Back to Journals » Cancer Management and Research » Volume 17

MRI Radiomics Predicts Early Biological Progression in a Preclinical Colon Cancer Model Following Mesenchymal Stem Cell Intervention
Authors Sun J, Yang Q, Ma W, Yu X, Feng J, He C, Guo Y, Li C
Received 19 March 2025
Accepted for publication 15 September 2025
Published 6 October 2025 Volume 2025:17 Pages 2297—2306
DOI https://doi.org/10.2147/CMAR.S529157
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Chien-Feng Li
Jun Sun,1,2,* Qingning Yang,1,* Wei Ma,2,3 Xiaoli Yu,4 Junbang Feng,1 Cheng He,1 Yi Guo,1 Chuanming Li1
1Department of Medical Imaging, Chongqing Emergency Medical Center, Chongqing Key Laboratory of Emergency Medicine, Chongqing University Central Hospital, School of Medicine, Chongqing University, Chongqing, 400010, People’s Republic of China; 2Department of Radiology, Children’s Hospital of Chongqing Medical University, Chongqing, 400014, People’s Republic of China; 3Department of Radiology, People’s Hospital of Chongqing Yubei District, Chongqing, 400000, People’s Republic of China; 4School of Medicine, Chongqing University, Chongqing, 400044, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chuanming Li; Yi Guo, Department of Medical Imaging, Chongqing Emergency Medical Center, Chongqing Key Laboratory of Emergency Medicine, Chongqing University Central Hospital, School of Medicine, Chongqing University, No. 1 Jiankang Road, Yuzhong District, Chongqing, 400010, People’s Republic of China, Email [email protected]; [email protected]
Background: Stem cell therapy is a potential approach for tumor treatment; however, its efficacy and safety remain incompletely controllable. Therefore, early prediction of tumor progression and therapeutic evaluation post-treatment to guide timely therapeutic adjustments is essential. Radiomics has recently been widely applied to assess tumor behavior and characteristics. This study aims to investigate the predictive value of MRI radiomics for therapeutic outcomes in the early stages of stem cell intervention in colon cancer.
Methods: Subcutaneous tumor models were established by implanting CM38 colon cancer cells into the inguinal region of C57BL/6 mice. Bone marrow mesenchymal stem cells (MSCs) were intravenously injected via the tail vein within 24 hours. T1 weighted MRI scans were performed on day 7 to extract radiomic features, monitor tumor growth, and evaluate neovascularization (CD34) and proliferation (Ki67) via immunohistochemistry. An early-stage MRI radiomics model was constructed to predict colon cancer progression.
Results: Tumors in the stem cell intervention group exhibited faster growth compared to the control group, though no significant volume difference was observed in the early phase. A total of 1162 radiomic features were extracted, with 17 strongly associated features (including texture features, first-order features texture and shape features) selected to build the prediction model. The final model demonstrated an AUC > 0.8 across both training and testing datasets.
Conclusion: Intravenous MSC injection promotes the progression of subcutaneously implanted CM38 colon cancer. An MRI radiomics-based predictive model was successfully established, enabling early prediction of tumor progression post-intervention.
Keywords: mesenchymal stem cells, radiomics predictive model, tumor microenvironment, magnetic resonance imaging, colon cancer
Introduction
Mesenchymal stem cells (MSCs) exhibit tumor-homing properties and modulate tumor microenvironments by regulating immune components and suppressing inflammatory responses, thereby exerting antitumor effects.1–4 Ghannam et al5 demonstrated that MSCs inhibit T-cell proliferation and alleviate inflammation, while Sabine François et al6 reported that intravenous MSC administration prolongs survival in carcinogen-exposed rats by reducing tumor incidence and delaying progression. However, the biosafety of MSCs requires critical attention. MSCs possess multidifferentiation potential, and their tumorigenic risks remain under investigation.7 Additionally, MSCs secrete paracrine factors (eg, chemokines, cytokines, and growth factors) that may promote tumor progression and metastasis. For example, MSC-derived IL-6 and IL-8 enhance the malignant potential of colon and breast cancers.8 Engineered MSCs have also been explored as drug delivery vehicles for targeted tumor therapy.9 However, prolonged in vitro culture during engineering processes may lead to cellular enlargement, senescence, or contamination, potentially reducing tumor-homing efficiency or increasing carcinogenic risks.7 Thus, the efficacy and safety of MSC-based therapies for colorectal cancer remain uncertain, necessitating early prediction of tumor progression to guide timely therapeutic adjustments.
Medical imaging serves as a cornerstone for tumor evaluation, enabling not only size measurement but also characterization of intratumoral features (eg, necrosis, hemorrhage, and invasion). Advanced MRI sequences, such as functional MRI (fMRI) and chemical exchange saturation transfer (CEST), provide insights into molecular alterations within tumor microenvironments. Studies by Kudo M and Niek Wijnen et al demonstrated that APTw imaging predicts Ki-67 expression in gliomas, meningiomas, and breast cancers,10–14 likely reflecting proliferative activity and extracellular components in high-grade tumors.15 However, these subtle differences are often imperceptible on conventional imaging. Radiomics offers a solution by enabling high-throughput extraction of quantitative features to detect microstructural variations.
Recent advances highlight radiomics’ role in noninvasive tumor characterization, genotyping, and survival prediction16,17. Johannes Müller et al correlated MRI texture features with hypoxic tumor microenvironments,18 while Roger Sun and Michal R Tomaszewski et al16,19 identified baseline CT radiomic features as predictors of PD-L1 immunotherapy response. MR-based radiomics has also been applied to predict tumor heterogeneity,20 survival in gliomas,21 and chemotherapy response in colorectal cancer metastases.22
Despite these advancements, it remains unclear whether radiomic features can detect early, subclinical tumor promoting effects of MSC therapy in colon cancer models. We hypothesize that MRI-based radiomics can non-invasively capture early biological changes such as increased neovascularization associated with MSC-induced tumor progression, before changes in tumor volume are apparent. Thus, MRI-based radiomics can serve as a non-invasive early treatment assessment to identify malignant responses as early as possible, offering more time for adjusting tumor treatment plans. This study leverages early-phase MRI radiomic features to monitor tumor progression and establish a predictive model, aiming to enable early intervention based on initial imaging data (Figure 1).
 |
Figure 1 The wiring diagram of the article. |
Materials and Methods
Ethics Statement
All animals were purchased from Hunan Laboratory Animal Co., Ltd. The animal experiments were approved by the Key Laboratory of Chongqing University Affiliated Central Hospital and conducted in accordance with the principles outlined by the Institutional Animal Care and Use Committee (IACUC).
Cells
Bone marrow mesenchymal stem cells (MSCs) were isolated from 1- to 7-day-old neonatal mice purchased from Hunan Laboratory Animal Co., Ltd. Bone marrow was extracted, and adherent cells were obtained after 48 hours of culture (with 37°C, 5% CO2, and 10% fetal bovine serum) by removing non-adherent cells. The adherent cells were expanded and passaged to passage 3 (P3) for subsequent experiments. Flow cytometry detected the surface markers (CD29, CD44, CD11b, CD45, BD Biosciences) expression of MSCs. A total of 106 CM38 cells (suspended in 100 μL phosphate buffered saline, PBS) were injected into the right inguinal region of the mice, followed by intravenous injection of 5 × 105 P3 MSCs (suspended in 100ul phosphate buffered saline) via the tail vein 12 hours later. Sixty mice were implanted with tumors, and one tumor was implanted in each mouse. The control group was injected with 100 μL PBS, while the intervention group was injected with 100 μL of mesenchymal stem cell suspension. There were 30 mice in each group.
Imaging
Magnetic resonance imaging (MRI) was performed 7 days post-tumor implantation. Mice were anesthetized with isoflurane (4–5% for induction; 1–2% for maintenance) and scanned using a 3.0T MRI system (Siemens MAGNETOM Prisma) with a dedicated small animal coil. Imaging parameters included: TE 5.6 ms, TR 12.7 ms, FOV 64 mm × 64 mm, slice thickness 0.5 mm, and interslice gap 1 mm. Thermal insulation was maintained during scanning by wrapping mice in cotton pads.
Tumor Growth
Tumor volume was recorded every 48 hours starting one week post-implantation. Tumor size was measured every 2 days using calipers, tumor volume (V) = (1/2) × length (L) × width (W) × height (H). Mice were euthanized via cervical dislocation under anesthesia when the tumor maximal diameter reached 15 mm–20 mm, and tumor tissues were harvested for subsequent analysis.
Hematoxylin-Eosin (HE) and Immunohistochemical
Excised tumor tissues were fixed in 4% phosphate-buffered formalin, paraffin-embedded, and sectioned into 3 μm continuous slices. HE staining was performed for histological examination. Immunohistochemistry (IHC) was conducted to assess CD34 (Beyotime) and Ki67 (HUABIO) expression. Stained images were analyzed using ImageJ software (National Institutes of Health, USA) to quantify expression rates. Independent sample t-test was used for comparison between the two groups of data, and a P value < 0.05 was considered statistically significant.
Radiomics Feature Extraction
T1WI images were selected for feature extraction. All regions of interest (ROIs) were delineated around the tumor boundaries using the Unified Imaging Intelligent One Stop Research Platform (uAI Research Portal, V20230515, https://urp.united-imaging.com/). Two radiologists with over 10 years of experience independently evaluated T1WI without knowledge of clinical outcomes. Automatically extracted radiomics features from each ROI, a total of 1162 image features were extracted, including shape features, firstorder features, and texture features.
Feature Selection and Models Building
A random seed of 20 was used to split the data into groups for the 5-fold cross-validation. Before feature selection, the Z-score normalization was used to standardize all the extracted radiomics features. We applied intraclass coefficient (ICC) analysis to test the consistency of features extracted from two radiologists, and features with an ICC > 0.75 were selected for further analysis. Subsequently, Use K-best to select 300 image features with the highest correlation. Finally, we applied the least absolute shrinkage and selection operator (LASSO) method to select the most powerful features in the training set.
We implemented six different machine learning algorithms on the training dataset, including Gaussian Process (GP), Logistic Regression (LR), Quadratic Discriminant Analysis (QDA), Random Forest (RF), Random Gradient Descent (RGD), and Support Vector Machine (SVM). For each model, receiver operating characteristic (ROC) curves and the average area under the curve (AUC) were used to evaluate predictive performance.
Intraclass correlation coefficients (ICCs) from a two-way random effects model were used to assess interreader agreement for measuring ROI. The RS for prediction of treatment groups was constructed using LASSO statistics. The penalty parameter (l) was selected by 5-foldcross-validationandminimizationofthecross-validationfunction. Independent sample t-test was used to compare the tumor volume between the two groups. p < 0.05 were considered significant.
Results
Third-passage mesenchymal stem cells (MSCs) exhibited a spindle-shaped morphology with adherent growth. Flow cytometry analysis revealed high positive expression of stem cell markers CD29 (90.6%) and CD44 (93.5%), while demonstrating negative expression of CD11b (92.6%) and CD45 (99.7%). CM38 cells displayed adherent growth characteristics with small cell size, high nuclear-to-cytoplasmic ratio, and dense cellular proliferation (Figure 2).
 |
Figure 2 (a) Bone mesenchymal stem cells (MSCs) and colon cancer cells (CM38); (b) The expression of CD11b, CD29, CD44, and CD45 on BMSCs. |
MRI examinations at postoperative day 7 confirmed tumor growth without visible cutaneous protrusion. One control group mouse died after the initial MRI scan due to hypothermia. All remaining mice developed tumors at the implantation site within 9 weeks. 5 tumors (2 in the control group; 3 in the intervention group) reached the maximal diameter of 15 mm–20 mm by Week 3.28 tumors (12 controls; 16 intervention) by Week 4.20 tumors (11 controls; 9 intervention) by Week 5.2 tumors (controls) by Week 7.1 tumor (control) by Week 10 (Table 1).
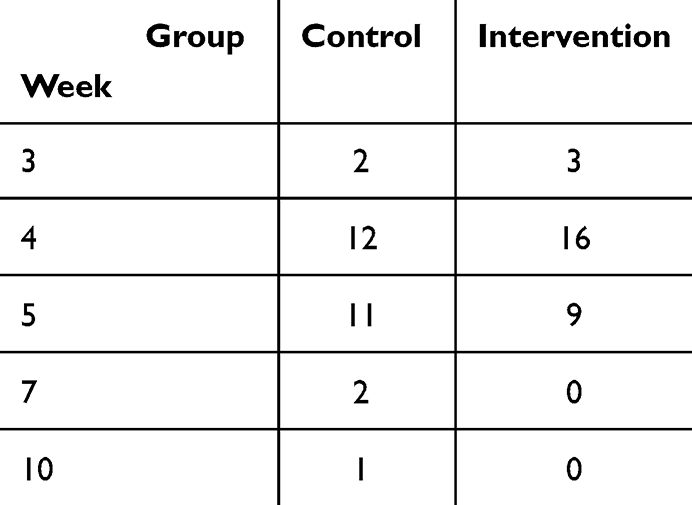 |
Table 1 Time of Tumor to Grow to a Diameter of 15–20 mm |
Additional mortality included 2 mice of control group died without cause at 2 and 3 weeks after tumor implantation, respectively, and the maximum diameter of tumor was less than 15 mm. It can be seen that the tumor growth rate in the intervention group is faster than that in the control group, which indicating tail vein injection of stem cells in the early stages of tumors can promote tumor growth.
At Week 1 post-implantation, MRI revealed no statistically significant difference in tumor volume between groups (P = 0.21). However, upon reaching the first tumor size threshold (15mm-20 mm maximal diameter at Week 3), the MSC intervention group demonstrated significantly larger tumor volumes (99.8 ± 45.9 mm³) compared to controls (72.0 ± 37.2 mm³, P < 0.05). Immunohistochemical analysis showed CD34 expression rate of intervention (3.05% ± 1.16%) compared to controls (2.72% ± 0.44%, P < 0.05), butKi67 expression levels had no significant intergroup differences (19.48% ± 7.02%, 26.81% ± 4.01%, P = 0.12). Which indicating that MSCs promote tumor angiogenesis but have no significant promoting effect on tumor cell proliferation (Figure 3).
 |
Figure 3 (a) Subcutaneous tumor-bearing mouse and the gross morphology of the tumor; (b) Tumor volume on the 1 week and 3 week; (c) HE staining of tumor and the CD34, ki67 expression of tumor. |
Radiomic analysis revealed a total of 1,162 radiomic features extracted from imaging data. Through rigorous feature selection, 17 robust predictive features were identified, including: 10 texture features, 6 first-order features, 1 shape-based feature. A total of 27 predictive models were successfully constructed, all demonstrating high discriminative performance with area under the curve (AUC) >0.8 in both training and test sets (Table 2 and Figure 4).
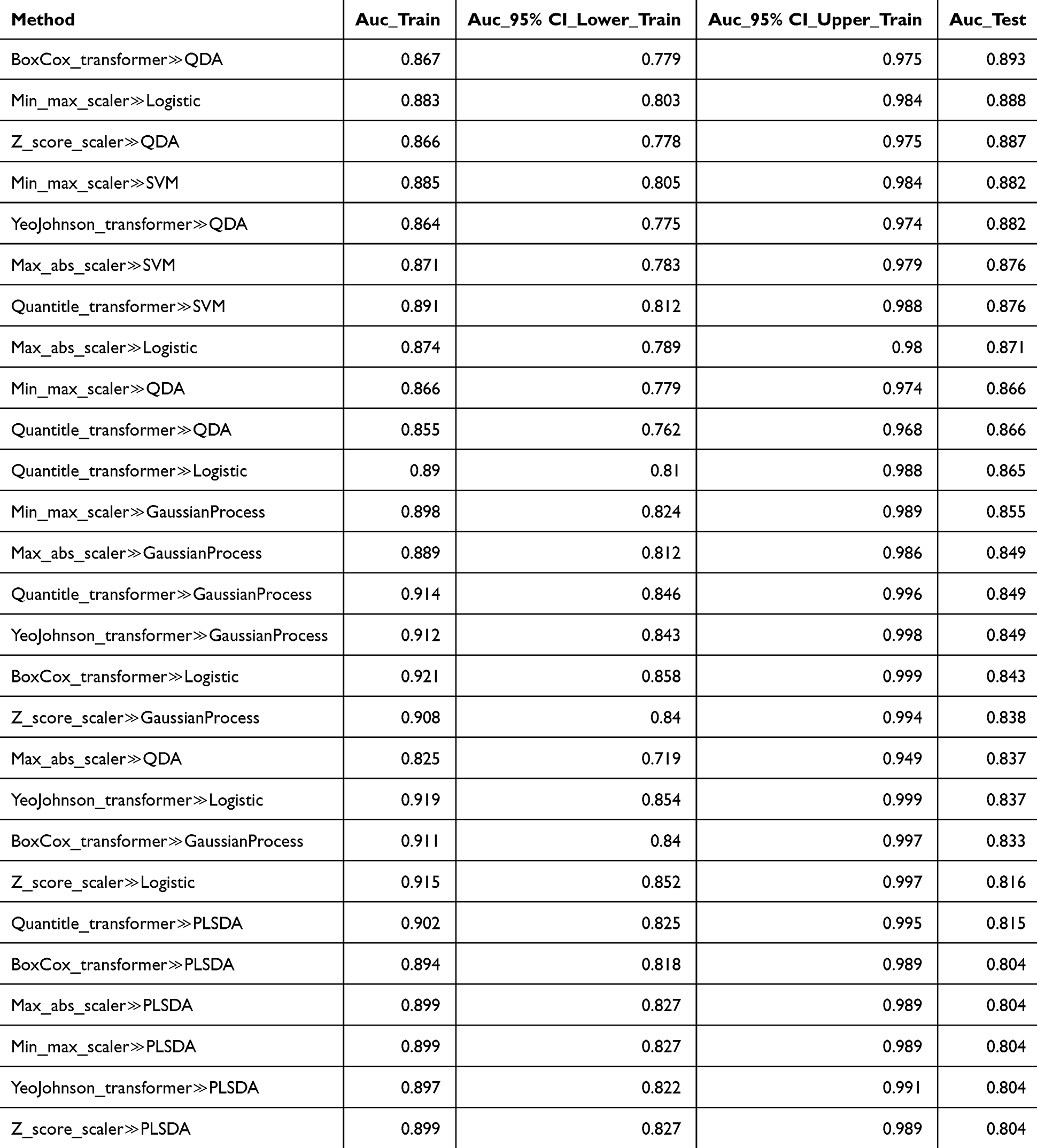 |
Table 2 AUC of the 27 Radiomics Models |
 |
Figure 4 (a) ROI delineation of tumor; (b) Voting results of strongly correlated features; (c) AUC of the radiomics model in training and test sets. |
Discussion
This study established a predictive framework linking early-phase MR radiomic features to tumor progression in a subcutaneous colon cancer model following intravenous mesenchymal stem cell (MSC) intervention. We successfully developed 27 robust models demonstrating strong predictive performance, with area under the curve (AUC) values exceeding 0.8 in both training and test sets and optimal models achieving AUCs up to 0.88. While tumor volume remains a conventional therapeutic monitoring metric, our findings revealed no significant volumetric differences during early intervention phases. This underscores radiomics’ capability to detect pre-morphological tumor alterations, particularly intratumoral heterogeneity, prior to measurable size changes. Notably, texture features dominated our selected high-correlation signatures, Dohan et al similarly demonstrated that texture analysis could predict chemotherapy response before volumetric changes, aligning with prior evidence that radiomic textures reflect tumor complexity,17,22 CD34 is a factor related to the expression of new blood vessels. Kai-Hung Wang et al indicated that MSCs promote ovarian cancer cell proliferation. Wang R et al research has shown that MSC-derived VEGF via HIF-1α signaling in hypoxic microenvironments.23 Contrastingly, Tang RJ et al24 reported tumor-suppressive MSC effects through Smad2/TGF-β-mediated Treg differentiation in colitis-associated cancer models. This discrepancy may arise from differences between our sterile subcutaneous model and inflammation-driven carcinogenesis paradigms. The role of bone marrow mesenchymal stem cells in tumors is controlled by various growth factors, cytokines and chemokines which affect the cell proliferation, angiogenesis and metastasis. Although numerous studies have been conducted to explore the interaction between mesenchymal stem cells and cancer cells, it remains unclear how mesenchymal stem cells communicate with cancer cells and the tumor microenvironment. Further research is needed to confirm this. In our study, consistent with pro-tumorigenic MSC effects, our intervention group exhibited enhanced CD34+ neovascularization compared to controls. It is hypothesized that these significant correlated radiomics features may have a certain correlation with CD34 expression.
While preoperative MR radiomics has been validated for Ki-67 prediction,25,26 we observed no significant Ki-67 expression differences between groups. This null result may reflect limited proliferative heterogeneity in our syngeneic tumor model compared to inter-tumoral variations in clinical studies. In addition, value-added often occurs after angiogenesis, so there can be a mismatch between Ki67 and CD34. This can also explain why Ki67 remains unchanged between groups while CD34 increases.
Despite achieving predictive success, our study has limitations. The modest sample size (n = 30), though ethically justified by animal use minimization principles, constrains radiomics’ generalizability. To mitigate overfitting, we implemented five-fold cross-validation, enhancing model reliability despite limited data. Additional limitation of this study is lack the complexity of an orthotopic model and its exclusive identification of tumor progression-promoting effects, with no capacity to detect or predict tumor-suppressive responses. This critical gap will be systematically addressed in subsequent experimental validations to delineate dual regulatory mechanisms of stem cell intervention.
Conclusion
Tail vein injection of mesenchymal stem cells in 12 hours after subcutaneous inoculation of tumor cells in the groin of mice, tumor growth was accelerated and CD34 expression in the tumor increased, indicating that mesenchymal stem cells have a promoting effect on tumor progression in the initial stage of tumor formation. In addition, the AUC of the model for predicting tumor progression using magnetic resonance imaging radiomics analysis in the early stage of tumor formation was greater than 0.8, indicating that radiomics can predict tumor progression in the early stage of tumor intervention.
Data Sharing Statement
Data can be made available upon reasonable request to the corresponding authors.
Acknowledgments
The technical support from the Chongqing Key Laboratory of Emergency Medicine team was instrumental in data collection. This work was funded by cstc2021jcyj-msxmX0841 and CSTB2024NSCQ-MSX0630 from the Natural Science Foundation of Chongqing and 2023KFKT04 and 2024RCCX04 from the Open subject of Chongqing Key Laboratory of Emergency Medicine and KJQN202300137 from the Science and Technology Research Program of Chongqing Municipal Education Commission.
Funding
1. Natural Science Foundation of Chongqing (No. cstc2021jcyj-msxmX0841 and No. CSTB2024NSCQ-MSX0630); 2. Open subject of Chongqing Key Laboratory of Emergency Medicine (No. 2023KFKT04 and No. 2024RCCX04); 3. Science and Technology Research Program of Chongqing Municipal Education Commission (grant numbers KJQN202300137).
Disclosure
There was no competing interest in this study, as no paid employment, no patent application, and no author will benefit from this study.
References
1. Helissey C, Cavallero S, Guitard N, Théry H, Chargari C, François S. Revolutionizing Radiotoxicity Management with Mesenchymal Stem Cells and Their Derivatives: a Focus on Radiation-Induced Cystitis. Int J Mol Sci. 2023;24(10):9068. doi:10.3390/ijms24109068
2. Iida Y, Yoshikawa R, Murata A, et al. Local injection of CCL19-expressing mesenchymal stem cells augments the therapeutic efficacy of anti-PD-L1 antibody by promoting infiltration of immune cells. J Immunother Cancer. 2020;8(2):e000582. doi:10.1136/jitc-2020-000582
3. Zanganeh E, Soudi S, Zavaran Hosseini A, Khosrojerdi A. Repeated intravenous injection of adipose tissue derived mesenchymal stem cells enhances Th1 immune responses in Leishmania major-infected BALB/c mice. Immunol Lett. 2019;216:97–105. doi:10.1016/j.imlet.2019.10.008
4. TomyTomcy A, Sindhu ER. Mesenchymal stem cells- an excellent therapeutic agent for cancer. Asia Pac J Clin Oncol. 2024;20(1):7–15. doi:10.1111/ajco.13969
5. Ghannam S, Pène J, Moquet-Torcy G, Jorgensen C, Yssel H. Mesenchymal stem cells inhibit human Th17 cell differentiation and function and induce a T regulatory cell phenotype. J Immunol. 2010;185(1):302–312. doi:10.4049/jimmunol.0902007
6. François S, Usunier B, Forgue-Lafitte ME, et al. Mesenchymal Stem Cell Administration Attenuates Colon Cancer Progression by Modulating the Immune Component within the Colorectal Tumor Microenvironment. Stem Cells Transl Med. 2019;8(3):285–300. doi:10.1002/sctm.18-0117
7. Mei R, Wan Z, Yang C, et al. Advances and clinical challenges of mesenchymal stem cell therapy. Front Immunol. 2024;15:1421854. doi:10.3389/fimmu.2024.1421854
8. Liu H, Deng S, Han L, et al. Mesenchymal stem cells, exosomes and exosome-mimics as smart drug carriers for targeted cancer therapy. Colloids Surf B Biointerfaces. 2022;209(Pt 1):112163. doi:10.1016/j.colsurfb.2021.112163
9. Yang J, Lv K, Sun J, Guan J. Anti-tumor effects of engineered mesenchymal stem cells in colon cancer model. Cancer Manag Res. 2019;11:8443–8450. doi:10.2147/CMAR.S209880
10. Zhu H, Li Y, Ding Y, et al. Multi-pool chemical exchange saturation transfer MRI in glioma grading, molecular subtyping and evaluating tumor proliferation. J Neurooncol. 2024;169(2):287–297. doi:10.1007/s11060-024-04729-9
11. Liang HX, Wang ZY, Li Y, et al. The application value of support vector machine model based on multimodal MRI in predicting IDH-1mutation and Ki-67 expression in glioma. BMC Med Imaging. 2024;24(1):244. doi:10.1186/s12880-024-01414-1
12. Liu Z, Wen J, Wang M, et al. Breast Amide Proton Transfer Imaging at 3 T: diagnostic Performance and Association With Pathologic Characteristics. J Magn Reson Imaging. 2023;57(3):824–833. doi:10.1002/jmri.28335
13. Yu H, Wen X, Wu P, et al. Can amide proton transfer-weighted imaging differentiate tumor grade and predict Ki-67 proliferation status of meningioma? Eur Radiol. 2019;29(10):5298–5306. doi:10.1007/s00330-019-06115-w
14. Kong L, Li H, Cai Q, et al. Amide Proton Transfer-Weighted Imaging in Assessing the Aggressive and Proliferative Potential of Bladder Cancer. J Magn Reson Imaging. 2025;61(2):704–712. doi:10.1002/jmri.29464
15. Lin YC, Lin G, Hong JH, et al. Diffusion radiomics analysis of intratumoral heterogeneity in a murine prostate cancer model following radiotherapy: pixelwise correlation with histology. J Magn Reson Imaging. 2017;46(2):483–489. doi:10.1002/jmri.25583
16. Ronot M, Soyer P. Can radiomics outperform pathology for tumor grading? Diagn Interv Imaging. 2024;105(1):3–4. doi:10.1016/j.diii.2023.09.001
17. Espedal H, Fasmer KE, Berg HF, et al. MRI radiomics captures early treatment response in patient-derived organoid endometrial cancer mouse models. Front Oncol. 2024;14:1334541. doi:10.3389/fonc.2024.1334541
18. Müller J, Leger S, Zwanenburg A, et al. Radiomics-based tumor phenotype determination based on medical imaging and tumor microenvironment in a preclinical setting. Radiother Oncol. 2022;169:96–104. doi:10.1016/j.radonc.2022.02.020
19. Sun R, Limkin EJ, Vakalopoulou M, et al. A radiomics approach to assess tumour-infiltrating CD8 cells and response to anti-PD-1 or anti-PD-L1 immunotherapy: an imaging biomarker, retrospective multicohort study. Lancet Oncol. 2018;19(9):1180–1191. doi:10.1016/S1470-2045(18)30413-3
20. Peterson KJ, Simpson MT, Drezdzon MK, et al. Predicting Neoadjuvant Treatment Response in Rectal Cancer Using Machine Learning: evaluation of MRI-Based Radiomic and Clinical Models. J Gastrointest Surg. 2023;27(1):122–130. doi:10.1007/s11605-022-05477-9
21. Beig N, Patel J, Prasanna P, et al. Radiogenomic analysis of hypoxia pathway is predictive of overall survival in Glioblastoma. Sci Rep. 2018;8(1):7. doi:10.1038/s41598-017-18310-0
22. Dohan A, Gallix B, Guiu B, et al. Early evaluation using a radiomic signature of unresectable hepatic metastases to predict outcome in patients with colorectal cancer treated with FOLFIRI and bevacizumab. Gut. 2020;69(3):531–539. doi:10.1136/gutjnl-2018-316407
23. Wang R, Wei W, Rong S, Wang T, Li B. Intravenous Injection of SDF-1α-overexpressing Bone Marrow Mesenchymal Stem Cells has a Potential Protective Effect on Myocardial Ischemia in Mice. Curr Stem Cell Res Ther. 2022;17(4):348–360. doi:10.2174/1574888X17666220318144608
24. Tang RJ, Shen SN, Zhao XY, et al. Mesenchymal stem cells-regulated Treg cells suppress colitis-associated colorectal cancer. Stem Cell Res Ther. 2015;6(1):71. doi:10.1186/s13287-015-0055-8
25. Qian X, Zhou C, Wang F, et al. Development and validation of combined Ki67 status prediction model for intrahepatic cholangiocarcinoma based on clinicoradiological features and MRI radiomics. Radiol Med. 2023;128(3):274–288. doi:10.1007/s11547-023-01597-7
26. Lee JY, Lee KS, Seo BK, et al. Radiomic machine learning for predicting prognostic biomarkers and molecular subtypes of breast cancer using tumor heterogeneity and angiogenesis properties on MRI. Eur Radiol. 2022;32(1):650–660. doi:10.1007/s00330-021-08146-8
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.