Back to Journals » Drug Design, Development and Therapy » Volume 20
Mosapride versus Metoclopramide in Critically Ill Patients with Enteral Feeding Intolerance: A Randomized, Double-Blinded Comparison
Authors Mohamed Elmokadem E, Khaled Abou El Fadl D, Bassiouny AM, Hanna Samy AE, Omar El Said N ![]()
Received 19 November 2025
Accepted for publication 14 March 2026
Published 23 March 2026 Volume 2026:20 582745
DOI https://doi.org/10.2147/DDDT.S582745
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Tamer Ibrahim
Eman Mohamed Elmokadem,1,* Dina Khaled Abou El Fadl,1,* Ahmed M Bassiouny,2,3 Amir Eskander Hanna Samy,4 Nouran Omar El Said1,*
1Department of Pharmacy Practice and Clinical Pharmacy, Faculty of Pharmacy, Future University in Egypt, Cairo, Egypt; 2Department of Radiodiagnosis, Faculty of Medicine, Ain Shams University, Cairo, Egypt; 3Department of Radiology, Quantum Radiology, Sydney, Australia; 4Critical Care Department, El Matarya Teaching Hospital, Cairo, Egypt
*These authors contributed equally to this work
Correspondence: Nouran Omar El Said, Department of Pharmacy Practice and Clinical Pharmacy, Faculty of Pharmacy, Future University in Egypt, 90th Street, New Cairo, Cairo, 12311, Egypt, Tel +201006526452, Email [email protected]
Background: Enteral feeding intolerance (EFI) from delayed gastric emptying is common in critically ill patients, leading to poor outcomes. Mosapride, a selective 5-HT4 agonist, may be a safer, more effective alternative to metoclopramide, which has limited efficacy due to tachyphylaxis and adverse effects.
Objective: To compare the safety and efficacy of mosapride with metoclopramide in reducing gastric residual volume (GRV) and improving enteral nutrition delivery in intensive care unit (ICU) patients with EFI.
Methods: In this prospective, randomized, double-blind, double-dummy trial, 100 mechanically ventilated ICU patients with EFI were allocated to receive either mosapride (5 mg enterally every 8 hours plus IV placebo) or metoclopramide (10 mg intravenously every 8 hours plus enteral placebo) for 7 days. GRV was measured daily via ultrasonography. Nutritional adequacy was evaluated through daily caloric and protein intake, calculated from delivered versus prescribed enteral volume. Clinical scores; including Acute Physiology and Chronic Health Evaluation (APACHE II), Sequential Organ Failure Assessment (SOFA), and the Modified Nutrition Risk in Critically Ill (mNUTRIC), as well as ICU length of stay were assessed. Adverse events were continuously monitored using a structured reporting tool.
Results: The mosapride group demonstrated a more significant reduction in GRV from day 1 to day 7 (68.03% vs 39.87%, p< 0.001) and higher enteral volume ratio (79.52% vs 69.48%, p< 0.001). Target energy ratio was more frequently achieved in the mosapride group (86% vs 28%, p< 0.001). Improvements in SOFA and mNUTRIC scores were significant only in the mosapride group. Adverse events were comparable between groups (p=0.643). ICU length of stay was non-significantly different between the two groups (p=0.051).
Conclusion: Mosapride is more effective than metoclopramide in reducing GRV and enhancing enteral nutrition delivery in critically ill patients with EFI, with a favorable safety profile. These findings support its consideration as a prokinetic agent in this population.
Clinical Trial Registration: NCT06826443.
Keywords: mosapride, enteral feeding intolerance, gastric residual volume, critically ill patients, prokinetic agents, metoclopramide, gastric emptying
Introduction
Critical illness is frequently associated with catabolic stress, which considerably intensifies the risk of infection, organ failure, and mortality. Malnutrition is predominantly prevalent among intensive care unit (ICU) patients, with rates reported between 38% and 78%.1,2 This results from the interplay of critical illness-induced hypermetabolism and catabolism, pre-existing nutritional deficits, and barriers to adequate feeding such as sedation, mechanical ventilation, and gastrointestinal intolerance. Together, these factors explain the high prevalence of ICU malnutrition and its association with increased mortality, prolonged ventilation, and poor outcomes.3
Early nutrition support therapy, mostly through the enteral route, is a fundamental intervention required for all critically ill patients. It is considered a proactive therapeutic approach because timely initiation of enteral nutrition has been shown to lessen disease severity, reduce complications, and positively influence patient outcomes.4,5 However, impaired gastrointestinal motility, common in critically ill patients due to various factors including mechanical ventilation, medications, renal dysfunction, hyperglycemia, or the systemic effects of critical illness, results in delayed gastric emptying.6 Consequently, nutritional targets are often not attained with enteral feeding, where more than 30% of critically ill patients exhibit intolerance to enteral feeding.7–9 These patients also have more prolonged stays in the ICU and a greater rate of mortality than the tolerant group.10
Enteral feeding intolerance (EFI) is defined as the inability to provide sufficient enteral nutrition because of delayed gastric emptying in the absence of mechanical blockage and high gastric residual volume (GRV) is its most prevalent indicator.11 It has been demonstrated that elevated GRV foretells delayed gastric emptying and a less favorable outcome in the ICU.12
Given the complications associated with parenteral nutrition and post-pyloric feeding in patients with delayed gastric emptying and a high GRV, prokinetic drugs are presently thought to be the first-line treatment for EFI, where they can reduce feed intolerance by 17.3%.6,13,14
Metoclopramide is a prokinetic and antiemetic drug that is often used as the first line of therapy for EFI. It has both central and peripheral effects and mostly functions as a dopamine antagonist.15 However, current research has only demonstrated a mild prokinetic impact of metoclopramide, which is constrained by the quick onset of tachyphylaxis.16 Additionally, its safety profile is linked to QT prolongation and adverse drug effects (ADEs) in the central nervous system (CNS).17 As a result, another prokinetic drug with comparable or superior efficacy, more desirable tolerability profile, and decreased risk of adverse effects is being sought for.
A selective 5-HT4 receptor agonist, mosapride, has been shown to stimulate gastric and colonic motility, where it was initially used to treat disorders of the upper gastrointestinal system, including nausea, vomiting, gastroesophageal reflux disease, and functional dyspepsia.18–22 Mosapride has shown more consistent improvement in gastric emptying and gastrointestinal motility, with a better safety profile and no significant QTc effects in non-ICU and perioperative studies. Only minor symptoms such as headache, dry mouth, and diarrhea are reported as ADEs.23,24 Recent studies suggest that by enhancing gastric emptying and gastric motility, mosapride may be useful in treating several motility complications.21,22,25–27 However, no randomized, double-blind trials have compared mosapride with metoclopramide specifically in critically ill ICU patients with EFI.
Thus, to explore the impact of mosapide on delayed gastric emptying, this study aims to evaluate its safety and effectiveness compared to metoclopramide in reducing GRV in critically ill patients who are receiving enteral nutrition and experiencing EFI. The findings provide evidence on efficacy, safety, and nutritional outcomes, with the potential to inform clinical guidelines, improve enteral nutrition delivery, and ultimately enhance patient prognosis in the ICU.
Patients and Methods
Study Design and Setting
This was a prospective, randomized, double-blind, parallel-group clinical trial conducted in the adult ICU of Almatareya Teaching Hospital, Cairo, Egypt. The study protocol was approved by the General Organization for Teaching Hospitals and Institutes (GOTHI) (approval no. HM000185) and registered at ClinicalTrials.gov (Identifier: NCT06826443). All procedures adhered to the principles of the Declaration of Helsinki. Written informed consent was obtained from patients’ legally authorized representatives prior to enrollment.
Study Population and Patient Enrollment
Patients presenting to the ICU between February 2025 and April 2025 expected to remain for at least 7 days, were assessed for eligibility. All enrolled patients were followed up for the full study duration. Eligibility criteria were predefined to ensure a homogeneous study population and are summarized below.
Inclusion Criteria
Patients were eligible for inclusion if they were aged between 18 and 65 years of either sex, mechanically ventilated, and receiving enteral nutrition via a nasogastric tube in the ICU. Enteral feeding intolerance was defined as a gastric residual volume ≥250 mL on two consecutive assessments during routine GRV monitoring performed multiple times daily, or the presence of clinical manifestations such as vomiting, regurgitation, abdominal distension, or diarrhea. A modified Nutrition Risk in Critically Ill (mNUTRIC) score of ≥5 was also required for inclusion.
Exclusion Criteria
Patients were excluded if they had known hypersensitivity to mosapride or metoclopramide, had received any prokinetic agent within 48 hours prior to enrollment, or had a history of gastric or major abdominal surgery. Additional exclusion criteria included suspected or confirmed gastrointestinal obstruction, perforation, or bleeding; severe hepatic or renal impairment; pregnancy; morbid obesity (BMI >40 kg/m2); significant cardiac arrhythmia or prolonged QTc interval; acute neurological injury or central nervous system infection; or anticipated extubation within 48 hours.
Eligible patients meeting the inclusion criteria and without any exclusion criteria were enrolled in the study. The ICU is a high-volume tertiary referral center with a diverse case mix, allowing continuous patient screening and enrollment throughout the study period.
Randomization and Blinding
Eligible patients were randomized in a 1:1 ratio to receive either mosapride or metoclopramide using a computer-generated random number sequence. Allocation concealment was ensured through sequentially numbered, sealed, opaque envelopes prepared and opened by an independent pharmacist who was not involved in patient care, outcome assessment, or data analysis.
The study followed a double-blind design; patients, treating physicians, nursing staff, radiologists performing ultrasonographic gastric residual volume assessments, and investigators involved in data collection and analysis were all blinded to treatment allocation.
Interventions
To maintain blinding despite the different routes of administration, a double-dummy design was employed. Patients in the mosapride group received enteral mosapride plus an intravenous placebo (normal saline), while patients in the metoclopramide group received intravenous metoclopramide plus an enteral identical-looking placebo. All enteral and intravenous preparations were identical in appearance, volume, and labeling, and were prepared by a pharmacist not involved in patient care or outcome assessment.
Mosapride Group
Patients randomized to the mosapride group received mosapride citrate 5 mg administered enterally every 8 hours, along with an intravenous infusion of normal saline matched in volume and rate to the metoclopramide infusion. This dosing regimen was selected based on established clinical use and prior studies demonstrating effective stimulation of gastric motility with an acceptable safety profile.24,28 The every-8-hour schedule was chosen to maintain sustained prokinetic activity throughout the day, consistent with the drug’s pharmacodynamic profile.
Metoclopramide Group
Patients assigned to the metoclopramide group received metoclopramide hydrochloride 10 mg intravenously every 8 hours, along with an enteral placebo identical in appearance to the mosapride preparation. This reflects the standard dosing regimen commonly used for the management of enteral feeding intolerance in critically ill patients.16,29,30 The dosing frequency was selected to ensure a continuous prokinetic effect while minimizing the risk of dose-related adverse events. Intravenous administration was used to reflect routine clinical practice in the ICU and to avoid variability in gastrointestinal absorption, thereby ensuring reliable systemic exposure in the comparator group.
For both groups, study medications were administered at least 30 minutes prior to the scheduled gastric residual volume (GRV) assessment to allow sufficient time for pharmacologic activity. Both treatments were continued for 7 consecutive days in addition to standard ICU supportive care.
Enteral Nutrition Protocol
Enteral nutrition was delivered as a continuous infusion using an enteral feeding pump. Feeding was initiated at a rate of 20 mL/h and progressively advanced by 20 mL/h every 8–12 hours as tolerated until the calculated nutritional targets were achieved. Nutritional targets were set at 25 kcal/kg/day and 1.4 g protein/kg/day based on actual body weight.4,31,32
All patients received the same standard polymeric enteral formula with a caloric density of 1.5 kcal/mL (Fresubin®, Fresenius Kabi, Egypt). This formula was selected to allow adequate caloric delivery within moderate fluid volumes, which is common practice in mechanically ventilated ICU patients who often require optimization of fluid balance. The use of a uniform enteral formula and identical advancement protocol in both study groups ensured that any potential effect of formula concentration on feeding tolerance was equally distributed and did not bias the comparative analysis.
Patients were maintained in a semi-recumbent position with head-of-bed elevation at 30–35° throughout enteral feeding to reduce the risk of aspiration. Feeding intolerance was assessed dynamically based on predefined clinical and ultrasonographic criteria rather than prescribed feeding volume alone. Enteral feeding was temporarily interrupted if patients developed persistent feeding intolerance, defined as a gastric residual volume ≥250 mL on two consecutive daily ultrasonographic assessments, or ongoing gastrointestinal symptoms despite minimal feeding rates.
Study Procedures
All clinical, laboratory, nutritional, and ultrasonographic data were prospectively collected using standardized case report forms. Data entry and verification were independently performed by two investigators to ensure accuracy. Outcome assessments were conducted according to a predefined schedule, and all analyses were performed on the full randomized study population.
At baseline, demographic and clinical characteristics (age, sex, body mass index, cause of ICU admission), comorbidities, and concomitant medications were recorded. Disease severity was assessed using the Acute Physiology and Chronic Health Evaluation II (APACHE II), Sequential Organ Failure Assessment (SOFA), and modified Nutrition Risk in Critically Ill (mNUTRIC) scores at baseline and repeated on day 7.31,32
Laboratory investigations included complete blood count, renal and liver function tests, electrolytes, fasting blood glucose, and lipid profile. A standard 12-lead electrocardiogram was performed at baseline and repeated on day 7 to assess the corrected QT (QTc) interval.
Gastric Residual Volume (GRV)
Gastric residual volume (GRV) was assessed once daily from day 1 to day 7 by a blinded assessor using a GE LOGIQ E9 ultrasound system. Measurements were performed 30 minutes after the scheduled morning assessment time while enteral feeding was ongoing via continuous infusion pump, with patients positioned in the right lateral decubitus position.33
The cross-sectional area (CSA) of the gastric antrum was measured, and GRV was estimated using a validated ultrasonographic formula:
GRV (mL) = 27 + 14.6 × right-lateral CSA − 1.28 × age.34
During continuous enteral nutrition, gastric volume reflects a dynamic steady-state balance between infusion input and gastric emptying output rather than a postprandial state.35,36 Therefore, measurement at any standardized timepoint during continuous feeding validly represents ongoing gastric emptying dynamics, consistent with studies performing ultrasound GRV assessment during uninterrupted continuous EN in mechanically ventilated patients37–39 Notably, no circadian variation was demonstrated in GRV between morning and evening assessments, supporting once-daily measurement validity.37 Ultrasonographic antral evaluation has been validated in both fasting and fed conditions as a reliable, noninvasive method that does not require feeding interruption.
To reduce interobserver variability, all ultrasound assessments were performed by trained radiologists blinded to treatment allocation, following a standardized measurement protocol with uniform patient positioning. Ultrasound-based GRV estimation reduces subjectivity associated with syringe aspiration and avoids technical limitations such as volume loss or feeding tube collapse. The validated Perlas formula was applied, as it has demonstrated good correlation with actual gastric volume across different patient positions.34 Patient positioning and timing relative to feeding were standardized for all assessments to ensure consistency throughout the study period.
Although current clinical guidelines do not recommend routine GRV monitoring for aspiration prevention, GRV remains a widely used surrogate marker of delayed gastric emptying in clinical trials evaluating prokinetic agents.12,40 In the present study, GRV was employed as a mechanistic endpoint to assess changes in gastric emptying dynamics rather than as a trigger for routine feeding interruption.
Nutritional Adequacy
Daily caloric and protein intake were recorded for each patient. The enteral nutrition volume ratio (EN VR %) was calculated as the ratio of the actual volume of enteral nutrition delivered to the prescribed target volume, expressed as a percentage.
Safety Monitoring
Adverse events were prospectively monitored and recorded using a structured adverse event reporting form specifically developed for this study. The form was designed based on the known safety profiles of prokinetic agents and the commonly reported gastrointestinal and neurological adverse effects in critically ill patients. It included predefined categories such as gastrointestinal symptoms (abdominal distension, diarrhea, constipation), neurological symptoms (headache, dizziness, delirium), cardiovascular events (QT prolongation, arrhythmias), and any other unexpected clinical events. Bedside physicians examined patients daily and completed the form accordingly. All reported adverse events were subsequently reviewed by the investigators to ensure accuracy and consistency. All materials, medications, and equipment used in the study were commercially available and are specified to allow independent replication.
Outcomes
Primary Outcome
Change in average daily GRV from day 1 to day 7, expressed as both absolute and percentage reduction.
Secondary Outcomes
Secondary outcomes included measures of enteral feeding tolerance and nutritional adequacy, such as enteral nutrition volume ratio, daily caloric and protein intake, and the proportion of patients achieving at least 80% of their target energy requirements by day 7. Changes in clinical severity scores (APACHE II, SOFA, and mNUTRIC) from baseline to day 7 were also evaluated. Additional secondary outcomes included the incidence of adverse events, QTc interval changes, and length of ICU stay.
Sample Size and Statistical Analysis
The required sample size was calculated using G*Power 3.1.14 software, assuming a medium effect size of 0.6 for the difference in gastric residual volume (GRV) between mosapride and metoclopramide, with α = 0.05 and 80% power for a two-tailed t-test. This yielded 45 patients per group. Accounting for a 10% dropout rate, the final sample size was 50 patients per group (total 100).
Data were analyzed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA). Normality was assessed with Kolmogorov–Smirnov and Shapiro–Wilk tests. Continuous variables were expressed as mean ± SD or median (IQR), and categorical variables as counts and percentages. Between-group comparisons used Student’s t-test or Mann–Whitney U-test, and Chi-square or Fisher’s exact test for categorical variables. Within-group comparisons used paired t-test or Wilcoxon signed-rank test. Multivariate linear regression (backward stepwise) identified predictors of GRV reduction, adjusting for baseline differences. A p-value < 0.05 was considered significant.
Potential confounders influencing gastrointestinal motility and nutritional tolerance were considered, including baseline disease severity (APACHE II, SOFA, mNUTRIC), concomitant medications, vasopressor use, and comorbidities. Randomization was expected to distribute measured and unmeasured confounders evenly, and multivariable regression further adjusted for clinically relevant variables, ensuring robust evaluation of factors associated with GRV reduction.
Results
Of 142 patients assessed for eligibility, 100 met the inclusion criteria and were randomized: 50 to the mosapride group and 50 to the metoclopramide group. The study included 63 males and 37 females. All randomized patients completed follow-up with no dropouts (Figure 1).
 |
Figure 1 CONSORT flowchart. |
Baseline Characteristics and Laboratory Parameters
As presented in Table 1, the studied groups were comparable in terms of age, gender, and BMI. The most commonly reported reason for ICU admission was surgical intervention, followed by trauma, with no statistically significant difference between the two groups. The only comorbidity reported among patients was hypertension (34% of the mosapride group and 30% of the metoclopramide group), with no difference. No statistically significant differences were recorded in terms of concomitant medications or observed in baseline biochemical laboratory parameters between the mosapride and metoclopramide groups.
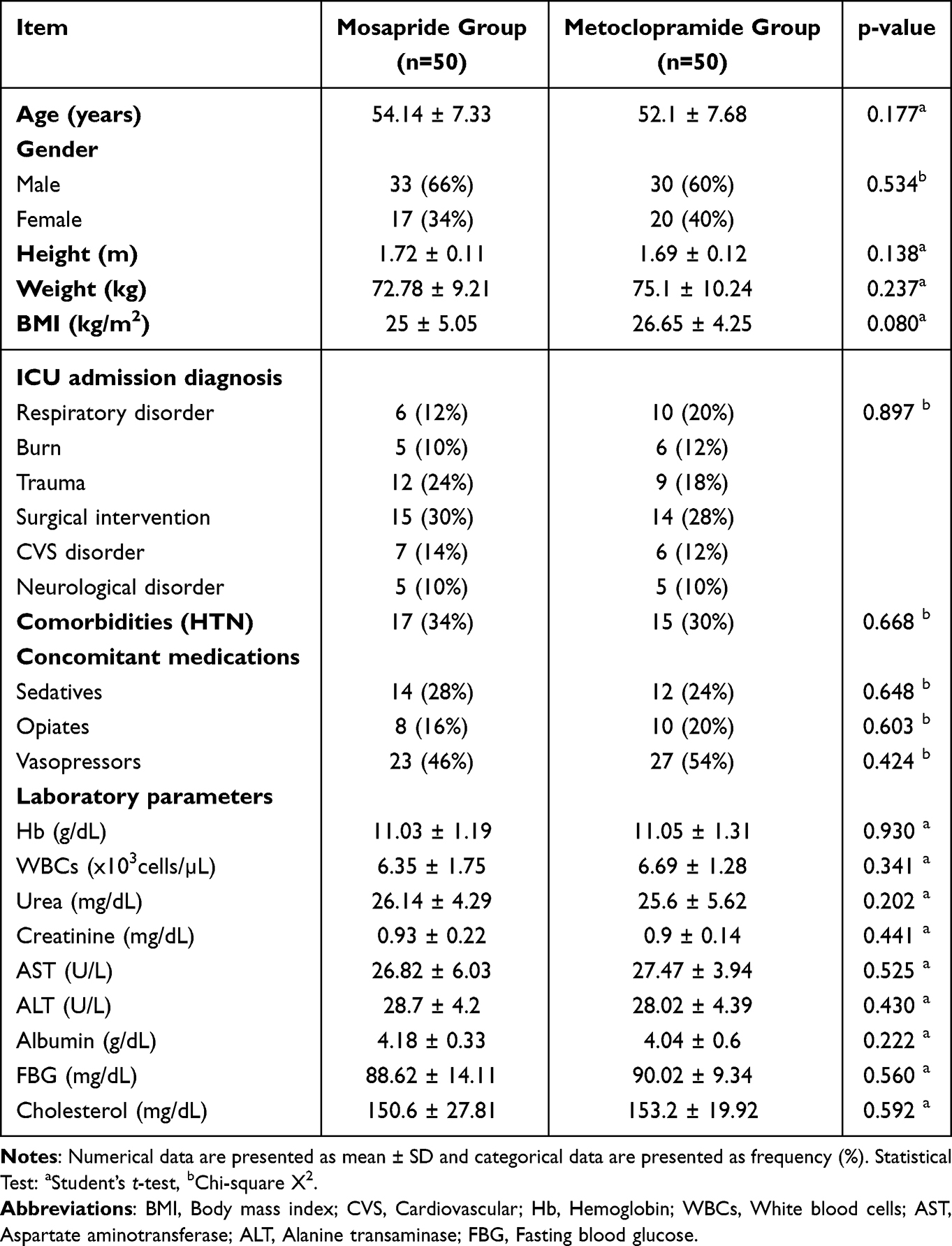 |
Table 1 Characteristics and Laboratory Parameters at Baseline |
Gastric Residual Volume and Enteral Volume Ratio
The primary outcome, gastric residual volume was significantly higher in the mosapride group at day 1 (380.2 ± 51.06 vs 351 ± 68.74 mL, p=0.018) and day 3 (370.94 ± 58.04 vs 274.18 ± 59.05 mL, p<0.001). However, mosapride showed significantly lower GRV from day 5 (171.7 ± 44.65 vs 215.94 ± 39.08 mL, p<0.001), day 6 (146.7 ± 31.6 vs 211.24 ± 52.52 mL, p<0.001), and day 7 (120.02 ± 50.56 vs 203.38 ± 31.66, p<0.001), indicating superior feed tolerance. Weekly GRV reduction was greater with mosapride (260.18 ± 67.29 vs 147.61 ± 74.23 mL, p<0.001), representing a mean percentage drop of 68.03 ± 13.21% vs 39.87 ± 15.66%. At day 7, mosapride achieved higher mean administered volume (954.2 ± 119.1 vs 833.8 ± 123.83 mL, p<0.001) and EN VR% (79.52 ± 9.92 vs 69.48 ± 10.32%, p<0.001) (Table 2, Figures 2 and 3).
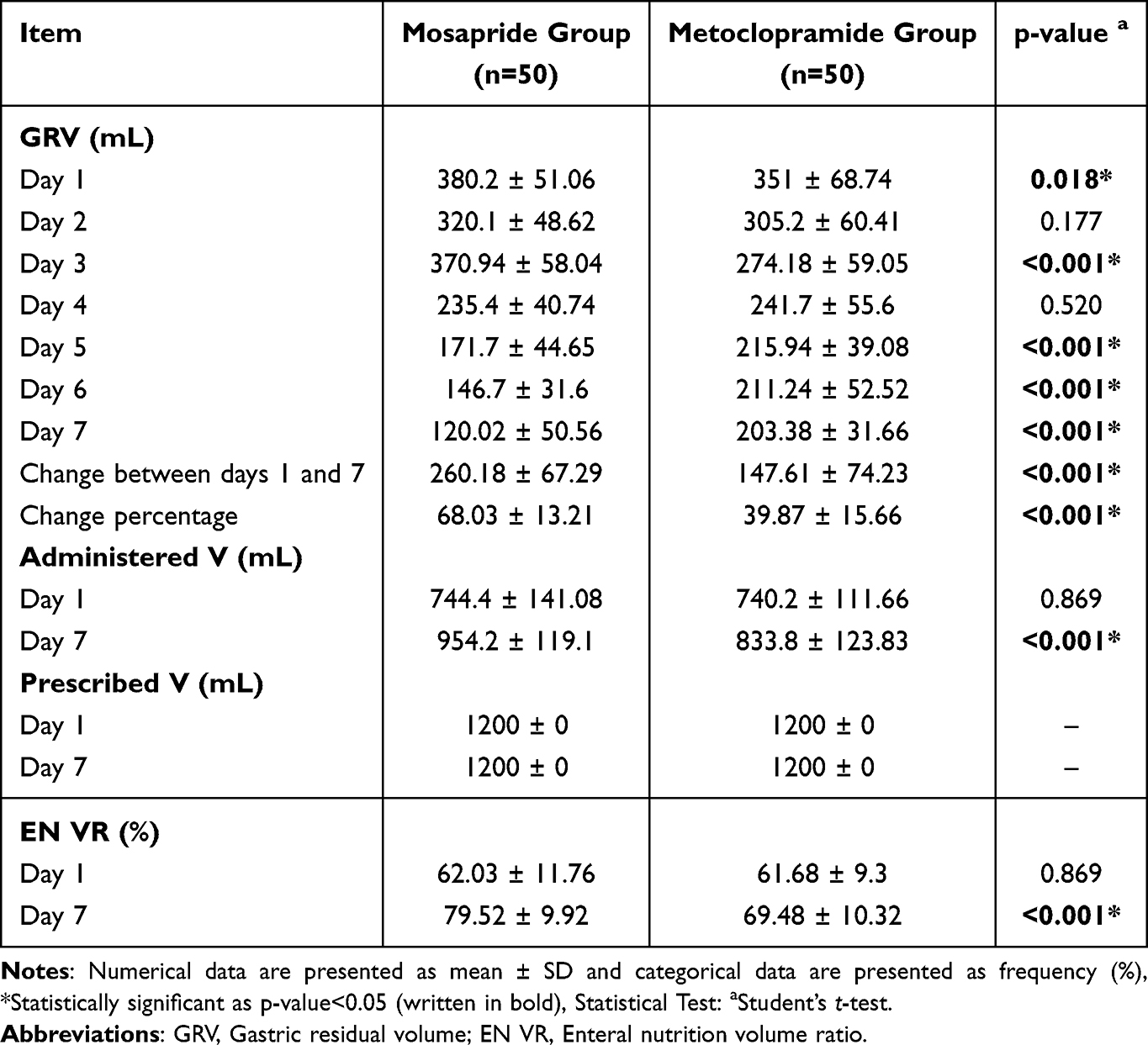 |
Table 2 GRV, Administered and Prescribed Volumes and EN VR of the Studied Groups |
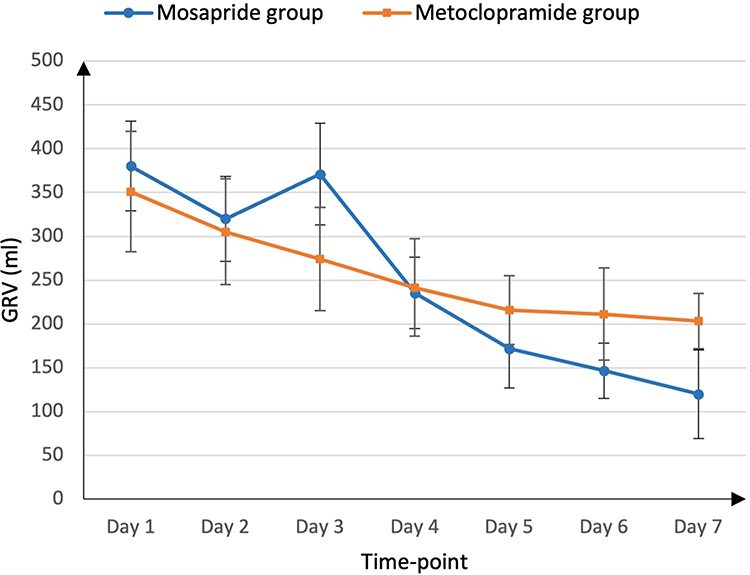 |
Figure 2 Gastric residual volume levels of the studied groups. GRV, gastric residual volume. |
 |
Figure 3 Nutritional outcomes comparing the mosapride and metoclopramide groups. (A) Average daily caloric intake over 7 days and achieved calories at day 7 in the mosapride versus metoclopramide groups. (B) Energy ratio percentage at day 7, comparing both treatment groups. (C) Proportion of patients achieving target energy ratio (>80%) in the mosapride versus metoclopramide groups. (D) Average protein ratio percentage at day 7 in the studied groups. |
Risk Scores
Both groups showed improvements in clinical severity and nutritional risk scores over the seven-day study period. APACHE II, SOFA, and mNUTRIC scores decreased in both groups, with statistically significant between-group differences favoring mosapride at day 7 (Table 3).
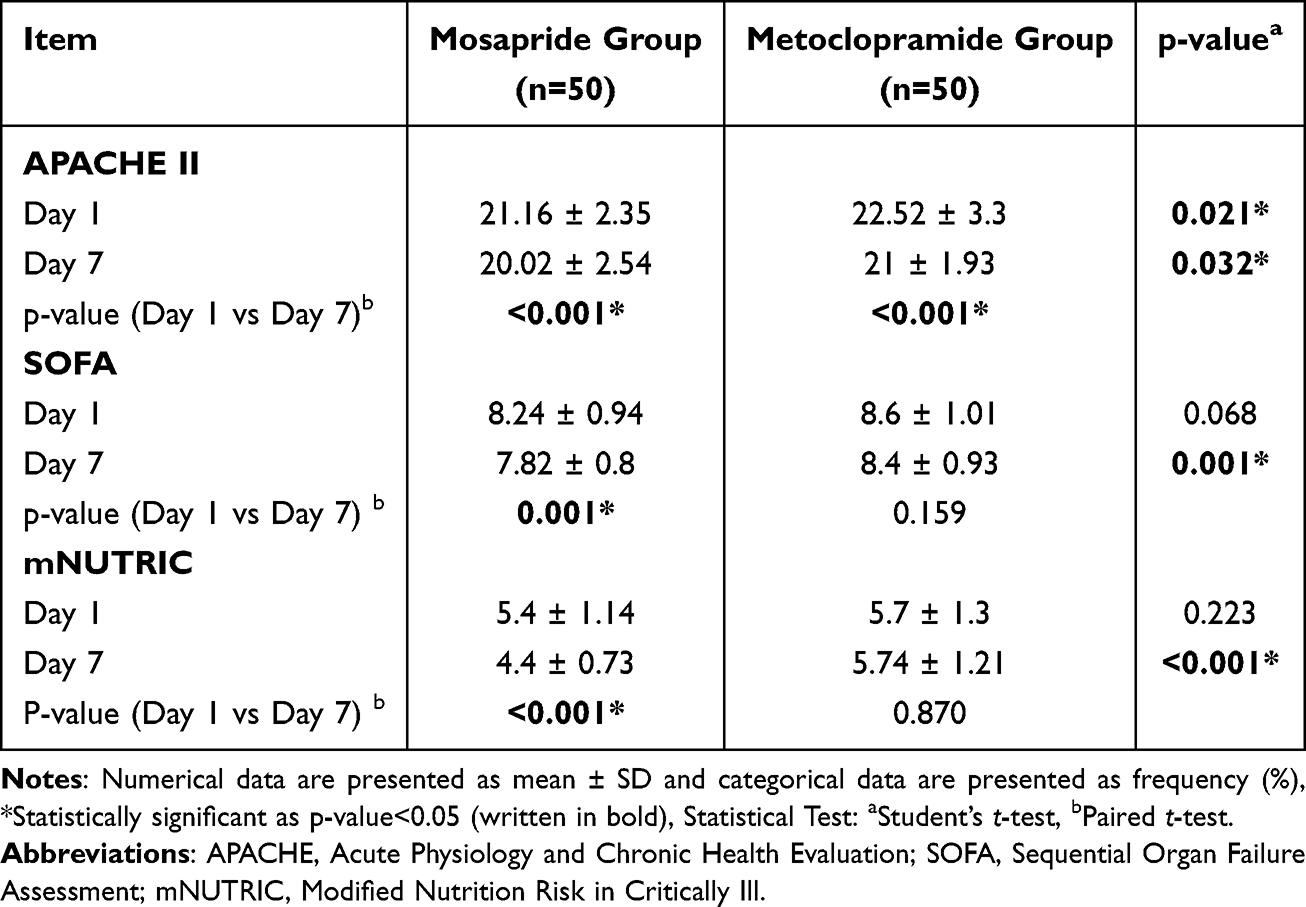 |
Table 3 Risk Scores of the Studied Groups |
Nutritional Adequacy
The mosapride group demonstrated significantly higher average daily calories over 7 days (1522 ± 209.02 vs 1389.1 ± 118.5), achieved calories (1600.2 ± 198.11 vs 1370.6 ± 168.36), energy ratio % (88.62 ± 10.01 vs 74.47 ± 14.39), and protein ratio % (81.69 ± 13.35 vs 75.69 ± 13.07) compared to metoclopramide (all P<0.05). Additionally, more mosapride patients achieved target energy ratio >80% (86% vs 28%, P<0.001) (Table 4 and Figure 3).
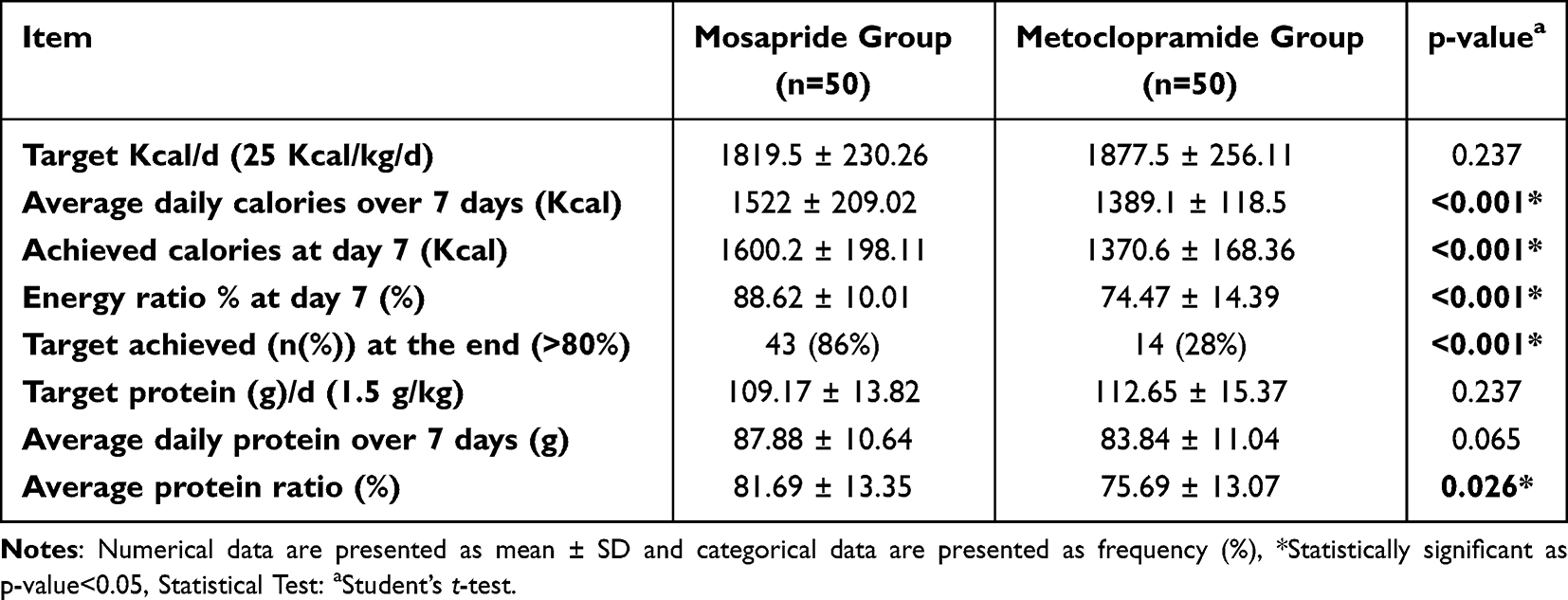 |
Table 4 Nutritional Parameters of the Studied Groups |
Safety Outcomes
Adverse events occurred in 24% of the mosapride group and 30% of the metoclopramide group (p=0.643). The most common adverse events were abdominal distension (10% vs 14%) and diarrhea (8% vs 6%). Less frequent events included headache (2% vs 4%), constipation (4% vs 0%), delirium (0% vs 2%), dizziness (0% vs 2%), and QT prolongation (0% vs 2%). No significant difference in adverse event rates was observed between groups. At Day 7, AST levels were similar between the mosapride and metoclopramide groups (26.12 ± 5.00 vs 26.20 ± 4.02 U/L, p=0.930), as were ALT levels (27.24 ± 5.37 vs 27.52 ± 3.36 U/L, p=0.755). Changes from baseline were also comparable for AST (−0.70 ± 4.81 vs −1.27 ± 4.40, p=0.538) and ALT (−1.46 ± 5.95 vs −0.50 ± 4.29, p=0.357), indicating no differential effect on liver function.
ICU Length of Stay
ICU length of stay was non-significantly different between patients receiving mosapride and those receiving metoclopramide (p=0.051), with a mean of 8.88 ± 1.57 vs 9.2 ± 1.92 days of ICU stay.
Linear Regression Analysis
In univariate analysis, mosapride significantly increased GRV reduction percentage versus metoclopramide (Coefficient=28.16, 95% CI: 22.41–33.91, p<0.001). Each 1-unit increase in age (Coefficient=0.53, 95% CI: 0.01–1.06, p=0.047), achieved calories at day 7 (Coefficient=0.04, 95% CI: 0.02–0.06, p<0.001), and EN VR% (Coefficient=0.67, 95% CI: 0.34–1, p<0.001) significantly increased GRV reduction percentage. Baseline SOFA score inversely affected GRV reduction (Coefficient=−4.19, 95% CI: −8.21 to −0.18, p=0.041). Achieving an energy ratio target >80% significantly increased GRV reduction (Coefficient=17.18, 95% CI: 9.81–24.55, p<0.001). In multivariate analysis, after adjustment for the included factors, mosapride remained significantly associated with greater GRV reduction (Coefficient=21.29, 95% CI: 11.1–31.48, p<0.001) (Table 5).
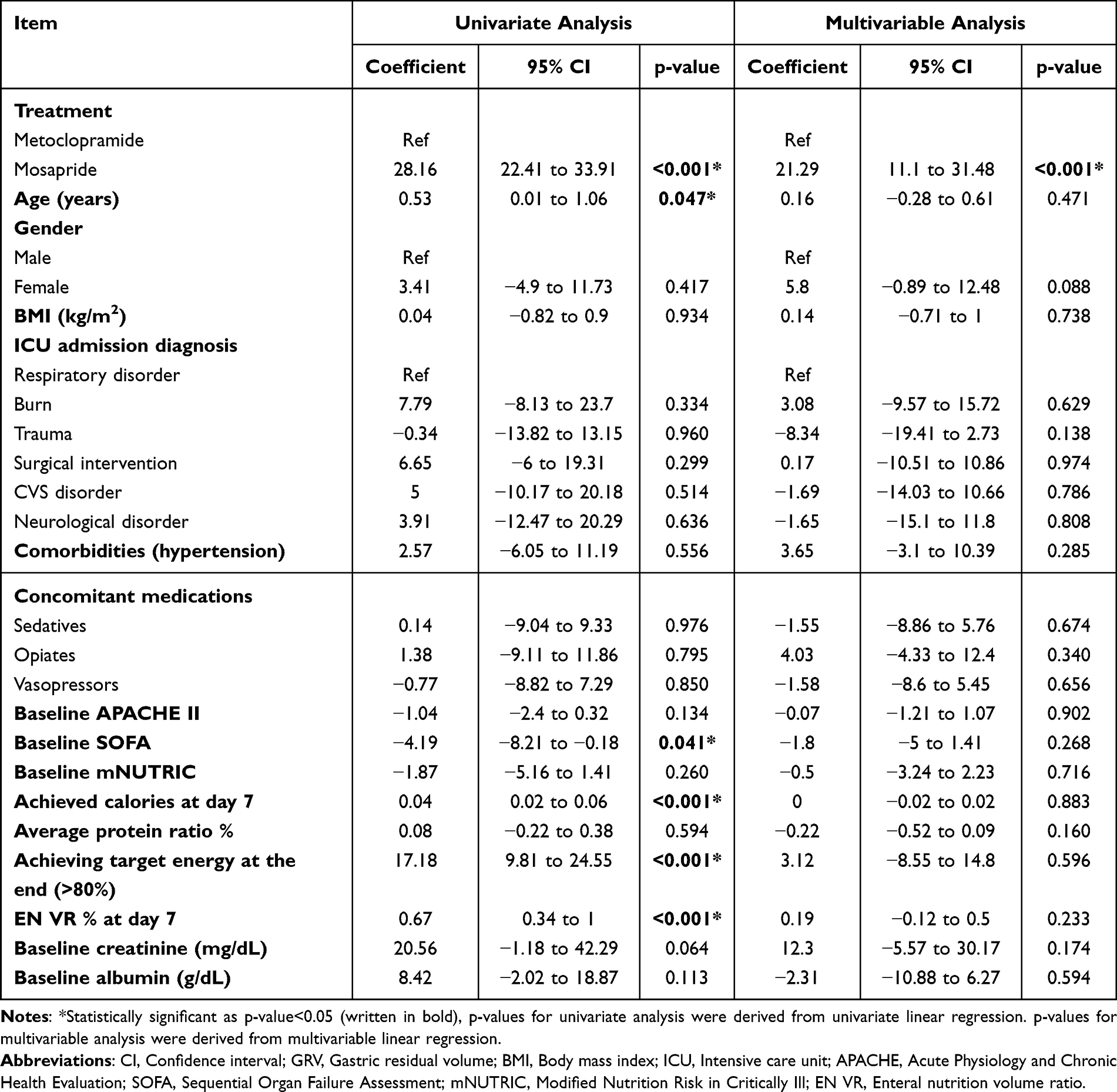 |
Table 5 Linear Regression Analysis for Factors Associated with the % of Drop in GRV |
Discussion
This randomized controlled trial demonstrated that mosapride is more effective than metoclopramide in improving gastric emptying in critically ill patients with enteral feeding intolerance. The mosapride group showed a significantly greater reduction in gastric residual volume (GRV) over seven days compared to the metoclopramide group.
Our findings are consistent with previous studies that have demonstrated mosapride’s prokinetic efficacy, although notably, all prior evidence was derived from non-critically ill populations using surrogate physiological endpoints rather than the clinically relevant GRV measure employed in the present trial. Endo et al (2002) reported that a single 10 mg dose of mosapride significantly enhanced gastric myoelectrical activity and ultrasonographic gastric emptying in 20 healthy volunteers.21 Similarly, Kusunoki et al (2010) demonstrated that mosapride 15 mg twice daily for 14 days significantly improved proximal gastric accommodation, gastric emptying rate, and antral contraction frequency compared to placebo in 14 healthy volunteers using ultrasonography.22 Jung et al (2010) confirmed dose-dependent gastric emptying enhancement in 15 healthy volunteers, with the 10 mg dose showing significant improvement on endoscopic and radiopaque marker assessments, whereas the 5 mg dose was ineffective.27 Sakamoto et al (2011) further showed in a crossover study of 6 healthy male volunteers that mosapride significantly reversed high-viscosity liquid-induced delayed gastric emptying, as measured by continuous real-time 13C breath testing.26 In the only study involving a diseased population, Ueno et al (2010) demonstrated that mosapride significantly increased bowel frequency in 32 diabetic patients with constipation over 8 weeks, suggesting its prokinetic effects extend beyond the stomach even in patients with autonomic dysfunction.25 Moreover, previous studies have demonstrated mosapride’s prokinetic benefits in accelerating postoperative gastrointestinal recovery in colorectal cancer surgical patients and improving colonic preparation quality in ambulatory patients undergoing colonoscopy.41,42
However, none of these studies included critically ill patients or used GRV as an outcome measure, and none directly compared mosapride to metoclopramide. The present study, therefore, extends the existing evidence to the most challenging clinical setting, the critically ill ICU patient with enteral feeding intolerance, demonstrating for the first time that mosapride produces significantly greater GRV reduction over seven days compared to metoclopramide in this population.
Both TAK-954 and prucalopride, 5-HT4 receptor agonists, outperformed metoclopramide in improving gastric emptying in critically ill patients with a favorable safety profile.43–45 This supports the current findings with mosapride, which works through the same mechanism, suggesting that this drug class effectively treats feeding intolerance in critical care. Furthermore, this adds to the growing evidence that 5-HT4 receptor activation may be a potential approach for managing feeding intolerance in critical care.6,14,43,45
The pattern of GRV reduction in the mosapride group is noteworthy. Despite initially higher GRV levels on days 1 and 3, the mosapride group demonstrated a more significant and consistent decline in GRV from day 4 onward, finally reaching significantly lower levels than the metoclopramide group by day 7. This pattern suggests that mosapride may have a more sustained prokinetic effect without the tachyphylaxis that has been reported with metoclopramide.17 Similar patterns were observed with prucalopride administration, supporting that this medication class does not suffer from the tachyphylaxis phenomenon shown with metoclopramide.45 The delayed but more pronounced effect of mosapride could be attributed to its selective 5-HT4 receptor agonist mechanism, which may require time to enhance gastric and colonic motility fully.19,21
This superior reduction in GRV translated into improved nutritional outcomes, with the mosapride group achieving significantly higher average daily calories, energy ratio, and enteral nutrition volume ratio by day 7. Furthermore, 86% of patients in the mosapride group achieved the target energy ratio (>80%) compared to only 28% in the metoclopramide group (p<0.001).
The improved gastrointestinal motility and enteral feeding outcomes observed with mosapride appear to have translated into clinical benefits. The mosapride group showed significant improvements in SOFA and mNUTRIC scores from day 1 to day 7, while the metoclopramide group did not demonstrate significant changes in these scores. This finding suggests that improved nutritional status may contribute to better organ function and reduced severity of illness, aligning with previous studies highlighting the importance of adequate enteral nutrition in critically ill patients.4,5,46
The observed differences are clinically meaningful, as the greater GRV reduction with mosapride translated into a markedly higher proportion of patients achieving a target energy ratio >80% and significant improvements in SOFA and mNUTRIC scores. In critically ill patients, even modest improvements in meeting nutritional targets are associated with reduced infectious complications, shorter mechanical ventilation duration, and improved outcomes.47
Linear regression analysis confirmed that mosapride treatment was independently associated with a higher percentage decrease in GRV after adjusting for potential confounding factors. Interestingly, baseline SOFA scores were negatively associated with GRV reduction in univariate analysis, suggesting that disease severity and organ dysfunction may impact gastrointestinal motility and response to prokinetic therapy. This finding highlights the correlation between critical illness, inflammatory responses, and gastrointestinal function.48–51
Our analysis also revealed a significant association between nutritional intake and GRV reduction. Patients who reached the target energy ratio (>80%) showed a substantially greater decrease in GRV compared to those who did not. Both higher caloric intake at day seven and higher enteral nutrition volume ratios were associated with more significant GRV reductions (p<0.001). These results point to the strong relationship between gastric emptying and nutritional status. As GRV decreases, gastrointestinal motility improves, which subsequently enhances nutritional delivery.
This relationship highlights the importance of initiating effective prokinetic therapy, such as mosapride, early in critically ill patients with feeding intolerance to optimize nutritional outcomes.14
The observed trend toward shorter ICU length of stay in the mosapride group suggests potential benefits, although this difference did not reach statistical significance. Similarly, other prokinetics failed to significantly reduce ICU length of stay, despite demonstrating superiority in reducing gastric residual volumes and improving nutritional outcomes.6,45,52
The safety profile of mosapride was comparable to that of metoclopramide, with no significant differences in adverse effects between the two groups. Most patients (76% in the mosapride group and 70% in the metoclopramide group) experienced no adverse effects. The most common adverse effects in both groups were abdominal distension and diarrhea, which are expected with prokinetic agents and enteral feeding. Importantly, no patients in the mosapride group experienced delirium, dizziness, or QT prolongation, which were reported in the metoclopramide group, albeit in small numbers. This finding aligns with previous studies reporting mosapride’s favorable safety profile without CNS effects or QT anomalies.23,24,53
As a selective 5-HT4 receptor agonist, mosapride’s effect is limited to the peripheral nervous system, which minimizes central nervous system (CNS) penetration and related adverse effects. This contributes to its favorable safety profile, with minimal reports of extrapyramidal symptoms or QT interval prolongation.54–56
Conversely, dopaminergic blockade by metoclopramide can bring about CNS-related adverse effects, including sedation, dystonia, and tardive dyskinesia, especially with prolonged use.57 Metoclopramide has also been associated with QT prolongation and cardiac arrhythmias, necessitating ECG monitoring in vulnerable populations.58
Better feeding tolerance and nutritional adequacy with mosapride, reflected in higher EN VR%, caloric intake, and protein ratios, may reduce infections, pressure ulcers, and delayed recovery, all of which drive ICU costs. Mosapride’s safer profile, with fewer CNS and cardiac side effects, could also decrease monitoring needs and interventions.54 While these findings suggest mosapride offers pharmacoeconomic benefits in critically ill patients, direct cost comparisons with metoclopramide, including drug costs, monitoring requirements, and clinical outcomes, remain unexplored.
The superior efficacy of mosapride over metoclopramide in reducing GRV and improving nutritional parameters suggests that mosapride could be considered an alternative prokinetic agent for EFI in critically ill patients, particularly in those who fail to respond to or experience adverse effects with metoclopramide.
Strengths and Limitations
This study has several strengths, including its randomized design with blinded outcome assessment, daily standardized ultrasound-based measurement of gastric residual volume (GRV), and being the first head-to-head comparison of mosapride and metoclopramide in critically ill patients with enteral feeding intolerance (EFI). These methodological features enhance the internal validity of the findings and support the robustness of the observed effects.
Several limitations should be acknowledged. First, the single-center design may limit generalizability, and the relatively modest sample size restricts the ability to detect differences in hard clinical outcomes such as ICU length of stay, infection rates, or mortality. Second, the seven-day intervention period may not fully capture long-term outcomes or the sustained effects of mosapride beyond the acute phase of critical illness. Third, GRV was used as the primary indicator of feeding intolerance; although this allows comparison with prior prokinetic trials and enables objective assessment using a validated ultrasound-based technique, additional measures such as gastrointestinal symptom scores, gastric emptying scintigraphy, or intestinal motility assessments could provide complementary insights.12,40
Moreover, GRV was assessed once daily rather than at multiple timepoints. While more frequent measurements might provide additional data, our standardized approach minimizes disruption and is consistent with published studies using ultrasound GRV during continuous EN.37,38 Jahreis et al found no circadian GRV variation during continuous feeding, supporting single daily assessment validity.
Additionally, mosapride was administered enterally, which may result in delayed absorption in patients with gastroparesis. However, mosapride reaches steady-state by day 2, exerts local prokinetic effects via gastric wall 5-HT4 receptor binding before systemic absorption, and accumulates in gastric tissue at concentrations exceeding plasma levels.59,60 Multiple ICU trials have demonstrated the efficacy of enteral prokinetics in this population.45,61 Moreover, repeated dosing and its prolonged duration of action were intended to mitigate this effect during the study period.
Third, comparison of enteral mosapride with IV metoclopramide involves different pharmacokinetic profiles. This reflects standard practice, as ESPEN recommends IV metoclopramide,30 and all major prokinetic RCTs used IV metoclopramide.11,45,61,62 The IV comparator ensures reliable drug exposure and represents a more stringent test for mosapride.
The study was not powered to evaluate clinical endpoints influenced by multiple confounding factors beyond gastrointestinal motility, and the primary focus was therefore on mechanistic outcomes related to gastric emptying and nutritional adequacy. Although patients were admitted to the ICU for heterogeneous primary diagnoses, all participants shared key characteristics relevant to the study question, including mechanical ventilation, nasogastric enteral feeding, and documented EFI.
Finally, the use of a standardized enteral nutrition protocol and uniform feeding formula minimized variability in nutritional delivery and helped isolate the effect of the prokinetic intervention on gastric emptying. This pragmatic design reflects real-world ICU practice and supports the external validity of the findings.
Future Directions
Further multicenter randomized trials with larger sample sizes are needed to confirm these findings and to determine whether mosapride’s benefits translate into improved long-term outcomes, including infection rates, ventilator-free days, and mortality. Direct comparisons of mosapride with other 5-HT4 agonists may clarify whether the observed effects represent a drug-specific or class-wide benefit. Future studies should incorporate pharmacoeconomic modeling to evaluate the cost-effectiveness of mosapride in EFI management, particularly in resource-limited settings where optimizing both clinical and economic outcomes is essential.
Conclusion
In conclusion, this single-centered randomized controlled trial found that mosapride led to greater reductions in gastric residual volume and improved caloric and protein delivery compared with metoclopramide in critically ill patients with enteral feeding intolerance. These effects remained significant after adjustment for baseline characteristics and cofounders. Adverse events were similar between groups, with no QT prolongation observed with mosapride. However, interpretation is limited by the single-center design and small sample size. No differences were seen in ICU length of stay, and the study was not powered to assess mortality or other major clinical outcomes. Larger, multicenter trials are needed to confirm these results and determine the impact of mosapride on clinically meaningful endpoints.
Clinical Trial Registration
ClinicalTrials.gov (Registration Number: NCT06826443).
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study protocol was approved by the Institutional Review Board of the General Organization for Teaching Hospitals and Institutes (GOTHI) (approval no. HM000185). All participants were informed about the study design and signed a written informed consent form.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Nouran Omar is the corresponding author, taking responsibility for the integrity of the work.
Funding
The authors received no financial support for the research and/or authorship of this article.
Disclosure
The authors declare that they have no competing interests.
References
1. Lew CCH, Yandell R, Fraser RJL, Chua AP, Chong MFF, Miller M. Association between malnutrition and clinical outcomes in the intensive care unit: a systematic review. J Parenteral Enteral Nutr. 2017;41(5):744–17. doi:10.1177/0148607115625638
2. Peng R, Li H, Yang L, et al. The efficacy and safety of prokinetics in critically ill adults receiving gastric feeding tubes: a systematic review and meta-analysis. PLoS One. 2021;16(1):e0245317. doi:10.1371/journal.pone.0245317
3. Reignier J, Rice TW, Arabi YM, Casaer M. Nutritional support in the ICU. BMJ. 2025;e077979. doi:10.1136/bmj-2023-077979
4. McClave SA, Taylor BE, Martindale RG, et al. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient. J Parenteral Enteral Nutr. 2016;40(2):159–211. doi:10.1177/0148607115621863
5. Elke G, van Zanten ARH, Lemieux M, et al. Enteral versus parenteral nutrition in critically ill patients: an updated systematic review and meta-analysis of randomized controlled trials. Crit Care. 2016;20(1):117. doi:10.1186/s13054-016-1298-1
6. Lewis K, Alqahtani Z, Mcintyre L, et al. The efficacy and safety of prokinetic agents in critically ill patients receiving enteral nutrition: a systematic review and meta-analysis of randomized trials. Crit Care. 2016;20(1):259. doi:10.1186/s13054-016-1441-z
7. Lehmann S, Ferrie S, Carey S. Nutrition management in patients with chronic gastrointestinal motility disorders: a systematic literature review. Nutr Clin Pract. 2020;35(2):219–230. doi:10.1002/ncp.10273
8. Li J, Wang L, Zhang H, et al. Different definitions of feeding intolerance and their associations with outcomes of critically ill adults receiving enteral nutrition: a systematic review and meta-analysis. J Intensive Care. 2023;11(1):29. doi:10.1186/s40560-023-00674-3
9. Eveleens RD, Joosten KFM, de Koning BAE, Hulst JM, Verbruggen SCAT. Definitions, predictors and outcomes of feeding intolerance in critically ill children: a systematic review. Clin Nutr. 2020;39(3):685–693. doi:10.1016/j.clnu.2019.03.026
10. Gungabissoon U, Hacquoil K, Bains C, et al. Prevalence, risk factors, clinical consequences, and treatment of enteral feed intolerance during critical illness. J Parenteral Enteral Nutr. 2015;39(4):441–448. doi:10.1177/0148607114526450
11. Heyland DK, van Zanten ARH, Grau-Carmona T, et al. A multicenter, randomized, double-blind study of ulimorelin and metoclopramide in the treatment of critically ill patients with enteral feeding intolerance: PROMOTE trial. Intensive Care Med. 2019;45(5):647–656. doi:10.1007/s00134-019-05593-2
12. Elke G, Felbinger TW, Heyland DK. Gastric residual volume in critically ill patients. Nutr Clin Pract. 2015;30(1):59–71. doi:10.1177/0884533614562841
13. Camilleri M, Atieh J. New developments in prokinetic therapy for gastric motility disorders. Front Pharmacol. 2021;12. doi:10.3389/fphar.2021.711500
14. Lv G, Zhang T, Wang L, et al. Prediction of prokinetic agents in critically ill patients with feeding intolerance: a prospective observational clinical study. Front Nutr. 2023;10. doi:10.3389/fnut.2023.1244517
15. Nguyen NQ. Pharmacological therapy of feed intolerance in the critically ills. World J Gastrointest Pharmacol Ther. 2014;5(3):148. doi:10.4292/wjgpt.v5.i3.148
16. Kalas MA, Trivedi B, Kalas M, Chavez LO, McCallum RW. Metoclopramide in gastroparesis: its mechanism of action and safety profile. Gastrointestinal Disord. 2023;5(3):317–328. doi:10.3390/gidisord5030026
17. van der Meer YG, Venhuizen WA, Heyland DK, van Zanten AR. Should we stop prescribing metoclopramide as a prokinetic drug in critically ill patients? Crit Care. 2014;18(5):502. doi:10.1186/s13054-014-0502-4
18. Quigley EMM. Prokinetics in the management of functional gastrointestinal disorders. Curr Gastroenterol Rep. 2017;19(10):53. doi:10.1007/s11894-017-0593-6
19. Bor S, Kalkan İH, Savarino E, et al. Prokinetics‐safety and efficacy: the European society of neurogastroenterology and motility/the American neurogastroenterology and motility society expert review. Neurogastroenterol Motil. 2024;36(5). doi:10.1111/nmo.14774
20. Maneerattanaporn M, Chang L, Chey WD. Emerging pharmacological therapies for the irritable bowel syndrome. Gastroenterol Clin North Am. 2011;40(1):223–243. doi:10.1016/j.gtc.2010.12.002
21. Endo J, Nomura M, Morishita S, et al. Influence of mosapride citrate on gastric motility and autonomic nervous function: evaluation by spectral analyses of heart rate and blood pressure variabilities, and by electrogastrography. J Gastroenterol. 2002;37(11):888–895. doi:10.1007/s005350200150
22. Kusunoki H, Haruma K, Hata J, et al. Efficacy of mosapride citrate in proximal gastric accommodation and gastrointestinal motility in healthy volunteers: a double-blind placebo-controlled ultrasonographic study. J Gastroenterol. 2010;45(12):1228–1234. doi:10.1007/s00535-010-0292-7
23. Naing LY, Heckroth M, Mathur P, Abell TL. Gastroparesis syndromes: emerging drug targets and potential therapeutic opportunities. Expert Opin Investig Drugs. 2023;32(3):245–262. doi:10.1080/13543784.2023.2186222
24. Curran MP, Robinson DM. Mosapride. Drugs. 2008;68(7):981–991. doi:10.2165/00003495-200868070-00007
25. Ueno N, Inui A, Satoh Y. The effect of mosapride citrate on constipation in patients with diabetes. Diabet Res Clin Pract. 2010;87(1):27–32. doi:10.1016/j.diabres.2009.09.024
26. Sakamoto Y, Sekino Y, Yamada E, et al. Mosapride accelerates the delayed gastric emptying of high-viscosity liquids: a crossover study using continuous real-time C breath test (BreathID system). J Neurogastroenterol Motil. 2011;17(4):395–401. doi:10.5056/jnm.2011.17.4.395
27. Jung IS, Kim JH, Lee HY, Park H, Lee SI. Endoscopic evaluation of gastric emptying and effect of mosapride citrate on gastric emptying. Yonsei Med J. 2010;51(1):33. doi:10.3349/ymj.2010.51.1.33
28. Hongo M, Harasawa S, Mine T, et al. Large‐scale randomized clinical study on functional dyspepsia treatment with mosapride or teprenone: Japan mosapride mega‐study (JMMS). J Gastroenterol Hepatol. 2012;27(1):62–68. doi:10.1111/j.1440-1746.2011.06949.x
29. Singer P, Blaser AR, Berger MM, et al. ESPEN practical and partially revised guideline: clinical nutrition in the intensive care unit. Clin Nutr. 2023;42(9):1671–1689. doi:10.1016/j.clnu.2023.07.011
30. Singer P, Blaser AR, Berger MM, et al. ESPEN guideline on clinical nutrition in the intensive care unit. Clin Nutr. 2019;38(1):48–79. doi:10.1016/j.clnu.2018.08.037
31. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13(10):818–829. doi:10.1097/00003246-198510000-00009
32. Vincent JL, de Mendonca A, Cantraine F, et al. Use of the SOFA score to assess the incidence of organ dysfunction/failure in intensive care units. Crit Care Med. 1998;26(11):1793–1800. doi:10.1097/00003246-199811000-00016
33. Kar P, Jones KL, Horowitz M, Chapman MJ, Deane AM. Measurement of gastric emptying in the critically ill. Clin Nutr. 2015;34(4):557–564. doi:10.1016/j.clnu.2014.11.003
34. Perlas A, Mitsakakis N, Liu L, et al. Validation of a mathematical model for ultrasound assessment of gastric volume by gastroscopic examination. Anesth Analg. 2013;116(2):357–363. doi:10.1213/ANE.0b013e318274fc19
35. Chowdhury AH, Murray K, Hoad CL, et al. Effects of bolus and continuous nasogastric feeding on gastric emptying, small bowel water content, superior mesenteric artery blood flow, and plasma hormone concentrations in healthy adults. Ann Surg. 2016;263(3):450–457. doi:10.1097/SLA.0000000000001110
36. Chang WK, McClave SA, Chao YC. Continuous nasogastric tube feeding: monitoring by combined use of refractometry and traditional gastric residual volumes. Clin Nutr. 2004;23(1):105–112. doi:10.1016/S0261-5614(03)00101-8
37. Jahreis T, Kretschmann J, Weidner N, Volk T, Meiser A, Groesdonk HV. Sonographic evaluation of gastric residual volume during enteral nutrition in critically ill patients using a miniaturized ultrasound device. J Clin Med. 2021;10(21):4859. doi:10.3390/jcm10214859
38. Bouvet L, Zieleskiewicz L, Loubradou E, et al. Reliability of gastric suctioning compared with ultrasound assessment of residual gastric volume: a prospective multicentre cohort study. Anaesthesia. 2020;75(3):323–330. doi:10.1111/anae.14915
39. Ceylan İ, Ekin S, Korkmaz HA. Ultrasonographic measurement of gastric volume in critically ill patients nourished with different enteral feeding protocols. Signa Vitae. 2025;21(8):37–44. doi:10.22514/sv.2025.111
40. Lew CCH, Lee Z, Day AG, Heyland DK. Correlation between gastric residual volumes and markers of gastric emptying: a post hoc analysis of a randomized clinical trial. J Parenteral Enteral Nutr. 2022;46(4):850–857. doi:10.1002/jpen.2234
41. Thampongsa T, Saengsawang B, Supsamutchai C, et al. The efficacy of mosapride on recovery of intestinal motility after elective colorectal cancer surgery: a randomized controlled trial. Ann Coloproctol. 2025;41(3):232–238. doi:10.3393/ac.2024.00892.0127
42. Tajika M. Efficacy of mosapride citrate with polyethylene glycol solution for colonoscopy preparation. World J Gastroenterol. 2012;18(20):2517. doi:10.3748/wjg.v18.i20.2517
43. Chapman MJ, Jones KL, Almansa C, Barnes CN, Nguyen D, Deane AM. Blinded, double‐dummy, parallel‐group, Phase 2a randomized clinical trial to evaluate the efficacy and safety of a highly selective 5‐hydroxytryptamine type 4 receptor agonist in critically ill patients with enteral feeding intolerance. J Parenteral Enteral Nutr. 2021;45(1):115–124. doi:10.1002/jpen.1732
44. De Maeyer JH, Lefebvre RA, Schuurkes JAJ. 5‐HT 4 receptor agonists: similar but not the same. Neurogastroenterol Motil. 2008;20(2):99–112. doi:10.1111/j.1365-2982.2007.01059.x
45. Elmokadem EM, Abou El Fadl DK, Eissa N, et al. Comparison of enteral prucalopride versus intravenous metoclopramide for feeding intolerance in patients with critical illness: a randomized double-blinded study. Front Pharmacol. 2024;15. doi:10.3389/fphar.2024.1413246
46. Adeyinka A, Rouster AS, Valentine M. Enteral Feeding. 2025.
47. Alberda C, Gramlich L, Jones N, et al. The relationship between nutritional intake and clinical outcomes in critically ill patients: results of an international multicenter observational study. Intensive Care Med. 2009;35(10):1728–1737. doi:10.1007/s00134-009-1567-4
48. Martinez EE, Fasano A, Mehta NM. Gastrointestinal function in critical illness—a complex interplay between the nervous and enteroendocrine systems. Pediatric Med. 2020;3:23. doi:10.21037/pm-20-74
49. Jung CY, Bae JM. Pathophysiology and protective approaches of gut injury in critical illness. Yeungnam Univ J Med. 2021;38(1):27–33. doi:10.12701/yujm.2020.00703
50. Soranno DE, Coopersmith CM, Brinkworth JF, et al. A review of gut failure as a cause and consequence of critical illness. Crit Care. 2025;29(1):91. doi:10.1186/s13054-025-05309-7
51. Mansour NO, Elnaem MH, Abdelaziz DH, et al. Effects of early adjunctive pharmacotherapy on serum levels of brain injury biomarkers in patients with traumatic brain injury: a systematic review of randomized controlled studies. Front Pharmacol. 2023;14. doi:10.3389/fphar.2023.1185277
52. Deane AM, Fraser RJ, Chapman MJ. Prokinetic drugs for feed intolerance in critical illness: current and potential therapies. Crit Care Resuscitation. 2009;11(2):132–143. doi:10.1016/S1441-2772(23)01538-7
53. Giudicessi JR, Ackerman MJ, Camilleri M. Cardiovascular safety of prokinetic agents: a focus on drug‐induced arrhythmias. Neurogastroenterol Motil. 2018;30(6). doi:10.1111/nmo.13302
54. Tonini M, Cipollina L, Poluzzi E, Crema F, Corazza GR, De Ponti F. Clinical implications of enteric and central D 2 receptor blockade by antidopaminergic gastrointestinal prokinetics. Aliment Pharmacol Ther. 2004;19(4):379–390. doi:10.1111/j.1365-2036.2004.01867.x
55. De Ponti F. Pharmacology of serotonin: what a clinician should know. Gut. 2004;53(10):1520–1535. doi:10.1136/gut.2003.035568
56. Tack J. Prokinetics and fundic relaxants in upper functional GI disorders. Curr Opin Pharmacol. 2008;8(6):690–696. doi:10.1016/j.coph.2008.09.009
57. Camilleri M, Parkman HP, Shafi MA, Abell TL, Gerson L. Clinical guideline: management of gastroparesis. Am J Gastroenterol. 2013;108(1):18–37. doi:10.1038/ajg.2012.373
58. Gavioli EM, Guardado N, Haniff F, Deiab N, Vider E. The risk of QTc prolongation with antiemetics in the palliative care setting: a narrative review. J Pain Palliat Care Pharmacother. 2021;35(2):125–135. doi:10.1080/15360288.2021.1900491
59. Sakashita M, Yamaguchi T, Miyazaki H, et al. Pharmacokinetics of the gastrokinetic agent mosapride citrate after single and multiple oral administrations in healthy subjects. Arzneimittelforschung. 1993;43(8):867–872.
60. Yasuko SY, Kohei T, Keiko T, et al. Ability of mosapride to bind to 5-HT4 receptor in the human stomach. Jpn J Pharmacol. 1999;79(4):493–496. doi:10.1254/jjp.79.493
61. Charoensareerat T, Bhurayanontachai R, Sitaruno S, et al. Efficacy and safety of enteral erythromycin estolate in combination with intravenous metoclopramide vs intravenous metoclopramide monotherapy in mechanically ventilated patients with enteral feeding intolerance: a randomized, double‐blind, controlled pilot study. J Parenteral Enteral Nutr. 2021;45(6):1309–1318. doi:10.1002/jpen.2013
62. Nguyen NQ, Chapman M, Fraser RJ, Bryant LK, Burgstad C, Holloway RH. Prokinetic therapy for feed intolerance in critical illness: one drug or two? Crit Care Med. 2007;35(11):2561–2567. doi:10.1097/01.CCM.0000286397.04815.B1
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.