Back to Journals » Clinical Ophthalmology » Volume 16
Morphologic and Cellular Changes Induced by Selective Laser Trabeculoplasty
Authors Gupta M, Heo JY ![]() , Gong H
, Gong H ![]() , Cha E, Latina M, Rhee DJ
, Cha E, Latina M, Rhee DJ
Received 17 October 2021
Accepted for publication 24 December 2021
Published 29 April 2022 Volume 2022:16 Pages 1383—1390
DOI https://doi.org/10.2147/OPTH.S342787
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Meenakashi Gupta,1 Jae Young Heo,2 Haiyan Gong,3 Elliot Cha,3 Mark Latina,4,5 Douglas J Rhee2
1Department of Ophthalmology, New York Eye & Ear Infirmary of Mt. Sinai, New York, NY, USA; 2Department of Ophthalmology & Visual Sciences, University Hospitals, Cleveland, OH, USA; 3Department of Ophthalmology, Boston University, Boston, MA, USA; 4Department of Ophthalmology, Massachusetts Eye & Ear Infirmary, Boston, MA, USA; 5Department of Ophthalmology, Advanced Glaucoma Specialists, Reading, MA, USA
Correspondence: Douglas J Rhee, Department of Ophthalmology & Visual Sciences, 10900 Euclid Ave, Lakeside, 4129, Cleveland, OH, 44105, USA, Tel +1 216-844-8590, Fax +1 216-983-0544, Email [email protected]
Purpose: Selective laser trabeculoplasty is a safe and effective procedure for reducing IOP, but its mechanism of action is not fully elucidated. We evaluated the morphologic and cellular changes as well as DNA synthesis after SLT treatment of human trabecular meshwork (TM) tissue explants.
Methods: Corneoscleral rim tissues that underwent SLT treatment were compared to control segments that had no laser treatment. Light microscopy (LM), transmission electron microscopy (TEM), and scanning electron microscopy (SEM) were used to assess cell morphology. The Click-iT 5-ethynyl-2’-deoxyuridine (EdU) imaging kit was used to compare DNA synthesis/cell proliferation with a confocal microscope. All tissues were assessed for vitality.
Results: SLT treatment does not reveal notable cell damage in the juxtacanalicular (JCT) region, but mildly disrupts superficial trabecular beams and uveal TM, ablates TM endothelial cells from the undamaged beams as detected by both LM and TEM. This superficial destruction was not observed in some SLT treatment spots on higher magnification by SEM. SLT treatment increased mitotic activity and DNA synthesis near the lining of Schlemm’s canal after several days.
Conclusion: SLT treatment disrupts endothelial cells in the corneoscleral TM and causes superficial ultrastructural changes to the uveal TM. SLT treatment also shows a trend towards dynamic time-dependent changes in (DNA synthesis) with an increase in mitotic activity at 7 days cell proliferation.
Keywords: DNA synthesis, electron microscopy, selective laser trabeculoplasty, glaucoma
Introduction
Selective laser trabeculoplasty (SLT) is an effective treatment for open-angle glaucomas.1 Clinically, the intraocular pressure (IOP) lowering effects of SLT may start within hours following laser application and can persist for several years.2 SLT is known to lyse intraocular melanosomes, selectively ablating pigmented trabecular meshwork (TM) cells, minimizing thermal damage to adjacent cells and structures.3
Anatomical studies of human TM tissue following SLT laser have demonstrated conflicting findings regarding the extent of tissue damage following SLT laser.4,5 SLT has shown elevated glycosylation levels to the TM compared to non-lasered TM.6 Some studies have shown alteration in gene expression7,8 and recruitment of macrophages to the TM.9 The underlying mechanism(s) by which SLT increases outflow facility, reducing intraocular pressure (IOP) remains uncertain.
Argon laser induces thermal damage of the TM and several biochemical changes, including secretion of cytokines IL-1β and TNFα,10 induction of matrix metalloproteinases stromelysin and gelatinase B and tissue inhibitors of metalloproteinase (TIMP-1).11,12 Studies of argon laser trabeculoplasty (ALT) and high powered Nd:YAG laser have demonstrated an increase in cell division and cell migration within the TM following treatment.13–17
SLT in clinical practice uses higher laser energy levels than those used in previous SLT cell culture studies.3 These in vitro results may not be fully representative of all the changes that occur clinically. The purpose of our study was to evaluate the morphological and cellular changes in DNA synthesis after treatment of human TM tissue explants with SLT using energy levels titrated to clinically relevant endpoints to mirror clinical conditions as closely as possible.
Materials and Methods
Tissue Preparation
Corneoscleral rim explants from eye bank human donor eyes stored in Optisol GS for no more than 48 hours (Bausch and Lomb; New Jersey) and discarded corneoscleral rims following corneal transplantation were used; all tissue used in the study was within 3 days of death. Donor ages were between 47 and 62 years of age with no known history of ocular disease. All donor tissues (n = 12) were obtained from regional eye banks and managed according to the Declaration of Helsinki guidelines on research involving human tissue and our institutional IRB. The tissue quality and degree of trabecular pigmentation was graded on a scale of 0 to 4 using a dissecting microscope. The tissue quality grading was subjectively based on tissue rigidity and stiffness as a surrogate estimate of tissue viability and freshness; 0 = very poor quality, low turgor, while 4 = very high quality, high turgor similar to cadaver tissue harvested within 12 hours of death. TM pigmentation grading was according to a previously published guideline commonly used clinically;18 briefly, 0 = no pigmentation and 4 = heavy pigmentation. All tissue rims used in the study were graded 3 or 4 for tissue quality and 2 and 3 for pigmentation. Corneoscleral rim explants were divided into 4 equal segments and stabilized for 2 days in serum-free media at 37 degree, 5% CO2 and 95% humidity prior to the onset of experimentation.19 Two days was chosen as the optimal time point allowing for stabilization of protein production, eg, GAPDH, matrix metalloproteinase 2 (MMP-2) and metalloproteinase inhibitor 4 (TIMP4), following tissue manipulation. The tissues were not perfused.
Laser Treatment
Tissue explants underwent SLT under similar conditions usually adopted for human subjects using a SLT Coherent Selecta 7000 (Palo Alto, CA). Q-switched, frequency-doubled with Nd:YAG laser at 532 nm wavelength, energy settings at 0.6–1.2 mJ/pulse, pulse duration 3.0 nsec and treatment spot size of 400 microns. The energy settings were titrated until the clinical endpoints of light blanching of the pigmented TM and champagne bubble formation were observed (Figure 1).
 |
Figure 1 Whole mount corneoscleral rim with blanching of the SLT treatment spots in the pigmented trabecular meshwork (arrows). |
The tissue was maintained in DPBS during the laser treatment which was accomplished by mounting the laser to be pointed downward. Laser was applied adjacent, without overlap, with the laser treatment spots spaced approximately by 1–2 laser spot widths, to the TM along the entire rim. Control segments were treated in a similar fashion without actual laser treatment. After laser or sham-laser (control) treatment, specimens were returned to culture in serum-free media.
Light Microscopy and Transmission Electron Microscopy
Control and laser-treated tissue explants were removed from culture one day and seven days following laser application and placed in fixative consisting of 2.5% glutaraldehyde and 2% formaldehyde in 0.1 M cacodylate buffer with 0.08 M CaCl2 at 4°C for 24 hours, washed in 0.1 M cacodylate buffer, and postfixed for 1.5 hours in 2% aqueous osmium tetroxide. Tissue was dehydrated in increasing concentrations of ethanol, transitioned in propylene oxide, infiltrated with propylene oxide and epon mixtures (TAAB 812 resin; Marivac, Quebec, Canada), embedded in epon, and cured for 48 hours at 60°C. Sections (1 μm) were cut (Leica Ultracut UCT; Leica Microsystems GmbH, Wetzlar, Germany) and stained with 1% toluidine blue in 1% borate buffer for light microscopy. Sections containing trabecular meshwork were then prepared for electron microscopy; thin sections (70 nm) were cut, stained with 4% uranyl acetate and lead citrate, and examined using a transmission electron microscope (JEM-1011; JEOL, Tokyo, Japan). Images were taken at varying magnifications.
Scanning Electron Microscopy
Control and laser-treated tissue explants were removed from culture two days and seven days following laser application. Tissue explants were fixed in 2.5% glutaraldehyde/2% paraformaldehyde solution. After tissue was fixed overnight in 4% glutaraldehyde buffered in 0.1M cacodylate buffer, the specimens were dehydrated in increasing concentrations of ethanol. After critical-point drying and coating with a thin film of gold palladium, the sections were examined with a scanning electron microscope. A Philips CM-10 scanning electron microscope was used for examination. The entire area of treatment was scanned at low and high power.
Evaluation of Cell Proliferation
Control and laser-treated tissue segments were incubated in serum-free media supplemented with 10 μM EdU (5-ethynyl-2’-deoxyuridine) per the Click-iT EdU imaging kit protocol (Invitrogen, Carlsbad, CA) for 2 days. EdU is a nucleoside analog of thymidine that is incorporated into DNA during active DNA synthesis indicating cell proliferation. After 2 days, one pair of control and laser-treated tissue segments was fixed. The remaining control and laser-treated tissue was returned to culture in serum-free media and EdU for 5 additional days. Serum-free media with EdU was changed every 2 to 3 days. After a total of 7 days in culture, the remaining control and laser-treated tissue segments were fixed. Tissue explants were fixed in 4% paraformaldehyde at 4°overnight and stored in 1% paraformaldehyde. Following fixation, control and laser-treated tissue explants were cut into 1 mm radial sections. The EdU Detection protocol from Click-iT EdU imaging kit was followed for mitotic staining using Alexa Fluor 555. Nuclei were stained with antifade reagent with DAPI (1:1) (SlowFade Gold; Invitrogen, Carlsbad, CA).
Confocal scanning laser microscopy images were acquired using the Axiovert LSM 700 (Carl Zeiss, Jena, Germany). Images were processed using Zen 2010 software (Carl Zeiss, Jena, Germany). Each control and treated tissue section was imaged in the x, y and z planes. Image stacks of 100 microns were taken at 2 micron intervals. The number of mitotic nuclei in a 100 micron z-stack was manually counted in the control and treated sections. At least four, 100 micron z-stacks from each tissue rim were imaged.
The mean number of cells undergoing DNA synthesis was calculated for each experimental set in each eye by dividing the total number of mitotic cells by the number of 100 micron z-stacks imaged. A two-tailed t-test was used to assess statistical significance.
Vitality Study
Following removal of each tissue rim from culture and fixation, a one to two mm tissue wedge was post-fixed for 1.5 hours in 2% aqueous OsO4. Tissue was dehydrated in increasing concentrations of ethanol, transitioned in propylene oxide, infiltrated with propylene oxide and epon mixtures (TAAB 812 resin, Marivac, Quebec, Canada) embedded in epon and cured for 48 hours at 60°C. One-micron sections were cut on a Leica Ultracut UCT and stained with 1% toluidine blue in 1% borate buffer. Light microscopy analysis was performed and tissue was graded on a four-point scale (Personal communication from Ethier). Tissue graded 3+ and above was utilized.
0: No cells present in the TM
+1: Cellularity of TM is less than 20% of normal with many swollen cells.
+2: Cellularity of juxtacanalicular tissue (JCT) is normal, but cellularity of TM is 50% of normal with some bare beams present. Some cell swelling evident.
+ 3: JCT and TM look essentially normal, with at least 75% of cells still present. Few, in any, uveal meshwork cells are present. Minimal swelling of cells evident.
+ 4: Eye is difficult to distinguish from a freshly fixed, normal human eye.
Results
Light Microscopy
One tissue explant was evaluated by light microscopy 1 day and 7 days following SLT application. Light microscopic analysis of toluidine blue stained sections showed mild disruption of superficial trabecular beams 1 day and 7 days following SLT treatment (Figure 2).
 |
Figure 2 Light microscopic images of the trabecular meshwork in day 1 (A) and day 7 (B) after SLT. Uveal TM beams are mildly disrupted (arrow), corneoscleral TM, juxtacanalicular tissue and the inner wall of Schlemm’s canal (SC) are well preserved (toluidine blue staining). |
The deeper trabecular beams appeared unaffected. The wall of Schlemm’s canal and scleral stroma appeared intact. Cell nuclei appeared preserved. Intracellular pigment granules were mainly found throughout the trabecular meshwork, with exception of areas of beam disruption. There was no difference in the extent and pattern of tissue alterations between day 1 and day 7 following SLT. No inflammatory reaction was observed.
Scanning Electron Microscopy
Two tissue explants from two eyes were evaluated by scanning electron microscopy two days and seven days after SLT treatment. Superficial damage of the trabecular beams was seen at low magnification (Figure 3).
 |
Figure 3 Scanning electron microscope photograph of the human uveal and corneoscleral trabecular meshwork (magnification 85x) 7 days after sham laser treatment (A) and 7 days after SLT treatment (B). There is superficial damage of trabecular beams in the region of laser treatment (arrow). |
At higher magnification within the laser spots, the rope like beams of the uveal meshwork and plate-like structures of the deeper corneoscleral trabecular meshwork appeared intact; the superficial alterations were not able to be ascertained in some laser spots (Figure 4).
 |
Figure 4 Scanning electron microscope photograph of the human uveal and corneoscleral trabecular meshwork (magnification 330x) at 2 days (B) and 7 days (D) after SLT treatment. (A) and (C) depict tissue 2 days and 7 days after sham laser treatment. The architecture of TM is well conserved, showing similar appearance in the control and treated segments. |
There was no evidence of crater formation and no disruption to the surrounding collagen scaffold or bleb formation along the trabecular beams or corneoscleral sheets, consistent with the absence of coagulative damage.
Transmission Electron Microscopy
Tissue explants, one from 1 day, one from 7 days following SLT application, and one sham control were evaluated by TEM. In sham control, the uveal and corneoscleral trabecular beams were covered by trabecular endothelial cells. One day following treatment, disrupted TM cells were seen, and some uveal trabecular beams lost their endothelial cell coverage. By day 7, cellular debris, pigment particles, and intracellular contents were seen extracellularly (Figure 5).
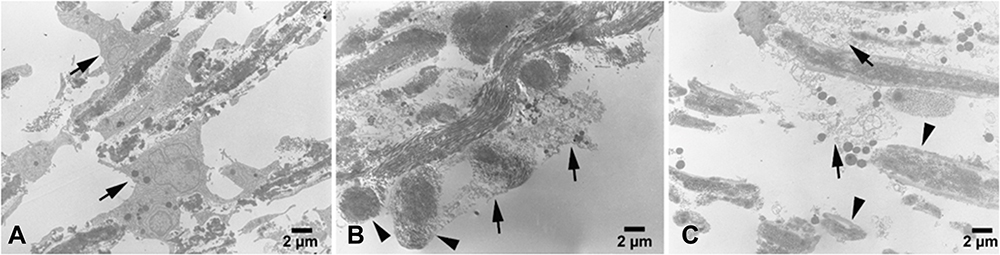 |
Figure 5 Transmission electron microscopy of human trabecular meshwork (TM) after SLT treatment compared to sham control. (A) In the sham treatment, trabecular beam are covered by TM endothelial cells (arrows), with pigment particles inside the cells. (B) One day after SLT treatment, TM cell damage (arrows) or loss of cells that cover TM beams (arrowheads) are seen in uveal beams. (C) Seven day after SLT treatment, TM cell damage (arrows) or cell loss (arrowheads) are seen in uveal beams. Pigment particles and intracellular contents released extracellularly following SLT treatment. |
Cell Proliferation
Nine tissue explants from nine eyes incubated in EdU were evaluated for DNA synthesis 2 days and 7 days following SLT using confocal microscopy. Two days following laser application there was no significant change in DNA synthesis when compared with control tissue (0.250 ± 0.280 mitotic cells/100 μm z stack for laser treatment vs 0.454 ± 0.477 mitotic cells/100 μm z stack for control, p = 0.305). (Table 1) By 7 days, there was a trend toward increased DNA synthesis in laser treated eyes (2.074 ± 2.659 mitotic cells/100 μm z stack for laser treatment vs 1.537 ±1.560 mitotic cells/100 μm z stack for control, p = 0.358). (Table 1) This increase was seen in 5 of 9 explants. The majority of the cells undergoing DNA synthesis were observed within the TM, outer wall cells of Schlemm’s canal and cells in the sclera near the outer wall of Schlemm’s canal (Figure 6).
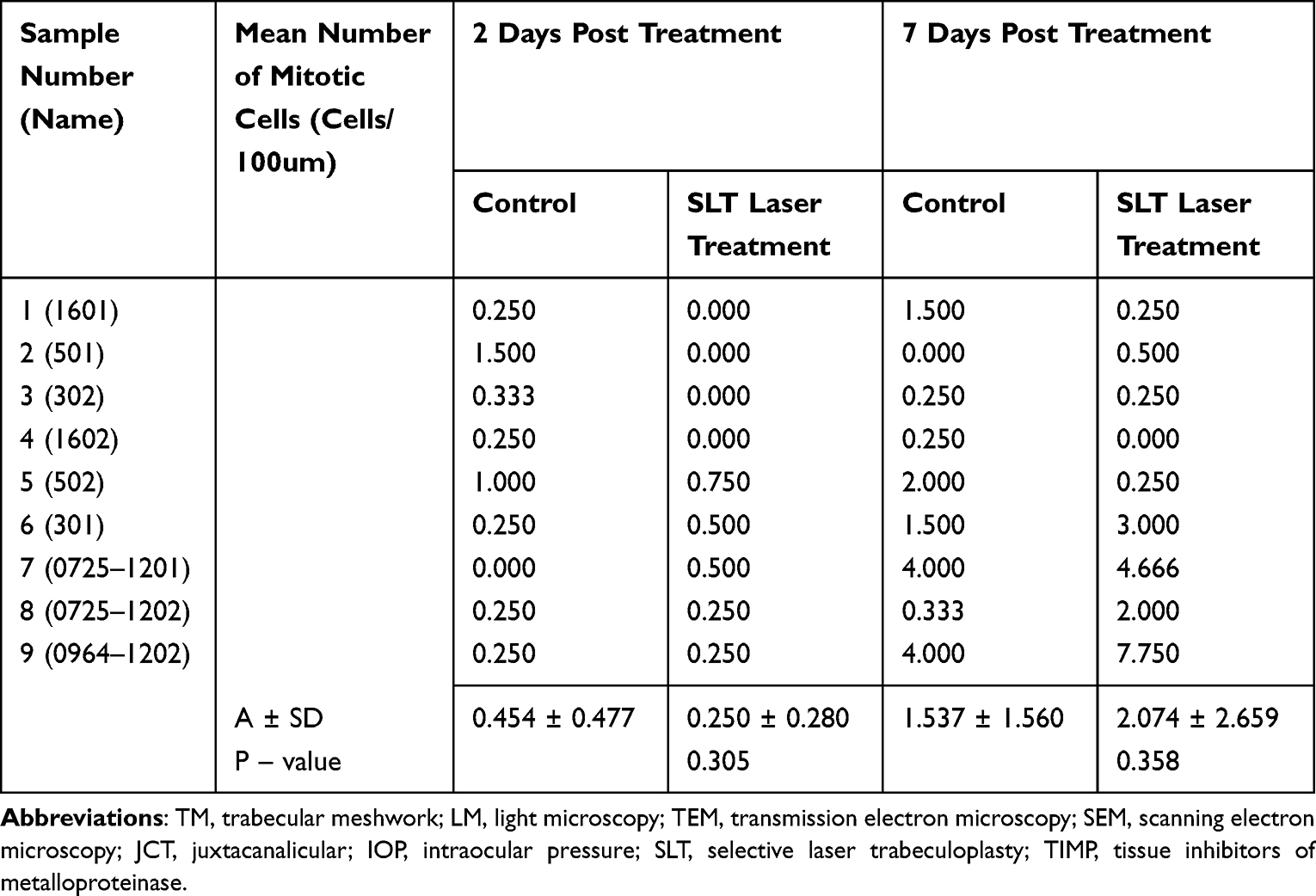 |
Table 1 Comparison of Mitotic Cells Between Control and SLT Laser Treated Tissue Segments 2 Days and 7 Days Post Treatment |
 |
Figure 6 Confocal microscopy of trabecular meshwork with DAPI stain (blue) and ErdU/Alexa Fluor axide (pink) after SLT treatment compared to sham control. No positive staining is observed in 2 days after sham treatment (A), and 2 days after SLT treatment (B). Compared to 7 days after sham treatment (C), an increase in DNA synthesis as indicated by increased ErdU/Alexa Fluor axide staining (D). Cells with increased DNA synthesis are noted in the TM, outer wall of Schlemm’s canal and sclera. |
Discussion
Our data show that the SLT delivers energy in a very selective zone within the TM. Within this zone, using the clinical treatment endpoints of champagne bubbles and blanching of pigment, there is some mild destruction of uveal TM, but overall relatively preserved TM and Schlemm’s canal structure. There is ablation of TM endothelial cells and disruption of superficial trabecular beams. The JCT region had no notable cell damage. The superficial destruction could be detected on cross sections by both light microscopy and TEM but not on the surface of the TM when viewed at higher magnification on SEM in some of the laser spots. These findings are similar to previous electron microscopy studies of the TM following SLT application that demonstrated less destruction with SLT compared with other forms of laser trabeculoplasty.4,5 However, we did not observe the fragmentation of deep trabeculae that was seen in eyes in which SLT was performed in patients prior to enucleation needed for clinical reasons.5 This difference may potentially be attributed to a greater photoacoustic effect of the laser causing mechanical energy to be dissipated focally causing a mechanical effect to deeper tissue in a whole eye model versus a more focal effect with dissipation of energy to the surroundings in the tissue explant system. In addition, another study of the TM following SLT application demonstrated that SLT can lead to ultrastructural damage at higher-powered treatments.20 We were not able to confirm any ultrastructural damage as our study utilized a max power of 1.2mJ which was less than the treatment power of 2.0mJ noted in the study.20 Nevertheless, our findings are consistent with their findings that SLT is less damaging particularly at lower power settings.20
Additionally, our data suggested a trend towards time-related changes in DNA synthesis activity following SLT. Two days following SLT application, there was a trend towards decreased activity, but subsequently, there was then a trend towards increased activity 7 days following laser. Prior studies examining the effects of ALT and high powered Nd:YAG laser on the trabecular meshwork noted an increase in DNA synthesis following laser application primarily in the trabecular inset, a non-filtering region anterior to Schlemm’s canal and resting place of trabecular stem cells.16,17 In these studies, the increase in DNA synthesis was attributed to increased mitotic activity. Furthermore, these mitotic cells were noted to migrate and repopulate the sites of laser burns in explant models following ALT.16 The increase in cell division occurred within 24–48 hours of laser application. Though our study noted a trend towards increased DNA synthesis most likely indicating increased mitotic activity, this was seen several days after laser application. Additionally, the mitotic cells, noted in our study, were observed primarily in the lining of Schlemm’s canal. The endothelial cells of Schlemm’s canal may play a significant role in regulation of aqueous outflow and intraocular pressure. Increased DNA synthetic activity can be observed in both states of increased cell division and DNA repair. Therefore, it is plausible that these observed changes in DNA synthesis reflect some level of DNA repair in addition to increased mitotic activity. One possibility is that SLT causes damage to nuclei material in the early phase followed by an increase in cell division in the later phase. This hypothesis would correlate with Izzotti et al’s findings of a microarray analysis in which 5 genes involved in DNA repair and 1 gene inhibiting cell cycle were upregulated and 3 genes inducing cell cycle progression were downregulated in TM cell cultures within hours following SLT application.7 This study did not follow the cell cultures for an extended period, so it possible that gene expression one week after treatment is different.
Conclusion
SLT results in disruption of the endothelial cells of the corneoscleral and uveal TM as well as superficial ultrastructural changes to the TM anatomy. There is a trend towards dynamic time-dependent alterations in nuclear division and/or cell proliferation that ultimately lead to the observed increased outflow facility and IOP reduction. The pathway is likely multifaceted involving changes at the nucleic acid level. The exact cascade of events remains to be fully elucidated.
Acknowledgments
We are grateful for the technical expertise of Dr. Normand A. Michaud with the scanning electron microscopy.
Funding
Supported by: National Eye Institute 5R01EY019654-02 (Rhee), R01EY022634 (Gong) and P30EY011373 (VSRC Core Grant), unrestricted funds from the Research to Prevent Blindness, unrestricted funds from the Cleveland Eye Bank Foundation and The Massachusetts Lions Eye Research Fund (Gong).
Disclosure
Declaration of interest for Corresponding author: Research Funding (to Institution): Allergan, Glaukos, Ivantis;Consultant: Aerie, Alcon, Allergan, Bausch and Lomb, Ivantis, pH-Pharma;Speakers Bureau: Aerie, Bausch and Lomb, Ivantis;Scientific Advisory Board: Ocular Therapeutix. Mr Jae Young Heo reports grants from National Eye Institute, grants from Research to Prevent Blindness, grants from Cleveland Eye Bank Foundation, grants from The Massachusetts Lions Eye Research Fund, during the conduct of the study. Dr Mark Latina reports a patent Selective Targeting of TM cells issued to Lumenis. The authors report no other conflicts in interest in this work.
References
1. Garg A, Gazzard G. Selective laser trabeculoplasty: past, present, and future. Eye. 2018;32:863–876.
2. Latina MA, de Leon JM. Selective laser trabeculoplasty. Ophthalmol Clin North Am. 2005;18:409–419,vi.
3. Latina MA, Park C. Selective targeting of trabecular meshwork cells: in vitro studies of pulsed and CW laser interactions. Exp Eye Res. 1995;60:359–371.
4. Kramer TR, Noecker RJ. Comparison of the morphologic changes after selective laser trabeculoplasty and argon laser trabeculoplasty in human eye bank eyes. Ophthalmology. 2001;108:773–779.
5. Cvenkel B, Hvala A, Drnovsek-Olup B, Gale N. Acute ultrastructural changes of the trabecular meshwork after selective laser trabeculoplasty and low power argon laser trabeculoplasty. Lasers Surg Med. 2003;33:204–208.
6. Amelinckx A, Castello M, Arrieta-Quintero E, et al. Laser trabeculoplasty induces changes in the trabecular meshwork glycoproteome: a pilot study. J Proteome Res. 2009;8:3727–3736.
7. Izzotti A, Longobardi M, Cartiglia C, Rathschuler F, Sacca SC. Trabecular meshwork gene expression after selective laser trabeculoplasty. PLoS One. 2011;6:e20110.
8. Alvarado JA, Yeh RF, Franse-Carman L, Marcellino G, Brownstein MJ. Interactions between endothelia of the trabecular meshwork and of Schlemm’s canal: a new insight into the regulation of aqueous outflow in the eye. Trans Am Ophthalmol Soc. 2005;103:148–162.
9. Alvarado JA, Katz LJ, Trivedi S, Shifera AS. Monocyte modulation of aqueous outflow and recruitment to the trabecular meshwork following selective laser trabeculoplasty. Arch Ophthalmol. 2010;128:731–737.
10. Bradley JM, Anderssohn AM, Colvis CM, et al. Mediation of laser trabeculoplasty-induced matrix metalloproteinase expression by IL-1beta and TNFalpha. Invest Ophthalmol Vis Sci. 2000;41:422–430.
11. Parshley DE, Bradley JM, Samples JR, Van Buskirk EM, Acott TS. Early changes in matrix metalloproteinases and inhibitors after in vitro laser treatment to the trabecular meshwork. Curr Eye Res. 1995;14:537–544.
12. Parshley DE, Bradley JM, Fisk A, et al. Laser trabeculoplasty induces stromelysin expression by trabecular juxtacanalicular cells. Invest Ophthalmol Vis Sci. 1996;37:795–804.
13. Bylsma SS, Samples JR, Acott TS, Pirouzkar B, Van Buskirk EM. DNA replication in the cat trabecular meshwork after laser trabeculoplasty in vivo. J Glaucoma. 1994;3:36–43.
14. Kimpel MW, Johnson DH. Factors influencing in vivo trabecular cell replication as determined by 3H-thymidine labelling; an autoradiographic study in cats. Curr Eye Res. 1992;11:297–306.
15. Dueker DK, Norberg M, Johnson DH, Tschumper RC, Feeney-Burns L. Stimulation of cell division by argon and Nd: yAGlaser trabeculoplasty in cynomolgus monkeys. Invest Ophthalmol Vis Sci. 1990;31:115–124.
16. Acott TS, Samples JR, Bradley JM, Bacon DR, Bylsma SS, Van Buskirk EM. Trabecular repopulation by anterior trabecular meshwork cells after laser trabeculoplasty. Am J Ophthalmol. 1989;107:1–6.
17. Bylsma SS, Samples JR, Acott TS, Van Buskirk EM. Trabecular cell division after argon laser trabeculoplasty. Arch Ophthalmol. 1988;106:544–547.
18. Scheie HG. Width and pigmentation of the angle of the anterior chamber; a system of grading by gonioscopy. AMA Arch Ophthalmol. 1957;58:510–512.
19. Bahler CK, Howell KG, Hann CR, Fautsch MP, Johnson DH. Prostaglandins increase trabecular meshwork outflow facility in cultured human anterior segments. Am J Ophthalmol. 2008;145:114–119.
20. SooHoo JR, Seibold LK, Ammar DA, Kahook MY. Ultrastructural changes in human trabecular meshwork tissue after laser trabeculoplasty. J Ophthalmol. 2015;2015:476138. doi:10.1155/2015/476138
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.