Back to Journals » Psychology Research and Behavior Management » Volume 15
More Positive Emotion, Less Stress Perception?
Authors Lin Y, Wang J, Liu W ![]() , Jia Y
, Jia Y
Received 22 July 2022
Accepted for publication 26 October 2022
Published 19 December 2022 Volume 2022:15 Pages 3721—3732
DOI https://doi.org/10.2147/PRBM.S381964
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Ying Lin,1 Jing Wang,2,3 Weizhi Liu,2– 4 Yanpu Jia2,3
1China Executive Leadership Academy-Pudong, Shanghai, 201204, People’s Republic of China; 2Lab for Post-Traumatic Stress Disorder, Faculty of Psychology and Mental Health, Naval Medical University, Shanghai, 200433, People’s Republic of China; 3The Emotion & Cognition Lab, Faculty of Psychology and Mental Health, Naval Medical University, Shanghai, 200433, People’s Republic of China; 4Key Laboratory of Molecular Neurobiology of the Ministry of Education, Naval Medical University, Shanghai, 200433, People’s Republic of China
Correspondence: Yanpu Jia, The Emotion & Cognition Lab, Faculty of Psychology and Mental Health, Naval Medical University, #800 Xiangyin Road, Shanghai, 200433, People’s Republic of China, Email [email protected] Weizhi Liu, Lab for Post-Traumatic Stress Disorder, Faculty of Psychology and Mental Health, Naval Medical University, #800 Xiangyin Road, Shanghai, 200433, People’s Republic of China, Tel/Fax +86-21-81871671, Email [email protected]
Purpose: Shanghai, a mega-city with a population of 25 million, was becoming the first city in mainland China to erupt in the Omicron pandemic. The pandemic and the quarantine measures of whole city static management brought out big challenges for the population. This study sought to examine the psychological impact of such quarantine measures.
Methods: A cross-sectional study was conducted in China between April 8 to April 14, 2022. The survey contained inventories of stress perception, emotion states, duration of quarantine, and demographic characteristics. A total of 1,051 participants in Shanghai who were quarantined at home were included by random sampling.
Results: We found moderate-to-mild perceived stress (3.248± 1.936) and emotion states (3.453± 2.094). Individuals with high negative emotions had high levels of perceived stress. Specifically, the population aged 30– 49, female, with higher household income, staying with the elderly or children, were more likely to report high stress and negative emotion. Hierarchical regression and the further path analysis indicated that emotion states partially mediated the relationship between quarantined days at home and perceived stress.
Conclusion: There was a moderate-to-mild level of perceived stress and emotion when quarantined at home for an average of 20 days in Shanghai. The present findings implicated more positive emotion then less stress perception at the same duration of quarantine. It was suggested to consider the measures taken to construct positive emotions for the public to overcome negativity and bring out a virtuous circle to thrive, if the quarantine has to be continued for preventing the pandemic.
Keywords: omicron pandemic, zero-COVID policy, perceived stress, emotion states, quarantine at home
Introduction
The increasing menace of the epidemic led to an international public health emergency for the world with the evolution of COVID-19 variants. Shanghai, a mega-city with a resident population of about 25 million, ushered in the impact of the Omicron variants in early March 2022. In terms of the basic reproductive number R0 (the average number of people infected by one infectious person during the infection period), Omicron was the environmental stability with high infectiousness,1 compared with the SARS-CoV-2de and the Delta variety. As a result of this pandemic in Shanghai, the number of new infections cases in a single day reached as high as 27,605. As of May 4, the cumulative infections in the whole city were 601,942, including 547,056 cases without pulmonary symptoms, and a total of 503 deaths.2 In order to stop the spread of the epidemic as soon as possible, with the zero-COVID policy,3 “whole city static management” was announced on March 28 in Shanghai. By April 1, 25 million people began to quarantine at home. The city locked down with traffic stoppage, markets closure, production suspension, logistics shutdown, online learning, and so on.
In this situation, people were facing huge challenges not only physically but also mentally both cross-sectionally4,5 and longitudinally.6 Most studies reported a negative psychological impact of quarantine, such as fear,7 anxiety and anger,8,9 emotional distress,10 symptoms of depression,11 symptoms of acute stress disorder,12,13 and post-traumatic stress symptoms.14 In quarantine, health care workers were more likely to suffer psychological consequences such as Post-Traumatic Stress Disorder (PTSD) than the general population.15 Frontline workers reported higher scores for stress, emotional exhaustion, and depersonalization as compared to colleagues working in units not directly serving patients with COVID-19.16 A few studies have discussed the effect of policy stringency on public mental health during quarantine. A recent one reviewed the data of the COVID-19 pandemic in 15 countries from April 2020 to June 2021, indicating that more stringent policies were associated with poorer mental health, and maintaining social distance was more closely associated with poor mental health than closing schools, workplaces, public transport, canceling public events, and restricting domestic travel.17 Consequently, the present study was concerned with the psychological impact of such quarantine measures which inevitably affected people’s daily life and social distance.
The mental health of the public during the quarantine may be caused by COVID-19, the pandemic itself, or by the measures of quarantine, or the result of the combination of both factors. Risk factors related to the pandemic itself (eg, contact history of COVID-19, risk perception, exposure to COVID-19 at work) had been identified as related to public mental health in China.18–20 Several characteristics of participants associated with negative psychological impacts were reported, such as younger age (16–24 years), female, lower levels of formal educational qualifications, lower household income, and having one child as opposed to no children.18,21 Analysis on effect of lockdown in Australia found that the lockdown was associated with a modest negative change in overall population mental health, and women were more likely to have adverse mental health outcomes, especially those aged 20–29 years old.22 Government and staff should pay special attention to the mental health of those susceptible populations during the outbreak of COVID-19.
Studies on stressors during quarantine showed what was associated with poorer mental health were duration of quarantine,9,23 fears of infection and concerns about its effects on family,24–26 inadequate basic supplies (eg, food, water, clothes, or accommodation),27 insufficient clear guidelines about actions to take and confusion about the purpose of quarantine from public health authorities,13,28 economic uncertainty, especially in vulnerable groups,29 etc. Whether it has a psychological impact or not, the social effects of lockdown measures such as concerns over availability of food and household goods and social isolation were present as important stressors.24,29 In addition, emotion states and stress were related and often discussed, especially in special circumstances. One study confirmed the efficacy of a brief online form of Emotional Freedom Techniques in the prevention of stress, anxiety, and burnout in nurses involved in the treatment of COVID patients.30 In order to reduce the stress of the masses during the quarantine period, it was necessary to understand related risk factors and underlying mechanisms.
Although emotion and stress were discussed as the public psychological impact of quarantine in previous studies, it seems little known about the psychological mechanisms underlying the mental health problems related to the COVID-19 pandemic.31 To our knowledge, few studies have explored the relationship between emotion states and stress perception in quarantine. Therefore, the present study would like to explore what and how this citywide, involving 25 million people, long-term quarantine in Shanghai affects public psychology in a pandemic. It was hypothesized that emotion states might play a moderating role on the relations between quarantine measures and stress perception. Based on the results of the present study, further measures can be taken to mitigate the negative consequences of the quarantine on public mental health.
Methods
Participants and Procedure
An online survey was conducted in Chinese by the Questionnaire Star platform (https://www.wjx.cn) to recruit participants between April 8 and April 14, 2022. At that time, it had been nearly 2 weeks since March 28 when the city started lockdown, and before that there were a considerable number of buildings and communities already in quarantine at home during the pandemic spreading. The survey was mainly distributed to the society through daily broadcasting on WeChat groups and psychological service institutions. On opening the link of the survey, there was an announcement to clarify the purpose of the study and then all the items for the study for those who volunteered to respond. This design was to make the participants clear about what private information needed to be provided before they decided to join in. Therefore, all participants were entirely voluntary and informed consent was obtained from the study participants prior to study commencement. This study was approved by the ethics committee of the Naval Medical University . All procedures were in accordance with the Helsinki Declaration.
We received responses from 1,320 participants and finally a total of 1,051 were included (626 males and 425 females). The inclusion criteria involved 1) willing to accept the investigation; 2) located in Shanghai; 3) normal levels of speech, comprehension, and expression. Then 219 were deleted because of not meeting the inclusion criterion, and 50 more were deleted for too many missing values (38 removed) or spending more than 30 minutes or less than 2 minutes to respond to the survey (12 removed). Supplementary Figure S1 is a flow diagram showing the selection process.
Measures
Demographic Characteristics
Age, gender, occupation, education, annual household income, stay with elderly or not, and stay with children or not were included in the questionnaire as demographic characteristics.
Duration of Quarantine
This was measured by quarantined days at home, which the participants would calculate and fill in according to the individual situation by the date of answering the questionnaire.
Stress Perception
We calculated quarantine stress at home for the participants as individual’s subjective feeling about the state of life in the meantime. It was assessed by 10 items involving the general stress perception and nine specific perceptions on the stressors including living provisions, risk of infection, family dysfunction, children learning online, medical or medicine demand, economic income, negative information, cramped space, and working load at home, which were integrated from the previous studies24,27,32 and were included according to the actual situation in Shanghai during quarantine. All perceptions were rated on a 9-point Likert scale ranging from 1 (no stress at all) to 9 (an enormous stress). The average score of 10 items was calculated to represent the state of stress perception, meaning people with higher scores had higher perceived stress.
Emotion States
We tried to make an emotional states inventory adapted to the non-clinical groups, which was not only focusing on the negative subjective experience of individuals, but also involving the disappearance of pleasure which is the core component of depression.33 Seven items with emotion states of binary opposites were included as orderly–flustered, calmed–jittery, delighted–indignant, meaningful–meaningless, active to social interaction–lonely, interested–bored, and hopeful–hopeless, with one side positive and the other side negative on a continuous axis. These emotion states were referenced to the State/Trait Depression Scale in Chinese Version (STDEP)33 and the Positive and Negative Affect Scale (PANAS). All items were rated on a 9-point Likert scale ranging from 1 (positive state) to 9 (negative state), with the instruction as “Scoring from 1 to 9 to express your psychological feelings since pandemic quarantine at home”. The average score of seven items was calculated to represent the state of emotion, meaning people with a higher score had more negative emotions.
Statistical Analysis
Statistical analysis was performed using IBM SPSS version 21.0. A two-tailed test was used, and p<0.05 was considered as statistically significant. Descriptive and frequency statistics (mean, [SD] and percentages) were used to describe baseline demographic information. First, descriptive statistics were calculated for the demographic variables, the average score of different perceived stresses, and negative emotion states of population. Then, one-way analysis of variance (ANOVA) was used to analyze the perceived stress and negative emotion state between different demographic categories. Next, hierarchical regression analysis was used to determine the independent variables related to perceived stress. Last, mediation analyses were conducted to determine the potential mediating effect on the relationship between quarantined days at home and perceived stress.
Results
Demographic Information of Participants
A total of 1,101 people were recruited to complete the survey. Of the 1,101 respondents, 38 participants were removed due to too many missing values or illogical answers (for example, all choices were one or zero), and 12 were removed due to spending more than 30 minutes or less than 2 minutes answering the questionnaire. Therefore, 1,051 participants were included in this analysis. As illustrated in Table 1, the average days of being quarantined at home were 20.08±8.411. The sample comprised 626 males and 425 females with an average age of 32.38±11.112 years and an average annual household income of 273.45±27.075. Most of these participants were bachelor degree (30.7%) level of education. There were 151 (14.4%) students and retired or unemployed personnel, 229 (21.8%) specialized persons (eg, teacher, doctor, government related staff), 206 (19.6%) company employees or managers, 388 (36.9%) military personnel, and 77 (7.3%) other occupations (eg, service workers, freelancer, no response). A total of 208 (19.8%) participants lived with the elderly and 439 (41.8%) lived with children when quarantined at home.
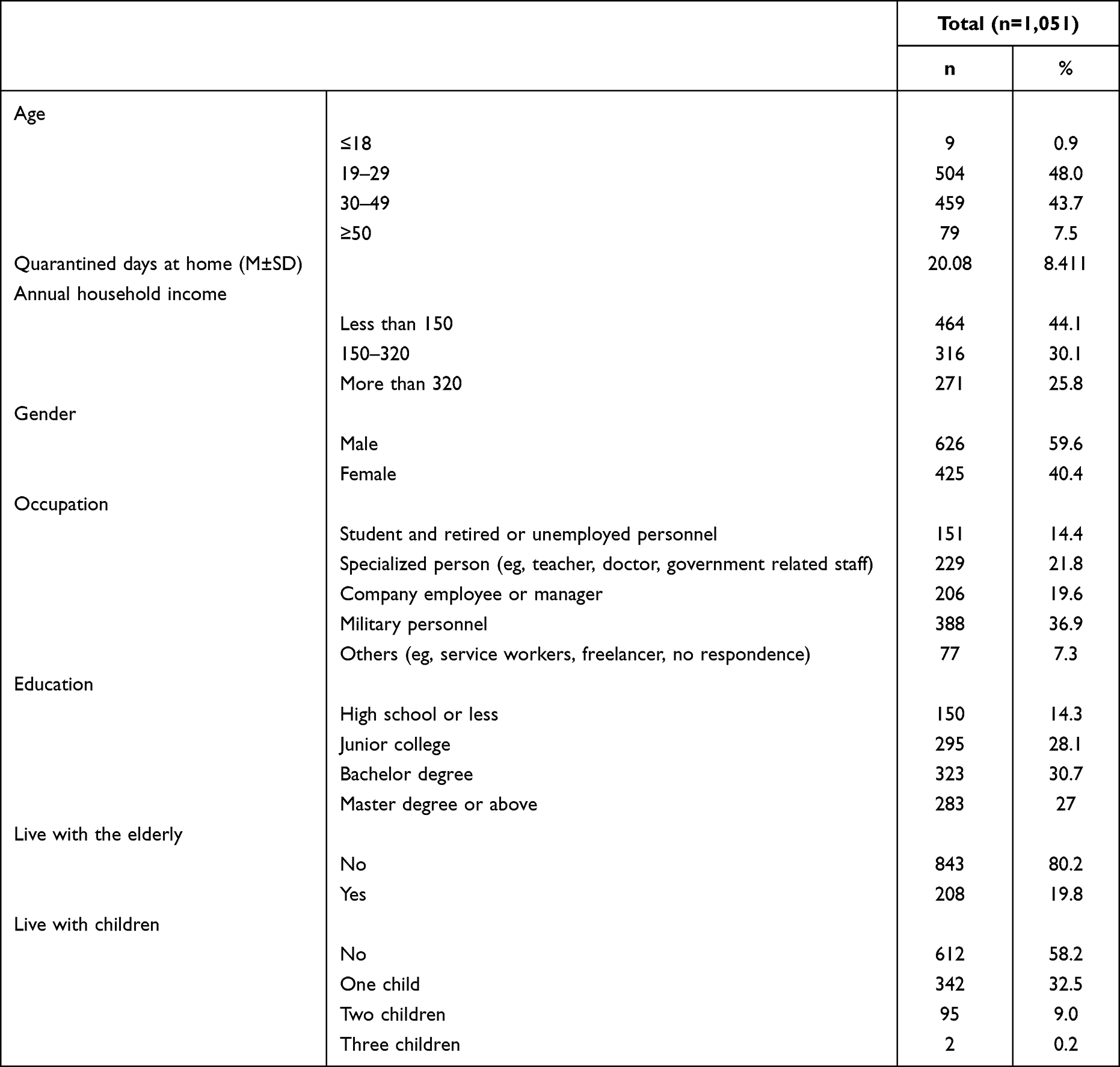 |
Table 1 Demographic Information of Participants |
Perceived Stress and Emotion States During Quarantine at Home
The average scores of different perceived stress and emotion states are shown in Figures 1 and 2, respectively. The average score of different perceived stress were 3.248±1.936, while emotion states were 3.453±2.094. During quarantine at home due to COVID-19, the participants reported moderate-to-mild perceived stress and emotions, regardless of the type. In detail, the stress from living provisions was significantly higher than others, and the stress from children’s learning was reported the lowest. It was reported that the negative emotion state of flustered, jittery, indignant, meaningless, lonely, bored, and hopeless, were 3.4, 3.53, 3.67, 3.73, 3.01, 3.31, and 3.51, respectively. Supplementary Materials Figure S2 shows a scatterplot of perceived stress and emotion states for every participant. There was a significant relationship between perceived stress and emotion states, suggesting that individuals with high negative emotions also had high levels of perceived stress.
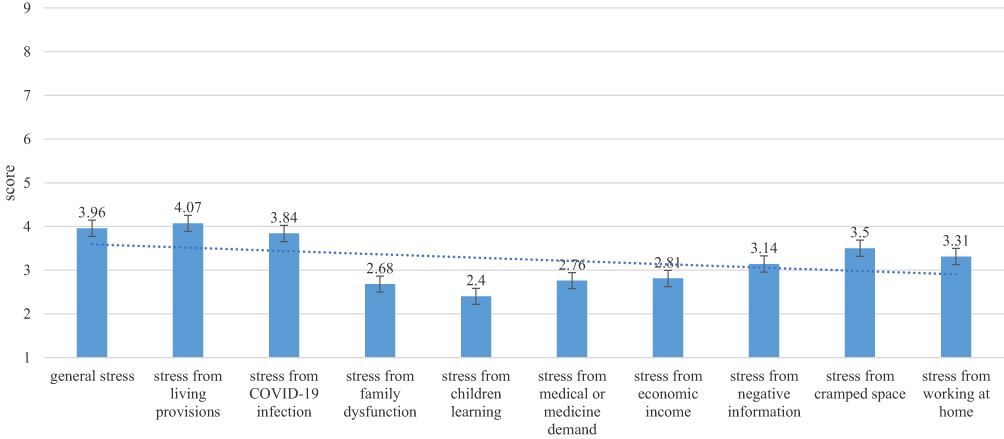 |
Figure 1 The average score of different perceived stress. |
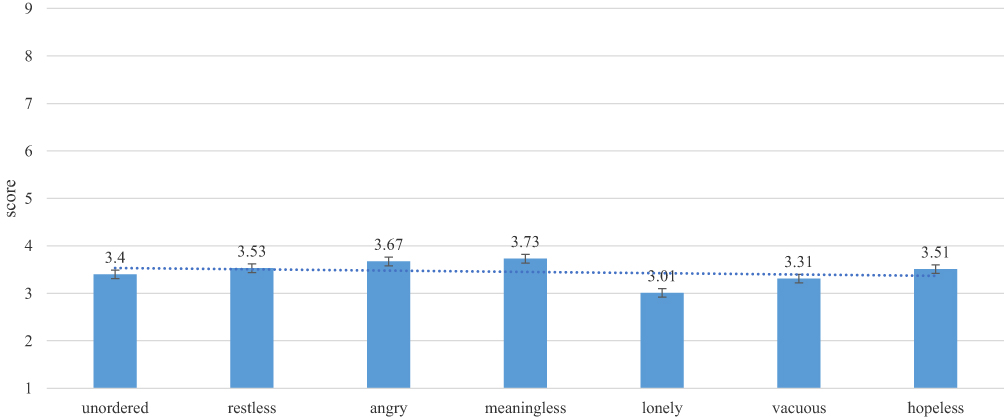 |
Figure 2 The average score of different negative emotion states. |
Profile of Perceived Stresses and Emotion States in Different Demographic Categories
The effect of demographic categories on the perceived stress and emotion state was analyzed (Table 2). The average score of perceived stress of participants at the age of 30–49 years (4.271±1.783) was significantly higher than at the age of ≤18 (p=0.023), 19–29 (p<0.001), and ≥50 (p=0.014). And the average score of emotional state of participants at the age of 30–49 years (4.504 ± 1.842) was significantly higher than at the age of ≤18 (p=0.011) or 19–29 (p<0.001). Those with more quarantined days at home had higher perceived stress (F=50.494, p<0.001) and a more negative emotional state (F=42.410, p<0.001) than those with less days. In terms of sampling dates, the change of perceived stress and negative emotional state similarly supported that perceived stress and negative emotion would increase over time during home quarantine, which is shown in Supplementary Materials Figure S3 in detail. Females had higher perceived stress (F=215.836, p<0.001) and a more negative emotional state (F=208.349, p<0.001) than males. There were significant differences between different income subgroups, meaning participants with an income of more than 320,000 exhibited higher perceived stress (p<0.001) and a more negative emotional state (p<0.001) than other income categories. The perceived stress of specialized people (eg, teacher, doctor, government related staff) was marginally significant when compared with company employees or managers (p=0.054), but significantly higher than other occupations. In terms of negative emotion state, specialized people (eg, teacher, doctor, government related staff) registered as significantly higher than other occupations, but significantly lower than company employees or managers (p=0.008). Those living with the elderly during quarantined days showed higher perceived stress (F=106.151, p<0.001) and negative emotional state (F=64.069, p<0.001). Similarly, those living with children during quarantined days showed higher perceived stress (F=102.778, p<0.001) and negative emotional state (F=78.027, p<0.001), regardless of the number of children.
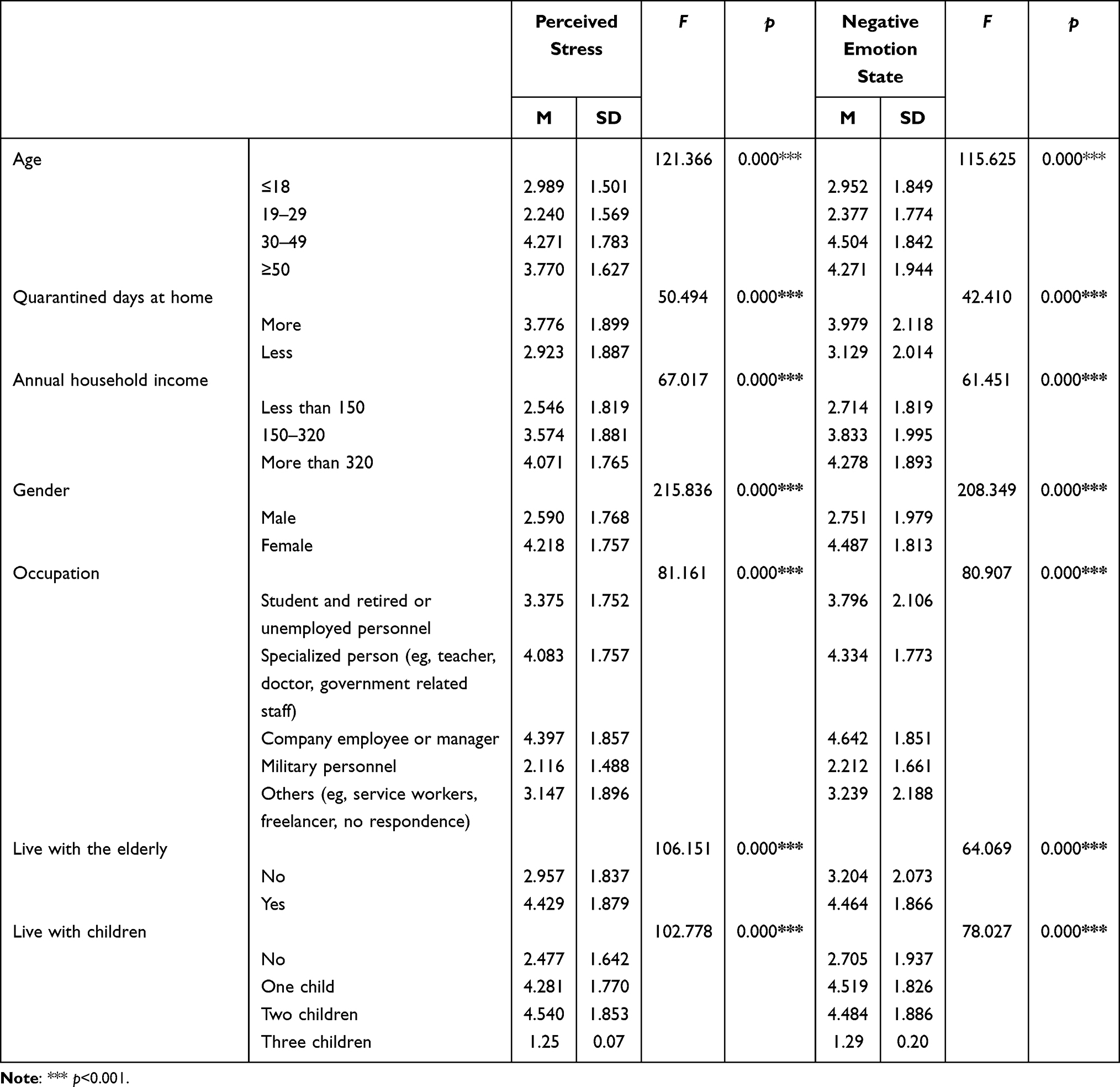 |
Table 2 Perceived Stress and Negative Emotion State by Demographic Information |
Factors Related to Perceived Stress
According to the results of ANOVA, we selected the significant characteristics and incorporated them into the hierarchical regression model. The results of the hierarchical regression analysis are listed in Table 3. In the first step, the gender and occupation variables were included accounting for 27% of the variance in perceived stress. In the second step, “live with the elderly”, “live with children”, and “quarantined days at home” were included in the model, and “female” “live with the elderly or children” and “quarantined days at home” had significant effects on the perceived stress. For the occupation, specialized person (eg, teacher, doctor, government related staff) had significantly higher perceived stress than other occupations besides company employees or managers. These features accounted for 31.2% of the variance. In the third step, emotion categories were included, accounting for 59.3% of the difference in the results. Female (β=0.076, p=0.002), living with the elderly (β=0.087, p<0.001), living with children (β=0.121, p<0.001), middle emotion state (β=0.515, p<0.001), and high emotion state (β=0.395, p<0.001) were positively correlated with perceived stress. Even though when we picked out the top three perceived stresses as dependent variables, such results also supported the influence of being female (p<0.001), living with the elderly (p<0.001) and living with children (p<0.001). This is detailed in Supplementary Materials Figure S4–S6.
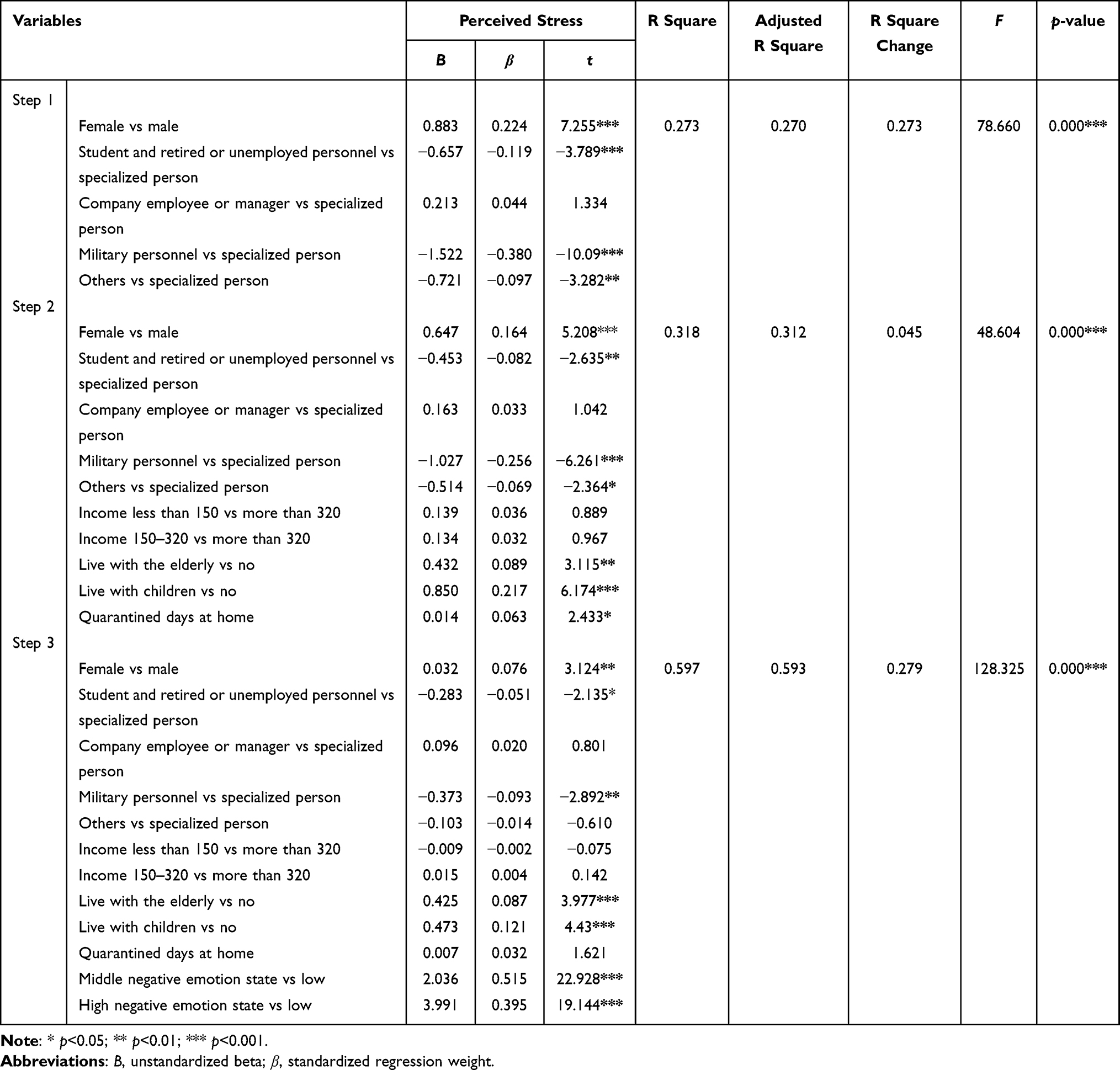 |
Table 3 Regression Analyses with Perceived Stress Score as the Dependent Variable |
The Mediating Effect of Emotion States on the Relationship Between Quarantined Days at Home and Perceived Stress
The results of ANOVA suggest that those with more quarantined days at home had higher perceived stress (F=50.494, p<0.001) and negative emotional state (F=42.410, p<0.001). Moreover, the hierarchical regression model 2 showed “quarantined days at home” had significant effects on the perceived stress. However, this significance was not noted when emotion categories were included in the third step. Therefore, it was assumed the existence of emotion state would influence the relationship between quarantined days at home and perceived stress. Thus, mediation analyses were further conducted to determine the relationship between emotion state, quarantined days at home, and perceived stress.
The average score of perceived stress was entered into the mediation model as a dependent variable, with emotion states as a possible mediator and quarantined days at home as a predictor. There were significant direct effects whereby more quarantined days at home was associated with a more negative emotional state (coefficient=0.018, p=0.015) and emotion state predicted perceived stress (coefficient=0.759, p<0.001). The direct effect from quarantined days at home to perceived stress was significant (coefficient=0.010, p=0.017). There was a significant indirect effect from quarantined days at home to perceived stress through emotion state (coefficient=0.0142, 95% confidence interval of Bootstrap test=[0.003, 0.026]). Coefficient of the total effect was 0.024 with a p-value at 0.001. The result of path analysis indicated that emotion state mediated the relationship between quarantined days at home and perceived stress (Figure 3).
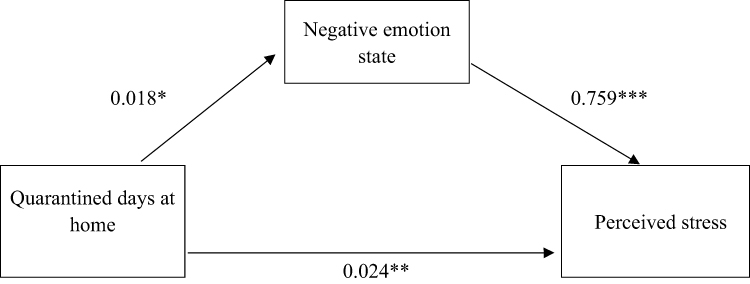 |
Figure 3 Negative emotion state mediates the relationship between quarantined days at home and perceived stress. Note: * p<0.05; ** p<0.01; *** p<0.001. |
Discussion
The current study aimed to investigate public psychology under the Shanghai quarantine at home and explore related risk factors on perceived stress. Results showed that the perceived stress on all sources and the emotional states of the public were moderate-to-mild. And there existed a significant relationship between perceived stress and negative emotion states, suggesting that individuals with high negative emotions also had high levels of perceived stress. Specifically, the population aged 30–49, female, with higher household income, staying with the elderly or children, were more likely to report high stress and negative emotion. Hierarchical regression and the further path analysis indicated that emotion states partially mediated the relationship between quarantined days at home and perceived stress.
Compared with the previous study that reported the psychological impact as moderate-to-severe during the initial phase of the outbreak of COVID-19 in China,20 the moderate-to-mild results here seemed to indicate less psychological impact of quarantine in Shanghai. This result might relate with the different measures of emotion states, low risk perception on the Omicron pandemic, and a comparatively short duration of quarantine (13–29 days, with Mean equal to 20.08±8.411) in this study. Inconsistent with the previous finding that participants worried about their family members contacting COVID-19,20 we found low risk perception on pandemic as the less stress perception from COVID-19 infection compared with stress from living provision and the general stress. This was confirmed when we further asked the participants to rank the ten stressors according to the stress perceptions changed most after quarantine at home, and mark the top three in order as 1–3, in which we found COVID-19 infection was ranked to a less important stressor compared with living provision. In other previous studies, fear seems more certainly a consequence of mass quarantine7 and social isolation was the main stressor during the pandemic.24 Inconsistently, we found the top three negative emotions were meaningless, indignant, and jittery, and the lowest score of lonely with more active to social interaction during the quarantine, which might also implicate the low risk of perception on pandemic or risk perception not as a most important stressor during the quarantine.
One of the main influencing factors of public psychology was the duration of quarantine.9,23 It was also proved in the present study that the longer the duration of quarantine, the higher perceived stress and more negative emotional state. During the COVID-19 pandemic, there is an urgent need to study the immediate psychological impact on the workforce who returned to work. Study emphasized that 10.8% of the workforce met the diagnostic criteria for PTSD just returning to work after lockdown and quarantine in Chongqing.34 Therefore, against the background of the normalization of the epidemic, governments, and company administrators to be aware of the extent and factors associated with stress, emotion states, and other mental health among members of the workforce when they just returned to work after quarantine and lockdown during the COVID-19 pandemic.
Females were more likely to report high stress and negative emotions. This was consistent with the previous findings, whether in China20 or other countries.4 Individuals aged 30–49 were more likely to experience a higher stress and negative emotions. Middle-aged adults are also high-risk groups for COVID-19 due to the start of decreasing function and chronic underlying diseases that may weaken the immune systems. However, the results were different from some previous studies, in which younger age (16–24 years) and lower household income were reported as the characteristics of participants associated with negative psychological impacts.18,21 Future studies should further explore inconsistent results with respect to age.
According to the result of hierarchical regression analysis, it was assumed the existence of emotion state would influence the relationship between quarantined days at home and perceived stress. And path analysis confirmed a mediating effect of emotion state on the relationship between quarantined days at home and perceived stress. To be specific, the existence of more positive emotions might bring out less perceived stress at the same duration of quarantine. Positive emotions like orderly, calmed, focused, meaningful, appreciative, interested, hopeful, esteem, love et al, would benefit individuals to overcome negativity, and bring out a virtuous circle to thrive.35 Given the mediating role of emotion state, interventions targeting it would contribute to stress reduction during quarantine. This is also consistent with previous studies. For example, one study confirmed the efficacy of a brief online form of Emotional Freedom Techniques in the prevention of stress, anxiety, and burnout in nurses involved in the treatment of COVID patients.30 To address the needs of the general population during a future pandemic, it is worthwhile to contemplate the use of online cognitive behavior therapy (CBT) or smartphone-based psychoeducation to promote mental wellness under quarantine. It was suggested that CBT can mitigate maladaptive coping behaviors such as avoidance, antagonistic confrontation, and self-blame by enhancing their ability to manage stress.36 A meta-analysis showed digital CBT significantly reduces insomnia severity index at post-intervention.37 As a result, such online psychological interventions were warrant in facing future epidemics.
Strengths and Limitations
Firstly, up to now, no mega-city has conducted such a global static management with high compulsion like Shanghai in China, which has been quarantined for almost 3 months, while all people’s work and learning activity have been carried out online at home. Moreover, the effectiveness of this pandemic prevention in Shanghai may make a difference to the subsequent pandemic prevention strategy in mainland China. Secondly, although emotion and stress were discussed as the public psychological impact of quarantine in previous studies, most usually focused on one or a few particular emotional problems or stressors perception, which were nearly all negative impacts. In the current study, more comprehensive dimensions of stress sources were included and the quarantine actuality was paid more attention.
While there existed certain strengths, some limitations still need to be discussed. First, we conducted a cross-sectional study on the public psychology during the quarantine in Shanghai from April 8 to 14, with an average quarantine duration of 20 days. The quarantine lasted nearly 3 months and the emotion states and perceived stress of the public might have changed over this period. In spite of this limitation, the results of the present study did reflect the true mentality of the participants who had been quarantined at home for an average of 20 days under the pandemic preventing measure of global static management in Shanghai. Second, the standard scales to assess the emotion state such as depression and anxiety was not used in the current study, but constructing an instrument with seven emotion states of binary opposites and asking the participants to rate on a 9-point Likert scale ranging from 1 (positive state) to 9 (negative state). This might limit the comparison with the results of previous researches. But, from another side, it was a way to avoid the limitation that the public could only report the negative subjective experiences but not present the actual emotion state under the certain context of quarantine, such as some degree of disappearance of positive emotion. In such special circumstances of prolonged isolation cases, it remains to be explored whether this would better describe emotional states and be more suitable for the general population. Third, the information of past history of COVID of participants was not collected. Given the important impact of infection history on mental health, it should also be an important factor for perceived stress. Future research should focus on the important role of COVID infection history.
Conclusion
The pandemic and the quarantine measures brought out a big challenge for Shanghai, a mega-city with a population of 25 million in China. We focused on the psychological impact of such quarantine measures which inevitably affected people’s daily life and social distance. The results showed that the perceived stress and the emotional states of the public were moderate-to-mild, and there existed a significant relationship between perceived stress and negative emotion states. The population aged 30–49, female, with higher household income, staying with the elderly or children were positively associated with a higher level of stress and negative emotion states. There existed a mediating effect of emotion state on the relationship between quarantined days at home and perceived stress, which implicated more positive emotions and less stress perception at the same duration of quarantine. It was suggested to consider the measures taken to construct positive emotions for the public to overcome negativity and bring out a virtuous circle to thrive, as the quarantine has to be continued for preventing the pandemic.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author.
Ethics Approval and Consent to Participate
This study was approved by the ethics committee of Naval Medical University and the informed consent obtained from the study participants prior to study commencement. All procedures were in accordance with the Helsinki Declaration.
Acknowledgments
The authors would like to acknowledge the volunteers who participated in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; have taken part in drafting, revising or critically reviewing the article; have reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage; have agreed to take responsibility and be accountable for the contents of the article.
Funding
The “13th Five-Year” Dual Construction Project (2020SZ15); Innovative Research Team Project (20200106); Science and Technology Supply Project (2020JY17); Special Project for Research and Development of Medical Science for FW (19WLMS-15).
Disclosure
The authors declared that they have no conflicts of interest.
References
1. Hirose R, Itoh Y, Ikegaya H, et al. Differences in environmental stability among SARS-CoV-2 variants of concern: both omicron BA.1 and BA.2 have higher stability. Clin Microbiol Infect. 2022;28(11):1486–1491. doi:10.1016/j.cmi.2022.05.020
2. Zhang X, Zhang W, Chen S. Shanghai’s life-saving efforts against the current omicron wave of the COVID-19 pandemic. Lancet. 2022;399(10340):2011–2012. doi:10.1016/S0140-6736(22)00838-8
3. Chen JM, Chen YQ. China can prepare to end its zero-COVID policy. Nat Med. 2022;28(6):1104–1105. doi:10.1038/s41591-022-01794-3
4. Le XTT, Dang AK, Toweh J, et al. Evaluating the psychological impacts related to COVID-19 of Vietnamese people under the first nationwide partial lockdown in Vietnam. Front Psychiatry. 2020;11:824. doi:10.3389/fpsyt.2020.00824
5. Gostin LO, Wiley LF. Governmental public health powers during the COVID-19 pandemic: stay-at-home orders, business closures, and travel restrictions. JAMA. 2020;323(21):2137–2138. doi:10.1001/jama.2020.5460
6. Wang C, Pan R, Wan X, et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav Immun. 2020;87:40–48. doi:10.1016/j.bbi.2020.04.028
7. Lima CKT, Carvalho PMM, Lima IAAS, et al. The emotional impact of Coronavirus 2019-nCoV (new Coronavirus disease). Psychiatry Res. 2020;287:112915. doi:10.1016/j.psychres.2020.112915
8. Jeong H, Yim HW, Song YJ, et al. Mental health status of people isolated due to middle east respiratory syndrome. Epidemiol Health. 2016;38:e2016048. doi:10.4178/epih.e2016048
9. Marjanovic Z, Greenglass ER, Coffey S. The relevance of psychosocial variables and working conditions in predicting nurses’ coping strategies during the SARS crisis: an online questionnaire survey. Int J Nurs Stud. 2007;44(6):991–998. doi:10.1016/j.ijnurstu.2006.02.012
10. Yoon MK, Kim SY, Ko HS, et al. System effectiveness of detection, brief intervention and refer to treatment for the people with post-traumatic emotional distress by MERS: a case report of community-based proactive intervention in South Korea. Int J Ment Health Syst. 2016;10:51. doi:10.1186/s13033-016-0083-5
11. Liu X, Kakade M, Fuller CJ, et al. Depression after exposure to stressful events: lessons learned from the severe acute respiratory syndrome epidemic. Compr Psychiatry. 2012;53(1):15–23. doi:10.1016/j.comppsych.2011.02.003
12. Bai Y, Lin CC, Lin CY, et al. Survey of stress reactions among health care workers involved with the SARS outbreak. Psychiatr Serv. 2004;55(9):1055–1057. doi:10.1176/appi.ps.55.9.1055
13. DiGiovanni C, Conley J, Chiu D, et al. Factors influencing compliance with quarantine in Toronto during the 2003 SARS outbreak. Biosecur Bioterror. 2004;2(4):265–272. doi:10.1089/bsp.2004.2.265
14. Sprang G, Silman M. Posttraumatic stress disorder in parents and youth after health-related disasters. Disaster Med Public Health Prep. 2013;7(1):105–110. doi:10.1017/dmp.2013.22
15. Rodríguez BO, Sánchez TL. The psychosocial impact of COVID-19 on health care workers. Int Braz J Urol. 2020;46(suppl.1):195–200. doi:10.1590/S1677-5538.IBJU.2020.S124
16. Di Giuseppe M, Nepa G, Prout TA, et al. Stress, burnout, and resilience among healthcare workers during the COVID-19 emergency: the role of defense mechanisms. Int J Environ Res Public Health. 2021;18(10):5258. doi:10.3390/ijerph18105258
17. Aknin LB, Andretti B, Goldszmidt R, et al. Policy stringency and mental health during the COVID-19 pandemic: a longitudinal analysis of data from 15 countries. Lancet Public Health. 2022;7(5):e417–e426. doi:10.1016/S2468-2667(22)00060-3
18. Xu J, Wang X, Xuan Z, et al. Factors related to perceived stress during the COVID-19 epidemic context among the general population in China: a cross-sectional nationwide study. J Affect Disord. 2021;294:816–823. doi:10.1016/j.jad.2021.07.097
19. Sun L, Sun Z, Wu L, et al. Prevalence and risk factors for acute posttraumatic stress disorder during the COVID-19 outbreak. J Affect Disord. 2021;283:123–129. doi:10.1016/j.jad.2021.01.050
20. Wang C, Pan R, Wan X, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in china. Int J Environ Res Public Health. 2020;17(5):1729. doi:10.3390/ijerph17051729
21. Taylor MR, Agho KE, Stevens GJ, et al. Factors influencing psychological distress during a disease epidemic: data from Australia’s first outbreak of equine influenza. BMC Public Health. 2008;8:347. doi:10.1186/1471-2458-8-347
22. Butterworth P, Schurer S, Trinh TA, Vera-Toscano E, Wooden M. Effect of lockdown on mental health in Australia: evidence from a natural experiment analysing a longitudinal probability sample survey. Lancet Public Health. 2022;7(5):e427–e436. doi:10.1016/S2468-2667(22)00082-2
23. Reynolds DL, Garay JR, Deamond SL, et al. Understanding, compliance and psychological impact of the SARS quarantine experience. Epidemiol Infect. 2008;136(7):997–1007. doi:10.1017/S0950268807009156
24. Brooks SK, Webster RK, Smith LE, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. 2020;395(10227):912–920. doi:10.1016/S0140-6736(20)30460-8
25. Nelson LM, Simard JF, Oluyomi A, et al. US public concerns about the COVID-19 pandemic from results of a survey given via social media. JAMA Intern Med. 2020;180(7):1020–1022. doi:10.1001/jamainternmed.2020.1369
26. Desclaux A, Badji D, Ndione AG, et al. Accepted monitoring or endured quarantine? Ebola contacts’ perceptions in Senegal. Soc Sci Med. 2017;178:38–45. doi:10.1016/j.socscimed.2017.02.009
27. Wilken JA, Pordell P, Goode B, et al. Knowledge, attitudes, and practices among members of households actively monitored or quarantined to prevent transmission of Ebola virus disease - margibi county, Liberia: February-March 2015. Prehosp Disaster Med. 2017;32(6):673–678. doi:10.1017/S1049023X17006720
28. Braunack-Mayer A, Tooher R, Collins JE, et al. Understanding the school community’s response to school closures during the H1N1 2009 influenza pandemic. BMC Public Health. 2013;13:344. doi:10.1186/1471-2458-13-344
29. Van Lancker W, Parolin Z. COVID-19`, school closures, and child poverty: a social crisis in the making. Lancet Public Health. 2020;5(5):e243–e244. doi:10.1016/S2468-2667(20)30084-0
30. Dincer B, Inangil D. The effect of emotional freedom techniques on nurses’ stress, anxiety, and burnout levels during the COVID-19 pandemic: a randomized controlled trial. Explore. 2021;17(2):109–114. doi:10.1016/j.explore.2020.11.012
31. Li R, Kajanoja J, Lindblom J, et al. The role of alexithymia and perceived stress in mental health responses to COVID-19: a conditional process model. J Affect Disord. 2022;306:9–18. doi:10.1016/j.jad.2022.03.024
32. Hamel L, Lopes L, Muñana C, et al. How the supreme court’s Dobbs decision played in 2022 midterm election: KFF/AP votecast analysis; 2020. Available from: https://www.kff.org/.
33. Lei ZH, Xu R, Luo YJ, et al. Reliability and validity of the Chinese version of state-trait depression scale in college students. Chin Ment Health J. 2011;25(2):136–140. Chinese.
34. Tan W, Hao F, McIntyre RS, et al. Is returning to work during the COVID-19 pandemic stressful? A study on immediate mental health status and psychoneuroimmunity prevention measures of Chinese workforce. Brain Behav Immun. 2020;87:84–92. doi:10.1016/j.bbi.2020.04.055
35. Fredrickson B. Positivity: groundbreaking research reveals how to embrace the hidden strength of positive emotions, overcome negativity, and thrive. Libr J. 2009;134(2):84.
36. Ho CS, Chee CY, Ho RC. Mental health strategies to combat the psychological impact of coronavirus disease 2019 (COVID-19) beyond paranoia and panic. Ann Acad Med Singapore. 2020;49(3):155–160. doi:10.47102/annals-acadmedsg.202043
37. Soh HL, Ho RC, Ho CS, et al. Efficacy of digital cognitive behavioural therapy for insomnia: a meta-analysis of randomised controlled trials. Sleep Med. 2020;75:315–325. doi:10.1016/j.sleep.2020.08.020
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.