Back to Journals » Cancer Management and Research » Volume 18

MPNFS Framework for Managing Herpes Zoster and Refractory Pain in an Immunotherapy-Treated Lung Cancer Patient: A Case Report
Authors Qiao S, Zhang X ![]() , Tian S, Wu Y
, Tian S, Wu Y ![]() , Li Y, Tong Y
, Li Y, Tong Y
Received 10 November 2025
Accepted for publication 29 January 2026
Published 5 February 2026 Volume 2026:18 579681
DOI https://doi.org/10.2147/CMAR.S579681
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Bilikere Dwarakanath
Shina Qiao,1 Xiaoming Zhang,1 Suming Tian,2 Yue Wu,2 Ying Li,1 Yingge Tong3
1Nursing Department, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China; 2Pain Department, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China; 3Public Health and Nursing College, Hangzhou Normal University, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Shina Qiao, Nursing Department, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, 310016, People’s Republic of China, Email [email protected]
Abstract: Patients undergoing treatment with immune checkpoint inhibitors (ICIs) for advanced lung cancer are at increased risk of viral reactivation and severe neuropathic pain. These complications exacerbate the overall symptom burden and psychological distress, underscoring the necessity for integrated nursing interventions aimed at enhancing both physical and psychological well-being. This constitutes a critical priority in contemporary clinical nursing research. We report a 63-year-old woman with stage IV lung adenocarcinoma (cT2aN2M1c, bone metastases) on sindilizumab and anlotinib, who developed severe cervical herpes zoster while carrying an implanted intrathecal drug delivery system (IDDS). She presented with explosive neuropathic pain (NRS 6– 7), cancer pain (NRS 5– 6), and severe anxiety (GAD-7 = 16). Guided by the Medication–Psychological–Nursing–Family–Support (MPNFS) framework, which underscores that nursing care should extend beyond routine medical management to incorporate integrated interventions, and in alignment with the integrative oncology guidelines from the Society for Integrative Oncology (SIO) and the American Society of Clinical Oncology (ASCO), we implemented a coordinated intervention. It encompassed antiviral therapy, multimodal analgesia, psychological support, family engagement, and structured WeChat follow-up. This led to lesion resolution, significant pain and anxiety reduction (NRS 2– 3; GAD-7 = 8), and safe IDDS retention, enabling transition to community for sustained symptom control. This case achieved key outcomes: safe IDDS preservation, effective symptom management, and seamless care continuity. It demonstrates that the MPNFS-guided integrative nursing is a clinical framework for managing complex immunotherapy-related complications, highlighting its vital role in facilitating multidisciplinary coordination and supporting patients through high-risk care transitions.
Keywords: immunotherapy, integrative oncology, lung cancer, MPNFS framework, neuropathic pain
Introduction
Lung cancer remains the foremost cause of cancer-related mortality worldwide, with an estimated 1.8 million deaths reported in 2022.1 The emergence of immune checkpoint inhibitors (ICIs), particularly those targeting programmed cell death protein 1 (PD-1) and programmed death-ligand 1 (PD-L1), has revolutionized the management of advanced lung cancer, significantly improving survival outcomes. Despite these therapeutic advances, ICIs are associated with a distinct spectrum of immune-related adverse events (irAEs) and an increased susceptibility to opportunistic infections.2 Among these, herpes zoster (HZ) reactivation has been increasingly recognized as a notable complication in patients undergoing immunotherapy.3,4 The coexistence of cancer-related pain, HZ-induced neuropathic pain, and psychological distress constitutes a refractory symptom cluster that presents substantial challenges to conventional management strategies.5,6
Conventional nursing practices often fail to incorporate a unified approach that addresses the biological, psychological, and social dimensions of care, focusing instead on symptomatic alleviation. In contrast, integrative oncology emphasizes patient-centered, evidence-informed strategies to support overall well-being throughout the cancer care continuum.6,7 Translating these integrative principles into daily nursing practice requires a systematic, theory-driven framework that bridges pharmacologic and psychosocial domains.
The Medication–Psychological–Nursing–Family–Support (MPNFS) framework provides a structured response to this limitation. Originally developed for the management of psychiatric disorders, the MPNFS framework has been adapted and validated in oncology settings.8–10 It emphasizes that nursing should not be limited to medical care alone but should encompass integrated interventions across five dimensions: Medication therapy optimization, Psychological intervention, specialized Nursing services, Family care coordination, and Social support mobilization.10 Empirical studies have demonstrated its effectiveness for chemotherapy support in reducing psychological distress, fatigue, and symptom burden among patients with acute leukemia and lung cancer.9–11
Nevertheless, the application of the MPNFS framework in the context of immunotherapy remains limited, particularly for complex clinical scenarios involving viral reactivation, refractory pain, and psychological distress. Such multifaceted symptom clusters often transcend the boundaries of conventional nursing approaches and demand integrative, collaborative interventions. To address this gap, the present case report explores the implementation of the MPNFS framework within the integrative oncology paradigm, incorporating intrathecal drug delivery systems (IDDS) and tele-nursing to manage herpes zoster–related neuropathic pain and psychological distress in a patient with advanced lung cancer undergoing immunotherapy.
Case Presentation
This case report follows the CARE guidelines.12
Patient Information
The patient was a 63-year-old woman diagnosed with adenocarcinoma of the right lower lobe (stage cT2aN2M1c) with bone metastases. She had received nine cycles of sindilizumab (200 mg IV every 3 weeks) combined with anlotinib (12 mg orally daily, held peri-operatively) for systemic control. For refractory cancer-related pain, she had undergone IDDS implantation one year earlier, maintaining an Eastern Cooperative Oncology Group (ECOG) performance status of 2.
The patient reported a previous minor wound dehiscence at the IDDS port site, though without infection. She lived with her husband, had one adult son, and reported good family support but expressed emotional exhaustion from prolonged treatment.
Initial Presentation and Assessment
She developed clustered vesicular eruptions on the left neck with intense burning pain radiating to the head. On examination, classic HZ rash was observed over the left cervical dermatome (C3–C4)—tense vesicles on an erythematous base containing clear fluid. The IDDS infusion consisted of morphine 1.5 mg/mL + ropivacaine 0.45% at 0.2 mL/h with a 0.5 mL bolus option. Pain: NRS 6–7 at the rash site, lancinating pain; NRS 5–6 at the left hip and lower back (metastatic pain), pressure-like pain. She exhibited marked anxiety (GAD-7 = 16) with frequent crying spells. IDDS port site showed minimal serous discharge but no erythema or swelling.
A brain CT scan and a wound culture from the IDDS site were obtained. CT revealed mild cerebral atrophy and ischemic changes without signs of infection. Microbiologic evaluation (Table 1) identified Klebsiella aerogenes and Enterobacter cloacae subsp. cloacae, demonstrating susceptibility to levofloxacin and most β-lactams, resistance to trimethoprim-sulfamethoxazole, and no evidence of fungal growth.
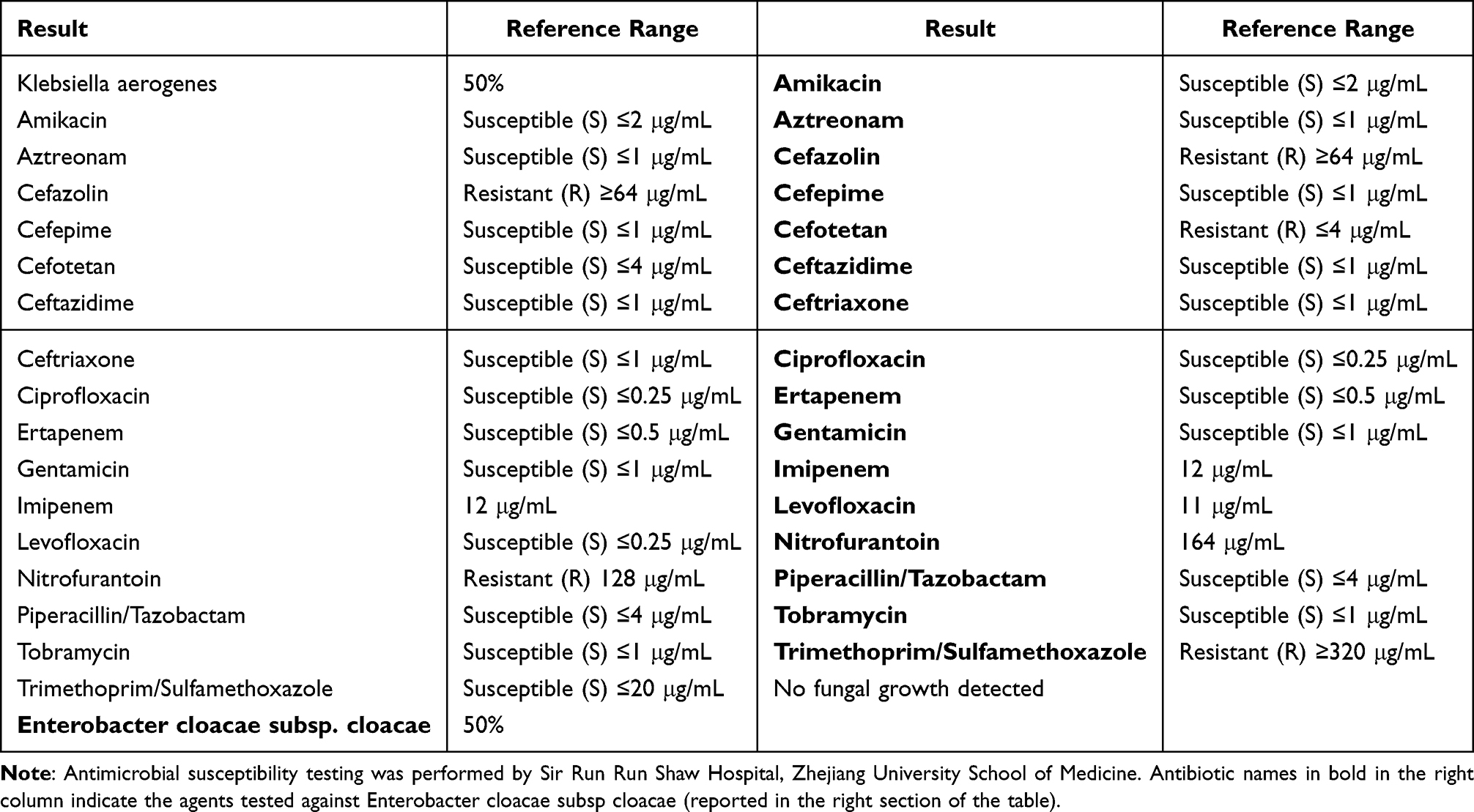 |
Table 1 Microbiology Laboratory Report (Wound Discharge) |
Diagnostic Assessment
Based on clinical, laboratory, and imaging findings, the patient was diagnosed with: Herpes zoster (left cervical dermatome); Refractory mixed pain syndrome (cancer pain + HZ-related neuropathic pain); Localized IDDS port infection (no intracranial involvement); Severe anxiety related to pain and disease stress. Our primary goal was to achieve infection control, pain relief, and psychological stabilization through an MPNFS-guided integrative nursing plan.
Therapeutic Intervention (MPNFS Framework Application)
The care plan was developed and implemented according to the MPNFS framework, encompassing five interdependent dimensions: Medication therapy optimization, Psychological intervention, specialized Nursing services, Family care coordination, and Social support mobilization. This structure enabled the systematic delivery of multimodal therapy, aligning with the SIO–ASCO Integrative Oncology principles of patient-centered, evidence-based care.6,7 The patient’s clinical course and main intervention were summarized in Figure 1.
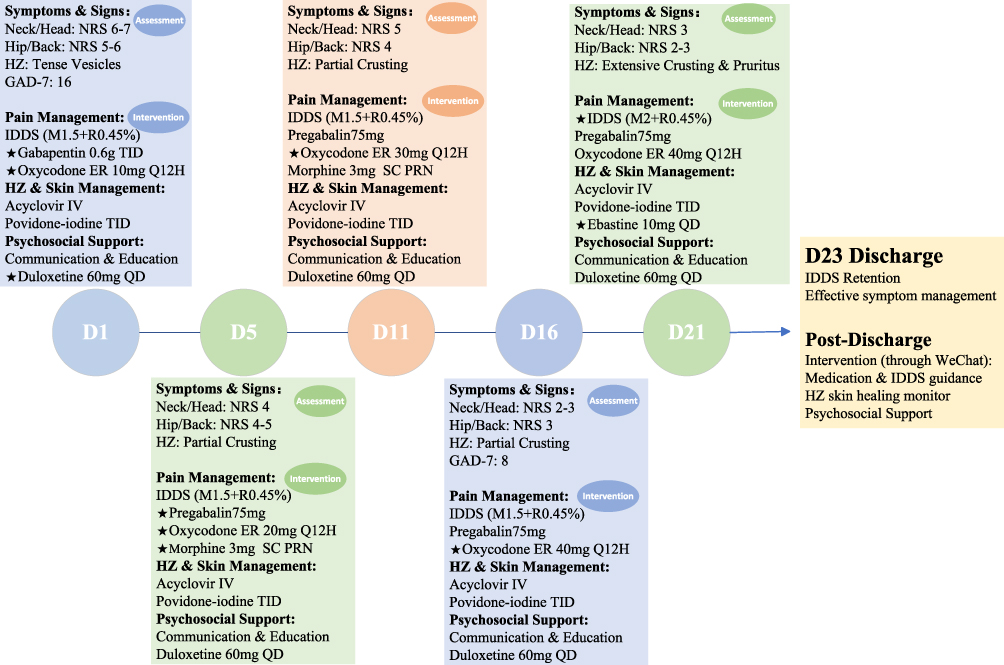 |
Figure 1 Disease Progression Diagram. Abbreviations: D, day; BID, twice daily; ER, extended-release; HZ, herpes zoster; IDDS, intrathecal drug delivery system (M, morphine [mg/mL]; R, ropivacaine [0.45%]); IV, intravenous (500mg Q12H); NRS, numeric rating scale; PRN, as needed; QD, once daily; SC, subcutaneous; TID, three times daily; ★, dose change or increase; Bold Text: key interventions or critical disease stages. |
Medication Therapy Optimization (M)
Antiviral and Supportive Therapy
Following dermatologic consultation, we initiated intravenous acyclovir 500 mg every 12 hours to inhibit viral replication and oral methylcobalamin 0.5 mg three times daily to promote neural repair.
Vesicles were aseptically aspirated, and povidone-iodine was applied by nurses three times daily. The lesions had crusted gradually, and then itching was controlled with ebastine 10 mg daily. Complete epithelialization occurred after 21 days, with no recurrence or adverse effects.
Multimodal Pain Management
In response to an inadequate analgesic regimen, a therapeutic adjustment was instituted, accompanied by vigilant monitoring for adverse effects.
Before the exclusion of intracranial infection, oxycodone was uptitrated to 40 mg q12h, and gabapentin was replaced with pregabalin (75 mg bid), with 3 mg subcutaneous morphine available for breakthrough pain. The IDDS was then optimized by increasing the morphine concentration to 2 mg/mL while maintaining the 0.2 mL/h and 0.5 mL bolus after the exclusion of intracranial infection. Duloxetine 60 mg daily was added to address both neuropathic pain and anxiety. After 15 days, pain scores improved and stabilized markedly (NRS reduced from 6–7 to 2–3). Consequently, oxycodone was successfully discontinued at discharge.
Infection Management
A small amount of serous secretion was shown at the IDDS port site, and therefore, a culture of wound secretion was performed. Although the pain management team recommended suspending IDDS therapy until culture results were available, the patient declined, and thus the treatment was continued in accordance with the patient’s preference. The culture results showed that both were sensitive to levofloxacin and most β-lactams. Accordingly, a 3-day course of oral levofloxacin (0.5 g once daily) was administered, which led to the resolution of drainage and normalization of inflammatory markers on follow-up.
Psychological Intervention (P)
At admission, the patient exhibited severe anxiety (GAD-7 = 16) and emotional instability. In accordance with SIO–ASCO guidance on managing anxiety and depression in cancer,6,7 we applied non-pharmaceutical and pharmaceutical psychological interventions.
A multi-component supportive strategy was implemented. This included empathetic communication and procedural education from the nursing team, coupled with relaxation training (eg, controlled breathing at 10–15 breaths/min, twice daily) directed by a mental health specialist nurse. Pharmacologically, duloxetine 60 mg daily was initiated for dual neuropathic pain and mood modulation. After 16 days of this combined regimen, the patient’s anxiety significantly improved (GAD-7 score: 8), and the patient subjectively reported feeling “in control again.”
Specialized Nursing Services (N)
The specialized nursing protocol included comprehensive medication management, continuous symptom monitoring, wound care, infection prevention, psychological support, and education on empowerment. Specifically, the pain nurse addressed gabapentin-related dizziness and nausea through dedicated education to improve adherence, conducted regular IDDS site assessments, monitored pain trends for analgesic titration, and educated the patient on recognizing early signs of infection to ensure effective self-management after discharge.
Family Care Coordination (F)
Recognizing that sustained cancer care relies critically on family involvement, the “F” (Family) dimension prioritized shared responsibility and emotional alignment. This was integrated into practice by involving the patient’s husband and son in educational sessions on pain observation, medication scheduling, and emotional support techniques. The family was coached to maintain a calm, supportive environment and to assist with gentle skin care. Before discharge, they received orientation on IDDS troubleshooting and guidance on when and how to seek professional help. This structured family engagement effectively alleviated anxiety in both the patient and her caregivers.
Social Support Mobilization(S)
A structured WeChat-based telemedicine follow-up was implemented post-discharge to bridge the care transition, utilizing a platform that is both culturally adapted and highly accessible in China.13 Its functions encompassed video monitoring of HZ healing and the IDDS site, standardized self-reporting of pain and anxiety, real-time medication guidance, and coordination with community hospitals for ongoing IDDS maintenance and terminal care.
This Social support mobilization dimension not only ensured ongoing professional oversight but also reduced the patient’s isolation, enabling care continuity. The family reported high satisfaction and gratitude for “always having someone to turn to.”
Follow-Up and Outcomes
At the 1-month follow-up, HZ had resolved, and cancer pain was stably controlled. Our hospital collaborates with a local community hospital to provide continuous IDDS analgesia during the terminal stage, guiding adjustments to analgesics and parameters based on the patient’s condition via WeChat. The patient continued using the IDDS for another year. At the terminal stage, the patient passed away in a local community hospital peacefully. The patient and her family are satisfied with the pain management.
Discussion
Varicella-zoster virus (VZV), a ubiquitous double-stranded DNA alpha herpesvirus, establishes lifelong latency in sensory ganglion neurons. It causes two main human illnesses: primary varicella (chickenpox) and reactivation as herpes zoster (shingles).14 The disease progresses through three primary stages. It begins with a prodromal (pre-rash) phase, characterized 2–3 days before rash onset by systemic symptoms (fatigue, headache, low-grade fever) and neuropathic sensations (itching, burning, or tingling) in the involved dermatome. This is followed by the acute/active phase, where a painful, dermatomal rash develops, frequently resulting in substantial quality-of-life impairment. In the chronic phase, roughly 20% of patients suffer from postherpetic neuralgia (PHN), a condition of persistent neuropathic pain that endures long after the rash resolves.14
The coexistence of cancer-related pain and PHN often leads to refractory symptoms, complicating conventional analgesic strategies due to drug interactions or systemic toxicity. The intrathecal drug delivery system (IDDS) has emerged as an effective therapeutic alternative for refractory pain.15,16 However, the prolonged home-based care required for IDDS management presents substantial challenges for both patients and caregivers. This case report illustrates the integrated management of an advanced lung cancer patient with postherpetic neuralgia during PD-1 inhibitor therapy, highlighting the critical role of MPNFS in oncological comorbidity management.
Studies17–19 demonstrate that the integrative care enhances symptom control, improves quality of life, and may extend survival. This case experienced overlapping cancer pain, herpes zoster–related neuropathic pain, and severe anxiety—conditions that are difficult to address through pharmacologic treatment alone. The MPNFS framework enabled seamless integration between antiviral therapy, multimodal analgesia, psychological stabilization, and family engagement.
During immunotherapy for lung cancer, this case developed herpes zoster, and serous discharge was observed at the IDDS port site. The patient faced multiple risks, including aggravated pain and infection that could lead to discontinuation of IDDS use. These acute complications caused significant physical and psychological distress. Based on the MPNFS framework, the healthcare team provided medication and education, closely monitored medication adverse reactions, reinforced psychological support, and guided relaxation exercises. Family members were encouraged to offer emotional support and actively participate in the healthcare. Continuous post-discharge nursing and social support were also provided, ultimately alleviating the patient’s symptoms.
Upon admission, the patient exhibited severe anxiety and was visibly distressed, crying. The medical team responded promptly by implementing comprehensive and individualized management tailored to the patient’s condition. To alleviate pain associated with herpes zoster, gabapentin was initiated; however, the patient experienced dizziness and nausea during the initial treatment phase, which exacerbated anxiety. The pain team strengthened medication education for patients and family members, providing coping strategies and enhancing medication safety and adherence. Due to suspected intracranial infection, the pain team initially advised discontinuation of the IDDS. However, the patient insisted on its continued use. Upon discussion with the patient, it was recommended to maintain the current IDDS parameters while introducing oxycodone and gabapentin. Due to persistent and worsening pain, the treatment was switched to pregabalin. After ruling out intracranial infection, the IDDS dosage was adjusted, and the analgesic regimen was continuously optimized, ultimately achieving effective pain relief.
Concurrently, interventions were delivered by mental health physicians and specialist nurses, including psychological counseling, bedside relaxation training, and the adjunct administration of duloxetine. Family members were also encouraged to offer active emotional support. Together, these measures contributed to the alleviation of the patient’s anxiety. These findings are consistent with prior studies,9,10 which demonstrated that the MPNFS model can effectively reduce negative emotional symptoms in lung cancer patients undergoing chemotherapy.
Following discharge, the medical team continued to monitor the healing of the herpes zoster lesions, pain levels, and IDDS usage via WeChat. In the terminal stage, through collaboration with community hospitals, effective symptom control was maintained, allowing the patient to pass away peacefully.
The patient experienced debilitating pain and severe anxiety during the acute phase, which profoundly disrupted daily function. She reported that the multimodal analgesia protocol provided crucial relief, while consistent communication from the healthcare team offered essential support. Although pain was well-controlled at discharge, residual skin pruritus remained bothersome. The structured WeChat follow-up plan enhanced her confidence during recovery at home. This case highlights the importance of early, aggressive multimodal analgesia combined with integrated psychosocial assessment and support. Management should be dynamically adjusted based on frequent reassessment, and continuity of care—including structured remote follow-up—should be planned from admission to optimize outcomes and prevent chronic pain.
However, this study has several limitations, primarily stemming from its single-case design. First, the findings are context-specific to the individual patient described; thus, they lack generalizability to broader populations undergoing PD-1 therapy. Second, the assessment of outcomes relied predominantly on subjective symptom scores. The absence of standardized, longitudinal objective measures limits the mechanistic interpretation of outcomes and the ability to track sustained intervention effects. While this report suggests the potential utility of the MPNFS framework, its efficacy and broader applicability must be rigorously evaluated through future multi-center trials or mixed-method studies incorporating controlled designs and objective biomarkers.
Conclusion
The MPNFS-guided integrative nursing framework offers a practical structure for managing multifaceted symptoms in cancer pain patients receiving immunotherapy, thereby facilitating holistic care continuity from hospital to home. This case demonstrates its initial feasibility in direct care. To support broader implementation, future initiatives should first develop specialized training to equip nurses with the competencies necessary for integrative symptom management in the organizations.
Ethics Approval from Hospital Committee
The Human Subjects Committee of Affiliated Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, approved this case.
Declaration of Patient Consent
Written informed consent was obtained from the patient and her family for publication of this case report and accompanying details. Personal identifiers have been fully anonymized.
Acknowledgments
We sincerely thank the patient and her family for consenting to share her experience and for their trust throughout her care journey.
Funding
The study was supported by the Zhejiang Provincial Hospital Association (No. 2022ZHA-YZJ207) and the Health Commission of Zhejiang province (No. 2023KY117, No. 2024KY1098). The funding agents played no role in the design of the study, data collection, analysis, interpretation, or manuscript writing. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no conflicts of interest related to this publication.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–8. doi:10.3322/caac.21834
2. Steinmann M, Lampe D, Grosser J, et al. Risk factors for herpes zoster infections: a systematic review and meta-analysis. Infection. 2024;52(3):1009–1026. doi:10.1007/s15010-023-02156-y
3. Thompson RR, Kong CL, Porco TC, Kim E, Ebert CD, Acharya NR. Herpes zoster and postherpetic neuralgia: changing incidence rates from 1994 to 2018 in the United States. Clin Infect Dis. 2021;73(9):e3210–e3217. doi:10.1093/cid/ciaa1185
4. Jung J, Park SY, Park JY, Kim D, Lee K, Choi S. Reactivation of varicella-zoster virus in patients with lung cancer receiving immune checkpoint inhibitors: a nationwide study. Cancers. 2024;16(8):1499. doi:10.3390/cancers16081499
5. Zeng Y, Jin Y. Research progress on risk factors for postherpetic neuralgia. Chin J Pain Med. 2020;26(8):603–607. doi:10.3969/j.issn.1006-9852.2020.08.009
6. Carlson LE, Ismaila N, Addington EL, et al. Integrative oncology care of symptoms of anxiety and depression in adults with cancer: society for integrative oncology–ASCO guideline. J Clin Oncol. 2023;41:4562–4591. doi:10.1200/JCO.23.00857
7. Carlson LE, Ismaila N, Addington EL, et al. Integrative oncology care of symptoms of anxiety and depression in adults with cancer: SIO–ASCO guideline summary and Q&A. JCO Oncol Pract. 2023;19(12):847–851. doi:10.1200/OP.23.00358
8. Deng K, Yuan X. Personality traits, anxiety and self-esteem in psychiatric patients: an analysis and reflection on the MPNFS model. J. Yangtze Univ. 2019;16(9):109–113.
9. Wang Z, Wang J, Ren J. Application of multi—directional nursing based on MPNFS theory in patients undergoing lung cancer chemotherapy and its influences on psychological distress and hope level. China J Health Psychol. 2023;31(7):1031–1035. doi:10.13342/j.cnki.cjhp.2023.07.014
10. Zhu Y, Liu Y. Application Efficacy of Nursing Interventions Guided by the Medication–Psychological–Nursing–Family–Support (MPNFS) Framework in Mitigating Cancer-Related Fatigue and Enhancing Pulmonary Function Among Lung Cancer Patients Undergoing Chemotherapy. Cancer Manage Res. 2025;17:1777–1787. doi:10.2147/CMAR.S536068
11. Tang Y, H W, Shen H, Yuan X, Du D. The effect of multidimensional supportive nursing on the mental health and caregiver burden of patients with acute leukemia under the guidance of MPNFS theory. Pract J. Clin. Med. 2023;20(6):126–130. doi:10.3969/j.issn.1672-6170.2023.06.030
12. Gagnier JJ, Kienle G, Altman DG, et al. The CARE guidelines: consensus-based clinical case reporting guideline development. Headache. 2013;53(10):1541–1547. doi:10.1111/head.12246
13. Qiao S, Tang L, Zhang W, et al. Nurse-led follow-up for outpatients with cancer pain treated with opioids: weChat vs. telephone-only support. Patient Prefer Adherence. 2019;13:923–931. doi:10.2147/PPA.S203900
14. Hasan S, Khan NI, Nake AA, Tarranum F. Herpes zoster with oro-facial involvement – report of a case and detailed review of literature. Indian J Dent. 2012;3(2):94–101. doi:10.1016/j.ijd.2012.03.011
15. Deer TR, Pope JE, Hayek SM, et al. The Polyanalgesic Consensus Conference (PACC): recommendations on Intrathecal Drug Infusion Systems Best Practices and Guidelines. Neuromodulation. 2017;20(2):96–132. doi:10.1111/ner.12538
16. Feng Z, Wang K, Jin Y. Chinese expert consensus on intrathecal drug delivery technology for cancer pain management (2022 edition). Chin J Pain Med. 2022;28(7):579–589. doi:10.3760/cma.j.cn101658-20220208-00140
17. Eom KY, Mann B, Halpern MT. Integrated care among patients with kidney or urinary bladder cancer: an NCI patterns-of-care analysis. Urol Oncol. 2025;43(3):
18. Weaver SJ, Jacobsen PB. Cancer care coordination: opportunities for healthcare delivery research. Transl Behav Med. 2018;8(3):503–508. doi:10.1093/tbm/ibx079
19. Hui D, Hannon BL, Zimmermann C, Bruera E. Improving patient and caregiver outcomes in oncology: team-based, timely, and targeted palliative care. CA Cancer J Clin. 2018;68(5):356–376. doi:10.3322/caac.21490
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.