Back to Journals » International Journal of General Medicine » Volume 15
Morphological and Functional Features in Patients with Idiopathic Macular Hole Treatment
Authors Li J, Wang W, Zhang X, Liu J ![]() , Zhang H, Cui T, Wang F, Zhou G
, Zhang H, Cui T, Wang F, Zhou G
Received 10 March 2022
Accepted for publication 20 April 2022
Published 28 April 2022 Volume 2022:15 Pages 4505—4511
DOI https://doi.org/10.2147/IJGM.S365886
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Jing Li, Wenjuan Wang, Xiaodan Zhang, Jinxing Liu, Haining Zhang, Tong Cui, Fangfang Wang, Guohong Zhou
Department of Ophthalmology, Shanxi Eye Hospital Affiliated to Shanxi Medical University, Taiyuan, 030002, People’s Republic of China
Correspondence: Guohong Zhou, Department of Ophthalmology, Shanxi Eye Hospital Affiliated to Shanxi Medical University, No. 100 Fudong St, Xinghualing District, Taiyuan, 030002, Shanxi, People’s Republic of China, Email [email protected]
Purpose: To evaluate the multifocal electroretinogram (mfERG) and optical coherence tomography (OCT) angiography features in patients with idiopathic macular hole (IMH) before and after vitrectomy.
Patients and Methods: This prospective study was conducted at Shanxi Eye Hospital from January 2019 to December 2021. Twenty-five eyes of 25 patients with unilateral IMH, the unaffected fellow eyes, and 30 eyes of healthy patients were investigated. All unilateral IMH eyes underwent vitrectomy.
Results: The IMH eyes had significantly delayed latency (rings 2– 5) of mfERG compared with the healthy control eyes, and the amplitude density of all rings of mfERG was reduced (P < 0.05). When comparing the mfERG components before surgery and at the follow-up, the amplitude density of IMH eyes (ring 1, 3, 4 and 5) was increased significantly (P < 0.05). The delayed implicit times of the second and fifth ring were significantly shortened compared with those of preoperative eyes (P < 0.05). The mean delayed implicit time of mfERG in six months after surgery was negatively correlated with visual acuity (r = − 0.890, P = 0.043). Significant differences of superficial retinal blood flow density (SRBFD, P < 0.001) and choroidal blood flow density (CBFD) (P < 0.05) got via OCTA were found between IMH before surgery and healthy control eyes. SRBFD of the fellow eyes were significantly different with the healthy control eyes (P = 0.038). Statistically significance of SRBFD and CBFD changes in IMH eyes were found before and after surgery (P < 0.05).
Conclusion: IMH eyes had a decreased amplitude density and a delayed implicit time in some regions. Additionally, SRBFD and CBFD were both increased after vitrectomy, which suggests that the blood supply of the retina and choroid is partially restored after vitrectomy.
Keywords: idiopathic macular hole, multifocal electroretinogram, OCT-angiography, pars plana vitrectomy
Introduction
Idiopathic macular hole (IMH) is the main cause of central vision loss in the elderly.1 Pars plana vitrectomy with internal limiting membrane (ILM) peeling has been identified as primary treatment for IMH.2,3 Although there is a high rate of macular hole closure after vitrectomy, the improvement of functional vision is still not ideal. The macula is vascularized by the capillary network circulation from the chorionic capillaries. Some studies have shown that the anatomical changes of the choroid may be related to the development of retinal defects and the progression of macular holes.4 Most studies on IMH surgery use best corrected visual acuity (BCVA) as the main indicator of recovery.5 Although BCVA is an effective measurement in some cases, it cannot completely reflect the function of the retina. Multifocal electroretinogram (mfERG) was developed by Sutter and Tran in 1992. It is a non-invasive and objective test that detects local functional changes of the central retina by measuring electrophysiological response, and it can directly reflect the local functions of the retina, especially the macula, in the form of a three-dimensional topographic map. Most of the previous studies have focused on the study of full-field ERG and pattern ERG, which are based on the electrical activity of the entire retina.6 When the cumulative lesion does not exceed 20% of the retinal area, the ERG measurements may appear normal. Based on this shortcoming, the advantages of mfERG are revealed.6 Previous study7 has shown that the measurements of mfERG decrease in the fovea in IMH eyes, and they would be improved with IMH closure. The use of mfERG to observe the preoperative lesions and postoperative recovery of IMH can provide new perspectives and deepen the understanding of this disease.
Previously, researchers speculated that the decrease of foveal choroidal blood flow may be related to the formation of IMH. However, since the imaging and quantification of the capillary layer with conventional inspection equipment is a challenge, the chorionic capillary network has not been systematically evaluated by using traditional coherence tomography (OCT). Moreover, the detection of choroidal blood flow has mostly used indocyanine green angiography (ICGA) in clinical practice.8 However, it requires intravenous injection of contrast agent, and it is an invasive examination, so it is not suitable for all people. OCT Angiography (OCTA) is a newly established three-dimensional OCT for visualization and evaluation of retinal blood vessels. The application of OCTA makes it possible to measure choroidal microvascular flow non-invasively.9,10 However, little is known on the changes of choroidal microvascular flow by OCTA in IMH eyes.
In this study, we investigated the changes in mfERG before and after IMH surgery. We also investigated the superficial retinal blood flow density and choroidal blood flow density of the macula in IMH, and compared these with unaffected fellow eyes and normal eyes to identify the formation of IMH as well as potential avenues for preventing and treating IMH.
Patients and Methods
This was a prospective study and was approved by the Institutional Review Board of Shanxi Eye Hospital, Taiyuan, China (NO.SXYYLL-20190802). The study protocol adhered to the tenets of the Declaration of Helsinki (as revised in 2013). All patients signed an informed consent before participation. Patients were recruited from January 2019 to December 2021 in Shanxi Eye Hospital. All participants received visual acuity, refraction, non-contact tonometry, anterior segment examination and detailed fundus examination, OCT, and OCTA. The IMH staging was determined according to the Gass classification9,11. The test was performed by a spectral domain optical coherence tomography (SD-OCT) system (Optovue, Angiovue imaging system, American). The exclusion criteria for all subjects were as follows: (I) refractive error <−6.00 D; (II) intraocular pressure (IOP) >22 mmHg; (III) patients with a history of any retinal disease; or (IV) patients who had undergone retinal surgery or other treatment. All IMH eyes underwent 25G pars plana vitrectomy (PPV) plus ILM peeling plus gas (C3F8 or sterilized air) or silicone oil implantation. The follow-up duration was 6 months. In the IMH eyes the best corrected visual acuity (logMAR) was tested before surgery and one month, three months and six months after the operation. Healthy subjects over 50 years old, whose BCVA was better than 0.9 without ocular disease, were included as healthy control.
The electrophysiological response of the eyes was recorded by the multifocal ERG (super color Ganzfeld Q450 SCX. Roland Consult). The amplitude density and delay time of 5 loops were measured. In order to quantify the retinal and choroid blood circulation, the Optovue software (version 2014.2.0.93) was used to analyze the blood flow density on the superficial retinal angiography and the blood flow density of the deep choroid layer, reflecting the choroidal capillary circulation in the macular area. Divide this data by the area of the selected area 3.142 to get the blood flow density of the choroid layer. OCTA indicators were measured using angio-retina mode scan (3mm×3mm size). The blood flow area of the superficial retinal capillaries in the macular area and the blood flow area of the choroidal capillaries are the blood flow area with a 3mm×3mm scanning range centered on the macular fovea with a radius of 1 mm.
Statistical Analysis
Data were entered in excel (Microsoft Corp, Redmond, WA, USA), and all analyses were performed in SPSS (Version 23.0, Inc, Chicago, IL, USA). Continuous variables were presented as mean ± standard deviation (SD) and categorical variables were recorded as percentages. Normality of parameters was assessed with the Shapiro–Wilk test. Independent samples t-test was used to compare the delayed times and response densities of mfERG in rings 1–5, vascular densities of superficial retinal capillary and choroidal flow area between IMH eyes and the unaffected fellow eyes with healthy control. Data of IMH eyes were compared before and 1, 3, 6 months after surgery using repeated measures ANOVA. Variables before and after operation were analyzed with Paired-samples t-test. Spearman correlation was performed to investigate the correlation between visual acuity and the delayed times and response densities of mfERG (rings 1–5), vascular densities of superficial retinal capillary and choroidal flow area. A P < 0.05 was considered statistically significant.
Results
In the current study, 25 eyes from 25 patients with unilateral IMH were included, and 30 eyes of 30 healthy people were included as control. Table 1 shows the characteristics of included eyes. There was no statistically significant difference in age, gender and BCVA between the IMH eyes, fellow eyes and health control eyes (all P > 0.05).
 |
Table 1 Baseline Characteristic of Included Patients |
The characteristics of mfERG components among normal eyes, fellow eyes and IMH eyes are shown in Table 2. Compared with normal eyes, the delayed implicit time of all the rings in the macular hole of the research subjects was significantly delayed, and the amplitude density of all the rings was reduced (except the third ring, P < 0.001). In the fellow eyes, it was found that the delayed implicit time of all the rings was significantly delayed, while the amplitude density of the fourth ring was significantly reduced (P < 0.001).
 |
Table 2 Comparison of Multifocal Electroretinogram Parameters of IMH Eyes, Fellow Eyes and Normal Eyes |
The CBFD between the IMH eyes and the fellow eyes group was statistically significant (P < 0.001). The SRBFD and CBFD between the IMH eyes and the normal control group were also statistically significant (P < 0.001, P = 0.002, respectively). The SRBFD levels of the fellow eye group were lower than those in the normal control group (P = 0.038, Table 3).
 |
Table 3 Comparisons of SRBFD and CBFD Measurements in Macular Area Between IMH Group, Fellow Eye Group and Healthy Control Group |
In IMH eyes, the amplitude density of the first, third, fourth and fifth rings was significantly increased after surgery, and there was a significant difference compared with preoperatively (P < 0.001). The delayed implicit time in the second and fifth rings was significantly reduced and there was a significant difference compared to preoperatively (P < 0.05) (Table 4).
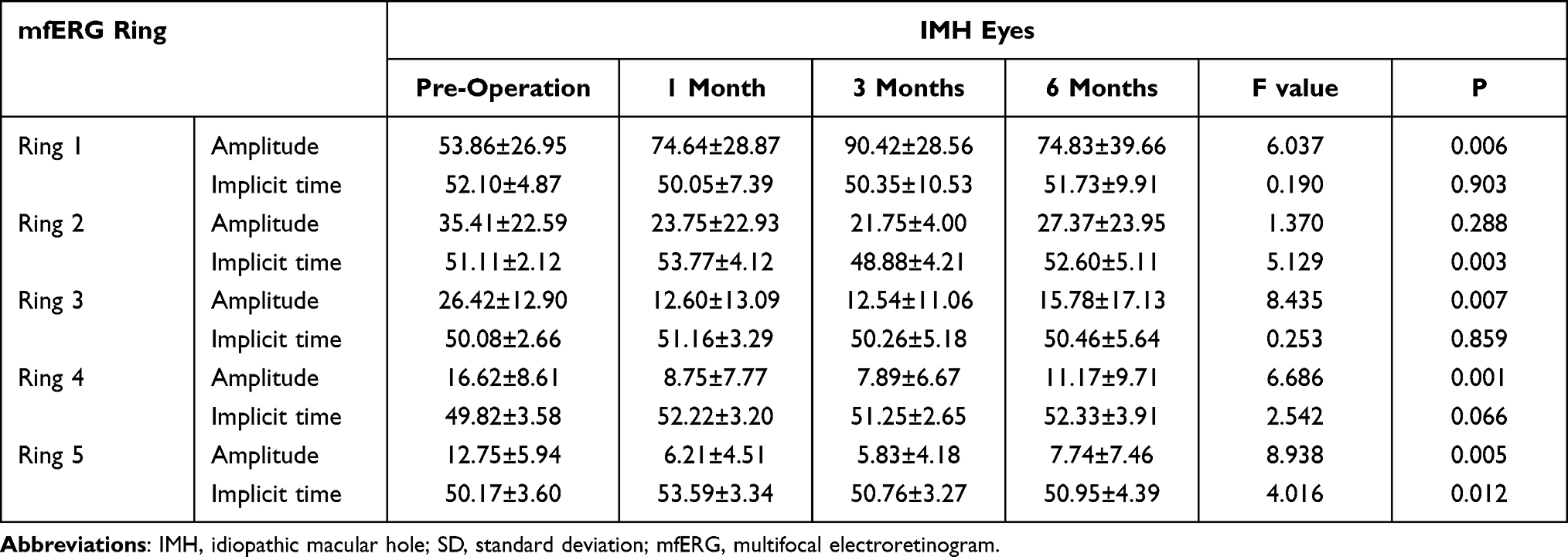 |
Table 4 Pre and Post-Surgery (1 Month, 3 Months, and 6 Months) Comparison of Multifocal Electroretinogram (mfERG) Components in IMH Eyes (Mean±SD) |
Table 5 shows the average delayed implicit time of six months after surgery was negatively correlated with visual acuity (r = −0.890, P = 0.043).
 |
Table 5 Correlation Between Visual Acuity in logMAR and Multifocal Electroretinogram (mfERG) Components Before and After Surgery in IMH Eyes and in the Fellow Eyes |
Furthermore, Table 6 shows the differences between SRBFD and CBFD before and after surgery (at 1 month, 3 months, and 6 months). There was a statistical significance on SRBFD at baseline, 1 month, 3 months, and 6 months after operation, and the SRBFD increased after operation (at 1 month, and 3 months). Similarly, the CBFD was statistically significant changes before operation, 1 month, 3 months, and 6 months after operation.
 |
Table 6 Pre and Post-Surgery (1 Month, 3 Months, and 6 Months) Comparison of SRBFD and CBFD in Eyes with IMH (Mean±SD) |
Discussion
The purpose of this study was to investigate the morphological and functional recovery of the retina and choroid before and after IMH surgery. After surgery, the macular hole was successfully closed and function of macular was improved in IMH eyes. The mfERG also showed varying degrees of recovery. All rings of delayed implicit times in the fellow eye were found to have significantly delayed, while the fourth ring of amplitude density had a significantly lower. In OCTA measurements, the SRBDF and the CBDF of the IMH eyes were significantly lower than those of normal eyes, and the SRBDF and CBDF levels increased after the operation. Interestingly, the SRBFD of the fellow eyes were lower than the normal eyes. Therefore, we should be alert to the occurrence of macular hole in the fellow eye, pay more attention in follow-up work, especially in early detection.
Multifocal ERG has its own unique advantages: it can accurately and quantitatively reflect the function of various parts of the retina.6 Tuzson et al studied the role of mfERG measurements in the diagnosis of IMH and concluded that the mfERG in the fellow eyes of patients with IMH seems clinically useful. The lower amplitude may forecast the propensity for subsequent development of IMH. Patients with low central ERG amplitude and lower ring ratios in the healthy fellow eyes should have stricter follow-up.12 Most studies focused on preoperative and postoperative comparisons, with no comparisons with the fellow eyes or normal controls.7,13,14 Our results suggested that the delayed implicit time of all the rings was significantly delayed in the fellow eyes. It revealed that we should be alert to the occurrence of macular holes in the fellow eye. Previous authors have reported varied results about the role of mfERG in macular hole. A positive correlation was seen between the postoperative visual acuity and mfERG amplitudes, however, the amplitudes tended to vary greatly even in patients with the same level of acuity.15 Conversely, improvement in ERG amplitudes were noted even with unchanged visual acuities after macular hole closure16. Si et al found that the decrease in retinal ERG response was not limited to the fovea but involved an area of the perifovea of 1.6 disc diameters. The ERG response density of these areas gradually improved after macular hole closure.14 In the current study, after macular hole surgery, we found that the amplitude density of the first, third, fourth, and fifth rings was significantly increased compared to preoperation, and the mean delayed implicit time of post-operation was significantly shortened, and it was negatively correlated with visual acuity. It shows that retinal function has been restored to different degrees, which indicate that the macular function of retinal has been partially recovered after IMH surgery.
As the only blood supply tissue in the center of the macula, the choroid maintains a high metabolic activity in the center of the macula, and choriocapillary damage can seriously affect the function of the macula. Therefore, it is extremely important to accurately understand the choroidal blood circulation. The changes of blood circulation are closely related to the occurrence, development and prognosis of maculopathy. The choroidal circulation can be detected to evaluate the progress of the disease and the effect of treatment. Choroidal perfusion is an important anatomical factor in macular physiology.8 Due to the lack of previous technical means to measure choroidal blood flow, the pathogenesis of IMH has mainly focused on changes in choroidal thickness. However, the results of various studies are controversial due to inconsistent quantitative methods for choroidal thickness measurement.17–19 Most literature reports only focused on morphological changes in macular holes. Apostolopoulos et al20 observed the changes of macular hole size and the recovery of retinal function of mfERG after surgery in IMH eyes, while it did not involve the blood supply of retina and choroid. With the advent of OCTA,21 quantitative analysis of retinal and choroidal blood flow became possible. The studies about retinal and choroidal circulation in the macular region before and after surgery of idiopathic macular hole were rare. Most of the previous studies focused on the morphological studies of the retina and choroid before and after macular hole surgery, such as the changes in the area of the avascular area in the superficial macular region and the changes in the thickness of the choroid.8,10,22 Wilczynski et al investigated the features of OCTA in patients with IMH eyes before and after surgical treatment and concluded that quantitative evaluation of vascular and morphological changes following IMH surgery using OCTA shows the potential for recovery due to vascular and neuronal plasticity. OCTA showing vascular changes and their quantitative characteristics might be a useful tool for the assessment of macular holes before and after surgical treatment.17 In the current study, the SRBFD showed an increase at one month and three months after the operation, indicating that the retinal function was partially restored, but the SRBFD decreased at 6 months after the operation. Compared with the fellow eyes, the CBFD in the IMH eyes was significantly reduced and it increases at different time periods after surgery (1 month, 3 months, and 6 months). These changes reflected that after IMH surgery, the choroidal blood supply was partially restored. However, the exact mechanism for choroidal capillary damage in full-thickness macular hole eyes is still unknown. One possible explanation is that the restoration of choriocapillaries is associated with the restoration of retinal structure.19 The main blood supply to the retina is the choroid because photoreceptors are metabolically very active. Ions and water continuously flow through the retina enters the choroid.23 Both the SRBFD and CBFD in the IMH eyes were significantly lower than those in the normal eyes, and the fellow eyes also changed, which also suggested us to be vigilant in the follow-up of the fellow eye group and closely observe the occurrence of macular hole in the fellow eye.
There are still some deficiencies in this study, the sample included is slightly less, the observation time is still short, and the results have certain limitations, and it is necessary to expand the sample and conduct in-depth research. Our follow-up time is half a year, it is necessary to conduct further long-term observations and continue to study the changes of retina and choroid function, and provide more theoretical basis.
Conclusion
Through the measurements of mfERG, the delayed implicit time of the IMH eyes was significantly delayed, and the amplitude density was reduced, and the fellow eyes were also damaged correspondingly, and the macular retinal function recovered after macular hole surgery. According to OCTA, the SRBFD and the CBFD of the IMH eyes were significantly lower than those of healthy eyes. The SRBFD increased at 1 month and 3 months after the operation, and the CBFD continued to increase after the operation. Our study revealed the retinal function and choroidal circulations in IMH eyes could be restored after the repair of macular hole. Furthermore, our findings imply that quantification of SRBFD and CBFD may serve as a parameter for assessing macular disease progression and prognosis.
Statement of Ethics
All participants gave the informed consent before their inclusion in the study. The study protocols were conducted according to the principles of the Declaration of Helsinki and were approved by the Scientific and Medical Ethical Committee of the Shanxi Eye Hospital.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This study was supported by Major Research and Development Program of Shanxi (No201903D321117), Medical major Research program of Shanxi (No2020RC22) and \ (No. 2020-195).
Disclosure
The authors do not have any conflicts of interest to report in this work.
References
1. McCannel C-A, Ensminger J-L, Diehl -N-N, et al. Population-based incidence of macular holes. Ophthalmology. 2009;116(7):1366–1369. doi:10.1016/j.ophtha.2009.01.052
2. Sayanagi K, Ikuno Y, Soga K, et al. Residual indocyanine green fluorescence pattern after vitrectomy for idiopathic macular hole with internal limiting membrane peeling. Br J Ophthalmol. 2007;91(7):939–944. doi:10.1136/bjo.2006.108746
3. Hu Z, Qian H, Fransisca S, et al. Minimal internal limiting membrane peeling with ILM flap technique for idiopathic macular holes: a preliminary study. BMC Ophthalmol. 2020;20(1):228. doi:10.1186/s12886-020-01505-x
4. Teng Y, Yu M, Wang Y, et al. OCT angiography quantifying choriocapillary circulation in idiopathic macular hole before and after surgery. Graefes Arch Clin Exp Ophthalmol. 2017;255(5):893–902. doi:10.1007/s00417-017-3586-0
5. Yip Y-W, Fok A-C, Ngai J-W, et al. Changes in first- and second-order multifocal electroretinography in idiopathic macular hole and their correlations with macular hole diameter and visual acuity. Graefes Arch Clin Exp Ophthalmol. 2010;248(4):477–484. doi:10.1007/s00417-009-1165-8
6. Creel DJ. Multifocal electroretinograms. J Visual Exp. 2011;(58). doi:10.3791/3176
7. Moreto R, De Lucca Perches ACB, Almeida F, Jorge R, Messias A, Gekeler K. Central mfERG amplitude ratio as a predictor for visual outcome of macular hole surgery. Documenta Ophthalmologica. 2020;140(1):23–30. doi:10.1007/s10633-019-09716-4
8. Cho J-H, Yi H-C, Bae S-H, et al. Foveal microvasculature features of surgically closed macular hole using optical coherence tomography angiography. BMC Ophthalmol. 2017;17(1):217. doi:10.1186/s12886-017-0607-z
9. Lauermann P, Dulk J, van Oterendorp C, et al. Reorganization of the perifoveal microvasculature after macular hole closure assessed via optical coherence tomography angiography. Exp Eye Res. 2020;198:108132.
10. Baba T, Kakisu M, Nizawa T, et al. Superficial foveal avascular zone determined by optical coherence tomography angiography before and after macular hole surgery. Retina. 2017;37(3):444–450. doi:10.1097/IAE.0000000000001205
11. Gass J-D. Idiopathic senile macular hole. Its early stages and pathogenesis. Arch Ophthalmol. 1988;106(5):629–639. doi:10.1001/archopht.1988.01060130683026
12. Tuzson R, Varsanyi B, Nagy BV, et al. Role of multifocal electroretinography in the diagnosis of idiopathic macular hole. Invest Ophthalmol Vis Sci. 2010;51(3):1666–1670. doi:10.1167/iovs.09-4375
13. Mendoza-Santiesteban CE, Fernández-Cherkasova L, Echavarria OH, Rodríguez RC, Columbié-Garbey Y, Riesgo TJ. Multifocal electroretinography. Semin Ophthalmol. 2010;25(4):155–164. doi:10.3109/08820538.2010.500210
14. Si Y-J, Kishi S, Aoyagi K. Assessment of macular function by multifocal electroretinogram before and after macular hole surgery. Br J Ophthalmol. 1999;83(4):420–424. doi:10.1136/bjo.83.4.420
15. Moschos M, Apostolopoulos M, Ladas J, et al. Multifocal ERG changes before and after macular hole surgery. Doc Ophthalmol. 2001;102:31–40. doi:10.1023/A:1017507220510
16. Terasaki H, Miyake Y, Nomura R, et al. Focal macular ERGs in eyes after removal of macular ILM during macular hole surgery. Invest Ophthalmol Vis Sci. 2001;42:229–234.
17. Wilczynski T, Heinke A, Niedzielska-Krycia A, et al. Optical coherence tomography angiography features in patients with idiopathic full-thickness macular hole, before and after surgical treatment. Clin Interv Aging. 2019;14:505–514.
18. Hashimoto Y, Saito W, Fujiya A, et al. Changes in inner and outer retinal layer thicknesses after vitrectomy for idiopathic macular hole: implications for visual prognosis. PLoS One. 2015;10(8):e0135925. doi:10.1371/journal.pone.0135925
19. Ahn J, Yoo G, Kim JT, Kim SW, Oh J. Choriocapillaris layer imaging with swept-source optical coherence tomography angiography in lamellar and full-thickness macular hole. Graefes Arch Clin Exp Ophthalmol. 2018;256(1):11–21. doi:10.1007/s00417-017-3814-7
20. Apostolopoulos M-N, Koutsandrea C-N, Moschos M-N, et al. Evaluation of successful macular hole surgery by optical coherence tomography and multifocal electroretinography. Am J Ophthalmol. 2002;134(5):667–674. doi:10.1016/S0002-9394(02)01700-2
21. de Carlo T-E, Romano A, Waheed N-K, et al. A review of optical coherence tomography angiography (OCTA). Int J Retina Vitreous. 2015;1:1–5.
22. Kim YJ, Jo J, Lee JY, Yoon YH, Kim JG. Macular capillary plexuses after macular hole surgery: an optical coherence tomography angiography study. Br J Ophthalmol. 2018;102(7):966–970. doi:10.1136/bjophthalmol-2017-311132
23. Rymer J, Wildsoet CF. The role of the retinal pigment epithelium in eye growth regulation and myopia: a review. Vis Neurosci. 2005;22(3):251–261. doi:10.1017/S0952523805223015
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.