Back to Journals » Neuropsychiatric Disease and Treatment » Volume 10
Motivation for treatment in patients with substance use disorder: personal volunteering versus legal/familial enforcement
Authors Bilici R, Yazici E, Tufan AE ![]() , Mutlu E, İzci F, Uğurlu GK
, Mutlu E, İzci F, Uğurlu GK
Received 25 April 2014
Accepted for publication 9 June 2014
Published 30 August 2014 Volume 2014:10 Pages 1599—1604
DOI https://doi.org/10.2147/NDT.S66828
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Rabia Bilici,1 Esra Yazici,2 Ali Evren Tufan,3 Elif Mutlu,4 Filiz İzci,1 Görkem Karakas Ugurlu5
1Erenkoy Mental Health and Neurology Training and Research Hospital, Department of Psychiatry, Istanbul; 2Sakarya University, Medical Faculty, Department of Psychiatry, Sakarya, 3Abant Izzet Baysal University, Medical Faculty, Department of Child and Adolescent Psychiatry, Bolu, 4Bakirköy Mental Health and Neurology Training and Research Hospital, Department of Psychiatry, Istanbul, 5Yildirim Beyazit University, Medical Faculty, Department of Psychiatry, Ankara, Turkey
Background: Motivation for treatment on the part of patients with addictive disorders is known to affect their prognosis, and lack thereof is reported to be among the most common reasons for failed treatment adherence and relapse after treatment. This study evaluated the relationship between volunteering, personality, demographic factors, and motivation for treatment.
Methods: The study was conducted at a substance dependence center in the eastern part of Turkey. Forty-five patients (mean age 37.9±11.2 years) with a substance use disorder were included. They were assessed using the Structured Clinical Interview for DSM (Diagnostic and Statistical Manual of Mental Disorders) Axis II disorders. Depression and anxiety were evaluated using the Beck depression and anxiety inventories, and motivation for treatment was measured using the Turkish version of the Texas Christian University Motivation for Treatment scale.
Results: All patients had been using substances daily and 41 (88.9%) had been using multiple drugs. The most commonly used substance was heroin (n=18, 40%). Voluntary admission was a predictor of motivation for treatment (P<0.05). Having a personality disorder and higher depression scores were related to less motivation for treatment.
Conclusion: Motivation for treatment is affected by external factors such as type of admission and internal factors such as personality disorder and depression. Investigation of ways to encourage voluntary admission for treatment instead of enforced strategies may be helpful for achieving higher levels of motivation for treatment in substance users.
Keywords: substance use, motivation, treatment, voluntary, personality, depression
Introduction
Motivation to change can be defined as an internal psychological state consisting of acceptance of and readiness for change. It can be affected by both internal and external factors.1 In the context of addictive disorders, those factors include internal as well as external pressures, readiness to receive treatment, and the patient’s perception of the treatment program, ie, lax or harsh, available support, and modes of therapy.2 Motivation for treatment on the part of patients with addictive disorders is known to affect their prognosis and is reported to be among the most common reasons for failed treatment adherence and relapse after treatment.3–5 Accordingly, motivation for and readiness to accept change and treatment have received much interest lately in addiction research.6
In recent years, the perception of substance use as a criminal issue has been changing to that of a health issue in Turkey, although the number of patients who are forced legally to undergo treatment for substance addiction has been increasing dramatically.7 It is known that motivation for treatment of addictive disorders among Turkish patients has received scant attention up until now.7 This paper presents an evaluation of motivation for involuntary versus voluntary treatment in patients predominantly from the south–eastern and eastern areas of Turkey. The aim of the study was to evaluate patients’ motivation, sociodemographic and clinical correlates, personality disorders, and anxiety and depression scores, all of which are thought to be related to motivation for treatment.
Materials and methods
Study center
The study was conducted in the Treatment Center for Alcohol and Substance Use Disorders at the Elazig Hospital for Mental Disorders. This treatment center has a capacity of ten beds and is for male patients only. Female patients are treated at other centers.
Sampling
Patients who applied or were referred to the Elazig Hospital for Mental Disorders for treatment of substance addiction were included in this study. Forty-five patients, diagnosed with substance dependence according to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision, who gave written informed consent and did not have severe comorbid psychopathology (ie, psychotic or organic brain disorder) were enrolled in the study.8 All inpatients approached agreed to participate in the study. The patients were evaluated according to the terms of their admission to hospital. Those who were admitted of their own free will comprised the voluntary group (n=26) and those who were admitted to hospital routinely as part of a legal follow-up program or at the insistence of their family comprised the enforced group (n=19). The duration of detoxification for different substances was taken into consideration and patients were re-evaluated after at least 2 weeks of treatment to clarify their diagnosis and for collection of sociodemographic and clinical data. The study protocol was carried out in accordance with the Declaration of Helsinki and local laws and regulations.9
Psychometric tests
Depression and anxiety were evaluated using the Beck depression and anxiety inventories, and motivation for treatment was measured using the Turkish version of the Texas Christian University (TCU) Motivation for Treatment (MfT) scale.
Beck Depression Inventory
The Beck Depression Inventory measures somatic, emotional, cognitive, and motivational symptoms of depression. This scale is used to assess the severity of depressive symptoms objectively rather than diagnosing depression per se. The scale consists of 21 questions, each with four choices that are graded between 0 and 3. The total sum of the questions is thought to correlate with the severity of depression. The reliability and validity of the Turkish version of this scale has been confirmed previously.10,11 The cut-off score for Turkish psychiatric outpatients was found to be 17.11
Beck Anxiety Inventory
The Beck Anxiety Inventory is a self-report instrument evaluating the frequency of anxiety symptoms experienced. It is a Likert-type scale consisting of 21 symptoms each graded from 0 to 3. The total score is thought to correlate with the severity of anxiety. The Turkish version has previously been found to be reliable and valid.12,13
Texas Christian University Motivation for Treatment scale
The TCU MfT scale was developed by Simpson and Joe,14 and the reliability and validity of the Turkish version was reported by Evren et al.7 It is a 24-item self-rating scale containing three subscales for problem recognition, desire for help, and treatment readiness. According to the study by Evren et al the Turkish version of the MfT can be used as a reliable and valid tool for measuring motivation in patients who are alcohol-dependent or drug-dependent.
Structured Clinical Interview for DSM-III-R Axis II disorders
The Structured Clinical Interview for DSM-III-R (Diagnostic and Statistical Manual of Mental Disorders Third Edition, Revised) Axis II disorders (SCID-II) is used to evaluate personality disorders.15 The interview was translated into the Turkish language in 1989, and the reliability and validity studies were reported by Sorias et al.16 After completion of this form, a semistructured interview was conducted. The final diagnoses were reached by a consensus of two psychiatrists, a child and adolescent psychiatrist, and two clinical psychologists on the basis of the SCID-II and the semistructured interview.
Statistical analysis
The data were entered into a database using Statistical Package for the Social Sciences version 15.0 software (SPSS Inc, Chicago, IL, USA). Descriptive analyses, including the chi-squared test, the independent samples t-test, and the Mann–Whitney U-test, were used. Fisher’s combined probability test was used when necessary. Linear regression analysis was conducted to determine predictors. All of the comparisons were two-tailed and the P-value was set at 0.05.
Results
Sociodemographic data
Forty-five male patients of mean age 37.9±11.2 years were enrolled in the study. Their mothers were all housewives and their fathers were mostly workers (n=17, 37.8%) or clerks (n=12, 26.7%). Most were married (n=35, 57.8%) and had children (n=32, 71.1%). Most lived with their spouse and children (n=26, 57.8%). Only 15 of the patients reported being able to work regularly (33.3%). Most of the patients came from Elazig county in Turkey (n=21, 46.7%), with the others coming from diverse backgrounds (eleven counties, nine from the eastern/south–eastern areas of the country).
Conscription status typically reflects the soundness of physical and mental health of males in traditional Turkish society,17 so this was also assessed. Most patients had completed their mandatory service without problems (n=39, 86.7%), but two had served longer terms due to psychiatric issues (4.4%). Four of the patients (8.9%) had not yet served at the time of the study. When questioning was broadened to include disciplinary problems, eight patients reported that they had been incarcerated in military prisons during their service for various petty offenses (17.8%).
Substance use
All of the patients had been using substances daily at the time of the study. Forty-one (88.9%) had been using multiple drugs, and five reported using only one type of drug (11.1%). The most commonly used substance was heroin. Most had made prior attempts to stop using substances (n=37, 82.2%) and most had applied voluntarily for treatment (n=26, 57.8%). The general profile of the participants is shown in Table 1.
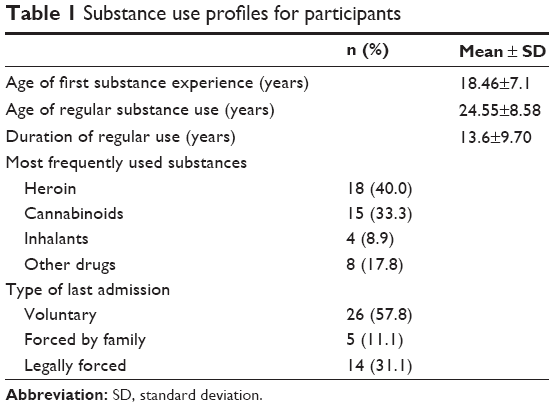 | Table 1 Substance use profiles for participants |
Factors related to motivation for treatment
Sociodemographic data
Age, education level, age at first substance use, and total duration of substance use showed no correlation with MfT (P>0.05). Family history of psychopathology and substance use, as well as prior attempts at treatment, had no effect on MfT or its subscales (P>0.05). The presence of social support (defined as living with family, being married, having a regular job) also had no effect (P>0.05).
Volunteering
The mean motivation score on the MfT was 67.4±11.4 for the whole study sample, and mean scores for the subscales of problem recognition, desire for help, and readiness for treatment were 29.3±5.8, 21.3±4.0, and 16.8±5.5, respectively.
The patients were divided into two groups according to whether they were admitted to hospital for treatment voluntarily (n=26) or involuntarily (n=19). The Student’s t-test was used to compare the two groups, and no statistically significant difference was found with regard to age or education level.
Motivation was compared between those who were being treated voluntarily and those who were forced to undergo treatment using the independent samples t-test. Total scores on the MfT (72.46±7.83 for the voluntary group and 60.47±12.02 for the involuntary group) and its subscales of desire for help (22.65±3.68 and 19.47±3.61, respectively) and treatment readiness (18.88±5.03 and 14.00±4.91) differed between the groups (P<0.05). Total scores on the MfT and its subscales are shown for both groups in Figure 1.
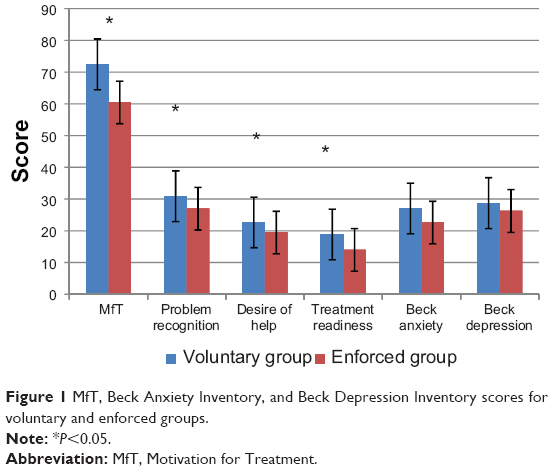 | Figure 1 MfT, Beck Anxiety Inventory, and Beck Depression Inventory scores for voluntary and enforced groups. |
Personality
Twenty-eight of the patients (62.2%) received an Axis II diagnosis on the basis of the SCID-II, semistructured interview, and clinician consensus. The most common Axis II diagnosis was antisocial personality disorder (n=13, 28.9%), followed by borderline personality disorder (n=9, 20.0%). Patients were categorized into two groups according to whether they were personality disorder positive (n=22) or personality disorder negative (n=23). The independent samples t-test was used to compare the groups. There was no significant difference between the groups for age and education level (P>0.05). Mean total MfT scores (64.78±12.38 for the group with personality disorder and 71.70±8.18 for the group without personality disorder) and treatment readiness scores (15.07±5.68 and 19.70±3.80, respectively) were higher in the group with personality disorder (Figure 2).
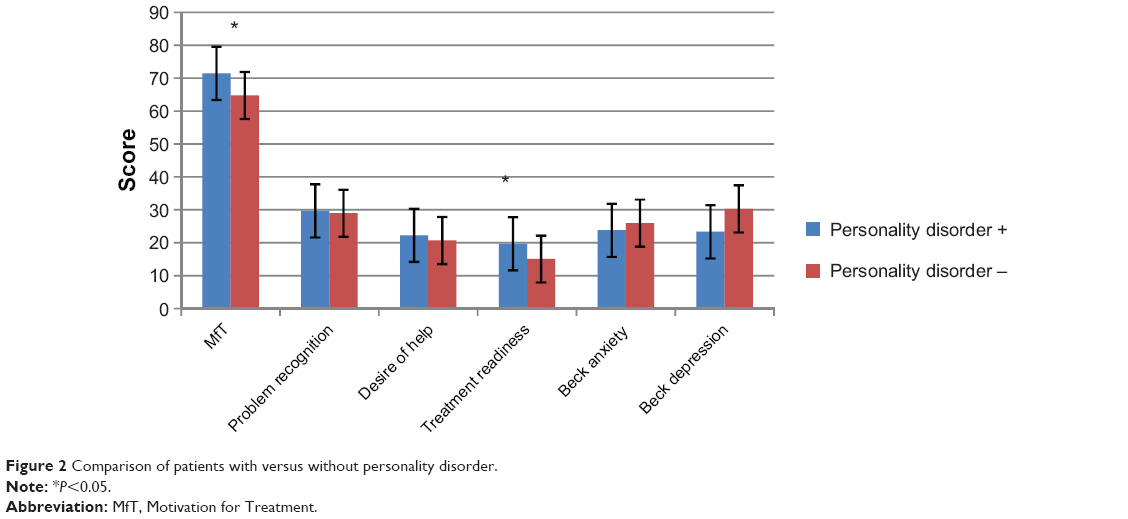 | Figure 2 Comparison of patients with versus without personality disorder. |
Depression
The mean score on the Beck Depression Inventory was 27.7±12.8 for all study participants. Depression and MfT scores were not correlated. When the cut-off score for the Beck Depression Inventory was taken as 17 and a score >17 was accepted to indicate depression, 36 patients (80.0%) were diagnosed as being depressed. When those deemed to be depressed were compared with the others using the Mann–Whitney U-test, there was no significant difference in total MfT scores (61.11±13.63 for the nondepressed group and 68.97±10.39 for the depressed group), and depressed patients scored significantly higher than nondepressed patients on the problem recognition subscale of the MfT (15.11±5.75 and 17.25±5.43, respectively, P=0.01).
Anxiety
The mean score on the Beck Anxiety Inventory was 25.2±5.2 for all participants. A significant correlation was identified between anxiety scores and problem recognition (r=0.332, P<0.05).
Predictors of MfT
A regression model was generated to determine the probable predictors of motivation for treatment. Significant parameters from previous statistical analyses were included in the model as independent variables. A linear regression analysis was conducted. The total motivation score was accepted as the dependent variable, and volunteering, personality disorder, and depression and anxiety scores were accepted as dependent variables in the model. The only predictor of MfT scores was volunteering for treatment (R2=0.391, P<0.05, Table 2).
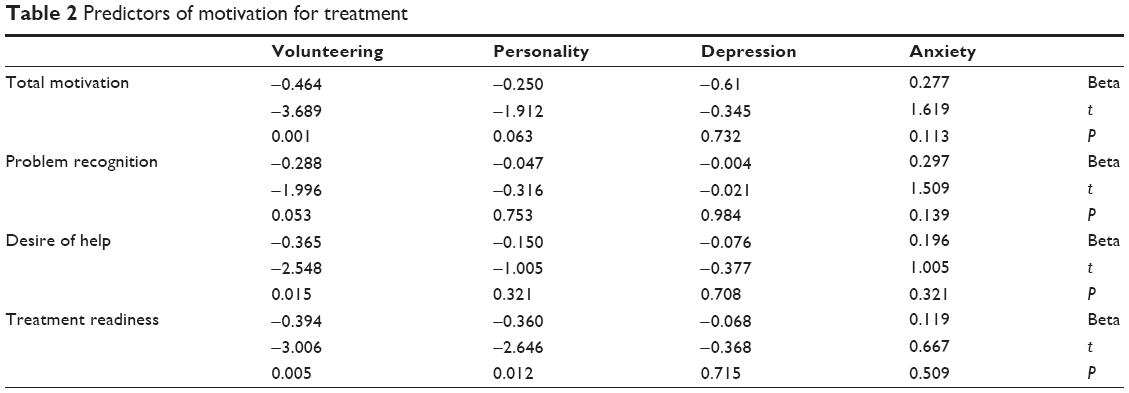 | Table 2 Predictors of motivation for treatment |
Discussion
This study assessed treatment motivation in Turkish patients with substance use disorders from the eastern and south–eastern areas of the country. Our results suggest that the circumstances of admission may affect levels of motivation for treatment and that motivation may be higher in patients undergoing treatment voluntarily. We observed that personality pathology may affect readiness for treatment and that depressive symptoms may be related to increased problem recognition.
Previous studies of motivation for treatment in patients with addiction have yielded conflicting results.18–21 It was found that internal sources of motivation, such as a feeling of achievement, were found to be related to long-term change, while external sources of motivation seemed to result in short-term abstinence. In particular, external pressure and legal enforcement were found to predict a better response to treatment among inpatients treated for alcohol dependence.22 It was also reported that even among patients legally enforced to undergo treatment, awareness of problems related to substance use was associated with more active involvement in treatment.22 As a result, it is currently accepted that although external pressures such as legal enforcement may provide an initial impetus for the patient to attempt treatment, internal factors such as readiness for treatment are more important for remission.23 Our results are similar to those reported previously, ie, that patients applying voluntarily for treatment of substance use have higher motivation overall, including desire for help and treatment readiness. However, because of the cross-sectional nature of our study, we could not delineate the prognosis for the two groups of patients. Future longitudinal studies in Turkish patients may help in this regard.
It has been posited previously that certain personality types may be at increased risk of addiction and less likely to be motivated for treatment.24 In contrast, it was shown that antisocial personality disorder was more common in patients who were admitted voluntarily than in patients admitted via the courts.25 Our results may support this position in that not having personality pathology may increase treatment readiness. However, due to the heterogeneity of Axis II diagnoses in our sample as well as its small sample size, our results should be evaluated with caution and further studies involving more homogeneous and larger samples may be needed to determine the interaction between personality pathology and motivation for treatment in Turkish patients with substance use disorders.
Lastly, we have found that depressive symptoms as measured by the Beck Depression Inventory were related to increased levels of problem recognition among the patients. Numerous studies have indicated a high degree of comorbidity between major depression and substance use disorders. This comorbidity is associated with a poorer effect of treatment, resulting in poorer psychosocial functioning, a higher number of days in treatment, higher attrition rates, more admissions, and a higher burden of disease arising from both major depression and substance use disorder.26 This study found a relationship between depression and problem recognition, and this finding is in accordance with a previous report.27 However, due to the cross-sectional nature of most of the research on motivation, including our study, the direction of the relationship between problem recognition and depressive symptoms in patients with substance use disorder remains elusive. Further studies may help to clarify the temporal relationship between those two phenomena.
The main limitations of our study are its small sample size, sampling bias, and the heterogeneity in personality disorders as well as the substances used. Despite these limitations, it is the first study to evaluate motivation for treatment in Turkish patients enrolling in a treatment program for substance abuse and for this reason it was deemed worthy of presentation. In conclusion, we suggest that the circumstances of admission may affect levels of motivation for treatment of substance use in Turkish patients. It can also be argued that the techniques used for motivational interviewing may be particularly important in patients undergoing enforced treatment.
Conclusion
Motivation for treatment is affected by external factors, including circumstances of admission, and by internal factors, such as personality disorder and depression. This study identifies voluntary admission as a predictor of motivation for treatment. Personality disorder and depression scores show significant relationships, but our small sample size precludes a clear relationship. Investigation of ways into encouraging voluntary admission for treatment instead of enforced admission may be helpful in increasing levels of motivation for treatment in substance users.
Disclosure
The authors report no conflicts of interest in this work.
References
Figlie NB, Dunn J, Laranjeira R. Motivation for change in alcohol dependent outpatients from Brazil. Addict Behav. 2005;30(1):159-165. | ||
De Leon G, Jainchill N. Circumstance, motivation, readiness and suitability as correlates of treatment tenure. J Psychoactive Drugs. 1986;18(3):203-208. | ||
Diclemente CC, Carbonari JP, Velasquez MM. Alcoholism treatment mismatching from a process of change perspective. In: Watson RR, editor. Alcohol Abuse Treatment. Totawa, NJ, USA: Humana Press; 1992. | ||
Ryan RM, Plant RW, O’Malley S. Initial motivations for alcohol treatment: relations with patient characteristics, treatment involvement, and dropout. Addict Behav. 1995;20(3):279-297. | ||
Laudet AB, Stanick V. Predictors of motivation for abstinence at the end of outpatient substance abuse treatment. J Subst Abuse Treat. 2010; 38(4):317-327. | ||
Burrow-Sanchez JJ, Lundberg KJ. Readiness to change in adults waiting for publicly funded substance abuse treatment. Addict Behav. 2007;32(1):199-204. | ||
Evren C, Saatcioglu O, Can Y, Cakmak D. [The reliability and validity of the Turkish version of the Texas Christian University Motivation for Treatment Scale]. Psikiyatri Psikoloji Psikofarmakoloji (3P) Dergisi. 2004;12(1):22-30. Turkish. | ||
American Psychiatric Association. [Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition]. Ankara, Turkey: Hekimler Yayin Birliği; 1994. Turkish. | ||
World Medical Association. World Medical Association declaration of Helsinki – ethical principles for medical research involving human subjects. Available from: http://www.wma.net/en/30publications/10policies/b3/. Accessed July 16, 2014. | ||
Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry. 1961;4:561-571. | ||
Hisli N. [A discussion on the validity of the Beck Depression Inventory]. Psikoloji Dergisi. 1988;6:118–122. Turkish. | ||
Beck AT, Epstein N, Brown G, Steer RA. An inventory for measuring clinical anxiety: psychometric properties. J Consult Clin Psychol. 1988; 56(6):893-897. | ||
Ulusoy M. The psychometric properties of the Beck Anxiety Inventory. Unpublished Dissertation. Istanbul, Turkey: Bakirkoy Mental and Nervous Disorders Training and Research Hospital; 1993. | ||
Simpson DD, Joe GW. Motivation as a predictor of early dropout from drug abuse treatment. Psychother Theor Res Pract Train. 1993;30(2): 357-368. | ||
Spitzer RL, Williams JBW, Gibbon M. Structured Clinical Interview for DSM-III-R Personality Disorders (SCID-II). New York, NY, USA: New York State Psychiatric Institute; 1987. | ||
Sorias S, Saygili R, Elbi H. Structured Clinical Interview for DSM-III-R Personality Disorders (SCID-II), Turkish Version. Izmir, Turkey: Ege University Press; 1990. | ||
Sinclair-Webb E. “Our bulent is now a commando:” military service and manhood in Turkey. In: Ghoussoub M, Sinclair-Webb E, editors. Imagined Masculinities: Male Identity and Culture in the Modern Middle-East. London, UK: Saqi Books; 2000. | ||
Deci EL, Ryan RM. The support of autonomy and the control of behavior. J Pers Soc Psychol. 1987;53(6):1024-1037. | ||
Higgins ST, Budney AJ. Treatment of cocaine dependence through the principles of behavior analysis and behavioral pharmacology. In: Onken LS, Blaine JD, Boren JJ, editors. Behavioral Treatments for Drug Abuse and Dependence NIDA Research Monograph No. 137. Rockville, MD, USA: National Institute on Drug Abuse; 1993. | ||
Stitzer ML, Iguchi MY, Kidorf M, Bigelow GE. Contingency management in methadone treatment: the case for positive incentives. In: Onken LS, Blaine JD, Boren JJ, editors. Behavioral Treatments for Drug Abuse and Dependence NIDA Research Monograph No. 137. Rockville, MD, USA: National Institute on Drug Abuse; 1993. | ||
Krampen G. Motivation in the treatment of alcoholism. Addict Behav. 1989;14(2):197-200. | ||
Broome KM, Knight DK, Knight K, Hiller ML, Simpson DD. Peer, family, and motivational influences on drug treatment process and recidivism for probationers. J Clin Psychol. 1997;53(4):387-397. | ||
Joe GW, Simpson DD, Broome KM. Effects of readiness for drug abuse treatment on client retention and assessment of process. Addiction. 1998;93(8):1177-1190. | ||
Eysenck H. Addiction, personality and motivation. Hum Psychopharmacol. 1997;12 Suppl 2:79-87. | ||
Banducci AN, Dahne J, Magidson JF, Chen K, Daughters SB, Lejuez CW. Clinical characteristics as a function of referral status among substance users in residential treatment. Addict Behav. 2013;38(4):1924-1930. | ||
Wusthoff LE, Waal H, Grawe RW. The effectiveness of integrated treatment in patients with substance use disorders co-occurring with anxiety and/or depression – a group randomized trial. BMC Psychiatry. 2014;14:67. | ||
Nwakeze PC, Magura S, Rosenblum A. Drug problem recognition, desire for help, and treatment readiness in a soup kitchen population. Subst Use Misuse. 2002;37(3):291-312. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.