Back to Journals » Cancer Management and Research » Volume 12
Most Adult Intussusceptions are Caused by Tumors: A Single-Centre Analysis
Authors Su T, He L, Zhou T, Wu M, Guo Y, Wang Q ![]() , Jiang J, Cao X
, Jiang J, Cao X
Received 23 June 2020
Accepted for publication 15 September 2020
Published 12 October 2020 Volume 2020:12 Pages 10011—10015
DOI https://doi.org/10.2147/CMAR.S268921
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Antonella D'Anneo
Tongrong Su,1 Liang He,1 Tianyu Zhou,1 Menghui Wu,1 Yaohua Guo,1 Quan Wang,1 Jing Jiang,2 Xueyuan Cao1
1Department of Gastric and Colorectal Surgery, The First Hospital of Jilin University, Changchun 130021, Jilin Province, People’s Republic of China; 2Division of Clinical Research, The First Hospital of Jilin University, Changchun 130021, Jilin Province, People’s Republic of China
Correspondence: Xueyuan Cao
Department of Gastric and Colorectal Surgery, The First Hospital of Jilin University, 71 Xinmin Street, Changchun 130021, Jilin Province, People’s Republic of China
Tel/Fax +86-431-81875602
Email [email protected]
Jing Jiang
Division of Clinical Research, The First Hospital of Jilin University, 71 Xinmin Street, Changchun 130021, Jilin Province, People’s Republic of China
Tel/Fax +86-431-81875408
Email [email protected]
Background: Adult intussusception is less common than paediatric intussusception. The aim of this study was to explore the clinical presentation, aetiology, diagnosis and treatment of adult intussusception.
Methods: Adults (> 18 years) with intussusception treated by surgical or conservative measures were included from January 2005 to January 2018, and the manifestation, types, diagnosis and treatment of adult intussusception in our centre were reviewed.
Results: A total of 150 patients with adult intussusception were included in this study. The clinical manifestations included 111 cases (74%) of abdominal pain, 38 cases (25.3%) of bloody stool, 37 cases (24.7%) of bowel obstructions, 33 cases (22%) of abdominal distension, 29 cases (19.3%) of nausea and vomiting, 19 cases (12.7%) of an abdominal mass, and 12 cases (8.0%) of diarrhoea. The types of intussusception were classified into 36 cases (24%) of enteric intussusception, 87 cases (58%) of intestine-colon intussusception and 27 cases (18%) of colonic intussusception. Surgical intervention was applied in 139 cases (92.7%), including 115 patients who underwent open surgery, and laparoscopy-assisted surgery was performed in 24 patients. The main pathogenesis of intussusception was malignant tumors in 51 cases (36.7%) and benign tumors and polyps in 49 cases (35.3%).
Conclusion: Malignant and benign tumors are the main causes of adult intussusception. Abdominal CT is the preferred evaluation method for the preoperative diagnosis of this condition. The choice of surgical procedure depends on the location and type of intussusception.
Keywords: adult intussusception, pathogenesis, surgical, treatment
Introduction
Intussusception is the invagination of a segment of the bowel into the lumen of an adjacent segment. The common form occurs in the proximal-to-distal direction. Intussusception was first proposed by Paul Barbette of the Netherlands in 1674. In 1876, Harald Hirschsprung introduced hydraulic enema reduction technology. Sir Jonathan Hutchinson was the first surgeon to perform surgery for a case of intussusception in 1871.1 Intestinal intussusception is a common disorder in children; however, it is a rare clinical entity in adult patients. Approximately 5% of all cases of intussusception occur in adults. Intussusception accounts for 1%~5% of the aetiology of intestinal obstruction in adults, and any intestinal disease that alters the normal pattern of peristalsis in the gut increases the risk of intussusception.2–4
In adult intussusception, the early and correct diagnosis of the aetiology and timely treatment are very important, and abdominal ultrasound and CT have high sensitivity for the diagnosis of intussusception.5 There is still some debate as to whether reduction is necessary before surgical resection.6
From January 2005 to January 2018, 150 patients with adult intussusception were admitted to the Department of Gastric and Colorectal Surgery, approximately 0.19% (150/78,000) of the total number of inpatients in the same period in the First Hospital of Jilin University. The clinical manifestation, examination results, aetiology, types and treatment of intussusception patients admitted to this single centre were analysed retrospectively. The aim of this study was to determine the possibility of preoperative diagnoses, underlying aetiology and treatment procedures.
Materials and Methods
General Patient Data
The medical records of all patients admitted with a diagnosis of intussusception in the Department of Gastric and Colorectal Surgery, the First Hospital of Jilin University, between January 2005 and January 2018 were reviewed. The inclusion criteria consisted of adult (>18 years of age) intussusception treated by either surgical or conservative measures. Rectal intussusception was not included in this study. The following information was recorded: patient age, sex, symptoms, radiological and operative findings, and pathologic records. Informed consent was obtained from all the participants.
Results
A total of 150 adults with intussusception were treated in our hospital. There were 71 men (47.3%) and 79 women (52.7%). The mean age of the patients was 54.5 years with a range of 18–96 years. In this group, 139 patients (92.7%) who underwent surgery and 11 patients (7.3%) who received conservative treatment recovered well and were cured and discharged. The patients were categorized according to the lead point of intussusception: 36 (24.0%) patients had enteric intussusceptions, 87 (58.0%) patients had intestine-colon intussusception (including ileocolic and ileocaecal types), and 27 (18.0%) had colonic intussusception.
Clinical Presentation
The most common complaint and clinical manifestation was abdominal pain (111 cases, 74%); the other symptoms and signs included 38 cases (25.3%) of bloody stool, 37 (24.7%) cases of bowel obstruction, 32 cases of abdominal distension (21.3%), 29 cases of nausea and vomiting (19.3%), 18 cases of abdominal mass (12%), 12 cases of diarrhoea (8.0%), and 5 cases of fever (3.3%) and other symptoms (Table 1).
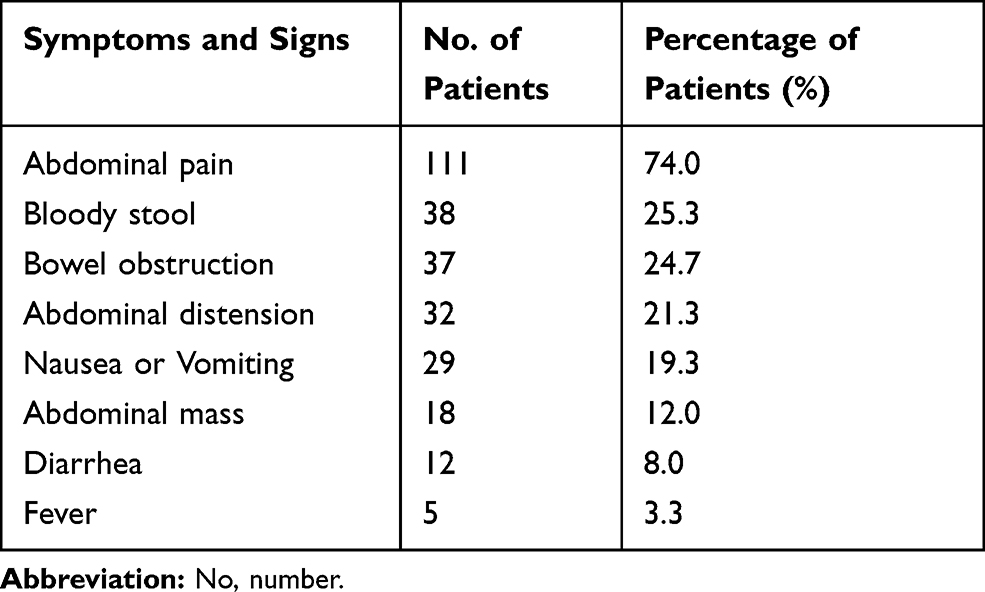 |
Table 1 Clinical Presentation of Patients with Intussusceptions |
Preoperative Examination
The preoperative diagnostic methods for intussusception included abdominal computed tomography (CT), abdominal ultrasonography, barium enema, and colonoscopy. Among the 150 patients, 138 patients (92%) with intussusception underwent abdominal CT, 26 patients (17.3%) underwent colonoscopy, and 22 patients (14.7%) underwent abdominal ultrasound. Three patients underwent barium enema examinations (Table 2).
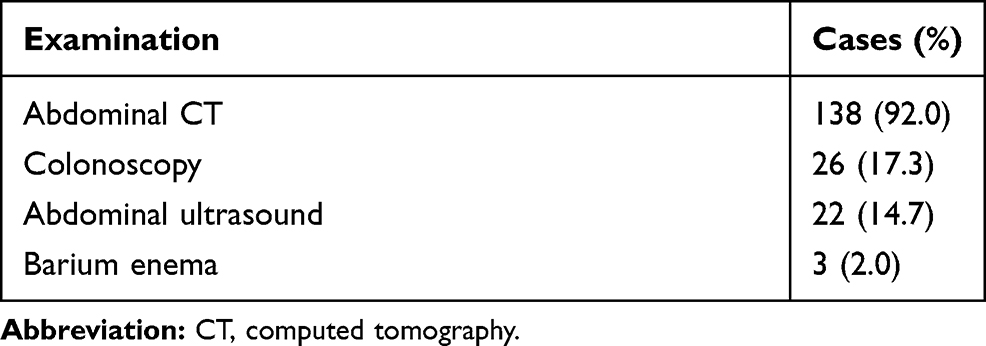 |
Table 2 Preoperative Evaluation in Adult Intussusception |
Aetiology
Among the 150 patients, the pathologic causes were identified in 139 patients who underwent surgery. The results showed that the intussusception of 100 (100/139, 71.9%) patients were related to tumors and polyps, among whom 51 patients (51/139, 36.7%) had malignant tumors, and 49 (49/139, 35.3%) had benign tumors. The other causes included 24 cases (17.3%) of postoperative, six cases (4.3%) of diverticulum, two cases (1.4%) of ectopic pancreas, and seven cases of idiopathic intussusception (5.0%) (Table 3).
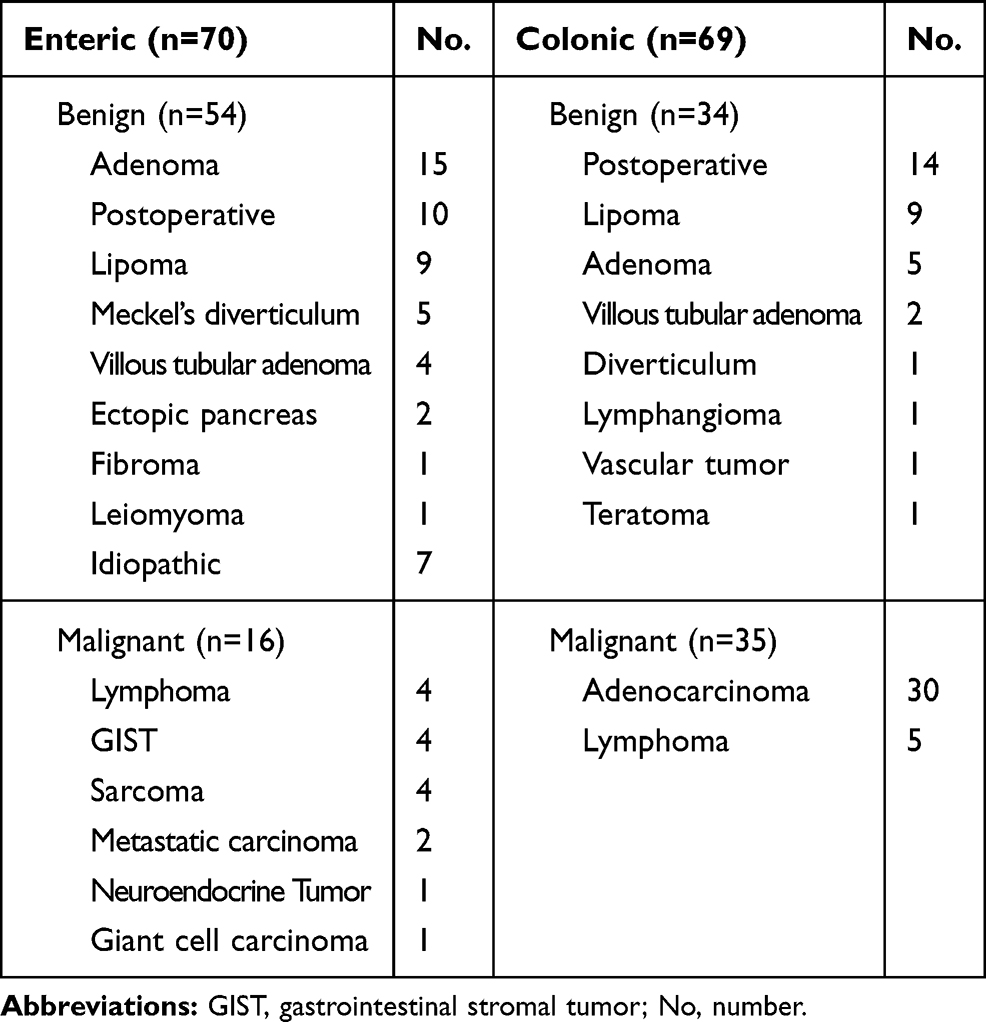 |
Table 3 Etiology of Adult Intussusceptions |
In the small intestine, malignant tumors were found in 16 (16/139, 11.5%) patients, including 14 primary tumors and two metastatic tumors. The 54 cases (54/139, 38.8%) of small intestinal benign diseases included 30 cases of benign tumors, 10 cases of postoperative adhesion, 7 cases of idiopathic causes, 5 cases of Meckel’s diverticulum and two cases of ectopic pancreas. A total of 54 (54/69, 78.3%) patients had tumors in the colon, including 35 patients with malignant tumors and 19 patients with benign tumors. Benign diseases were also found in 14 patients with postoperative adhesions and one patient with diverticulum in the colon (Table 3).
Treatment
A total of 139 patients with intussusception underwent surgical treatment, including 115 patients (82.7%) who underwent open surgery and 24 patients (17.3%) who underwent laparoscopy-assisted surgery. The operations included 51 small bowel resections, 20 ileocecectomies, 40 right hemicolectomies, 2 left hemicolectomies, 7 partial colon resections, one transverse colectomy, 9 intussusception reductions, 6 enterolysis procedures, one small intestinal perforation repair, one mesenteric lymph node biopsy and one small intestinal wall biopsy. In this study, a total of 11 patients with intussusception received conservative treatment. The conservative treatments including fasting, gastrointestinal decompression, parenteral nutrition, anti-inflammatory, correct electrolyte and acid-base balance disorders, and enema treatment.
Discussion
Intussusception is the most common form of intestinal obstruction in children, and the incidence of intussusception among adult intestinal obstruction patients is approximately 1%, accounting for 5–10% of all patients with intussusception. The average age of these individuals was 54.5 years with no sex predominance. More than 90% of children with intussusception have idiopathic disease, with no obvious related aetiology.7 In contrast, more than 90% of adults with intussusception have a definite cause, and more than 65% of these cases are caused by tumors.8,9
Most adult intussusception patients often experience intermittent abdominal pain and vomiting.10 The most common symptoms correspond to the symptoms of intestinal obstruction, including abdominal pain, nausea, vomiting, bloating and tenderness. In our study, 74% of the patients had abdominal pain, and the incidence of haemafecia, nausea and vomiting were 25.3% and 19.3%, respectively.
In the literature, 1214 cases of adult intussusception were reviewed, and approximately 63% of intussusception in adults were related to tumors, 50% of which were malignant. Malignant tumors accounted for 48% of adult colon intussusception cases, and 17% of the related to malignant tumors were in the small intestine.3,5,11 After tumors, postoperative factors are the second most common cause of intussusception in adults. The current result is consistent with previous studies.
Many children with intussusception could be treated conservatively.12,13 However, in most cases, adult intussusception requires surgical treatment.14 Therefore, an early and correct diagnosis is crucial in adult intussusception. Barium enema or gastrointestinal angiography has been used as a classic examination method for intussusception, while abdominal ultrasound and CT are increasingly used in the diagnosis of intussusception. CT scans usually clearly reveal the three-layer structure of intussusception. Moreover, with the development of contrast-enhanced multislice spiral CT, abdominal CT could help to correctly diagnose the aetiology and was considered an effective evaluation method in adult intussusception.15,16 In this study, CT examination was used in 92% of the cases. Furthermore, colonoscopy, abdominal ultrasound, and barium enema examinations were applied in only 17.3%, 14.7%, and 2.0% of the cases, respectively. Obviously, CT examinations have become increasingly important in preoperative examinations.
Surgery is the main treatment for adult intussusception.9,17 There is still some debate as to whether reduction is necessary before surgical resection.8 Because of the high incidence of malignant diseases associated with intussusception, the researchers suggested that adult intussusception should be removed without consideration of reduction, while the removal of bowel segments should be determined according to the length of the intestine affected by the intussusception.1 In our study, 92.7% of patients with intussusception underwent surgical treatment. Of these patients, 87.1% received enterotomy, and 6.5% received intussusception reduction.
Laparoscopic surgical management of the abdomen was associated with a quicker gastrointestinal recovery, shorter postoperative length of stay, and reduced overall complications than open surgery. Laparoscopic surgery has been shown to be safe and feasible, and the laparoscopic approach includes the benefits of minimally invasive surgery.18 A previous report also showed that laparoscopy is safe and effective in the treatment of paediatric intussusception.19 In the current study, 115 patients (115/139, 82.7%) underwent open surgery, and laparoscopy-assisted surgery was performed in 24 (24/139, 17.3%) patients. Laparoscopic surgery was considered better suited for intussusception reduction and patients without bowel obstruction.20 This is perhaps partly because intussusception in adults is rare; the use of laparoscopic surgery remains to be further studied.
The aetiology of adult intussusception is complex, with nonspecific clinical symptoms and signs. We also found two cases of ectopic pancreas in this study. Ectopic pancreas may arise anywhere along the primitive foregut but is most common in the stomach, duodenum, and Meckel’s diverticulum. Clinically, ectopic nodules may result in bleeding, ulceration or bowel obstruction caused by intussusception. The diagnosis and treatment of adult intussusception is still a challenge for abdominal surgeons.21 Because 71.9% of the cases of adult intussusception were found to be related to tumors and polyps in this study, the results suggested that surgical treatment should be the preferred choice for adult intussusception patients.
Previous studies have reported that the incidence of intussusception after Laparoscopic Roux-En-Y gastric bypass (LRYGB) is 0.1% to 0.3% of the cases.22 Since there were few cases of gastric bypass surgery for weight loss performed in our center, we did not find patients with retrograde intussusception after gastric bypass in the current study. Once the diagnosis of retrograde intussusception is made, the first choice is to perform diagnostic laparoscopy and reduce intussuscepted bowel. If the intussusception is not reduced, due to the possibility of bowel necrosis and perforation, conservative treatment is not recommended, laparotomy resection and revision of the anastomosis should be carried out. There were 23 cases of intestinal adhesions and one case of intestinal perforation was found in this study. All of the above 24 patients with intussusception have a history of abdominal surgery, and adhesions and intestinal perforation were found near the intussusception. None of the other etiologies was found during the operation. Thus, the cause of intussusception was diagnosed as “Postoperative” according to previous report.2 Almost 90% of the cases of adult intussusceptions are secondary to pathologic condition. However, there have few cases that are still idiopathic without an exact lesion. In our study, there were seven cases of idiopathic intussusception, and colonoscopy was arranged after cure, but no lesions were found. It should be investigated in future.
The current study was a retrospective study from single centre. We admit the results have some limitations. There have been many previous reports on adult intussusception. Since the incidence of intussusception in adults is low, we collected 150 cases of adult intussusception patients, the sample size was considered was relatively larger among similar reports. In this study, the etiology, diagnosis and treatment of adult intussusceptions were analyzed in detail. We will continue to collect more samples from multi-centres,and provide new findings in the future.
Conclusion
In conclusion, we reviewed the diagnosis and treatment of 150 cases of adult intussusception, and the current retrospective case series may help to summarize the clinical features of this rare condition and suggest the best surgical plans for adult intussusception.
Ethical Approval
This project was approved by the Human Ethics Review Committee of the First Hospital of Jilin University (Changchun, China) (approval number: 2020-393).
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ghaderi H, Jafarian A, Aminian A, Mirjafari Daryasari SA. Clinical presentations, diagnosis and treatment of adult intussusception, a 20 years survey. Int J Surg. 2010;8:318–320. doi:10.1016/j.ijsu.2010.02.013.
2. Azar T, Berger DL. Adult intussusception. Ann Surg. 1997;226:134–138. doi:10.1097/00000658-199708000-00003
3. Cochran AA, Higgins GL, Strout TD. Intussusception in traditional pediatric, nontraditional pediatric, and adult patients. Am J Emerg Med. 2011;29:523–527. doi:10.1016/j.ajem.2009.11.023.
4. Begos DG, Sandor A, Modlin IM. The diagnosis and management of adult intussusception. Am J Surg. 1997;173:88–94. doi:10.1016/S0002-9610(96)00419-9.
5. Omori H, Asahi H, Inoue Y, Irinoda T, Takahashi M, Saito K. Intussusception in adults: a 21-year experience in the university-affiliated emergency center and indication for nonoperative reduction. Dig Surg. 2003;20:433–439. doi:10.1159/000072712.
6. Takeuchi K, Tsuzuki Y, Ando T, et al. The diagnosis and treatment of adult intussusception. J Clin Gastroenterol. 2003;36:18–21. doi:10.1097/00004836-200301000-00007
7. Cha PI, Gurland B, Forrester JD. First reported case of intussusception caused by Escherichia coli O157:H7 in an adult: literature review and case report. Surg Infect (Larchmt). 2019;20:95–99. doi:10.1089/sur.2018.137.
8. Haas EM, Etter EL, Ellis S, Taylor TV. Adult intussusception. Am J Surg. 2003;186:75–76. doi:10.1016/s0002-9610(03)00108-9.
9. Hanan B, Diniz TR, da Luz MM, da Conceicao SA, da Silva RG, Lacerda-Filho A. Intussusception in adults: a retrospective study. Colorectal Dis. 2010;12:574–578. doi:10.1111/j.1463-1318.2009.01865.x.
10. Honjo H, Mike M, Kusanagi H, Kano N. Adult intussusception: a retrospective review. World J Surg. 2015;39:134–138. doi:10.1007/s00268-014-2759-9.
11. Marsicovetere P, Ivatury SJ, White B, Holubar SD. Intestinal intussusception: etiology, diagnosis, and treatment. Clin Colon Rectal Surg. 2017;30:30–39. doi:10.1055/s-0036-1593429.
12. AlSamman MA, Ferreira JD, Moustafa A, Moveson J, Akerman P. Successful endoscopic reduction of an ileocolonic intussusception in an adult with peutz-jeghers syndrome. Gastroenterol Res. 2019;12:40–42. doi:10.14740/gr1130.
13. Chang -C-C, Chen -Y-Y, Chen Y-F, Lin C-N, Yen -H-H, Lou H-Y. Adult intussusception in Asians: clinical presentations, diagnosis, and treatment. J Gastroenterol Hepatol. 2007;22:1767–1771. doi:10.1111/j.1440-1746.2007.04907.x
14. Cakir M, Tekin A, Kucukkartallar T, Belviranli M, Gundes E, Paksoy Y. Intussusception: as the cause of mechanical bowel obstruction in adults. Korean J Gastroenterol. 2013;61:17–21. doi:10.4166/kjg.2013.61.1.17
15. Knight AM, Haurani C, Hollenbeck A, Greene F, Mostafa G. Intussusception in the adult population: a challenge to surgeons. Am Surg. 2017;83:e131–e3. doi:10.1177/000313481708300410
16. Al-Radaideh AM, Omari HZ, Bani-Hani KE. Adult intussusception: a 14-year retrospective study of clinical assessment and computed tomography diagnosis. Acta Gastroenterol Belg. 2018;81:367–372.
17. Hong KD, Kim J, Ji W, Wexner SD. Adult intussusception: a systematic review and meta-analysis. Tech Coloproctol. 2019;23:315–324. doi:10.1007/s10151-019-01980-5.
18. Siow SL, Goo ZQ, Mahendran HA, Wong CM. Laparoscopic versus open management of adult intussusception. Surg Endosc. 2019. doi:10.1007/s00464-019-07220-z.
19. Apelt N, Featherstone N, Giuliani S. Laparoscopic treatment of intussusception in children: a systematic review. J Pediatr Surg. 2013;48:1789–1793. doi:10.1016/j.jpedsurg.2013.05.024.
20. Eisen LK, Cunningham JD, Aufses AH. Intussusception in adults: institutional review. J Am Coll Surg. 1999;188:390–395. doi:10.1016/S1072-7515(98)00331-7
21. Wang N, Cui XY, Liu Y, et al. Adult intussusception: a retrospective review of 41 cases. World J Gastroenterol. 2009;15:3303–3308. doi:10.3748/wjg.15.3303.
22. Goverman J, Greenwald M, Gellman L, Gadaleta D. Antiperistaltic (retrograde) intussusception after Roux-en-Y gastric bypass. Am Surg. 2004;70:67–70.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.