")
Back to Journals » Risk Management and Healthcare Policy » Volume 14
Mothers’ Opinions on Vaccinations and Penal Responsibility for Vaccination Avoidance in Nine Selected European Countries: Findings from a Cross-Sectional Survey
Authors Pisaniak P , Konarska M , Tarczon A , Stawowy B , Bejster K, Piórek W, Mędrzycka-Dąbrowska W , Ozga D
Received 29 September 2020
Accepted for publication 29 January 2021
Published 23 March 2021 Volume 2021:14 Pages 1241—1254
DOI https://doi.org/10.2147/RMHP.S283796
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Marco Carotenuto
Paulina Pisaniak,1 Milena Konarska,2 Aleksander Tarczon,1 Bartłomiej Stawowy,3 Karolina Bejster,3 Weronika Piórek,1 Wioletta Mędrzycka-Dąbrowska,4 Dorota Ozga5
1EMS Students Association, Medical College, Rzeszów University, Rzeszów, Poland; 2Department of Pathophysiology, Jessenius Faculty of Medicine in Martin, Comenius University in Bratislava, Bratislava, Slovakia; 3EMS Students Association, College of Social Sciences, Rzeszów University, Rzeszów, Poland; 4Department of Anaesthesiology Nursing & Intensive Care, Medical University in Gdansk, Gdansk, Poland; 5Institute of Health Sciences, College of Medical Sciences of the University of Rzeszow, Rzeszów, 35-310, Poland
Correspondence: Dorota Ozga
Institute of Health Sciences, College of Medical Sciences of the University of Rzeszow, St. Warzywna 1A, Rzeszow, 35-310, Poland
Email [email protected]
Aim: Relations between penal responsibility and vaccination obligation can be essential for raising the vaccination rate. Social media play a vital role in distributing information. The attitude towards vaccination consists of many factors, including the criminal law situation in the field of vaccination in a given country. The aim of the study was to assess the impact of criminal law liability and other social factors such as age and education on mothers’ desire to vaccinate their children.
Methods: Survey target: mothers from nine European countries (Poland, Germany, Slovakia, France, Norway, Serbia, Romania, Greece, Italy). Response count: 2205. Questionnaire content: adjusted to country-specific legal regulations concerning vaccinations - considering whether vaccines are mandatory, recommended, additional, and how to cover costs. The way of dissemination of the questionnaire: general parental groups on Facebook.
Results: The respondents: Poles (30%), Italians, Germans, Slovaks, Greeks (10% each), Norwegians, Frenchwomen, Romanians, Serbians (5% each). The average respondent age: highest: Norway (38.14± 10.08) and Italy (37.35± 8.12), lowest: Slovakia (30.22± 6.19). Respondents with higher, secondary, vocational, primary education represent 58%, 27%, 12%, 3%, respectively, of the group. Countries with above 90% rate of answers that they vaccinate their children: Greece, Norway, Slovakia, France. The lowest rate (55%) recorded for Romania. Sixty-seven percent aware of the existence of anti-vaccination movements. High rates were recorded for Norway (88%), Romania (82%), Poland (78%), Serbia (71%), Greece (67%), Germany (66%). The lowest rate for France (31%). Countries without vaccination at all (Germany, Norway, Romania, Greece), the rest of the countries mentioned above – have some mandatory, recommended and additional vaccinations.
Conclusion: In countries with mandatory vaccinations parents have their children vaccinated less willingly than in countries with voluntary vaccinations. The rising level of education and providing information about complications following infectious diseases appear to increase the vaccination rate.
Keywords: vaccinations, vaccination obligation, vaccination rate, anti-vaccination movements, recommended vaccinations, additional vaccinations, mandatory vaccinations
Introduction
Immunization can annually save from two to three million lives worldwide, according to WHO data. High immunization rates provide the population with herd immunity, owing to which also people who cannot be vaccinated for health reasons are protected against numerous contagious diseases.1,2 Due to the collective immunity of the vaccinations, they are regulated by the law and vaccines are divided into mandatory, optional and additional. Each country has different legal conditions [Table 1]. While the Internet provides countless sources of information based on up-to-date medical science, the vast majority of Internet users rely on information found in social networks, which are easier to access, but provide mostly unconfirmed information.3 This results in a low awareness of widespread vaccination advantages and in the population’s deteriorating trust in vaccination safety.4 The number of vaccination objectors, that is people who for various reasons do not want to vaccinate themselves or their children has been growing in Europe.5 That is why vaccine-preventable diseases are still present in this day and age and can lead even to an outbreak of epidemic which could otherwise have been prevented. The fewer vaccinated people in a community, the easier it is for the disease to spread. In 2001 the WHO Regional Office for Europe speculated that measles would have been eradicated by 2020 in all countries of the WHO European Region.6 However, it is now known that measles has not been eradicated. Numerous countries of the Region are no longer considered measles-free.7,8 Traveling has never been so easy as it is nowadays. The tourism industry has changed over the last decades and offers unlimited exploring possibilities all over the world. It means that the expansion of contagious diseases is also easier than ever before. With that in mind, we should carefully monitor rates of immunization as well as the progress of infectious disease spread. It is also urgent to strengthen parents’ trust in healthcare professionals, who should never stop sharing reliable information.9 The aim of our survey was to learn the opinion on vaccinations among young mothers from nine European countries. Under individual national jurisdictions, various legal regimes are applicable in terms of the schedule of mandatory vaccinations and administrative or penal sanctions for vaccine refusal [Table 1].
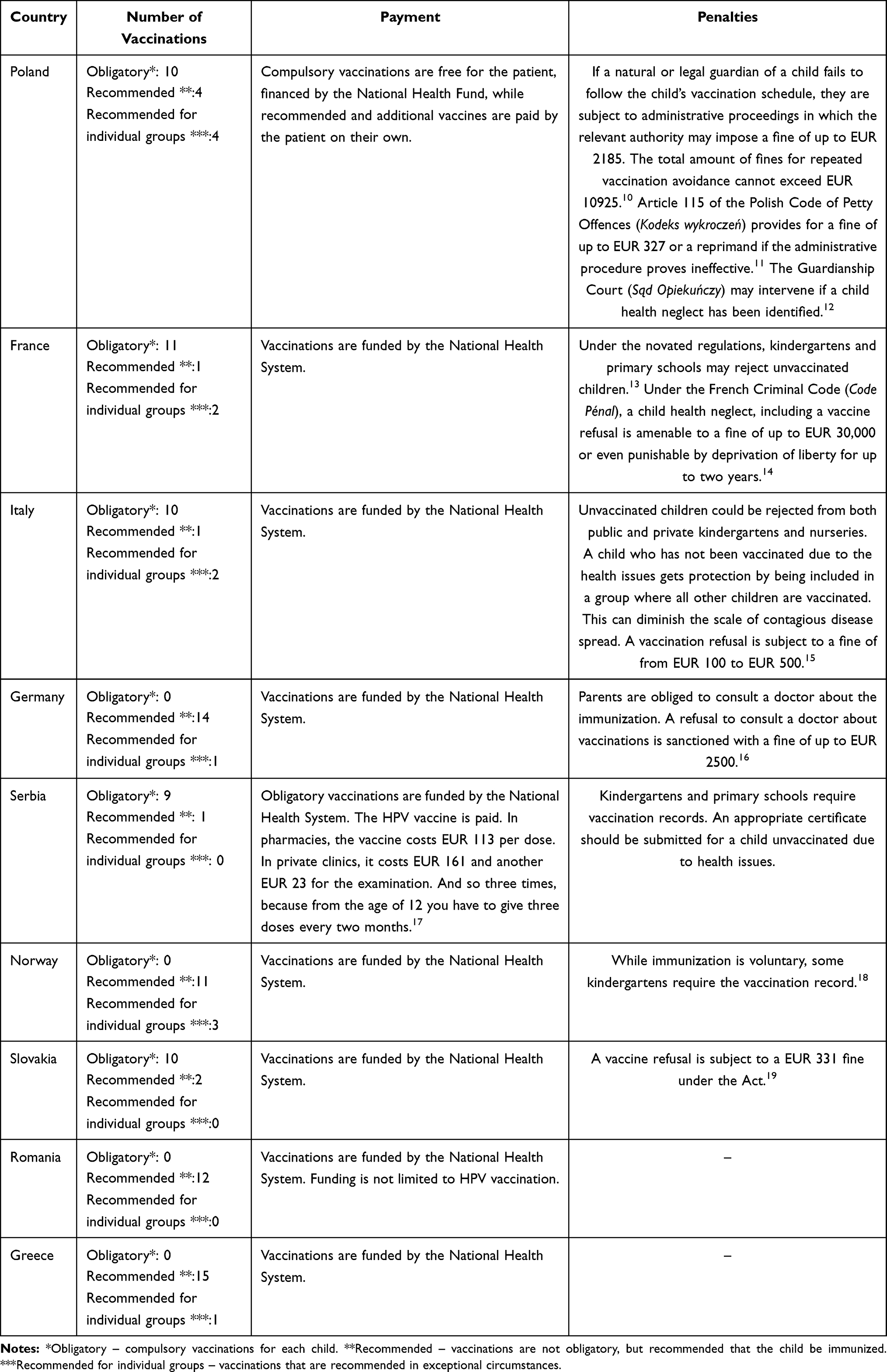 |
Table 1 Number of Vaccinations in Each Country, Payment for Vaccines and Sanctions Imposed on Parents for Not Vaccinating Their Children |
Materials and Methods
The surveyed group consisted of mothers from nine European countries: Poland, Germany, Slovakia, France, Norway, Serbia, Romania, Greece and Italy. There were 2205 responses in total. The collection of all responses was supported by Facebook, which enables participation in various virtual groups, for exchanging experience and advice. The questionnaire was disseminated by authors in thematic groups, searched on the basis of keywords such as motherhood, child, pregnancy, childbirth, upbringing, parents and other related keywords that referred to the topic of children, but did not refer to the subject of vaccination. Owing to the fact, the groups were in the general theme of parenthood. Thanks to this, the groups were general thematic. Parents discuss the broadly understood motherhood and upbringing of children in such groups. The responses were collected from February 12th to March 25th 2020. The respondent selection criteria were connected not so much with vaccinations. It enabled extreme opinions from both anti- and pro-vaxxers to be eliminated, which rendered the results more credible. Participation in the survey was voluntary. The research tool was a questionnaire of 12–16 questions (depending on the country), prepared by the researchers. Ultimately, the final version of the Polish instrument was approved (see Appendix). The differences in the question count resulted from differences between law systems of individual countries. Using the vaccine scheduler service20 and the paper by Kowalcze et al,21 the question list was adjusted, so that in each country, the questionnaire reflected the local vaccination policy. Owing to courtesy of residents of individual countries, up-to-date information on vaccinations was obtained via online communication. The questionnaire was accessible online and covered demographic parameters, opinion on vaccinations, opinion on vaccination safety and efficacy, and the level of respondents’ knowledge of the vaccinations. There were single-choice questions, multiple-choice ones, as well as two open questions. The question concerning the “five in a single injection” vaccination with sub-question “a” was added only in the Polish questionnaire, as this vaccination is paid by its own resources only in Poland. The question concerning additional paid vaccinations (paid for by own means) enabled information to be gained about the mothers’ intention to use such vaccinations. The subsection “a” of the aforementioned question enabled establishing which vaccinations are being chosen by mothers for their children, while sub-question “b” - what makes mothers decide to choose an additional vaccination and sub-question “c” - why mothers do not have their children vaccinated with non-refundable vaccinations. This question was absent from the Norwegian, German, Italian and Greek questionnaires, as all vaccinations are free of charge in those countries. The remaining questions were added to all of the questionnaires. The questionnaires were translated into the native languages of the countries selected and then shared by the authors in groups on Facebook, the search method has been described above.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki. The questionnaire was accepted by the administrator of each group where it was shared. Respondents were invited to participate in the study on a voluntary basis. Each of them was informed about the purpose of the study. Participants were assured that the data collected during the study was anonymous and confidential. In addition, they were also informed of their right not to complete the questionnaire at any time. It was assumed that informed consent to participate in the study was tantamount to sending a completed questionnaire.
Results
Geographical Distribution of Respondents
The surveyed group consists of 2205 respondents from nine European countries. Every third respondent comes from Poland. Italians, Germans, Slovaks, and Greeks represent 10% of the surveyed group each. The remaining countries are Norway, France, Romania, and Serbia representing 5% of the surveyed group each.
Age
The age of respondents varies among countries (F = 34.17, p < 0.001). The highest average age is that of the Norwegians (38.14±10.08), with a median of 37.7, and the Italians (37.35±8.12), with a median of 37. The youngest respondent group comes from Slovakia (30.22±6.19), with a median of 30. For the designated questions, average age levels were checked in each response group and compared with the ANOVA test (F). The significance level was assumed to be p<0.05.
Place of Residence
Village residents represent 28% of the respondents, as do residents of cities with a population of at least 250,000. Twenty-six percent of the respondents live in cities with a population of up to 50,000, with the remaining 18% living in cities with a population between 50,000 and 250.000.
The p-value representing the distribution of place of residence is statistically significant (χ2 = 272, p < 0.00001).
Education
The respondents declaring having higher, secondary, vocational and primary education represent 58%, 27%, 12% and 3%, respectively, of the group surveyed.
The p-value representing the distribution of respondents’ education is statistically significant (χ2 = 897, p < 0.00001) [Table 2].
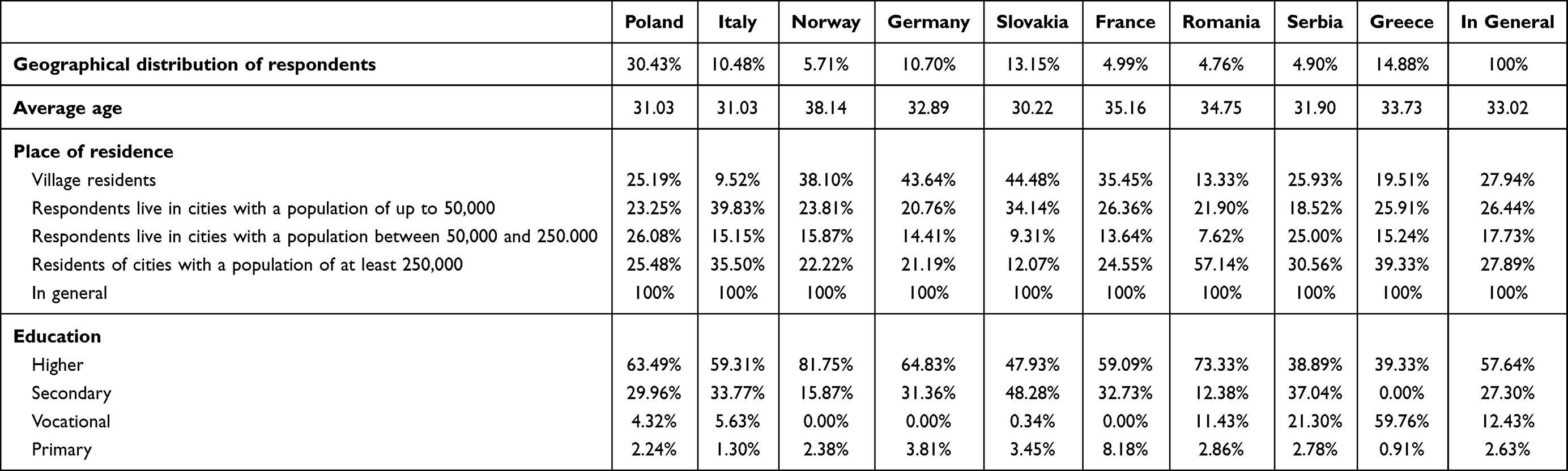 |
Table 2 Distribution of Answers to the Question About the Opinion on the Frequency of the Adverse Events Following Immunization |
Vaccination Rates
In the entire group, 86% of the respondents said they had their children vaccinated, while 14% said they did not. The p-value representing the distribution of answers to the question analysed in the surveyed countries is statistically significant (χ2 = 150, p < 0.00001). High (over 90%) rates of positive answers are recorded in Greece (97%), Norway (96%), Slovakia (93%) and France (93%). It is only 55% in Romania. In the other countries, the rate varies between 80% and 90% [Figure 1]. A significant difference was noted in the impact of education on the desire to vaccinate a child in Slovakia (χ2=10.35, p<0.02) – parents with higher education were more likely not to fill in the mandatory vaccination calendar. In other countries, such dependence was not noticed. After analyzing the answers in relation to age, it was noted that in Poland the average age of people who declare to vaccinate children is significantly lower than that of people who do not vaccinate children (p<0.01), while in Serbia the average age of people who declare to vaccinate children is significantly higher than that of people who do not vaccinate children (p<0.04).
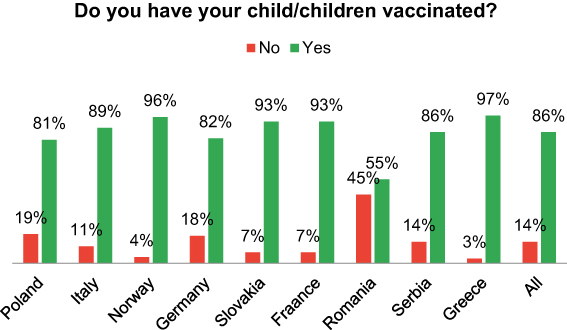 |
Figure 1 Answers to the question “Do you have your child/children vaccinated?” by country. |
Further analysis was conducted to determine the level of knowledge of the adverse events following immunization. To the question of how often such events occur, the answers “Rarely”, “Frequently”, “Very frequently” and “I do not know” were given by 71%, 18%, 11%, and 1%, respectively, of the respondents [Figure 2].
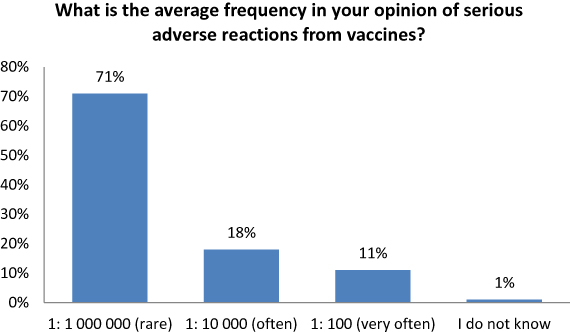 |
Figure 2 Distribution of answers to the question about the frequency of the adverse events following immunization. |
The p-value representing the level of knowledge of the adverse effects following immunization is statistically significant (χ2 = 165.29, p < 0.00001).
Anti-Vaccination Movements and Their Social Impact
- In the entire group surveyed, 63% claimed having met with anti-vaccination movements, 37% claimed the opposite. The p-value representing the awareness of anti-vaccination movements’ activity is statistically significant (χ2 = 445.09, p < 0.00001). The highest rates of the awareness were recorded in Norway (88%), Romania (82%), Poland (78%), Serbia (71%), Greece (67%) and Germany (66%). In France, the rate was materially lower, at 31%. In Poland and Slovakia a significant (p<0.00008, p<0.003) influence of education on the knowledge of anti-vaccine movements was found. In these countries people with higher education significantly more often declared the knowledge of anti-vaccine movements. The average age level for which the answer “7. Are you familiar with anti-vaccine movements?” was significantly different in Poland and Greece. The age of people who are not familiar with anti-vaccination movements in Greece and Poland was significantly lower than the age of people who are familiar with anti-vaccination movements.
- In the group of 1411 respondents, 36.01% gave no answer to the question “How do you assess anti-vaccination movements activity?”. Around one-third (32.47%) assessed the activity as “unsatisfactory”. 17.87% of the respondents expressed a neutral opinion. The anti-vaccination movements’ activity was assessed as “satisfactory” by 13.65% of the respondents. The p-value representing the distribution of the opinion on anti-vaccination movements’ activity is statistically significant (χ2 = 337.35, p < 0.00001). The highest rates of the “unsatisfactory” answer were recorded in Norway (84%), Italy (64%), Greece (53%) and Germany (53%). The highest rate of the neutral answer was recorded in France (48%). The highest rates of the “satisfactory” answer were recorded in Romania (71%) and Slovakia (37%). In Serbia, there were significant differences in the education level groups regarding the evaluation of anti-vaccine movements. Bad anti-vaccination movements were significantly more often assessed by people with vocational schooling. People with secondary school education were significantly more indifferent. Individuals with higher education were significantly more likely to have a good opinion of anti-vaccination movements. The average age of people in Norway who misjudged the activity of anti-vaccination organizations was significantly higher than people who were neutral towards this assessment.
- More than half (58%) of the respondents claimed to have encountered an attempt to persuade them about the harmfulness of the vaccinations and the remaining 42% said no. The p-value representing the respondents’ exposure to the effort to convince them into an anti-vaccination attitude is statistically significant (χ2 = 39.49, p < 0.00001). In the group surveyed, country by country, the highest rates of respondents who have been exposed to attempts of convincing of the harmfulness of vaccination were recorded in Serbia, France and Norway (67%, 66% and 66%, respectively). Relatively high rates were also recorded in Poland (64%) and Italy (60%). Lower values were recorded in Romania, Greece and Slovakia (45%, 50%, and 53%, respectively). In Romania, a significant (p<0.03) impact of education on the declarations of attempted persuasion about the harmfulness of vaccination was found. In this country, people with vocational education significantly more often declared attempts to convince people about the harmfulness of vaccination. The average age level for which the answer “Has anyone ever tried to convince you of the harmfulness of vaccination?” was analysed and was significantly different in Poland. People who tried to convince them about the harmfulness of vaccinations were significantly younger than those who did not have such attempts [Table 3].
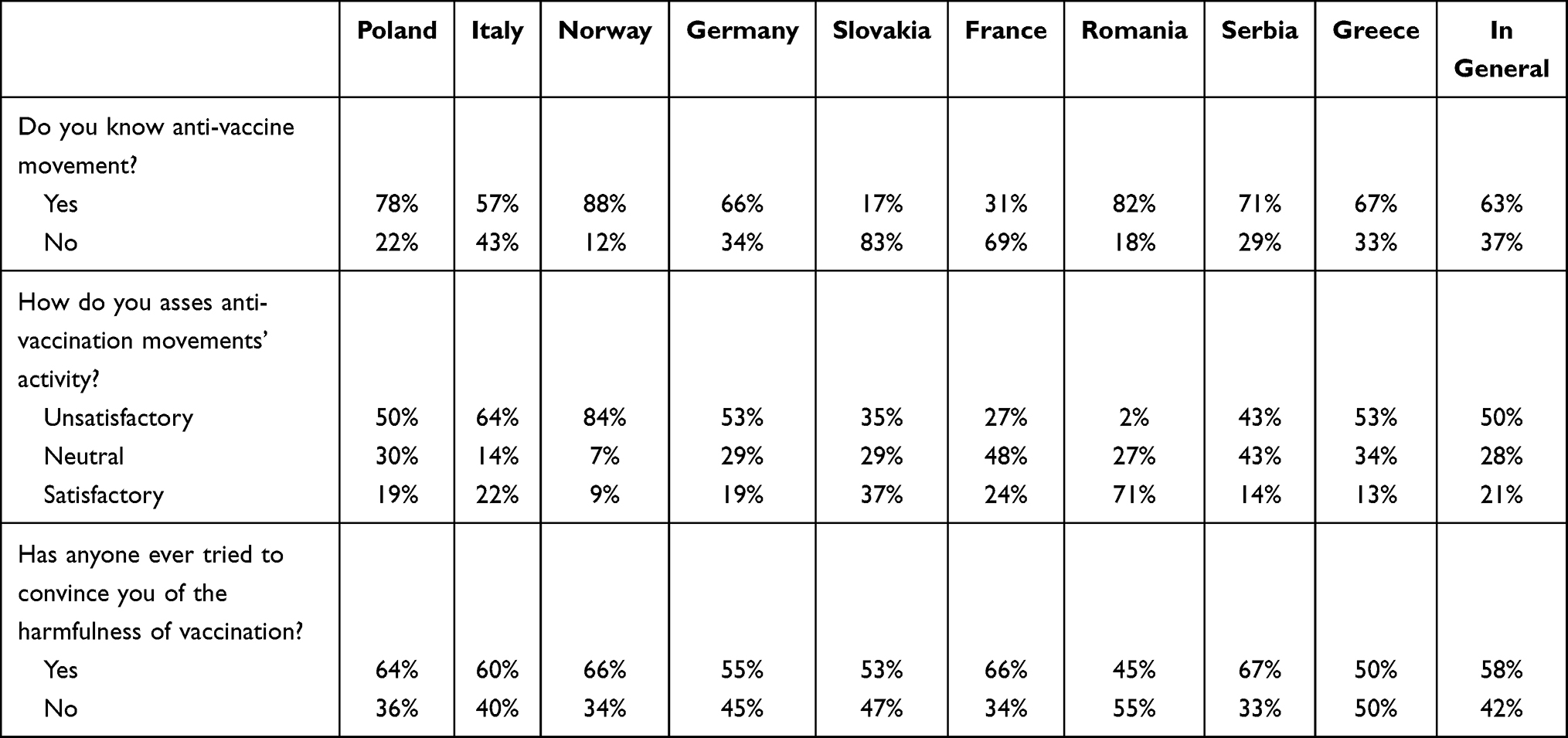 |
Table 3 Characteristics of the View on Sanctions Against Parents Who Do Not Vaccinate Their Children in Individual Countries |
Restrictions Concerning Vaccine Hesitancy
The answer distribution for the question: “Do you think that parents who do not have their children vaccinated should be penalized?” varies significantly among the countries surveyed (χ2 = 230.72, p < 0.00001). The rates of the “No” answer were highest in Romania (60%) and France (42%). The highest rates of the “Yes” answer were in Greece and Poland (53% and 38%, respectively). Fifty-seven percent of the Slovak respondents and 55% of the Norwegian ones stated that the penalization issue depends on the circumstances [Figure 3]. The distribution of views in Poland was significantly different in various educational groups. In Poland, people with higher education were more likely to be in charge of not imposing financial penalties, and people with secondary education were more likely to be responsible for the situation.
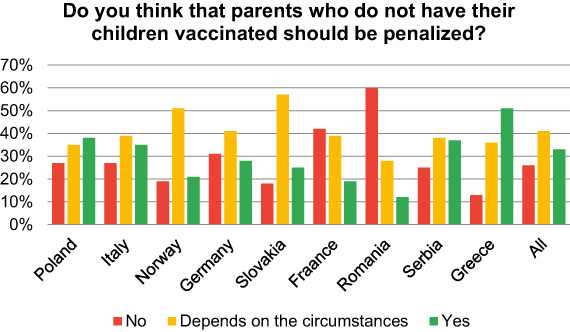 |
Figure 3 Characteristics of the view on sanctions against parents who do not vaccinate their children in individual countries. |
The Cost of Vaccinations
The question “Do you have your children vaccinated with additional paid vaccinations?” was answered by 1738 respondents from six countries, in which some of the recommended vaccines are paid by the citizen. Forty-five percent of the respondents answered “Yes”, while 55% answered “No”.
The p-value representing the rate of positive answers to the question referred to above is statistically significant (χ2 = 80.93, p < 0.00001). In Serbia (68%), France (57%) and Poland (51%) materially high rates of the “No” answer (68%, 57% and 51%, respectively) were recorded. On the other hand, the “Yes” answer had the highest rates in Greece (71%) and Italy (65%).
In Poland and France, there were significant differences in education groups regarding additional paid vaccinations. People with higher education significantly more often performed additional paid vaccinations [Table 4].
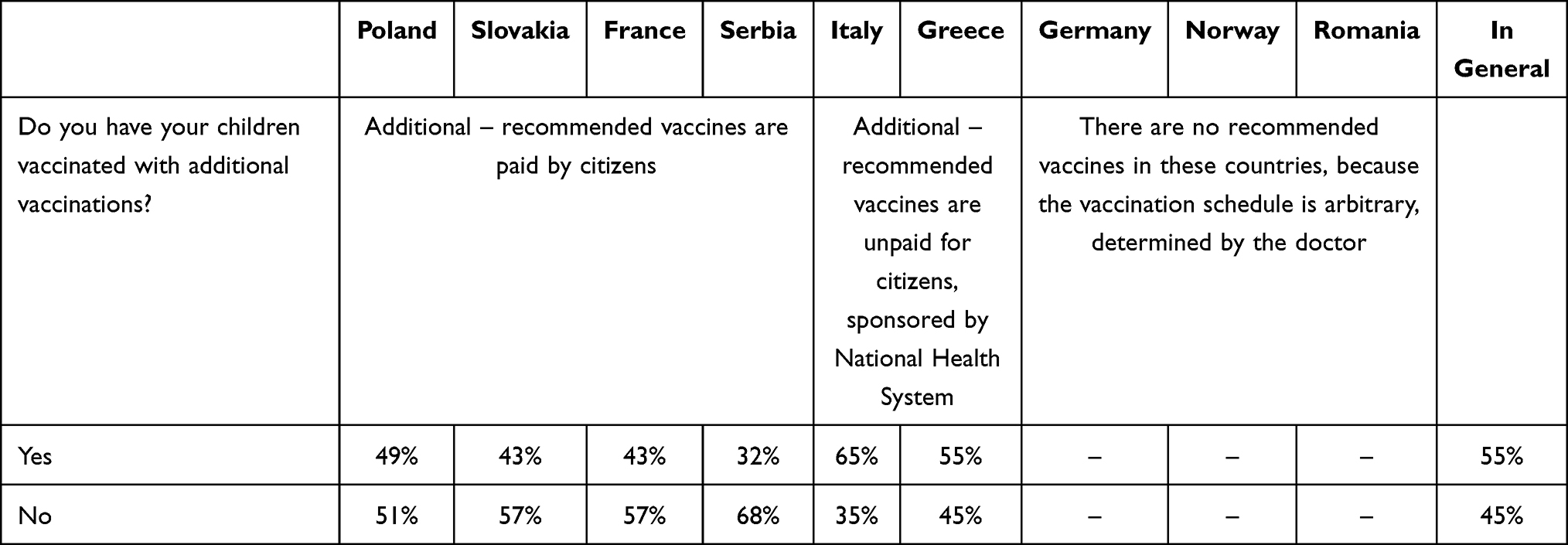 |
Table 4 Characteristics of the Opinion on the Validity of Limiting Access to Nurseries and Kindergartens for Unvaccinated Children |
Attitude to Sanctions Resulting from Vaccination Avoidance
Another question was “Do you consider it right to limit the access to nurseries and kindergartens for unvaccinated children?”. In the group surveyed, 65.76% of respondents considered it right, whereas every fourth of the respondents declared the opposite. 7.66% expressed no opinion on the subject [Figure 4].
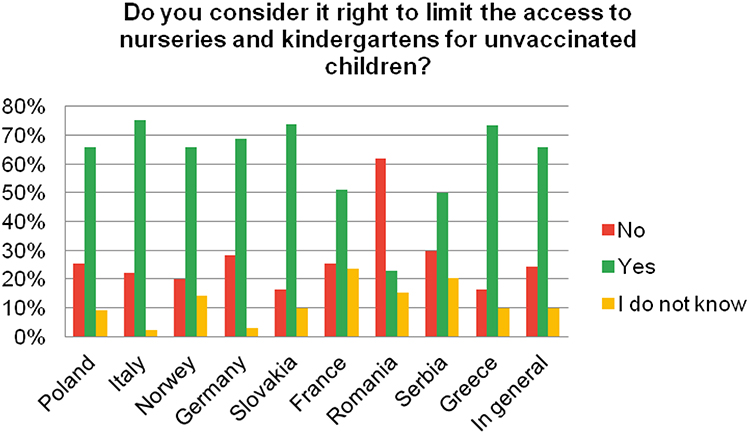 |
Figure 4 Characteristics of the opinion on the validity of limiting access to nurseries and kindergartens for unvaccinated children. |
Distribution of the opinions on the limitations varies significantly among the surveyed countries (χ2 = 314.27, p < 0.00001). The rate of the “No” answer was significantly high in Romania (62%). The highest rates of the “Yes” answer were recorded in Italy (75%), Slovakia (74%) and Greece (73%). The characteristics of the view on limiting access to nurseries and kindergartens for non-vaccinated children in different countries in education groups were significantly different in Romania, where people with higher education were significantly more often against such limitations. For comparison, in Greece, a similar view was presented by persons with vocational education, and persons with higher education were significantly more often not of an opinion on the subject.
Discussion
Mother’s Age and Her Approach to Vaccinations
Scientific research in the vaccination issue often omits the mother’s age. The survey run by Salmon’s team in the USA in 2009 revealed that the vaccination rate for children of 17-year-old mothers stood at 64%, while for children of 26-year-old mothers at 80.6%. For older (26+) mothers no material deviation from the latter value was recorded.22 In 2009 an analysis was performed of vaccination rates for children born in Pennsylvania in 2002–2004. It was clearly demonstrated that the lower the mother’s age, the larger is the number of children who lack some vaccination included in the vaccination schedule.23 The latter was also found to be positively correlated with lower education, larger number of children in the family and lower socioeconomic status. Our survey revealed a similar relation in Serbia, where mothers who do not have their children vaccinated are younger than those who do.
Among the issues covered by the questionnaire was the respondents’ position on limiting access to nurseries and kindergartens for children lacking mandatory vaccinations. Quite interestingly, the results revealed no clear relation between the approach to the issue and the average age of mothers. This is most clearly seen when results for Poland and Serbia are compared. In Poland, the highest average age (32.55) was recorded for parents who were against sanctions, while the lowest average age (29.51) for parents who answered that “it depends on the circumstances”. In Serbia, it was the other way round: the highest average age was recorded for parents who chose the answer “it depends on the circumstances”, while the average age of those for the sanctions and the average age of those against the sanctions were similar (31.07 and 30.25, respectively).
A statistically important difference was revealed by comparing the results for Poland and Romania. In Poland, for all answers to the question “Do you consider it right to impose financial penalties on parents who do not have their children vaccinated?”, the average age of respondents was around 30. In Romania, the highest average age was recorded for parents who answered they did not know whether imposing financial penalties was right or wrong.
Mother’s Education and Her Approach to Vaccinations
Our survey revealed practically no significant relation between parents’ education and their answer to the question whether they had their children vaccinated: such relation was only observed for Slovak respondents. In Slovakia, persons with higher education declared they did not have their children vaccinated materially more frequently (p < 0.02) than the other parents. A broad range analysis performed by Larson’s team in 2007–201224 discusses numerous studies covering, inter alia, China,25 Lebanon,26 Israel,27 Bangladesh28 and the US29 and reveals that the higher the parents’ education, the larger the percentage of children who do not get vaccinated, which was also revealed in Slovakia in our survey. On the other hand, is six studies conducted in India,30–34,36 it was found that the higher the parents’ education, the larger the percentage of children who do get vaccinated. Similar data were obtained in a literature analysis of the situation in Saudi Arabia carried out by Alabadi et al, which showed that the low level of education of parents was correlated with more frequent deficiencies in vaccinating children.35 In the Democratic Republic of the Congo, the attitudes of both the highest and lowest educated parents proved it infeasible to reach the intended vaccination rate in the country.36 The data referred to above leads to a conclusion that parents’ education alone has no decisive impact on the decision whether to have one’s children vaccinated.
Having a higher education seems to have an adverse effect on the approach to vaccination.38 For instance, Opel et al found that parents with higher education were almost fourfold more concerned about vaccine safety than parents with lower education.39 Similarly, Smith et al determined that parents with higher education more often refused to have their children vaccinated with any child vaccine than parents with lower education;40 these findings are consistent with the results of this survey for Slovakia. Reluctance and doubts with regard to vaccinations, as well as vaccination avoidance were to a large extent correlated with the position that it is right to neither impose financial penalties on parents who do not have their children vaccinated nor limit the access to day-care and educational institutions for unvaccinated children. Commentaries to open questions from parents who did not have their children vaccinated reveal that such parents were for free choice and doubted in vaccine efficacy and safety, as well as deemed it pointless to limit access to nurseries for unvaccinated children, as they pose no threat to vaccinated (hence, immunized) peers. Other studies39,41,42 reveal that also parents’ low education renders them distrustful to healthcare personnel and vaccinations. Distrust to vaccinations is accompanied by the opinion that it is right to neither impose financial penalties on parents who do not have their children vaccinated nor limit the access to public institutions for unvaccinated children.
Vaccination Rate and Availability of Free of Charge Additional Vaccinations
Our research revealed a correlation between the availability of free additional vaccinations and child vaccination rate. In Poland (situation in 2005 year), France, Serbia and Slovakia, additional vaccinations, for instance against rotavirus, are offered with a charge.43 In Poland from January 2021 rotavirus vaccination is included into mandatory vaccines and is free of charge. Analysis of submitted questionnaires shows that vaccination rates in these countries were lower than in, for instance, Italy and Greece, where the cost of additional child vaccinations is fully refunded [Table 4], with the only exception being rotavirus vaccination in Greece, where 75% of the cost is refunded; still much more than, for example, 20% in Slovakia. A preliminary conclusion would thus be that the financial burden of vaccinations definitely affects the child vaccination rate. In Poland, France and Serbia more than half (in Serbia as much as 68%) of the respondents were not willing to have their children vaccinated with additional paid vaccines. In Slovakia, the rate was close to a half (44%). In Italy and Greece, where additional child vaccinations are fully refunded, it was mere 35% and 29%, respectively. What is surprising is that it was only in Poland that financial considerations have a material share (slightly over 20%) in all reasons for not having one’s children vaccinated with additional vaccines. In the other questionnaire versions (in France, Slovakia and Serbia), the share of financial considerations is only around 6%. An in-depth analysis of answers to the question why mothers do not have their children vaccinated with additional vaccines reveals that the most often reason for such a decision was the mother’s belief that such preventive measure is useless. Thus, it can be concluded that respondents from all countries covered by the research put larger emphasis on other, non-financial aspects while deciding whether to have their children vaccinated. Consequently, based on our research, one may conclude that the above-stated hypothesis “the financial burden of vaccinations definitely affects the child vaccination rate” is not true. For the sake of comparison, let us observe that according to Malerba et al among most important drivers of child vaccination rate (in the study referred to, for meningococcal and pneumococcal vaccines) there are the family’s socioeconomic status and the cost of the paid additional vaccine.44 A family’s higher income and higher socioeconomic status are among primary factors raising the child vaccination rates for meningococcal and pneumococcal vaccines. The high cost of vaccination prevented less affluent families from having their children vaccinated.45,46
Opinions on Financial Penalties and Limited Access to Nurseries
In Italy, Slovakia and Greece three-fourths of the respondents said it was right to limit access to nurseries for unvaccinated children.
Italy has such sanction in place and the majority of respondents were for it. A study performed there47 revealed that the majority of the country’s population deem vaccinations as a duty for public benefit, as they prevent the spread of infectious diseases. A study carried out in Italy in 201848 indicates that the extension of mandatory vaccination chart and implementation of related legal regulations pushed vaccination rates up. Thus, law proves instrumental in increasing vaccination rates. In Greece and Slovakia, the access to nurseries is not limited, but still three-fourths of the respondents would support such limitations. In Romania, on the other hand, as much as 62% of the respondents were against such sanction, which has not been implemented there anyway. In Norway and Germany, where vaccinations are not mandatory, 66% of the respondents supported the sanction. In France and Italy, children have to be vaccinated with mandatory vaccines before starting school. The studies carried out indicate that in the majority of countries, the existing governmental policies have failed to eliminate, for instance, measles epidemic occurrences.49 In Romania, 62% of the respondents opposed the sanction. Studies revealed that one-third of parents refuse to have their children vaccinated, with main reasons being information sourced from media and anti-vaccination movements.50
In Romania, the main reason for vaccination reluctance proved a lack of knowledge of vaccinations and on their beneficial effects, as confirmed by a study.52
In our survey, over 50% of respondents in each of six out of nine countries (in Greece, Serbia, Slovakia, Poland, Norway and Italy) said it was right to impose financial penalty for refusing to have one’s children vaccinated. In Poland, 66% of the respondents supported such penalties. These results are consistent with the findings of the survey conducted to the order of the Wirtualna Polska Internet portal by the country-wide survey portal Ariadna on November 15th–19th 2019. In the survey, 55% of the respondents supported financial penalties.51 The highest rate of respondents opposing financial penalties (71%) was recorded in Romania.52 Such penalties have not been introduced in that country and, should they be introduced, they would not enjoy much support. This proves that financial sanctions alone may not induce parents into having their children vaccinated. The study carried out by Kaufman et al indicates that educating parents and making them aware of vaccination benefits are significant drivers of vaccination rates.53 Perhaps appropriate legal regulations in combination with education of the society and limitation of the access to nurseries would enable WHO’s objectives to be achieved. Findings of the research conducted by Bechini et al emphasize that, while mandatory vaccinations and legal sanctions for vaccination avoidance are useful tools to increase vaccination rates, the effect of using those tools changes from country to country in response to numerous other factors.54
Vaccination Price and Support of Anti-Vaccination Movements
Vaccinations are refundable in Norway, Germany, Italy and Greece, whereas they are paid (or partly refundable) in Poland, Slovakia, France, Romania and Serbia. In our research, 86% of the respondents said they had their children vaccinated, while 14% said they did not. Among the nine countries covered by the research, three were identified where the percentage of unvaccinated children was higher than the median value. These countries are Poland (19%), Germany (18%) and Romania, where up to 45% of the respondents declared they did not have their children vaccinated. When it comes to the vaccination rate, the highest, worth noting values were recorded for Italy (89%), Slovakia (93%), France (93%), Norway (96%) and Greece (98%). All in all, among the countries covered by the Wellcome Global Monitor 2018 study, almost 8 people in 10 (79%) “to some extent or fully approve the opinion that vaccines are safe”.55 Nineteen percent of the respondents from Poland did not have their children vaccinated, according to our research. According to the Statistics Poland’s (Główny Urząd Statystyczny) data, in 2018, the percentages of children/youth for whom immunization charts were issued at healthcare centres were as follows: 98.1%, 98.3%, 97.8%, 93.3%, 93.8% and 91.3% for children/youth in the second, third, seventh, eleventh, fifteenth and twentieth, respectively, year of life. Thus, almost 10% of young adults were not issued immunisation charts.56 The Wellcome Global Monitor 2018 results indicate that every third inhabitant of France doubts vaccination safety. Doubts concerning vaccinations declared by the French do not reflect their real behaviour. Out of all French mothers covered by the Wellcome Global Monitor 2018 study, 91% declared they had their children vaccinated,55 which was corroborated in our survey.
In the entire surveyed population, 63% had knowledge of anti-vaccination movement existence and 37% did not. Country by country, the highest rate of those familiar with movements existence was recorded in Norway (88%), where 86% of the respondents declared they had their children vaccinated. There are three countries where the unfamiliarity rate was higher than the mean value of 37%: Italy (43%), France (69%) and Slovakia (83%). In May 2018, a new five-year plan entitled “13th General Programme of Work” for 2019–2023 was adopted.58 From among numerous health hazards identified in that document, WHO selected ten which posed the largest threats to human population in 2019. It is no surprise that anti-vaccination attitudes and movements were included in that inglorious ten. WHO warns that mass refusals to undergo protective vaccination may annihilate to-date successes in fighting infectious diseases. Protective vaccinations have proved to be among most efficient preventive medical procedures.
In the entire population surveyed, the distribution of answers to the question “How do you assess anti-vaccination movements activity?” was as follows: bad – 51%, neutral – 28%, good – 21%. The highest percentage of the respondents supporting such movements was recorded in Romania (71%). What is also worth noting is that in Slovakia the percentage of the positive assessments of the anti-vaccination movements is higher than the mean value (37%). High percentages of unsatisfactory or very unsatisfactory ratings of anti-vaccination movements’ activity were recorded in Norway (84%), Italy (64%) and Germany (53%).
Next, we may ask the following question:
In the countries with free-of-charge vaccination, is the percentage of antivaxxers higher or lower than in the countries with paid vaccinations? We have identified no clear relations in this respect. However, analysing data gathered in Romania and Norway, we can find a relation between the popularity of anti-vaccination movements and vaccination refunding by the government. In Romania, where vaccinations are given against a payment, the largest percentages were recorded of parents refusing to have their children vaccinated (45%), as well familiar with (82%) and supporting (71%) anti-vaccination movements. At the other end of the spectrum is Norway, where all vaccinations are financed by the government and the vaccination rate is among the highest in the countries surveyed. Further, it is in Norway that the highest percentages were recorded of respondents familiar with anti-vaccination movements (88%) and those assessing anti-vaccination movements’ activity as socially harmful (84%). In the context of these results, we refer to another survey, conducted by the Ministry of Sport and Tourism of the Republic of Poland and pertaining to health matters and precisely to sports and recreation. Conclusions from the survey included the following: the higher the household income, the higher the sports activity. However, for the respondents, low income was not the highest barrier for sports activity. A similar conclusion can be drawn from our survey: it is not the vaccine price but prejudices that keep vaccination rates down in countries covered by the survey.59
Another aim of our survey was to determine how many parents have their children vaccinated in selected European countries. Eighty-six percent of the respondents answered “Yes” and 14% answered “No” to the question “Do you have your children vaccinated?”. This data is very close to official figures provided by WHO.60 According to official statistics, Norway has one of the highest immunization rates.18 The data which we have collected is consistent with official figures: our survey shows that as many as 96% of the respondents from Norway had their children vaccinated. On the other hand, according to our data, Romania has a vaccination rate of 55%. These data deviates from official figures, which give the vaccination rate of at least 70% (depending on the disease).61 The deviation may be attributable to a small size of the surveyed sample (105), which may render the result not indicative for the attitudes of entire population of the country. In the remaining countries with mandatory vaccinations, the vaccination rates are not less than 81%. The official statistics for the countries surveyed57 also support such a conclusion.
The research tool was a questionnaire prepared by the authors. The questionnaire was published on Facebook. This results in our research having several limitations. Firstly, the surveyed group was of a particular type; the questionnaire was distributed throughout the parenting groups. What must be taken into consideration is that such groups do not reflect the opinions of the entire population of parents. Members of such groups are skilled at using the Internet and spend a particular amount of time in that type of environment. That is why they can copy opinions expressed by other users. We were not able to reach parents who are not involved in the aforementioned groups and do not use the Internet. Such parents can get their knowledge of vaccinations from other sources. Another limitation was the lack of control over the credibility of the responses, due to the anonymous nature of the questionnaire. We cannot undertake any measures preventing filling in the questionnaire by the same person twice. Furthermore, it is worth mentioning that the question “have you vaccinated your child” and the results obtained are not equivalent to the level of vaccination in a given country. This is due to the subiquity of the question, as some parents responded before the first vaccination and some parents halfway through the vaccination calendar and gave up on immunization. In addition, the answers relate to the parent-to-vaccine ratio and not to the number of actual injections.
Conclusions
The subject of our survey was to determine the impact of certain factors on the mothers’ opinions on vaccinations and willingness to have their children vaccinated. The analysed factors were the penal responsibility and the cost of the vaccinations. On the basis of the overall statistics, it can be concluded that parents have their children vaccinated less willingly in the countries with mandatory vaccinations than in the countries without such an obligation. Therefore, the positive influence on the population vaccination rates is not so much a matter of raising restrictions as of raising awareness through education and programmes showing possible complications following infectious diseases.
Acknowledgments
The authors wish to thank the Rector of the University of Rzeszów Sylwester Czopek responsible for funding a research project under a grant Students' Scientific UR.
“In every department of physical science there is only so much science, properly so-called, as there is mathematics.” [Immanuel Kant]
Disclosure
The authors report no conflicts of interest for this work.
References
1. Skinner E. Vaccination policies: requirements and exemptions for entering school. NCSL Legisbrief. 2017;25(48):1–2.
2. Hadjipanayis A, van Esso D, Del Torso S, et al. Vaccine confidence among parents: large scale study in eighteen European countries. Vaccine. 2020;38(6):1505–1512. doi:10.1016/j.vaccine.2019.11.068
3. Stahl J-P, Cohen R, Denis F, et al. The impact of the web and social networks on vaccination. New challenges and opportunities offered to fight against vaccine hesitancy. Med Mal Infect. 2016;46(3):117–122. doi:10.1016/j.medmal.2016.02.002
4. Bozzola E, Spina G, Russo R, Bozzola M, Corsello G, Villani A. Mandatory vaccinations in European countries, undocumented information, false news and the impact on vaccination uptake: the position of the Italian pediatric society. Ital J Pediatr. 2018;44(1):67. doi:10.1186/s13052-018-0504-y
5. Larson H, de Figueiredo A, Karafilakis E, Rawal M, State of vaccine confidence in the EU 2018. European Commission; 2018. Available from: https://ec.europa.eu/health/sites/health/files/vaccination/docs/2018_vaccine_confidence_en.pdf.
6. National Institute of Public Health - National Institute of Hygiene. WHO program for the elimination of measles and rubella; 2018. Available from: https://www.pzh.gov.pl/serwisy-tematyczne/program-who-eliminacji-odry-rozyczki/.
7. National Institute of Public Health - National Institute of Hygiene. Over 140,000 measles deaths worldwide in 2018; 2019. Available from: https://szczepienia.pzh.gov.pl/ponad-140-000-zgonow-w-powodu-odry-na-swiecie-w-2018-roku/.
8. ESNO. Nurses as stable factor in Vaccination uptake; 2018. Available from: https://www.esno.org/assets/files/ESNO_Position_Sstatement_on_Vaccination_04-9-2018.pdf.
9. Ammon A, Prats Monné X. Vaccines, trust and European public health. Eurosurveillance. 2018;23(17):1–3. doi:10.2807/1560-7917.ES.2018.23.17.18-00210
10. The Seym of the Republic of Poland. The Act of 17 June 1966 on enforcement proceedings in administration. Dz.U. 1966 nr 24 poz. 151; 1966. Available from: https://isap.sejm.gov.pl/isap.nsf/download.xsp/WDU19660240151/O/D19660151.pdf.
11. The Seym of the Republic of Poland. The Act of May 20, 1971, Petty Offenses Code. Dz.U. 1971 nr 12 poz. 114; 1971. Available from: http://isap.sejm.gov.pl/isap.nsf/download.xsp/WDU19710120114/O/D19710114.pdf.
12. The Sejm of the Republic of Poland. The Act of February 25, 1964, Family and Guardianship Code. Dz. U. 1964 nr 9 poz. 59; 1964. Available from: http://isap.sejm.gov.pl/isap.nsf/download.xsp/WDU19640090059/O/D19640059.pdf.
13. National Institute of Public Health - National Institute of Hygiene. How is vaccination compulsory in different countries? 2020. Available from: https://szczepienia.pzh.gov.pl/dla-lekarzy/organizacja-szczepien-europie/.
14. Institut français d’information juridique. Code pénal [French Institute for Legal Information. Penal Code]; 2020. Available from: http://codes.droit.org/PDF/Code%20pénal.pdf?fbclid=IwAR1uvm9Ui0L6lac8DIYCxDF-V6DiIsy08LB1EQfPG2Wg46hvH_N4kRBCNfA.
15. Ministero della Salute. Legge Vaccini [Ministry of Health. Vaccines Law.]; 2018. Available from: http://www.salute.gov.it/portale/vaccinazioni/dettaglioContenutiVaccinazioni.jsp?lingua=italiano&id=4824&area=vaccinazioni&menu=vuoto.
16. Bundesministerium für Gesundheit. Impfpflicht soll Kinder vor Masern schützen [Federal Ministry of Health. Compulsory vaccination should protect children from measles.]; 2020.
17. Radivojević B. Vakcina koja štiti od raka grlića materice papreno skupa, ali tu nije kraj mukama roditelja. Novosti [The vaccine that protects against cervical cancer is very expensive, but that is not the end of the parents’ suffering. News]. ; 2019.
18. National Institute of Public Health - National Institute of Hygiene. Comparison of the Vaccination Program in Norway and Poland; 2019. Available from: https://szczepienia.pzh.gov.pl/dla-lekarzy/porownanie-programu-szczepien-w-norwegii-i-polsce/.
19. Ministerstvo zdravotníctva Slovenskej republiky. Vyhláška z 10. decembra 2008, ktorou sa ustanovujú podrobnosti o prevencii a kontrole prenosných ochorení [Ministry of Health of the Slovak Republic. Decree of 10 December 2008 laying down details on the prevention and control of communicable diseases.]; 2008.
20. European Centre for Disease Prevention and Control. Vaccine Scheduler; 2020. Available from: https://vaccine-schedule.ecdc.europa.eu.
21. Kowalcze K, Krysiak R, Obuchowicz A. Criminal law regulations concerning the implementation of preventive vaccinations of children and adolescents in selected European countries. Rev Med. 2019;76(7):397. [in Polish].
22. Salmon DA, Smith PJ, Pan WK, Navar AM, Omer SB, Halsey NA. Disparities in preschool immunization coverage associated with maternal age. Hum Vaccin. 2009;5(8):557–561. doi:10.4161/hv.5.8.9009
23. Feemster KA, Spain CV, Eberhart M, Pati S, Watson B. Identifying infants at increased risk for late initiation of immunizations: maternal and provider characteristics. Public Health Rep. 2009;124(1):42–53. doi:10.1177/003335490912400108
24. Larson HJ, Jarrett C, Eckersberger E, Smith DMD, Paterson P. Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: a systematic review of published literature, 2007–2012. Vaccine. 2014;32(19):2150–2159. doi:10.1016/j.vaccine.2014.01.081
25. Zhang S, Yin Z, Suraratdecha C, et al. Knowledge, attitudes and practices of caregivers regarding Japanese encephalitis in Shaanxi Province, China. Public Health. 2011;125(2):79–83. doi:10.1016/j.puhe.2010.10.011
26. Sinno DD, Shoaib HA, Musharrafieh UM, Hamadeh GN. Prevalence and predictors of immunization in a health insurance plan in a developing country. Pediatr Int. 2009;51(4):520–525. doi:10.1111/j.1442-200X.2008.02769.x
27. Muhsen K, Abed El-Hai R, Amit-Aharon A, et al. Risk factors of underutilization of childhood immunizations in ultraorthodox Jewish communities in Israel despite high access to health care services. Vaccine. 2012;30(12):2109–2115. doi:10.1016/j.vaccine.2012.01.044
28. Rahman M, Obaida-Nasrin S. Factors affecting acceptance of complete immunization coverage of children under five years in rural Bangladesh. Salud Publica Mex. 2010;52(2):134–140. doi:10.1590/S0036-36342010000200005
29. Wei F, Mullooly JP, Goodman M, et al. Identification and characteristics of vaccine refusers. BMC Pediatr. 2009;9(1):18. doi:10.1186/1471-2431-9-18
30. Nilanjan PA. Probe into the ways to stimulate childhood immunisation in India: findings from National Family Health Survey-III. Int J Child Adolesc Health. 2012;5:1.
31. Kumar D, Aggarwal A, Gomber S. Immunization status of children admitted to a tertiary-care hospital of north India: reasons for partial immunization or non-immunization. J Health Popul Nutr. 2010;28(3):300–304. doi:10.3329/jhpn.v28i3.5560
32. Phukan RK, Barman MP, Mahanta J. Factors associated with immunization coverage of children in Assam, India: over the first year of life. J Trop Pediatr. 2009;55(4):249–252. doi:10.1093/tropej/fmn025
33. Chhabra P, Nair P, Gupta A, Sandhir M, Kannan AT. Immunization in urbanized villages of Delhi. Indian J Pediatr. 2007;74(2):131–134. doi:10.1007/s12098-007-0004-3
34. Rammohan A, Awofeso N, Fernandez RC. Paternal education status significantly influences infants’ measles vaccination uptake, independent of maternal education status. BMC Public Health. 2012;12(1):336. doi:10.1186/1471-2458-12-336
35. Alabadi M, Aldawood Z. Parents’ knowledge, attitude and perceptions on childhood vaccination in Saudi Arabia: a systematic literature review. Vaccines. 2020;8(4):750. doi:10.3390/vaccines8040750
36. Vikram K, Vanneman R, Desai S. Linkages between maternal education and childhood immunization in India. Soc Sci Med. 2012;75(2):331–339. doi:10.1016/j.socscimed.2012.02.043
37. Mapatano MA, Kayembe K, Piripiri L, Nyandwe K. Immunisation-related knowledge, attitudes and practices of mothers in Kinshasa, Democratic Republic of the Congo. S Afr Fam Pract. 2008;50(2):61. doi:10.1080/20786204.2008.10873699
38. Gowda C, Dempsey AF. The rise (and fall?) of parental vaccine hesitancy. Hum Vaccin Immunother. 2013;9(8):1755–1762. doi:10.4161/hv.25085
39. Opel DJ, Taylor JA, Mangione-Smith R, et al. Validity and reliability of a survey to identify vaccine-hesitant parents. Vaccine. 2011;29(38):6598–6605. doi:10.1016/j.vaccine.2011.06.115
40. Smith PJ, Chu SY, Barker LE. Children who have received no vaccines: who are they and where do they live? Pediatrics. 2004;114(1):187–195. doi:10.1542/peds.114.1.187
41. Prislin R, Dyer JA, Blakely CH, Johnson CD. Immunization status and sociodemographic characteristics: the mediating role of beliefs, attitudes, and perceived control. Am J Public Health. 1998;88(12):1821–1826. doi:10.2105/AJPH.88.12.1821
42. Gust DA, Kennedy A, Shui I, Smith PJ, Nowak G, Pickering LK. Parent attitudes toward immunizations and healthcare providers: the role of information. Am J Prev Med. 2005;29(2):105–112. doi:10.1016/j.amepre.2005.04.010
43. Poelaert D, Pereira P, Gardner R, Standaert B, Benninghoff B. A review of recommendations for rotavirus vaccination in Europe: arguments for change. Vaccine. 2018;36(17):2243–2253. doi:10.1016/j.vaccine.2018.02.080
44. Malerba V, Costantino C, Napoli G, et al. Antimeningococcal and antipneumococcal vaccination determinants: a European systematic literature review. Epidemiol Prev. 2015;6.
45. Theeten H, Vandermeulen C, Roelants M, Hoppenbrouwers K, Depoorter A-M, Damme PV. Coverage of recommended vaccines in children at 7–8 years of age in Flanders, Belgium. Acta Paediatr. 2009;98(8):1307–1312. doi:10.1111/j.1651-2227.2009.01331.x
46. Ganczak M, Dmytrzyk-Daniłów G, Karakiewicz B, Korzeń M, Szych Z. Determinants influencing self-paid vaccination coverage, in 0–5 years old Polish children. Vaccine. 2013;48(48):5687–5692. doi:10.1016/j.vaccine.2013.09.056
47. Chirico F. The new Italian mandatory vaccine Law as a health policy instrument against the anti-vaccination movement. Ann Ig. 2018;30(3):251–256. doi:10.7416/ai.2018.2217
48. Signorelli C, Odone A, Cella P, Iannazzo S. Childhood vaccine coverage in Italy after the new law on mandatory immunization. Ann Ig. 2018;30(Suppl. 1):1–10. doi:10.7416/ai.2018.2227
49. Trentini F, Poletti P, Melegaro A, Merler S. The introduction of ‘No jab, No school’ policy and the refinement of measles immunisation strategies in high-income countries. BMC Med. 2019;17(1):86. doi:10.1186/s12916-019-1318-5
50. Miko D, Costache C, Colosi HA, Neculicioiu V, Colosi IA. Qualitative assessment of vaccine hesitancy in Romania. Medicina. 2019;55(6):282. doi:10.3390/medicina55060282
51. Mielcarek D More than half of Poles want financial penalties for not vaccinating children. Findings; 2020. Available from: https://parenting.pl/ponad-polowa-polakow-chce-wprowadzenia-kar-finansowych-za-nieszczepienie-dzieci-wyniki-badan.
52. Deleanu D, Petricau C, Leru P, et al. Knowledge influences attitudes toward vaccination in Romania. Exp Ther Med. 2019;18(6):5088–5094. doi:10.3892/etm.2019.8124
53. Kaufman J, Ryan R, Walsh L, et al. Face-to-face interventions for informing or educating parents about early childhood vaccination. Cochrane Database Syst Rev. 2018;5(5). doi:10.1002/14651858.CD010038.pub3
54. Bechini A, Boccalini S, Ninci A, et al. Childhood vaccination coverage in Europe: impact of different public health policies. Expert Rev Vaccines. 2019;18(7):693–701. doi:10.1080/14760584.2019.1639502
55. Lavaud S Vaccination: the French Paradox. Medscape, Wellcome Global Monitor 2018; 2019. Available from: wellcome.ac.uk/sites/default/files/wellcome-global-monitor-2018.pdf.
56. Central Statistical Office. Protective vaccinations for children and adolescents; 2020. Available from: https://stat.gov.pl/obszary-tematyczne/zdrowie/zdrowie/szczepienia-ochronne-dzieci-i-mlodziezy,19,1.html.
57. WHO thirteenth general programme of work 2019−2023; 2019. Available from: https://www.who.int/about/what-we-do/thirteenth-general-programme-of-work-2019---2023.
58. WHO anti-vaccine movements one of the greatest health risks; 2019. Available from: http://ptwakc.org.pl/2019/01/22/who-ruchy-antyszczepionkowe-jednym-z-najwiekszych-zagrozen-dla-zdrowia/.
59. Ministry of Sport and Tourism of the Republic of Poland. Sport and recreation: a nationwide survey of Poles; 2013. Available from: https://www.gov.pl/web/sport/aktywnosc-fizyczna-spoleczenstwa.
60. WHO. Reported estimated of BCG coverage; 2020. Available from: https://apps.who.int/immunization_monitoring/globalsummary/timeseries/tscoveragebcg.html.
61. WHO. WHO vaccine-preventable diseases: monitoring system, 2020 global summary; 2020. Available from: https://apps.who.int/immunization_monitoring/globalsummary.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.