv Res. 2022;22(1):1148. doi:10.1186/s12913-022-08527-9
18. Boonstra MD, Reijneveld SA, Westerhuis R, et al. A longitudinal qualitative study to explore and optimize self-management in mild to end stage chronic kidney disease patients with limited health literacy: perspectives of patients and health care professionals. Patient Educ Couns. 2022;105(1):88–104. doi:10.1016/j.pec.2021.05.016
19. Liu A-K, Liu -Y-Y, Su J. Self-efficacy and self-management mediate the association of health literacy and quality of life among patients with TB in Tibet, China: a cross-sectional study. International Health. 2023;15(5):585–600. doi:10.1093/inthealth/ihad040
20. Allen-Meares P, Lowry B, Estrella ML, Mansuri S. Health literacy barriers in the health care system: barriers and opportunities for the profession. Health Social Work. 2020;45(1):62–64. doi:10.1093/hsw/hlz034
21. Murugesu L, Heijmans M, Rademakers J, Fransen MP. Challenges and solutions in communication with patients with low health literacy: perspectives of healthcare providers. Nayyar A. editor. PLoS One. 2022;17(5)e0267782. doi:10.1371/journal.pone.0267782
22. Bhardwaj AK. Tuberculosis control programme from NTCP to RNTCP to NTEP. Indian J Community Health. 2020;32(3):469–470. doi:10.47203/IJCH.2020.v32i03.001
23. Rockwood N, Du Bruyn E, Morris T, Wilkinson RJ. Assessment of treatment response in tuberculosis. Expert Rev Respir Med. 2016;10(6):643–654. doi:10.1586/17476348.2016.1166960
24. Singh UB, Rade K, Rao R, et al. Lessons and updates from India’s national tuberculosis elimination program – bold decisions and innovative ways of fast-tracking progress toward ending tuberculosis. IJID Regions. 2025;14:100599. doi:10.1016/j.ijregi.2025.100599
25. Tavousi M, Haeri-Mehrizi A, Rakhshani F, et al. Development and validation of a short and easy-to-use instrument for measuring health literacy: the Health Literacy Instrument for Adults (HELIA). BMC Public Health. 2020;20(1):656. doi:10.1186/s12889-020-08787-2
26. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
27. Chen X, Hay JL, Waters EA, et al. Health literacy and use and trust in health information. J Health Commun. 2018;23(8):724–734. doi:10.1080/10810730.2018.1511658
28. Yuen E, Winter N, Savira F, et al. Digital health literacy and its association with sociodemographic characteristics, health resource use, and health outcomes: rapid review. Interact J Med Res. 2024;13:e46888. doi:10.2196/46888
29. Greaney ML, Wallington SF, Rampa S, Vigliotti VS, Cummings CA. Assessing health professionals’ perception of health literacy in Rhode Island community health centers: a qualitative study. BMC Public Health. 2020;20(1):1289. doi:10.1186/s12889-020-09382-1
30. Lazaro G. When positive is negative: health literacy barriers to patient access to clinical laboratory test results. Journal Appl Laboratory Med. 2023;8(6):1133–1147. doi:10.1093/jalm/jfad045
31. Miller TA. Health literacy and adherence to medical treatment in chronic and acute illness: a meta-analysis. Patient Educ Couns. 2016;99(7):1079–1086. doi:10.1016/j.pec.2016.01.020
32. Foo CD, Shrestha P, Wang L, et al. Integrating tuberculosis and noncommunicable diseases care in low- and middle-income countries (LMICs): a systematic review. PLoS Med. Suthar AB, editor. 2022;19(1):e1003899. doi:10.1371/journal.pmed.1003899
33. Garg T, Panibatla V, Carel JP, Shanta A, Bhardwaj M, Brouwer M. Can patient navigators help potential TB patients navigate the diagnostic and treatment pathways? An implementation research from India. TropicalMed. 2021;6(4):200. doi:10.3390/tropicalmed6040200
34. Budde H, Williams GA, Winkelmann J, Pfirter L, Maier CB. The role of patient navigators in ambulatory care: overview of systematic reviews. BMC Health Serv Res. 2021;21(1):1166. doi:10.1186/s12913-021-07140-6
35. Ramos JP, Vieira M, Pimentel C, Argel M, Barbosa P, Duarte R. Building bridges: multidisciplinary teams in tuberculosis prevention and care. Breathe. 2023;19(3):230092. doi:10.1183/20734735.0092-2023
36. Murugesu L, Heijmans M, Rademakers J, Fransen MP. Challenges and solutions in communication with patients with low health literacy: perspectives of healthcare providersNayyar Aeditor. PLoS One. 2022;175:e0267782
37. Achterbosch M, Vart P, Van Dijk L, Van Boven JFM. Shared decision making and medication adherence in patients with COPD and/or asthma: the ANANAS study. Front Pharmacol. 2023;14:1283135. doi:10.3389/fphar.2023.1283135
38. Gómez-Velasco DV, Almeda-Valdes P, Martagón AJ, Galán-Ramírez GA, Aguilar Salinas CA. Empowerment of patients with type 2 diabetes: current perspectives. DMSO. 2019;12:1311–1321. doi:10.2147/DMSO.S174910
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.