Back to Journals » Journal of Inflammation Research » Volume 19
Mucosal Involvement in Bullous Pemphigoid: Severity Indicator and Associated Clinical Features from a Retrospective Cohort Study
Authors Cui S ![]() , Zhang B, Chen F, Liu Y, Zhang J, Jin H, Li L
, Zhang B, Chen F, Liu Y, Zhang J, Jin H, Li L
Received 16 March 2026
Accepted for publication 27 May 2026
Published 18 June 2026 Volume 2026:19 608150
DOI https://doi.org/10.2147/JIR.S608150
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Adrian Lee
Shengnan Cui, Bingjie Zhang, Fangyuan Chen, Yangchun Liu, Jialing Zhang, Hongzhong Jin, Li Li
Department of Dermatology, State Key Laboratory of Complex Severe and Rare Diseases, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100730, People’s Republic of China
Correspondence: Hongzhong Jin, Department of Dermatology, Peking Union Medical College Hospital, No. 1 Shuaifuyuan, Dongcheng District, Beijing, 100730, People’s Republic of China, Tel +86-10-69151500, Email [email protected] Li Li, Department of Dermatology, Peking Union Medical College Hospital, No. 1 Shuaifuyuan, Dongcheng District, Beijing, 100730, People’s Republic of China, Tel +86-10-69151500, Email [email protected]
Purpose: Bullous pemphigoid (BP) is the most common autoimmune subepidermal blistering disorder. Although mucosal involvement is uncommon, it may indicate a more severe clinical phenotype. This study evaluated the prevalence and clinical features associated with mucosal involvement in BP.
Patients and Methods: This retrospective cohort study included 265 patients with BP diagnosed at Peking Union Medical College Hospital between January 2013 and May 2022. Clinical, laboratory, immunological, and treatment-related characteristics were compared between patients with and without mucosal involvement. Logistic regression analyses were performed to identify factors associated with mucosal involvement, and model performance was assessed using receiver operating characteristic analysis.
Results: Seventy-one patients (26.8%) had mucosal involvement, most commonly affecting the oral mucosa, followed by genital and ocular sites. Compared with patients without mucosal lesions, those with mucosal involvement were younger at disease onset, more frequently had a history of malignancy, and showed a more severe clinical phenotype, including higher hospitalization rates, more infections within 1 year, higher corticosteroid requirements, higher BPDAI scores, and more frequent head/neck and hands/feet involvement. Indirect immunofluorescence seropositivity and peripheral eosinophilia were less frequent in patients with mucosal involvement. In multivariate analysis, head/neck involvement (adjusted OR 8.276, 95% CI 2.211– 30.977), hands/feet involvement (adjusted OR 34.559, 95% CI 8.191– 145.805), and higher BPDAI score (adjusted OR 1.055, 95% CI 1.020– 1.091) were independently associated with mucosal involvement, whereas peripheral eosinophilia was inversely associated (adjusted OR 0.027, 95% CI 0.005– 0.148). The model demonstrated excellent apparent discrimination (AUC 0.937).
Conclusion: Mucosal involvement in BP is associated with a more severe clinical phenotype. Head/neck and acral involvement, higher BPDAI scores, and a lower frequency of peripheral eosinophilia may serve as practical clinical indicators for identifying patients who require closer mucosal assessment and more intensive monitoring.
Plain Language Summary: Bullous pemphigoid is a skin disease that mainly affects older adults and causes large blisters on the skin. In some patients, the disease also affects the mouth or other mucosal surfaces. Doctors consider this type of involvement uncommon, and they still know little about which patients are more likely to develop it. In this study, we analyzed medical records from 265 patients with bullous pemphigoid treated at a large hospital in China. We compared patients who had mucosal involvement with those who did not. We aimed to identify clinical features that may help doctors recognize patients who need closer mucosal assessment and monitoring. We found that about one in four patients had mucosal involvement. These patients tended to develop the disease at a younger age and often had more severe skin disease. They were also more likely to require hospitalization and stronger treatment. Skin lesions on the head, neck, hands, and feet were more common in these patients. In addition, these patients less often had increased eosinophils, a type of white blood cell, in their blood. Our results suggest that mucosal involvement may represent a more severe form of bullous pemphigoid. Recognizing these clinical features may help doctors identify these patients earlier and provide closer monitoring and more appropriate treatment.
Keywords: autoimmune blistering diseases, eosinophilia, disease severity, retrospective cohort
Introduction
Bullous pemphigoid (BP) is a chronic, subepidermal autoimmune blistering disease that primarily affects older adults and is increasingly regarded as an autoantibody-driven inflammatory disorder.1 The cumulative incidence of BP ranges from 0.12 to 6.6 per 100,000 person-years, with a global incidence averaging approximately 0.82 per 100,000 annually.2 Clinical features of BP comprise tense blisters and erosions on erythematous, urticarial, or normal-appearing skin; most patients experience intense pruritus. The pathogenesis involves autoantibodies toward the hemidesmosomal proteins non-collagenous 16A domain of bullous pemphigoid antigen 180 (BP180NC16A) and bullous pemphigoid antigen 230 (BP230), which trigger complement activation, inflammatory cell infiltration, and proteolytic enzyme release, followed by subepidermal blister formation.3
Mucosal involvement is uncommon in BP and has traditionally been reported in approximately 10%–20% of patients, most commonly affecting the oral mucosa.1 However, recent cohort studies suggest that the reported prevalence may vary across populations and referral settings.4,5 In rare cases, the pharyngeal and gastrointestinal mucosa may be involved.6–8 Patients with mucosal lesions often exhibit distinct clinical features and treatment responses relative to those with cutaneous manifestations alone.4,9–11 Mucosal involvement is increasingly considered a marker of heightened inflammatory activity and broader immune dysregulation. These patients frequently experience pain and dysphagia, leading to substantial reductions in quality of life and presenting considerable challenges for clinical management. Current evidence is limited to small retrospective studies; the prevalence and factors associated with mucosal involvement in BP remain poorly defined. Given the association of mucosal involvement with more severe disease and therapeutic difficulties, larger studies are required to clarify its clinical significance.
Here, we investigated factors associated with mucosal involvement in BP and compared our findings with previous reports to identify shared and distinct clinical features. These insights provide a basis for understanding the clinical relevance of mucosal involvement in BP.
Materials and Methods
Study Design and Population
We conducted a retrospective cohort study of BP patients treated at Peking Union Medical College Hospital between January 2013 and May 2022. The diagnosis of BP was established according to the S2k diagnostic guidelines.12 A confirmed diagnosis required compatible clinical manifestations, including tense blisters and/or urticarial plaques predominantly involving the skin, together with supportive histopathological and immunopathological findings. Hematoxylin–eosin staining demonstrated subepidermal blister formation with an eosinophil-rich inflammatory infiltrate in the superficial dermis. Direct immunofluorescence (DIF) of perilesional skin showed linear deposition of IgG and/or C3 along the basement membrane zone. Circulating autoantibodies were assessed, when available, by indirect immunofluorescence (IIF) on salt-split human skin and/or enzyme-linked immunosorbent assay (ELISA) for serum anti-BP180 NC16A IgG antibodies. Serum anti-BP180 NC16A IgG levels were measured using a commercially available ELISA kit (MESACUP BP180 TEST, Code No. 7695E; Medical & Biological Laboratories Co., Ltd., Nagoya, Japan) according to the manufacturer’s instructions. To minimize misclassification with mucous membrane pemphigoid, patients were classified as having BP only when cutaneous disease was predominant and mucosal lesions, if present, were limited and non-scarring. Patients with primary mucosal-dominant disease, persistent or progressive mucosal disease, ocular scarring, or other clinical features suggestive of mucous membrane pemphigoid were excluded. In patients with mucosal lesions, IIF on salt-split skin demonstrating IgG binding to the epidermal side of the split was considered supportive of BP.
Inclusion criteria were no prior history of BP and receipt of the initial diagnosis at our institution. Exclusion criteria were: (1) other autoimmune blistering diseases involving mucosal lesions, including mucous membrane pemphigoid; and (2) incomplete medical records. This study was reported in accordance with the Reporting of studies Conducted using Observational Routinely collected health Data (RECORD) guidelines. The completed RECORD checklist and study flowchart are provided in the Supplementary Material 1 and Supplementary Figure S1.
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Peking Union Medical College Hospital (Approval No. S-K7602). All patients were informed of the study purpose and methodology, and they provided written informed consent.
Data Collection
Data were systematically extracted from the hospital electronic database and individual medical records. Demographic variables included age at diagnosis and sex, and hospitalization status at initial presentation was recorded. Clinical characteristics comprised lesion morphology and distribution, disease severity assessed using the Bullous Pemphigoid Disease Area Index (BPDAI), and the presence and anatomical distribution of mucosal involvement. BPDAI scores were categorized as mild (≤19), moderate (20–56), or severe (≥57). Mucosal involvement was assessed at baseline, at the time of BP diagnosis and before the initiation of systemic treatment. It was defined as clinically documented erosions, blisters, or ulcerations involving the oral, ocular, genital, or other mucosal sites. Mucosal lesions that developed only during follow-up were not used to define baseline mucosal involvement. Medical history included diabetes mellitus, cardiovascular diseases, neurological disorders, and malignancy. Baseline laboratory parameters obtained at the time of diagnosis prior to systemic treatment included complete blood count indices: white blood cell (WBC) count, neutrophil (NEU) count and percentage, lymphocyte (LY) count and percentage, eosinophil (EOS) count and percentage, hemoglobin (HGB), and platelet (PLT) count. Biochemical markers included serum albumin (ALB) and prealbumin (PA) levels. Immunopathological findings comprised direct immunofluorescence (DIF), indirect immunofluorescence (IIF) and serum anti–BP180 NC16A IgG levels, when available. Treatment variables included initial therapeutic regimens, particularly systemic corticosteroids and/or immunosuppressive agents. Complications were documented, including infections occurring within one year after BP diagnosis. Clinical outcomes were evaluated based on relapse status. Relapse was defined as the development of more than three new lesions within one month that failed to resolve within one week, or progression of pre-existing lesions after prior achievement of disease control, in accordance with published criteria.5,13 Follow-up duration was calculated from the date of BP diagnosis to the last documented dermatology visit, death, or the end of the predefined follow-up period, whichever occurred first. Infection was assessed within 1 year after BP diagnosis, whereas relapse was assessed during the 2-year follow-up period. Patients without relapse were censored at the date of their last available follow-up. Patients with insufficient follow-up information were excluded from the corresponding outcome analysis, and the available denominators are reported in the tables.
Statistical Analyses
All statistical analyses were performed using IBM SPSS Statistics, version 26.0. The Shapiro–Wilk test was used to assess the normality of continuous variables. Normally distributed variables were presented as mean ± standard deviation and compared using the independent-samples t test. Non-normally distributed variables were expressed as median (interquartile range) and compared using the Mann–Whitney U-test. Categorical variables were presented as counts and percentages and compared using the chi-square test or Fisher’s exact test, as appropriate. Univariate logistic regression analysis was conducted to identify potential factors associated with mucosal involvement. Missing data were not imputed because of the retrospective design. Descriptive analyses were performed using available data, and the corresponding denominators are reported in the tables. Logistic regression analyses were performed using complete cases for the variables included in each model. Variables were selected for multivariable analysis based on clinical relevance, previous literature, baseline group differences, and a P value < 0.10 in univariate analysis. Anti-BP180 NC16A IgG levels were additionally included in the multivariable model based on clinical relevance. No formal sample-size or power calculation was performed because this was an exploratory retrospective cohort study including all eligible patients during the study period. Adjusted odds ratios (ORs) with 95% confidence intervals (CIs) were calculated. To evaluate the discriminative performance of the final multivariable model, receiver operating characteristic (ROC) curve analysis was performed using the predicted probabilities derived from the model. The area under the curve (AUC) and corresponding 95% confidence interval were calculated. A nomogram was constructed based on the factors retained in the final multivariable logistic regression model to provide individualized probability estimation. Model calibration was assessed using a calibration curve with bootstrap resampling. Decision curve analysis was performed to evaluate the potential clinical utility of the model. All tests were two-sided, and P values < 0.05 were considered statistically significant.
Results
Baseline Patient Characteristics
The clinical characteristics of the 265 patients included in this study are summarized in Table 1. The cohort comprised 149 men and 116 women, with a median age of 68 years at diagnosis. Among these patients, 70 (26.4%) required hospitalization, and 62 (23.5%) developed pulmonary, cutaneous, or bloodstream infections within 1 year of diagnosis. In total, 175 patients (66.0%) had relevant comorbidities. The most common were cardiovascular diseases (n = 89; 33.6%), including hypertension, coronary artery disease, and arrhythmias; neurological disorders (n = 56; 21.1%), such as stroke, Parkinson’s disease, and dementia; diabetes mellitus (n = 43; 16.2%); and malignancies (n = 17; 6.4%), including lung, gastrointestinal, and genitourinary cancers. Cutaneous lesions were distributed across multiple anatomical regions, with head and neck involvement observed in 109/256 patients (42.6%), trunk involvement in 231/256 (90.2%), limb involvement in 241/256 (94.1%), and hands/feet involvement in 105/256 (41.0%). According to BPDAI scores, 102 patients (40.8%) displayed mild to moderate disease, whereas 148 (59.2%) exhibited severe disease. The median BPDAI score was 60.0, ranging from 17 to 148.
 |
Table 1 Characteristics of BP Patients at Baseline |
Regarding immunologic markers, direct immunofluorescence (DIF) results were positive in 131 patients (57.5%) and negative in 97 (42.5%). Indirect immunofluorescence (IIF) results were positive in 127 patients (55.5%) and negative in 102 (44.5%). Among patients with positive IIF results, titers were 1:40 in seven (2.6%), 1:80 in three (1.1%), 1:160 in 25 (9.2%), 1:320 in 27 (10.0%), and ≥1:320 in 65 (24.0%). Serum anti-BP180 NC16A IgG levels were measured by ELISA in 172 patients, among whom 145 (84.3%) were positive. Eosinophilia, defined as an eosinophil count >0.5 × 109/L, was observed in 94 patients (45.6%).
In terms of treatment, 192 patients (73.3%) received oral prednisone, with a median effective dose of 40.0 mg/day. Adjuvant immunosuppressive agents such as Tripterygium wilfordii polyglycoside, methotrexate, cyclophosphamide, and thalidomide were administered to 177 patients (67.6%). Topical corticosteroids alone were used in 10 patients (3.8%). The median follow-up duration was 2.7 years (range, 1.6–4.5 years). During the 2-year follow-up period, disease relapse occurred in 109 of 192 patients with available follow-up data (56.8%). Patients without relapse were censored at their last documented follow-up visit. A total of 73 patients were censored before 2 years because of loss to follow-up, death, or absence of further documented visits.
General Characteristics and Clinical Features of Patients with Mucosal Involvement
Among the 265 patients with BP, varying degrees of mucosal involvement were identified in 71 cases (26.8%). The oral mucosa was the most frequently affected site (62 patients, 23.4%), followed by the genital mucosa (23 patients, 8.7%) and ocular mucosa (5 patients, 1.9%). Isolated mucosal involvement was observed in 54 patients (20.4%), including 46 (17.4%) with oral lesions alone and eight (3.0%) with isolated genital lesions. Dual-site mucosal involvement occurred in 15 patients (5.7%), including oral and genital mucosa in 12 (4.5%), oral and ocular mucosa in two (0.8%), and ocular and genital mucosa in one (0.4%). Concurrent involvement of all three sites—oral, ocular, and genital—was documented in two patients (0.8%). Overall, ocular mucosal involvement was documented in five patients, and no patient showed progressive ocular scarring suggestive of mucous membrane pemphigoid.
Clinical differences between BP patients with (n = 71) and without (n = 194) mucosal involvement are summarized in Table 2. Patients with mucosal lesions were significantly younger at diagnosis (median age: 64.0 [57.0–76.0] vs. 71.0 [59.0–79.3] years; P = 0.040). The hospitalization rate was also significantly higher among patients with mucosal involvement (53.5% vs. 16.5%; P < 0.001). Additionally, these patients had higher incidences of malignancy (11.3% vs. 4.6%; P = 0.046) and infectious complications (33.8% vs. 19.6%; P = 0.013). No significant differences were observed between the two groups regarding sex distribution (P = 0.461), other comorbidities (66.2% vs. 66.0%; P = 0.974), or relapse rates (52.9% vs. 58.2%; P = 0.519).
 |
Table 2 Baseline Demographic Characteristics, Clinical Features, and Treatment of BP Patients with and without Mucosal Involvement |
Regarding the anatomical distribution of bullous lesions, patients with mucosal involvement demonstrated significantly more frequent involvement of the head and neck (71.8% vs. 31.4%; P < 0.001) and the hands and feet (83.1% vs. 24.9%; P < 0.001). BPDAI scores also were significantly higher in patients with mucosal involvement relative to those without (median: 70.0 [59.0–94.0] vs. 58.0 [46.0–69.0]; P < 0.001).
In terms of immunologic markers, there were no significant differences in anti-BP180NC16A antibody positivity rates or antibody titers between patients with and without mucosal involvement. IIF seropositivity was less frequent in patients with mucosal involvement than in those without mucosal involvement (48.4% vs 58.1%; P = 0.040). Notably, peripheral eosinophilia was less frequent in the mucosal involvement group (31.6% vs. 51.0%; P = 0.012). No other significant differences in immunologic markers were identified between the two groups.
Patients with mucosal involvement required significantly higher doses of systemic corticosteroids to achieve disease control relative to those without mucosal involvement (40.0 [30.0–60.0] mg/day vs. 30.0 [30.0–40.0] mg/day; P = 0.001). However, no significant difference was observed between the groups in the use of adjuvant immunosuppressants (70.0% vs. 65.6%; P = 0.507).
Factors Associated with Mucosal Involvement According to Univariate and Multivariate Logistic Regression Analysis
Univariate analysis was conducted to identify factors associated with mucosal involvement in BP. Variables were selected based on clinical relevance, literature review, and baseline group differences. Factors included were age at diagnosis, malignancy, lesion distribution (head/neck, hands/feet), BPDAI score, anti-BP180NC16A antibody levels, peripheral eosinophilia. Detailed results of univariate and multivariate analyses are presented in Table 3.
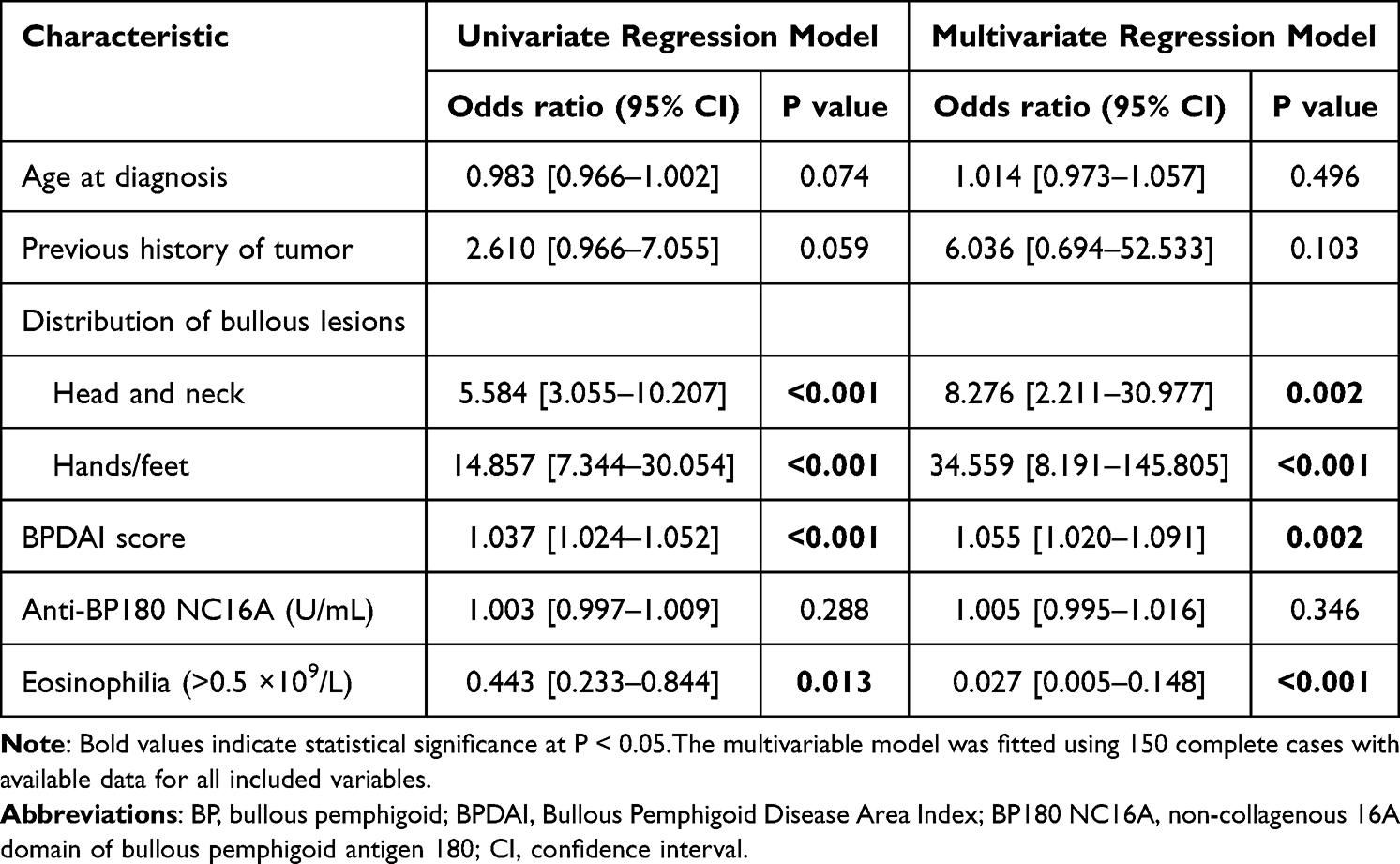 |
Table 3 Univariate and Multivariate Analyses of Factors Associated with Mucosal Involvement in BP |
Univariate logistic regression analysis identified head and neck involvement (odds ratio [OR] 5.584, 95% confidence interval [CI] 3.055–10.207; P < 0.001), hands and feet involvement (OR 14.857, 95% CI 7.344–30.054; P < 0.001), higher BPDAI score (OR 1.037, 95% CI 1.024–1.052; P < 0.001), and peripheral eosinophilia (>0.5 × 109/L) (OR 0.443, 95% CI 0.233–0.844; P = 0.013) as significantly associated with mucosal involvement. Age at diagnosis, previous history of tumor, and anti-BP180NC16A antibody levels were not significantly associated.
Variables with P < 0.10 in univariate analysis were included in the multivariate logistic regression model, together with anti-BP180NC16A antibody titers based on clinical considerations. In the adjusted analysis, head and neck involvement (OR 8.276, 95% CI 2.211–30.977; P = 0.002), hands and feet involvement (OR 34.559, 95% CI 8.191–145.805; P < 0.001), and higher BPDAI score (OR 1.055, 95% CI 1.020–1.091; P = 0.002) remained independently associated with mucosal involvement. Peripheral eosinophilia was inversely associated with mucosal involvement (OR 0.027, 95% CI 0.005–0.148; P < 0.001). Anti-BP180NC16A antibody titers were not independently associated.
To assess the discriminative ability of the multivariate logistic regression model, ROC curve analysis was conducted using the predicted probabilities derived from the final model. The model showed excellent apparent discrimination, with an AUC of 0.937 (95% CI, 0.899–0.975; P < 0.001), indicating good discrimination between patients with and without mucosal involvement in this cohort (Figure 1). Additional model performance assessments, including the nomogram, calibration curve, and decision curve analysis, are presented in Supplementary Figure S2.
 |
Figure 1 Receiver operating characteristic (ROC) curve of the multivariate logistic regression model for identifying patients with mucosal involvement in bullous pemphigoid. The area under the curve (AUC) was 0.937 (95% CI, 0.899–0.975), indicating excellent discriminative performance. |
Discussion
In this study, we analyzed a cohort of 265 patients with BP to identify factors associated with mucosal involvement. Mucosal lesions were evident in 26.8% of patients, indicating that a substantial subset of BP cases involves mucous membranes. This prevalence is consistent with the upper range reported in previous studies.9 Our findings closely align with the 25.5% detected in a large Chinese cohort of 1,018 BP patients and are higher than the 17.1% observed in an Israeli cohort.4,5 Such variations may reflect differences in population characteristics, referral patterns, mucosal assessment, or diagnostic thresholds. Nevertheless, the consistent documentation of mucosal involvement in approximately 20% to 25% of BP cases across studies suggests that this manifestation is clinically relevant. Clinicians should remain vigilant for mucosal symptoms, such as oral discomfort or dysphagia, although BP is generally regarded as a cutaneous disease.
In our cohort, the oral mucosa was the most frequently affected site among BP patients with mucosal involvement, consistent with previous reports.4,5 This predominance may be related to repeated mechanical trauma in the oral cavity, such as mastication, and local microenvironmental factors that may facilitate epithelial injury or autoantibody-mediated inflammation. In contrast, involvement of other mucosal sites, including the ocular surface, larynx, and genital mucosa, was uncommon. It is essential to distinguish mucosal involvement in BP from mucous membrane pemphigoid, a distinct autoimmune blistering disease that primarily affects mucous membranes. Mucous membrane pemphigoid is characterized by subepithelial blistering and a propensity for scarring, particularly in the ocular and nasal mucosa, and less frequently in the oral cavity.14 Mucosal involvement in BP is often transient and non-scarring. This clinical distinction may reflect differences in autoantibody specificity, antigen distribution, and downstream inflammatory responses. In BP, antibodies predominantly target BP180 NC16A, whereas mucous membrane pemphigoid may involve antibodies against laminin-332 or the C-terminal domain of BP180, which are more closely associated with persistent inflammation and fibrosis. In addition, immunoglobulin A autoantibodies have been implicated in some forms of mucous membrane pemphigoid, especially in ocular disease, and may contribute to scarring and treatment resistance.15
We found no significant sex differences according to mucosal involvement status, consistent with most studies on BP. Patients with mucosal involvement were younger at diagnosis than those without mucosal involvement. This observation aligns with data from an Israeli cohort, which showed a 7.5-year younger mean age among patients with mucosal BP.4 One possible explanation is that younger individuals may mount a more robust immune response, which could be associated with more extensive disease phenotypes, including mucosal involvement.16 External triggers such as malignancies—more frequently implicated in early-onset BP—may also predispose patients to mucosal manifestations. Although some previous studies did not identify an age difference, the consistency of our findings with prior large-scale data, such as the study by Kridin et al, implies an association with younger age.4,17,18 Clinicians should maintain a high index of suspicion for mucosal symptoms among younger patients with BP.
A novel aspect of our study is the investigation of comorbidities associated with mucosal involvement in BP. The prevalence of malignancy was higher in patients with mucosal involvement than in those without mucosal involvement (11.3% vs 4.6%). Although this association was not significant in multivariable analysis, it raises the possibility that malignancy-associated immune dysregulation may be related to a broader inflammatory phenotype in some patients. Tumor cells might expose cryptic basement membrane antigens or mimic BP180 epitopes, resulting in loss of immune tolerance and a broader autoimmune response that includes mucosal sites.9,19 Additionally, patients with mucosal involvement experienced more infections and had higher hospitalization rates, supporting the notion that such involvement represents a more severe disease phenotype. A recent study of BP-related complications revealed increased risks of sepsis and infectious events in patients with mucosal involvement, possibly due to the need for stronger immunosuppression and the presence of exposed mucosal surfaces that offer potential entry points for pathogens.20
A principal finding of this study was the robust association between mucosal involvement and more extensive cutaneous disease. In multivariable analysis, involvement of the head and neck region, involvement of the hands and feet, and higher BPDAI scores remained independently associated with mucosal lesions. Head and neck involvement was associated with approximately eightfold higher odds of mucosal involvement, whereas acral involvement demonstrated an even stronger association. The magnitude of the odds ratio for acral involvement warrants cautious interpretation in light of the wide confidence interval, which indicates limited precision. This imprecision may reflect sparse data in some subgroups, the limited number of complete cases after missing data exclusion, or correlation between anatomical distribution and overall disease severity. This pattern likely reflects a phenotype characterized by disseminated or more severe cutaneous inflammation rather than a site-specific causal effect.9 Collectively, these findings support the concept that mucosal involvement preferentially arises in patients with a widespread inflammatory burden of bullous pemphigoid. Larger, adequately powered studies are needed to define the true effect size and its clinical relevance.
The distinct immunologic profiles observed in our study may provide insights into potential disease mechanisms. Patients with mucosal involvement had a lower frequency of peripheral eosinophilia, although absolute eosinophil counts did not differ significantly between groups. The underlying mechanism remains unclear, and further research is needed to determine whether circulating or tissue-infiltrating eosinophils are protective against mucosal involvement.4 One possibility is that mucosal involvement may reflect a distinct inflammatory pathway rather than the classic eosinophil-dominant inflammatory pattern of BP. For example, mucosal tissues are rich in IgA production and harbor different resident immune cells, implying that certain mucosal-predominant BP subtypes involve a shift toward neutrophil-driven inflammation, potentially mediated by IgA or IgG subclass variations. Moreover, reduced Th2 polarization in this subset may contribute to lower eosinophilia despite active disease.21,22 Further studies are needed to clarify whether circulating or tissue-infiltrating eosinophils play a protective or modulatory role in this context. In contrast, anti-BP180 NC16A antibody titers were not independently associated with mucosal involvement in our cohort, suggesting that antibody level alone may not fully explain the development of mucosal lesions.23
From a clinical perspective, these readily accessible variables may assist clinicians in identifying patients who warrant more meticulous mucosal evaluation at the time of diagnosis. Patients presenting with head and neck involvement, acral involvement, higher BPDAI scores, or a lower frequency of peripheral eosinophilia may benefit from targeted assessment of the oral, genital, and ocular mucosa, together with closer surveillance during treatment. The proposed model may serve as a preliminary tool for recognizing patients who are more likely to have mucosal involvement. Nevertheless, the retrospective single-center design imposes important limitations, and the model should therefore be considered exploratory until external validation is achieved in prospective multicenter cohorts.
In terms of treatment and prognosis, patients with mucosal involvement required substantially higher doses of systemic corticosteroids to achieve disease control relative to those without mucosal involvement. However, relapse rates did not significantly differ between the two groups.
This study has several limitations. First, its retrospective single-center design may limit the generalizability of the findings and may have introduced selection bias, as our institution is a tertiary referral center. Because mucosal involvement and most clinical variables were assessed at baseline or near the time of diagnosis, the associations identified in this study should not be interpreted as causal risk factors. Rather, they represent clinical features associated with the mucosal involvement phenotype. Second, some immunological data, including anti-BP230 antibody results, were incomplete, which restricted further evaluation of autoantibody profiles. Third, the prediction model may be subject to overfitting, particularly given the high odds ratios and wide confidence intervals for some variables, such as acral involvement. These estimates should therefore be interpreted cautiously. External validation in independent prospective multicenter cohorts is required before the model can be applied in routine clinical practice.
Conclusion
This study comprised a focused analysis of clinical features associated with mucosal involvement in BP. We found that mucosal lesions were linked to a more severe disease phenotype, characterized by younger age at onset, higher rates of malignancy, broader cutaneous distribution, particularly involving the head, neck, and acral regions, lower frequency of peripheral eosinophilia, and a requirement for stronger treatment. Head/neck and acral involvement, higher BPDAI scores, and lower frequency of peripheral eosinophilia may serve as clinical indicators for early identification and closer mucosal assessment. These findings suggest differences in the underlying immunopathology, such as distinct triggers or antibody profiles, which may contribute to the mucosal phenotype. Recognition of this patient subset is clinically relevant because they often require closer monitoring and individualized management to prevent complications such as infection or mucosal damage. Given the retrospective single-center design, these findings should be interpreted as associations and require external validation in prospective multicenter cohorts.
Data Sharing Statement
All data supporting the findings of this study are available on request from the corresponding author upon reasonable request ([email protected]).
Acknowledgments
We thank all the patients and their families for participating in the study.
Author Contributions
Shengnan Cui: Data curation, Formal analysis, Methodology, Visualization, Writing – original draft, Writing – review & editing. Bingjie Zhang: Methodology, Validation, Writing – review & editing. Fangyuan Chen: Data curation, Investigation, Validation, Writing – review & editing. Yangchun Liu: Data curation, Investigation, Validation, Writing – review & editing. Jialing Zhang: Data curation, Investigation, Validation, Writing – review & editing. Hongzhong Jin: Conceptualization, Supervision, Project administration, Resources, Writing – review & editing. Li Li: Conceptualization, Methodology, Supervision, Project administration, Resources, Funding acquisition, Writing – review & editing. All authors made a significant contribution to the work reported; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (No. 81972945) and the Milstein Medical Asian American Partnership Foundation.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Akbarialiabad H, Schmidt E, Patsatsi A, et al. Bullous pemphigoid. Nat Rev Dis Primers. 2025;11(1):12. doi:10.1038/s41572-025-00595-5
2. Persson MSM, Begum N, Grainge MJ, Harman KE, Grindlay D, Gran S. The global incidence of bullous pemphigoid: a systematic review and meta-analysis. Br J Dermatol. 2022;186(3):414–12. doi:10.1111/bjd.20743
3. Egami S, Yamagami J, Amagai M. Autoimmune bullous skin diseases, pemphigus and pemphigoid. J Allergy Clin Immunol. 2020;145(4):1031–1047. doi:10.1016/j.jaci.2020.02.013
4. Kridin K, Bergman R. Assessment of the prevalence of mucosal involvement in bullous pemphigoid. JAMA Dermatol. 2019;155(2):166–171. doi:10.1001/jamadermatol.2018.5049
5. Cao S, Li W, Wang Z, et al. Clinical outcomes and prognostic factors in bullous pemphigoid patients: a 15-year review in China. Am J Clin Dermatol. 2025;26:457–470. doi:10.1007/s40257-025-00925-z
6. Hamdan AL, Abou Chaar J, Abou Rahal J. Laryngeal Manifestations of Bullous Pemphigoid: case Report and Review of the Literature. Ear Nose Throat J. 2024;1455613241230252. doi:10.1177/01455613241230252
7. Hussain MH, Tanweer F, Sakagiannis G, Mair M, Mahmood S, Ashokkumar S. Pemphigus vulgaris and bullous pemphigoid of the upper aerodigestive tract: a review article and novel approaches to management. ORL J Otorhinolaryngol Relat Spec. 2021;83(6):395–403. doi:10.1159/000515229
8. Castelo Branco C, Fonseca T, Marcos-Pinto R. Esophageal Bullous Pemphigoid. Eur J Case Rep Intern Med. 2022;9(2):003160. doi:10.12890/2022_003160
9. Chen X, Zhao W, Jin H, Li L. Risk factors for mucosal involvement in bullous pemphigoid and the possible mechanism: a review. Front Med. 2021;8:680871. doi:10.3389/fmed.2021.680871
10. Lee J, Seiffert-Sinha K, Attwood K, Sinha AA. A retrospective study of patient-reported data of bullous pemphigoid and mucous membrane pemphigoid from a us-based registry. Front Immunol. 2019;10:2219. doi:10.3389/fimmu.2019.02219
11. Eftekhari H, Rafiei R, Yousefkhani L, et al. Association between immunofluorescence pattern and mucosal involvement in patients with bullous pemphigoid. Acta Dermatovenerol Croat. 2018;26(3):243–248.
12. Borradori L, Van Beek N, Feliciani C, et al. Updated S2 K guidelines for the management of bullous pemphigoid initiated by the European Academy of Dermatology and Venereology (EADV). J Eur Acad Dermatol Venereol. 2022;36(10):1689–1704. doi:10.1111/jdv.18220
13. Liu Y, Wang Y, Zhang J, et al. Risk factors predisposing relapse of bullous pemphigoid at initial diagnosis: a retrospective cohort study of 205 patients. Int Immunopharmacol. 2023;125:111082. doi:10.1016/j.intimp.2023.111082
14. Hofmann SC, Günther C, Böckle BC, et al. S2k Guideline for the diagnosis and treatment of mucous membrane pemphigoid. J Dtsch Dermatol Ges. 2022;20(11):1530–1550. doi:10.1111/ddg.14905
15. Mariotti F, Pira A, De Luca N, et al. Bullous pemphigoid and mucous membrane pemphigoid humoral responses differ in reactivity towards BP180 midportion and BP230. Front Immunol. 2024;15:1494294. doi:10.3389/fimmu.2024.1494294
16. Chen X, Zhang B, Mao X, et al. Clinical characteristics of bullous pemphigoid patients of different ages and the possible mechanism. J Dermatol. 2025;52(4):672–681. doi:10.1111/1346-8138.17616
17. Kirtschig G, Venning VA, Wojnarowska F. Bullous pemphigoid: correlation of mucosal involvement and mucosal expression of autoantigens studied by indirect immunofluorescence and immunoblotting. Clin Exp Dermatol. 1999;24(3):208–212. doi:10.1046/j.1365-2230.1999.00457.x
18. Clapé A, Muller C, Gatouillat G, et al. Mucosal involvement in bullous pemphigoid is mostly associated with disease severity and to absence of anti-bp230 autoantibody. Front Immunol. 2018;9:479. doi:10.3389/fimmu.2018.00479
19. Hodge L, Marsden RA, Black MM, Bhogal B, Corbett MF. Bullous pemphigoid: the frequency of mucosal involvement and concurrent malignancy related to indirect immunofluorescence findings. Br J Dermatol. 1981;105(1):65–69. doi:10.1111/j.1365-2133.1981.tb00883.x
20. Chen J, Mao X, Zhao W, et al. Assessment of the characteristics and associated factors of infectious complications in bullous pemphigoid. Front Immunol. 2020;11:1607. doi:10.3389/fimmu.2020.01607
21. Amber KT, Valdebran M, Kridin K, Grando SA. The role of eosinophils in bullous pemphigoid: a developing model of eosinophil pathogenicity in mucocutaneous disease. Front Med Lausanne. 2018;5:201. doi:10.3389/fmed.2018.00201
22. Limberg MM, Weihrauch T, Gray N, Ernst N, Hartmann K, Raap U. Eosinophils, basophils, and neutrophils in bullous pemphigoid. Biomolecules. 13(7). doi:10.3390/biom13071019
23. Maurice PD, Allen BR, Marriott DW, Powell RJ, Reeves WG. Skin immunofluorescence in the diagnosis of primary bullous diseases--a review of 279 cases. Clin Exp Dermatol. 1986;11(4):352–364. doi:10.1111/j.1365-2230.1986.tb00475.x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.