Back to Journals » Clinical Ophthalmology » Volume 16
Motorcycle-Associated Ocular Injuries: A Narrative Review
Authors Kim EJ, Ganga A, Kang C, Elnemer W, Lee JY, Ronquillo YC ![]() , Hoopes PC
, Hoopes PC ![]() , Moshirfar M
, Moshirfar M ![]()
Received 21 August 2022
Accepted for publication 6 October 2022
Published 18 October 2022 Volume 2022:16 Pages 3457—3479
DOI https://doi.org/10.2147/OPTH.S387034
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Eric J Kim,1 Arjun Ganga,1 Chaerim Kang,2 William Elnemer,3 James Y Lee,4 Yasmyne C Ronquillo,5 Phillip C Hoopes,5 Majid Moshirfar5– 7
1Division of Ophthalmology, Warren Alpert Medical School at Brown University, Providence, RI, USA; 2Program in Liberal Medical Education, Brown University, Providence, RI, USA; 3Johns Hopkins School of Medicine, Baltimore, MD, USA; 4Brown University, Providence, RI, USA; 5Hoopes Vision Research Center, Draper, UT, USA; 6John A. Moran Eye Center, University of Utah School of Medicine, Salt Lake City, UT, USA; 7Utah Lions Eye Bank, Murray, UT, USA
Correspondence: Eric J Kim, Division of Ophthalmology, Warren Alpert Medical School at Brown University, Providence, RI, USA, Tel +1 978-289-0659, Email [email protected]
Purpose: Motorcycle-related injuries involving the eye and orbit are not well characterized, with a paucity of prospective studies focusing specifically on motorcycle-associated eye injuries nor literature reviews having been conducted on the subject. To better understand the injury types and descriptive characteristics of patients experiencing motorcycle-associated eye injuries, we sought to conduct a narrative review.
Methods: The research team utilized the following databases: PubMed, EMBASE, and Web of Science to query for English articles from peer-reviewed journals that provided some patient data regarding eye injury due to motorcycle or moped accidents or usage.
Results: A total of 65 studies were included in our qualitative synthesis. Of these studies, 40 (61.5%) were case reports, 20 retrospective case series (30.8%), and five (7.69%) were observational prospective studies. Among the 25 retrospective and prospective studies, 12 (48.0%) of these studies primarily focused on motorcycle-associated injuries. These 65 studies described a wide variety of motorcycle-associated eye injuries, including but not limited to orbital fractures and associated sequelae, foreign bodies, vitreoretinal trauma, neuro-ophthalmic trauma, corneal injuries, open globe injuries, lacerations, and globe avulsions.
Conclusion: The current state of the literature indicates that knowledge regarding the ocular manifestations of motorcycle accidents is limited to mostly case reports and few retrospective cohort studies focused specifically on motorcycle-associated eye injuries. However, it is evident that the types of motorcycle-associated eye injuries are legion and predominantly seen in adult males, potentially leading to severe injuries and loss of vision and blindness.
Keywords: motorcycle, ocular injury, eye, trauma, orbital fracture, ruptured globe, corneal injury, vitreoretinal damage, vehicular accidents
Introduction
Road traffic accidents lead to millions of injuries and are the leading cause of death in 5–29 year-olds globally.1 Among road traffic accidents, those associated with motorcycles carry a particularly high risk of injury and death, with the US federal government estimating that per mile traveled, motorcycle-related deaths were nearly 29 times higher than those associated with cars in 2019.2 The number of motorcycle fatalities is also increasing, with the most recent data in the United States showing a 9% increase in 2021 from 2020.3 The issue of motorcycle injury and deaths also disproportionately affects low- and middle-income countries, with countries with lower GDP per capita having an increased prevalence of motorcycle-related deaths compared to car-related deaths.4,5
The literature identifying and characterizing limb and head injuries associated with motorcycle crashes is well established, with closed fractures of the limbs and traumatic brain injuries identified as common injury types.6–12 However, motorcycle-related injuries involving the eye and orbit are not well characterized, with a paucity of large cohort studies focusing specifically on motorcycle-associated eye injuries nor literature reviews having been conducted on the subject, to our knowledge. While it can be reasoned that penetrating eye injuries and orbital fractures may be common and motorcycle-associated eye injuries can lead to permanent visual deficits, the prevalence of additional injury types and outcomes of motorcycle-related ocular injuries are not well understood. One way to possibly lower the risk of ocular injuries is through the use of protective equipment such as visors, goggles, and windscreens.13–15 However, the use of protective equipment may not be widespread. The most recent report on the subject demonstrated that in 73% of motorcycle accidents, the rider wore no eye protection, implying that foreign bodies or the effect of wind caused impaired vision that consequently delayed the detection of possible hazards. In addition, there is a possible elevated risk of direct ocular injuries resulting from the crashes themselves.16,17
To better understand the injury types and descriptive characteristics of patients experiencing motorcycle-associated eye injuries, we sought to review the literature on the subject. Using our findings, we hope to fill a significant gap in the literature and combine all existing knowledge of motorcycle- and moped-associated eye injuries. To our knowledge, such a literature review has not been performed. We hope this study raises provider awareness of motorcycle-related eye injuries and care, particularly in acute trauma settings.
Materials and Methods
Literature Search
The research team utilized the following databases: PubMed, EMBASE, and Web of Science, and the following search terms for each database: (Motorcycle OR motorbike OR mini bikes OR pocket bikes OR mopeds OR motorized-bike OR motorized bike OR motorized cycle OR motorized-cycle OR scooter) AND (eye OR optic OR ophthalmic OR ophthalmologic OR ophthalmological OR globe OR orbit OR ophthalmology OR eyeball OR ocular OR orbital). Among our search terms, we included the term “scooter” because it can be used as a colloquial term for mopeds. However, we did not include kick scooters or recreational electric scooters in our analysis. The search was conducted from July 1st to July 4th, 2022, and our searches were not restricted by date.
Selection of Studies
The abstract and title and full-text screenings were conducted by two independent reviewers (EK and AG) using Covidence (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia). Both reviewers had to concur on a study’s eligibility to progress to the next stage of the literature screening process. Any conflicts were mediated through meetings and discussions.
All English articles from peer-reviewed journals that provided some patient data regarding eye injury due to motorcycle or moped accidents or usage were included in our analysis. Studies were only eligible if the described eye injuries were incurred while operating a motorcycle or riding a motorcycle as a passenger. For example, studies reporting eye injuries incurred by pedestrians being struck by a motorcyclist did not fit our inclusion criteria. We also excluded abstracts, conference proceedings, and studies that utilized previously published data.
Risk of Bias Assessment
For non-randomized studies, we utilized Cochrane’s ROBINS-I tools to assess whether a study had a low, moderate, serious, or critical risk of bias.18 All domains provided by the ROBINS-I tools were considered when determining bias ratings for each study. Two reviewers (EK and AG) independently determined the risk of bias scores for each study, and any discrepancies in ratings were resolved through discussion.
Results
Search Results
The details of the narrative review literature screening process can be found in our flowchart (Figure 1). From the three queried databases, we identified a total of 1529 total studies to be screened, 65 of which were included in our qualitative synthesis.
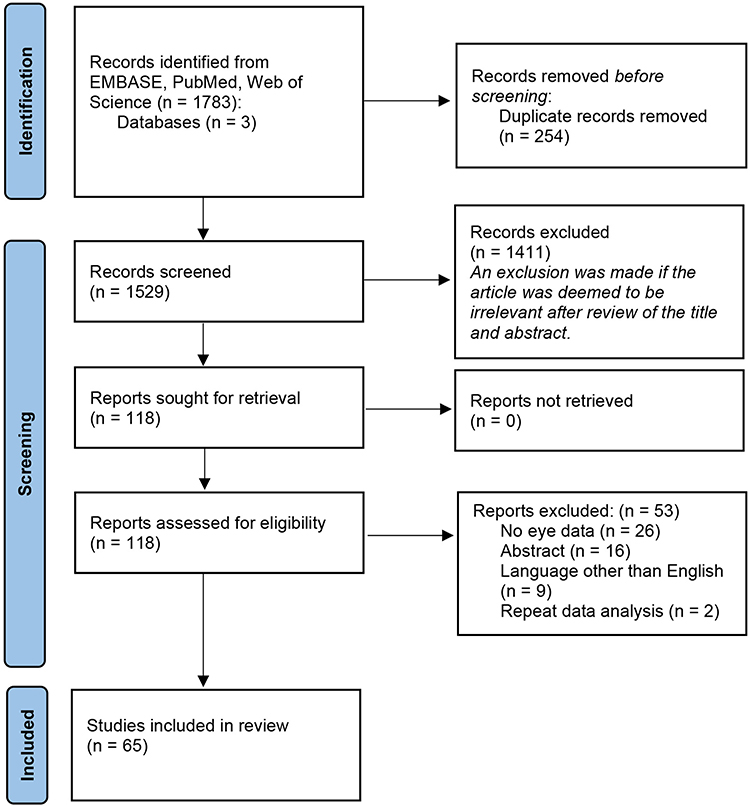 |
Figure 1 The initial search of three total databases yielded a total of 1529 results after 254 duplicates were removed by Covidence. A total of 118 full texts were assessed, 65 of which were eligible for qualitative synthesis. Adapted from Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi: 10.1136/bmj.n. |
General Characteristics of Studies
Table 1 provides an overview of the 65 studies that met our inclusion criteria. A total of 65 studies provided data regarding eye injuries that could be attributed to motorcycle usage and/or accidents.19–83 Of these studies, 40 (61.5%) were case reports, 20 (30.8%) retrospective case series, and five (7.69%) were observational prospective studies.19–83 Among the 25 retrospective and prospective studies, 12 (48.0%) of these studies primarily focused on motorcycle-associated injuries. The other 13 (52.0%) studies primarily focused on describing the epidemiology of a given type of injury (ie orbital fractures) or a specific etiology (ie motor vehicle accidents in general) and secondarily provided brief data regarding motorcycle-associated eye injuries. These 65 studies described a wide variety of motorcycle-associated eye injuries, including but not limited to orbital fractures and associated sequelae, foreign bodies, vitreoretinal trauma, neuro-ophthalmic trauma, corneal injuries, open globe injuries, lacerations, and globe avulsions. Many of these articles were conducted by authors from the United States (14/65, 21.5%). Thirty-seven (56.7%) of these studies were published between 2012–2022. Fifteen (15/25, 60.0%) studies were rated as having low bias, eight (8/25, 32.0%) moderate, and two (2/25, 8.00%) high risk of bias.
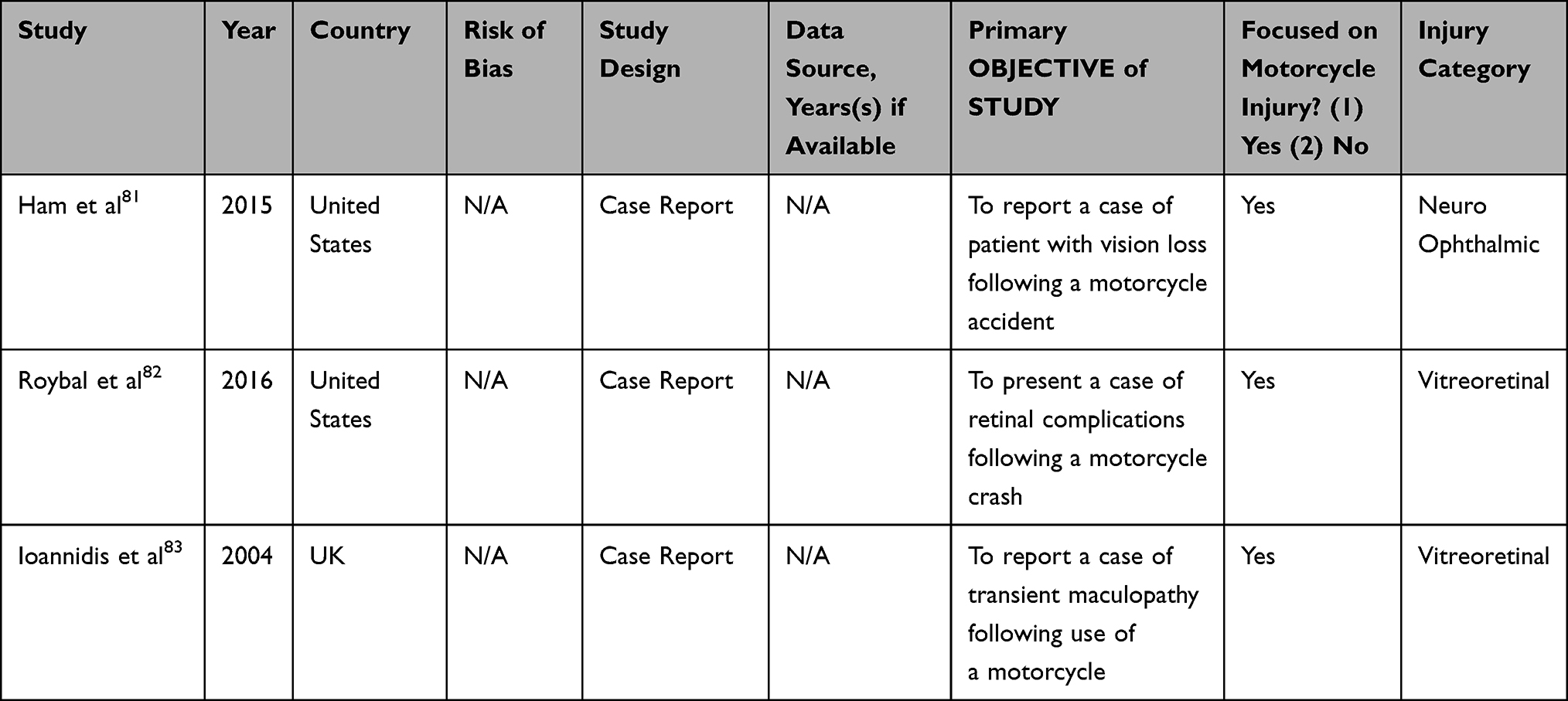 |
Table 1 General Characteristics of Studies That Include Motorcycle-Related Eye Injury Data |
It is important to note that the relative distribution of male and female patients, data regarding age and long-term sequelae could not be determined in many of the retrospective and prospective studies because of how the aggregate data were reported (Tables 2–8). As aforementioned above, many of these retrospective and prospective studies did not primarily focus on motorcycle-associated injury, and therefore data regarding motorcycles were inconsistently reported among the studies. In addition, several studies reported aggregate, mixed data in a manner that precluded the reviewers from parsing out any motorcycle-specific data and made it impossible to determine whether reported eye injuries were indeed caused by motorcycles.84,85 Therefore, these studies were excluded from our analysis.
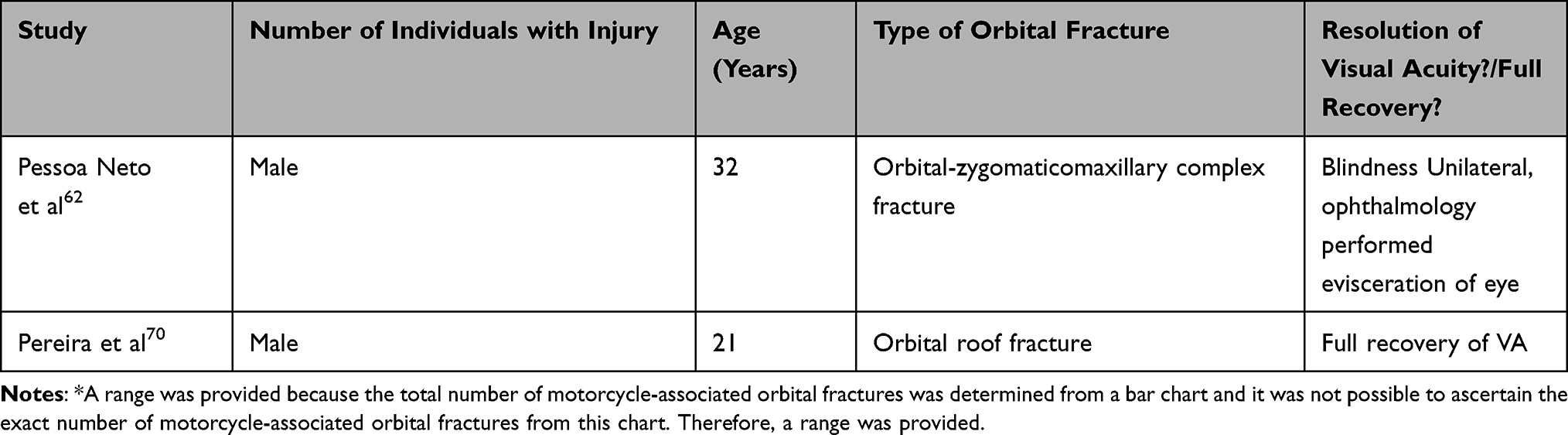 |
Table 2 Characteristics of Patients with Motorcycle-Associated Orbital Fractures |
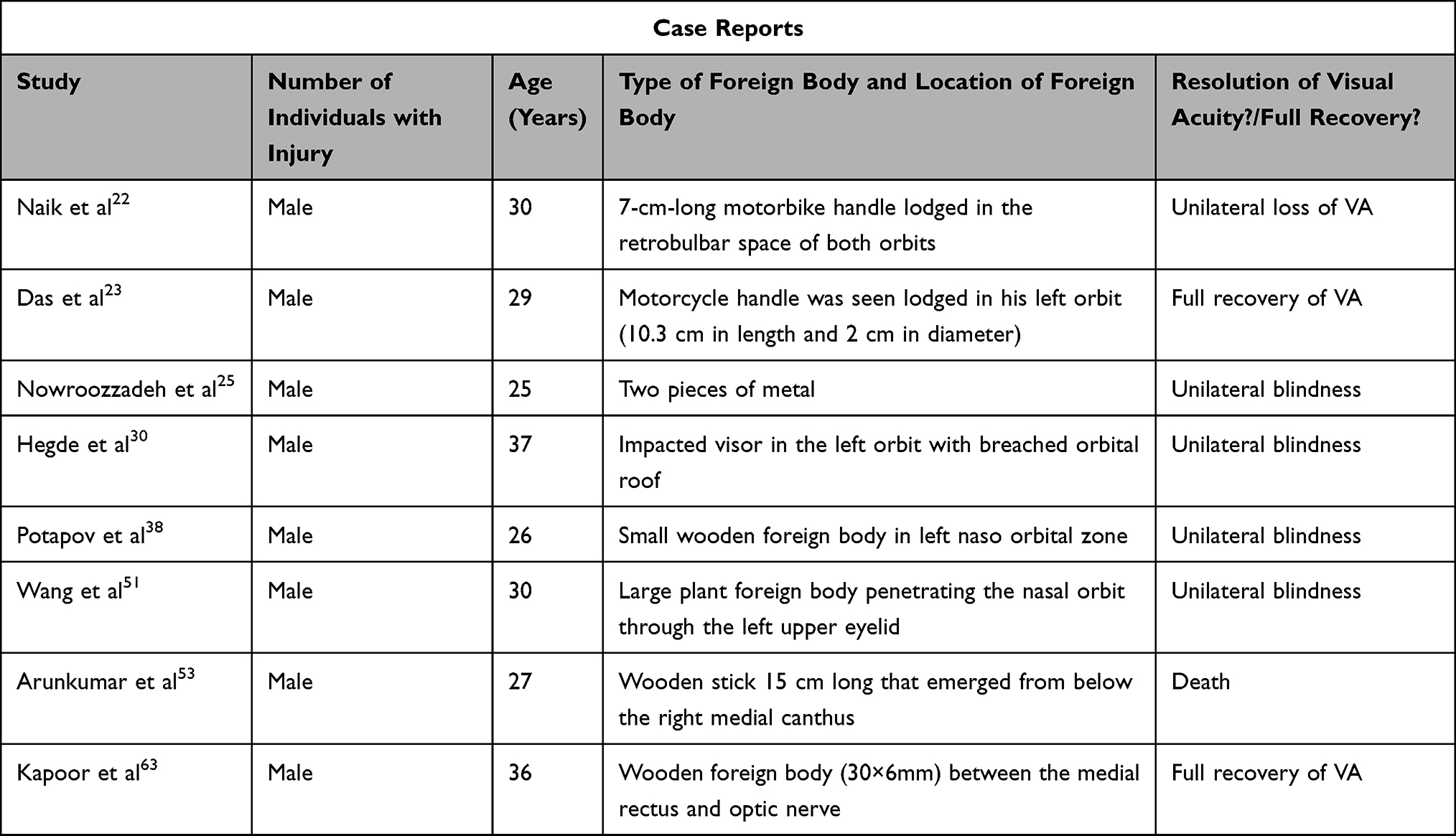 |
Table 3 Characteristics of Patients with Motorcycle-Associated Foreign Body Injuries |
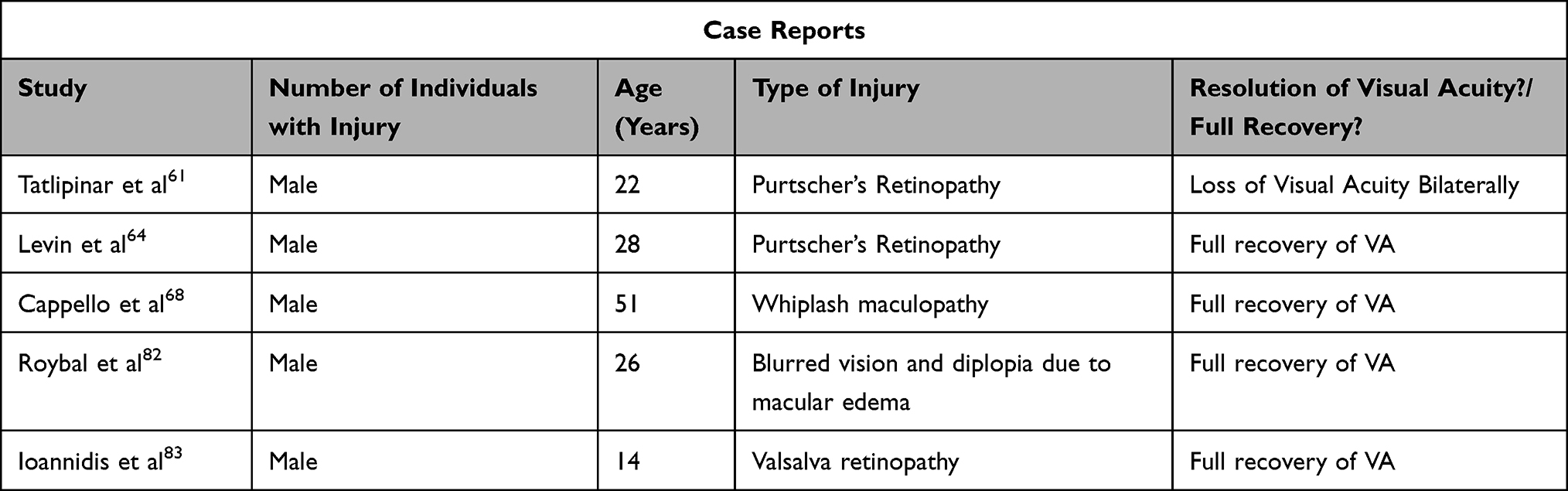 |
Table 4 Characteristics of Patients with Motorcycle-Associated Vitreoretinal Trauma |
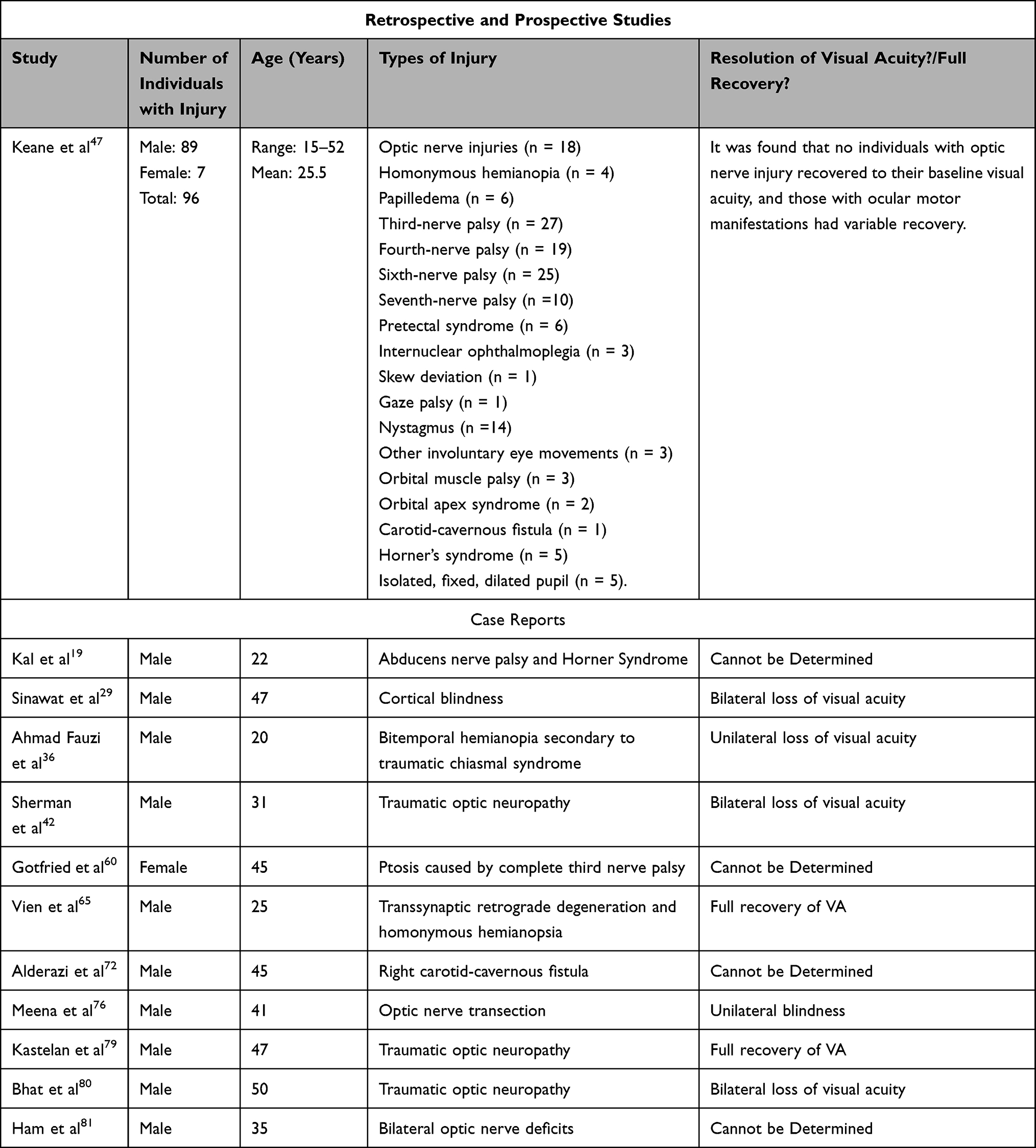 |
Table 5 Characteristics of Patients with Motorcycle-Associated Neuro-Ophthalmic Trauma |
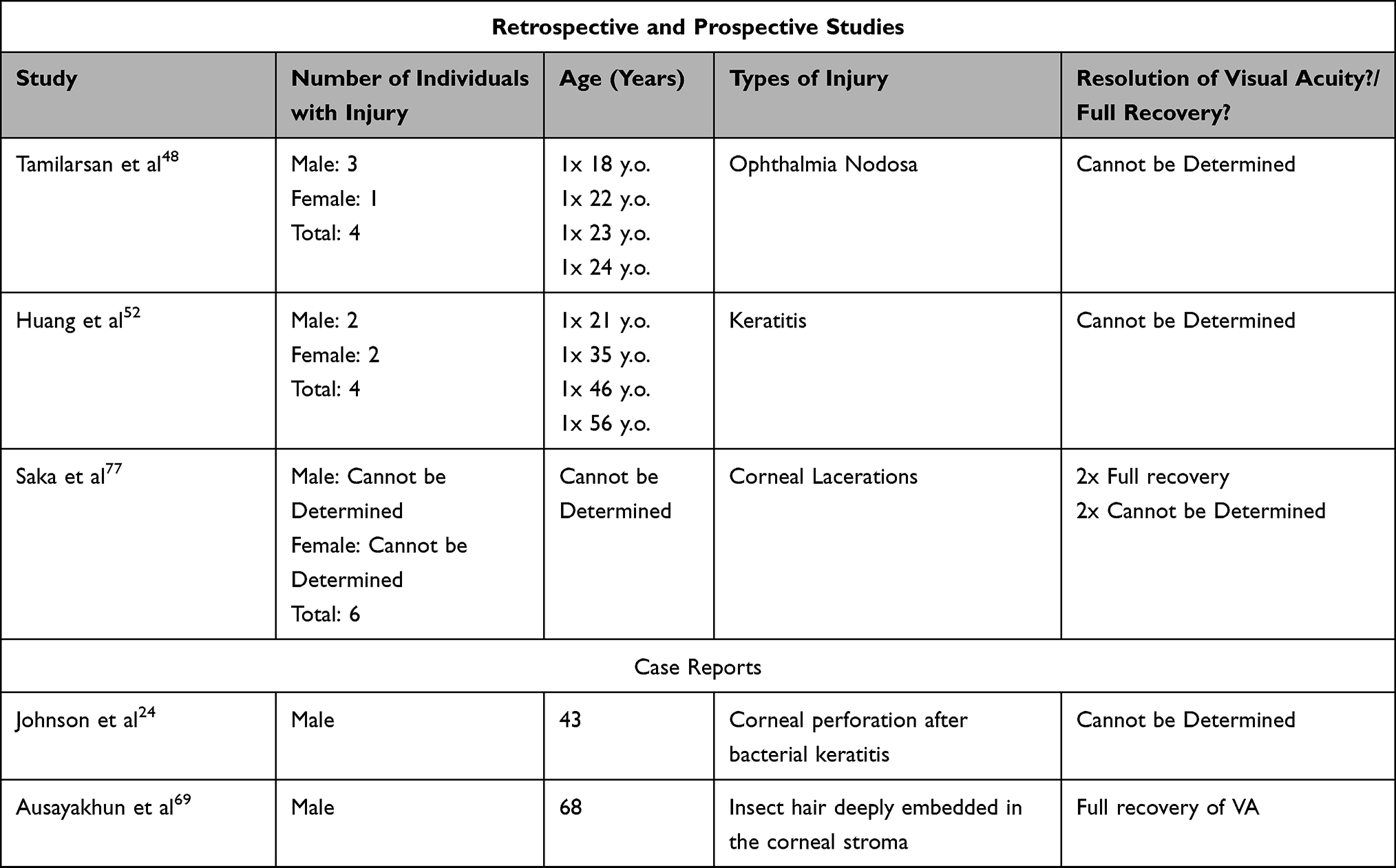 |
Table 6 Characteristics of Patients with Motorcycle-Associated Corneal Trauma |
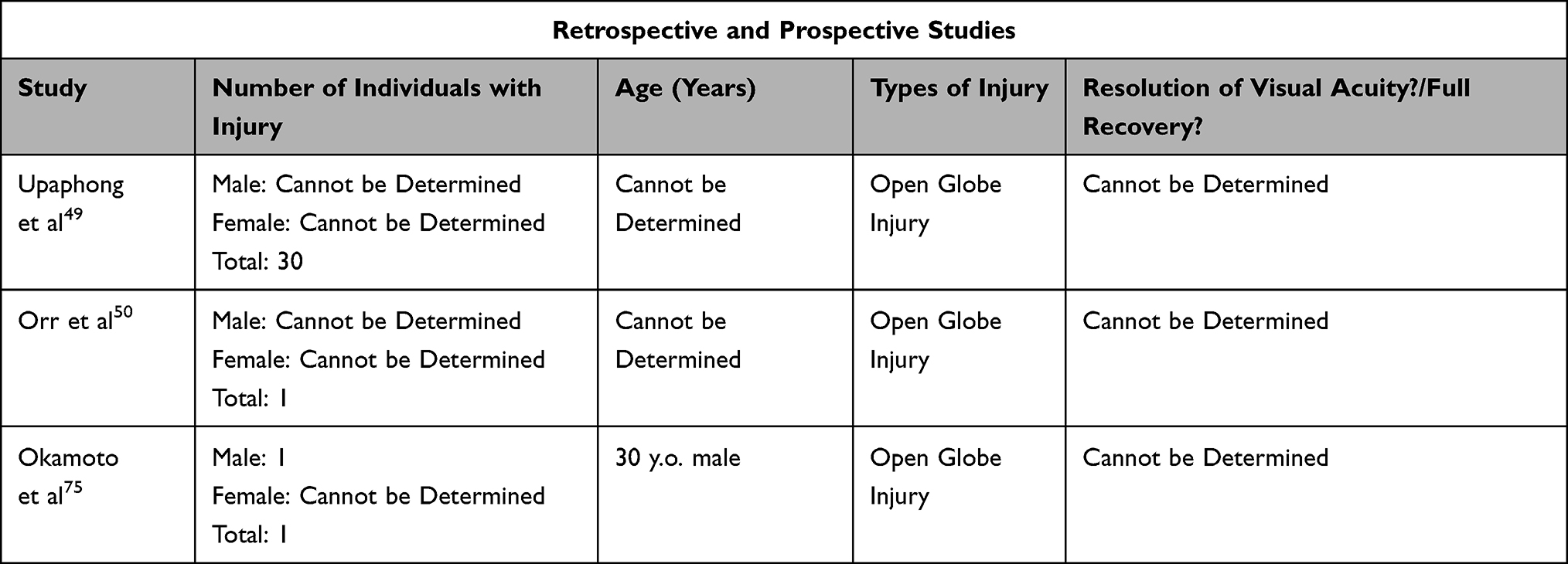 |
Table 7 Characteristics of Patients with Motorcycle-Associated Open Globe Injuries |
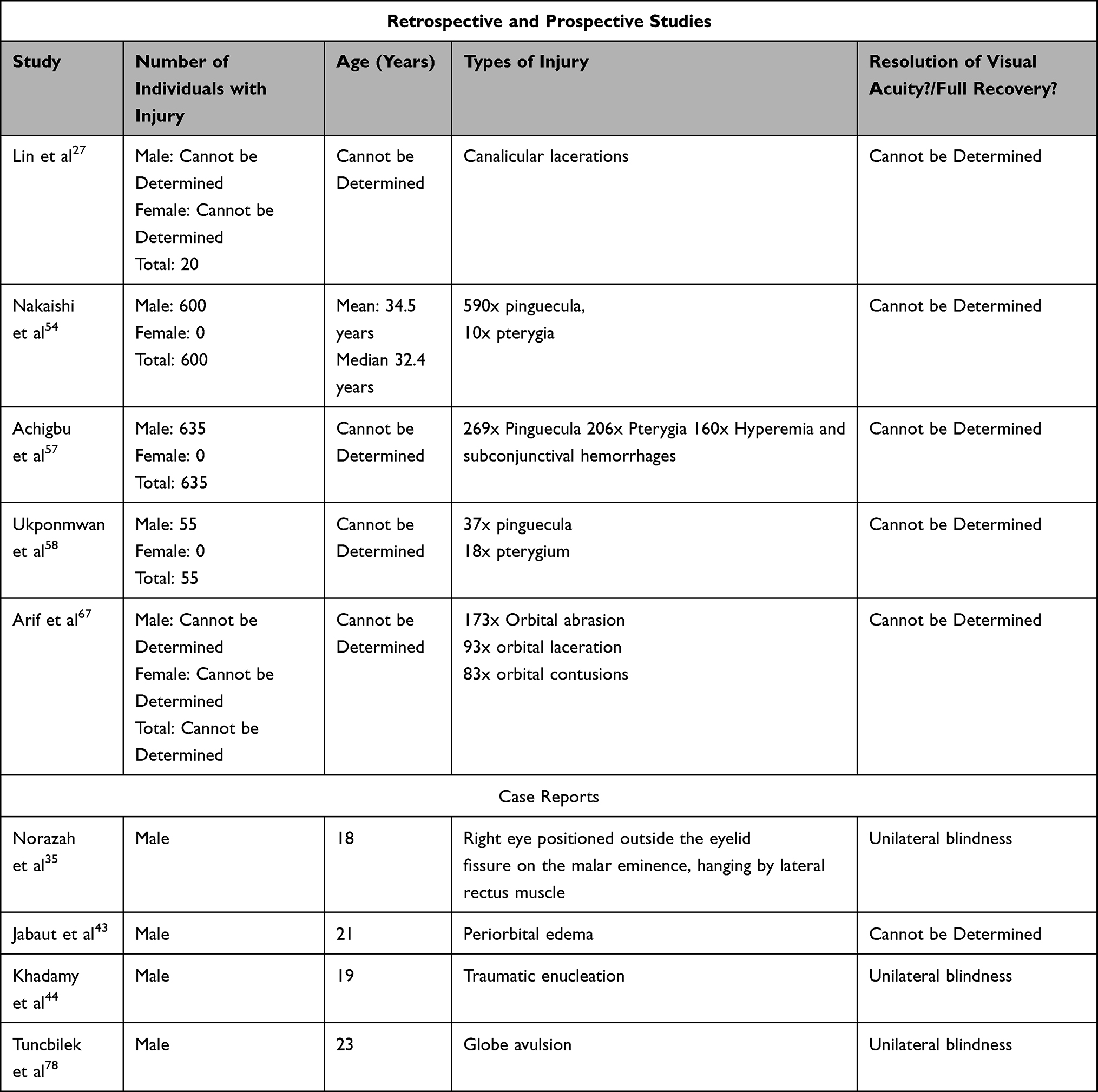 |
Table 8 Characteristics of Patients with Other Types of Motorcycle-Associated Eye Injuries |
Orbital Fractures
A total of 23 studies described orbital fractures secondary to motorcycle accidents. Ten studies were case reports, 11 were retrospective case series, and two were prospective studies (Table 1).20,21,26,28,31–34,37,39–41,45,46,55,56,59,62,66,70,71,73,74 Overall, the findings of these studies provided detailed information regarding the types and sequelae of orbital fractures and the characteristics of those who developed motorcycle-accident associated orbital fractures (Table 2).
One study found that significantly more males were involved in motorcycle crashes and subsequently developed orbital fractures than females.66 Another study found that orbital fractures associated with motorcycle accidents were more common in adults than in the elderly.46 Analyzing these studies in aggregate, we found that motorcycle accidents can lead to the following types of orbital fractures: orbital roof, orbital floor, blow-out fractures, tripod fractures, orbito-zygomatic fractures, naso-orbito fractures, maxilla-orbital fractures, and complex naso-orbito-ethmoid fractures.21,41,45,66,71 In addition, several studies noted that at a given center, the most common etiology for orbital fractures and facial fractures involving the orbit was motorcycle accidents.66,74 For example, Ellis et al found that at a single center, motorcycle accidents not only commonly caused zygomatico-orbital fracture, but were the most frequent cause of bilateral orbital fractures and were associated with more major trauma than any other etiology.21 Studies also found that the presence of orbital fractures can be a strong indicator for other injuries or clinical outcomes such as neurological deficits. For example, Kraus et al found that the presence of orbital fracture in the setting of motorcycle accidents was a strong predictor of traumatic brain injury, while Yu et al found that certain types of orbital fractures were a predictor of a poor Glasgow Coma Score.34,71 Christian et al also found that motorcyclists who did not wear helmets were at higher risk of orbital fractures, and Johnson et al surprisingly found that wearing eye protection (ie motorcycle goggles) without a helmet may increase the risk of periorbital injury31,73 (Table 2).
Orbital fractures due to motorcycle accidents can potentially lead to other sequelae. For example, orbital fractures and their associated mechanical trauma can lead to enophthalmos, central retinal vein occlusions, retrobulbar hematomas, pneumatization of the intraorbital optic nerve, globe prolapse, and Brown’s syndrome after entrapment of the superior oblique muscle.20,26,33,37,40,55 There were also reports of complications following motorcycle-associated orbital fracture repair, such as infection and pneumo-orbital cysts39,56 (Table 2).
Foreign Body Injuries
Our literature search yielded eight articles describing foreign body injuries secondary to motorcycle accidents.22,23,25,30,38,51,53,63 All eight articles were case reports. All eight cases of foreign body injuries involved adult males between the ages of 25–40 years old. Two cases involved a motorcycle handle being lodged in the orbit.22,23 Three cases involved wooden objects penetrating the orbit, while the remaining cases involved a large plant, motorcycle visor, and metal objects.25,30,38,51,53,63 Five (62.5%) of these foreign body cases resulted in permanent loss of visual acuity or unilateral blindness due to irreversible injury to the optic nerve22,25,30,38,51 (Table 3).
Vitreoretinal Injury
Similar to knowledge regarding motorcycle-associated foreign body injuries, current knowledge of motorcycle-associated vitreoretinal trauma is limited to case reports (n = 5).61,64,68,82,83 Only one case of vitreoretinal damage did not involve an adult.83 In fact, this case involved a 14-year-old who developed Valsalva retinopathy while riding a motorcycle and attempting to perform stunts, ultimately achieving a full recovery after rest and avoiding strenuous activity.83 Two of these vitreoretinal cases described the development of Purtscher’s Retinopathy after severe head trauma from a motorcycle accident, one case resulting in permanent loss of visual acuity bilaterally while the other fully recovered.61,64 Another case involved a 51-year-old who developed a whiplash maculopathy after being involved in a crash, later achieving a full recovery after one year.68 The final case described a 26-year-old who developed retinopathy and macular edema secondary to a carotid-cavernous fistula caused by head trauma during a motorcycle accident but eventually recovered fully82 (Table 4).
Neuro-Ophthalmic Manifestations
A total of 12 studies were identified that described neuro-ophthalmic manifestations secondary to motorcycle accidents.19,29,36,42,47,60,65,72,76,79–81 Only one of these 12 studies was not a case report and described the neuro-ophthalmic complications associated with motorcycle and moped accidents observed in two centers over an 18-year period.47 This study described 94 motorcycle-associated neuro-ophthalmic injuries and 2 moped-associated neuro-ophthalmic injuries. Of these patients, 89 were operators and 7 were passengers, and all 96 patients also had associated head injuries.47 In addition, almost all of these patients were male (89/96), and only four (4/96, 4.2%) were confirmed to be wearing helmets.47 Neuro-ophthalmic injuries included optic nerve injuries (n = 18), homonymous hemianopia (n = 4), papilledema (n = 6), third-nerve palsy (n = 27), fourth-nerve palsy (n = 19), sixth-nerve palsy (n = 25), seventh-nerve palsy (n =10), pretectal syndrome (n = 6), internuclear ophthalmoplegia (n = 3), skew deviation (n = 1), gaze palsy (n = 1), nystagmus (n =14), other involuntary eye movements (n = 3), orbital muscle palsy (n = 3), orbital apex syndrome (n = 2), carotid-cavernous fistula (n = 1), Horner’s syndrome (n = 5), and isolated, fixed, dilated pupil (n = 5).47 It was found that no individuals with optic nerve injury recovered to their baseline visual acuity, and those with ocular motor manifestations had variable recovery. Keane et al also described how alcohol consumption was a precipitating factor in many of these motorcycle accidents, although the exact number was unspecfied47 (Table 5).
Four of the remaining 11 case reports describing neuro-ophthalmic injuries also described the same types of injuries observed by Keane et al19,60,72,81 The other seven case reports described other neuro-ophthalmic manifestations secondary to motorcycle accidents, including bitemporal hemianopia secondary to traumatic chiasmal syndrome, permanent cortical blindness, traumatic optic neuropathy, optic nerve transection, and retrograde degeneration of retinal ganglion cells.29,36,42,65,76,79,80 All but one of these case reports involved males, and all cases of neuro-ophthalmic injury were observed in adults (Table 5).
Corneal Injuries
A total of six studies that described corneal manifestations due to motorcycle accidents were identified, two of which were case reports and the remaining three were retrospective case series.24,48,52,69,77,79 Males constituted most of the reported cases of corneal injuries. Again, across all six studies, almost all patients were adults (Table 6).
From these six studies, two retrospective case series and one case report described corneal injuries, such as ophthalmia nodosa and keratitis, that resulted from insects entering the motorcyclists’ eye.48,52,69 For example, Tamilarasan et al described how four patients presented with ocular irritation after an insect entered their eye while operating a motorcycle.48 In all four patients, the insect penetrated the cornea and the resulting insect hairs or spines caused anterior chamber reactions.48 Tamilarasan et al, in this case, emphasized the importance of eye protection in preventing injuries such as ophthalmia nodosa when operating a motorcycle. Motorcycle accidents were also shown to cause corneal lacerations.77 One study found that after a motorcycle crash significant secondary trauma and systemic infection, a patient developed bacterial keratitis and subsequently a corneal perforation24 (Table 6).
Open Globe Injuries
We identified three retrospective cases series that provided some data that showed motorcycle accidents could lead to open globe injuries.49,50,75 Unfortunately, all three studies focused on traffic accident-related open globe injuries and secondarily reported data regarding motorcycles. Therefore, there was less available data from these studies regarding motorcycle-associated open globe injuries. Due to how the aggregate data was reported in all three studies, we could not determine information regarding the stratification by age and sex from any of these studies nor could we determine any of the long-term sequelae associated with motorcycle-associated open globe injuries (Table 7).
Other
There were nine identified studies that provided data on other ocular manifestations that can occur secondary to motorcycle accidents and usage, such as pinguecula, pterygia, canalicular lacerations, orbital abrasions, subconjunctival hemorrhages, lacerations, and contusions, and globe avulsions.27,35,43,44,54,57,58,67,78 Four of these studies were case reports, two were retrospective case series, and three were prospective studies. Among the three studies that investigated the prevalence of pterygia and pinguecula among motorcyclists, the reported prevalence across studies varied widely for both pterygia (12.5 – 33.5%) and pinguecula (37.7 – 43.7%).54,57,58 Among all of these studies, nearly all patients were adult males (Table 8).
Discussion
The objectives of this study were to characterize the literature regarding motorcycle-associated eye injuries, provide an all-encompassing review of the types of motorcycle-associated ocular injuries, and classify descriptive characteristics of those most afflicted. Unfortunately, we could not discern the relative distribution of males and females in many of the non-case report studies. However, most studies that did report data regarding sex commonly found that motorcycle accidents involved males. This result is not surprising, as most motorcycle owners are males.86 It was also notable that among all ocular injuries associated with motor vehicle accidents, motorcycle accidents comprised one of the most common causes of ocular injuries, only second to car accidents.45
We also found that overall publications regarding motorcycle related-eye injuries are lacking, consisting mostly of case reports and retrospective studies that are not focused specifically on motorcycle eye injuries. In fact, out of the 65 studies that reported at least some data regarding motorcycle-associated eye injuries, 40 (61.5%) were case reports. In addition, among the 25 retrospective and prospective studies identified in our literature search, only 12 (48.0%) studies were exclusively focused on motorcycle-associated injuries and 15 (60.0%) were considered to have a low risk of bias. There is also less knowledge regarding certain types of motorcycle-associated ocular injuries. For example, motorcycle-associated foreign body injuries are limited to case reports. This review highlights existing gaps in knowledge and will hopefully encourage future studies to address these gaps.
From the results of this review, motorcycle eye injuries can at times lead to permanent loss of visual acuity and, in severe cases, blindness. However, the role of eye protection, such as helmet visors and goggles, in preventing eye injuries is poorly characterized in the medical literature. Eye protection presumably serves two functions: firstly, to reduce the risk of motorcycle accidents by preventing vision obstruction caused by foreign objects and wind; secondly, to reduce or even possibly prevent eye injuries in the event of a motorcycle accident.87 The most recent study that investigated the role of eye protection in preventing motorcycle crashes was the Hurt Report of 1981.16,17 They found that in 73% of motorcycle accidents, the operator was not wearing eye protection, likely causing wind and foreign bodies to impair vision on unprotected eyes and subsequently reduce awareness of potential surrounding hazards. According to the present study, while it is clear that there were instances in which the use of eye protection could have directly prevented eye injury (ie ophthalmia nodosa), it is unclear how many eye injuries caused by the motorcycle accident themselves could have been prevented with eye protection, as reporting concerning the use of eye protection was severely limited. It is also important to note that there were instances in which the eye protection device was the primary modality of eye injury (ie impacted visor in left orbit).30 In addition, it was notable that Johnson et al found that wearing eye protection (ie motorcycle goggles) without a helmet can surprisingly increase the risk of periorbital injury, indicating that helmet use in tandem with eye protection may be indicated.31 In fact, helmet use could also possibly attenuate or even prevent certain motorcycle-associated eye injuries, as Keane et al found that all cases of neuro-ophthalmic trauma were associated with head trauma.47 Further studies need to be conducted to better characterize the roles of eye protection in preventing crashes and eye injuries in the event of an accident. This research should include case-control studies to investigate more quantitatively the associations with protective and risk factors.
There were several limitations to this narrative review of the literature. Firstly, for many studies, we were unable to determine the nature of the motorcycle accidents (ie fall from a motorcycle, crash into another vehicle), which could play a role in the type and severity of eye injury incurred by the motorcyclist. In addition, due to inconsistent reporting, we could not ascertain whether an injured motorcyclist was wearing some form of eye protection and/or a helmet at the time of the accident for many studies, preventing us from conducting a more insightful analysis. In addition, the decision to exclude languages other than English could have led to language bias. Finally, the decision to exclude grey literature could have led to publication bias, as it is understood that published studies are more likely to report positive results.
Conclusion
The current state of the literature indicates that knowledge regarding the ocular manifestations of motorcycle accidents is limited to mostly case reports and few retrospective cohort studies focused specifically on motorcycle-associated eye injuries. However, it is evident that the types of motorcycle-associated eye injuries are legion and predominantly seen in adult males, potentially leading to severe injuries and loss of vision and blindness. Future research needs to be conducted in order to better characterize the epidemiology of certain types of motorcycle-associated eye injuries (ie foreign body injuries) and to better understand the roles of eye protection in reducing eye injuries, both through its prevention of visual interruptions that cause crashes and through the attenuation of eye injury severity in the event of an accident.
Data Sharing Statement
All data for the research reported herein is available upon reasonable request from the corresponding author (EJK).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Global status report on road safety 2018. Available from: https://www.who.int/publications-detail-redirect/9789241565684.
2. National Highway Traffic Safety Administration. Traffic safety facts, 2019: Motorcycles (Report No. DOT HS-813-112) (U.S. Department of Transportation); April, 2021.
3. Newly released estimates show traffic fatalities Reached a 16-year high in 2021 | NHTSA. Available from: https://www.nhtsa.gov/press-releases/early-estimate-2021-traffic-fatalities.
4. Sirajudeen AO, Law TH, Wong SV, Ng CP. The motorcycle deaths to passenger car deaths ratio and economic performance: a panel data analysis. Accid Anal Prev. 2022;165:106533. doi:10.1016/j.aap.2021.106533
5. Kitara DL, Ikoona EN. Poor incomes and economic hardships among commercial motorcycle drivers (boda-boda) are associated with accidents and injuries in Gulu Municipality, Northern Uganda: a cross-sectional study. Pan Afr Med J. 2022;41:274. doi:10.11604/pamj.2022.41.274.31302
6. Sayyed Hoseinian SH, Ebrahimzadeh MH, Peivandi MT, et al. Injury patterns among motorcyclist trauma patients: a cross sectional study on 4200 patients. Arch Bone Jt Surg. 2019;7(4):367–372.
7. Dischinger PC, Ryb GE, Ho SM, Braver ER. Injury patterns and severity among hospitalized motorcyclists: a comparison of younger and older riders. Annu Proc Assoc Adv Automot Med. 2006;50:237–249.
8. Kortor JN, Yinusa W, Ugbeye ME. Lower limb injuries arising from motorcycle crashes. Niger J Med. 2010;19(4):475–478. doi:10.4314/njm.v19i4.61980
9. Peek C, Braver ER, Shen H, Kraus JF. Lower extremity injuries from motorcycle crashes: a common cause of preventable injury. J Trauma. 1994;37(3):358–364. doi:10.1097/00005373-199409000-00004
10. Hasan O, Sheikh S, Fatima A, Abbas A, Zahid N, Baloch N. Motor-vehicle crash patient injury patterns from a level one trauma center in a metropolitan city: a cross-sectional study. Cureus. 2019;11(2):e4073. doi:10.7759/cureus.4073
11. Adeleye AO, Ogun MI. Clinical epidemiology of head injury from road-traffic trauma in a developing country in the current era. Front Neurol. 2017;8:695. doi:10.3389/fneur.2017.00695
12. Lam C, Wiratama BS, Chang WH, et al. Effect of motorcycle helmet types on head injuries: evidence from eight level-I trauma centres in Taiwan. BMC Public Health. 2020;20(1):78. doi:10.1186/s12889-020-8191-1
13. Thomas R, McManus JG, Johnson A, Mayer P, Wade C, Holcomb JB. Ocular injury reduction from ocular protection use in current combat operations. J Trauma. 2009;66(4 Suppl):S99–103. doi:10.1097/TA.0b013e31819d8695
14. Fong LP, Taouk Y. The role of eye protection in work-related eye injuries. Aust N Z J Ophthalmol. 1995;23(2):101–106. doi:10.1111/j.1442-9071.1995.tb00137.x
15. Whyte T, Gibson T, Eager D, Milthorpe B. Full-face motorcycle helmet protection from facial impacts: an investigation using THOR dummy impacts and SIMon finite element head model. Inj Prev. 2017;23(3):205–210. doi:10.1136/injuryprev-2015-041925
16. Hurt HH, Ouellet JV, Thom DR. Motorcycle accident cause factors and identification of countermeasures. volume 1: Technical report. University of Southern California. Traffic Safety Center; 1981. Available from: https://rosap.ntl.bts.gov/view/dot/6450.
17. Motorcycle statistics: Harry Hurt interview. Available from: https://soundrider.com/archive/safety-skills/harry_hurt_interview.aspx.
18. ROBINS-I tool | Cochrane methods. Available from: https://methods.cochrane.org/methods-cochrane/robins-i-tool.
19. Kal A, Ercan ZE, Duman E, Arpaci E. Abducens nerve palsy and ipsilateral Horner syndrome in a patient with carotid–cavernous fistula. J Craniofac Surg. 2015;26(7):e653–e655. doi:10.1097/SCS.0000000000002131
20. Baldwin L, Baker RS. Acquired Brown’s syndrome in a patient with an orbital roof fracture. J Neuroophthalmol. 1988;8(2):127–130.
21. Ellis E, El-Attar A, Moos KF. An analysis of 2067 cases of zygomatico-orbital fracture. J Oral Maxillofac Surg. 1985;43(6):417–428. doi:10.1016/S0278-2391(85)80049-5
22. Naik MN, Das S, Oluyemi F, Honavar SG. An extraordinary orbital foreign body. Ophthal Plast Reconstr Surg. 2011;27(6):e149–e152. doi:10.1097/IOP.0b013e3182078e88
23. Das D, Singh P, Modaboyina S, Bajaj MS, Agrawal S. An eye capturing clutch – an orbital foreign body. Cureus. 2021. doi:10.7759/cureus.15867
24. Johnson JL, Sagraves SG, Feild CJ, Block EF, Cheatham ML. An unusual case of corneal perforation secondary to Pseudomonas keratitis complicating a patient’s surgical/trauma intensive care unit stay. Am Surg. 2000;66(10):972–974.
25. Nowroozzadeh M. An unusual intraorbital foreign body: a brake lever. Indian J Ophthalmol. 2009;57(5):400. doi:10.4103/0301-4738.55063
26. Himori N, Kunikata H, Otomo T, Fuse N, Nishida K. Central retinal artery occlusion following severe blow-out fracture in young adult. Clin Ophthalmol. 2009;3:325–328. doi:10.2147/opth.s5343
27. Lin CH, Wang CY, Shen YC, Wei LC. Clinical characteristics, intraoperative findings, and surgical outcomes of canalicular laceration repair with monocanalicular stent in Asia. J Ophthalmol. 2019;2019:1–6. doi:10.1155/2019/5872485
28. Day KM, Phillips PM, Sargent LA. Correction of a posttraumatic orbital deformity using three-dimensional modeling, virtual surgical planning with computer-assisted design, and three-dimensional printing of custom implants. Craniomaxillofacial Trauma Reconstr. 2018;11(1):078–082. doi:10.1055/s-0037-1601432
29. Sinawat S, Ratanapakorn T, Yospaiboon Y. Cortical blindness after motorcycle accident: a case report. J Med Assoc Thai. 2006;89(3):380–383.
30. Hegde V, Appaswamy S, Ahluwalia H. Cranio-orbital injury with internal carotid artery laceration and a missing eyelid. Ophthal Plast Reconstr Surg. 2005;21(6):467–469. doi:10.1097/01.iop.0000181348.64958.da
31. Johnson RM, McCarthy MC, Miller SF, Peoples JB. Craniofacial trauma in injured motorcyclists: the impact of helmet usage. J Trauma Inj Infect Crit Care. 1995;38(6):876–878. doi:10.1097/00005373-199506000-00008
32. Gopalakrishna G, Peek-Asa C, Kraus JF. Epidemiologic features of facial injuries among motorcyclists. Ann Emerg Med. 1998;32(4):425–430. doi:10.1016/S0196-0644(98)70170-2
33. Chen HH, Pan CH, Leow AM, Tsay PK, Chen CT. Evolving concepts in the management of orbital fractures with enophthalmos: a retrospective comparative analysis. Formos J Surg. 2016;49(1):1–8. doi:10.1016/j.fjs.2015.06.002
34. Kraus JF, Rice TM, Peek-Asa C, McArthur DL. Facial trauma and the risk of intracranial injury in motorcycle riders. Ann Emerg Med. 2003;41(1):18–26. doi:10.1067/mem.2003.1
35. Norazah AR, Akmal HZ, Hashima H, Vasantha T, Samsudin A. Globe avulsion secondary to maxillofacial trauma. Med J Malaysia. 2011;66(4):359–360.
36. Ahmad Fauzi S, Nor Sharina Y, Ibrahim M. Isolated traumatic bitemporal hemianopia. Cureus. 2021. doi:10.7759/cureus.17593
37. Zhang-Nunes SX, Jarullazada I, Mancini R. Late central visual recovery after traumatic globe displacement into the maxillary sinus. Ophthal Plast Reconstr Surg. 2012;28(1):e17–e19. doi:10.1097/IOP.0b013e318213f5fb
38. Potapov AA, Eropkin SV, Kornienko VN, et al. Late diagnosis and removal of a large wooden foreign body in the cranio-orbital region. J Craniofac Surg. 1996;7(4):311–314. doi:10.1097/00001665-199607000-00012
39. Ueki S, Rikimaru H, Rikimaru-Nishi Y, Midorikawa M, Kiyokawa K. Late-onset infection of resorbable plates after multiple facial fractures. J Craniofac Surg. 2020;31(3):e280–e282. doi:10.1097/SCS.0000000000006271
40. Chen YA, Singhal D, Chen YR, Chen CT. Management of acute traumatic retrobulbar haematomas: a 10-year retrospective review. J Plast Reconstr Aesthet Surg. 2012;65(10):1325–1330. doi:10.1016/j.bjps.2012.04.037
41. Haug RH. Management of the trochlea of the superior oblique muscle in the repair of orbital roof trauma. J Oral Maxillofac Surg. 2000;58(6):602–606. doi:10.1016/S0278-2391(00)90148-4
42. Sherman AL, Cardenas DD, Swedberg S. Management of traumatic optic neuropathy with coexistent spinal cord injury: a case report. Arch Phys Med Rehabil. 1997;78(9):1012–1014. doi:10.1016/S0003-9993(97)90068-X
43. Jabaut JM, Kotora J, Ambrosio A. Mandibular degloving: a case report and literature review. J Emerg Med. 2017;53(2):262–264. doi:10.1016/j.jemermed.2017.03.022
44. Khadamy J, Khademi P, Kashkouli M. Missing globe: a case of severe head trauma, eyelid laceration, and traumatic enucleation. Cureus. 2017. doi:10.7759/cureus.1988
45. Ruslin M, Brucoli M, Boffano P, et al. Motor vehicle accidents–related maxillofacial injuries: a multicentre and prospective study. Oral Surg Oral Med Oral Pathol Oral Radiol. 2019;128(3):199–204. doi:10.1016/j.oooo.2018.12.009
46. Hsieh CH, Liu HT, Hsu SY, Hsieh HY, Chen YC. Motorcycle-related hospitalizations of the elderly. Biomed J. 2017;40(2):121–128. doi:10.1016/j.bj.2016.10.006
47. Keane JR. Neurologic eye signs following motorcycle accidents. Arch Neurol. 1989;46(7):761–762. doi:10.1001/archneur.1989.00520430055017
48. Tamilarsan SS, Jaafar J, Chew-Ean T, Masnon NA, Wan Hitam WH. Ocular injuries due to insect spines (ophthalmia nodosa): potential hazard to motorcyclists. Cureus. 2022. doi:10.7759/cureus.23084
49. Upaphong P, Supreeyathitikul P, Choovuthayakorn J. Open globe injuries related to traffic accidents: a retrospective study. J Ophthalmol. 2021;2021:1–5. doi:10.1155/2021/6629589
50. Orr CK, Bauza A, Langer PD, Zarbin MA, Bhagat N. Open-globe injuries with motor vehicle accidents: a 12-year review. Graefes Arch Clin Exp Ophthalmol. 2015;253(8):1313–1317. doi:10.1007/s00417-015-2929-y
51. Wang X, Xie Q, Wang X, Chen H, Sheng X. Orbital trauma with a large plant foreign body: a case report. Eye Sci. 2013;28(1):44–47.
52. Huang FC, Chen WJ, Shih MH. Paederus-Induced keratitis. Cornea. 2010;29(8):941–943. doi:10.1097/ICO.0b013e3181ca2ec0
53. Arunkumar MJ, Selvapandian S, Rajshekhar V. Penetrating intracranial wooden object: case report and review of CT morphology, complications, and management. Surg Neurol. 1999;51(6):617–620. doi:10.1016/S0090-3019(99)00029-4
54. Nakaishi H, Yamamoto M, Ishida M, Someya I, Yamada Y. Pingueculae and pterygia in motorcycle policemen. Ind Health. 1997;35(3):325–329. doi:10.2486/indhealth.35.325
55. Agarwal SA, Maloof AJ, Gomes LJ. Pneumatization of the intraorbital optic nerve after severe head trauma. Ophthal Plast Reconstr Surg. 2002;18(6):469–471. doi:10.1097/00002341-200211000-00017
56. Neves RB, Yeatts RP, Martin TJ. Pneumo-orbital cyst after orbital fracture repair. Am J Ophthalmol. 1998;125(6):879–880. doi:10.1016/S0002-9394(98)00050-6
57. Achigbu E, Ezepue U. Prevalence and severity of pterygium among commercial motorcycle riders in south eastern Nigeria. Ghana Med J. 2014;48(3):153. doi:10.4314/gmj.v48i3.6
58. Ukponmwan CU, Dawoda OA, Edema OF, Okojie O. Prevalence of pterygium and pingueculum among motorcyclists in Nigeria. East Afr Med J. 2008;84(11):516–521. doi:10.4314/eamj.v84i11.9570
59. Do Ó Silva AL, Dias IJ, Grempel RG, de Morais HHA, da Silva Oliveira NM, de Castro Gomes DQ. Prototyping for the treatment of late zygomatic-orbital fracture: a case report. Int J Surg Case Rep. 2017;38:91–94. doi:10.1016/j.ijscr.2017.06.065
60. Gotfried R. Ptosis after motorcycle accident. J Fam Pract. 2021;70:4. doi:10.12788/jfp.0192
61. Tatlipinar S, Toprak İ, Yaylali V, Yildirim C, Keskin N, Özden S. Purtscher’s retinopathy: a case report. Neuro-Ophthalmol. 2007;31(3):83–85. doi:10.1080/01658100701436199
62. Pessoa Neto JV, Cetira Filho EL, Sampaio FD, Mello de MJR, Menezes Junior JMS. Removal of foreign bodies in orbit-zygomatic-maxillary complex. J Craniofac Surg. 2019;30(7):e598–e600. doi:10.1097/SCS.0000000000005604
63. Kapoor AG, Vijitha VS, Fernandes M. Retained intraorbital wooden foreign body presenting with combined anterior and posterior scleritis. BMJ Case Rep. 2020;13(2):e232237. doi:10.1136/bcr-2019-232237
64. Levin LA, Seddon JM, Topping T. Retinal pigment epithelial tears associated with trauma. Am J Ophthalmol. 1991;112(4):396–400. doi:10.1016/S0002-9394(14)76246-4
65. Vien L, DalPorto C, Yang D. Retrograde degeneration of retinal ganglion cells secondary to head trauma. Optom Vis Sci. 2017;94(1):125–134. doi:10.1097/OPX.0000000000000899
66. Calderoni DR, Guidi de MC, Kharmandayan P, Nunes PHF. Seven-year institutional experience in the surgical treatment of orbito-zygomatic fractures. J Cranio-Maxillofac Surg. 2011;39(8):593–599. doi:10.1016/j.jcms.2010.11.018
67. MdZ Arif, Rajanikanth BR, Prasad K. Soft tissue injuries of the maxillofacial region occurring from motorcycle accidents. J Maxillofac Oral Surg. 2019;18(3):432–439. doi:10.1007/s12663-018-1149-5
68. Cappello E, Della Guardia C, Cecchin E, Morselli S. Spectral domain optical coherence tomography findings in a case of whiplash maculopathy with incomplete resolution. Retin Cases Brief Rep. 2021;15(4):421–425. doi:10.1097/ICB.0000000000000805
69. Ausayakhun S, Pathanapitoon K, Siriwanasan R, Watananikorn S. Spontaneous resorption of an insect hair in the corneal stroma: a case report. J Med Assoc Thai. 2005;88(3):423–425.
70. RafaelMA P, Barbosa O, Basílio AP, Santana AS, De Paula D, Marangon JH. Surgical decompression of the orbit due to frontal bone and roof of the orbit fractures - A case report. Ann Maxillofac Surg. 2020;10(2):495. doi:10.4103/ams.ams_87_20
71. Yu DY, Chen CH, Tsay PK, Leow AM, Pan CH, Chen CT. Surgical timing and fracture type on the outcome of diplopia after orbital fracture repair. Ann Plast Surg. 2016;76(Supplement 1):S91–S95. doi:10.1097/SAP.0000000000000726
72. Alderazi YJ, Dharmadhikari S, Haussen DC, Yavagal DR. Teaching NeuroImages: reversible pontomesencephalic edema caused by traumatic carotid cavernous fistula. Neurology. 2014;83(2):e18–e18. doi:10.1212/WNL.0000000000000562
73. Christian JM, Thomas RF, Scarbecz M. The incidence and pattern of maxillofacial injuries in helmeted versus non-helmeted motorcycle accident patients. J Oral Maxillofac Surg. 2014;72(12):2503–2506. doi:10.1016/j.joms.2014.07.015
74. Manana W, Odhiambo WA, Chindia ML, Koech K. The pattern of orbital fractures managed at two referral centers in Nairobi, Kenya. J Craniofac Surg. 2017;28(4):e338–e342. doi:10.1097/SCS.0000000000003579
75. Okamoto Y, Morikawa S, Okamoto F, et al. Traffic accident–related open globe injuries. Retina. 2019;39(4):779–785. doi:10.1097/IAE.0000000000002012
76. Meena S, Rakheja V, Sahu S, Rathore P. Traumatic avulsion of the globe with optic nerve transection: an unusual presentation. BMJ Case Rep. 2020;13(10):e233148. doi:10.1136/bcr-2019-233148
77. Saka ES, Monsudi KF, Olatuji V. Traumatic corneal laceration in northwestern Nigeria. J West Afr Coll Surg. 2017;7(4):72–84.
78. Tunçbilek G, Traumatic IE. Evulsion of the globe: a very rare complication of maxillofacial trauma. J Craniofac Surg. 2008;19(2):313–315. doi:10.1097/SCS.0b013e318163e2db
79. Kaštelan S. Traumatic optic neuropathy – case report with discussion on diagnostic procedures and therapy. Acta Clin Croat. 2018;57(1):166–172. doi:10.20471/acc.2018.57.01.22
80. Bhat PM. Traumatic Optic Neuropathy (TON) and Ayurveda - A case report. J Ayurveda Integr Med. 2022;13(1):100494. doi:10.1016/j.jaim.2021.07.010
81. Ham PB, Cunningham AJ, Mentzer CJ, Ahmad A, Young LS, Abuzeid AM. Traumatic panhypopituitarism resulting in acute adrenal crisis. J Trauma Acute Care Surg. 2015;79(3):484–489. doi:10.1097/TA.0000000000000771
82. Roybal CN, Kucukevcilioglu M, Huckfeldt R, Elshatory Y, Thurtell MJ, Folk JC. Treatment of retinopathy and macular edema secondary to a carotid-cavernous fistula. Retin Cases Brief Rep. 2016;10(3):225–228. doi:10.1097/ICB.0000000000000234
83. Ioannidis AS, Tranos PG, Harris M. Valsalva retinopathy associated with riding a motorcycle. Eye. 2004;18(3):329–331. doi:10.1038/sj.eye.6700658
84. Scariot R, Oliveira de IA, Passeri LA, Rebellato NLB, Müller PR. Maxillofacial injuries in a group of Brazilian subjects under 18 years of age. J Appl Oral Sci. 2009;17(3):195–198. doi:10.1590/S1678-77572009000300012
85. Zhou HH, Ongodia D, Liu Q, Yang RT, Li ZB. Incidence and pattern of maxillofacial fractures in children and adolescents: a 10 years retrospective cohort study. Int J Pediatr Otorhinolaryngol. 2013;77(4):494–498. doi:10.1016/j.ijporl.2012.12.017
86. Motorcycle trends in the United States | Bureau of Transportation Statistics. Available from: https://www.bts.gov/archive/publications/special_reports_and_issue_briefs/special_report/2009_05_14/entire.
87. National agenda for motorcycle safety. Available from: https://one.nhtsa.gov/people/injury/pedbimot/motorcycle/00-nht-212-motorcycle/human27-29.html.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Orbital Fractures and Risk Factors for Ocular Injury
Zhong E, Chou TY, Chaleff AJ, Scofield-Kaplan SM, Perzia BM, Naqvi J, Hou W
Clinical Ophthalmology 2022, 16:4153-4161
Published Date: 14 December 2022